
Search
- Page Path
- HOME > Search
Research Article
- The effects of gingival blood flow on pulpal blood flow detection using ultrasound Doppler flowmetry: animal study
- Dohyun Kim, Hyoung-Seok Ko, Soo-Yeon Park, Seung-Yeon Ryu, Sung-ho Park
- Restor Dent Endod 2023;48(1):e9. Published online January 30, 2023
- DOI: https://doi.org/10.5395/rde.2023.48.e9
-
 Abstract
Abstract
 PDF
PDF PubReader
PubReader ePub
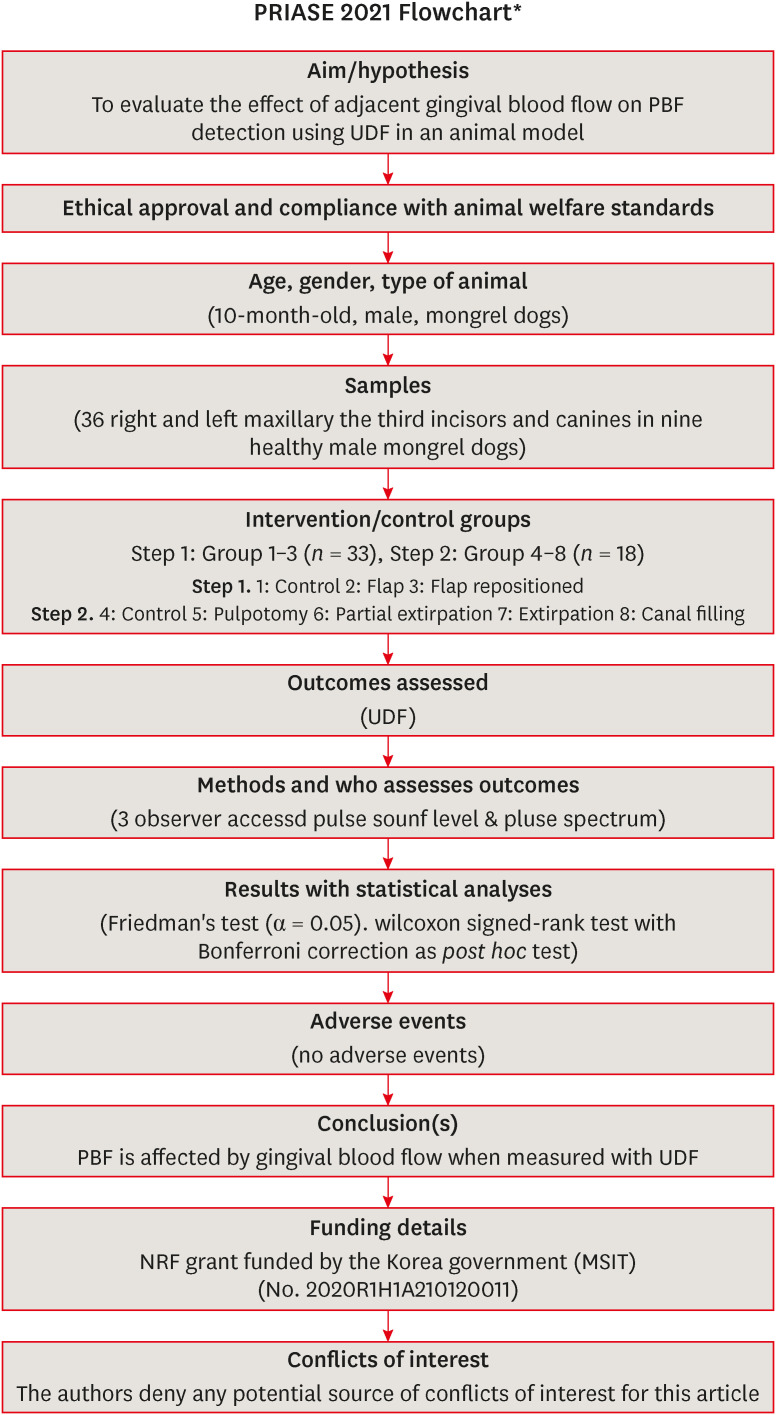
ePub Objectives This study evaluated the effect of adjacent gingival blood flow on detection of pulpal blood flow (PBF) using ultrasound Doppler flowmetry (UDF) through animal study.
Materials and Methods The study included 36 right and left maxillary the third incisors and canines in 9 experimental dogs. The study included 2 main steps: In the first step, the pulse sound level (PSL) was recorded on the cervical part of each tooth without flap elevation (Group 1), with flap elevation (Group 2), and after it was repositioned in place (Group 3). In the second step, the PSL was recorded on the cervical part of each tooth (Group 4), after pulpotomy (Group 5), after partial pulp extirpation (Group 6), after complete extirpation (Group 7), and after canal filling (Group 8). In Groups 5–8, the study was performed with and without flap elevation in the left and right teeth, respectively. The PSL was graded as follows: 0, inaudible; 1, heard faintly; and 2, heard well. The difference between each group was analyzed using Friedman’s test with Wilcoxon signed-rank tests (α = 0.05).
Results In step 1, the PSL results were Group 1 > 2 and 3. In step 2, there was no significant difference between the groups when the flap was not elevated, while PSL results were Group 4 > 5 ≥ 6 and 7 ≥ 8 when the flap was elevated.
Conclusions PBF is affected by gingival blood flow when measured with UDF. UDF measurements require isolation of gingiva from the tooth.
-
Citations
Citations to this article as recorded by
- Modern aspects of the use of hardware methods for diagnosing pulp vitality (Part 2. Non-traditional diagnostic methods)
K. V. Shadrina, L. Yu. Orekhova, V. D. Goncharov, V. Yu. Vashneva, E. S. Silina, E. V. Kosova, A. A. Petrov
Endodontics Today.2025; 23(3): 423. CrossRef - Exploring approaches to pulp vitality assessment: A scoping review of nontraditional methods
Farzaneh Afkhami, Patricia Paule Wright, Philip Yuan‐Ho Chien, Chun Xu, Laurence James Walsh, Ove Andreas Peters
International Endodontic Journal.2024; 57(8): 1065. CrossRef
- Modern aspects of the use of hardware methods for diagnosing pulp vitality (Part 2. Non-traditional diagnostic methods)
- 3,410 View
- 49 Download
- 1 Web of Science
- 2 Crossref

Case Report
- Use of ultrasound Doppler to determine tooth vitality in a discolored tooth after traumatic injury: its prospects and limitations
- Yong-Wook Cho, Sung-Ho Park
- Restor Dent Endod 2014;39(1):68-73. Published online January 20, 2014
- DOI: https://doi.org/10.5395/rde.2014.39.1.68
-
Abstract
PDFPubReaderePub
When a tooth shows discoloration and does not respond to the cold test or electric pulp test (EPT) after a traumatic injury, its diagnosis can be even more difficult due to the lack of proper diagnostic methods to evaluate its vitality. In these case reports, we hope to demonstrate that ultrasound Doppler might be successfully used to evaluate the vitality of the tooth after trauma, and help reduce unnecessary endodontic treatments. In all three of the present cases, the teeth were discolored after traumatic injuries and showed negative responses to the cold test and EPT. However, they showed distinctive vital reactions in the ultrasound Doppler test during the whole observation period. In the first case, the tooth color returned to normal, and the tooth showed a positive response to the cold test and EPT at 10 wk after the injury. In the second case, the tooth color had returned to its normal shade at 10 wk after the traumatic injury but remained insensitive to the cold test and EPT. In the third case, the discoloration was successfully treated with vital tooth bleaching.
-
Citations
Citations to this article as recorded by- Determination of Blood Flow in Superficial Arteries of Human Face using Doppler Ultrasonography in Young Adults
Nedal Iqbal, Khubaib Shahid, Muhammad Imtiaz, Faiqua Yasser, Ayesha Ashraf, Muhammad Zain ul Abdin
The International Journal of Frontier Sciences.2024; 5(1): 1. CrossRef - The effects of gingival blood flow on pulpal blood flow detection using ultrasound Doppler flowmetry: animal study
Dohyun Kim, Hyoung-Seok Ko, Soo-Yeon Park, Seung-Yeon Ryu, Sung-ho Park
Restorative Dentistry & Endodontics.2023;[Epub] CrossRef - Evaluation of blood flow in superficial arteries of face by Doppler ultrasound in young adults
Izza Javaid, Anjum Tazeen, Syeda Khadija, Zareen Fatima, Muhammad Adeel Saleem, Mehreen Fatima, Umme Rubab
Pakistan BioMedical Journal.2022; : 165. CrossRef - Comparison of the Response to Pulpal Sensibility Tests in Well‐Controlled and Uncontrolled Type II Diabetes Mellitus Patients: A Cross‐Sectional Study
Fatemeh Owlia, Faezeh Zarezadeh, Sara Jambarsang, Maryam Kazemipoor, Giuseppe Minervini
International Journal of Dentistry.2022;[Epub] CrossRef - Detection of pulsed blood flow through a molar pulp chamber and surrounding tissue in vitro
S. Knörzer, K.-A. Hiller, M. Brandt, A. Niklas, J. Putzger, G. J. Monkman, S. N. Danilov, S. D. Ganichev, I. Schulz, G. Schmalz
Clinical Oral Investigations.2019; 23(3): 1121. CrossRef - Evaluation of microcirculation in the pulp of immature permanent teeth by ultrasound doppler after direct pulp capping with bioactive materials
N. U. Dmitrienko, L. R. Sarap, E. A. Kirienkova
Regional blood circulation and microcirculation.2018; 17(2): 26. CrossRef - Detection of atrial fibrillation during pulpal blood flow assessment using Doppler ultrasound: a case report
Chan-Hyun Lee, Euiseong Kim, Dohyun Kim
Dentomaxillofacial Radiology.2018; : 20170354. CrossRef - Long-term Prognosis of Pulpal Status of Traumatized Teeth Exhibiting Contradictory Results between Pulp Sensibility Test and Ultrasound Doppler Flowmetry: A Retrospective Study
So-Yeon Ahn, Dohyun Kim, Sung-Ho Park
Journal of Endodontics.2018; 44(3): 395. CrossRef
- Determination of Blood Flow in Superficial Arteries of Human Face using Doppler Ultrasonography in Young Adults
- 2,505 View
- 8 Download
- 8 Crossref
Research Articles
- Micro-CT evaluation of internal adaptation in resin fillings with different dentin adhesives
- Seung-Hoon Han, Sung-Ho Park
- Restor Dent Endod 2014;39(1):24-31. Published online January 20, 2014
- DOI: https://doi.org/10.5395/rde.2014.39.1.24
-
Abstract
PDFPubReaderePub
Objectives The purpose of present study was to evaluate the internal adaptation of composite restorations using different adhesive systems.
Materials and Methods Typical class I cavities were prepared in 32 human third molars. The teeth were divided into the following four groups: 3-step etch-and-rinse, 2-step etch-and-rinse, 2-step self-etch and 1-step self-etch system were used. After the dentin adhesives were applied, composite resins were filled and light-cured in two layers. Then, silver nitrate solution was infiltrated, and all of the samples were scanned by micro-CT before and after thermo-mechanical load cycling. For each image, the length to which silver nitrate infiltrated, as a percentage of the whole pulpal floor length, was calculated (%SP). To evaluate the internal adaptation using conventional method, the samples were cut into 3 pieces by two sectioning at an interval of 1 mm in the middle of the cavity and they were dyed with Rhodamine-B. The cross sections of the specimens were examined by stereomicroscope. The lengths of the parts where actual leakage was shown were measured and calculated as a percentage of real leakage (%RP). The values for %SP and %RP were compared.
Results After thermo-mechanical loading, all specimens showed significantly increased %SP compared to before thermo-mechanical loading and 1-step self-etch system had the highest %SP (
p < 0.05). There was a tendency for %SP and %RP to show similar microleakage percentage depending on its sectioning.Conclusions After thermo-mechanical load cycling, there were differences in internal adaptation among the groups using different adhesive systems.
-
Citations
Citations to this article as recorded by- Effect of different factors on microleakage and fracture strength of CAD‐CAM produced inlays
Meryem Gülce Subaşı, Gürel Pekkan, Meral Arslan Malkoç, Hilal Ekşi Özsoy
Journal of Prosthodontics.2025;[Epub] CrossRef - Non-Destructive In Vitro Evaluation of an Internal Adaptation of Recent Pulp-Capping Materials in Permanent Teeth Using OCT and Micro-CT
Ahmed Y. Alzahrani, Amani A. Al Tuwirqi, Nada O. Bamashmous, Turki A. Bakhsh, Eman A. El Ashiry
Children.2023; 10(8): 1318. CrossRef - Internal Adaptation of Cusp-weakened Class I Preparations Restored with Bulk-fill, Bi-layered, and Incremental Restorative Techniques: A Micro-CT Analysis
DH Floriani, RN Rached, SA Ignácio, EM Souza
Operative Dentistry.2022; 47(5): 527. CrossRef - An in vitro micro-CT assessment of bioactive restorative materials interfacial adaptation to dentin
Priyanka Angadala, Jyothi Mandava, Ravichandra Ravi, KoteswarRao Hanumanthu, Prasanthi Penmatsa, Hema Pulidindi
Dental Research Journal.2022; 19(1): 56. CrossRef - Tomographic Evaluation of the Internal Adaptation for Recent Calcium Silicate‐Based Pulp Capping Materials in Primary Teeth
A. A. Al Tuwirqi, E. A. El Ashiry, A. Y. Alzahrani, N. Bamashmous, T. A. Bakhsh, Iole Vozza
BioMed Research International.2021;[Epub] CrossRef - Micro-computed tomography in preventive and restorative dental research: A review
Mehrsima Ghavami-Lahiji, Reza Tayefeh Davalloo, Gelareh Tajziehchi, Paria Shams
Imaging Science in Dentistry.2021; 51(4): 341. CrossRef - Validation of a method of quantifying 3D leakage in dental restorations
Fabio A.P. Rizzante, Rana A.F. Sedky, Adilson Y. Furuse, Sorin Teich, Sérgio K. Ishikiriama, Gustavo Mendonça
The Journal of Prosthetic Dentistry.2020; 123(6): 839. CrossRef - Comparison of micro-CT and conventional dye penetration for microleakage assessment after different aging conditions
Rayssa Ferreira Zanatta, Annette Wiegand, Christian Dullin, Alessandra Bühler Borges, Carlos Rocha Gomes Torres, Marta Rizk
International Journal of Adhesion and Adhesives.2019; 89: 161. CrossRef - Comparison of Internal Adaptation of Bulk-fill and Increment-fill Resin Composite Materials
FS Alqudaihi, NB Cook, KE Diefenderfer, MC Bottino, JA Platt
Operative Dentistry.2019; 44(1): E32. CrossRef - Effects of occlusal cavity configuration on 3D shrinkage vectors in a flowable composite
Dalia Kaisarly, Moataz El Gezawi, Guangyun Lai, Jian Jin, Peter Rösch, Karl-Heinz Kunzelmann
Clinical Oral Investigations.2018; 22(5): 2047. CrossRef - Bonding Strategies of Resin Cement to Er, Cr:YSGG Lased Dentin: Micro-CT Evaluation and Microshear Bond Strength Testing
Gökçe Meriç, Simge Taşar, Kaan Orhan
The International Journal of Artificial Organs.2016; 39(2): 72. CrossRef - Calcium hypochlorite as a dentin deproteinization agent: Microleakage, scanning electron microscopy and elemental analysis
Michele Bortoluzzi de Conto Ferreira, Bruno Carlini Júnior, Daniel Galafassi, Delton Luiz Gobbi
Microscopy Research and Technique.2015; 78(8): 676. CrossRef
- Effect of different factors on microleakage and fracture strength of CAD‐CAM produced inlays
- 2,169 View
- 8 Download
- 12 Crossref
-
Inhibition of
Streptococcus mutans biofilm formation on composite resins containing ursolic acid - Soohyeon Kim, Minju Song, Byoung-Duck Roh, Sung-Ho Park, Jeong-Won Park
- Restor Dent Endod 2013;38(2):65-72. Published online May 28, 2013
- DOI: https://doi.org/10.5395/rde.2013.38.2.65
-
Abstract
PDFPubReaderePub
Objectives To evaluate the inhibitory effect of ursolic acid (UA)-containing composites on
Streptococcus mutans (S. mutans ) biofilm.Materials and Methods Composite resins with five different concentrations (0.04, 0.1, 0.2, 0.5, and 1.0 wt%) of UA (U6753, Sigma Aldrich) were prepared, and their flexural strengths were measured according to ISO 4049. To evaluate the effect of carbohydrate source on biofilm formation, either glucose or sucrose was used as a nutrient source, and to investigate the effect of saliva treatment, the specimen were treated with either unstimulated whole saliva or phosphate-buffered saline (PBS). For biofilm assay, composite disks were transferred to
S. mutans suspension and incubated for 24 hr. Afterwards, the specimens were rinsed with PBS and sonicated. The colony forming units (CFU) of the disrupted biofilm cultures were enumerated. For growth inhibition test, the composites were placed on a polystyrene well cluster, andS. mutans suspension was inoculated. The optical density at 600 nm (OD600) was recorded by Infinite F200 pro apparatus (TECAN). One-way ANOVA and two-way ANOVA followed by Bonferroni correction were used for the data analyses.Results The flexural strength values did not show significant difference at any concentration (
p > 0.01). In biofilm assay, the CFU score decreased as the concentration of UA increased. The influence of saliva pretreatment was conflicting. The sucrose groups exhibited higher CFU score than glucose group (p < 0.05). In bacterial growth inhibition test, all experimental groups containing UA resulted in complete inhibition.Conclusions Within the limitations of the experiments, UA included in the composite showed inhibitory effect on
S. mutans biofilm formation and growth.-
Citations
Citations to this article as recorded by- Environmental Stress Induces Altered Composition of Streptococcus mutans Membrane Vesicles: pH‐Driven Changes in Membrane Vesicle Production and Composition
Taylor C. Boone, Swetha K. Shankar, Melodie L. Weller
Molecular Oral Microbiology.2026; 41(3): 145. CrossRef - Anti-cariogenic effect of experimental resin cement containing ursolic acid using dental microcosm biofilm
Jonghyun Jo, Mi-Jeong Jeon, Sun Kyu Park, Su-Jung Shin, Baek-il Kim, Jeong-Won Park
Journal of Dentistry.2024; 151: 105447. CrossRef - Rapid specific detection of oral bacteria using Cas13-based SHERLOCK
Jett Liu, Camden Carmichael, Hatice Hasturk, Wenyuan Shi, Batbileg Bor
Journal of Oral Microbiology.2023;[Epub] CrossRef - Novel Bioactive Nanocomposites Containing Calcium Fluoride and Calcium Phosphate with Antibacterial and Low-Shrinkage-Stress Capabilities to Inhibit Dental Caries
Abdullah Alhussein, Rashed Alsahafi, Abdulrahman A. Balhaddad, Lamia Mokeem, Abraham Schneider, Mary-Ann Jabra-Rizk, Radi Masri, Gary D. Hack, Thomas W. Oates, Jirun Sun, Michael D. Weir, Hockin H. K. Xu
Bioengineering.2023; 10(9): 991. CrossRef - Quorum sensing inhibition and antibiofilm action of triterpenoids: An updated insight
Sudipta Paul Bhattacharya, Snigdha Karmakar, Kusumita Acharya, Arijit Bhattacharya
Fitoterapia.2023; 167: 105508. CrossRef - The Application of Small Molecules to the Control of Typical Species Associated With Oral Infectious Diseases
Sirui Yang, Xiaoying Lyu, Jin Zhang, Yusen Shui, Ran Yang, Xin Xu
Frontiers in Cellular and Infection Microbiology.2022;[Epub] CrossRef - Anti-Planktonic and Anti-Biofilm Properties of Pentacyclic Triterpenes—Asiatic Acid and Ursolic Acid as Promising Antibacterial Future Pharmaceuticals
Zuzanna Sycz, Dorota Tichaczek-Goska, Dorota Wojnicz
Biomolecules.2022; 12(1): 98. CrossRef - Development and Physicochemical Characterization of Eugenia brejoensis Essential Oil-Doped Dental Adhesives with Antimicrobial Action towards Streptococcus mutans
Maury Luz Pereira, Danyelle Cristina Pereira Santos, Carlos Alberto Mendes Soares Júnior, Tamyris Alicely Xavier Nogueira Bazan, Clovis Macêdo Bezerra Filho, Márcia Vanusa da Silva, Maria Tereza dos Santos Correia, Andres Felipe Millan Cardenas, Fabiana S
Journal of Functional Biomaterials.2022; 13(3): 149. CrossRef - Does Secondary Plant Metabolite Ursolic Acid Exhibit Antibacterial Activity against Uropathogenic Escherichia coli Living in Single- and Multispecies Biofilms?
Zuzanna Sycz, Dorota Wojnicz, Dorota Tichaczek-Goska
Pharmaceutics.2022; 14(8): 1691. CrossRef - Prolonged Inhibition of Streptococcus mutans Growth and Biofilm Formation by Sustained Release of Chlorhexidine from Varnish Coated Dental Abutments: An in Vitro Study
Mark Feldman, Walid Shaaban Moustafa Elsayed, Michael Friedman, Irith Gati, Doron Steinberg, Hesham Marei, Paolo Francesco Manicone
International Journal of Dentistry.2022;[Epub] CrossRef - Interkingdom Signaling Interference: The Effect of Plant-Derived Small Molecules on Quorum Sensing in Plant-Pathogenic Bacteria
Janak Raj Joshi, Netaly Khazanov, Amy Charkowski, Adi Faigenboim, Hanoch Senderowitz, Iris Yedidia
Annual Review of Phytopathology.2021; 59(1): 153. CrossRef - Small Molecule Compounds, A Novel Strategy against Streptococcus mutans
Sirui Yang, Jin Zhang, Ran Yang, Xin Xu
Pathogens.2021; 10(12): 1540. CrossRef - Titanium dioxide nanotubes added to glass ionomer cements affect S. mutans viability and mechanisms of virulence
Isaac Jordão de Souza ARAÚJO, Mariana Gallante RICARDO, Orisson Ponce GOMES, Priscila Alves GIOVANI, Júlia PUPPIN-RONTANI, Vanessa Arias PECORARI, Elizabeth Ferreira MARTINEZ, Marcelo Henrique NAPIMOGA, Francisco Humberto NOCITI JUNIOR, Regina Maria PUPPI
Brazilian Oral Research.2021;[Epub] CrossRef - Effect of Ursolic and Oleanolic Acids on Lipid Membranes: Studies on MRSA and Models of Membranes
Sandrine Verstraeten, Lucy Catteau, Laila Boukricha, Joelle Quetin-Leclercq, Marie-Paule Mingeot-Leclercq
Antibiotics.2021; 10(11): 1381. CrossRef - Ursolic acid inhibits multi-species biofilms developed by Streptococcus mutans, Streptococcus sanguinis, and Streptococcus gordonii
Xiaoying Lyu, Liang Wang, Yusen Shui, Qingsong Jiang, Lan Chen, Wen Yang, Xiaoya He, Jumei Zeng, Yuqing Li
Archives of Oral Biology.2021; 125: 105107. CrossRef - The physical properties and anticariogenic effect of experimental resin cement containing ursolic acid
Hyunkyung Yoo, So Youn Kim, Su-Jung Shin, Jeong-Won Park
Odontology.2021; 109(3): 641. CrossRef - Ursolic acid: A systematic review of its pharmacology, toxicity and rethink on its pharmacokinetics based on PK-PD model
Qiang Sun, Man He, Meng Zhang, Sha Zeng, Li Chen, Lijuan Zhou, Haibo Xu
Fitoterapia.2020; 147: 104735. CrossRef - Effects of UVB and UVC irradiation on cariogenic bacteria in vitro
Shigeki Uchinuma, Yasushi Shimada, Khairul Matin, Keiichi Hosaka, Masahiro Yoshiyama, Yasunori Sumi, Junji Tagami
Lasers in Medical Science.2019; 34(5): 981. CrossRef - Ursolic acid (UA): A metabolite with promising therapeutic potential
Dharambir Kashyap, Hardeep Singh Tuli, Anil K. Sharma
Life Sciences.2016; 146: 201. CrossRef - Protective Effects on Gastric Lesion of Ursolic acid
Sun Whoe Kim, In Young Hwang, Sun Yi Lee, Choon Sik Jeong
Journal of Food Hygiene and Safety.2016; 31(4): 286. CrossRef - Ursolic Acid—A Pentacyclic Triterpenoid with a Wide Spectrum of Pharmacological Activities
Łukasz Woźniak, Sylwia Skąpska, Krystian Marszałek
Molecules.2015; 20(11): 20614. CrossRef - Antibacterial effect of self-etching adhesive systems onStreptococcus mutans
Seung-Ryong Kim, Dong-Hoon Shin
Restorative Dentistry & Endodontics.2014; 39(1): 32. CrossRef - Dental materials with antibiofilm properties
Zhejun Wang, Ya Shen, Markus Haapasalo
Dental Materials.2014; 30(2): e1. CrossRef - Antibacterial properties of composite resins incorporating silver and zinc oxide nanoparticles onStreptococcus mutansandLactobacillus
Shahin Kasraei, Lida Sami, Sareh Hendi, Mohammad-Yousef AliKhani, Loghman Rezaei-Soufi, Zahra Khamverdi
Restorative Dentistry & Endodontics.2014; 39(2): 109. CrossRef - Synergistic effect of xylitol and ursolic acid combination on oral biofilms
Yunyun Zou, Yoon Lee, Jinyoung Huh, Jeong-Won Park
Restorative Dentistry & Endodontics.2014; 39(4): 288. CrossRef - The virulence of Streptococcus mutans and the ability to form biofilms
W. Krzyściak, A. Jurczak, D. Kościelniak, B. Bystrowska, A. Skalniak
European Journal of Clinical Microbiology & Infectious Diseases.2014; 33(4): 499. CrossRef
- Environmental Stress Induces Altered Composition of Streptococcus mutans Membrane Vesicles: pH‐Driven Changes in Membrane Vesicle Production and Composition
- 2,722 View
- 9 Download
- 26 Crossref
Case Reports
- Vital tooth with periapical lesion: spontaneous healing after conservative treatment
- Hyun-Joo Kim, Seung-Jong Lee, Il-Young Jung, Sung-Ho Park
- Restor Dent Endod 2012;37(2):123-126. Published online May 18, 2012
- DOI: https://doi.org/10.5395/rde.2012.37.2.123
-
Abstract
PDFPubReaderePub
It is often presumed that apical periodontitis follows total pulp necrosis, and consequently root canal treatment is commonly performed. Periapical lesion development is usually caused by bacteria and its byproduct which irritate pulp, develop pulpitis, and result in necrosis through an irreversible process. Afterwards, apical periodontitis occurs. This phenomenon is observed as an apical radiolucency in radiographic view. However, this unusual case presents a spontaneous healing of periapical lesion, which has developed without pulp necrosis in a vital tooth, through conservative treatment.
- 3,225 View
- 38 Download
- Re-establishment of occlusion after unilateral condylar fracture
- Yookyung Kim, Sung-Ho Park, Byoung-Duck Roh
- Restor Dent Endod 2012;37(2):110-113. Published online May 18, 2012
- DOI: https://doi.org/10.5395/rde.2012.37.2.110
-
Abstract
PDFPubReaderePub
Complications resulting from condylar fracture include occlusal disturbance due to loss of leverage from temporomandibular joint (TMJ). In general, closed reduction with active physical training has been performed, and under favorable circumstances, adaptation occurs in attempt to restore the articulation. The patient in this case report had unilateral condylar fracture accompanied with multiple teeth injuries, but he was left without any dental treatment for 1 mon which led to unrestorable occlusal collapse. Fortunately, delayed surgical repositioning of dislocated maxillary anterior teeth followed by consistent long-term physical training has been proved successful. Normal occlusion and satisfactory remodeling of condyle were obtained on 10 mon follow-up.
- 1,458 View
- 5 Download
Research Articles
- Evaluation of internal adaptation of dental adhesive restorations using micro-CT
- Oh-Hyun Kwon, Sung-Ho Park
- Restor Dent Endod 2012;37(1):41-49. Published online March 2, 2012
- DOI: https://doi.org/10.5395/rde.2012.37.1.41
-
Abstract
PDFPubReaderePub
Objectives The internal adaptation of composite restorations with or without resin modified glass ionomer cement (RMGIC) was analyzed non-destructively using Microcomputed tomography (micro-CT).
Materials and Methods Thirty intact human teeth were used. The specimens were divided into 3 groups. In the control group, the cavities were etched with 10% phosphoric acid for 15 sec. Composite resin was filled into the cavity without adhesive. In group 1, light cured glass ionomer cement (GIC, Fuji II LC, GC) was applied as a base. The cavities were then etched, bonded, light cured and filled with composites. In group 2, the cavities were then etched, bonded, light cured and filled with composites without base application. They were immersed in a 25% silver nitrate solution. Micro-CT was performed before and after mechanical loading. One-way ANOVA with Duncan analysis was used to compare the internal adaptation between the groups before or after loading. A paired
t -test was used to compare internal adaptation before and after mechanical loading. All statistical inferences were made within the 95% confidence interval.Results The silver nitrate solution successfully penetrated into the dentinal tubules from the pulp spaces, and infiltrated into the gap between restoration and pulpal floor. Group 2 showed a lower adaptation than the control group and group 1 (
p < 0.05). There was no significant difference between the control group and group 1. For all groups, there was a significant difference between before and after mechanical loading (p < 0.05).Conclusions The internal adaptation before and after loading was better when composites were bonded to tooth using adhesive than composites based with RMGIC.
-
Citations
Citations to this article as recorded by- Micro-computed tomography in preventive and restorative dental research: A review
Mehrsima Ghavami-Lahiji, Reza Tayefeh Davalloo, Gelareh Tajziehchi, Paria Shams
Imaging Science in Dentistry.2021; 51(4): 341. CrossRef - Gaps at the interface between dentine and self‐adhesive resin cement in post‐endodontic restorations quantified in 3D by phase contrast‐enhanced micro‐CT
A. P. Soares, K. Bitter, A. Lagrange, A. Rack, H. Shemesh, P. Zaslansky
International Endodontic Journal.2020; 53(3): 392. CrossRef - Hard X-ray phase-contrast-enhanced micro-CT for quantifying interfaces within brittle dense root-filling-restored human teeth
Ana Prates Soares, Uwe Blunck, Kerstin Bitter, Sebastian Paris, Alexander Rack, Paul Zaslansky
Journal of Synchrotron Radiation.2020; 27(4): 1015. CrossRef - Comparison of micro-CT and conventional dye penetration for microleakage assessment after different aging conditions
Rayssa Ferreira Zanatta, Annette Wiegand, Christian Dullin, Alessandra Bühler Borges, Carlos Rocha Gomes Torres, Marta Rizk
International Journal of Adhesion and Adhesives.2019; 89: 161. CrossRef - Comparison of Internal Adaptation of Bulk-fill and Increment-fill Resin Composite Materials
FS Alqudaihi, NB Cook, KE Diefenderfer, MC Bottino, JA Platt
Operative Dentistry.2019; 44(1): E32. CrossRef - Polymerization shrinkage assessment of dental resin composites: a literature review
Dalia Kaisarly, Moataz El Gezawi
Odontology.2016; 104(3): 257. CrossRef - Non-destructive evaluation of an internal adaptation of resin composite restoration with swept-source optical coherence tomography and micro-CT
Seung-Hoon Han, Alireza Sadr, Junji Tagami, Sung-Ho Park
Dental Materials.2016; 32(1): e1. CrossRef - Micro-CT evaluation of internal adaptation in resin fillings with different dentin adhesives
Seung-Hoon Han, Sung-Ho Park
Restorative Dentistry & Endodontics.2014; 39(1): 24. CrossRef
- Micro-computed tomography in preventive and restorative dental research: A review
- 2,490 View
- 9 Download
- 8 Crossref
- Effect of fluoride concentration in pH 4.3 and pH 7.0 supersaturated solutions on the crystal growth of hydroxyapatite
- Haneol Shin, Sung-Ho Park, Jeong-Won Park, Chan-Young Lee
- Restor Dent Endod 2012;37(1):16-23. Published online March 2, 2012
- DOI: https://doi.org/10.5395/rde.2012.37.1.16
-
Abstract
PDFPubReaderePub
Objectives Present study was undertaken to investigate the crystal growth onto synthetic hydroxyapatite (HA) seeds in pH 4.3 and pH 7.0 supersaturated solutions with different fluoride concentrations.
Materials and Methods 8 groups of pH 4.3 and 7.0 calcium phosphate supersaturated solutions were prepared with different fluoride concentrations (0, 1, 2 and 4 ppm). Calcium phosphate precipitates yield crystal growth onto the HA seed surface while solutions flow. For evaluation of crystallizing process, the changes of Ca2+, PO43-, F- concentrations of the inlet and outlet solutions were determined. The recovered solid samples were weighed to assess the amount of minerals precipitated, and finally determined their composition to deduce characteristics of crystals.
Results During the seeded crystal growth, there were significantly more consumption of Ca2+, PO43-, F- in pH 4.3 solutions than pH 7.0 (
p < 0.05). As fluoride concentration increased in pH 4.3 solution, Ca2+, PO43-, F- consumption in experimental solutions, weight increment of HA seed, and fluoride ratio in crystallized samples were increased. There were significant differences among the groups (p < 0.05). But in pH 7.0 solution, these phenomena were not significant. In pH 7.0 solutions, analyses of crystallized samples showed higher Ca/P ratio in higher fluoride concentration. There were significant differences among the groups (p < 0.05). But in pH 4.3 solution, there were not significant differences in Ca/P ratio.Conclusions Crystal growth in pH 4.3 solutions was superior to that in pH 7.0 solutions. In pH 4.3 solutions, crystal growth increased with showed in higher fluoride concentration up to 4 ppm.
-
Citations
Citations to this article as recorded by- Qualitative analysis on crystal growth of synthetic hydroxyapatite influenced by fluoride concentration
Sumi Kang, Jeong Taeg Seo, Sung-Ho Park, Il Young Jung, Chan Young Lee, Jeong-Won Park
Archives of Oral Biology.2019; 104: 52. CrossRef
- Qualitative analysis on crystal growth of synthetic hydroxyapatite influenced by fluoride concentration
- 1,811 View
- 2 Download
- 1 Crossref
Case Report
- Subcutaneous emphysema during fracture line inspection: case report
- Min-Young Kim, Sung-Ho Park, Yoo-Seok Shin, Euiseong Kim
- J Korean Acad Conserv Dent 2011;36(6):506-509. Published online November 30, 2011
- DOI: https://doi.org/10.5395/JKACD.2011.36.6.506
-
Abstract
PDFPubReaderePub
The development of subcutaneous emphysema is a well-known complication that has been reported after dental extraction, endodontic treatment, or restorative preparation. Gaseous invasion, leading to swelling, crepitus on palpation, is commonly restricted to the connective tisssues immediately adjacent to the entry site. However, the use of compressed air- and water-cooled turbines may allow large amounts of air and water to be driven through the fascial planes into the mediastinum, pleural space, or even the retroperitoneum.
This case report is about the patient who presented with subcutaneous emphysema that occurred after fracture line inspection. Possible cause, treatment, and prevention of emphysema will be discussed.
- 1,638 View
- 6 Download
Basic Researchs
- Influence of post types and sizes on fracture resistance in the immature tooth model
- Jong-Hyun Kim, Sung-Ho Park, Jeong-Won Park, Il-Young Jung
- J Korean Acad Conserv Dent 2010;35(4):257-266. Published online July 31, 2010
- DOI: https://doi.org/10.5395/JKACD.2010.35.4.257
-
Abstract
PDFPubReaderePub
The purpose of this study was to determine the effect of post types and sizes on fracture resistance in immature tooth model with various restorative techniques. Bovine incisors were sectioned 8 mm above and 12 mm below the cementoenamel junction to simulate immature tooth model. To compare various post-and-core restorations, canals were restored with gutta-percha and resin core, or reinforced dentin wall with dual-cured resin composite, followed by placement of D.T. LIGHT-POST, ParaPost XT, and various sizes of EverStick Post individually. All of specimens were stored in the distilled water for 72 hours and underwent 6,000 thermal cycles. After simulation of periodontal ligament structure with polyether impression material, compressive load was applied at 45 degrees to the long axis of the specimen until fracture was occurred.
Experimental groups reinforced with post and composite resin were shown significantly higher fracture strength than gutta-percha group without post placement (p < 0.05). Most specimens fractured limited to cervical third of roots. Post types did not influence on fracture resistance and fracture level significantly when cement space was filled with dual-cured resin composite. In addition, no statistically significant differences were seen between customized and standardized glass fiber posts, which cement spaces were filled with resin cement or composite resin individually. Therefore, root reinforcement procedures as above in immature teeth improved fracture resistance regardless of post types and sizes.
-
Citations
Citations to this article as recorded by- Effect of Dental Posts used in Restoring Badly Broken Primary teeth
Tebra Alkayakh, Abdulrahim Aldarewesh
Libyan Journal of Medical Research.2024; 18(1): 65. CrossRef - An in vitro comparison of fracture resistance of immature teeth subjected to apexification using three different bioactive materials
Aarshati Vyas, Shilpa Shah, Nishtha K Patel, Krushnangi Yagnik, Vyoma Hirpara, Rajvi Shah
IP Indian Journal of Conservative and Endodontics.2023; 7(4): 172. CrossRef - Comparative Evaluation of the Fracture Resistance of Simulated Immature Teeth Reinforced with a Novel Anatomic Post and MTA or Biodentine as an Apical Barrier: An In Vitro Study
Shivani H Dholakia, Mrunalini J Vaidya
Journal of Operative Dentistry & Endodontics.2020; 4(2): 62. CrossRef - Rehabilitation of compromised permanent incisors with anatomically adjustable fiber post
Talat M. Beltagy
Tanta Dental Journal.2018; 15(1): 52. CrossRef - Fracture resistance of upper central incisors restored with different posts and cores
Maryam Rezaei Dastjerdi, Kamran Amirian Chaijan, Saeid Tavanafar
Restorative Dentistry & Endodontics.2015; 40(3): 229. CrossRef - Retentive strength of different intracanal posts in restorations of anterior primary teeth: anin vitrostudy
Mahtab Memarpour, Fereshteh Shafiei, Maryam Abbaszadeh
Restorative Dentistry & Endodontics.2013; 38(4): 215. CrossRef
- Effect of Dental Posts used in Restoring Badly Broken Primary teeth
- 2,435 View
- 5 Download
- 6 Crossref
- The remineralization aspect of enamel according to change of the degree of saturation of the organic acid buffering solution in pH 5.5
- Jin-Sung Park, Sung-Ho Park, Jeong-Won Park, Chan-Young Lee
- J Korean Acad Conserv Dent 2010;35(2):96-105. Published online March 31, 2010
- DOI: https://doi.org/10.5395/JKACD.2010.35.2.096
-
Abstract
PDFPubReaderePub
The purpose of this study is to observe and compare the remineralization tendencies of artificial enamel caries lesion by remineralization solutions of different degree of saturations at pH 5.5, using a polarizing microscope and computer programs (Photoshop, Image pro plus, Scion Image, Excel).
For this study, 48 sound permanent teeth with no signs of demineralization, cracks, or dental restorations were used. The specimens were immersed in lactic acid demineralization solution for 2 days in order to produce artificial dental caries that consist of surface and subsurface lesions. Each of 9 or 10 specimens was immersed in pH 5.5 lactic acid buffering remineralization solution of four different degrees of saturation (0.507, 0.394, 0.301, and 0.251) for 12 days. After the demineralization and remineralization, images were taken by a polarizing microscope (×100). The results were obtained by observing images of the specimens, and using computer programs, the density of caries lesions were estimated.
While the group with the lowest degree of saturation (0.251) showed total remineralization feature from the surface to the subsurface of the lesion, the group with the highest degree of saturation (0.507) showed demineralization mainly on the surface of the lesion at the constant organic acid concentration 0.01 M and pH 5.5.
-
Citations
Citations to this article as recorded by- A Randomized, Double-Blind, Placebo-Controlled Clinical Trial of a Mouthwash Containing Glycyrrhiza uralensis Extract for Preventing Dental Caries
Yu-Rin Kim, Seoul-Hee Nam
International Journal of Environmental Research and Public Health.2021; 19(1): 242. CrossRef - Effect of fluoride concentration in pH 4.3 and pH 7.0 supersaturated solutions on the crystal growth of hydroxyapatite
Haneol Shin, Sung-Ho Park, Jeong-Won Park, Chan-Young Lee
Restorative Dentistry & Endodontics.2012; 37(1): 16. CrossRef
- A Randomized, Double-Blind, Placebo-Controlled Clinical Trial of a Mouthwash Containing Glycyrrhiza uralensis Extract for Preventing Dental Caries
- 1,796 View
- 1 Download
- 2 Crossref
Original Articles
- The remineralizing features of pH 5.5 solutions of different degree of saturations on artificially demineralized enamel
- Young-Jun Kwak, Eui-seoug Kim, Sung-Ho Park, Hyung Kyu Gong, Yoon Lee, Chan-Young Lee
- J Korean Acad Conserv Dent 2008;33(5):481-492. Published online September 30, 2008
- DOI: https://doi.org/10.5395/JKACD.2008.33.5.481
-
Abstract
PDFPubReaderePub
The purpose of this study is to observe and compare the remineralization tendencies of artificially demineralized enamel by remineralization solutions of different degree of saturations at pH 5.5, using a polarizing microscope and computer programs (Photoshop, Image pro plus, Scion Image, Excel).
For this study, 36 sound permanent teeth with no signs of demineralization, cracks, or dental restorations were used. The specimens were immersed in lactic acid demineralization solution for 3 days in order to produce dental caries artificially that consist of surface and subsurface lesions. Each of 9 or 10 specimens was immersed in pH 5.5 lactic acid buffered remineralization solution of three different degrees of saturation (0.25, 0.30, 0.35) for 12 days. After the demineralization and remineralization, images were taken by a polarizing microscope (× 100). The results were obtained by observing images of the specimens, and using computer programs, the density of caries lesions were determined.
In conclusion, in the group with the lowest degree of saturation, remineralization occurred thoroughly from the surface to the subsurface lesion, whereas in the groups with greater degree of saturation showed no significant change in the subsurface lesion, although there was corresponding increase in the remineralization width on the surface zones.
-
Citations
Citations to this article as recorded by- Effect of fluoride concentration in pH 4.3 and pH 7.0 supersaturated solutions on the crystal growth of hydroxyapatite
Haneol Shin, Sung-Ho Park, Jeong-Won Park, Chan-Young Lee
Restorative Dentistry & Endodontics.2012; 37(1): 16. CrossRef
- Effect of fluoride concentration in pH 4.3 and pH 7.0 supersaturated solutions on the crystal growth of hydroxyapatite
- 1,952 View
- 3 Download
- 1 Crossref
- The effect of intermittent composite curing on marginal adaptation
- Yong-Hwan Yun, Sung-Ho Park
- J Korean Acad Conserv Dent 2007;32(3):248-259. Published online May 31, 2007
- DOI: https://doi.org/10.5395/JKACD.2007.32.3.248
-
Abstract
PDFPubReaderePub
The aim of this research was to study the effect of intermittent polymerization on marginal adaptation by comparing the marginal adaptation of intermittently polymerized composite to that of continuously polymerized composite.
The materials used for this study were Pyramid (Bisco Inc., Schaumburg, U.S.A.) and Heliomolar (Ivoclar Vivadent, Liechtenstein). The experiment was carried out in class II MOD cavities prepared in 48 extracted human maxillary premolars. The samples were divided into 4 groups by light curing method; group 1- continuous curing (60s light on with no light off); group 2- intermittent curing (cycles of 3s with 2s light on & 1s light off for 90s); group 3- intermittent curing (cycles of 2s with 1s light on & 1s light off for 120s); group 4- intermittent curing (cycles of 3s with 1s light on & 2s light off for 180s). Consequently the total amount of light energy radiated was same in all the groups. Each specimen went through thermo-mechanical loading (TML) which consisted of mechanical loading (720,000 cycles, 5.0 kg) with a speed of 120 rpm for 100 hours and thermocycling (6000 thermocycles of alternating water of 50℃ and 55℃). The continuous margin (CM) (%) of the total margin and regional margins, occlusal enamel (OE), vertical enamel (VE), and cervical enamel (CE)) was measured before and after TML under a × 200 digital light microscope.
Three-way ANOVA and Duncan's Multiple Range Test was performed at 95% level of confidence to test the effect of 3 variables on CM (%) of the total margin: light curing conditions, composite materials and effect of TML. In each group, One-way ANOVA and Duncan's Multiple Range Test was additionally performed to compare CM (%) of regions (OE, VE, CE).
The results indicated that all the three variables were statistically significant (p < 0.05). Before TML, in groups using Pyramid, groups 3 and 4 showed higher CM (%) than groups 1 and 2, and in groups using Heliomolar, groups 3 and 4 showed higher CM (%) than group 1 (p < 0.05). After TML, in both Pyramid and Heliomolar groups, group 3 showed higher CM (%) than group 1 (p < 0.05). CM (%) of the regions are significantly different in each group (p < 0.05). Before TML, no statistical difference was found between groups within the VE and CE region. In the OE region, group 4 of Pyramid showed higher CM (%) than group 2, and groups 2 and 4 of Heliomolar showed higher CM (%) than group 1 (p < 0.05). After TML, no statistical difference was found among groups within the VE and CE region. In the OE region, group 3 of Pyramid showed higher CM (%) than groups 1 and 2, and groups 2,3 and 4 of Heliomolar showed higher CM (%) than group 1 (p < 0.05).
It was concluded that intermittent polymerization may be effective in reducing marginal gap formation.
-
Citations
Citations to this article as recorded by- Effect of the exponential curing of composite resin on the microtensile dentin bond strength of adhesives
So-Rae Seong, Duck-kyu Seo, In-Bog Lee, Ho-Hyun Son, Byeong-Hoon Cho
Journal of Korean Academy of Conservative Dentistry.2010; 35(2): 125. CrossRef
- Effect of the exponential curing of composite resin on the microtensile dentin bond strength of adhesives
- 1,579 View
- 6 Download
- 1 Crossref
- Correlation between Linear polymerization shrinkage & tooth cuspal deflection
- Soon-Young Lee, Sung-Ho Park
- J Korean Acad Conserv Dent 2005;30(6):442-449. Published online November 30, 2005
- DOI: https://doi.org/10.5395/JKACD.2005.30.6.442
-
Abstract
PDFPubReaderePub
The purpose of the present study was to evaluate the relationship between the amount of cuspal deflection and linear polymerization shrinkage in resin composite and polyacid modified resin composite. For cuspal defelction and shrinkage measurement, Dyract AP, Compoglass F, Z100, Surefil, Pyramid, Synergy Compact, Heliomolar and Heliomolar HB were used.
For measuring polymerization shrinkage, a custom made linometer (R&B, Daejon, Korea) was used. The amount of shrinkage among materials was compared using One-way ANOVA analysis and Tukey's test at the 95% of confidence level.
For measuring cuspal deflection of teeth, standardized MOD cavities were prepared in extracted maxillary premolars. After a self-etching adhesive was applied, cavities were bulk filled with one of the filling materials.Fifteen teeth were used for each material. Cuspal deflection was measured by a custom made cuspal-deflection measuring device. One-way ANOVA analysis and Tukey's test were used to determine differences between the materials at the 95% of confidence level.
Correlation of polymerization shrinkage and cuspal deflection were analyzed by regression analysis.
The amount of polymerization shrinkage from least to greatest was Heliomolar, Surefil < Heliomolar HB < Z100, Synergy Compact < Dyract AP < Pyramid, Compoglass F (p < 0.05).
The amount of cuspal deflection from least to greatest was Z100, Heliomolar, Heliomolar HB, Synergy Compact Surefil < Compoglass F < Pyramid, Dyract AP (p < 0.05).
The amount of polymerization shrinkage and cuspal deflection showed a correlation (p < 0.001).
-
Citations
Citations to this article as recorded by- Comparison of Premolar Cuspal Deflection in Bulk or in Incremental Composite Restoration Methods
ME Kim, SH Park
Operative Dentistry.2011; 36(3): 326. CrossRef
- Comparison of Premolar Cuspal Deflection in Bulk or in Incremental Composite Restoration Methods
- 2,312 View
- 6 Download
- 1 Crossref
- Measurements of shrinkage stress and reduction of inter-cuspal distance in maxillary premolars resulting from polymerization of composites and compomers
- Soon-Young Lee, Sung-Ho Park
- J Korean Acad Conserv Dent 2004;29(4):346-352. Published online July 31, 2004
- DOI: https://doi.org/10.5395/JKACD.2004.29.4.346
-
Abstract
PDFPubReaderePub
The purpose of present study was to evaluate the polymerization shrinkage stress and cuspal deflection in maxillary premolars resulting from polymerization shrinkage of composites and compomers.
Composites and compomers which were used in this study were as follows: Dyract AP, Z100, Surefil, Pyramid, Synergy Compact, Heliomolar, Heliomolar HB, and Compoglass F. For measuring of polymerization shrinkage stress, Stress measuring machine (R&B, Daejon, Korea) was used. One-way ANOVA analysis with Duncan's multiple comparison test were used to determine significant differences between the materials.
For measuring of cuspal deflection of tooth, MOD cavities were prepared in 10 extracted maxillary premolars. And reduction of intercuspal distance was measured by strain measuring machine (R&B, Daejon, Korea) One-way ANOVA analysis with Turkey test were used to determine significant differences between the materials.
Polymerization shrinkage stress is 『Heliomolar, Z100, Pyramid < Synergy Compact Compoglass F < Dyract AP < Heliomolr HB, surefil』 (P < 0.05). And cuspal delfelction is 『Z100, Heliomolar, Heliomolar HB, Synergy Compact Surefil, < Compoglass F < Pyramid, Dyract AP』 (P < 0.05).
Measurements of ploymerization shrinkage stress and those of cuspal deflection of the teeth was different. There is no correlation between polymerization shrinkage stress and cuspal deflection of the teeth (p > 0.05).
-
Citations
Citations to this article as recorded by- Influence of thermal and thermomechanical stimuli on a molar tooth treated with resin-based restorative dental composites
Jerrin Thadathil Varghese, Behzad Babaei, Paul Farrar, Leon Prentice, B. Gangadhara Prusty
Dental Materials.2022; 38(5): 811. CrossRef - Effect of intermittent polymerization on the rate of polymerization shrinkage and cuspal deflection in composite resin
Min Kyung Kim, Sung Ho Park, Deog Gyu Seo, Yun Jung Song, Yoon Lee, Chan Young Lee
Journal of Korean Academy of Conservative Dentistry.2008; 33(4): 341. CrossRef - The effect of intermittent composite curing on marginal adaptation
Yong-Hwan Yun, Sung-Ho Park
Journal of Korean Academy of Conservative Dentistry.2007; 32(3): 248. CrossRef - Correlation Between the Amount of Linear Polymerization Shrinkage and Cuspal Deflection
S-Y. Lee, S-H. Park
Operative Dentistry.2006; 31(3): 364. CrossRef - Correlation between Linear polymerization shrinkage & tooth cuspal deflection
Soon-Young Lee, Sung-Ho Park
Journal of Korean Academy of Conservative Dentistry.2005; 30(6): 442. CrossRef
- Influence of thermal and thermomechanical stimuli on a molar tooth treated with resin-based restorative dental composites
- 1,632 View
- 0 Download
- 5 Crossref
- Micro-shear bond strength to dentin under simulated pulpal pressure
- Yun-Jung Song, Sung-Ho Park
- J Korean Acad Conserv Dent 2004;29(4):339-345. Published online July 31, 2004
- DOI: https://doi.org/10.5395/JKACD.2004.29.4.339
-
Abstract
PDFPubReaderePub
The aim of this study was to measure and compare the micro shear bond strengths of the following dentin bonding systems to the dentin surfaces under simulated pulpal pressure; All Bond 2®, Second®, AdheSE®, Adper Prompt L-Pop®. The occlusal surfaces of 180 extracted human molars were prepared so the dentin bonding surfaces could be exposed. The teeth were randomly assigned to 3 equal groups of 60 each and subdivided. The dentin surfaces were treated with the above mentioned bonding system and resin composite cylinders were built up under a simulated pulpal pressure when saline (Group II) or diluted bovine serum (Group III) was used as the pulpal fluid. As a control, the same procedures were performed in the dried dentin surfaces (Group I). After one day of storage in water, the micro shear bond strengths were measured using an EZ tester. Group II and III showed significantly lower shear bond strength than Group I statistically (p < 0.05). SEbond® and AdheSE® showed no difference among the different dentin condition. In the Adper Prompt L-Pop®, a simulated pulpal pressure were applied to the specimens using diluted bovine serum, which showed a higher strength than the specimens in which saline was used (p < 0.05).
- 1,153 View
- 2 Download
- The amounts and speed of polymerization shrinkage and microhardness in LED cured composites
- Sung-Ho Park, Su-Sun Kim, Yong-Sik Cho, Soon-Young Lee, Do-Hyun Kim, Yong-Joo Jang, Hyun-Sung Mun, Jung-Won Seo, Byung-Duk Noh
- J Korean Acad Conserv Dent 2003;28(4):354-359. Published online July 31, 2003
- DOI: https://doi.org/10.5395/JKACD.2003.28.4.354
-
Abstract
PDFPubReaderePub
This study evaluated the effectiveness of the light emitting diode(LED) units for composite curing. To compare its effectiveness with conventional quartz tungsten halogen (QTH) light curing unit, the microhardness of 2mm composite, Z250, which had been light cured by the LEDs (Ultralume LED2, FreeLight, Developing product D1) or QTH (XL 3000) were compared on the upper and lower surface. One way ANOVA with Tukey and Paired t-test was used at 95% levels of confidence. In addition, the amount of linear polymerization shrinkage was compared between composites which were light cured by QTH or LEDs using a custom-made linometer in 10s and 60s of light curing, and the amount of linear polymerization shrinkage was compared by one way ANOVA with Tukey.
The amount of polymerization shrinkage at 10s was
XL3000 > Ultralume 2, 40, 60> FreeLight, D1 (P<0.05)
The amount of polymerization shrinkage at 60s was
XL3000 > Ultralume 2, 60> Ultralume 2,40> FreeLight, D1 (P<0.05)
The microhardness on the upper and lower surface was as follows;
It was concluded that the LEDs produced lower polymerization shrinkage in 10s and 60s compared with QTH unit. In addition, the microhardness of samples which had been cured with LEDs was lower on the lower surfaces than the upper surfaces whereas there was no difference in QTH cured samples.
-
Citations
Citations to this article as recorded by- The polymerization rate and the degree of conversion of composite resins by different light sources
Joo-Hee Ryoo, In-Bog Lee, Hyun-Mee Yoo, Mi-Ja Kim, Chang-In Seok, Hyuk-Choon Kwon
Journal of Korean Academy of Conservative Dentistry.2004; 29(4): 386. CrossRef - Measurements of shrinkage stress and reduction of inter-cuspal distance in maxillary premolars resulting from polymerization of composites and compomers
Soon-Young Lee, Sung-Ho Park
Journal of Korean Academy of Conservative Dentistry.2004; 29(4): 346. CrossRef
- The polymerization rate and the degree of conversion of composite resins by different light sources
- 1,728 View
- 0 Download
- 2 Crossref
- Amount of polymerization shrinkage and shrinkage stress in composites and compomers for posterior restoration
- Sung-Ho Park, Soon-Young Lee, Yong-Sik Cho, Su-Sun Kim, Chang-Jae Lee, Young-Joo Kim, Bong-Hee Lee, Kouang-Sung Lee, Byung-Duk Noh
- J Korean Acad Conserv Dent 2003;28(4):348-353. Published online July 31, 2003
- DOI: https://doi.org/10.5395/JKACD.2003.28.4.348
-
Abstract
PDFPubReaderePub
The purpose of present study was to evaluate the polymerization shrinkage stress and amount of linear shrinkage of composites and compomers for posterior restoration.
For this purpose, linear polymerization shrinkage and polymerization stress were measured.
For linear polymerization shrinklage and polymerization stress measurement, custom made Linometer (R&B, Daejon, Korea) and Stress measuring machine was used (R&B, Daejon, Korea). Compositers and compomers were evaluated; Dyract AP (Dentsply Detrey, Gumbh. German) Z100 (3M Dental Products, St. Paul, USA) Surefil (Dentsply Caulk, Milford, USA) Pyramid(Bisco, Schaumburg, USA) Synergy Compact (Coltene, Altstatten, Switzerland), Heliomolar (Vivadent/Ivoclar, Liechtenstein), and Compoglass (Vivadent Ivoclar/Liechtenstein) were used. 15 measurements were made for each material. Linear polymerization shrinkage or polymerization stress for each material was compared with one way ANOVA with Tukey at 95% levels of confidence.
For linear shrinkage; Heliomolar, Surefil<Synergy Compact, Z100<Dyract AP<Pyramid, Compoglass F (p<0.05)
For Shrinkage stress; Heliomolar<Z100, Pyramid<Synergy Compact, Compoglass F<Dyract AP<Heliomolar HB, Surefil (p<0.05)
-
Citations
Citations to this article as recorded by- A comparative study on color and dimensional stability of esthetic indirect dental materials
Hye-Yun Heo, Hyo-Jin Son, Yu-Ri Heo, Mee-Kyoung Son
Oral Biology Research.2019; 43(4): 306. CrossRef - Measurement of the Internal Adaptation of Resin Composites Using Micro-CT and Its Correlation With Polymerization Shrinkage
HJ Kim, SH Park
Operative Dentistry.2014; 39(2): e57. CrossRef - Comparison of Premolar Cuspal Deflection in Bulk or in Incremental Composite Restoration Methods
ME Kim, SH Park
Operative Dentistry.2011; 36(3): 326. CrossRef - Effect of intermittent polymerization on the rate of polymerization shrinkage and cuspal deflection in composite resin
Min Kyung Kim, Sung Ho Park, Deog Gyu Seo, Yun Jung Song, Yoon Lee, Chan Young Lee
Journal of Korean Academy of Conservative Dentistry.2008; 33(4): 341. CrossRef - Correlation Between the Amount of Linear Polymerization Shrinkage and Cuspal Deflection
S-Y. Lee, S-H. Park
Operative Dentistry.2006; 31(3): 364. CrossRef - Correlation between Linear polymerization shrinkage & tooth cuspal deflection
Soon-Young Lee, Sung-Ho Park
Journal of Korean Academy of Conservative Dentistry.2005; 30(6): 442. CrossRef
- A comparative study on color and dimensional stability of esthetic indirect dental materials
- 3,591 View
- 1 Download
- 6 Crossref
- Development of chewing simulator
- Sung-Ho Park, Il-Young Jung, Kwon-Yong Lee
- J Korean Acad Conserv Dent 2003;28(1):34-40. Published online January 31, 2003
- DOI: https://doi.org/10.5395/JKACD.2003.28.1.034
-
Abstract
PDFPubReaderePub
Chewing simulator, which can partly mimic the motion of chewing motion of human, has been successfully developed. The purpose of its development was to make a new machine which can anticipate the clinical results of restoration in the human teeth more accurately in vitro condition It is composed of 4 major parts; chewing part, motor part, water bath, controlling part. The controlling part control the chewing force, frequency, the temperature and running time of water. Additionally, the actual chewing force and remaining time is shown in the monitor of controlling part. At present, the chewing cycle is composed depending on the pre-published data of foreign people. Long term clinical data should be additionally collected for the simulator to mimic the clinical results more accurately.
-
Citations
Citations to this article as recorded by- The effect of intermittent composite curing on marginal adaptation
Yong-Hwan Yun, Sung-Ho Park
Journal of Korean Academy of Conservative Dentistry.2007; 32(3): 248. CrossRef
- The effect of intermittent composite curing on marginal adaptation
- 1,813 View
- 12 Download
- 1 Crossref
- Comparison of linear polymerization shrinkage in composites and compomer polymerized by plasma arc or conventional visible light curing
- Jae-Ik Lee, Sung-Ho Park
- J Korean Acad Conserv Dent 2002;27(5):488-492. Published online September 30, 2002
- DOI: https://doi.org/10.5395/JKACD.2002.27.5.488
-
Abstract
PDFPubReaderePub
The purpose of this study was to evaluate the effectiveness of plasma arc curing (PAC) unit for composite and compomer curing. To compare its effectiveness with conventional quartz tungsten halogen (QTH) light curing unit, the polymerization shrinkage rates and amounts of three composites (Z100, Z250, Synergy Duo Shade) and one compomer, that had been light cured by PAC unit or QTH unit, was compared using a custome made linometer. The measurement of polymerization shrinkage was performed after polymerization with either QTH unit or PAC unit. In case of curing with the PAC unit, the composite was light cured with Apollo 95E for 6s, the power density of which was recorded as 1350 mW/cm2 by Coltolux Light Meter. For light curing with QTH unit, the composite was light cured for 30s with the XL2500, the power density of which was recorded as 800 mW/cm2 by Coltolux Light Meter. The amount of linear polymerization shrinkage was recorded in the computer every 0.5s for 60s. Ten measurements were made for each material. The amount of linear polymerization shrinkage for each material in 10s and 60s which were cured with PAC or QTH unit were compared with t test. The amount of polymerization shrinkage in the tested materials were compared with 1way ANOVA with Duncan's multiple range test.
As for the amounts of polymerization shrinkage in 60s, there was no difference between PAC unit and QTH unit in Z250 and Synergy Duo Shade. In Z100 and Dyract AP, it was lower when it was cured with PAC unit than when it was cured with QTH unit (p<0.05).
As for the amounts of polymerization shrinkage in 10s, there was no difference between PAC unit and QTH unit in Z100 and Dyract AP. The amounts of polymerization shrinkage was significantly higher when it was cured with PAC unit in Z250 and Synergy Duo Shade (p<0.05). The amounts of polymerization shrinkage in the tested materials when they were cured with QTH unit were Z250 (6.6um) < Z100 (9.3um), Dyract AP (9.7um) < Synergy Duo Shade (11.2um) (p<0.05). The amount of polymerization shrinkage when the materials were cured with PAC unit were Dyract AP (5.6um) < Z100 (8.1um), Z250(7.0um) < Synergy Duo Shade (11.2um) (p<0.05).
- 1,580 View
- 0 Download
- 1 year follow-up study of direct and indirect composite restorations
- Sung-Ho Park
- J Korean Acad Conserv Dent 2002;27(3):284-289. Published online May 31, 2002
- DOI: https://doi.org/10.5395/JKACD.2002.27.3.284
-
Abstract
PDFPubReaderePub
Background The purpose of the present study was to evaluate the direct and indirect composite restorations which had been placed for 1 year.
Methods The composite restorations which had been placed between 1999. Mar and 1999, Dec was evaluated after 1 year. For direct restorations, Spectrum (Dentsply, USA) and Z100 (3M, USA) were used in the anterior teeth and Surefil (Dentsply, USA) were used. For class V restorations of anterior and posterior teeth, Spectrum was used. For indirect restorations, Targis/Vectris system (Vivadent/Ivoclar, Liechtenstein) was used. 2 examiners evaluated marginal quality, proximal contact, discoloration, presence of 2nd caries, loss of filling and hypersensitivity of restorations. The restorations was clinically evaluated by modified methods based on USPHS.
Results 60 teeth were evaluated. 59 were clinically acceptable and 1 restoration which was placed in class v cavity in the posterior tooth was fallen out. In most cases, the restorations were clinically acceptable. For restorations which had been directly placed in the class II cavities, loose proximal contact was indicated as the main complaints.
Conclusions Most of Anterior and posterior restorations which bad been directly or indirectly placed for 1 year were clinically acceptable. For posterior teeth, loose proximal contact was indicated as the main problem in the directly placed Class II restorations. Long term clinical study is needed.
-
Citations
Citations to this article as recorded by- Effec of different zirconia primers on shear bond strengths of composite resin to bonded zirconia
Hong-Bing Shi, Tae-Seok Kim, Jae-Seok Ahn, Jung-Hwan Lee
Journal of Korean Acedemy of Dental Technology.2016; 38(3): 135. CrossRef
- Effec of different zirconia primers on shear bond strengths of composite resin to bonded zirconia
- 3,103 View
- 6 Download
- 1 Crossref
- A confocal microscopic study on dentinal infiltration of one-bottle adhesive systems and self-etching priming system bonded to class V cavities
- Hyung-Su Kim, Sung-Ho Park
- J Korean Acad Conserv Dent 2002;27(3):257-269. Published online May 31, 2002
- DOI: https://doi.org/10.5395/JKACD.2002.27.3.257
-
Abstract
PDFPubReaderePub
Objective The purpose of this study was to evaluate the resin infiltration into dentin of one-bottle adhesive systems and self-etching primer bonded to Class V cavities using confocal laser scanning microscope(CLSM).
Material and Methods Forty Class V cavities were prepared from freshly extracted caries-free human teeth. These teeth were divided into two groups based on the presence of cervical abrasion: Group I, cervical abrasion; Group II, wedge-shaped cavity preparation. Resin-dentin interfaces were produced with two one-bottle dentin bonding systems-ONE COAT BOND(OCB; Coltene®) and Syntac®Srint™(SS; VIVADENT)-, one self-etching priming system-CLEARFIL™ SE BOND(SB; KURARAY)- and one multi-step dentin bonding system-Scotchbond™Multi-Purpose(SBMP, 3M Dental Products)-as control according to manufacturers'instructions. Cavities were restored with Spectrum®(Dentsply). Specimens were immersed in saline for 24 hours and sectioned longitudinally with a low-speed diamond disc. The resin-dentin interfaces were microscopically observed using CLSM. The quality of resin-infiltrated dentin layers were evaluated by five dentists using 0-4 scale.
Results Confocal laser scanning microscopal investigations using primer labeled with rhodamine B showed that the penetration of the primer occurred along the cavity margins.
Statistical analysis using one-way ANOVA followed by Duncan's Multiple Range test revealed that the primer penetration of the group 2(wedge-shaped cavity preparation) was more effective than group 1(cervical abrasion) and that of the gingival interfaces was more effective than the occlusal interfaces. In the one-bottle dentin bonding systems, the resin penetration score of OCB was compatible to SBMP, but those of SS and self-etching priming system, SB were lower than SBMP.
- 1,268 View
- 1 Download
- The effect of irradiation modes on polymerization and microleakage of composite resin
- Jong-Jin Park, Jeong-Won Park, Sung-Ho Park, Ju-Myong Park, Tae-Kyung Kwon, Sung-Kyo Kim
- J Korean Acad Conserv Dent 2002;27(2):158-174. Published online March 31, 2002
- DOI: https://doi.org/10.5395/JKACD.2002.27.2.158
-
Abstract
PDFPubReaderePub
The aim of this study was to investigate the effect of light irradiation modes on polymerization shrinkage, degree of cure and microleakage of a composite resin.
VIP™ (Bisco Dental Products, Schaumburg, IL, USA) and Optilux 501™ (Demetron/Kerr, Danbury, CT, USA) were used for curing Filtek™ Z-250 (3M Dental Products, St. Paul., MN, USA) composite resin using following irradiation modes: VIP™ (Bisco) 200mW/cm2 (V2), 400mW/cm2 (V4), 600mW/cm2 (V6), Pulse-delay (200 mW/cm2 3 seconds, 5 minutes wait, 600mW/cm2 30seconds, VPD) and Optilux 501™ (Demetron/Kerr) C-mode (OC), R-mode (OR).
Linear polymerization shrinkage of the composite specimens were measured using Linometer (R&B, Daejeon, Korea) for 90 seconds for V2, V4, V6, OC, OR groups and for up to 363 seconds for VPD group (n=10, each).
Degree of conversion was measured using FTIR spectrometer (IFS 120 HR, Bruker Karlsruhe, Germany) at the bottom surface of 2 mm thick composite specimens. V2, V4, V6, OC groups were measured separately at five irradiation times (5, 10, 20, 40, 60 seconds) and OR, VPD groups were measured in the above mentioned irradiation modes (n=5, each).
Microhardness was measured using Digital microhardness tester (FM7, Future-Tech Co., Tokyo, Japan) at the top and bottom surfaces of 2mm thick composite specimens after exposure to the same irradiation modes as the test of degree of conversion(n=3, each).
For the microleakage test, class V cavities were prepared on the distal surface of the ninety extracted human third molars. The cavities were restored with one of the following irradiation modes: V2/60 seconds, V4/40 seconds, V6/30 seconds, VPD, OC and OR. Microleakage was assessed by dye penetration along enamel and dentin margins of cavities.
Mean polymerization shrinkage, mean degree of conversion and mean microhardness values for all groups at each time were analyzed using one-way ANOVA and Duncan's multiple range test, and using chi-square test for microleakage values.
The results were as follows:
·Polymerization shrinkage was increased with higher light intensity in groups using VIP™ (Bisco): the highest with 600mW/cm2, followed by Pulse-delay, 400mW/cm2 and 200mW/cm2 groups. The degree of polymerization shrinkage was higher with Continuous mode than with Ramp mode in groups using Optilux 501™ (Demetron/Kerr).
·Degree of conversion and microhardness values were higher with higher light intensity. The final degree of conversion was in the range of 44.7 to 54.98% and the final microhardness value in the range of 34.10 to 56.30.
·Microleakage was greater in dentin margin than in enamel margin. Higher light intensity showed more microleakage in dentin margin in groups using VIP™ (Bisco). The micoleakage was the lowest with Continuous mode in enamel margin and with Ramp mode in dentin margin when Optilux 501™(Demetron/Kerr) was used.
-
Citations
Citations to this article as recorded by- Study on the Effect of Soft-Start Light on Microleakage in Pit and Fissure Closure
Yong Chen, Ling Guo
Journal of Hard Tissue Biology.2023; 32(2): 105. CrossRef - Power density of light curing units through resin inlays fabricated with direct and indirect composites
Hoon-Sang Chang, Young-Jun Lim, Jeong-Mi Kim, Sung-Ok Hong
Journal of Korean Academy of Conservative Dentistry.2010; 35(5): 353. CrossRef
- Study on the Effect of Soft-Start Light on Microleakage in Pit and Fissure Closure
- 1,742 View
- 0 Download
- 2 Crossref
- ANTICARIOGENCI EFFECT OF COMPOMER AND RMGIC
- Sung-Ho Park
- J Korean Acad Conserv Dent 2002;27(1):12-15. Published online January 14, 2002
- DOI: https://doi.org/10.5395/JKACD.2002.27.1.012
-
Abstract
PDFPubReaderePub
ABSTRACT The first purpose of present study was to compare the anticariogenic effect of compomer, resin modified glass ionomer cement and composite (RMGIC).
The second purpose was to evaluate the recently introduced methods, which use confocal scanning microscope, in detecting initial caries around restoration.
2×4×1.5mm cavities were prepared from the recently extracted 50 human teeth on the buccal or lingual surface. The prepared teeth were randomly devided into 5 groups and restored with each filling material. Group 1: Dyract AP, Group 2: compoglass F, Group 3: F2000, Group 4: Z100, Group 5:Fuji Ⅱ LC. The teeth were stored for 30 days in the distilled water, then stored in the buffer solution for artificial caries development; pH 4.3, lactic acid 100 mM, calcium 16 mM, phosphate 8mM, sodium azide 3mM. Then, the samples were sectioned longitudinally and examined with confical scanning microscope. The results showed that the use of compomer and resin modified glass ionomer cement showed caries inhibition zone whereas the composite did not. There was no difference in the width of caries inhibition zone between compomers and RMGIC. The confocal scanning microscope was useful in detecting initial caries around restoration.
- 1,688 View
- 3 Download
 First
First Prev
Prev

