
Articles
- Page Path
- HOME > Restor Dent Endod > Volume 41(1); 2016 > Article
- Case Report Endodontic treatment of a C-shaped mandibular second premolar with four root canals and three apical foramina: a case report
- Thikamphaa Bertrand, Sahng Gyoon Kim
-
2016;41(1):-73.
DOI: https://doi.org/10.5395/rde.2016.41.1.68
Published online: January 19, 2016
Division of Endodontics, Columbia University College of Dental Medicine, New York, NY, USA.
- Correspondence to Sahng Gyoon Kim, DDS, MS. Assistant Professor, Division of Endodontics, Columbia University College of Dental Medicine, 630 W. 168 St. - PH7Stem #128, New York, NY, USA 10032. TEL, +1-212-305-4594; FAX, +1-212-305-9313; sgk2114@columbia.edu
• Received: September 8, 2015 • Accepted: December 4, 2015
©Copyrights 2016. The Korean Academy of Conservative Dentistry.
This is an Open Access article distributed under the terms of the Creative Commons Attribution Non-Commercial License (http://creativecommons.org/licenses/by-nc/3.0/) which permits unrestricted non-commercial use, distribution, and reproduction in any medium, provided the original work is properly cited.
- 3,834 Views
- 21 Download
- 5 Crossref
Abstract
- This case report describes a unique C-shaped mandibular second premolar with four canals and three apical foramina and its endodontic management with the aid of cone-beam computer tomography (CBCT). C-shaped root canal morphology with four canals was identified under a dental operating microscope. A CBCT scan was taken to evaluate the aberrant root canal anatomy and devise a better instrumentation strategy based on the anatomy. All canals were instrumented to have a 0.05 taper using 1.0 mm step-back filing with appropriate apical sizes determined from the CBCT scan images and filled using a warm vertical compaction technique. A C-shaped mandibular second premolar with multiple canals is an anatomically rare case for clinicians, yet its endodontic treatment may require a careful instrumentation strategy due to the difficulty in disinfecting the canals in the thin root area without compromising the root structure.
Introduction
Mandibular second premolars have wide variations in root canal anatomy. Although the incidence of the variations is not as common as that of mandibular first premolars, the root canal aberrations in mandibular second premolars are as diverse as those in mandibular first premolars. Their anatomical variations include multiple root canals1,2,3,4,5,6,7,8,9 and C-shaped root canal configurations.10,11
The C-shaped root canal morphology is rare in mandibular second premolars, although it is not uncommon in other tooth types.10,11 A study by Yu et al. showed that the prevalence of C-shaped root canals was 0.6% in the investigation of 178 mandibular second premolars from a Chinese population using CBCT.10 A study by Rahimi et al. showed that 2% of 103 extracted mandibular second premolars from an Iranian population had C-shaped canals.11 Until now, two prevalence studies and two case reports presenting C-shaped root canals have been published (Table 1). The reported prevalence of C-shaped canals in all tooth types ranges from 2.7% to 8%, and the C-shaped configurations are most commonly found in mandibular second molars, followed by mandibular first premolars, mandibular third molars, mandibular second premolars, and maxillary first molars.10,11,12,13,14,15
The etiology of C-shaped root configuration is thought to be a failure of Hertwig's epithelial root sheath to fuse during the stage of tooth development or coalescence by the continuous cementum deposition.16,17 Therefore, the development of additional roots is considered a prerequisite for C-shaped root formation in mandibular second premolars. It was reported that patients with X-linked human inherited diseases showed increased additional root formation in mandibular premolars, suggesting that the genetic change on X chromosome may be a factor contributing to the C-shaped root formation.18,19,20
Due to the presence of concavities and small root thicknesses in C-shaped mandibular premolars, cleaning and shaping of C-shaped canals pose challenges for clinicians.16,22 Inadvertent mechanical instrumentation may remove excessive dentin and cause a strip perforation. Therefore, the evaluation of the root canal morphology along with the root thickness using cone-beam computed tomography (CBCT) may be useful for the chemomechanical root canal preparation in C-shaped mandibular second premolars.
The aim of this case report is to present an endodontic therapy of a C-shaped mandibular second premolar with four canals and three apical foramina. This case report describes a unique C-shaped mandibular second premolar with four canals and its endodontic treatment with the aid of CBCT. We also report a finding of bilateral C-shaped first and second premolars in the patient.
Case Report
A 14 year old African American female was referred to the postgraduate endodontic clinic by her general dentist for the consultation and treatment of the left mandibular second premolar (tooth #35). The patient's medical history was noncontributory. Her chief complaint was pain around her lower left tooth whenever she drank something cold. Clinical examination showed occlusal caries on tooth #35 and a tooth colored restoration on tooth #36. Teeth #37, 36, and 34 had normal responses to cold testing using Endo-Ice (Coltene/Whaledent Inc., Cuyahoga Falls, OH, USA) and no pain to percussion and palpation. Tooth #35 had sharp, lingering pain to cold testing with Endo-Ice, no pain to percussion and palpation. No gingivitis or periodontitis was observed. Clinical and radiographic examination revealed occlusal caries approaching the pulp horn in tooth #35 and no periapical radiolucency around the root apex of tooth #35 (Figure 1a). Tooth #35 was diagnosed with symptomatic irreversible pulpitis and normal apical tissues on the basis of clinical and radiographic examinations. Non-surgical root canal treatment was given as a treatment plan for tooth #35.
An informed consent was obtained from the patient and patient's mother, and endodontic treatment on tooth #35 was initiated. At the first visit, local anesthesia was obtained using 3.4 mL of 2% lidocaine (1:100,000 epinephrine) for inferior alveolar nerve block and 1.7 mL of 4% articaine (1:100,000 epinephrine) for buccal infiltration. After rubber dam isolation, caries were removed, and an access cavity was made. A long pulp chamber with a C-shaped canal configuration was identified under a dental operating microscope (Carl Zeiss Meditec Inc., Dublin, CA, USA, Figure 2b). A pulpotomy was performed with a sterile #4 carbide round bur followed by copious irrigation using 5.25% NaOCl. Four canals (mesial, M; mesiobuccal, MB; distobuccal, DB; distal, D canals) were identified within the C-shaped root canal configuration. The tooth was medicated with Ca(OH)2 (Dental Therapeutics AB, Nacka, Sweden). A cotton pellet was placed in the pulp chamber, and the tooth was temporized with Cavit (3M ESPE, St. Paul, MN, USA). In order to evaluate the aberrant anatomy and perform careful mechanical instrumentation based on the anatomy, a CBCT scan was suggested. Upon the patient's agreement, a referral was made to the maxillofacial oral radiology department for a CBCT scan.
A CBCT scan (i-CAT, Imaging Sciences International, Hatfield, PA, USA) was taken and analyzed with i-CAT Vision 3D imaging software (Imaging Sciences International). The scan confirmed a C-shaped canal morphology with four canals (Figure 2a) and a fused root configuration (Figure 2d). The axial views of the CBCT scan showed that the mesial and mesiobuccal canals joined into one canal in the coronal third of the root. The root thicknesses around all canals were measured at all levels, from the apical foramina to the canal orifices, in 0.3 mm interval from the outer surface of the root (Figure 2e). The axial views of the scan also revealed that the root thicknesses gradually increased in the coronal direction in all four root canals. The root thickness around the M canal ranged from 1.08 mm (apical foramen) to 2.34 mm (canal orifice). The root thickness around the MB canal ranged from 1.08 mm (apical foramen) to 2.32 mm (canal orifice). The root thickness around the DB canal ranged from 0.86 mm (apical foramen) to 2.16 mm (canal orifice). The root thickness around the D canal ranged from 1.32 mm (apical foramen) to 3.30 mm (canal orifice). Considering that the residual dentin thickness around the root canals should exceed the one third of the root thickness, the apical instrumentation sizes in M, MB, DB, and D canals were determined not to be greater than sizes 30, 30, 25, and 40, respectively, and the instrument tapers of the root canals were determined not to be greater than 0.06.23,24,25,26 The presence of C-shaped canal morphology in teeth #34, 44, and 45 was incidentally identified in the scan images (Figure 2c).
At the second visit, the patient was asymptomatic. 3.2 mL of 2% lidocaine (1:100,000 epinephrine) was administered as a buccal infiltration followed by rubber dam isolation. Cavit and a cotton pellet were removed. The working length of all four canals were determined by an electronic apex locator (Root ZX II mini, J Morita USA, Irvine, CA, USA). Instrumentation was performed with K-Flexo hand files (Dentsply Maillefer, Tulsa, OK, USA) with a step-back technique after orifices were carefully enlarged with Protaper S1 and SX (Dentsply Tulsa Dental, Tulsa, OK, USA), and isthmus areas were cleaned and shaped using excessive irrigation with 5.25% NaOCl and hand files (size 6K, 8K, and 10K files). All canals were instrumented to have a 0.05 taper using 1.0 mm step-back filing. M, MB, and D canals were instrumented to the working length with a size 30K-Flexo hand file, and DB canals with a size 25 K-Flexo hand file. 5.25% NaOCl was used as an irrigant throughout the procedure, and final irrigation was performed for 1 minute with 17% ethylenediaminetetraacetic acid (EDTA) to remove the smear layer. Canals were dried using paper points, filled with gutta percha and AH26 sealer (Dentsply Maillefer) using a warm vertical compaction technique (Figures 1b and 1c). A cotton pellet was placed in the pulp chamber, and the tooth was temporized with TERM (Dentsply Maillefer) (Figure 1d). Postoperative instructions were provided, and the patient was referred to her general dentist for a permanent restoration.
Discussion
Endodontic treatment of mandibular premolars may require a high level of clinical skills due to their wide anatomical variations.3,4,5,6,7,8,9,10,11,15 The most common root canal morphology in mandibular second premolars is one canal whose prevalence is reported to be as high as 98.8%.1 This tooth type also often has two canals, of which the occurrence ranges from 1.2% to 29%.1,2 The prevalence of three canals varies from 0.4% to 0.5%, and the presence of four and five canals has been reported only in case reports.3,4,5,6,7,8,9 The endodontic treatment of C-shaped mandibular second premolars with multiple canals is a challenge to clinicians although they are rarely encountered. There was only one case report describing the C-shaped canal morphology with two root canals in a mandibular second premolar and its endodontic management.22 We described the endodontic treatment of a C-shaped mandibular second premolar with four canals with the aid of CBCT in this case report.
The endodontic treatment of the C-shaped mandibular second premolar required a careful instrumentation strategy due to the difficulty in disinfecting the canals in the thin root area around a concavity, without compromising the root structure. Therefore, we used three-dimensional imaging to analyze the aberrant anatomy prior to chemomechanical preparations. In the analysis, the root thicknesses around all four canals were measured at all levels of the root using the axial and sagittal views of the CBCT scan. Based on the root widths, the instrumentation size and taper for each canal was determined in order to provide sufficient mechanical instrumentation and prevent excessive dentin removal.
The residual radicular dentin thickness after mechanical preparation is critical for fracture resistance. The guideline with respect to the minimum residual dentin thickness has been initially proposed for post space preparation, and is also being used for root canal preparation.27 It is suggested that the residual dentin thickness should be at least one third of the root or 0.3 mm because the mechanical instrumentation beyond this threshold may increase the risk of vertical root fracture or strip perforation.23,24,25,26 It is reasonable to assume that a tooth with multiple canals around a concavity (danger zone) such as a C-shaped premolar has a greater chance of having these complications during and after mechanical instrumentation. Jafarzadeh and Wu recommended that the isthmuses should not be instrumented with files larger than size 25 in order to prevent strip perforations.12 Jerome suggested that anticurvature filing in the coronal third to avoid strip perforations.28 In our case, all canals were instrumented using the anticurvature filing technique away from the concavity. Copious irrigation with 5.25% NaOCl and hand files (size 6K, 8K, and 10K files) were used to clean and shape the isthmus in the C-shaped canal as suggested by Jafarzadeh and Wu.12 The use of ultrasonics or sonics could be efficacious in cleaning the isthmus area, although it was not used in our case. Extreme care should be taken to avoid perforation in the C-shaped roots with the narrow isthmus when ultrasonics is used.12
In the present report, a dental operating microscope and CBCT were used to verify the presence of a C-shaped canal in the mandibular second premolar. It is considered difficult or impossible to diagnose C-shaped canals with periapical radiographs alone, although the presence of conical shaped or fused roots may be an indicator of the presence of a C-shaped canal.29,30 In our case, the C-shaped canals were diagnosed through visual inspection under the microscope. Due to the wide variations in anatomy below the C-shaped canal orifices in mandibular second premolars, a CBCT scan was also taken and analyzed.10 However, CBCT scans should not be prescribed for the routine endodontic treatment of mandibular premolars and should be suggested only when aberrant anatomy is suspected based on clinical examination and two-dimensional radiographic imaging of the teeth requiring endodontic treatment.
An incidental finding on the CBCT scan was C-shaped root canal morphology in all mandibular premolars in the present case. Until now, there has been one case report describing bilateral C-shaped mandibular first and second premolars in a patient.21 The prevalence of C-shaped root canal morphology in mandibular first premolars is reported to range from 1.1% to 18%.3,10,13 C-shaped root canal morphology in mandibular second premolars is reported to be rare (Table 1). The prevalence of C-shaped root canal anatomy in mandibular first premolars varies greatly among ethnic groups, while the prevalence of C-shaped mandibular second premolars seem to have a smaller variations among the different populations, perhaps due to the very low prevalence.3,10,13
Conclusions
A C-shaped mandibular second premolar with multiple canals poses significant clinical difficulty in nonsurgical root canal treatment, although it is rarely reported. The endodontic treatment of this C-shaped premolar may require a careful instrumentation strategy due to the difficulty in disinfecting the canals in the thin root area without compromising the root structure. Use of CBCT might be beneficial in the assessment of root canal shape and endodontic treatment of the mandibular second premolar with this aberrant root canal morphology.
- 1. Pineda F, Kuttler Y. Mesiodistal and buccolingual roentgenographic investigation of 7,275 root canals. Oral Surg Oral Med Oral Pathol 1972;33:101-110.ArticlePubMed
- 2. Sert S, Bayirli GS. Evaluation of the root canal configurations of the mandibular and maxillary permanent teeth by gender in the Turkish population. J Endod 2004;30:391-398.ArticlePubMed
- 3. Awawdeh LA, Al-Qudah AA. Root form and canal morphology of mandibular premolars in a Jordanian population. Int Endod J 2008;41:240-248.ArticlePubMed
- 4. Zillich R, Dowson J. Root canal morphology of mandibular first and second premolars. Oral Surg Oral Med Oral Pathol 1973;36:738-744.ArticlePubMed
- 5. Holtzman L. Root canal treatment of mandibular second premolar with four root canals: a case report. Int Endod J 1998;31:364-366.ArticlePubMed
- 6. Bram SM, Fleisher R. Endodontic therapy in a mandibular second bicuspid with four canals. J Endod 1991;17:513-515.PubMed
- 7. Rhodes JS. A case of unusual anatomy: a mandibular second premolar with four canals. Int Endod J 2001;34:645-648.ArticlePubMedPDF
- 8. Macri E, Zmener O. Five canals in a mandibular second premolar. J Endod 2000;26:304-305.ArticlePubMed
- 9. Sachdeva GS, Ballal S, Gopikrishna V, Kandaswamy D. Endodontic management of a mandibular second premolar with four roots and four root canals with the aid of spiral computed tomography: a case report. J Endod 2008;34:104-107.ArticlePubMed
- 10. Yu X, Guo B, Li KZ, Zhang R, Tian YY, Wang H, Hu T. Cone-beam computed tomography study of root and canal morphology of mandibular premolars in a western Chinese population. BMC Med Imaging 2012;12:18.ArticlePubMedPMCPDF
- 11. Rahimi S, Shahi S, Yavari HR, Manafi H, Eskandarzadeh N. Root canal configuration of mandibular first and second premolars in an Iranian population. J Dent Res Dent Clin Dent Prospects 2007;1:59-64.PubMedPMC
- 12. Jafarzadeh H, Wu YN. The C-shaped root canal configuration: a review. J Endod 2007;33:517-523.ArticlePubMed
- 13. Lu TY, Yang SF, Pai SF. Complicated root canal morphology of mandibular first premolar in a Chinese population using the cross section method. J Endod 2006;32:932-936.ArticlePubMed
- 14. Sidow SJ, West LA, Liewehr FR, Loushine RJ. Root canal morphology of human maxillary and mandibular third molars. J Endod 2000;26:675-678.ArticlePubMed
- 15. Cleghorn BM, Christie WH, Dong CC. Root and root canal morphology of the human permanent maxillary first molar: a literature review. J Endod 2006;32:813-821.ArticlePubMed
- 16. Manning SA. Root canal anatomy of mandibular second molars. Part II. C-shaped canals. Int Endod J 1990;23:40-45.PubMed
- 17. Barnett F. Mandibular molar with C-shaped canal. Endod Dent Traumatol 1986;2:79-81.ArticlePubMed
- 18. Varrela J. Effect of 45,X/46,XX mosaicism on root morphology of mandibular premolars. J Dent Res 1992;71:1604-1606.ArticlePubMedPDF
- 19. Varrela J. Root morphology of mandibular premolars in human 45,X females. Arch Oral Biol 1990;35:109-112.ArticlePubMed
- 20. Kusiak A, Sadlak-Nowicka J, Limon J, Kochńska B. Root morphology of mandibular premolars in 40 patients with Turner syndrome. Int Endod J 2005;38:822-826.ArticlePubMed
- 21. Chauhan R, Singh S, Chandra A. A rare occurrence of bilateral C-shaped roots in mandibular first and second premolars diagnosed with the aid of spiral computed tomography. J Clin Exp Dent 2014;6:e440-e443.ArticlePubMedPMC
- 22. Shah DY. C-shaped root canal configuration in mandibular second premolar: report of an unusual case and its endodontic management. J Int Clin Dent Res Organ 2012;4:18-20.Article
- 23. Hunter AJ, Feiglin B, Williams JF. Effects of post placement on endodontically treated teeth. J Prosthet Dent 1989;62:166-172.ArticlePubMed
- 24. Tilk MA, Lommel TJ, Gerstein H. A study of mandibular and maxillary root widths to determine dowel size. J Endod 1979;5:79-82.ArticlePubMed
- 25. Johnson JK, Schwartz NL, Blackwell RT. Evaluation and restoration of endodontically treated posterior teeth. J Am Dent Assoc 1976;93:597-605.ArticlePubMed
- 26. Lim SS, Stock CJ. The risk of perforation in the curved canal: anticurvature filing compared with the stepback technique. Int Endod J 1987;20:33-39.ArticlePubMed
- 27. Zuckerman O, Katz A, Pilo R, Tamse A, Fuss Z. Residual dentin thickness in mesial roots of mandibular molars prepared with Lightspeed rotary instruments and Gates-Glidden reamers. Oral Surg Oral Med Oral Pathol Oral Radiol Endod 2003;96:351-355.ArticlePubMed
- 28. Jerome CE. C-shaped root canal systems: diagnosis, treatment, and restoration. Gen Dent 1994;42:424-427.PubMed
- 29. Cooke HG 3rd, Cox FL. C-shaped canal configurations in mandibular molars. J Am Dent Assoc 1979;99:836-839.ArticlePubMed
- 30. Haddad GY, Nehme WB, Ounsi HF. Diagnosis, classification, and frequency of C-shaped canals in mandibular second molars in the Lebanese population. J Endod 1999;25:268-271.ArticlePubMed
REFERENCES
Figure 1
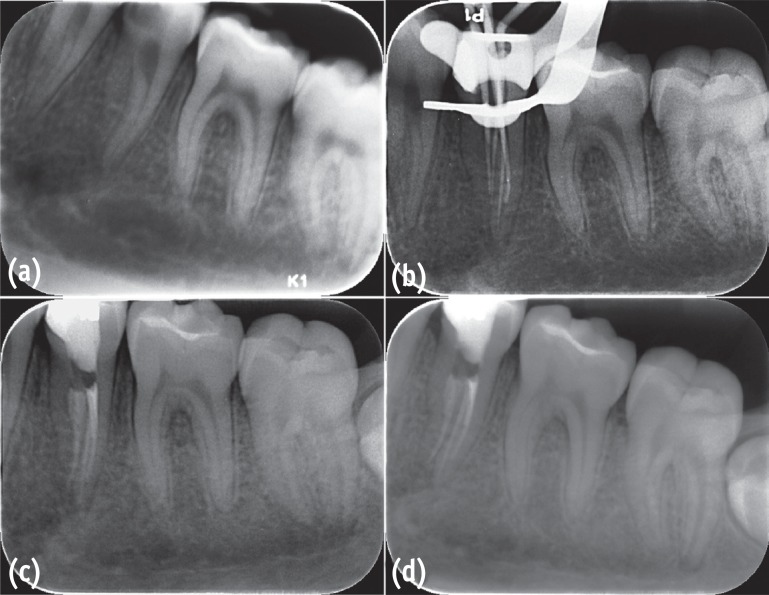
Root canal treatment of the C-shaped left mandibular second premolar with four canals and three apical foramina. (a) A preoperative periapical radiograph; (b) Master cone fit; (c, d) Postoperative periapical radiographs showing mesial and mesiobuccal canals joining in the coronal third of the root.
Figure 2
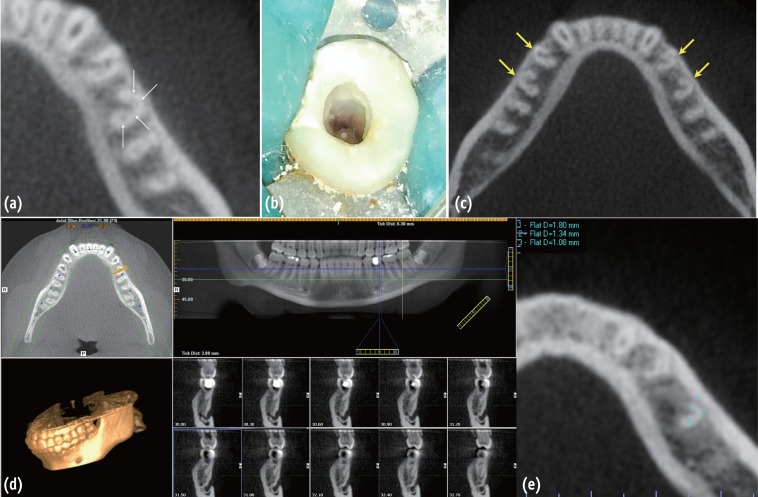
A CBCT scan and access cavity of the C-shaped left mandibular second premolar. (a) Axial view showing four canals in the C-shaped left mandibular second premolar; (b) Occlusal view of access cavity showing a C-shaped root canal configuration; (c) Axial view showing bilateral C-shaped mandibular first and second premolars; (d) Axial, panoramic, and sagittal views showing a fused root configuration of the left mandibular second premolar; (e) Axial view showing a measurement of root thicknesses around canals. The root thicknesses were measured individually at all levels with 0.3 mm interval from each canal to the outer surface of the root, and from the apical foramina to the canal orifices.
Table 1
Previous studies of mandibular second premolars with C-shaped root canals
| Reference | Type of study | No. of teeth | Ethnicity | Prevalence |
|---|---|---|---|---|
| Yu et al.10 | Radiographic study (CBCT) | 178 | Chinese | 0.6% |
| Rahimi et al.11 | Clearing | 103 | Iranian | 2% |
| Chauhan et al.21 | Case report (Spiral CT) | 2 | Indian | N/A |
| Shah22 | Case report (Clinical RCT) | 1 | Indian | N/A |
Tables & Figures
REFERENCES
Citations
Citations to this article as recorded by 
- Unique root anatomy of mandibular second premolars: clinical strategies for effective disinfection and preservation of dentine structure in root canal treatment—a case report
Ji Wook Jeong, Erika Silguero Gonzalez, Scott R. Makins, Timothy Kirkpatrick
Frontiers in Dental Medicine.2024;[Epub] CrossRef - PRICE 2020 guidelines for reporting case reports in Endodontics: explanation and elaboration
V. Nagendrababu, B. S. Chong, P. McCabe, P. K. Shah, E. Priya, J. Jayaraman, S. J. Pulikkotil, P. M. H. Dummer
International Endodontic Journal.2020; 53(7): 922. CrossRef - A cone-beam computed tomography study of C-shaped root canal systems in mandibular second premolars in a Taiwan Chinese subpopulation
Yi-Chin Chen, Chia-Lun Tsai, Yi-Chen Chen, Gin Chen, Shue-Fen Yang
Journal of the Formosan Medical Association.2018; 117(12): 1086. CrossRef - Anatomic Comparison of Contralateral Premolars
Gaute Floer Johnsen, Sazan Dara, Sameenah Asjad, Pia Titterud Sunde, Håvard Jostein Haugen
Journal of Endodontics.2017; 43(6): 956. CrossRef - Endodontic Management of Dilacerated Maxillary Central Incisor fused to a Supernumerary Tooth using Cone Beam Computed Tomography: An Unusual Clinical Presentation
Thilla S Vinothkumar, Deivanayagam Kandaswamy, Ganesh Arathi, Sathishkumar Ramkumar, Gnanasekaran Felsypremila
The Journal of Contemporary Dental Practice.2017; 18(6): 522. CrossRef
 ePub Link
ePub Link Cite
CiteEndodontic treatment of a C-shaped mandibular second premolar with four root canals and three apical foramina: a case report
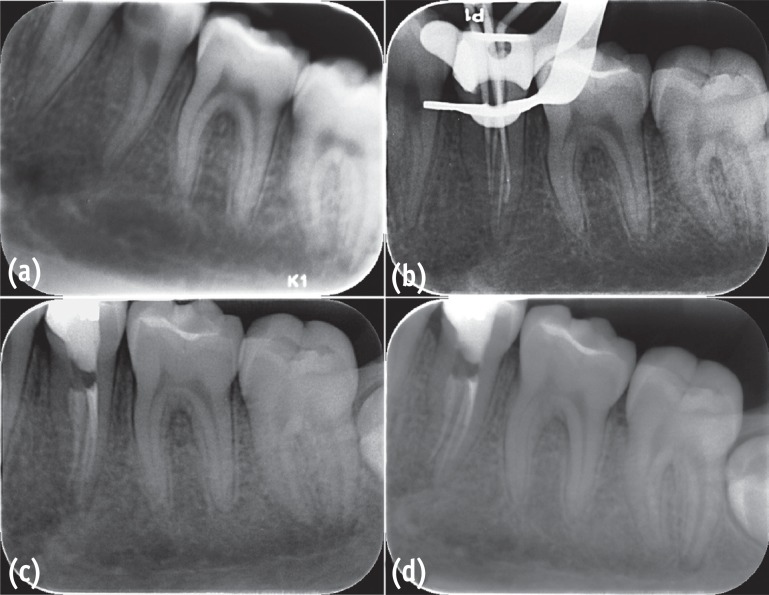
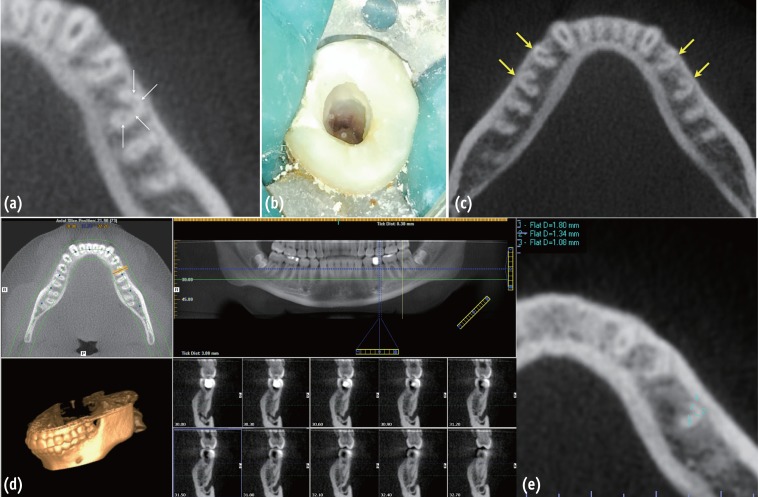
Figure 1 Root canal treatment of the C-shaped left mandibular second premolar with four canals and three apical foramina. (a) A preoperative periapical radiograph; (b) Master cone fit; (c, d) Postoperative periapical radiographs showing mesial and mesiobuccal canals joining in the coronal third of the root.
Figure 2 A CBCT scan and access cavity of the C-shaped left mandibular second premolar. (a) Axial view showing four canals in the C-shaped left mandibular second premolar; (b) Occlusal view of access cavity showing a C-shaped root canal configuration; (c) Axial view showing bilateral C-shaped mandibular first and second premolars; (d) Axial, panoramic, and sagittal views showing a fused root configuration of the left mandibular second premolar; (e) Axial view showing a measurement of root thicknesses around canals. The root thicknesses were measured individually at all levels with 0.3 mm interval from each canal to the outer surface of the root, and from the apical foramina to the canal orifices.
Figure 1
Figure 2
Endodontic treatment of a C-shaped mandibular second premolar with four root canals and three apical foramina: a case report
Previous studies of mandibular second premolars with C-shaped root canals
| Reference | Type of study | No. of teeth | Ethnicity | Prevalence |
|---|---|---|---|---|
| Yu et al. | Radiographic study (CBCT) | 178 | Chinese | 0.6% |
| Rahimi et al. | Clearing | 103 | Iranian | 2% |
| Chauhan et al. | Case report (Spiral CT) | 2 | Indian | N/A |
| Shah | Case report (Clinical RCT) | 1 | Indian | N/A |
CBCT, cone-beam computed tomography; CT, computed tomography; RCT, root canal treatment.
Table 1 Previous studies of mandibular second premolars with C-shaped root canals
CBCT, cone-beam computed tomography; CT, computed tomography; RCT, root canal treatment.

