
Articles
- Page Path
- HOME > Restor Dent Endod > Volume 40(1); 2015 > Article
- Case Report Endodontic treatment of a mandibular first molar with 8 canals: a case report
- Ankit Arora1, Shashi Rashmi Acharya2, Padmaja Sharma3
-
2014;40(1):-78.
DOI: https://doi.org/10.5395/rde.2015.40.1.75
Published online: October 13, 2014
1Department of Conservative Dentistry and Endodontics, M.P. Dental College, Hospital and Oral Research Institute, Vadodara, India.
2Department of Conservative Dentistry and Endodontics, Manipal College of Dental Sciences, Manipal University, Karnataka, India.
3Department of Orthodontics and Dentofacial Orthopaedics, M.P. Dental College, Hospital and Oral Research Institute, Vadodara, India.
- Correspondence to Ankit Arora, BDS, MDS. Senior Lecturer, Department of Conservative Dentistry and Endodontics, M.P. Dental College, Hospital and Oral Research Institute, Vishwajyoti Ashram, Munjmahuda, Vadodara, Gujarat, India 390011. TEL, +9033975629; FAX, +0265-2780644; aroraankit24@gmail.com
• Received: April 23, 2014 • Accepted: August 14, 2014
©Copyrights 2015. The Korean Academy of Conservative Dentistry.
This is an Open Access article distributed under the terms of the Creative Commons Attribution Non-Commercial License (http://creativecommons.org/licenses/by-nc/3.0/) which permits unrestricted non-commercial use, distribution, and reproduction in any medium, provided the original work is properly cited.
- 6,545 Views
- 36 Download
- 8 Crossref
Abstract
- Presented here is a case where 8 canals were located in a mandibular first molar. A patient with continuing pain in mandibular left first molar even after completion of biomechanical preparation was referred by a dentist. Following basic laws of the pulp chamber floor anatomy, 8 canals were located in three steps with 4 canals in each root. In both of the roots, 4 separate canals commenced which joined into two canals and exited as two separate foramina. At 6 mon follow-up visit, the tooth was found to be asymptomatic and revealed normal radiographic periapical area. The case stresses on the fact that understanding the laws of pulp chamber anatomy and complying with them while attempting to locate additional canals can prevent missing canals.
Introduction
Adequate knowledge of root canal system anatomy is indispensable to perform endodontic therapy.1 A major cause of root canal therapy failure is the inability to understand the internal anatomy of the tooth and subsequent incomplete endodontic treatment.2 A good pre-operative radiograph is essential for preventing missed anatomy but it does not always necessarily reveal the actual number of canals present in the root.3 Krasner and Rankow proposed specific laws of symmetry, law of color change, and laws of orifice location based on consistent and identifiable anatomic configurations of pulp chamber.4 These laws help to locate canal orifices on the pulp chamber floor in a systematic way. Visual and diagnostic aids also play an important role in detecting atypical root canal anatomy.5,6
Many investigations using different methodologies have been carried out to understand the internal anatomy of mandibular first molar. Although most prevalent root canal system configuration found are type IV and type I in mesial and distal roots respectively, it is common to find complex anatomy in mandibular first molar.7,8 Number of cases have been reported with more than 5 canals in mandibular first molar.9,10,11,12 Martinez-Berna and Badanelli reported 2 cases where 6 canals were present in mandibular first molar.9 Both the teeth had merging of the canals in distal root. Reeh reported presence of 7 canals in mandibular first molar with 4 canals in mesial root and 3 canals in distal root based on clinical and intra-oral periapical radiographic findings.10 Baziar et al. detected 6 canals in a mandibular first molar using CBCT, with 2 canals in mesial root and 4 canals in the distal root.12 However, following a Pubmed search, no cases reporting more than 7 canals could be found. This case report describes successful non surgical management of a mandibular first molar with 8 canals. Both the roots presented with type II configuration according to modified Vertucci classification.7
Case Report
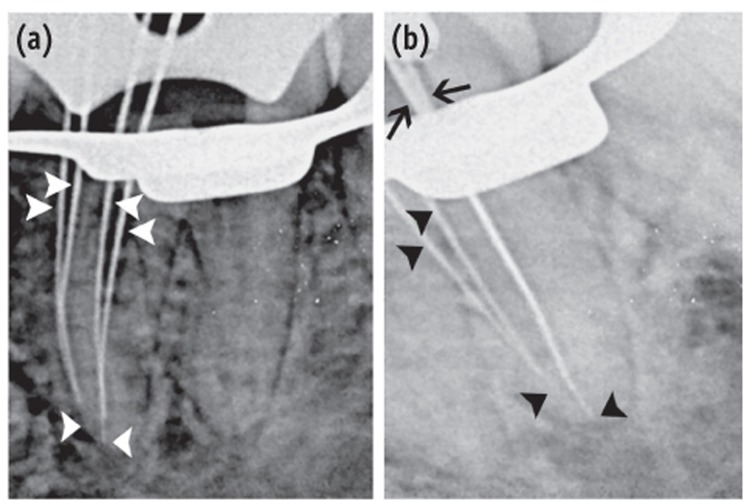
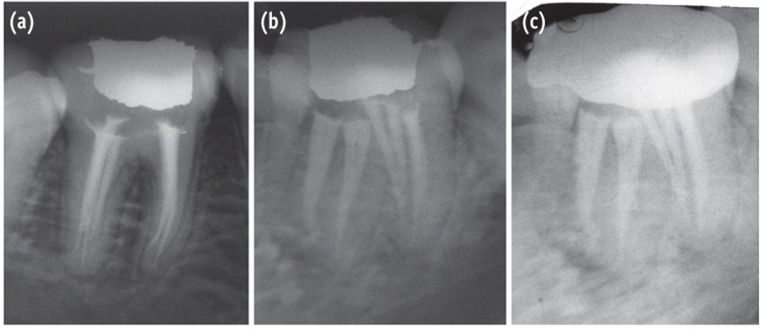
A 30 year-old female patient was referred by a local dentist to the Department of Conservative Dentistry and Endodontics with the chief complaint of continuous pain in lower left back tooth even after completion of the biomechanical preparation. On clinical examination, tenderness on vertical percussion was elicited on mandibular left first molar. Pre-operative radiograph (Figure 1a) and working length radiograph (Figure 1b) were provided by the previous dentist. The preoperative radiograph suffered from an artifact but working length radiograph revealed two important findings. Endodontic files were well short of apex in both roots, and roof of the pulp chamber was partially intact (Figure 1b). Based on the above findings, we could anticipate the reasons for the continuing symptoms. A diagnosis of irreversible pulpitis with apical periodontitis was formulated and completion of root canal treatment was planned. Inferior alveolar nerve block was administered using 2% Lignocaine with 1 : 80,000 epinephrine (Indoco Remedies Ltd., Mumbai, India) followed by isolation of the tooth using rubber dam. After removal of the temporary restoration, the remaining roof of the chamber was removed. Three canal orifices (mesiobuccal, mesiolingual and distolingual) were visible initially. Following the first law of symmetry reported by Krasner and Rankow, distobuccal canal was located in the first step (Figure 2a).4 In the second step, as the mesiobuccal and mesiolingual canals were widely separated, exploration using DG 16 explorer (Manipal Instruments, Manipal, Karnataka, India) was done at the floor wall junction as suggested by the first law of orifice location.4 Two additional canals were located between mesiobuccal and mesiolingual canals (Figure 2a). In the third step, exploration was carried out along the isthmus extending between and beyond the distolingual and distobuccal canals. Two additional canals were located, one buccal to the previously assumed distobuccal canal and the other one lingual to it (Figure 2b). Hence, a total of 8 canal orifices were located with 4 in each root. They were termed as mesiobuccal, linguo-mesiobuccal, bucco-mesiolingual and mesiolingual in mesial root, and distobuccal, linguodistobuccal, bucco-distolingual and distolingual in distal root according to proposed anatomically based nomenclature.13 Magnifying loupes (2.5X, STAC dental equipments Inc., Brampton, Canada) were used during the procedure. All the canals could be separately negotiated to a length of at least 17 mm from the orifice, beyond which merging of the canals was anticipated. Separate working length radiographs were taken for mesial (Figure 3a) and distal root (Figure 3b) as 8 files could not be accommodated together. This also helped in preventing overlapping of files' radiographic image. Radiographs clearly hinted towards existence of two separate foramina in each root. Working lengths for all mesial and distal canals were determined to be 19 and 19.5 mm respectively. Correlating the clinical and radiographic findings, the configuration of both roots was inferred as type 11 or 4-2.7 A cone beam computed tomography (CBCT) scan was required to confirm the anatomy but it was not feasible. Following working length determination, biomechanical preparation was completed using Protaper Ni-Ti rotary files (Dentsply Maillefer, Ballaigues, Switzerland). Irrigation was performed using 10 mL of 2.5% sodium hypochlorite solution and 10 mL of 17% ethylenediaminetetraacetic acid (EDTA) alternatively. Interappointment calcium hydroxide dressing was placed for two weeks. In the next appointment, following a final rinse with 4 mL of 2% chlorhexidine, all the canals were obturated with laterally compacted gutta-percha and AH plus sealer (Figures 4a and 4b). At 6 month follow-up visit, the tooth was found to be asymptomatic with normal radiographic periapical area (Figure 4c).
Discussion
In the present case, the canals could be located simply by following the guidelines of the pulp chamber floor anatomy and application of basic concepts.4 Additional canals in mandibular molars are generally hidden by a dentinal projection which is lighter in color as compared to the pulp chamber floor.3 This was clearly seen in the present case. Loupes were used during the procedure as microscope was not available. Although operative microscopes improve the probability of finding additional canals with decreased incidence of mishaps, it is proven that loupes also increase the possibility of detecting additional canals.5,14
In the mesial root of mandibular first molar, the presence of three canals is reported in many previous literatures.14,15,16 Most common configurations found in mesial root were type II and type IV.7 Four canals have also been reported in few case reports.10,17,18,19,20 In the distal root of mandibular first molar, presence of one canal has been the most common finding, but two canals have been found as high as 57.7% of molars in a study.5,21 Literature also exists confirming the presence of three and four canals in distal root.10,12,22,23,24 This is the first case reporting coexistence of 4 canals each in mesial and distal root of a mandibular first molar as no previous literature could be found following Pubmed search.
The uniqueness of the case is justified by the presence of 8 distinct orifices and type 11 or 4-2 configuration in both roots. The configuration of 4-2 has been mentioned as type VI in the Gulabivala et al.'s supplemental canal configurations and included in Vertucci modified classification as type 11.7,24 Such complicated anatomy is a consequence of secondary dentin deposition forming numerous partitions resulting in reticular form in which multiple vertical canals are present.25 An element of doubt was created by the radiographic image of files in distal root regarding existence of separate distolingual and bucco-distolingual canal. But, as all the orifices were separate and the canals could be individually instrumented to a minimum depth of 16 mm, it was legitimate to count all of them as separate canals. The above definitions have been used to identify a separate canal.26,27
Conclusions
The above case reinforces the fact that finding additional canals is not entirely dependent on the use of advanced visual and diagnostic aids. Sound knowledge coupled with commitment to unveil the internal anatomy can lead to discovery of atypical anatomy.
- 1. Vertucci FJ. Root canal anatomy of the human permanent teeth. Oral Surg Oral Med Oral Pathol 1984;58:589-599.ArticlePubMed
- 2. Vertucci FJ. Root canal morphology and its relationship to endodontic procedures. Endod Topics 2005;10:3-29.Article
- 3. Cantatore G, Berutti E, Castellucci A. Missed anatomy: frequency and clinical impact. Endod Topics 2006;15:3-31.Article
- 4. Krasner P, Rankow HJ. Anatomy of the pulp-chamber floor. J Endod 2004;30:5-16.ArticlePubMed
- 5. Carr GB, Murgel CA. The use of the operating microscope in endodontics. Dent Clin North Am 2010;54:191-214.ArticlePubMed
- 6. Cotton TP, Geisler TM, Holden DT, Schwartz SA, Schindler WG. Endodontic applications of cone-beam volumetric tomography. J Endod 2007;33:1121-1132.ArticlePubMed
- 7. de Pablo OV, Estevez R, Péix Sánchez M, Heilborn C, Cohenca N. Root anatomy and canal configuration of the permanent mandibular first molar: a systematic review. J Endod 2010;36:1919-1931.ArticlePubMed
- 8. Nur BG, Ok E, Altunsoy M, Aglarci OS, Colak M, Gungor E. Evaluation of the root and canal morphology of mandibular permanent molars in a south-eastern Turkish population using cone-beam computed tomography. Eur J Dent 2014;8:154-159.ArticlePubMedPMC
- 9. Martinez-Berna A, Badanelli P. Mandibular first molars with six root canals. J Endod 1985;11:348-352.ArticlePubMed
- 10. Reeh ES. Seven canals in a lower first molar. J Endod 1998;24:497-499.ArticlePubMed
- 11. Mortman RE, Ahn S. Mandibular first molars with three mesial canals. Gen Dent 2003;51:549-551.PubMed
- 12. Baziar H, Daneshvar F, Mohammadi A, Jafarzadeh H. Endodontic management of a mandibular first molar with four canals in a distal root by using cone-beam computed tomography: a case report. J Oral Maxillofac Res 2014 4 01 5(1):e5; doi: 10.5037/jomr.2014.5105. [Epub ahead of print].ArticlePubMedPMC
- 13. Valerian Albuquerque D, Kottoor J, Velmurugan N. A new anatomically based nomenclature for the roots and root canals-part 2: mandibular molars. Int J Dent 2012;2012:814789; doi: 10.1155/2012/814789. [Epub ahead of print].PubMedPMC
- 14. Kottoor J, Sudha R, Velmurugan N. Middle distal canal of the mandibular first molar: a case report and literature review. Int Endod J 2010;43:714-722.ArticlePubMed
- 15. Baugh D, Wallace J. Middle mesial canal of the mandibular first molar: a case report and literature review. J Endod 2004;30:185-186.ArticlePubMed
- 16. Faramarzi F, Fakhri H, Javaheri HH. Endodontic treatment of a mandibular first molar with three mesial canals and broken instrument removal. Aust Endod J 2010;36:39-41.ArticlePubMed
- 17. Goel NK, Gill KS, Taneja JR. Study of root canals configuration in mandibular first permanent molar. J Indian Soc Pedod Prev Dent 1991;8:12-14.PubMed
- 18. Jacobsen EL, Dick K, Bodell R. Mandibular first molars with multiple mesial canals. J Endod 1994;20:610-613.ArticlePubMed
- 19. Kontakiotis EG, Tzanetakis GN. Four canals in the mesial root of a mandibular first molar. A case report under the operating microscope. Aust Endod J 2007;33:84-88.ArticlePubMed
- 20. Aminsobhani M, Shokouhinejad N, Ghabraei S, Bolhari B, Ghorbanzadeh A. Retreatment of a 6-canalled mandibular frirst molar with four mesial canals: a case report. Iran Endod J 2010;5:138-140.PubMedPMC
- 21. al-Nazhan S. Incidence of four canals in root-canal-treated mandibular first molars in a Saudi Arabian subpopulation. Int Endod J 1999;32:49-52.ArticlePubMed
- 22. Beatty RG, Interian CM. A mandibular first molar with five canals: report of case. J Am Dent Assoc 1985;111:769-771.ArticlePubMed
- 23. Friedman S, Moshonov J, Stabholz A. Five root canals in a mandibular first molar. Endod Dent Traumatol 1986;2:226-228.ArticlePubMed
- 24. Gulabivala K, Aung TH, Alavi A, Ng YL. Root and canal morphology of Burmese mandibular molars. Int Endod J 2001;34:359-370.ArticlePubMedPDF
- 25. Peiris HR, Pitakotuwage TN, Takahashi M, Sasaki K, Kanazawa E. Root canal morphology of mandibular permanent molars at different ages. Int Endod J 2008;41:828-835.ArticlePubMed
- 26. Nosonowitz DM, Brenner MR. The major canals of the mesiobuccal root of the maxillary 1st and 2nd molars. N Y J Dent 1973;43:12-15.PubMed
- 27. Seidberg BH, Altman M, Guttuso J, Suson M. Frequency of two mesiobuccal root canals in maxillary permanent first molars. J Am Dent Assoc 1973;87:852-856.ArticlePubMed
REFERENCES
Figure 1
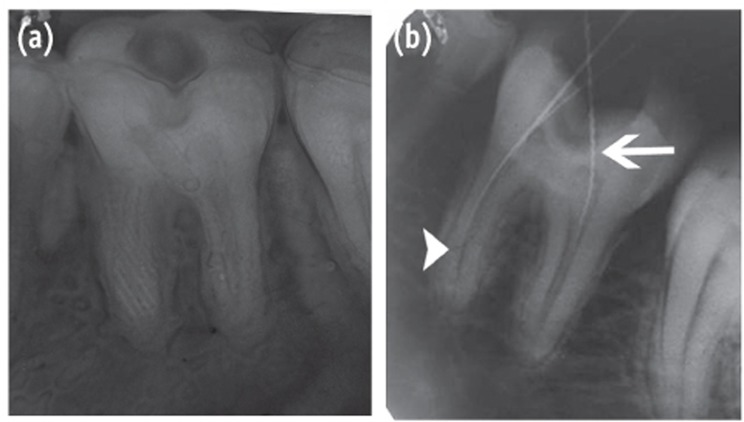
Radiographs with which patient reported. (a) Pre-operative radiograph with artifact; (b) Working length radiograph. Files short of apex (short arrow) and intact pulp chamber roof (long arrow).
Figure 2
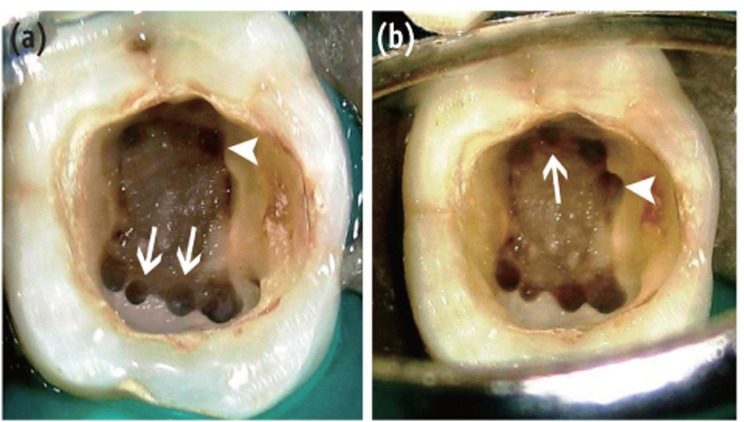
Location of additional canals. (a) Distobuccal canal (short arrow) and additional mesial canals (long arrows); (b) Additional distal canals. Buccal (short arrow) and lingual (long arrow) to previously assumed distobuccal canal.
Tables & Figures
REFERENCES
Citations
Citations to this article as recorded by 
- Birooted Mandibular Canine: A Systematic Review and Meta-Analysis
Amelia Hoppe, Kamila Chęcińska, Maciej Chęciński, Natalia Turosz, Maciej Sikora
Journal of Clinical Medicine.2026; 15(9): 3381. CrossRef - How Do Different Image Modules Impact the Accuracy of Working Length Measurements in Digital Periapical Radiography? An In Vitro Study
Vahide Hazal Abat, Rabia Figen Kaptan
Diagnostics.2025; 15(3): 305. CrossRef - Determinants of the Number of Main Canals in a Tooth: Deciphering Potential Mechanisms
Andrea Alejandra Moreno Robalino, José Luis Álvarez Vásquez
Universitas Odontologica.2023;[Epub] CrossRef - Application Of Cone-Beam Computed Tomography In Diagnosis And Treatment Of Multiple Canals– A Case Report
Gyanendra Pratap Singh, Shruthi H Attavar, Sivaji Kavuri
Annals of Dental Specialty.2022; 10(2): 15. CrossRef - Four distal root canals in a two-rooted permanent mandibular first molar
Urvashi M. Ujariya, Foram H. Patel, Rajendra P. Bharatiya, Anjali K. Kothari
Endodontology.2022; 34(3): 212. CrossRef - Utilizing Cone-Beam Computed Tomography for Identifying and Managing Multiple Canals: A Case Report
Gyanendra Pratap Singh, Shruthi H Attavar, Sivaji Kavuri
Journal of Current Research in Oral Surgery.2022; 2(1): 37. CrossRef - Morphology and prevalence of middle canals in the mandibular molars: A systematic review
Rashmi Bansal, Sapna Hegde, Madhusudan Astekar
Journal of Oral and Maxillofacial Pathology.2018; 22(2): 216. CrossRef - Endodontic management of a permanent mandibular first molar with unusual root canal configurations: Two case reports
Mohammad Ahmad Alenezi, Mustafa Aldajani, Hind O. Al-Qathami, Seraj Al-Shommrani
Saudi Endodontic Journal.2017; 7(3): 181. CrossRef
 ePub Link
ePub Link Cite
CiteEndodontic treatment of a mandibular first molar with 8 canals: a case report
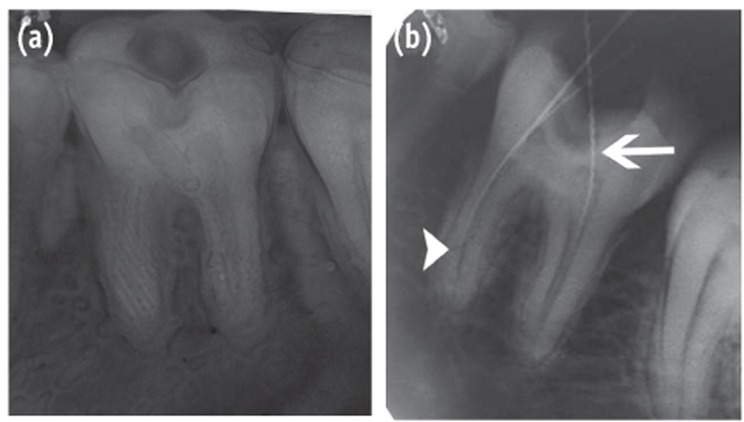
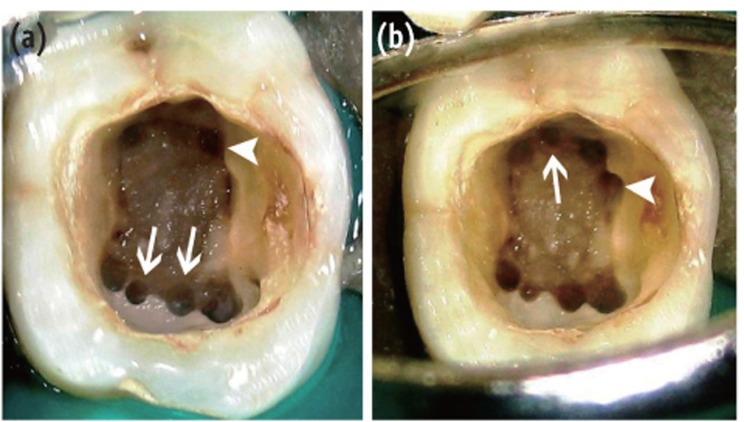
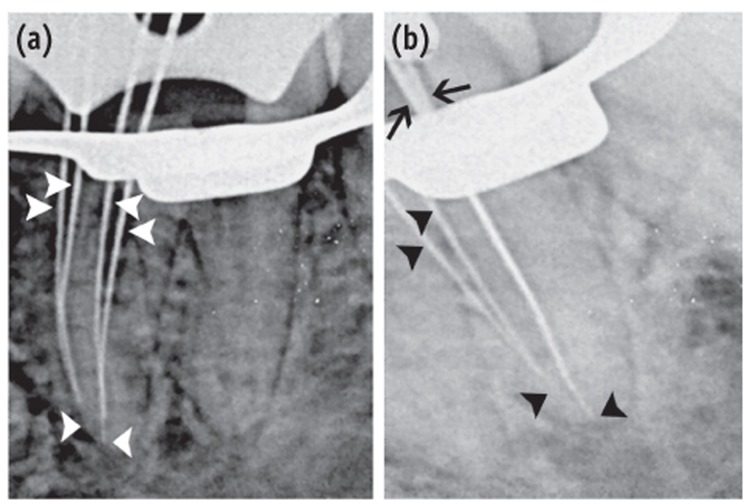
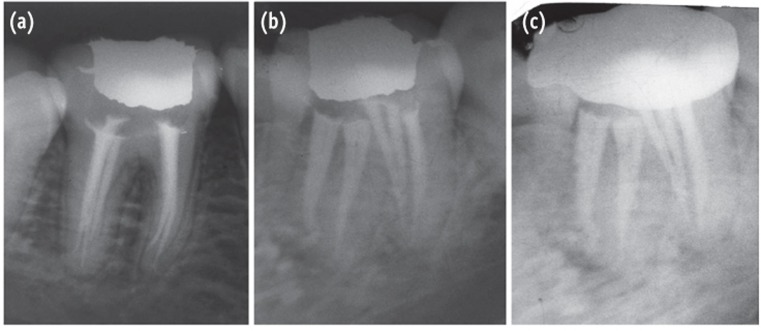
Figure 1 Radiographs with which patient reported. (a) Pre-operative radiograph with artifact; (b) Working length radiograph. Files short of apex (short arrow) and intact pulp chamber roof (long arrow).
Figure 2 Location of additional canals. (a) Distobuccal canal (short arrow) and additional mesial canals (long arrows); (b) Additional distal canals. Buccal (short arrow) and lingual (long arrow) to previously assumed distobuccal canal.
Figure 3 Working length radiographs. (a) Mesial root. 4-2 configuration is clearly illustrated (short white arrows); (b) Distal root. Superimposed files seen in distolingual and bucco-distolingual canal (long black arrows).
Figure 4 Post obturation radiographs. (a) Straight on angulation; (b) Distal angulation; (c) 6 month follow up.
Figure 1
Figure 2
Figure 3
Figure 4
Endodontic treatment of a mandibular first molar with 8 canals: a case report

