
Search
- Page Path
- HOME > Search
Case Report
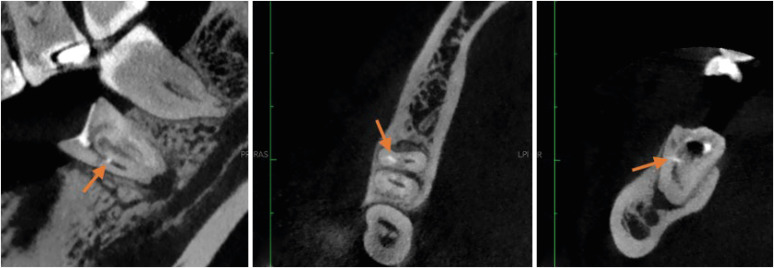
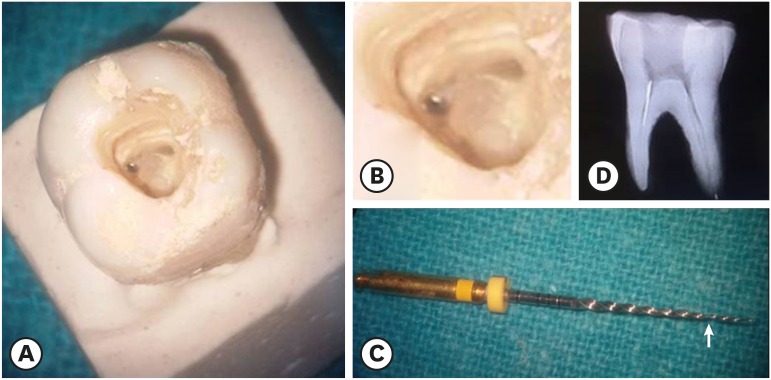
- Multidisciplinary management of an endo-perio lesion complicated by a cemental tear: a case report
- Nishanth D. Sadhak, Akshaya Pallod, Shreyas Oza
- Restor Dent Endod 2025;50(3):e31. Published online August 22, 2025
- DOI: https://doi.org/10.5395/rde.2025.50.e31
-
 Abstract
Abstract
 PDF
PDF PubReader
PubReader ePub
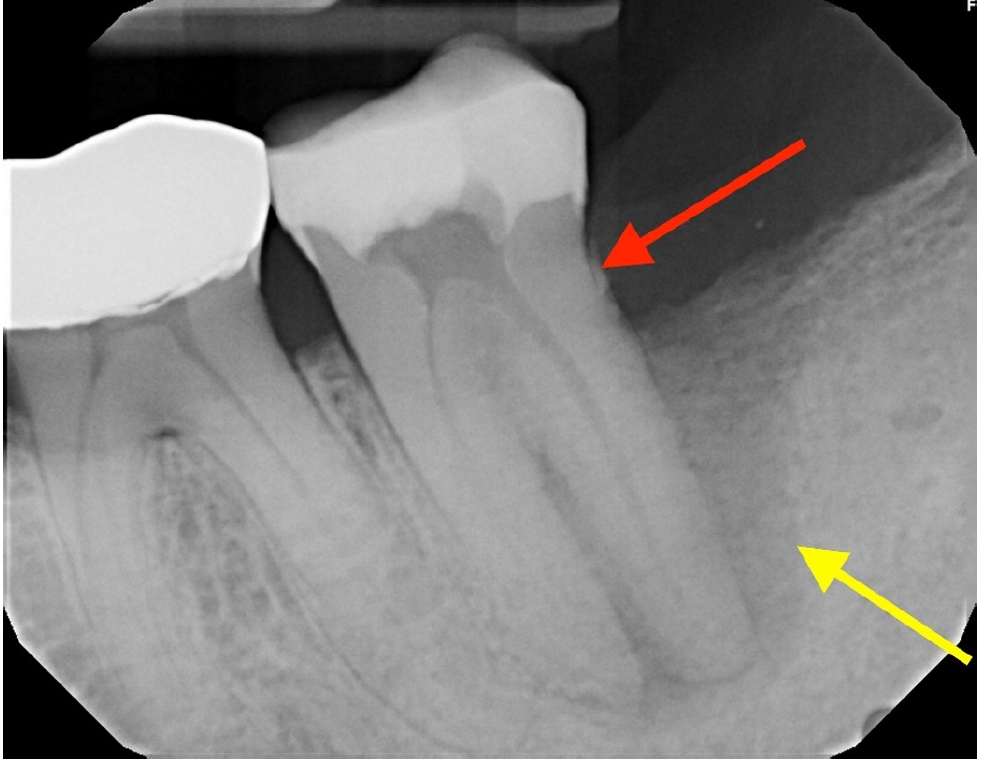
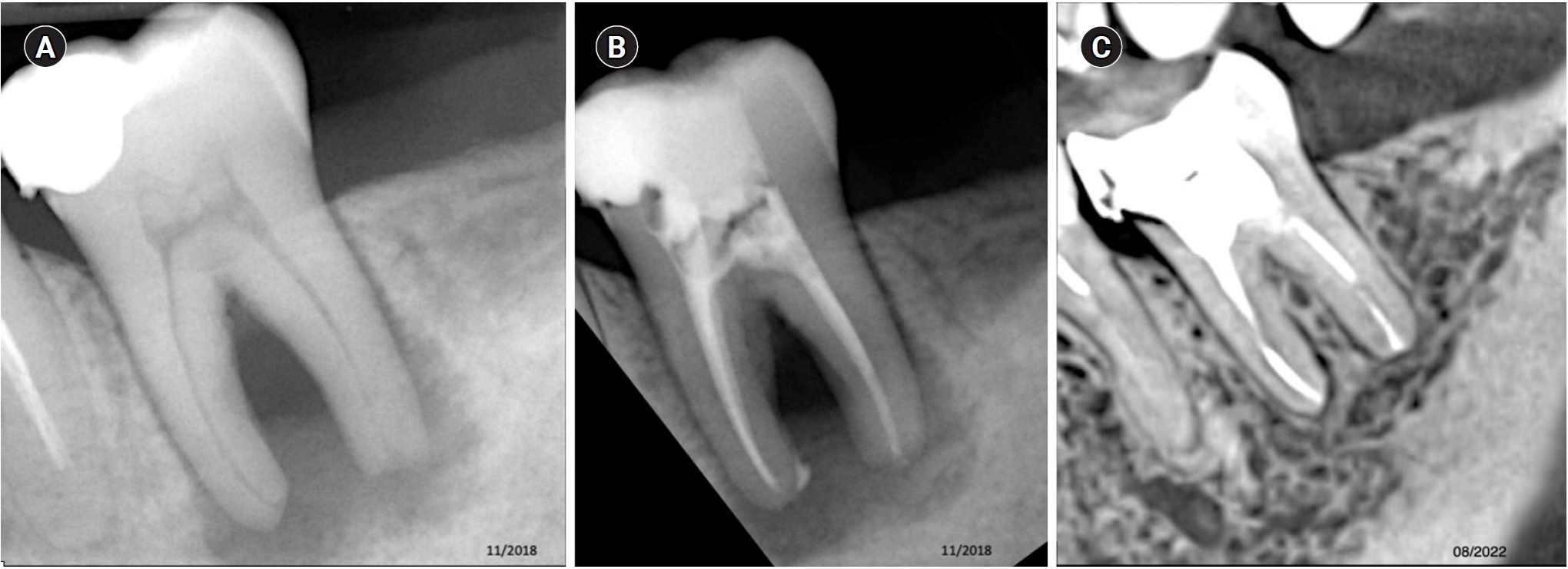
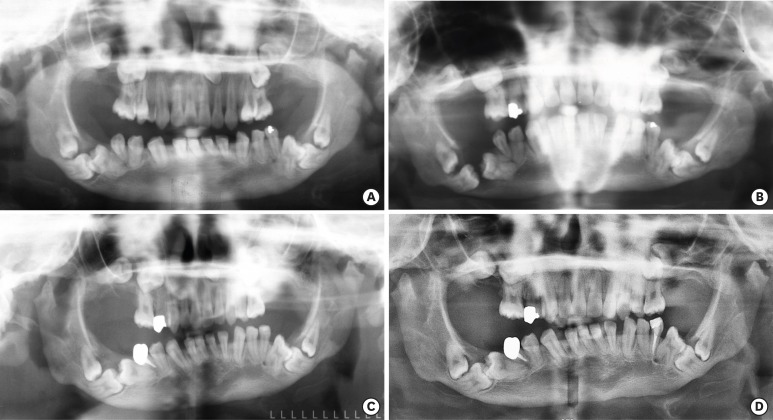
ePub - Endodontic-periodontal lesions (EPLs) complicated by cemental tears present a diagnostic and therapeutic challenge. This case report describes the successful management of a 66-year-old male patient with a mandibular second molar (#18) exhibiting an EPL complicated by a cemental tear. Clinical examination revealed a draining sinus tract, deep periodontal pockets, and radiographic evidence of a “J-shaped” lesion and a radiopaque cemental fragment. The tooth had previously initiated endodontic treatment. A multidisciplinary approach involving endodontic treatment and surgical removal of the cemental tear was implemented. At 24-month follow-up, clinical and radiographic examination revealed significant improvement in periodontal health, bone regeneration, and resolution of the lesion. This case highlights the importance of considering cemental tears in the differential diagnosis of EPLs and demonstrates the efficacy of a combined endodontic-periodontal approach for achieving predictable outcomes.
- 4,873 View
- 359 Download

Research Articles
- Impact of the use of high-power 810-nm diode laser as monotherapy on the clinical and tomographic success of the treatment of teeth with periapical lesions: an observational clinical study
- Fabricio Hinojosa Pedraza, Abel Victor Isidro Teves-Cordova, Murilo Priori Alcalde, Marco Antonio Hungaro Duarte
- Restor Dent Endod 2025;50(2):e15. Published online May 15, 2025
- DOI: https://doi.org/10.5395/rde.2025.50.e15
-
Abstract
PDFPubReaderePub
- Objectives
The aim of this study was to demonstrate the impact of a high-power 810-nm diode laser as monotherapy on the clinical and tomographic success of treating teeth with periapical lesions, through a series of 31 cases.
Methods
Teeth with apical lesions underwent endodontic treatment in which a high-power 810-nm diode laser with saline solution was used as monotherapy for disinfection. This type of therapy aimed to replace the traditional irrigation protocol with sodium hypochlorite. This research is the first to assess the clinical success of this alternative treatment, along with tomographic evaluations conducted over periods ranging from 2 to 7 years, analyzed using the periapical index based on cone-beam computed tomography (CBCTPAI). All cases were performed by a single clinician following the same laser protocol, which involved using 1 W of continuous power and four cycles of 20 seconds of laser activation.
Results
All teeth showed no clinical symptoms upon follow-up examination. However, the tomographic evaluation revealed that the success rates for teeth receiving primary treatment were 60% and 80% according to strict and loose criteria, respectively. For teeth requiring retreatment, the success rates were 12.5% and 37.5% using strict and loose criteria, respectively.
Conclusions
The teeth with apical lesions that underwent primary treatment did not present clinical symptoms, but they showed a moderate success rate on tomographic evaluation. However, despite lacking clinical symptoms, teeth with apical lesions that required retreatment had a very low success rate on tomographic evaluation. -
Citations
Citations to this article as recorded by
- Adherence to core outcome set for endodontic treatments (COSET) international consensus: Two-year before/after bibliometric systematic review
Carolina Bender Hoppe, Pauline Mastella Lang, Lara Dotto, Mateus Silveira Martins Hartmann, Fabiana Soares Grecca
Journal of Dentistry.2026; 173: 106834. CrossRef - Diode Laser-Guided Protocol for Endo-Perio Lesions: Toward a Multi-Stage Therapeutic Strategy—A Case Series and Brief Literature Review
Ioana-Roxana Munteanu, George-Dumitru Constantin, Ruxandra-Elena Luca, Ioana Veja, Mariana-Ioana Miron
Medicina.2025; 61(12): 2157. CrossRef
- Adherence to core outcome set for endodontic treatments (COSET) international consensus: Two-year before/after bibliometric systematic review
- 5,330 View
- 235 Download
- 2 Web of Science
- 2 Crossref
- Bibliometric analysis of the GentleWave system: trends, collaborations, and research gaps
- Raimundo Sales de Oliveira Neto, Thais de Moraes Souza, João Vitor Oliveira de Amorim, Thaine Oliveira Lima, Guilherme Ferreira da Silva, Rodrigo Ricci Vivan, Murilo Priori Alcalde, Marco Antonio Hungaro Duarte
- Restor Dent Endod 2025;50(2):e17. Published online May 12, 2025
- DOI: https://doi.org/10.5395/rde.2025.50.e17
-
Abstract
PDF
 Supplementary MaterialPubReaderePub
Supplementary MaterialPubReaderePub - Objectives
The study aimed to conduct a bibliometric analysis of the GentleWave system (Sonendo, Inc.).
Methods
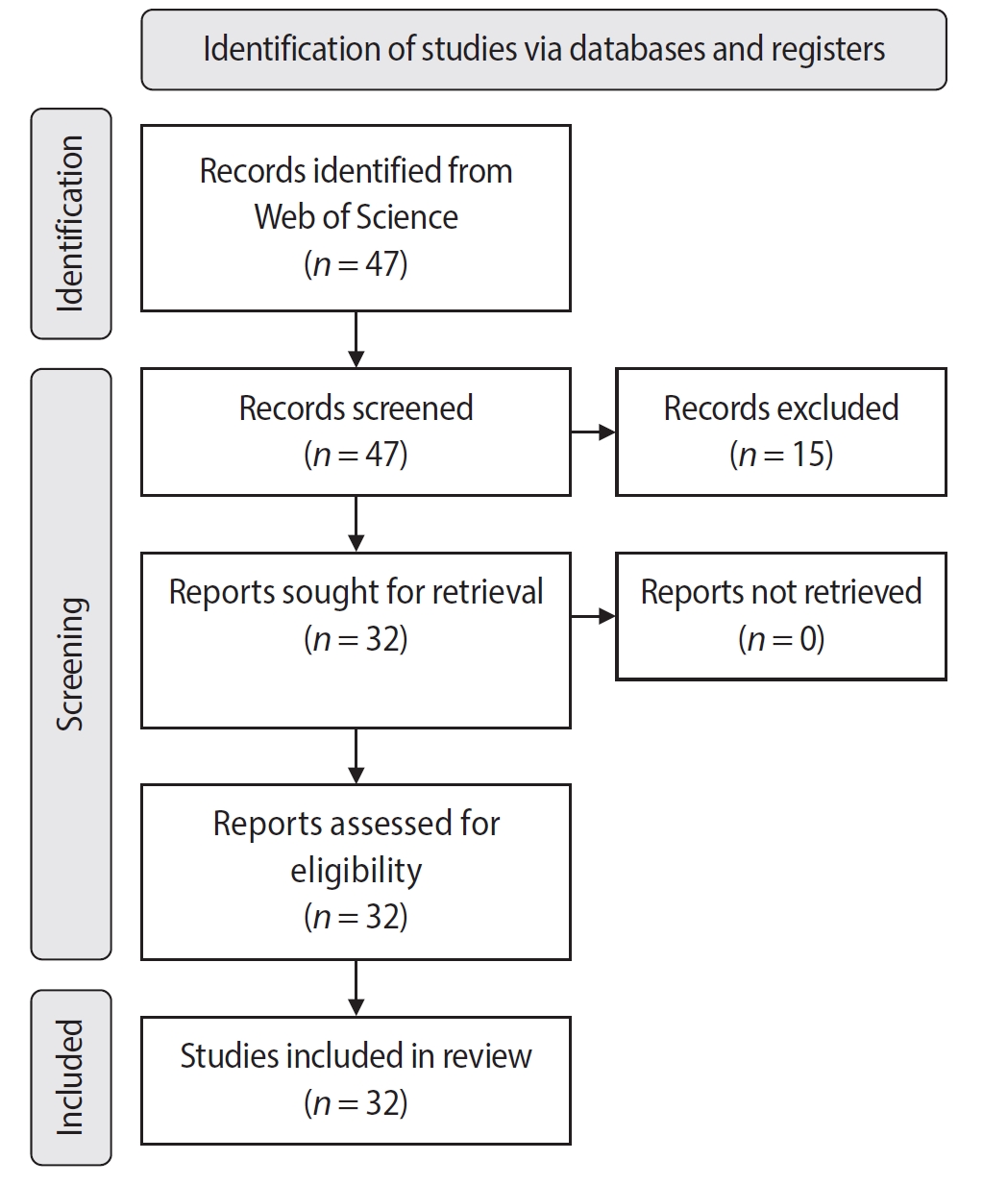
An electronic search was conducted in June 2024 using the Web of Science Collection database. Two reviewers independently screened publications, extracting data on authorship, publication details, study design, and citation metrics. Statistical analyses were performed in R to assess variable correlations, while the VOSviewer (Visualization of Similarities Viewer) software was used to map author and keyword networks.
Results
The search yielded 47 records, with 32 studies included. Publications spanned 2014 to 2024. The Journal of Endodontics published the highest number of studies (n = 15), and the International Endodontic Journal had the highest impact factor (5.4). The University of British Columbia and Sonendo, Inc. were the most frequent affiliations. Among the 32 articles, 28 were in vitro studies, primarily focusing on microbiology (n = 9). A total of 95 authors were identified, with Haapasalo and Shen being the most cited (n = 229). The articles accumulated 495 citations, demonstrating a strong positive correlation between the number of studies and citation counts (r = 0.98).
Conclusions
The analysis highlights a predominance of in vitro studies. Geographic concentration in the United States and Canada limits diversity, while the strong correlation between study numbers and citations suggests that increased publication volume enhances visibility. -
Citations
Citations to this article as recorded by- Three-year Outcomes of Conventional Versus Minimally Invasive Endodontic Treatment Protocols: A Retrospective Study
Kiavash Hossini, He Liu, Ya Shen, Jolanta Aleksejuniene, Fahda Algahtani, Ahmed Hieawy
Journal of Endodontics.2026; 52(4): 558. CrossRef
- Three-year Outcomes of Conventional Versus Minimally Invasive Endodontic Treatment Protocols: A Retrospective Study
- 4,983 View
- 104 Download
- 1 Web of Science
- 1 Crossref
- Shaping ability and cyclic fatigue resistance between Genius ProFlex, ZenFlex, and TruNatomy rotary systems: an experimental study
- Raimundo Sales de Oliveira Neto, Murilo Priori Alcalde, Pedro Cesar Gomes Titato, Pedro Henrique Souza Calefi, Carlos Alberto Spironelli Ramos, Guilherme Ferreira da Silva, Rodrigo Ricci Vivan, Marco Antonio Hungaro Duarte
- Restor Dent Endod 2025;50(1):e9. Published online February 13, 2025
- DOI: https://doi.org/10.5395/rde.2025.50.e9
-
Abstract
PDFPubReaderePub
- Objectives
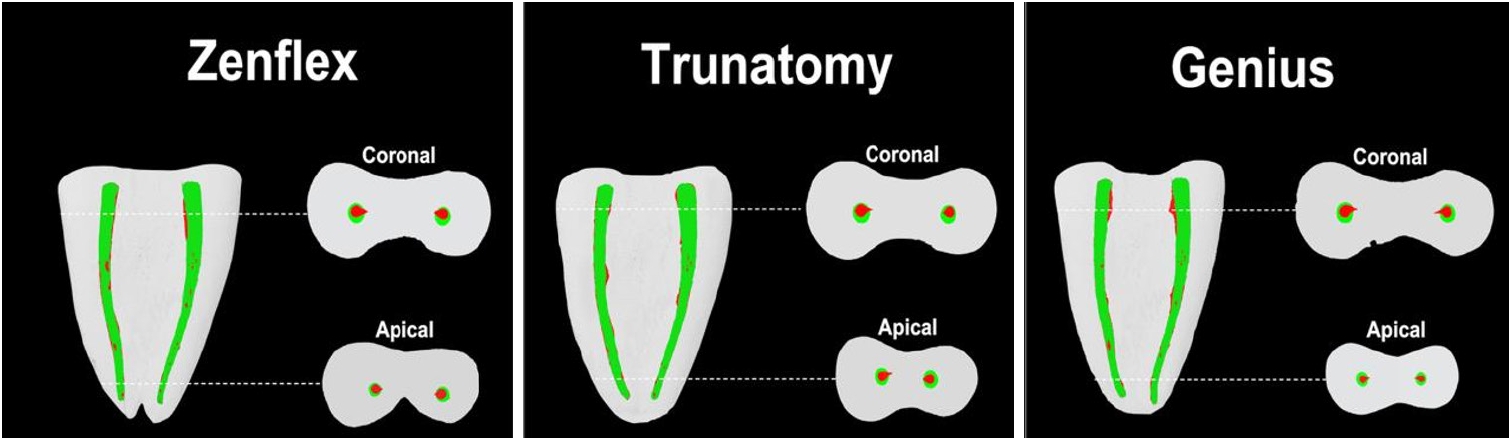
The aim of this study was to investigate the efficacy of three newly introduced rotary endodontic systems: Genius ProFlex (Medidenta), TruNatomy (Dentsply Maillefer), and ZenFlex (Kerr).
Methods
Forty-five mandibular molars with root canal curvatures <5° were utilized. Micro-computed tomography scans were performed pre- and post-preparation to assess apical transportation, centralization, percentage of dentin wear, and canal volume alterations. Eight instruments of each diameter underwent cyclic fatigue testing.
Results
The percentage of dentin wear on mesial and distal walls showed no significant differences among ZenFlex, TruNatomy, and Genius ProFlex at 1, 2, 3, and 4 mm from the apical foramen and root canal orifice (p > 0.05). Centering ability varied in the mesiolingual canal (p < 0.05). No notable differences were observed in transportation (p > 0.05). Genius ProFlex demonstrated lower volumetric changes (p < 0.05). There were significant differences in cyclic fatigue, with higher values for Genius ProFlex and lower values for TruNatomy (p < 0.05).
Conclusions
The three nickel-titanium rotary instruments are safe and efficient for root canal preparation, with Genius ProFlex exhibiting superior cyclic fatigue resistance. -
Citations
Citations to this article as recorded by- Influence of kinematic motion and instrumentation strategy on apical debris extrusion during root canal preparation: An in vitro study
Amira Alghazaly, Jumanah Aljohani, Khadijah Mohabat, Rafah Ghous
Journal of Conservative Dentistry and Endodontics.2026; 29(7): 741. CrossRef - Comparison of Shaping Ability and Apical Debris Extrusion Using 4 Different Nickel–Titanium Single‐File Systems
Siyu Li, Mengzhen Tang, Xi Wang, Jian Yang, Hyun-Do Jung
International Journal of Biomaterials.2025;[Epub] CrossRef
- Influence of kinematic motion and instrumentation strategy on apical debris extrusion during root canal preparation: An in vitro study
- 4,410 View
- 191 Download
- 1 Web of Science
- 2 Crossref
-
Procedural errors detected by cone beam tomography in cases with indication for retreatment:
in vivo cross-sectional study - Henry Paul Valverde Haro, Carmen Rosa Garcia Rupaya, Flávio R. F. Alves
- Restor Dent Endod 2024;49(3):e26. Published online June 24, 2024
- DOI: https://doi.org/10.5395/rde.2024.49.e26
-
Abstract
PDFPubReaderePub
Objectives This study aimed to investigate the frequency and type of endodontic procedural errors in cases indicated for retreatment through cone-beam computed tomography (CBCT) analysis.
Materials and Methods The sample consisted of 96 CBCT scans, encompassing 122 permanent teeth with fully formed roots. Errors included perforation, instrument fracture, canal transportation, missed canals, and inadequate apical limit of filling. Additionally, potential risk factors were analyzed and subjected to statistical modeling.
Results The most frequent procedural error observed was the inadequate apical limit of filling, followed by canal transportation, perforation, missed canal, and instrument fracture. Statistically significant associations were identified between various procedural errors and specific factors. These include canal transportation and root canal wall, with the buccal wall being the most commonly affected; missed canal and tooth type, particularly the palatine and second mesiobuccal canal canals; inadequate apical limit of filling and root curvature, showing a higher deviation to the mesial direction in severely curved canals; inadequate apical limit of filling and the presence of calcifications, with underfilling being the most frequent; canal transportation and periapical lesion, notably with deviation to the buccal direction; and the direction of perforation and periapical lesion, most frequently occurring to buccal direction.
Conclusions CBCT emerges as a valuable tool in identifying procedural errors and associated factors, crucial for their prevention and management.
-
Citations
Citations to this article as recorded by- Regenerative endodontic treatment of a necrotic immature taurodont mandibular second molar with endodontic infection
Ali Mohammed Addokhi, Ahmed Abuhaimed
Saudi Endodontic Journal.2026; 16(2): 271. CrossRef - Repair of furcal perforations using different calcium silicate cements: An in vitro study
Ariana Esperanza Apolo Aguilar, Maria Soledad Peñaherrera Manosalvas, Henry Paul Valverde Haro
Journal of Conservative Dentistry and Endodontics.2025; 28(10): 1007. CrossRef - Impact of Downward Load and Rotational Kinematics on Root Canal Instrumentation with a Heat-Treated Nickel–Titanium Rotary Instrument
Risako Yamamoto, Keiichiro Maki, Shunsuke Kimura, Satoshi Omori, Keiko Hirano, Arata Ebihara, Yoshio Yahata, Takashi Okiji
Materials.2025; 19(1): 108. CrossRef - ANALYSIS OF THE QUALITY OF ROOT CANAL OBTURATION AND PREVALENCE OF APICAL PERIODONTITIS IN ENDODONTICALLY TREATED TEETH
Cristina Coralia Nistor, Ioana Suciu , Elena Zabrac , Ruxandra Ioana Bartok , Bogdan Dimitriu , Andreea Baluta
Romanian Journal of Oral Rehabilitation.2024; 16(4): 311. CrossRef
- Regenerative endodontic treatment of a necrotic immature taurodont mandibular second molar with endodontic infection
- 4,322 View
- 142 Download
- 2 Web of Science
- 4 Crossref
Case Reports
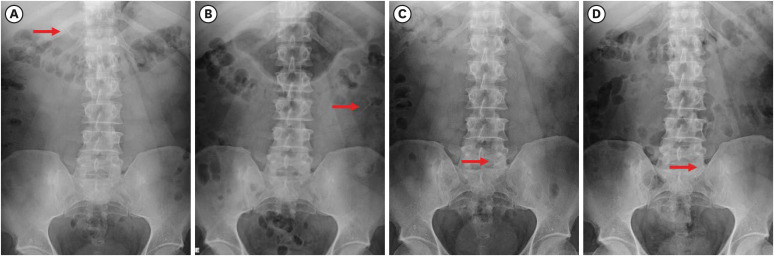
- Ingestion and surgical retrieval of an endodontic file: a case report
- Devon Marta Ptak, Elinor Alon, Robert Bruce Amato, Julia Tassinari, Adrian Velasquez
- Restor Dent Endod 2023;48(4):e32. Published online September 2, 2023
- DOI: https://doi.org/10.5395/rde.2023.48.e32
-
Abstract
PDFPubReaderePub
Ingestions and aspirations of foreign bodies are rare, but do occasionally occur during dental treatment. Although reports exist, few include photos demonstrating the extensive surgical intervention that may be necessary to manage such events. Perhaps this lack of visualization, and associated lack of awareness, is one of the reasons some clinicians still provide non-surgical root canal therapy (NSRCT) without a rubber dam. This case report outlines the medical treatment of a 30-year-old male who initially presented to a general dentist’s office (not associated with the authors) for NSRCT of their mandibular right first molar. A rubber dam was not used for this procedure, during which the accidental ingestion of an endodontic K-file occurred. The patient was subsequently hospitalized for evaluation and treatment, consisting of numerous imaging studies, endoscopic evaluation, and surgical removal of the file from his small intestine. The ingestion of foreign bodies, and the associated complications, can be reduced through the routine use of a rubber dam, which is considered the standard of care for NSRCT. This case graphically illustrates the potential consequences associated with deviating from the standard of care and should remind clinicians that a rubber dam is necessary for all cases of NSRCT.
-
Citations
Citations to this article as recorded by- Advantages and limitations of the rubber dam. Part 2: advantages of rubber dam use
Artemy Vadimovich Karmanov, Alena Sergeevna Silkina, Natalia Alexandrovna Sokolovich
Dental Update.2026; 53(3): 198. CrossRef - Anesthesiological Management of a Sewing Needle Impacted in the Larynx in an Adult: A Case Report
Stefanie R. Senn, Felix C. Jansen, Caveh Madjdpour, Isabel Besozzi, Daniel A. Button
Clinical Case Reports.2026;[Epub] CrossRef - Dental Dam Isolation for Crown Removal, Atraumatic Tooth Extraction, Immediate Implant Placement, and Restoration Cementation: A Case Study
G Guzman-Perez, S Rojas-Rueda, F Floriani, A Unnadkat, C-C Fu, CA Jurado
Operative Dentistry.2025; 50(1): 5. CrossRef - Patient and Operator Experiences with Conventional Rubber Dam and OptiDam: A Randomized Clinical Trial
Rashed F. Binqali, Abdulwahab M. Alghamdi, Mishal S. Aloufi, Suliman A. Alharbi, Omair M. Bukhari, Reham M. Alsamman
Journal of International Society of Preventive and Community Dentistry.2025; 15(6): 554. CrossRef
- Advantages and limitations of the rubber dam. Part 2: advantages of rubber dam use
- 6,152 View
- 134 Download
- 2 Web of Science
- 4 Crossref
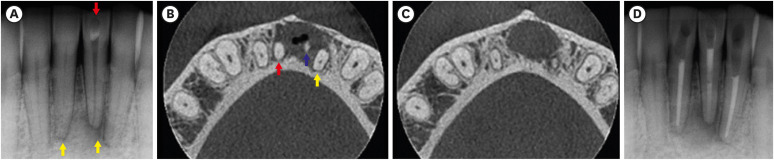
- Persistent pain after successful endodontic treatment in a patient with Wegener’s granulomatosis: a case report
- Ricardo Machado, Jorge Aleixo Pereira, Filipe Colombo Vitali, Michele Bolan, Elena Riet Correa Rivero
- Restor Dent Endod 2022;47(3):e26. Published online June 9, 2022
- DOI: https://doi.org/10.5395/rde.2022.47.e26
-
Abstract
PDFPubReaderePub
Wegener’s granulomatosis (WG) is a condition with immune-mediated pathogenesis that can present oral manifestations. This report describes the case of a patient diagnosed with WG 14 years previously, who was affected by persistent pain of non-odontogenic origin after successful endodontic treatment. A 39-year-old woman with WG was diagnosed with pulp necrosis and apical periodontitis of teeth #31, #32, and #41, after evaluation through a clinical examination and cone-beam computed tomography (CBCT). At the first appointment, these teeth were subjected to conventional endodontic treatment. At 6- and 12-month follow-up visits, the patient complained of persistent pain associated with the endodontically treated teeth (mainly in tooth #31), despite complete remission of the periapical lesions shown by radiographic and CBCT exams proving the effectiveness of the endodontic treatments, thus indicating a probable diagnostic of persistent pain of non-odontogenic nature. After the surgical procedure was performed to curette the lesion and section 3 mm of the apical third of tooth #31, the histopathological analysis suggested that the painful condition was likely associated with the patient's systemic condition. Based on clinical, radiographic, and histopathological findings, this unusual case report suggests that WG may be related to non-odontogenic persistent pain after successful endodontic treatments.
-
Citations
Citations to this article as recorded by- Toothaches of Non-odontogenic Origin
Davis C. Thomas, Tanvee Somaiya, Ahana Ajayakumar, Vaishnavi Prabhakar
Dental Clinics of North America.2026; 70(1): 209. CrossRef - Prevalence of persistente pain after endodontic treatment
Edmundo Duarte Martins, Allya Francisca Marques Borges, Lidiane Oliveira Leão, Bianca Marques de Mattos de Araujo, José Stechman Neto, Tatiana Carvalho Kowaltschuk, Camila de Castro Corrêa Corrêa, Cristiano Miranda de Araújo, Karinna Veríssimo Meira Tave
Brazilian Journal of Oral Sciences.2026; 25: e269272. CrossRef
- Toothaches of Non-odontogenic Origin
- 6,994 View
- 87 Download
- 2 Crossref
Research Articles
- Effect of post space preparation drills on the incidence of root dentin defects
- Thaíse Ayres Bezerra Zuli, Orlando Aguirre Guedes, Gislaine Figueiredo Zarza Arguello Gonçalves, Aurélio Rosa da Silva Júnior, Álvaro Henrique Borges, Andreza Maria Fábio Aranha
- Restor Dent Endod 2020;45(4):e53. Published online October 16, 2020
- DOI: https://doi.org/10.5395/rde.2020.45.e53
-
Abstract
PDFPubReaderePub
Objectives This study investigated the incidence of root dentin defects after the use of different post space preparation (PSP) drills.
Materials and Methods Seventy-two bovine incisors were selected and obtained 14-mm-long root sections. Twelve roots served as controls with no intervention (G1). The 60 root canals remaining were instrumented using the crown-down technique with the ProTaper Next system and obturated using the lateral condensation technique. Specimens were randomly distributed into 5 groups (
n = 12) according to the operative steps performed: G2, root canal instrumentation and filling (I+F); G3, I+F and PSP with Gates-Glidden drills; G4, I+F and PSP with Largo-Peeso reamers; G5, I+F and PSP with Exacto drill; and G6, I+F and PSP with WhitePost drill. Roots were sectioned at 3, 6, 9, and 12 mm from the apex, and digital images were captured. The presence of root dentin defects was recorded. Data were analyzed by the χ2 test, withp < 0.05 considered to indicate statistical significance.Results Root dentin defects were observed in 39.6% of the root sections. No defects were observed in G1. G5 had significantly more cracks and craze lines than G1, G2, and G3 (
p < 0.05), and more fractures than G1, G2, G3, and G4 (p < 0.05). When all root sections were analyzed together, significantly more defects were observed at the 12-mm level than at the 3-mm level (p < 0.05).Conclusions PSP drills caused defects in the root dentin. Gates-Glidden drills caused fewer root defects than Largo-Peeso reamers and Exacto drills.
-
Citations
Citations to this article as recorded by- Fracture Strength of CAD/CAM Endocrown and Post-Core Restorations with Fiber Strip Reinforcement in Mandibular Premolars
Kerem Yılmaz, Hakan Aydın, Zeynep Soylu, Özge Çiloğlu, Esma Fatıma Delican, Mehmet Mustafa Özarslan, Fehmi Gönüldaş
Journal of Functional Biomaterials.2026; 17(5): 248. CrossRef - Evaluation of dentinal crack formation during post space preparation using different fiber post systems with micro-computed tomography
Ayşe Nur Kuşuçar, Damla Kırıcı
BMC Oral Health.2025;[Epub] CrossRef - Fracture and Crack Behavior of Weakened Incisors Restored With Fiber Posts, Polyethylene Reinforcement, or 3D-Printed Endocrowns
Diana Codas-Duarte, Laís L Pelozo, Jardel F Mazzi-Chaves, Fabiane C Lopes-Olhê, Manoel D Sousa-Neto, Aline E Souza-Gabriel
Cureus.2025;[Epub] CrossRef - Selecting drill size for post space preparation based on final endodontic radiographs: An in vitro study
Farzaneh Farid, Julfikar Haider, Marjan Sadeghpour Shahab, Nika Rezaeikalantari
Technology and Health Care.2024; 32(4): 2575. CrossRef - Cone Beam Computed Tomography Analysis of Post Space in Bifurcated Premolars Using ParaPost and Peeso Reamer Drills
Abdulaziz Saleh Alqahtani, Omar Nasser Almonabhi, Abdulmajeed Moh. Almutairi, Reem R. Alnatsha
The Open Dentistry Journal.2024;[Epub] CrossRef - A Comparative Evaluation of Real-Time Guided Dynamic Navigation and Conventional Techniques for Post Space Preparation During Post Endodontic Management: An In Vitro Study
Sherifa Shervani, Sihivahanan Dhanasekaran, Vijay Venkatesh
Cureus.2024;[Epub] CrossRef - The effect of ultrasonic vibration protocols for cast post removal on the incidence of root dentin defects
Giulliano C. Serpa, Orlando A. Guedes, Neurinelma S. S. Freitas, Julio A. Silva, Carlos Estrela, Daniel A. Decurcio
Journal of Oral Science.2023; 65(3): 190. CrossRef
- Fracture Strength of CAD/CAM Endocrown and Post-Core Restorations with Fiber Strip Reinforcement in Mandibular Premolars
- 3,841 View
- 43 Download
- 7 Crossref
- Comparative evaluation of the effectiveness of ultrasonic tips versus the Terauchi file retrieval kit for the removal of separated endodontic instruments
- Preeti Jain Pruthi, Ruchika Roongta Nawal, Sangeeta Talwar, Mahesh Verma
- Restor Dent Endod 2020;45(2):e14. Published online February 6, 2020
- DOI: https://doi.org/10.5395/rde.2020.45.e14
-
Abstract
PDFPubReaderePub
Objective The aim of this study was to perform a comparative evaluation of the effectiveness of ultrasonic tips versus the Terauchi file retrieval kit (TFRK) for the removal of broken endodontic instruments.
Materials and Methods A total of 80 extracted human first mandibular molars with moderate root canal curvature were selected. Following access cavity preparation canal patency was established with a size 10/15 K-file in the mesiobuccal canals of all teeth. The teeth were divided into 2 groups of 40 teeth each: the P group (ProUltra tips) and the T group (TFRK). Each group was further subdivided into 2 smaller groups of 20 teeth each according to whether ProTaper F1 rotary instruments were fractured in either the coronal third (C constituting the PC and TC groups) or the middle third (M constituting the PM and TM groups). Instrument retrieval was performed using either ProUltra tips or the TFRK.
Results The overall success rate at removing the separated instrument was 90% in group P and 95% in group T (
p > 0.05) The mean time for instrument removal was higher with the ultrasonic tips than with the TFRK (p > 0.05).Conclusion Both systems are acceptable clinical tools for instrument retrieval but the loop device in the TFRK requires slightly more dexterity than is needed for the ProUltra tips.
-
Citations
Citations to this article as recorded by- Comparative evaluation of success rate and operator variability in loop.based versus ultrasonic retrieval of fractured endodontic instruments: An ex vivo study
Tanushree Saxena, Vivek Devidas Mahale, Manish Ranjan, Sanyuta Singh, E. Aparna Mohan, M. Hema
Saudi Endodontic Journal.2026; 16(1): 73. CrossRef - Comparative evaluation of time efficiency and dentin preservation in ultrasonic versus loop retrieval of separated endodontic files: An ex vivo study with pilot nano-computed tomography analysis
Tanushree Saxena, Vivek Devidas Mahale, Manish Ranjan, M. Hema, Sanyukta Singh, E. Aparna Mohan
Saudi Endodontic Journal.2026; 16(1): 90. CrossRef - In Vitro Characterisation of Resonant Behaviour of Separated Ni–Ti Endodontic File Fragments Using a Biomechanical Modelling Approach
Vidhi Kiran Bhalla, Devender Nath Maurya, Amit Malhotra, Ruchika Roongta Nawal, Shahid Malik, Sangeeta Talwar
International Endodontic Journal.2026;[Epub] CrossRef - Root Fracture Resistance After Management of Separated Intracanal Instruments: An Ex Vivo Study
Rawan Ballan, Hisham Alafif
International Journal of Prosthodontics and Restorative Dentistry.2026; 16(2): 57. CrossRef - Effects of different platform preparation and retrieval techniques on broken file removal and fracture strength
Esra YAVAS, Selen KUCUKKAYA EREN
Brazilian Oral Research.2026;[Epub] CrossRef - Minimally Invasive Approach to the Retrieval of Fractured Intracanal Instruments: A Clinical Report of Two Cases
Farsana Thasni CT, J Hariharan, K Binu Nathan, Tisson V Job, Parvathy VB, Raseena AK
Journal of Dentistry and Bio-Allied Health Sciences.2026; 3(1): 37. CrossRef - Dental Microscope-Assisted and Indirect Ultrasonic Technique for Retrieval of Separated Endodontic Instruments: A Case Report
Juan Carlos Ortiz Hugues
Journal of Clinical Advances in Dentistry.2026; : 7. CrossRef - Comparison of the pull-out force of different microtube-based methods in fractured endodontic instrument removal: An in-vitro study
Nasim Hashemi, Mohsen Aminsobhani, Mohammad Javad Kharazifard, Fatemeh Hamidzadeh, Pegah Sarraf
BMC Oral Health.2025;[Epub] CrossRef - Fracture resistance and volumetric dentin change after management of broken instrument using static navigation – An in vitro study
Shady Atef Adeeb Yassa, Mohamed Nabeel, Ahmed M. Ghobashy, Moataz B. Alkhawas
Journal of Conservative Dentistry and Endodontics.2025; 28(4): 319. CrossRef - Remoção de instrumento fraturado com a técnica do laço: relato de caso
Larissa Sousa Rangel, Ryhan Menezes Cardoso, Thayane Kelly Trajano da Silva, Robeci Alves Macêdo Filho, Andressa Cartaxo de Almeida, Mariana Camilly Tavares Ferreira, Thalles Gabriel Germano Lima, Diana Santana de Albuquerque
Caderno Pedagógico.2025; 22(7): e16332. CrossRef - Would It Necessarily Require Retrieving Endodontic Files on Every Instance? Implementing Separated Files with the Bypass Technique: Report of Three Cases
Mohit S. Zarekar, Apurva S. Satpute, Mohini S. Zarekar
Journal of Primary Care Dentistry and Oral Health.2025; 6(2): 118. CrossRef - Novel electromagnetic device to retrieve fractured stainless steel endodontic files: an in-vitro investigation
Ashraf Mohammed Alhumaidi, Mubashir Baig Mirza, Ahmed A. Alelyani, Raid A. Almnea, Amal S. Shaiban, Ahmed Altuwalah, Riyadh Alroomy, Ahmed Abdullah Al Malwi, Ahmad Jabali, Mohammed M. Al Moaleem
BMC Oral Health.2025;[Epub] CrossRef - Efficiency of Root Canal Treatment Using Loops While Endodontic Treatment: A Clinical Study
Chitharanjan Shetty, Kodithala Sravya, Abhilasha Bhawalkar, Alok Dubey, Tejaswi Kala, Prachi Sethy
Journal of Pharmacy and Bioallied Sciences.2025; 17(Suppl 5): S3735. CrossRef - Efficiency of fractured file retrieval according to different nickel-titanium alloys and fragment lengths
Joon Hyuk Yoon, Yoshitsugu Terauchi, Jae-Hoon Kim, Sang Won Kwak, Hyeon-Cheol Kim
BMC Oral Health.2025;[Epub] CrossRef - Broken Instrument Removal Methods with a Minireview of the Literature
Mohsen Aminsobhani, Nasim Hashemi, Fatemeh Hamidzadeh, Pegah Sarraf, Giovanni Mergoni
Case Reports in Dentistry.2024;[Epub] CrossRef - Comprehensive Assessment of Cyclic Fatigue Strength in Five Multiple-File Nickel–Titanium Endodontic Systems
Jorge N. R. Martins, Emmanuel J. N. L. Silva, Duarte Marques, Francisco M. Braz Fernandes, Marco A. Versiani
Materials.2024; 17(10): 2345. CrossRef - Management of an Intracanal Separated Instrument in the Lower Right First Molar: A Case Report
Pratik Rathod, Aditya Patel, Anuja Ikhar, Manoj Chandak, Joyeeta Mahapatra, Tejas Suryawanshi, Jay Patil, Priti Mahale
Cureus.2024;[Epub] CrossRef - Predictive factors in the retrieval of endodontic instruments: the relationship between the fragment length and location
Ricardo Portigliatti, Eugenia Pilar Consoli Lizzi, Pablo Alejandro Rodríguez
Restorative Dentistry & Endodontics.2024;[Epub] CrossRef - Efficacy of two instrument retrieval techniques in removing separated rotary and reciprocating nickel-titanium files in mandibular molars – An in vitro study
S. Jitesh, Smita Surendran, Velmurugan Natanasabapathy
Journal of Conservative Dentistry and Endodontics.2024; 27(12): 1240. CrossRef - Effect of Heat Treatment on Mechanical Properties of Nickel-Titanium Instruments
Eunmi Kim, Jung-Hong Ha, Samuel O. Dorn, Ya Shen, Hyeon-Cheol Kim, Sang Won Kwak
Journal of Endodontics.2024; 50(2): 213. CrossRef - Efficacy of instrument removal techniques in root canal treatment: a literature review
Rómulo Guillermo López Torres, Jairo Romario Moreno Ochoa, Verónica Alejandra Salame Ortiz
Salud, Ciencia y Tecnología - Serie de Conferencias.2024;[Epub] CrossRef - Efficacy of the HBW Ultrasonic Ring for retrieval of fragmented manual or rotatory instruments
Jennifer Galván-Pacheco, Verónica Méndez-González, Ana González-Amaro, Heriberto Bujanda-Wong, Amaury Pozos-Guillén, Arturo Garrocho-Rangel
Journal of Oral Science.2023; 65(4): 278. CrossRef - Retrieving Fragments
Swayangprabha Sarangi, Manoj Ghanshyamdasji Chandak, Kajol Naresh Relan, Payal Sandeep Chaudhari, Pooja Chandak, Anuja Ikhar
Journal of Datta Meghe Institute of Medical Sciences University.2022; 17(2): 429. CrossRef - A novel approach for retrieval of separated endodontic instrument: Two case reports
Tanvi Kohli, Syed Shahid Hilal
IP Indian Journal of Conservative and Endodontics.2022; 7(3): 143. CrossRef - A novel endodontic extractor needle for separated instrument retrieval
Saaid Al Shehadat, Colin Alexander Murray, Sunaina Shetty Yadadi
Advances in Biomedical and Health Sciences.2022; 1(2): 116. CrossRef - Present status and future directions: Removal of fractured instruments
Yoshi Terauchi, Wagih Tarek Ali, Mohamed Mohsen Abielhassan
International Endodontic Journal.2022; 55(S3): 685. CrossRef - Ultrasonic Use in Endodontic Management Approach, Review Article
Bakheet Mohammed Al-Ghannam, Khalid Abdulmohsen Almuhrij, Rund Talal Basfar, Raghad Omar Alamoudi, Aseel Mohammed Alqahtani, Ahmed Atef Sait, Ahmed Loay Ghannam, Sultan Khalid Abdoun
World Journal of Environmental Biosciences.2021; 10(1): 61. CrossRef - The Time Taken for Retrieval of Separated Instrument and the Change in Root Canal Volume after Two Different Techniques Using Cbct
Balu Santhosh Kumar, Sridevi Krishnamoorthy, Sandhya Shanmugam, Angambakkam Rajasekharan PradeepKumar
Indian Journal of Dental Research.2021; 32(4): 489. CrossRef
- Comparative evaluation of success rate and operator variability in loop.based versus ultrasonic retrieval of fractured endodontic instruments: An ex vivo study
- 5,655 View
- 152 Download
- 28 Crossref
Case Reports
- Oral manifestation and root canal therapy of the patient with mucopolysaccharidosis
- Ji-Hye Yoon, Hyo-Il Lee, Ji-Hyun Jang, Sung-Hyeon Choi, Hoon-Sang Chang, Yun-Chan Hwang, In-Nam Hwang, Bin-Na Lee, Won-Mann Oh
- Restor Dent Endod 2019;44(2):e14. Published online April 4, 2019
- DOI: https://doi.org/10.5395/rde.2019.44.e14
-
Abstract
PDFPubReaderePub
Mucopolysaccharidosis (MPS) is an inherited metabolic disorder caused by a deficiency in enzymes that participate in the degradation of glycosaminoglycans (GAGs) such as heparin sulfate and dermatan sulfate. Left untreated, patients show progressive mental and physical deterioration due to deposition of GAGs in organs. Death often occurs due to cardiac or respiratory failure before patients reach their early twenties. MPS has several oral and dental manifestations. An enlarged head, short neck, and open mouth associated with a large tongue are major characteristics of MPS patients. Dental complications can be severe, including unerupted dentition, dentigerous cyst-like follicles, malocclusions, condylar defects, and gingival hyperplasia. A 21-year-old female patient with MPS was described in this article, with special emphasis on oral manifestations and dental treatment.
-
Citations
Citations to this article as recorded by- Clinical and Radiological Features Suggestive of Mucopolysaccharidosis in Two Siblings From Sudan: A Case Series
Alaa Bella, Mumen Abdalazim Dafallah, Ashraf Yousif Fadlalla, Bothaina Faisal Elmardi, Yomna Mohialdin Alataya, Abdalla Abdelmahmoud Abdalla, Mohammed Almeldin Ahmed Ibrahim, Mawada Faisal Nugud, Salah Elamin Ahmed Babiker, Hiba faroug Al_amin, Safaa Ayou
Clinical Case Reports.2026;[Epub] CrossRef - Pediatric Interventions in a Sanfilippo Syndrome Patient Under General Anesthesia: A Case Report
Ahmad Al Malak, Hassan Issawi, Mohammad Hassoun, Mohammad Al Halabi, Darko Macan
Case Reports in Dentistry.2025;[Epub] CrossRef - Behavioural disorders and sleep problems in Sanfilippo syndrome: overlaps with some other conditions and importance indications
Karolina Wiśniewska, Jakub Wolski, Paulina Anikiej-Wiczenbach, Magdalena Żabińska, Grzegorz Węgrzyn, Karolina Pierzynowska
European Child & Adolescent Psychiatry.2025; 34(6): 1795. CrossRef - Hurler syndrome: Oral and radiographic findings of a rare clinical case
W. Kabbassi, H. Hessissen, J. Hammouti
Medical Reports.2025; 14: 100325. CrossRef - Sanfilippo syndrome: consensus guidelines for clinical care
Nicole Muschol, Roberto Giugliani, Simon A. Jones, Joseph Muenzer, Nicholas J. C. Smith, Chester B. Whitley, Megan Donnell, Elise Drake, Kristina Elvidge, Lisa Melton, Cara O’Neill
Orphanet Journal of Rare Diseases.2022;[Epub] CrossRef - Manifestaciones bucales de pacientes con mucopolisacaridosis. Serie de casos
Andrea Verónica Ríos, Mariana Llorensi
Revista de la Asociación Odontológica Argentina.2021;[Epub] CrossRef
- Clinical and Radiological Features Suggestive of Mucopolysaccharidosis in Two Siblings From Sudan: A Case Series
- 2,438 View
- 7 Download
- 6 Crossref
- Revitalization of necrotic mature permanent incisors with apical periodontitis: a case report
- Emre Nagas, M. Ozgur Uyanik, Zafer C. Cehreli
- Restor Dent Endod 2018;43(3):e31. Published online July 5, 2018
- DOI: https://doi.org/10.5395/rde.2018.43.e31
-
Abstract
PDFPubReaderePub
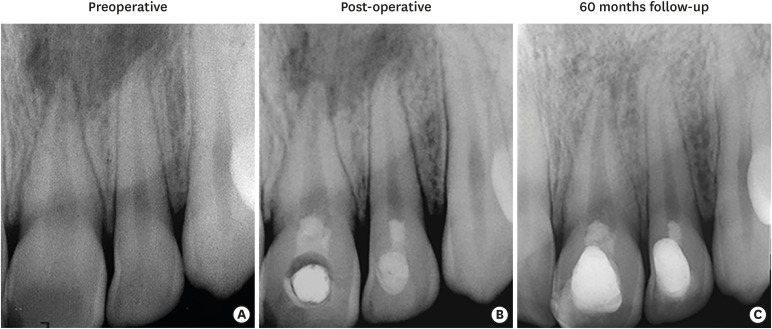
Despite considerable focus on the regenerative endodontic treatment of immature teeth with necrotic infected pulps and apical periodontitis, little data exist with regard to its possible implementation in necrotic permanent teeth with complete apical and radicular development. The present report describes the procedures and outcome of a regenerative endodontic treatment approach in 2 previously-traumatized incisors with closed apex with apical periodontitis. A 2-visit treatment procedure was employed. At initial visit, the root canals were copiously irrigated, followed by placement of a triple antibiotic paste containing ciprofloxacin, metronidazole, and clindamycin into the root canals. After 4 weeks, the antibiotic paste was removed, and apical bleeding was initiated with size 10 hand files beyond the apices. The root canals were coronally sealed with mineral trioxide aggregate, and the access cavities were restored with bonded resin composite. At post-operative 60 months, both teeth were remained asymptomatic, with the recall radiographs showing complete resolution of apical radiolucency and reestablishment of periradicular tissues. In both teeth, the dimensions of root space remained unchanged as verified by image analysis. The revitalization protocol utilizing root canal disinfection and induced apical bleeding in necrotic, closed-apex incisors may offer a clinically acceptable alternative to conventional root canal treatment.
-
Citations
Citations to this article as recorded by- Effect of chitosan medicaments loaded with green-synthesized silver nanoparticles on basic fibroblast growth factor release from infected dentin
Dilek Hancerliogullari, Zehra Gun Gok, Nebahat Aytuna Cerci, Eray Ceylanoglu, Bengisu Ozturk, Ozum Hekim Harput, Sevda Durust Baris, Filiz Kiper, Ali Erdemir
Odontology.2026; 114(3): 1593. CrossRef - The Role and Efficacy of Scaffolds in Regenerative Endodontics: A Survey of Current Practices and Perspective among Clinicians: A Questionnaire-based Study
Minusha Mohanan, Shabna Moyin, Shamsheer Thayyil, Anju Balachandran, Mary Elizabeth Nellickapalley Jacob, Koroth Valappil Harsha
Conservative Dentistry and Endodontic Journal.2026; 8(1): 10. CrossRef - Evaluation of Regenerative Endodontic Therapy in Young Permanent Teeth with Pulp Necrosis: A Retrospective Study
Işıl Özgül Kalyoncu, Ayşe Nur Sadıkoğlu, Figen Eren Giray, Betul Kargul
Current Research in Dental Sciences.2026; 36(2): 163. CrossRef - Regeneration Versus Granulation Tissue Healing in a Hopeless Mature Mandibular Molar Post-Endodontic Management: A 40-Month Follow-Up Case Report
Elhassan Hassanein, Petra Gierthmuehlen, Almaha S. Algazlan, Dalia Kaisarly, Moataz Elgezawi
Dentistry Journal.2026; 14(4): 243. CrossRef - The outcome of pulp revascularization of necrotic mature permanent teeth with periapical lesions using platelet-rich fibrin versus induced bleeding: a prospective preliminary randomized clinical trial
Lama Awawdeh, Bushra Almesleh, Hanan Hammouri, Aladdin Al-Qudah
Clinical Oral Investigations.2026;[Epub] CrossRef - Regenerative potential of concentrated growth factor compared to platelet-rich fibrin in treatment of necrotic mature teeth: a randomized clinical trial
Taghreed Salah, Wael Hussein, Heba Abdelkafy
BDJ Open.2025;[Epub] CrossRef - Efficacy of Pulp Revascularization in the Treatment of Apical Periodontitis in Mature Necrotic Teeth: An Umbrella Review
Wanderson Limeira de Sousa Barbosa, Luiz Renato Paranhos, Márcia Valente de Brito Dantas, Rômulo Dias Jesuino, João Marcos da Costa Ribeiro, Walbert A. Vieira, Felipe de Souza Matos
Australian Endodontic Journal.2025; 51(2): 495. CrossRef - Clinical and radiographic outcomes of non-surgical retreatment of mature maxillary incisors using two regenerative endodontic techniques in adolescents: a 24-month randomized clinical trial
Ahmad Abdel Hamid Elheeny, Sherif Shafik EL Bahnasy, Yassmin Mohamed ElMakawi, Mohammed Turky, Eman Farouk Ahmed, Norhan Khaled Omar Wahba
BDJ Open.2025;[Epub] CrossRef - Revolutionizing Endodontics: Innovative Approaches for Treating Mature Teeth With Closed Apices and Apical Lesions: A Report of Two Cases
Claudia Brizuela, Gastón Meza, Maroun Khoury
Journal of Endodontics.2024; 50(5): 596. CrossRef - Current Aspects of Regenerative Endodontics: A Systematic Review
A. V. Mitronin, K. A. Archakov, D. A. Ostanina, Yu. A. Mitronin, T. V. Khizrieva
Endodontics Today.2024; 21(4): 287. CrossRef - Correlation between pulp sensibility and magnetic resonance signal intensity following regenerative endodontic procedures in mature necrotic teeth- a retrospective cohort study
Noha Mohamed El-Kateb, Amr Mohamed Abdallah, Rania Noaman ElBackly
BMC Oral Health.2024;[Epub] CrossRef - Influence of periapical lesion size on healing outcome following regenerative endodontic procedures: a clinical investigation
Noha Mohamed El Kateb, Mahmoud Mostafa Fata
Oral Radiology.2022; 38(4): 480. CrossRef - Do alternative scaffolds used in regenerative endodontics promote better root development than that achieved with blood clots?
Letícia de Araújo, Taynara Santos Goulart, Ana Clara Kuerten Gil, Daniela Peressoni Vieira Schuldt, Beatriz Serrato Coelho, Daniela de Rossi Figueiredo, Lucas da Fonseca Roberti Garcia, Josiane de Almeida
Brazilian Dental Journal.2022; 33(2): 22. CrossRef - Endodontic Regenerative Procedures in Necrotic Adult Teeth
Sara Garrido-Parada, Pablo Castelo-Baz, Nancy Feijoo-Pato, José Gaviño-Orduña, Benjamín Martín-Biedma
Applied Sciences.2022; 12(9): 4212. CrossRef - Combined conventional and regenerative treatment in molars with coexistent closed and open apices: A case series
Zafer C. Cehreli, Gizem Erbas Unverdi, Pinar Eymirli, Irem Mergen, Ezgihan Arslan, Gulce Esenturk
Australian Endodontic Journal.2022; 48(1): 197. CrossRef - Regenerative Endodontic Procedures for the Treatment of Necrotic Mature Teeth with Apical Periodontitis: A Systematic Review and Meta-analysis of Randomized Controlled Trials
Antonios Glynis, Federico Foschi, Ismini Kefalou, Despina Koletsi, Giorgos N. Tzanetakis
Journal of Endodontics.2021; 47(6): 873. CrossRef - Different Approaches to the Regeneration of Dental Tissues in Regenerative Endodontics
Anna M. Krupińska, Katarzyna Skośkiewicz-Malinowska, Tomasz Staniowski
Applied Sciences.2021; 11(4): 1699. CrossRef - Quantitative Assessment of Intracanal Regenerated Tissues after Regenerative Endodontic Procedures in Mature Teeth Using Magnetic Resonance Imaging: A Randomized Controlled Clinical Trial
Noha Mohamed El-Kateb, Rania Noaman El-Backly, Wessam Mohamed Amin, Amr Mohamed Abdalla
Journal of Endodontics.2020; 46(5): 563. CrossRef
- Effect of chitosan medicaments loaded with green-synthesized silver nanoparticles on basic fibroblast growth factor release from infected dentin
- 3,432 View
- 35 Download
- 18 Crossref
Research Articles
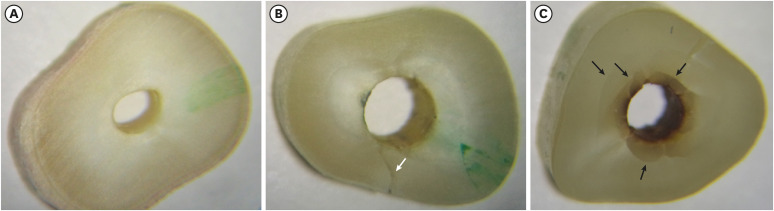
- Light-emitting diode assessment of dentinal defects: the role of presumed extraction forces
- Marcelo Santos Coelho, Steven J. Card, Peter Z. Tawil
- Restor Dent Endod 2017;42(3):232-239. Published online July 24, 2017
- DOI: https://doi.org/10.5395/rde.2017.42.3.232
-
Abstract
PDFPubReaderePub
Objectives The evaluation of iatrogenic dentinal defects in extracted teeth may be influenced by extraction forces and prolonged dry times. The purpose of this study was to compare the presence of dentinal defects in freshly extracted, periodontally compromised teeth with those in a group of teeth with uncontrolled extraction forces and storage time.
Materials and Methods The experimental group consisted of eighteen roots obtained from teeth extracted due to periodontal reasons with class II or III mobility. They were kept in saline and sectioned within 1 hour following extraction. The control group consisted of matched root types obtained from an anonymous tooth collection, consistent with previous dentinal defect studies. The slices were obtained at 3, 6, and 9 mm from the apex. The imaging process exposed all specimens to no more than 60 seconds of dry time. The × 12.8 magnification was used for the 9 mm slices and × 19.2 magnification for the 3 mm and 6 mm slices under light-emitting diode (LED) transillumination. The root canal spaces and periodontal tissues were masked to minimize extraneous factors that might influence the evaluators. Chi-square test was used for statistical analysis.
Results Dentinal defects were detected in 17% of the experimental group teeth, compared to 61% of control teeth (
p = 0.015).Conclusions LED transillumination assessment of freshly extracted roots with class II or III mobility showed smaller number of dentinal defects than roots with uncontrolled storage time and extraction forces. The use of freshly extracted roots with mobility should be considered for future dental defect assessment studies.
-
Citations
Citations to this article as recorded by- Dentinal microcracks on freshly extracted teeth: the impact of the extraction technique
F. N. Arashiro, G. De‐Deus, F. G. Belladonna, D. M. Cavalcante, M. S. Coelho, E. J. N. L. Silva, K. F. S. Pereira, P. G. da Silva, R. T. Lopes, E. M. Souza
International Endodontic Journal.2020; 53(4): 440. CrossRef - The relationship between the storage methods and the formation of dentinal defects (cracks)
Fábio Nakao ARASHIRO, Michelle Tavares Galotto NANTES, Pedro Gregol da SILVA, Key Fabiano Souza PEREIRA, Muryllo Eduardo Sales dos SANTOS
RGO - Revista Gaúcha de Odontologia.2019;[Epub] CrossRef - Effect of Reciproc blue, XP‐endo shaper, and WaveOne gold instruments on dentinal microcrack formation: A micro‐computed tomographic evaluation
Zeliha Uğur Aydın, Neslihan Büşra Keskin, Taha Özyürek
Microscopy Research and Technique.2019; 82(6): 856. CrossRef - Periapical Microsurgery: Do Root Canal–retreated Teeth Have More Dentinal Defects?
Peter Z. Tawil, Elisa K. Arnarsdottir, Ceib Phillips, Sigurdur R. Saemundsson
Journal of Endodontics.2018; 44(10): 1487. CrossRef - Root-originating dentinal defects: methodological aspects and clinical relevance
Peter Zahi Tawil, Elisa Kristin Arnarsdottir, Marcelo Santos Coelho
Evidence-Based Endodontics.2017;[Epub] CrossRef
- Dentinal microcracks on freshly extracted teeth: the impact of the extraction technique
- 2,053 View
- 4 Download
- 5 Crossref
- The use of auxiliary devices during irrigation to increase the cleaning ability of a chelating agent
- Marina Carvalho Prado, Fernanda Leal, Renata Antoun Simão, Heloisa Gusman, Maíra do Prado
- Restor Dent Endod 2017;42(2):105-110. Published online February 3, 2017
- DOI: https://doi.org/10.5395/rde.2017.42.2.105
-
Abstract
PDFPubReaderePub
Objectives This study investigated the cleaning ability of ultrasonically activated irrigation (UAI) and a novel activation system with reciprocating motion (EC, EasyClean, Easy Equipamentos Odontológicos) when used with a relatively new chelating agent (QMix, Dentsply). In addition, the effect of QMix solution when used for a shorter (1 minute) and a longer application time (3 minutes) was investigated.
Materials and Methods Fifty permanent human teeth were prepared with K3 rotary system and 6% sodium hypochlorite. Samples were randomly assigned to five groups (
n = 10) according to the final irrigation protocol: G1, negative control (distilled water); G2, positive control (QMix 1 minute); G3, QMix 1 minute/UAI; G4, QMix 1 minute/EC; G5, QMix 3 minutes. Subsequently the teeth were prepared and three photomicrographs were obtained in each root third of root walls, by scanning electron microscopy. Two blinded and pre-calibrated examiners evaluated the images using a four-category scoring system. Data were statistically analyzed using Kruskal-Wallis and Dunn tests (p < 0.05).Results There were differences among groups (
p < 0.05). UAI showed better cleaning ability than EC (p < 0.05). There were improvements when QMix was used with auxiliary devices in comparison with conventional irrigation (p < 0.05). Conventional irrigation for 3 minutes presented significantly better results than its use for 1 minute (p < 0.05).Conclusions QMix should be used for 1 minute when it is used with UAI, since this final irrigation protocol showed the best performance and also allowed clinical optimization of this procedure.
-
Citations
Citations to this article as recorded by- Comparative Evaluation of Different Methods of Activation of Chelating Solution for Smear Layer Removal in the Apical Portion of the Root Canal Using a Scanning Electron Microscopy: An In Vitro Study
Mrunal B Alhat, Sudha B Mattigatti, Rushikesh R Mahaparale, Kapil D Wahane, Apoorva Jadhav
Cureus.2024;[Epub] CrossRef - The Impact of Laser-Activated and Conventional Irrigation Techniques on Sealer Penetration into Dentinal Tubules
Dilara Koruk, Fatma Basmacı, Dilan Kırmızı, Umut Aksoy
Photobiomodulation, Photomedicine, and Laser Surgery.2022; 40(8): 565. CrossRef - Utilização dos atuais métodos de agitação de soluções endodônticas no canal radicular
Lívia Rodrigues Schneider, Larissa Giovanella
Revista Científica Multidisciplinar Núcleo do Conhecimento.2022; : 135. CrossRef - Smear layer removal by passive ultrasonic irrigation and 2 new mechanical methods for activation of the chelating solution
Ricardo Machado, Isadora da Silva, Daniel Comparin, Bianca Araujo Marques de Mattos, Luiz Rômulo Alberton, Ulisses Xavier da Silva Neto
Restorative Dentistry & Endodontics.2021;[Epub] CrossRef - Proteomic analysis of human dental pulp in different clinical diagnosis
Poliana Amanda Oliveira Silva, Stella Maris de Freitas Lima, Mirna de Souza Freire, André Melro Murad, Octávio Luiz Franco, Taia Maria Berto Rezende
Clinical Oral Investigations.2021; 25(5): 3285. CrossRef - Effect of QMix irrigant in removal of smear layer in root canal system: a systematic review of in vitro studies
Margaret Soo Yee Chia, Abhishek Parolia, Benjamin Syek Hur Lim, Jayakumar Jayaraman, Isabel Cristina Celerino de Moraes Porto
Restorative Dentistry & Endodontics.2020;[Epub] CrossRef - The effect of 17% EDTA and QMiX ultrasonic activation on smear layer removal and sealer penetration: ex vivo study
Felipe de Souza Matos, Fabrício Rutz da Silva, Luiz Renato Paranhos, Camilla Christian Gomes Moura, Eduardo Bresciani, Marcia Carneiro Valera
Scientific Reports.2020;[Epub] CrossRef - Micro-CT evaluation of different final irrigation protocols on the removal of hard-tissue debris from isthmus-containing mesial root of mandibular molars
Emmanuel João Nogueira Leal Silva, Carla Rodrigues Carvalho, Felipe Gonçalves Belladonna, Marina Carvalho Prado, Ricardo Tadeu Lopes, Gustavo De-Deus, Edson Jorge Lima Moreira
Clinical Oral Investigations.2019; 23(2): 681. CrossRef
- Comparative Evaluation of Different Methods of Activation of Chelating Solution for Smear Layer Removal in the Apical Portion of the Root Canal Using a Scanning Electron Microscopy: An In Vitro Study
- 2,161 View
- 11 Download
- 8 Crossref
- Effects of canal enlargement and irrigation needle depth on the cleaning of the root canal system at 3 mm from the apex
- Ho-Jin Moon, Chan-Ui Hong
- Restor Dent Endod 2012;37(1):24-28. Published online March 2, 2012
- DOI: https://doi.org/10.5395/rde.2012.37.1.24
-
Abstract
PDFPubReaderePub
Objectives The aim of this study was to test the hypothesis, that the effectiveness of irrigation in removing smear layer in the apical third of root canal system is dependent on the depth of placement of the irrigation needle into the root canal and the enlargement size of the canal.
Materials and Methods Eighty sound human lower incisors were divided into eight groups according to the enlargement size (#25, #30, #35 and #40) and the needle penetration depth (3 mm from working length, WL-3 mm and 9 mm from working length, WL-9 mm). Each canal was enlarged to working length with Profile.06 Rotary Ni-Ti files and irrigated with 5.25% NaOCl. Then, each canal received a final irrigation with 3 mL of 3% EDTA for 4 min, followed by 5 mL of 5.25% NaOCl at different level (WL-3 mm and WL-9 mm) from working length. Each specimen was prepared for the scanning electron microscope (SEM). Photographs of the 3mm area from the apical constriction of each canal with a magnification of ×250, ×500, ×1,000, ×2,500 were taken for the final evaluation.
Results Removal of smear layer in WL-3 mm group showed a significantly different effect when the canal was enlarged to larger than #30. There was a significant difference in removing apical smear layer between the needle penetration depth of WL-3 mm and WL-9 mm.
Conclusions Removal of smear layer from the apical portion of root canals was effectively accomplished with apical instrumentation to #35/40 06 taper file and 3 mm needle penetration from the working length.
-
Citations
Citations to this article as recorded by- Numerical Evaluation of Flow Pattern for Root Canal Irrigation Including icrobubbles
Joon Hyun Kim, Chan U Lee, Inwhan Lee, Jaeyong Sung
Journal of the Korean Society of Manufacturing Technology Engineers.2023; 32(5): 251. CrossRef
- Numerical Evaluation of Flow Pattern for Root Canal Irrigation Including icrobubbles
- 1,847 View
- 6 Download
- 1 Crossref
 First
First Prev
Prev

