
Articles
- Page Path
- HOME > Restor Dent Endod > Volume 40(2); 2015 > Article
- Case Report Use of cone-beam computed tomography and three-dimensional modeling for assessment of anomalous pulp canal configuration: a case report
- Alper Sinanoglu1, Dilek Helvacioglu-Yigit2, Ibrahim Mutlu3
-
2014;40(2):-165.
DOI: https://doi.org/10.5395/rde.2015.40.2.161
Published online: December 4, 2014
1Department of Oral and Maxillofacial Radiology, Faculty of Dentistry, Kocaeli University, Kocaeli, Turkey.
2Department of Endodontics, Faculty of Dentistry, Kocaeli University, Kocaeli, Turkey.
3Department of Biomechanical Engineering, Faculty of Technology, Kocaeli University, Kocaeli, Turkey.
- Correspondence to Alper Sinanoglu, DDS, PhD. Assistant Professor, Department of Oral and Maxillofacial Radiology, Faculty of Dentistry, Kocaeli University, Yuvacık Yerleşkesi, Başiskele, Kocaeli, Turkey 41190. TEL, +90 2623442222; FAX, +90 2623442109; alpersinanoglu@yahoo.com
• Received: August 8, 2014 • Accepted: October 22, 2014
©Copyrights 2015. The Korean Academy of Conservative Dentistry.
This is an Open Access article distributed under the terms of the Creative Commons Attribution Non-Commercial License (http://creativecommons.org/licenses/by-nc/3.0/) which permits unrestricted non-commercial use, distribution, and reproduction in any medium, provided the original work is properly cited.
- 2,051 Views
- 9 Download
- 3 Crossref
Abstract
- Three-dimensional (3D) reconstruction of cone-beam computed tomography (CBCT) scans appears to be a valuable method for assessing pulp canal configuration. The aim of this report is to describe endodontic treatment of a mandibular second premolar with aberrant pulp canal morphology detected by CBCT and confirmed by 3D modeling. An accessory canal was suspected during endodontic treatment of the mandibular left second premolar in a 21 year old woman with a chief complaint of pulsating pain. Axial cross-sectional CBCT scans revealed that the pulp canal divided into mesiobuccal, lingual, and buccal canals in the middle third and ended as four separate foramina. 3D modeling confirmed the anomalous configuration of the fused root with a deep lingual groove. Endodontic treatment of the tooth was completed in two appointments. The root canals were obturated using lateral compaction of gutta-percha and root canal sealer. The tooth remained asymptomatic and did not develop periapical pathology until 12 months postoperatively. CBCT and 3D modeling enable preoperative evaluation of aberrant root canal systems and facilitate endodontic treatment.
Introduction
Conventional endodontics relies on intraoral radiograph which can provide various information on the diagnosis of anatomical variations, the morphology and curvature of roots, configuration and number of root canals, and estimation of the preoperative canal length. Intraoral radiographs obtained at different beam angulations reveal various perspectives of multirooted teeth, but such two-dimensional imaging of three-dimensional (3D) anatomy is limited by superimposition and geometric distortion.1 Cone-beam computed tomography (CBCT) provides precise 3D images to facilitate diagnosis and treatment.2 However, endodontics requires a high level of image detail, and CBCT scans have lower spatial resolution than intraoral radiographs. CBCT may be justifiable where intraoral radiographs provide equivocal or inadequate information for treatment planning, as in the case of root canal system anomalies.1,2,3
The success of endodontic treatment depends partly on recognition of anatomic variations.4 For example, the pulp canal configuration of mandibular second premolars varies in about one-third of the population and may present as C-shaped canals.5,6 The reported incidence rate of two or more foramina in mandibular second premolars is 8.2%, whereas that in mandibular first premolars is 21.1%.5 Reports of three or more canals in mandibular second premolars are quite rare.7,8,9,10,11 Such anatomic variations have been investigated by micro-computed tomography (micro-CT). Micro-CT enables 3D assessment of the root canal system, but it can be used only in vitro.12,13
Here, we describe the endodontic treatment of a mandibular second premolar with aberrant pulp canal morphology detected by CBCT and confirmed by 3D modeling.
Case Report
A 21 year old woman was referred to the Faculty of Dentistry, Kocaeli University, Turkey, because of the pulsating pain in mandibular permanent left second premolar. The first premolar had been extracted. Intraoral examination revealed a carious lesion on the mesial and distal aspect of the tooth in proximity to the pulp chamber. The tooth was sensitive to percussion. Cold test revealed a strong and prolonged reaction. Periapical radiograph suggested abnormal root canal morphology dividing into multiple root canals with no periapical radiolucency (Figure 1a). The tooth was diagnosed as irreversible pulpitis, and endodontic treatment was initiated. Access was gained to the pulp chamber under rubber dam isolation, and all carious material was removed. Canal orifices were not easily located because of their apical positioning. Exploration with magnifying loupes (Heine HR Binocular Loupe, Heine Optotechnik, Herrsching, Germany) disclosed three pulp canal orifices. Intraoral radiographs taken at different angulations to evaluate working length suggested the presence of an accessory canal, and advanced imaging was performed. Informed consent was obtained from the patient.
CBCT (96 kVp, 12 mA, 5.5 cm-diameter field of view, and 5.0 cm-height, Planmeca ProMax 3D Max, Planmeca Oy, Helsinki, Finland) revealed a single pulp canal at the cervical third of the root. A high resolution (voxel size, 0.100 mm3) was used to investigate the cross-sectional morphology. After image acquisition, the CBCT images were subsequently reconstructed with Planmeca Romexis (Planmeca Oy). For 3D modeling, images were exported into the computer in DICOM format and were imported into MIMICS software (MIMICS version 12.1, Materialise, Leuven, Belgium). A thresholding process was performed to separate the tooth and its root canal from soft tissue. The manual editing tools (i.e., draw and erase functions) were used to restore the mask after the region-growing process. 3D reconstruction of the root surface and root canal configuration models were developed with a smoothing algorithm using 8 and 6 iterations and smoothing factors of 0.6 and 0.4, respectively.
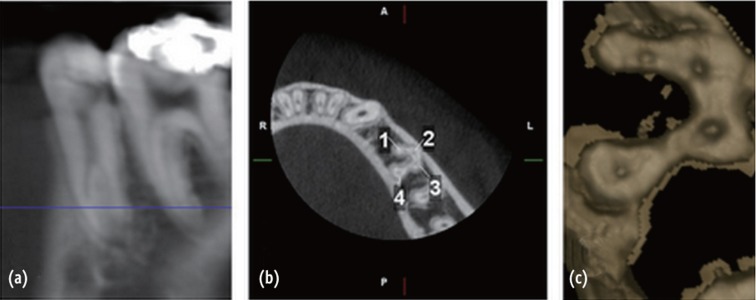
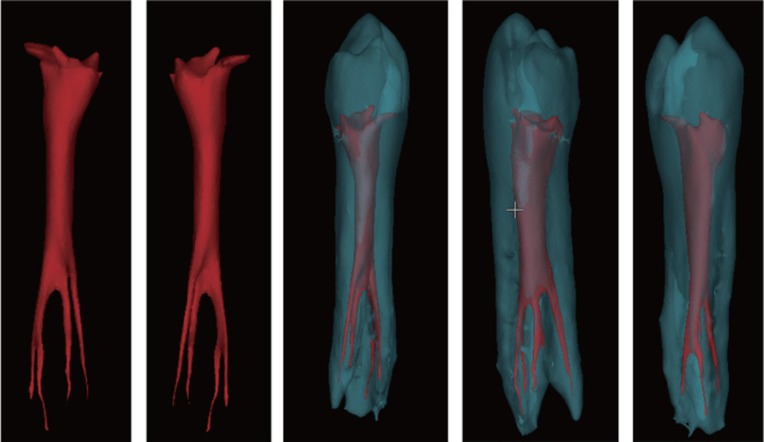
Axial cross-sectional images obtained with 1 mm interval demonstrated three canals in the middle third. One canal bifurcated in the apical third, and four foramina were identified (Figure 2). The root surface had a proximal lingual groove in the middle third. These findings suggested C-shaped canal morphology (Figure 3).14 3D modeling of the CBCT images confirmed an oval-shaped pulp canal in the cervical third and three branches in the middle third of the root. The mesiobuccal canal divided into buccal and lingual branches in the apical third of the root. The root was fused and had a deep lingual groove (Figure 4).
Working length was determined by periapical radiograph and verified with an electronic apex locator (Raypex 6, VDW GmbH, Munich, Germany) (Figure 1b). To gain sufficient access to the canals, the existing opening was enlarged with Gates-Glidden drills (sizes 1 - 3). The canals were cleaned and shaped with rotary files (ProTaper Universal, Dentsply Maillefer, Ballaigues, Switzerland). Obturation was performed by lateral compaction of gutta-percha and root canal sealer (AH Plus, Dentsply Maillefer) (Figure 1c). Twelve months postoperative clinical and radiographic examinations revealed that the tooth was asymptomatic and did not have periapical pathology (Figure 1d).
Discussion
Effective cleaning and disinfection as well as complete obturation of the root canal system are prerequisite for successful endodontic treatment.15 An operating microscope enhances visualization of canal orifices.16 Nevertheless, the lower two-thirds of the pulp canal is difficult to assess from the morphology of the cervical third in mandibular premolars with anomalous pulp canal configuration.14 Yu et al. reported a high probability of pulp canal variations in the middle or apical third of mandibular premolar roots and suggested that most mandibular premolars have an oval cross-sectional morphology in the cervical third.6 We identified a similar morphology. The pulp canal divided in the middle third and the orifice of the fourth canal could not be confirmed by exploration with magnifying loupes.
Relative root outline and shape must be carefully examined in periapical radiographs before endodontic management. Sudden narrowing of a pulp canal on a radiograph suggests the presence of multiple canals.17 CBCT can provide valuable information for assessing such complex morphology.16,18 However, its use in endodontics has been limited to selected cases in which intraoral radiographs were unsatisfactory for treatment planning.19,20 In the present study, CBCT revealed a fourth canal and 3D modeling of the tooth anatomy provided information about both the internal and the external morphology of the root, enabling preoperative evaluation and facilitating treatment.
Evaluation of anamolus root morphology with intraoral radiographs may suffer from the buccolingual superimposition. There may be a fused root with C-shaped canal configuration with seperate foramina, which may mimic seperate root canals in working length radiographs and postoperative radiographs after obturation. In this case, an additional root canal was suspected during the evaluation of working length radiographs and fusion of the root canals were revealed by CBCT.
Mandibular premolars tend to have anatomic variations with complex pulp canal morphology.7,8,11,21,22 The incidence of variations in the number of canals, roots, and foramina is lower for the mandibular second premolar than for the mandibular first premolar.23 Fan et al. classified C-shaped canals in mandibular first premolars and reported that the cross-sectional morphology of pulp canals may change from the orifice to the apex.14 The reported incidence rate of this anomaly in mandibular second premolars is 0.6%.6 In our patient, the isthmus and fused root morphology presented a C-shaped canal. To the best of our knowledge, this is the first report of a C-shaped canal with four separate foramina in a mandibular second premolar.
Conclusions
CBCT and 3D modeling can aid in pre-operative evaluation of anomalous root canal systems and facilitate endodontic treatment. The CBCT-based approach is particularly important in cases where anatomic variations cannot be adequately confirmed using intraoral radiographs.
- 1. Directorate-General for Energy Directorate D-Nuclear Energy Unit D4-Radiation Protection: Radiation protection no. 172: cone beam CT for dental and maxillofacial radiology, Evidence Based Guidelines. Luxembourg: European Commission; 2012. p. 61-64. updated 2014 Nov 13]. Available from: http://ec.europa.eu/energy/nuclear/radiation_protection/doc/publication/172.pdf.
- 2. American Association of Endodontists: Endodontics. Colleagues for excellence: cone beam computed tomography in endodontics. 2011;Summer. 7. updated 2014 Nov 13]. Available from: http://www.aae.org/colleagues/.
- 3. Lee MH, Ha JH, Jin MU, Kim YK, Kim SK. Endodontic treatment of maxillary lateral incisors with anatomical variations. Restor Dent Endod 2013;38:253-257.ArticlePubMedPMC
- 4. Robinson S, Czerny C, Gahleitner A, Bernhart T, Kainberger FM. Dental CT evaluation of mandibular first premolar root configurations and canal variations. Oral Surg Oral Med Oral Pathol Oral Radiol Endod 2002;93:328-332.ArticlePubMed
- 5. Cleghorn BM, Christie WH, Dong CC. The root and root canal morphology of the human mandibular second premolar: a literature review. J Endod 2007;33:1031-1037.ArticlePubMed
- 6. Yu X, Guo B, Li KZ, Zhang R, Tian YY, Wang H, DDS TH. Cone-beam computed tomography study of root and canal morphology of mandibular premolars in a western Chinese population. BMC Med Imaging 2012;12:18.ArticlePubMedPMCPDF
- 7. Holtzman L. Root canal treatment of mandibular second premolar with four root canals: a case report. Int Endod J 1998;31:364-366.ArticlePubMed
- 8. Sachdeva GS, Ballal S, Gopikrishna V, Kandaswamy D. Endodontic management of a mandibular second premolar with four roots and four root canals with the aid of spiral computed tomography: a case report. J Endod 2008;34:104-107.ArticlePubMed
- 9. Glassman GD. Flare-up with associated paresthesia of a mandibular second premolar with three root canals. Oral Surg Oral Med Oral Pathol 1987;64:110-113.ArticlePubMed
- 10. Wong M. Four root canals in a mandibular second premolar. J Endod 1991;17:125-126.ArticlePubMed
- 11. Rhodes JS. A case of unusual anatomy: a mandibular second premolar with four canals. Int Endod J 2001;34:645-648.ArticlePubMedPDF
- 12. Yu DC, Tam A, Schilder H. Root canal anatomy illustrated by microcomputed tomography and clinical cases. Gen Dent 2006;54:331-335.PubMed
- 13. Plotino G, Grande NM, Pecci R, Bedini R, Pameijer CH, Somma F. Three-dimensional imaging using microcomputed tomography for studying tooth macromorphology. J Am Dent Assoc 2006;137:1555-1561.ArticlePubMed
- 14. Fan B, Yang J, Gutmann JL, Fan M. Root canal systems in mandibular first premolars with C-shaped root configurations. Part I: microcomputed tomography mapping of the radicular groove and associated root canal cross-sections. J Endod 2008;34:1337-1341.ArticlePubMed
- 15. Schilder H. Cleaning and shaping the root canal. Dent Clin North Am 1974;18:269-296.ArticlePubMed
- 16. Karanxha L, Kim HJ, Hong SO, Lee W, Kim PS, Min KS. Endodontic management of a C-shaped maxillary first molar with three independent buccal root canals by using cone-beam computed tomography. Restor Dent Endod 2012;37:175-179.ArticlePubMedPMC
- 17. Yoshioka T, Villegas JC, Kobayashi C, Suda H. Radiographic evaluation of root canal multiplicity in mandibular first premolars. J Endod 2004;30:73-74.ArticlePubMed
- 18. Matherne RP, Angelopoulos C, Kulild JC, Tira D. Use of cone-beam computed tomography to identify root canal systems in vitro. J Endod 2008;34:87-89.ArticlePubMed
- 19. Fan B, Ye W, Xie E, Wu H, Gutmann JL. Three-dimensional morphological analysis of C-shaped canals in mandibular first premolars in a Chinese population. Int Endod J 2012;45:1035-1041.ArticlePubMed
- 20. Helvacioglu-Yigit D, Sinanoglu A. Use of cone-beam computed tomography to evaluate C-shaped root canal systems in mandibular second molars in a Turkish subpopulation: a retrospective study. Int Endod J 2013;46:1032-1038.PubMed
- 21. Al-Fouzan KS. The microscopic diagnosis and treatment of a mandibular second premolar with four canals. Int Endod J 2001;34:406-410.ArticlePubMedPDF
- 22. Farmakis ET. Four-rooted mandibular second premolar. Aust Endod J 2008;34:126-128.ArticlePubMed
- 23. Cleghorn BM, Christie WH, Dong CC. The root and root canal morphology of the human mandibular first premolar: a literature review. J Endod 2007;33:509-516.ArticlePubMed
REFERENCES
Figure 1
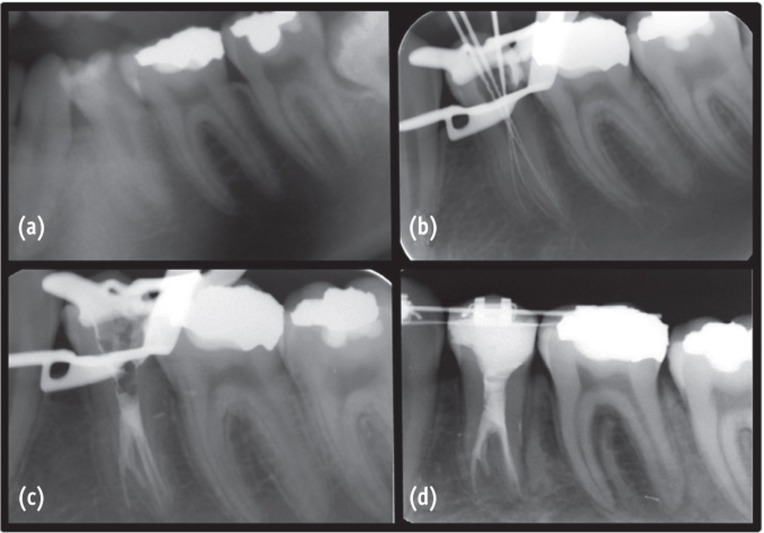
(a) Pre-operative periapical radiograph; (b) Intra-operative periapical radiograph; (c) Post-operative periapical radiograph; (d) 12 months follow-up periapical radiograph of the case.
Figure 2
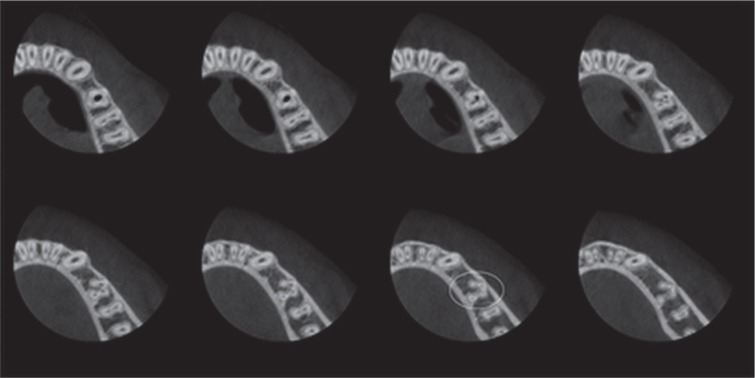
Axial sectional images revealed by CBCT. Note the 4 separate canal configurations marked by circle.
Tables & Figures
REFERENCES
Citations
Citations to this article as recorded by 
- Exploring Technological Progress in Three-Dimensional Imaging for Root Canal Treatments: A Systematic Review
Kanwalpreet Kaur, Ravinder S. Saini, Sunil Kumar Vaddamanu, Shashit Shetty Bavabeedu, Vishwanath Gurumurthy, Shan Sainudeen, Vinod Babu Mathew, Shafait Ullah Khateeb, Aida Mokhlesi, Seyed Ali Mosaddad, Artak Heboyan
International Dental Journal.2025; 75(2): 1097. CrossRef - Root Canal Treatment of Oehlers Type III Dens Invaginatus in Maxillary Lateral Incisor and Remote Sinus Tract Using Dental Surgical Microscope and Cone-Beam Computed Tomography
Rie Fujii, Tomohiro Asai, Masashi Yamada, Ryo Sako, Yoshiki Tamiya, Masahiro Furusawa
The Bulletin of Tokyo Dental College.2023; 64(2): 67. CrossRef - CBCT and Micro-CT analysis of the mandibular first premolars with C-shaped canal system in a Chinese population author
Yimeng Zhang, Xunben Weng, Yu Fu, Xuekai Qi, Yihuai Pan, Yu Zhao
BMC Oral Health.2023;[Epub] CrossRef
 ePub Link
ePub Link Cite
CiteUse of cone-beam computed tomography and three-dimensional modeling for assessment of anomalous pulp canal configuration: a case report
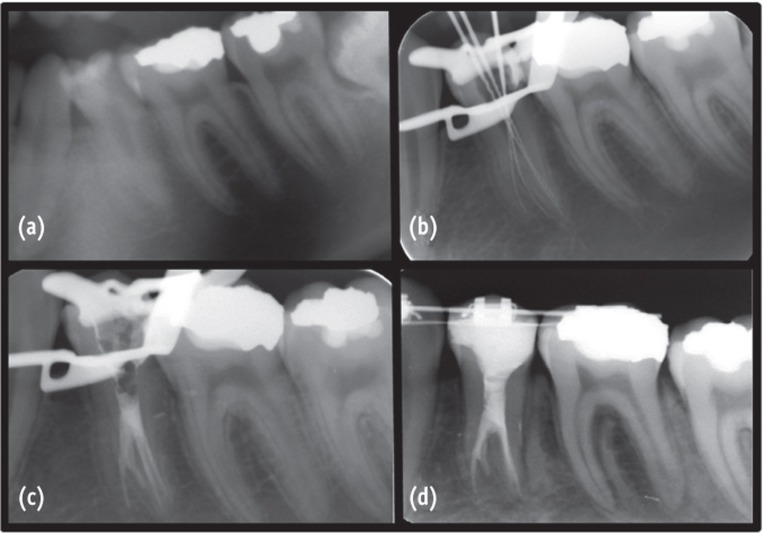
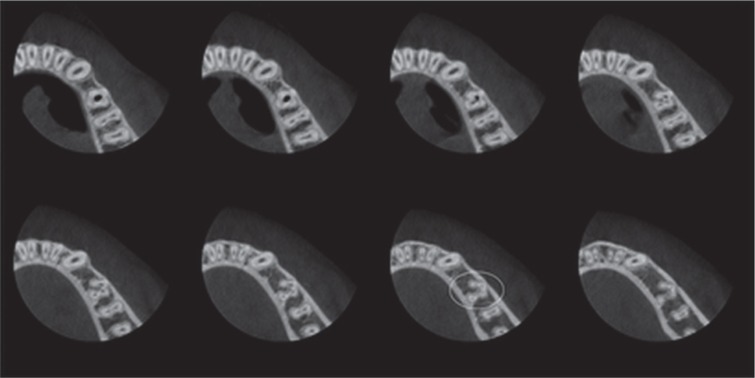
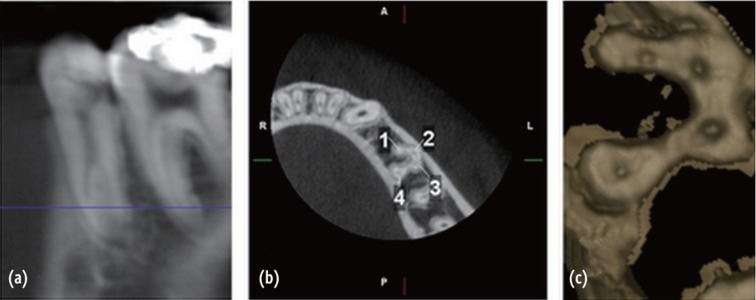

Figure 1 (a) Pre-operative periapical radiograph; (b) Intra-operative periapical radiograph; (c) Post-operative periapical radiograph; (d) 12 months follow-up periapical radiograph of the case.
Figure 2 Axial sectional images revealed by CBCT. Note the 4 separate canal configurations marked by circle.
Figure 3 (a) Sagittal image of the root; (b) Axial image at the apical third presenting a C-shaped canal configuration; (c) Cross-sectional three-dimensional reconstruction demonstrating 4 separate canals.
Figure 4 Three-dimensional modeling of the internal and external root canal morphology. Internal view (red) shows the separate root canal configuration, and the external view (blue) presents fused formation of the anomalous root.
Figure 1
Figure 2
Figure 3
Figure 4
Use of cone-beam computed tomography and three-dimensional modeling for assessment of anomalous pulp canal configuration: a case report

