
Search
- Page Path
- HOME > Search
Research Articles
- Dentin thickness of C-shaped root canal walls in mandibular premolars based on cone-beam computed tomography: a retrospective cross-sectional study
- Elif Aslan, Ali Canberk Ulusoy, Bilge Hakan Sen, B. Guniz Baksi, Erinc Onem, Ali Mert
- Restor Dent Endod 2025;50(2):e18. Published online May 15, 2025
- DOI: https://doi.org/10.5395/rde.2025.50.e18
-
 Abstract
Abstract
 PDF
PDF PubReader
PubReader ePub
ePub - Objectives
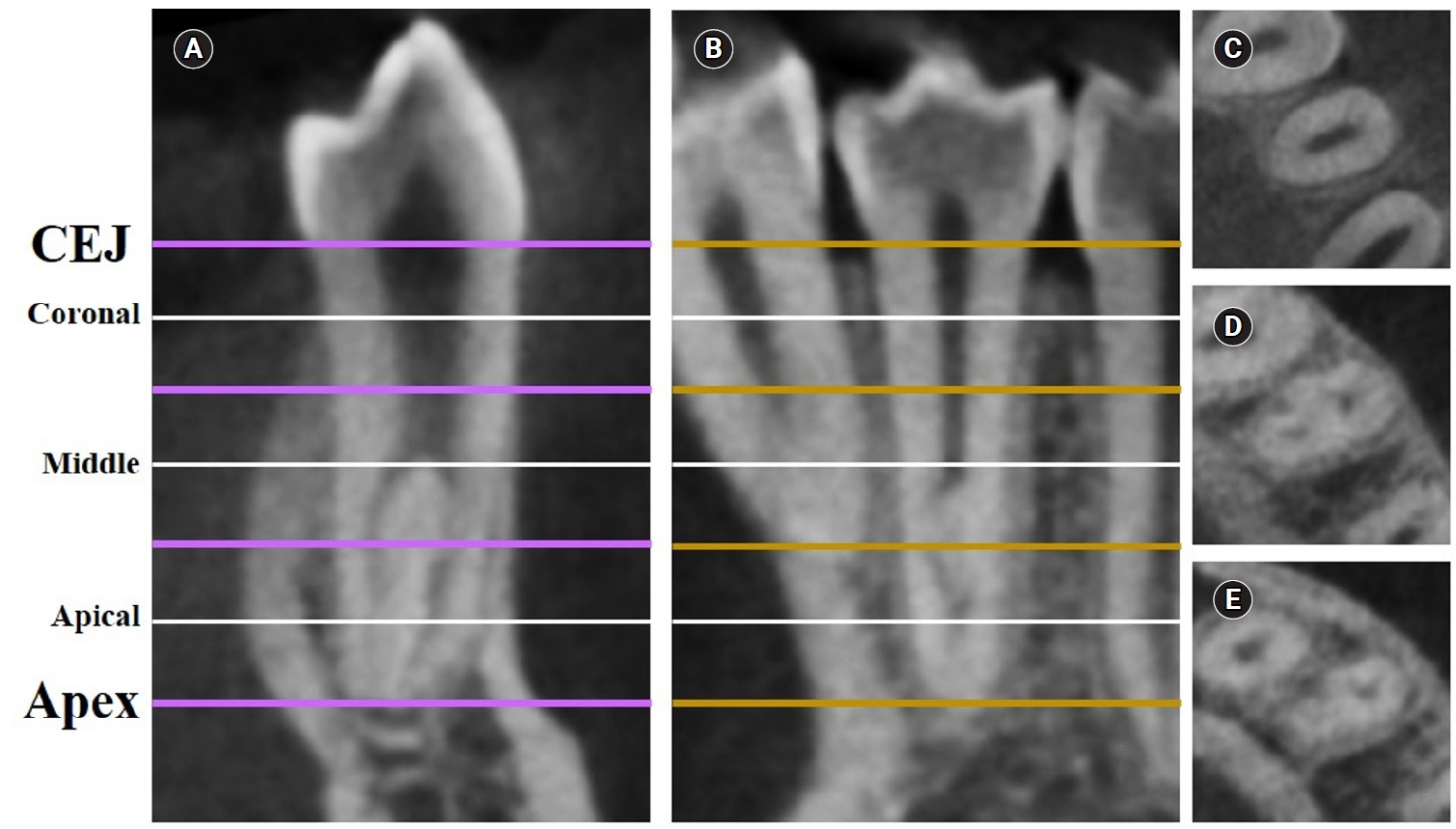
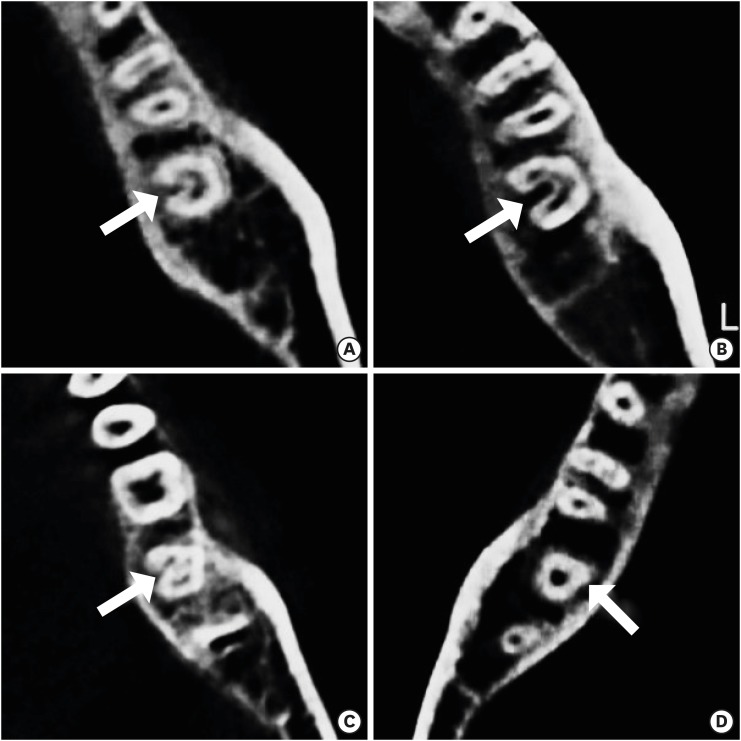
This study aimed to measure the dentin thickness of C-shaped canals in mandibular first and second premolars at coronal, middle, and apical root levels using cone-beam computed tomography (CBCT).
Methods
Dentin thicknesses of buccal, lingual, mesial, and distal root walls of 41 C-shaped premolars were measured at three different root levels on axial CBCT slices. The measurements were made at the midpoint of each third, along with 1 mm below and above the midpoint. C-shape configurations of the premolar root canals were also recorded. Analysis of variance, Kruskal-Wallis, and the independent samples t-tests were used for the comparisons (p = 0.05).
Results
The thickest walls for both premolars were buccal and lingual walls at all three root levels (p < 0.05). The thinnest walls for the first premolar teeth were mesial and distal walls of the lingual canal, while it was the mesial end of the buccal and lingual canals for the second premolars (p < 0.05). Dentin wall thicknesses at the mesial end of buccal and lingual canals of C1-shaped first premolars were thinner than C2-shaped first premolars at the apical level (p < 0.05).
Conclusions
Danger zones for C-shaped mandibular first and second premolars are predominantly mesial walls facing the radicular groove and distal wall of the lingual canal. CBCT imaging during endodontic treatment is recommended to avoid complications. -
Citations
Citations to this article as recorded by
- Anatomical complexity in mandibular second molars: prevalence of C-shaped canals, radicular grooves, taurodontism, and radices molarum in Saudi population
Ahmed A. Madfa, Abdullah F. Alshammari, Eyad Almagadawyi, Ebtsam A. Aledaili, Afaf Al-Haddad
Scientific Reports.2025;[Epub] CrossRef
- Anatomical complexity in mandibular second molars: prevalence of C-shaped canals, radicular grooves, taurodontism, and radices molarum in Saudi population
- 4,934 View
- 157 Download
- 1 Web of Science
- 1 Crossref

- Predictor factors of 1-rooted mandibular second molars on complicated root and canal anatomies of other mandibular teeth
- Hakan Aydın, Hatice Harorlı
- Restor Dent Endod 2024;49(1):e2. Published online January 3, 2024
- DOI: https://doi.org/10.5395/rde.2024.49.e2
-
Abstract
PDFPubReaderePub
Objectives This study aimed to determine the effects of 1-rooted mandibular second molar (MnSM) teeth on root canal anatomy complexities of the mandibular central incisor (MnCI), mandibular lateral incisor (MnLI), mandibular canine (MnCn), mandibular first premolar (MnFP), mandibular second premolar (MnSP), and mandibular first molar (MnFM) teeth.
Materials and Methods Cone-beam computed tomography images of 600 patients with full lower dentition were examined. Individuals with 1-rooted MnSMs were determined, and the complexity of root canal anatomy of other teeth was compared with individuals without 1-rooted MnSMs (Group-1; subjects with at least one 1-rooted MnSM, Group-2; subjects with more than a single root in both MnSMs). A second canal in MnCIs, MnLIs, MnCns, MnFPs, and MnSPs indicated a complicated root canal. The presence of a third root in MnFMs was recorded as complicated.
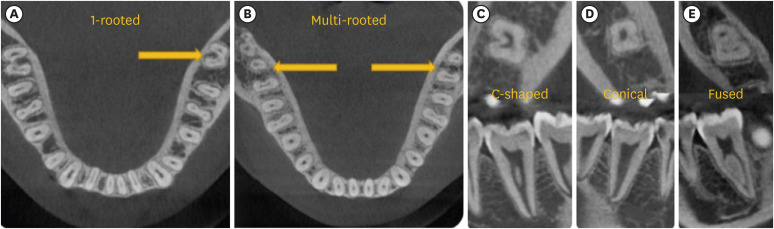
Results The prevalence of 1-rooted MnSMs was 12.2%, with the C-shaped root type being the most prevalent (9%). There were fewer complicated root canals in MnCIs (
p = 0.02), MnLIs (p < 0.001), and MnFPs (p < 0.001) in Group 1. The other teeth showed no difference between the groups (p > 0.05). According to logistic regression analysis, 1-rooted right MnSMs had a negative effect on having complex canal systems of MnLIs and MnFPs. Left MnSMs were explanatory variables on left MnLIs and both MnFPs.Conclusions In individuals with single-rooted MnSMs, a less complicated root canal system was observed in all teeth except the MnFMs.
-
Citations
Citations to this article as recorded by- Repair of furcal perforations using different calcium silicate cements: An in vitro study
Ariana Esperanza Apolo Aguilar, Maria Soledad Peñaherrera Manosalvas, Henry Paul Valverde Haro
Journal of Conservative Dentistry and Endodontics.2025; 28(10): 1007. CrossRef
- Repair of furcal perforations using different calcium silicate cements: An in vitro study
- 2,929 View
- 76 Download
- 1 Crossref
- Shape and anatomical relationship of the mental foramen to the mandibular premolars in an Indian sub-population: a retrospective CBCT analysis
- Komal Sheth, Kulvinder Singh Banga, Ajinkya M. Pawar, James L. Gutmann, Hyeon-Cheol Kim
- Restor Dent Endod 2022;47(1):e1. Published online December 13, 2021
- DOI: https://doi.org/10.5395/rde.2022.47.e1
-
Abstract
PDFPubReaderePub
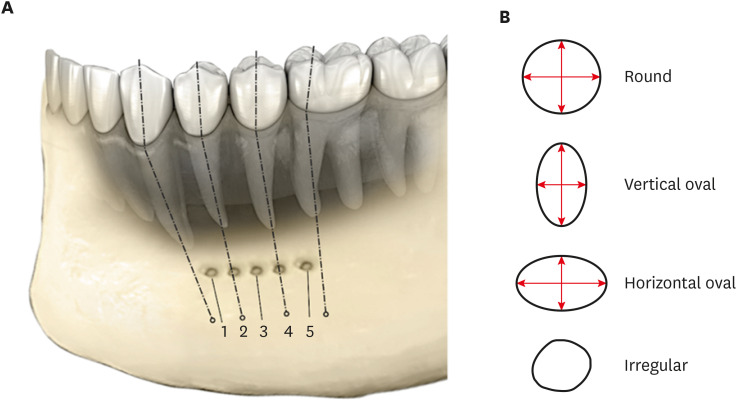
Objectives This study assessed the shape and anatomical relationship of the mental foramen (MF) to mandibular posterior teeth in an Indian sub-population.
Materials and Methods In total, 475 existing cone-beam computed tomography records exhibiting 950 MFs and including the bilateral presence of mandibular premolars and first molars were assessed. Images were evaluated 3-dimensionally to ascertain the position, shape, and anatomical proximity of MFs to mandibular teeth. The position and shape of MFs were measured and calculated. The Pythagorean theorem was used to calculate the distance between the root apex of the mandibular teeth and the MF.
Results MFs exhibited a predominantly round shape (left: 67% and right: 65%) followed by oval (left: 30% and right: 31%) in both males and females and in different age groups. The root apices of mandibular second premolars (left: 71% and right: 62%) were closest to the MF, followed by distal to the first premolars and mesial to the second premolars. The mean vertical distance between the MF and the nearest tooth apex calculated on sagittal sections was 2.20 mm on the right side and 2.32 mm on the left side; no significant difference was found according to sex or age. The distance between the apices of the teeth and the MF was ≥ 4 mm (left; 4.09 ± 1.27 mm and right; 4.01 ± 1.15 mm).
Conclusions These findings highlight the need for clinicians to be aware of the location of the MF in treatment planning and while performing non-surgical and surgical endodontic procedures.
-
Citations
Citations to this article as recorded by- Morphometric analysis of mental foramen in retained cadaveric specimens of mandibles of Sri Lankan population
Dadallage Tharanga De Silva, Usliyanage Clifford Priyantha Perera
Anatomical Science International.2026; 101(3): 340. CrossRef - Anatomical and radiographic assessment of variations of the mental foramen and their impact on success of local anaesthesia administration
Isratul Jannat, M. Ummay Salma, Nipu Rani Chowdhury, Kulsum Nahar, Dilruba Binte Mostafa, Khandokar Emanuzzaman Emon, Shahela Sarmin
International Journal of Research in Medical Sciences.2026; 14(3): 823. CrossRef - Clinical Implications of the Localization and Morphological Variability of the Mental Foramen—A Systematic Review
Mariola Krzykawska-Krupska, Janusz Pach, Piotr Regulski, Jacek Tomczyk, Izabela Strużycka, Kazimierz Szopiński, Katarzyna Osipowicz, Anna Pogorzelska
Diagnostics.2026; 16(5): 779. CrossRef - Optimising Treatment Strategies: Labial versus Labio-inferior Plating Using Three-dimensional Miniplates for Mandibular Symphysis and Parasymphysis Fractures
Akash P Muralidharan, Kalyani Bhate, K Mithun Nilgiri, Sumithra S Nair, Lakshmi Shetty, Rose Johnson
Advances in Human Biology.2025; 15(2): 242. CrossRef - A Cross-Sectional CBCT Study of Anterior Loop, Accessory Mental Foramen, and Lingual Foramina in Patients’ Mandibles: Implications for Safer Implant Planning
Abbas Shokri, Mohammad Mahdi Maleki, Leili Tapak
Journal of Maxillofacial and Oral Surgery.2025;[Epub] CrossRef - Radiographic Recognition of Mental Nerve for Secured Dental Implant Placement by Cone-Beam Computed Tomography in Mosul City Population
Asmaa B. Al-Saffar, Mekdad H. Alrigbo, Rawaa Y. Al-Rawee
Journal of Craniofacial Surgery.2024; 35(7): 2049. CrossRef - Accuracy of Implant Size Prediction Based on Edentulous Ridge Dimension on Cone-beam Computed Tomography - A Retrospective Study
Hunter R. Jolicoeur, Gerard A. Camargo, Tamara G. Stephenson, Wenjian Zhang
Annals of Maxillofacial Surgery.2024; 14(2): 187. CrossRef - Mental Foramenin Panoramik Radyografi ve Konik Işınlı Bilgisayarlı Tomografi Görüntüleri Üzerinde Morfolojik Analizi
Ezgi UZUN, Burak Kerem APAYDIN, Ayşen TİL
Selcuk Dental Journal.2023; 10(3): 540. CrossRef - Evaluation of the Possible Relationship between the Curvature and
Horizontal Course of the Inferior Alveolar Canal
Cansu G. Koca, M. Fatih Çiçek, Sanaz Sadry, Ozan Yenidünya, Fatma Akkoca Kaplan, Aras Erdil
Current Medical Imaging Formerly Current Medical Imaging Reviews.2023;[Epub] CrossRef
- Morphometric analysis of mental foramen in retained cadaveric specimens of mandibles of Sri Lankan population
- 3,982 View
- 70 Download
- 10 Web of Science
- 9 Crossref
- The prevalence of radix molaris in the mandibular first molars of a Saudi subpopulation based on cone-beam computed tomography
- Hassan AL-Alawi, Saad Al-Nazhan, Nassr Al-Maflehi, Mazen A. Aldosimani, Mohammed Nabil Zahid, Ghadeer N. Shihabi
- Restor Dent Endod 2020;45(1):e1. Published online November 14, 2019
- DOI: https://doi.org/10.5395/rde.2020.45.e1
-
Abstract
PDFPubReaderePub
Objectives The purpose of this study was to determine the incidence of radix molaris (RM) (entomolaris and paramolaris) in the mandibular first permanent molars of a sample Saudi Arabian subpopulation using cone-beam computed tomography (CBCT).
Materials and Methods A total of 884 CBCT images of 427 male and 457 female Saudi citizens (age 16 to 70 years) were collected from the radiology department archives of 4 dental centers. A total of 450 CBCT images of 741 mature mandibular first molars that met the inclusion criteria were reviewed. The images were viewed at high resolution by 3 examiners and were analyzed with Planmeca Romexis software (version 5.2).
Results Thirty-three (4.5%) mandibular first permanent molars had RM, mostly on the distal side. The incidence of radix entomolaris (EM) was 4.3%, while that of radix paramolaris was 0.3%. The RM roots had one canal and occurred more unilaterally. No significant difference in root configuration was found between males and females (
p > 0.05). Types I and III EM root canal configurations were most common, while type B was the only RP configuration observed.Conclusions The incidence of RM in the mandibular first molars of this Saudi subpopulation was 4.5%. Identification of the supernumerary root can avoid missing the canal associated with the root during root canal treatment.
-
Citations
Citations to this article as recorded by- A comprehensive investigation into the prevalence of dental anomalies across Saudi Arabia, a systematic review
Abdulrahman K. Alshammari, Muteb A. Algharbi, Freah L. Alshammary, Nabeel S. Almotairy, Hatem D. Alshammari, Amjad M. Alsogaih, Ahmed A. Madfa
Critical Public Health.2026;[Epub] CrossRef - Anatomical Variations in Permanent Mandibular Molars in the Sharjah Population: A Cohort Study Using Cone‐Beam Computed Tomography
Shaima Dheyab, Entisar AlRasasi, Ahmed M. Aziz, Saad Albayatti, Mehmet Omer Gorduysus, Hannah Wesley
International Journal of Dentistry.2026;[Epub] CrossRef - Evaluation of the variations of mandibular molars and the distance from root apex to the inferior alveolar nerve in Saudi Sub-population: Three-dimensional radiographic evaluation
Tariq Mohammed Aqili, Esam Sami Almuzaini, Abdulbari Saleh Aljohani, Ahmed Khaled Al Saeedi, Hassan Abdulmuti Hammudah, Muath Alassaf, Muhannad M. Hakeem, Mohmed Isaqali Karobari
PLOS ONE.2025; 20(2): e0317053. CrossRef - Prevalence of radix molaris in mandibular molars of a subpopulation of Brazil’s Northeast region: a cross-sectional CBCT study
Yasmym Martins Araújo de Oliveira, Maria Clara Mendes Gomes, Maria Fernanda da Silva Nascimento, Ricardo Machado, Danna Mota Moreira, Hermano Camelo Paiva, George Táccio de Miranda Candeiro
Scientific Reports.2025;[Epub] CrossRef - Prevalence of radix entomolaris and distolingual canals and their association with the incidence of middle mesial canals in mandibular first molars of a Saudi subpopulation
Ahmed A. Madfa, Abdullah F. Alshammari, Eyad Almagadawyi, Afaf Al-Haddad, Ebtsam A. Aledaili
Scientific Reports.2025;[Epub] CrossRef - Assessment of the root and canal morphology in the permanent dentition of Saudi Arabian population using cone beam computed and micro-computed tomography – a systematic review
Mohammed Mustafa, Rumesa Batul, Mohmed Isaqali Karobari, Hadi Mohammed Alamri, Abdulaziz Abdulwahed, Ahmed A. Almokhatieb, Qamar Hashem, Abdullah Alsakaker, Mohammad Khursheed Alam, Hany Mohamed Aly Ahmed
BMC Oral Health.2024;[Epub] CrossRef - Prevalence of radix accesoria dentis in a northern Peruvian population evaluated by cone-beam tomography
Karla Renata León-Almanza, Anthony Adrián Jaramillo-Nuñez, Catherin Angélica Ruiz-Cisneros, Paul Martín Herrera-Plasencia
Heliyon.2024; 10(16): e35919. CrossRef - Radix molaris is a hidden truth of mandibular first permanent molars: A descriptive- analytic study using cone beam computed tomography
Mohammed A. Alobaid, Saurabh Chaturvedi, Ebtihal Mobarak S. Alshahrani, Ebtsam M. Alshehri, Amal S. Shaiban, Mohamed Khaled Addas, Giuseppe Minervini
Technology and Health Care.2023; 31(5): 1957. CrossRef - Prevalence of Radix Entomolaris in Mandibular Permanent Molars Analyzed by Cone-Beam CT in the Saudi Population of Ha'il Province
Moazzy I Almansour, Ahmed A Madfa, Adhwaa F Algharbi, Reem Almuslumani, Noeer K Alshammari, Ghufran M Al Hussain
Cureus.2023;[Epub] CrossRef - Prevalence of radix entomolaris in India and its comparison with the rest of the world
Sumit MOHAN, Jyoti THAKUR
Minerva Dental and Oral Science.2022;[Epub] CrossRef - Radix Paramolaris an Endodontic Challenge: A Case Report
Ashwini B Prasad, Deepak Raisingani, Ridhima Gupta, Rimjhim Jain
Journal of Mahatma Gandhi University of Medical Sciences and Technology.2022; 7(1): 32. CrossRef - Evaluation of Radix Entomolaris and Middle Mesial Canal in Mandibular Permanent First Molars in an Iraqi Subpopulation Using Cone‐Beam Computed Tomography
Ranjdar Mahmood Talabani, Kazhan Omer Abdalrahman, Rawa Jamal Abdul, Dlsoz Omer Babarasul, Sara Hilmi Kazzaz, Heng Bo Jiang
BioMed Research International.2022;[Epub] CrossRef - Evaluation of Root Canal Configuration of Maxillary and Mandibular First Molar by CBCT: A Retrospective Cross-Sectional Study
Rakan Rafdan Alhujhuj, Rizwan Jouhar, Muhammad Adeel Ahmed, Abdullatif Abdulrahman Almujhim, Mohammed Tariq Albutayh, Necdet Adanir
Diagnostics.2022; 12(9): 2121. CrossRef - Ethnical Anatomical Differences in Mandibular First Permanent Molars between Indian and Saudi Arabian Subpopulations: A Retrospective Cross-sectional Study
Abdulwahab Alamir, Mohammed Mashyakhy, Apathsakayan Renugalakshmi, Thilla S Vinothkumar, Anandhi S Arthisri, Ahmed Juraybi
The Journal of Contemporary Dental Practice.2021; 22(5): 484. CrossRef
- A comprehensive investigation into the prevalence of dental anomalies across Saudi Arabia, a systematic review
- 3,512 View
- 53 Download
- 14 Crossref
- C-shaped root canals of mandibular second molars in a Korean population: a CBCT analysis
- Hee-Sun Kim, Daun Jung, Ho Lee, Yoon-Sic Han, Sohee Oh, Hye-Young Sim
- Restor Dent Endod 2018;43(4):e42. Published online November 1, 2018
- DOI: https://doi.org/10.5395/rde.2018.43.e42
-
Abstract
PDFPubReaderePub
Objectives The purpose of this study was to investigate the C-shaped root canal anatomy of mandibular second molars in a Korean population.
Materials and Methods A total of 542 teeth were evaluated using cone-beam computed tomography (CBCT). The canal shapes were classified according to a modified version of Melton's method at the level where the pulp chamber floor became discernible.
Results Of the 542 mandibular second molars, 215 (39.8%) had C-shaped canals, 330 (53%) had 3 canals, 17 (3.3%) had 2 canals, 12 (2.2%) had 4 canals, and 8 (1.7%) had 1 canal. The prevalence of C-shaped canals was 47.8% in females and 28.4% in males. Seventy-seven percent of the C-shaped canals showed a bilateral appearance. The prevalence of C-shaped canals showed no difference according to age or tooth position. Most teeth with a C-shaped canal system presented Melton's type II (45.6%) and type III (32.1%) configurations.
Conclusions There was a high prevalence of C-shaped canals in the mandibular second molars of the Korean population studied. CBCT is expected to be useful for endodontic diagnosis and treatment planning of mandibular second molars.
-
Citations
Citations to this article as recorded by- A cone-beam computed tomography-based morphometric comparison of mandibular molars between Han Chinese and Malays
Jacob John, Wei Cheong Ngeow, Ting-Chun Shen, Lih-Jyh Fuh, Phrabhakaran Nambiar, Yen-Wen Shen, Jui-Ting Hsu
Journal of Dental Sciences.2026; 21(1): 265. CrossRef - Prevalence of C‐Shaped Canals in Maxillary Molars in an Iranian Population: A Cone‐Beam Computed Tomography Analysis
Amin Salem Milani, Shahin Namvar Asl Amirkhizi, Tahmineh Razi, Ahmad Nouroloyouni, Pouya Sabanik, Nikhat Kaura
International Journal of Clinical Practice.2026;[Epub] CrossRef - Evaluation of mandibular and maxillary second molar root canal anatomy in a Turkish subpopulation using CBCT: comparison of Briseno-Marroquin and Vertucci classifications
Hüseyin Gürkan Güneç, İpek Öreroğlu, Kemal Çağlar, Kader Cesur Aydin
BMC Medical Imaging.2025;[Epub] CrossRef - Dentin thickness of C-shaped root canal walls in mandibular premolars based on cone-beam computed tomography: a retrospective cross-sectional study
Elif Aslan, Ali Canberk Ulusoy, Bilge Hakan Sen, B. Guniz Baksi, Erinc Onem, Ali Mert
Restorative Dentistry & Endodontics.2025; 50(2): e18. CrossRef - Prevalence of c-shaped canal morphology in premolar and molar teeth assessed by cone-beam computed tomography: systematic review and meta-analysis
Faezeh Yousefi, Younes Mohammadi, Elham Shokri
BMC Oral Health.2025;[Epub] CrossRef - Anatomical complexity in mandibular second molars: prevalence of C-shaped canals, radicular grooves, taurodontism, and radices molarum in Saudi population
Ahmed A. Madfa, Abdullah F. Alshammari, Eyad Almagadawyi, Ebtsam A. Aledaili, Afaf Al-Haddad
Scientific Reports.2025;[Epub] CrossRef - Imaging Findings of Clinical Significance in Endodontics During Cone Beam Computed Tomography Scanning of the Upper Airway—The Anterior, Bilateral, C-Shaped, Dual of Mandibular Root Canals: A Brief Case Report
Edgar García-Torres, Diana Laura Grissel Guerrero-Falcón, Hugo Alejandro Bojórquez-Armenta, Oscar Eduardo Almeda-Ojeda, Víctor Hiram Barajas-Pérez, Luis Javier Solís-Martínez
Diagnostics.2025; 15(24): 3157. CrossRef - Frequency of C-Shaped Root Canals in Permanent Mandibular Second Molars in a Sample of Pakistani Population using Cone Beam Computed Tomography
Syed Nabeel Ahmed, Muhammad Mansoor Majeed, Sakina Kazmi, Muhammad Omar Ansari
Pakistan Journal of Health Sciences.2024; : 109. CrossRef - ANÁLISE DAS VARIAÇÕES ANATÔMICAS DE CANAIS C-SHAPED NOS MOLARES INFERIORES: UMA REVISÃO INTEGRATIVA DA LITERATURA
Larissa Eulália Pereira, Thayana Karla Guerra Lira dos Santos
Revista Contemporânea.2024; 4(5): e4264. CrossRef - External Validation of the Effect of the Combined Use of Object Detection for the Classification of the C-Shaped Canal Configuration of the Mandibular Second Molar in Panoramic Radiographs: A Multicenter Study
Sujin Yang, Kee-Deog Kim, Yoshitaka Kise, Michihito Nozawa, Mizuho Mori, Natsuho Takata, Akitoshi Katsumata, Yoshiko Ariji, Wonse Park, Eiichiro Ariji
Journal of Endodontics.2024; 50(5): 627. CrossRef - A Cone‐Beam Computed Tomography Evaluation of C‐Shaped Canal Configuration in Maxillary Molars Among an Iranian Population
Nafiseh Nikkerdar, Mohammad Moslehi, Amin Golshah, Mario Dioguardi
International Journal of Dentistry.2024;[Epub] CrossRef - Root and canal morphology of mandibular second molars in an Egyptian subpopulation: a cone-beam computed tomography study
Shehabeldin Mohamed Saber, Mohammed abou El Seoud, Shaimaa Mohamed Abu el Sadat, Nawar Naguib Nawar
BMC Oral Health.2023;[Epub] CrossRef - Comprehensive evaluation of root and root canal morphology of mandibular second molars in a Saudi subpopulation evaluated by cone-beam computed tomography
Moazzy I. Almansour, Saad M. Al‑Zubaidi, Abdulmjeed S. Enizy, Ahmed A. Madfa
BMC Oral Health.2022;[Epub] CrossRef - Assessment of C-Shaped Canal Morphology in Mandibular and Maxillary Second Molars in an Iraqi Subpopulation Using Cone-Beam Computed Tomography
Kazhan Abdalrahman, Ranjdar Talabani, Sara Kazzaz, Dlsoz Babarasul, Berndt Koslowski
Scanning.2022; 2022: 1. CrossRef - Cone-beam computed tomography evaluation of C-shaped root canal system in mandibular second molars in kuwaiti sub-population
AbdullahJassim Alenezi, Saad Al-Nazhan, Nassr Al-Maflehi, MazenA Aldosimani
Saudi Endodontic Journal.2022; 12(3): 283. CrossRef - Prevalence and morphology of C‐shaped and non‐C‐shaped root canal systems in mandibular second molars
T Fenelon, P Parashos
Australian Dental Journal.2022;[Epub] CrossRef - Evaluation of C-shaped canals in mandibular second molars of a selected patient group using cone beam computed tomography: prevalence, configuration and radicular groove types
Sema Sönmez Kaplan, Tuna Kaplan, Güzide Pelin Sezgin
Odontology.2021; 109(4): 949. CrossRef - Prevalência estimada de canais “C- Shaped”: Uma revisão sistemática e meta-análise
Natália Pereira da Silva Falcão, Sandro Junio de Oliveira Tavares, Ludmila Silva Guimarães, Katherine Azevedo Batistela Rodrigues Thuller, Leonardo dos Santos Antunes, Estefano Borgo Sarmento, Fellipe Navarro Azevedo de Azevedo, Cinthya Cristina Gomes, Ca
Revista Científica Multidisciplinar Núcleo do Conhecimento.2020; : 91. CrossRef - Preferred Reporting Items for Epidemiologic Cross-sectional Studies on Root and Root Canal Anatomy Using Cone-beam Computed Tomographic Technology: A Systematized Assessment
Jorge N.R. Martins, Anil Kishen, Duarte Marques, Emmanuel João Nogueira Leal Silva, João Caramês, António Mata, Marco A. Versiani
Journal of Endodontics.2020; 46(7): 915. CrossRef - Clinical and radiological assessment of the anatomical and topographic structure of the root canals of teeth in patients of different age groups
N.B. Petrukhina, O.A. Zorina, O.A. Boriskina, I.S. Berkutova, V.A. Venediktova, R.R. Saltovets
Stomatologiya.2020; 99(5): 32. CrossRef
- A cone-beam computed tomography-based morphometric comparison of mandibular molars between Han Chinese and Malays
- 3,209 View
- 15 Download
- 20 Crossref
- CBCT study of mandibular first molars with a distolingual root in Koreans
- Hee-Ho Kim, Hyoung-Hoon Jo, Jeong-Bum Min, Ho-Keel Hwang
- Restor Dent Endod 2018;43(3):e33. Published online July 30, 2018
- DOI: https://doi.org/10.5395/rde.2018.43.e33
-
Abstract
PDFPubReaderePub
Objectives This study aimed to investigate the prevalence of a separate distolingual root and to measure the thickness of the buccal cortical bone in mandibular first molars in Koreans using cone-beam computed tomography (CBCT) images.
Materials and Methods High-quality CBCT data from 432 patients were analyzed in this study. The prevalence of a separate distolingual root of the mandibular first molar was investigated. The distance from the distobuccal and distolingual root apices to the outer surface of the buccal cortical bone was measured. We also evaluated the thickness of the buccal cortical bone.
Results The prevalence of a separate distolingual root (2 separate distal roots with 1 canal in each root; 2R2C) was 23.26%. In mandibular first molars with 2R2C, the distance from the distobuccal root apex to the outer surface of the buccal cortical bone was 5.51 mm. Furthermore, the distance from the distolingual root apex to the outer surface of the buccal cortical bone was 12.09 mm. In mandibular first molars with 2R2C morphology, the thickness of the buccal cortical bone at the distobuccal root apex of the mandibular first molar was 3.30 mm. The buccal cortical bone at the distobuccal root apex was significantly thicker in the right side (3.38 mm) than the left side (3.09 mm) (
p < 0.05).Conclusions A separate distolingual root is not rare in mandibular first molars in the Korean population. Anatomic and morphologic knowledge of the mandibular first molar can be useful in treatment planning, including surgical endodontic treatment.
-
Citations
Citations to this article as recorded by- The association between complex root canal morphology of mandibular anteriors and distolingual roots in mandibular first molars in a Turkish population
Özge Kurt, Elif Solakoğlu
BMC Oral Health.2025;[Epub] CrossRef - Radix molaris is a hidden truth of mandibular first permanent molars: A descriptive- analytic study using cone beam computed tomography
Mohammed A. Alobaid, Saurabh Chaturvedi, Ebtihal Mobarak S. Alshahrani, Ebtsam M. Alshehri, Amal S. Shaiban, Mohamed Khaled Addas, Giuseppe Minervini
Technology and Health Care.2023; 31(5): 1957. CrossRef - Prevalence of radix entomolaris in India and its comparison with the rest of the world
Sumit MOHAN, Jyoti THAKUR
Minerva Dental and Oral Science.2022;[Epub] CrossRef - A critical analysis of laboratory and clinical research methods to study root and canal anatomy
Hany Mohamed Aly Ahmed
International Endodontic Journal.2022; 55(S2): 229. CrossRef - Three‐Rooted Permanent Mandibular First Molars: A Meta‐Analysis of Prevalence
Nyan M. Aung, Kyaw K. Myint, Luca Testarelli
International Journal of Dentistry.2022;[Epub] CrossRef - Reproducibilidad en el diagnóstico imagenológico de periodontitis apical a partir de CBCT
Sandra Milena Buitrago Rojas, Yeny Zulay Castellanos Dominguez, Jhonny Alexander Contreras Vargas, Yosdi Tomás Solano Diaz, Eder Fabián Gutierrez Argote
Acta Odontológica Colombiana.2020;[Epub] CrossRef - Assessment of Root and Root Canal Morphology of Human Primary Molars using CBCT
Yoomin Choi, Seonmi Kim, Namki Choi
THE JOURNAL OF THE KOREAN ACADEMY OF PEDTATRIC DENTISTRY.2020; 47(1): 25. CrossRef - The prevalence of radix molaris in the mandibular first molars of a Saudi subpopulation based on cone-beam computed tomography
Hassan AL-Alawi, Saad Al-Nazhan, Nassr Al-Maflehi, Mazen A. Aldosimani, Mohammed Nabil Zahid, Ghadeer N. Shihabi
Restorative Dentistry & Endodontics.2020;[Epub] CrossRef - Preferred Reporting Items for Epidemiologic Cross-sectional Studies on Root and Root Canal Anatomy Using Cone-beam Computed Tomographic Technology: A Systematized Assessment
Jorge N.R. Martins, Anil Kishen, Duarte Marques, Emmanuel João Nogueira Leal Silva, João Caramês, António Mata, Marco A. Versiani
Journal of Endodontics.2020; 46(7): 915. CrossRef - Evaluation of roots and canal systems of mandibular first molars in a vietnamese subpopulation using cone-beam computed tomography
KhoaVan Pham, AnhHoang Lan Le
Journal of International Society of Preventive and Community Dentistry.2019; 9(4): 356. CrossRef
- The association between complex root canal morphology of mandibular anteriors and distolingual roots in mandibular first molars in a Turkish population
- 2,565 View
- 10 Download
- 10 Crossref
Case Report
- Mandibular bone necrosis after use of paraformaldehyde-containing paste
- Chi-hwan Lee, Yoorina Choi, Sujung Park
- Restor Dent Endod 2016;41(4):332-337. Published online November 8, 2016
- DOI: https://doi.org/10.5395/rde.2016.41.4.332
-
Abstract
PDFPubReaderePub
Paraformaldehyde has been used in the past as a pulpotomy agent. However, it has a severe cytotoxic effect and may cause alveolar bone necrosis. Depulpin, a devitalizing agent containing 49% paraformaldehyde, is no longer used frequently due to its severe side effects. In the two cases described in the present study, Depulpin was used as a devitalizing agent during root canal treatment. It caused a gradual loss of sensibility in adjacent teeth, gingival necrosis, and osteomyelitis. This case report demonstrates the serious side effects of using a paraformaldehyde-containing paste as a devitalizing agent for pulp, particularly mandibular bone necrosis.
-
Citations
Citations to this article as recorded by- Numb chin syndrome caused by paraformaldehyde-containing devitalizing agent – Case report
Jyh-Kwei Chen, Yeung-Yi Hsu, Chun-Pin Chiang, Meng-Ling Chiang
Journal of Dental Sciences.2023; 18(2): 955. CrossRef - Non-radiation and non-drug–induced maxillary osteomyelitis: Study of underlying risk factors, presentation, management and treatment outcomes
Kumar Nilesh, Pankaj Patil, Digvijay Patil, Monica Patil
Medical Journal Armed Forces India.2022; 78: S145. CrossRef - Acute toxicity potential and impact on periodontal and periapical tissue of Pulp Out: A paste contained jatropha, sidaguri, and melittin
Maria Tanumihardja, A.M. Windha, N. Musfirah, G.K. Punggawa, Andi Fatima, A.H.M. Nur Fadhila, Esfandiary, Nurhayaty Natsir, Husni Cangara, Lukman Muslimin
Toxicology Reports.2022; 9: 1788. CrossRef - Comparative evaluation of the effect of two pulpal medicaments on pain and bleeding status of mandibular molars with irreversible pulpitis post-failure of inferior alveolar nerve block: a double-blind, randomized, clinical trial
Naomi Ranjan Singh, Lora Mishra, Ajinkya M. Pawar, Nike Kurniawati, Dian Agustin Wahjuningrum
PeerJ.2022; 10: e13397. CrossRef - Dental implant restoration of mandibular bone necrosis defects caused by use of paraformaldehyde-containing paste: A case report
Won-Pyo Lee, Ho-Keel Hwang, Hyoung-Hoon Jo
Oral Biology Research.2019; 43(1): 110. CrossRef - Is Panoramic Radiography an Accurate Imaging Technique for the Detection of Endodontically Treated Asymptomatic Apical Periodontitis?
Cosimo Nardi, Linda Calistri, Giulia Grazzini, Isacco Desideri, Chiara Lorini, Mariaelena Occhipinti, Francesco Mungai, Stefano Colagrande
Journal of Endodontics.2018; 44(10): 1500. CrossRef - A case of high density abnormality in x-ray findings of mandible caused by leakage of root canal filling paste
Haruko Kashiwamura, Kyoko Oka, Yoko Tuchihashi, Hanako Yoshioka, Mayumi Kato, Atsuko Baba, Toyohiro Kagawa, Kazuhiko Okamura, Masao Ozaki
Pediatric Dental Journal.2017; 27(3): 162. CrossRef
- Numb chin syndrome caused by paraformaldehyde-containing devitalizing agent – Case report
- 4,673 View
- 25 Download
- 7 Crossref
Research Articles
- Healing outcomes of root canal treatment for C-shaped mandibular second molars: a retrospective analysis
- Hye-Ra Ahn, Young-Mi Moon, Sung-Ok Hong, Min-Seock Seo
- Restor Dent Endod 2016;41(4):262-270. Published online August 29, 2016
- DOI: https://doi.org/10.5395/rde.2016.41.4.262
-
Abstract
PDFPubReaderePub
Objectives This study aimed to evaluate the healing rate of non-surgical endodontic treatment between C-shaped and non-C-shaped mandibular second molars.
Materials and Methods Clinical records and radiological images of patients who had undergone endodontic treatment on mandibular second molars between 2007 and 2014 were screened. The periapical index scoring system was applied to compare healing outcomes. Information about preoperative and postoperative factors as well as the demographic data of the patients was acquired and evaluated using chi-square and multinomial logistic regression tests.
Results The total healing rate was 68.4%. Healing rates for the mandibular second molar were 70.9% in C-shaped canals (
n = 79) and 66.6% in non-C-shaped ones (n = 117). The difference was not statistically significant.Conclusions The presence of a C-shaped canal in the mandibular second molar did not have a significantly negative effect on healing after treatment. Instead, proper pulpal diagnosis and final restoration were indicated as having significantly greater influence on the healing outcomes of C-shaped and non-C-shaped canals, respectively.
-
Citations
Citations to this article as recorded by- Predicting early endodontic treatment failure following primary root canal treatment
Young-Eun Jang, Yemi Kim, Sin-Young Kim, Bom Sahn Kim
BMC Oral Health.2024;[Epub] CrossRef - Factors Influencing Non-Surgical Root Canal Treatment Outcomes in Mandibular Second Molars: A Retrospective Cone-Beam Computed Tomography Analysis
Da-Min Park, Woo-Hyun Seok, Ji-Young Yoon
Journal of Clinical Medicine.2024; 13(10): 2931. CrossRef - Retrospective Assessment of Healing Outcome of Endodontic Treatment for Mandibular Molars with C-shaped Root Canal
Kishore Kumar Majety, Basanta Kumar Choudhury, Anika Bansal, Achla Sethi, Jaina Panjabi
The Journal of Contemporary Dental Practice.2017; 18(7): 591. CrossRef
- Predicting early endodontic treatment failure following primary root canal treatment
- 2,912 View
- 26 Download
- 3 Crossref
- Proximity of the mandibular molar root apex from the buccal bone surface: a cone-beam computed tomographic study
- Dokyung Kim, Jung-Hong Ha, Myoung-Uk Jin, Young-Kyung Kim, Sung Kyo Kim
- Restor Dent Endod 2016;41(3):182-188. Published online July 14, 2016
- DOI: https://doi.org/10.5395/rde.2016.41.3.182
-
Abstract
PDFPubReaderePub
Objectives The purpose of this study was to evaluate the proximity of the mandibular molar apex to the buccal bone surface in order to provide anatomic information for apical surgery.
Materials and Methods Cone-beam computed tomography (CBCT) images of 127 mandibular first molars and 153 mandibular second molars were analyzed from 160 patients' records. The distance was measured from the buccal bone surface to the root apex and the apical 3.0 mm on the cross-sectional view of CBCT.
Results The second molar apex and apical 3 mm were located significantly deeper relative to the buccal bone surface compared with the first molar (
p < 0.01). For the mandibular second molars, the distance from the buccal bone surface to the root apex was significantly shorter in patients over 70 years of age (p < 0.05). Furthermore, this distance was significantly shorter when the first molar was missing compared to nonmissing cases (p < 0.05). For the mandibular first molars, the distance to the distal root apex of one distal-rooted tooth was significantly greater than the distance to the disto-buccal root apex (p < 0.01). In mandibular second molar, the distance to the apex of C-shaped roots was significantly greater than the distance to the mesial root apex of non-C-shaped roots (p < 0.01).Conclusions For apical surgery in mandibular molars, the distance from the buccal bone surface to the apex and apical 3 mm is significantly affected by the location, patient age, an adjacent missing anterior tooth, and root configuration.
-
Citations
Citations to this article as recorded by- Expert consensus on intentional tooth replantation
Zhengmei Lin, Dingming Huang, Shuheng Huang, Zhi Chen, Qing Yu, Benxiang Hou, Lihong Qiu, Wenxia Chen, Jiyao Li, Xiaoyan Wang, Zhengwei Huang, Jinhua Yu, Jin Zhao, Yihuai Pan, Shuang Pan, Deqin Yang, Weidong Niu, Qi Zhang, Shuli Deng, Jingzhi Ma, Xiuping
International Journal of Oral Science.2025;[Epub] CrossRef - Outcome of intentional replantation of endodontically treated teeth with periapical pathosis: A systematic review and meta‐analysis
Faizan Javed, Kamil Zafar, Farhan R. Khan
Australian Endodontic Journal.2023; 49(S1): 494. CrossRef - Proximity of maxillary molar apexes to the cortical bone surface and the maxillary sinus
Han Shin Lee, Dokyung Kim, Sung Kyo Kim
Restorative Dentistry & Endodontics.2022;[Epub] CrossRef - Alveolar bone thickness overlying healthy maxillary and mandibular teeth: A systematic review and meta-analysis
Marziyeh Shafizadeh, Azita Tehranchi, Armin Shirvani, Saeed Reza Motamedian
International Orthodontics.2021; 19(3): 389. CrossRef - Relationship between the anatomic structures and mandibular posterior teeth for endodontic surgery in a Turkish population: a cone-beam computed tomographic analysis
Zeliha Uğur Aydın, Duygu Göller Bulut
Clinical Oral Investigations.2019; 23(9): 3637. CrossRef
- Expert consensus on intentional tooth replantation
- 3,008 View
- 7 Download
- 5 Crossref
Case Reports
- Endodontic treatment of a C-shaped mandibular second premolar with four root canals and three apical foramina: a case report
- Thikamphaa Bertrand, Sahng Gyoon Kim
- Restor Dent Endod 2016;41(1):68-73. Published online January 19, 2016
- DOI: https://doi.org/10.5395/rde.2016.41.1.68
-
Abstract
PDFPubReaderePub
This case report describes a unique C-shaped mandibular second premolar with four canals and three apical foramina and its endodontic management with the aid of cone-beam computer tomography (CBCT). C-shaped root canal morphology with four canals was identified under a dental operating microscope. A CBCT scan was taken to evaluate the aberrant root canal anatomy and devise a better instrumentation strategy based on the anatomy. All canals were instrumented to have a 0.05 taper using 1.0 mm step-back filing with appropriate apical sizes determined from the CBCT scan images and filled using a warm vertical compaction technique. A C-shaped mandibular second premolar with multiple canals is an anatomically rare case for clinicians, yet its endodontic treatment may require a careful instrumentation strategy due to the difficulty in disinfecting the canals in the thin root area without compromising the root structure.
-
Citations
Citations to this article as recorded by- Unique root anatomy of mandibular second premolars: clinical strategies for effective disinfection and preservation of dentine structure in root canal treatment—a case report
Ji Wook Jeong, Erika Silguero Gonzalez, Scott R. Makins, Timothy Kirkpatrick
Frontiers in Dental Medicine.2024;[Epub] CrossRef - PRICE 2020 guidelines for reporting case reports in Endodontics: explanation and elaboration
V. Nagendrababu, B. S. Chong, P. McCabe, P. K. Shah, E. Priya, J. Jayaraman, S. J. Pulikkotil, P. M. H. Dummer
International Endodontic Journal.2020; 53(7): 922. CrossRef - A cone-beam computed tomography study of C-shaped root canal systems in mandibular second premolars in a Taiwan Chinese subpopulation
Yi-Chin Chen, Chia-Lun Tsai, Yi-Chen Chen, Gin Chen, Shue-Fen Yang
Journal of the Formosan Medical Association.2018; 117(12): 1086. CrossRef - Anatomic Comparison of Contralateral Premolars
Gaute Floer Johnsen, Sazan Dara, Sameenah Asjad, Pia Titterud Sunde, Håvard Jostein Haugen
Journal of Endodontics.2017; 43(6): 956. CrossRef - Endodontic Management of Dilacerated Maxillary Central Incisor fused to a Supernumerary Tooth using Cone Beam Computed Tomography: An Unusual Clinical Presentation
Thilla S Vinothkumar, Deivanayagam Kandaswamy, Ganesh Arathi, Sathishkumar Ramkumar, Gnanasekaran Felsypremila
The Journal of Contemporary Dental Practice.2017; 18(6): 522. CrossRef
- Unique root anatomy of mandibular second premolars: clinical strategies for effective disinfection and preservation of dentine structure in root canal treatment—a case report
- 3,835 View
- 21 Download
- 5 Crossref
- Use of cone-beam computed tomography and three-dimensional modeling for assessment of anomalous pulp canal configuration: a case report
- Alper Sinanoglu, Dilek Helvacioglu-Yigit, Ibrahim Mutlu
- Restor Dent Endod 2015;40(2):161-165. Published online December 4, 2014
- DOI: https://doi.org/10.5395/rde.2015.40.2.161
-
Abstract
PDFPubReaderePub
Three-dimensional (3D) reconstruction of cone-beam computed tomography (CBCT) scans appears to be a valuable method for assessing pulp canal configuration. The aim of this report is to describe endodontic treatment of a mandibular second premolar with aberrant pulp canal morphology detected by CBCT and confirmed by 3D modeling. An accessory canal was suspected during endodontic treatment of the mandibular left second premolar in a 21 year old woman with a chief complaint of pulsating pain. Axial cross-sectional CBCT scans revealed that the pulp canal divided into mesiobuccal, lingual, and buccal canals in the middle third and ended as four separate foramina. 3D modeling confirmed the anomalous configuration of the fused root with a deep lingual groove. Endodontic treatment of the tooth was completed in two appointments. The root canals were obturated using lateral compaction of gutta-percha and root canal sealer. The tooth remained asymptomatic and did not develop periapical pathology until 12 months postoperatively. CBCT and 3D modeling enable preoperative evaluation of aberrant root canal systems and facilitate endodontic treatment.
-
Citations
Citations to this article as recorded by- Exploring Technological Progress in Three-Dimensional Imaging for Root Canal Treatments: A Systematic Review
Kanwalpreet Kaur, Ravinder S. Saini, Sunil Kumar Vaddamanu, Shashit Shetty Bavabeedu, Vishwanath Gurumurthy, Shan Sainudeen, Vinod Babu Mathew, Shafait Ullah Khateeb, Aida Mokhlesi, Seyed Ali Mosaddad, Artak Heboyan
International Dental Journal.2025; 75(2): 1097. CrossRef - Root Canal Treatment of Oehlers Type III Dens Invaginatus in Maxillary Lateral Incisor and Remote Sinus Tract Using Dental Surgical Microscope and Cone-Beam Computed Tomography
Rie Fujii, Tomohiro Asai, Masashi Yamada, Ryo Sako, Yoshiki Tamiya, Masahiro Furusawa
The Bulletin of Tokyo Dental College.2023; 64(2): 67. CrossRef - CBCT and Micro-CT analysis of the mandibular first premolars with C-shaped canal system in a Chinese population author
Yimeng Zhang, Xunben Weng, Yu Fu, Xuekai Qi, Yihuai Pan, Yu Zhao
BMC Oral Health.2023;[Epub] CrossRef
- Exploring Technological Progress in Three-Dimensional Imaging for Root Canal Treatments: A Systematic Review
- 2,073 View
- 9 Download
- 3 Crossref
- Endodontic treatment of a mandibular first molar with 8 canals: a case report
- Ankit Arora, Shashi Rashmi Acharya, Padmaja Sharma
- Restor Dent Endod 2015;40(1):75-78. Published online October 13, 2014
- DOI: https://doi.org/10.5395/rde.2015.40.1.75
-
Abstract
PDFPubReaderePub
Presented here is a case where 8 canals were located in a mandibular first molar. A patient with continuing pain in mandibular left first molar even after completion of biomechanical preparation was referred by a dentist. Following basic laws of the pulp chamber floor anatomy, 8 canals were located in three steps with 4 canals in each root. In both of the roots, 4 separate canals commenced which joined into two canals and exited as two separate foramina. At 6 mon follow-up visit, the tooth was found to be asymptomatic and revealed normal radiographic periapical area. The case stresses on the fact that understanding the laws of pulp chamber anatomy and complying with them while attempting to locate additional canals can prevent missing canals.
-
Citations
Citations to this article as recorded by- Birooted Mandibular Canine: A Systematic Review and Meta-Analysis
Amelia Hoppe, Kamila Chęcińska, Maciej Chęciński, Natalia Turosz, Maciej Sikora
Journal of Clinical Medicine.2026; 15(9): 3381. CrossRef - How Do Different Image Modules Impact the Accuracy of Working Length Measurements in Digital Periapical Radiography? An In Vitro Study
Vahide Hazal Abat, Rabia Figen Kaptan
Diagnostics.2025; 15(3): 305. CrossRef - Determinants of the Number of Main Canals in a Tooth: Deciphering Potential Mechanisms
Andrea Alejandra Moreno Robalino, José Luis Álvarez Vásquez
Universitas Odontologica.2023;[Epub] CrossRef - Application Of Cone-Beam Computed Tomography In Diagnosis And Treatment Of Multiple Canals– A Case Report
Gyanendra Pratap Singh, Shruthi H Attavar, Sivaji Kavuri
Annals of Dental Specialty.2022; 10(2): 15. CrossRef - Four distal root canals in a two-rooted permanent mandibular first molar
Urvashi M. Ujariya, Foram H. Patel, Rajendra P. Bharatiya, Anjali K. Kothari
Endodontology.2022; 34(3): 212. CrossRef - Utilizing Cone-Beam Computed Tomography for Identifying and Managing Multiple Canals: A Case Report
Gyanendra Pratap Singh, Shruthi H Attavar, Sivaji Kavuri
Journal of Current Research in Oral Surgery.2022; 2(1): 37. CrossRef - Morphology and prevalence of middle canals in the mandibular molars: A systematic review
Rashmi Bansal, Sapna Hegde, Madhusudan Astekar
Journal of Oral and Maxillofacial Pathology.2018; 22(2): 216. CrossRef - Endodontic management of a permanent mandibular first molar with unusual root canal configurations: Two case reports
Mohammad Ahmad Alenezi, Mustafa Aldajani, Hind O. Al-Qathami, Seraj Al-Shommrani
Saudi Endodontic Journal.2017; 7(3): 181. CrossRef
- Birooted Mandibular Canine: A Systematic Review and Meta-Analysis
- 6,579 View
- 36 Download
- 8 Crossref
- Asymmetry in mesial root number and morphology in mandibular second molars: a case report
- Gurudutt Nayak, Shashit Shetty, Rhitu Shekhar
- Restor Dent Endod 2014;39(1):45-50. Published online January 20, 2014
- DOI: https://doi.org/10.5395/rde.2014.39.1.45
-
Abstract
PDFPubReaderePub
Ambiguity in the root morphology of the mandibular second molars is quite common. The most common root canal configuration is 2 roots and 3 canals, nonetheless other possibilities may still exist. The presence of accessory roots is an interesting example of anatomic root variation. While the presence of radix entomolaris or radix paramolaris is regarded as a typical clinical finding of a three-rooted mandibular second permanent molar, the occurrence of an additional mesial root is rather uncommon and represents a possibility of deviation from the regular norms. This case report describes successful endodontic management of a three-rooted mandibular second molar presenting with an unusual accessory mesial root, which was identified with the aid of multiangled radiographs and cone-beam computed tomography imaging. This article also discusses the prevalence, etiology, morphological variations, clinical approach to diagnosis, and significance of supernumerary roots in contemporary clinical dentistry.
- 2,834 View
- 8 Download
Research Article
- An evaluation of canal curvature at the apical one third in type II mesial canals of mandibular molars
- Hye-Rim Yun, Dong-Kyun Lee, Ho-Keel Hwang
- Restor Dent Endod 2012;37(2):104-109. Published online May 18, 2012
- DOI: https://doi.org/10.5395/rde.2012.37.2.104
-
Abstract
PDFPubReaderePub
Objectives The purpose of this study was to evaluate the buccolingual curvature at the apical one third in type II mesial canals of mandibular molars using the radius and angle of curvature.
Materials and Methods Total 100 mandibular molars were selected. Following an endodontic access in the teeth, their distal roots were removed. #15 H- or K-files (Dentsply Maillefer) were inserted into the mesiobuccal and mesiolingual canals of the teeth. Radiographs of the teeth were taken for the proximal view. Among them, type II canals were selected and divided into two subgroups, IIa and IIb. In type IIa, two separate canals merged into one canal before reaching the apex and in type IIb, two separate canals merged into one canal within the apical foramen. The radius and angle of curvature of specimens were examined.
Results In type II, mean radius of curvature in mesiolingual and mesiobuccal canals were 2.82 mm and 3.58 mm, respectively. The radius of the curvature of mesiolingual canals were significantly smaller than that of mesiobuccal canals in type II, and especially in type IIa. However, there were no statistically significant differences in radius of curvature between mesiobuccal and mesiolingual canals in type IIb and there were no significant differences in angle of curvature between type IIa and IIb.
Conclusion In this study, type II mesial canals of mandibular molars showed severe curvature in the proximal view. Especially, mesiolingual canals of type IIa had more abrupt curvature than mesiobuccal canals at the apical one third.
- 1,622 View
- 2 Download
Basic Research
- A retrospective study of the intentionally replanted mandibular second molars with C-shaped root canal configurations
- Won-Jun Shon, Kee-Yeon Kum, Seung-Ho Baek, Woo-Cheol Lee
- J Korean Acad Conserv Dent 2011;36(1):19-25. Published online January 31, 2011
- DOI: https://doi.org/10.5395/JKACD.2011.36.1.19
-
Abstract
PDFPubReaderePub
Objectives The purpose of this retrospective study was to evaluate the success rate of intentionally replanted mandibular second molar with C-shaped canal configurations and to access the impact of preoperative periapical lesion on the success of intentional replantation procedure.
Materials and Methods This retrospective chart review study evaluated 52 intentionally replanted mandibular second molar teeth treated at Seoul National University Dental Hospital Department of Conservative Dentistry from January 2005 to December 2007. Seventeen teeth were lost for the follow-up, and another 6 teeth did not meet inclusion criteria of C-shaped root canal configurations. Healing outcome such as success, uncertain healing, and failure after follow-up was evaluated by clinical criteria and radiographs.
Results The overall success rate was 72.4% for the 29 intentionally replanted C-shaped mandibular second molars. The success rate of replanted teeth with preoperative periapical lesions was similar to that of replanted teeth which have no periapical lesions.
Conclusions Therefore, root canal treatment failure on C-shaped mandibular second molar can be predictably treated by intentional replantation regardless of the presence of periapical lesion.
- 1,931 View
- 10 Download
Case Report
- Root canal treatment of a mandibular second premolar with three separate root canals
- Seok-Ryun Lee, Seol-Hee Shin, Sung-Ok Hong, Chang-Kyu Song, Hoon-Sang Chang, Kyung-San Min
- J Korean Acad Conserv Dent 2010;35(4):302-305. Published online July 31, 2010
- DOI: https://doi.org/10.5395/JKACD.2010.35.4.302
-
Abstract
PDFPubReaderePub
Mandibular premolars show a wide variety of root canal anatomy. Especially, the occurrence of three canals with three separate foramina in mandibular second premolars is very rare. This case report describes the root canal treatment of an unusual morphological configuration of the root canal system and supplements previous reports of the existence of such configuration in mandibular second premolar.
-
Citations
Citations to this article as recorded by- Effective management of mandibular second premolar with root anomalies
Ashwaq Faia Asiri
Saudi Endodontic Journal.2023; 13(1): 28. CrossRef
- Effective management of mandibular second premolar with root anomalies
- 2,804 View
- 11 Download
- 1 Crossref
Original Articles
- A retrospective study on incidence of C-shaped canals in mandibular second molars
- Hee-Sun Kim
- J Korean Acad Conserv Dent 2009;34(4):346-349. Published online July 31, 2009
- DOI: https://doi.org/10.5395/JKACD.2009.34.4.346
-
Abstract
PDFPubReaderePub
Mandibular second molars have many variations in canal configuration. Technical modifications in cleaning, shaping and obturation are required. The purpose of this study was to investigate the root canal anatomy of mandibular second molars. 86 teeth of 85 patients were accessed and evaluated with taking radiographs for working length determination. 27 teeth(31.4%) had C-shaped canals, 43 teeth(50%) had 3 canals, 11 teeth(12.7%) had 4 canals, 5 teeth(5.8%) had 2 canals. Incidence of C-shaped canal was 31.7% in male and 31.1% in female. 30.9% of left mandibular second molar and 31.8% of right mandibular second molar showed C-shaped canals.
- 1,222 View
- 1 Download
- Morphology of the apical root canal system in Korean mandibular first molar
- Hyeon Jeong, Sang-jin Park, Sang-Hyuk Park, Gi-Woon Choi
- J Korean Acad Conserv Dent 2009;34(2):137-144. Published online March 31, 2009
- DOI: https://doi.org/10.5395/JKACD.2009.34.2.137
-
Abstract
PDFPubReaderePub
The aim of this study was to investigate the shapes and diameters of the physiological foramen and anatomy of the root canal at 3mm from apex in mandibular first molars.
Sixty mandibular first molars were randomly selected. The apical anatomy of 60 mandibular first molars was investigated by means of a stereomicroscope (60x magnification).
The results were as follows;
1. There was a high percentage of two physiological foramina in mesial (61.67%) and one foramen in distal(71.66%) roots of mandibular first molars.
2.There was a high frequency of accessory foramina in mesial roots with one foramen (26.07%).
3. The diameters of physiological foramen was as follows:
0.329mm in single mesial foramen
0.266mm in mesiobuccal foramen and 0.246mm in mesiolingual foramen
0.375mm in single distal foramen
0.291mm in distobuccal foramen and 0.237mm in distolingual foramen
4. The most common physiological foramen shape was oval (69.93%).
5. The incidence of isthmus in mesial root at 3mm from apex was 55%. The 3mm-sections contained a complete isthmus 31.66% and a partial isthmus 23.34%.
6. 3mm from the apex, the most common canal shape was oval (50.64%).
Knowledge of the apical anatomy of mandibular first molar would be necessary for success of surgical and nonsurgical endodontic treatment.
-
Citations
Citations to this article as recorded by- Variations in Canal Morphology, Shapes, and Positions of Major Foramen in Maxillary and Mandibular Teeth
B. Swathika, Md. Kalim Ullah, S. Ganesan, Prabu Muthusamy, Prasanna Vuyyuru, Kongkana Kalita, C. Swarnalatha, Suresh J. Babu, Abhishek Singh Nayyar
Journal of Microscopy and Ultrastructure.2021; 9(4): 190. CrossRef - Assessment of Root and Root Canal Morphology of Human Primary Molars using CBCT
Yoomin Choi, Seonmi Kim, Namki Choi
THE JOURNAL OF THE KOREAN ACADEMY OF PEDTATRIC DENTISTRY.2020; 47(1): 25. CrossRef - An evaluation of canal curvature at the apical one third in type II mesial canals of mandibular molars
Hye-Rim Yun, Dong-Kyun Lee, Ho-Keel Hwang
Restorative Dentistry & Endodontics.2012; 37(2): 104. CrossRef
- Variations in Canal Morphology, Shapes, and Positions of Major Foramen in Maxillary and Mandibular Teeth
- 1,794 View
- 1 Download
- 3 Crossref
- A study on the C-shaped root canal system of mandibular second molar
- Dong-Gyun Lee, Jun-Mo Park, Ho-Keel Hwang
- J Korean Acad Conserv Dent 2007;32(4):335-342. Published online July 31, 2007
- DOI: https://doi.org/10.5395/JKACD.2007.32.4.335
-
Abstract
PDFPubReaderePub
C-shaped canals are known to present a complex canal anatomy with numerous fins connecting individual canals, thus requiring supplementary effort to accomplish a successful root canal treatment. This study examined the frequency of the C-shaped mandibular second molars and interrelation between the clinical records and radiographs to recognize them treated in the Department of Conservative Dentistry of the Chosun University Dental Hospital during a six-year period (1998 - 2004). This study reviewed the clinical records of 227 patients who underwent root canal treatment of the mandibular second molars. After opening the chamber, those cases with C-shaped orifices in the pulpal floor were selected, and the C-shaped root canal types were classified according to Melton's criteria. Three experienced dentists evaluated the radiographs of the C-shaped mandibular second molar on a viewer using a magnifying glass in order to determine if the root apex was fused or separated, the distal root canal was either centered or mesial shifted in the distal root, and if there was bilateral symmetry in a panorama. In conclusion, there is a high frequency of C-shaped mandibular second molars in Koreans. Simultaneous interpretation of the root shape and distal root canal using the preoperative, working length and post-treatment radiographs is important for diagnosing a C-shaped mandibular second molar.
-
Citations
Citations to this article as recorded by- An evaluation of canal curvature at the apical one third in type II mesial canals of mandibular molars
Hye-Rim Yun, Dong-Kyun Lee, Ho-Keel Hwang
Restorative Dentistry & Endodontics.2012; 37(2): 104. CrossRef - A retrospective study on incidence of C-shaped canals in mandibular second molars
Hee-Sun Kim
Journal of Korean Academy of Conservative Dentistry.2009; 34(4): 346. CrossRef
- An evaluation of canal curvature at the apical one third in type II mesial canals of mandibular molars
- 2,791 View
- 15 Download
- 2 Crossref
- Cross-sectional morphology and minimum canal wall widths in C-shaped root of mandibular molars
- Byung-Chul Song, Yong-Bum Cho
- J Korean Acad Conserv Dent 2007;32(1):37-46. Published online January 31, 2007
- DOI: https://doi.org/10.5395/JKACD.2007.32.1.037
-
Abstract
PDFPubReaderePub
The C-shaped canal system is an anatomical variation mostly seen in mandibular second molars, although it can also occur in maxillary and other mandibular molars. The main anatomical feature of C-shaped canals is the presence of fins or web connecting the individual root canals. The complexity of C-shaped canals prevents these canals from being cleaned, shaped, and obturated effectively during root canal therapy, and sometimes it leads to an iatrogenic perforation from the extravagant preparation.
The purpose of this study was to provide further knowledge of the anatomical configuration and the minimal thickness of dentinal wall according to the level of the root.
Thirty extracted mandibular second molars with fused roots and longitudinal grooves on lingual or buccal surface of the root were collected from a native Korean population. The photo images and radiographs from buccal, lingual, apical direction were taken. After access cavity was prepared, teeth were placed in 5.25% sodium hypochlorite solution for 2 hours to dissolve the organic tissue of the root surface and from the root canal system. After bench dried and all the teeth were embedded in a self-curing resin. Each block was sectioned using a microtome (Accutom-50, Struers, Denmark) at interval of 1 mm. The sectioned surface photograph was taken using a digital camera (Coolpix 995, Nikon, Japan) connected to the microscope. 197 images were evaluated for canal configurations and the minimal thickness of dentinal wall between canal and external wall using' Root Thickness Gauge Program' designed with Visual Basic.
The results were as follows:
1. At the orifice level of all teeth, the most frequent observed configuration was Melton's Type C I (73%), however the patterns were changed to type C II and C III when the sections were observed at the apical third. On the other hand, the type C III was observed at the orifice level of only 2 teeth but this type could be seen at apical region of the rest of the teeth.
2. The C-shaped canal showed continuous and semi-colon shape at the orifice level, but at the apical portion of the canal there was high possibility of having 2 or 3 canals.
3. Lingual wall was thinner than buccal wall at coronal, middle, apical thirds of root but there was no statistical differences.
- 1,493 View
- 1 Download
- The influence of different access cavity designs on the fracture strength in endodontically treated mandibular anterior teeth
- Young-Gyun Lee, Hye-Jin Shin, Se-Hee Park, Kyung-Mo Cho, Jin-Woo Kim
- J Korean Acad Conserv Dent 2004;29(6):515-519. Published online November 30, 2004
- DOI: https://doi.org/10.5395/JKACD.2004.29.6.515
-
Abstract
PDFPubReaderePub
Straight access cavity design allows the operator to locate all canals, helps in proper cleaning and shaping, ultimately facilitates the obturation of the canal system. However, change in the fracture strength according to the access cavity designs was not clearly demonstrated yet. The purpose of this study was to determine the influence of different access cavity designs on the fracture strength in endodontically treated mandibular anterior teeth.
Recently extracted mandibular anterior teeth that have no caries, cervical abrasion, and fracture were divided into three groups (Group 1 : conventional lingual access cavity, Group 2 : straight access cavity, Group 3 : extended straight access cavity) according to the cavity designs. After conventional endodontic treatment, cavities were filled with resin core material. Compressive loads parallel to the long axis of the teeth were applied at a crosshead speed of 2mm/min until the fracture occurred. The fracture strength analyzed with ANOVA and the Scheffe test at the 95% confidence level.
The results of this study were as follows :
1. The mean fracture strength decrease in following sequence Group 1 (558.90 ± 77.40 N), Group 2 (494.07 ± 123.98 N) and Group 3 (267.33 ± 27.02 N).
2. There was significant difference between Group 3 and other groups (P = 0.00).
Considering advantage of direct access to apical third and results of this study, straight access cavity is recommended for access cavity form of the mandibular anterior teeth.
-
Citations
Citations to this article as recorded by- Fracture resistance of crown-root fractured teeth repaired with dual-cured composite resin and horizontal posts
Seok-Woo Chang, Yong-Keun Lee, Seung-Hyun Kyung, Hyun-Mi Yoo, Tae-Seok Oh, Dong-Sung Park
Journal of Korean Academy of Conservative Dentistry.2009; 34(5): 383. CrossRef
- Fracture resistance of crown-root fractured teeth repaired with dual-cured composite resin and horizontal posts
- 1,729 View
- 3 Download
- 1 Crossref
 First
First Prev
Prev

