
Articles
- Page Path
- HOME > Restor Dent Endod > Volume 43(3); 2018 > Article
- Case Report Revitalization of necrotic mature permanent incisors with apical periodontitis: a case report
-
Emre Nagas1
 , M. Ozgur Uyanik1, Zafer C. Cehreli2
, M. Ozgur Uyanik1, Zafer C. Cehreli2 -
Restor Dent Endod 2018;43(3):e31.
DOI: https://doi.org/10.5395/rde.2018.43.e31
Published online: July 5, 2018
1Department of Endodontics, Faculty of Dentistry, Hacettepe University, Ankara, Turkey.
2Department of Pediatric Dentistry, Faculty of Dentistry, Hacettepe University, Ankara, Turkey.
- Correspondence to Emre Nagas, DDS, PhD. Associate Professor, Department of Endodontics, Faculty of Dentistry, Hacettepe University, Sihhiye, Ankara 06100, Turkey. emrenagas@yahoo.com, enagas@hacetttepe.edu.tr
• Received: March 16, 2018 • Accepted: June 4, 2018
Copyright © 2018. The Korean Academy of Conservative Dentistry
This is an Open Access article distributed under the terms of the Creative Commons Attribution Non-Commercial License (https://creativecommons.org/licenses/by-nc/4.0/) which permits unrestricted non-commercial use, distribution, and reproduction in any medium, provided the original work is properly cited.
- 3,345 Views
- 34 Download
- 18 Crossref
Abstract
- Despite considerable focus on the regenerative endodontic treatment of immature teeth with necrotic infected pulps and apical periodontitis, little data exist with regard to its possible implementation in necrotic permanent teeth with complete apical and radicular development. The present report describes the procedures and outcome of a regenerative endodontic treatment approach in 2 previously-traumatized incisors with closed apex with apical periodontitis. A 2-visit treatment procedure was employed. At initial visit, the root canals were copiously irrigated, followed by placement of a triple antibiotic paste containing ciprofloxacin, metronidazole, and clindamycin into the root canals. After 4 weeks, the antibiotic paste was removed, and apical bleeding was initiated with size 10 hand files beyond the apices. The root canals were coronally sealed with mineral trioxide aggregate, and the access cavities were restored with bonded resin composite. At post-operative 60 months, both teeth were remained asymptomatic, with the recall radiographs showing complete resolution of apical radiolucency and reestablishment of periradicular tissues. In both teeth, the dimensions of root space remained unchanged as verified by image analysis. The revitalization protocol utilizing root canal disinfection and induced apical bleeding in necrotic, closed-apex incisors may offer a clinically acceptable alternative to conventional root canal treatment.
INTRODUCTION
Regenerative endodontic procedures have become a viable therapeutic approach to save or extend the life of necrotic, immature teeth, as well as to preserve the alveolar bone and maintain optimal function in the long term [1,2]. Currently, the common clinical protocol for regenerative endodontic therapies includes disinfection of the root canal with an antibiotic paste for several weeks, followed by evoked apical bleeding to form a blood clot containing stem cells from the apical papilla (SCAP) and growth factors released from platelets [3,4,5]. Coupled with the release of growth factors sequestered in root dentin [6,7], this blood clot is thought to act as a scaffold to promote cellular growth and differentiation, followed by generation or ingrowth of tissue in the root canal space [8].
In contrast to a growing body of published regenerative endodontic cases in immature necrotic teeth, only one recent report [9] has attempted a modified regenerative endodontic procedure for mature necrotic permanent teeth since the initial reports by Östby [10] and Nygaard-Ostby and Hjortdal [11]. This limitation might be due to concerns in achieving adequate bleeding and subsequent angiogenesis through a narrow apical pathway [12], as well as the age-related decline in the amount and function of stem/progenitor cells that could be delivered into the empty canal space [9,13]. However, the presence of a wide-open apex and abundance of stem/progenitor cells residing in the periapical region do not necessarily warrant successful and predictable treatment outcomes, as evidenced by different tissue responses in immature permanent teeth [14].
The ultimate goals in the regenerative endodontic treatment of immature necrotic teeth are continuation of root development and regeneration of functional pulp tissue [15]. These goals partially apply to that of mature permanent teeth, since the latter already possess normal root dimensions (i.e., width and length) and a physiologic apical closure. Thus, implementation of current biologically-based treatment procedures might be a logical step toward achieving vital tissue formation in the root canal space of necrotic mature teeth. The present report describes the procedures and the outcome of a regenerative endodontic treatment approach in 2 previously-traumatized, necrotic mature incisors with apical periodontitis.
CASE REPORT
A healthy, 21-year-old female was referred to the Department of Endodontics for evaluation of teeth #21 and #22. Reportedly, the incisors had been traumatized in an accident at the age of 14, but the patient and parents did not seek dental treatment owing to the absence of tooth fracture or pain. Over the years, the teeth remained asymptomatic without discoloration, and more recently, presented with intermittent pain. Clinically, both tooth crowns were intact, had physiologic mobility and probing depths (< 3 mm), and showed little sensitivity to percussion. There were no signs of swelling or sinus tracts. Both teeth were non-responsive to a cold test (Endo-Ice, Coltene/Whaledent, Altstätten, Switzerland) and electric pulp test (Parkell Inc., Farmingdale, NY, USA), while the contralateral teeth responded positively to both tests. Radiographic examination revealed well-developed roots with closed apices and a large periradicular radiolucency involving both incisors (Figure 1). On the basis of clinical and radiographic findings, a diagnosis of pulp necrosis and symptomatic apical periodontitis was made. A biologically based endodontic treatment plan was considered, and possible treatment outcomes and applicability of conventional endodontic treatment in case of failure were thoroughly discussed with the patient. Following the patient's approval and written consent, the treatment was initiated at the same visit.
Figure 1
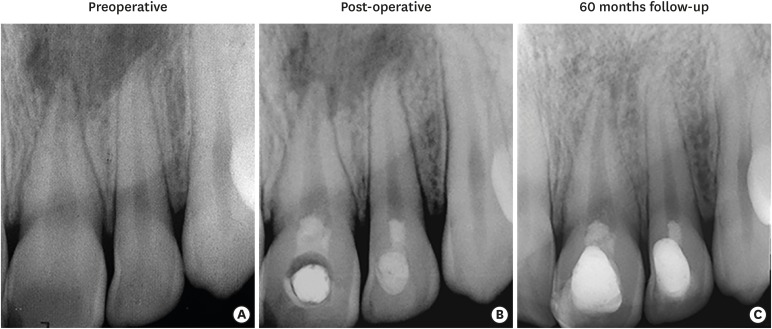
Preoperative (A), post-operative (B), and 60-month recall (C) radiographs of the patient. The post-operative and follow-up radiographs were corrected by using the TurboReg plug-in as a preparation for quantitative assessment of changes in root dimensions by using Image-J.
The teeth were anesthetized using 2% lidocaine with 1:100,000 epinephrine and isolated with rubber dam. Following endodontic access, a hemorrhagic, purulent exudate was observed. The canals were gently irrigated with approximately 20 mL of 5.25% NaOCl without instrumentation, and thereafter with 10 mL of saline. After drying the root canals with sterile paper points, a triple antibiotic paste (TAP) containing ciprofloxacin, metronidazole, and clindamycin (each 100 mg) was freshly prepared by mixing with sterile distilled water to a thin, creamy paste. The antibiotic paste was placed into the root canals using a lentulo spiral, and the access cavities were sealed with sterile cotton pellet and glass ionomer cement (Ketac Molar, 3M ESPE, Seefeld, Germany). The patient was recalled 4 weeks later.
Both teeth were asymptomatic at the second appointment. The teeth were anesthetized with 2% mepivacaine (Citanest, AstraZeneca, London, UK) without a vasoconstrictor followed by rubber dam isolation, and the antibiotic paste in the canal was removed by copious irrigation with 5.25% NaOCl [16,17], and thereafter with 10 mL sterile distilled water. The root canals received a final rinse of 17% ethylenediaminetetraacetic acid for 1 minute, and the excess was removed with sterile paper points. Apical bleeding was induced by gentle instrumentation with sterile size 10 K-files 1–2 mm beyond the apices. After formation of a blood clot approximately 3 mm below the cement-enamel junction, ProRoot MTA (Dentsply Tulsa Dental, Tulsa, OK, USA) was mixed with sterile distilled water and carefully placed above the blood clot. Finally, a wet cotton pellet was placed over the MTA, and the access cavity was temporarily restored with conventional glass ionomer cement (Kavitan Plus, SpofaDental, Jičín, Czech Republic). The teeth were restored with acid-etch resin composite (3M ESPE Dental Products, St. Paul, MN, USA) 1 week later.
At 1-month follow-up, the teeth were asymptomatic and showed decreased periradicular radiolucency (Figure 1B). The patient was recalled every six months for clinical and radiographic evaluations. Complete resolution of the radiolucency, and regeneration of the periradicular tissues were evident at the 60-month follow-up radiograph (Figure 1C). Clinically, both teeth were asymptomatic with no sensitivity to percussion and palpation. As with the initial visit, the teeth were non-responsive to the cold test and the electric pulp test. To examine possible changes in root and root space dimensions, the radiographs were subjected to image analysis using Image-J software (V.1.44p, National Institutes of Health, Bethesda, MD, USA) as described previously [18,19]. Using the preoperative radiograph as the source image, the recall and final radiographs were digitally aligned with the TurboReg plug-in (Biomedical Imaging Group, Swiss Federal Institute of Technology, Lausanne, Switzerland), followed by linear measurements in Image-J [18,19]. The results of the measurements showed that the dimensions of the root space had remained unchanged during the 60-month follow-up period.
DISCUSSION
Revascularization is essential in both wound healing and the development of vital tissue in the root canal space [4,20,21]. It has been reported that the size of the apical foramen could be a critical factor to promote revascularization, with a radiographic apical width of 1 mm or greater offering greater chance for cell migration and proliferation [12]. It should be noted; however, this conclusion was based on long-term follow-up of autotransplanted teeth without evoked apical bleeding [12], which may be a critical step in the revascularization phase of regenerative endodontic treatment in mature necrotic teeth [9]. A recent study using an animal model showed that an apical width of as small as 0.32 mm could be sufficient to permit ingrowth of vital tissue in the canal space [22]. With extreme caution in extrapolating results of animal experimentation to the clinical situation, it is logical to assume that the apical diameters of mature central and lateral incisors, which are greater than 0.32 mm (approximately 0.425 mm, 0.369 mm, respectively) [23], may offer a suitable dimension for promotion of angiogenesis, and that passing the files beyond the apex of necrotic mature teeth might be a practical method to further enlarge the apical diameter as well as to evoke apical bleeding, which both can enhance revascularization [9,24].
Although the exact nature of tissue formed in the canal of revascularized teeth is yet unknown, results of recent case reports involving histologic analysis of revascularized teeth [25,26,27], and the resemblance of their findings with those obtained in the animal model [28] strongly suggest that the tissue within the pulp space is not functional pulp tissue, but rather a vascular, nonspecific vital tissue [29], comprised of both connective and hard tissue components [25,26,27,28,29]. Based on these observations, the generic term ‘revitalization’ has been suggested to better describe the technique and the outcome of currently-employed regenerative endodontic procedures [29,30]. Compared with necrotic immature teeth, the revitalization procedure of mature teeth may encounter additional challenges, owing to the scarcity or absence of SCAP, which are thought to play an important role for pulp/dentin regeneration in immature teeth [31]. According to Paryani and Kim [9], periodontal ligament stem cells, bone marrow mesenchymal stem cells, and surviving dental pulp stem cells residing around the root apex of mature necrotic teeth may initiate vital tissue growth when migration of these cells into the root canal are facilitated by evoked apical bleeding using gentle overinstrumentation. Their assumptions may be justified to some extent by the successful clinical and radiographic outcome of their case series involving closed-apex teeth of young patients (11 and 14 years old) [9]. Further, the observation of positive response to cold and electric pulp tests in one of their cases may suggest that some vital innervated tissue still existed within the root canal, and became produced by reestablishment of vascular support over the time [15]. Unlike those patients, the present case utilized the revitalization procedure in the closed-apex teeth of an older individual (21 years old). Since the teeth had been traumatized 7 years ago, it is highly unlikely that any vital tissue still existed in the root canal. Thus, if tissue ingrowth did take place in the canal space, it was probably the result of the migration of cells capable of revitalization through evoked apical bleeding and the maintenance of the blood clot, which provided sufficient scaffold for replacement of vital tissue over the long term [29]. A recent animal study on closed-apex teeth with apical periodontitis [32] showed that vital tissue formation can take place with a promising success rate (approximately 72%) in the presence of an induced blood clot. In addition, the outcome of this regenerative approach is not inferior to that obtained using an induced blood clot combined with platelet-rich plasma, bone marrow, or both.
Disinfection of the root canal space is a critical step in the regenerative endodontic treatment of necrotic permanent teeth. Although TAP may eliminate all possible bacteria from apical periodontitis, an undesirable side effect of the minocycline (a semi-synthetic tetracycline) was tooth discoloration. More recently, clindamycin has been substituted with minocycline because its spectrum of activity without causing discoloration [33]. Therefore, in the present case, a TAP consisting ciprofloxacin, metronidazole, and clindamycin was used, since combination antibiotics can effectively disinfect uninstrumented root canals [33]. It has been shown that high concentrations of TAP have a detrimental effect on stem cell survival [34], necessitating the use of diluted concentrations of antibiotics. Here, the antibiotic paste was applied as a very thin mixture, but it is still questionable whether the concentration of antibiotics in this consistency may prevent their possible adverse effects, particularly in mature permanent teeth of older patients where the smaller number and type of stem/progenitor cells are available. It was, however, evident that the TAP was effective in initiating the healing of the periradicular infection.
An ideal endodontic treatment is incomplete without prevention of reinfection by creating a bacteria-tight coronal seal. In regenerative endodontic procedures, this is commonly accomplished by placement of MTA as a pulp space barrier, followed by adhesive resin-based restorations. In the present case, the absence of pulpal and periapical complications at 60 months may partially be attributed to the successful coronal seal, although the longevity of this effect is yet to be demonstrated. A recent histologic analysis of an extracted revitalized premolar has shown that the ability of MTA in resisting bacterial penetration is questionable when the final adhesive restoration fails [27].
Although this case report shows a successful outcome of the revitalization protocol in mature permanent teeth, in the absence of histologic evidence, many issues remain to be clarified, with the possibility of an empty pulp space being the most important one. A revitalized tooth may remain asymptomatic with an empty canal space as long as a good coronal seal is maintained [29,35]. Coupled with the fact that development of root apex is possible in the absence of regenerated pulp tissue [29,35], the clinical and radiographic success of many revitalization cases may not be easily attributed to regeneration of a functional pulp or pulp-like tissue. Thus, until more effective regenerative procedures become employed in the routine, the outcome of current revitalization protocols should be interpreted with caution.
CONCLUSIONS
Based on clinical and radiographic outcomes of the present case, it can be concluded that the revitalization protocol involving root canal disinfection and evoked bleeding by gentle instrumentation beyond the apex provided an acceptable alternative to conventional root canal therapy over the 60-month follow-up period.
-
Conflict of Interest: No potential conflict of interest relevant to this article was reported.
-
Author Contributions:
- 1. Law AS. Considerations for regeneration procedures. J Endod 2013;39:S44-S56.ArticlePubMed
- 2. Zhou R, Wang Y, Chen Y, Chen S, Lyu H, Cai Z, Huang X. Radiographic, histologic, and biomechanical evaluation of combined application of platelet-rich fibrin with blood clot in regenerative endodontics. J Endod 2017;43:2034-2040.ArticlePubMed
- 3. Banchs F, Trope M. Revascularization of immature permanent teeth with apical periodontitis: new treatment protocol? J Endod 2004;30:196-200.ArticlePubMed
- 4. Miller AA, Takimoto K, Wealleans J, Diogenes A. Effect of 3 bioceramic materials on stem cells of the apical papilla proliferation and differentiation using a dentin disk Model. J Endod 2018;44:599-603.ArticlePubMed
- 5. Lovelace TW, Henry MA, Hargreaves KM, Diogenes A. Evaluation of the delivery of mesenchymal stem cells into the root canal space of necrotic immature teeth after clinical regenerative endodontic procedure. J Endod 2011;37:133-138.ArticlePubMed
- 6. Sloan AJ, Smith AJ. Stimulation of the dentine-pulp complex of rat incisor teeth by transforming growth factor-beta isoforms 1–3 in vitro. Arch Oral Biol 1999;44:149-156.PubMed
- 7. Galler KM, D'Souza RN, Federlin M, Cavender AC, Hartgerink JD, Hecker S, Schmalz G. Dentin conditioning codetermines cell fate in regenerative endodontics. J Endod 2011;37:1536-1541.ArticlePubMed
- 8. Galler KM, Buchalla W, Hiller KA, Federlin M, Eidt A, Schiefersteiner M, Schmalz G. Influence of root canal disinfectants on growth factor release from dentin. J Endod 2015;41:363-368.ArticlePubMed
- 9. Paryani K, Kim SG. Regenerative endodontic treatment of permanent teeth after completion of root development: a report of 2 cases. J Endod 2013;39:929-934.ArticlePubMed
- 10. Östby BN. The role of the blood clot in endodontic therapy. An experimental histologic study. Acta Odontol Scand 1961;19:324-353.PubMed
- 11. Nygaard-Ostby B, Hjortdal O. Tissue formation in the root canal following pulp removal. Scand J Dent Res 1971;79:333-349.ArticlePubMed
- 12. Andreasen JO, Paulsen HU, Yu Z, Bayer T, Schwartz O. A long-term study of 370 autotransplanted premolars. Part II. Tooth survival and pulp healing subsequent to transplantation. Eur J Orthod 1990;12:14-24.ArticlePubMed
- 13. Van Zant G, Liang Y. The role of stem cells in aging. Exp Hematol 2003;31:659-672.ArticlePubMed
- 14. Chen MY, Chen KL, Chen CA, Tayebaty F, Rosenberg PA, Lin LM. Responses of immature permanent teeth with infected necrotic pulp tissue and apical periodontitis/abscess to revascularization procedures. Int Endod J 2012;45:294-305.ArticlePubMed
- 15. Hargreaves KM, Diogenes A, Teixeira FB. Treatment options: biological basis of regenerative endodontic procedures. J Endod 2013;39:S30-S43.ArticlePubMedPMC
- 16. Cotti E, Mereu M, Lusso D. Regenerative treatment of an immature, traumatized tooth with apical periodontitis: report of a case. J Endod 2008;34:611-616.ArticlePubMed
- 17. Chueh LH, Huang GT. Immature teeth with periradicular periodontitis or abscess undergoing apexogenesis: a paradigm shift. J Endod 2006;32:1205-1213.ArticlePubMed
- 18. Bose R, Nummikoski P, Hargreaves K. A retrospective evaluation of radiographic outcomes in immature teeth with necrotic root canal systems treated with regenerative endodontic procedures. J Endod 2009;35:1343-1349.ArticlePubMed
- 19. Cehreli ZC, Isbitiren B, Sara S, Erbas G. Regenerative endodontic treatment (revascularization) of immature necrotic molars medicated with calcium hydroxide: a case series. J Endod 2011;37:1327-1330.ArticlePubMed
- 20. Folkman J, Shing Y. Angiogenesis. J Biol Chem 1992;267:10931-10934.ArticlePubMed
- 21. Zhang R, Cooper PR, Smith G, Nör JE, Smith AJ. Angiogenic activity of dentin matrix components. J Endod 2011;37:26-30.ArticlePubMed
- 22. Laureys WG, Cuvelier CA, Dermaut LR, De Pauw GA. The critical apical diameter to obtain regeneration of the pulp tissue after tooth transplantation, replantation, or regenerative endodontic treatment. J Endod 2013;39:759-763.ArticlePubMed
- 23. Mizutani T, Ohno N, Nakamura H. Anatomical study of the root apex in the maxillary anterior teeth. J Endod 1992;18:344-347.ArticlePubMed
- 24. Skoglund A. Pulpal changes in replanted and autotransplanted apicoectomized mature teeth of dogs. Int J Oral Surg 1981;10:111-121.ArticlePubMed
- 25. Martin G, Ricucci D, Gibbs JL, Lin LM. Histological findings of revascularized/revitalized immature permanent molar with apical periodontitis using platelet-rich plasma. J Endod 2013;39:138-144.ArticlePubMed
- 26. Shimizu E, Ricucci D, Albert J, Alobaid AS, Gibbs JL, Huang GT, Lin LM. Clinical, radiographic, and histological observation of a human immature permanent tooth with chronic apical abscess after revitalization treatment. J Endod 2013;39:1078-1083.ArticlePubMed
- 27. Becerra P, Ricucci D, Loghin S, Gibbs JL, Lin LM. Histologic study of a human immature permanent premolar with chronic apical abscess after revascularization/revitalization. J Endod 2014;40:133-139.ArticlePubMed
- 28. Wang X, Thibodeau B, Trope M, Lin LM, Huang GT. Histologic characterization of regenerated tissues in canal space after the revitalization/revascularization procedure of immature dog teeth with apical periodontitis. J Endod 2010;36:56-63.ArticlePubMed
- 29. Lenzi R, Trope M. Revitalization procedures in two traumatized incisors with different biological outcomes. J Endod 2012;38:411-414.ArticlePubMed
- 30. Torabinejad M, Turman M. Revitalization of tooth with necrotic pulp and open apex by using platelet-rich plasma: a case report. J Endod 2011;37:265-268.ArticlePubMed
- 31. Huang GT, Sonoyama W, Liu Y, Liu H, Wang S, Shi S. The hidden treasure in apical papilla: the potential role in pulp/dentin regeneration and bioroot engineering. J Endod 2008;34:645-651.ArticlePubMedPMC
- 32. Fayazi S, Takimoto K, Diogenes A. Comparative evaluation of chemotactic factor effect on migration and differentiation of stem cells of the apical papilla. J Endod 2017;43:1288-1293.ArticlePubMed
- 33. Windley W 3rd, Teixeira F, Levin L, Sigurdsson A, Trope M. Disinfection of immature teeth with a triple antibiotic paste. J Endod 2005;31:439-443.ArticlePubMed
- 34. Ruparel NB, Teixeira FB, Ferraz CC, Diogenes A. Direct effect of intracanal medicaments on survival of stem cells of the apical papilla. J Endod 2012;38:1372-1375.ArticlePubMed
- 35. Nosrat A, Li KL, Vir K, Hicks ML, Fouad AF. Is pulp regeneration necessary for root maturation? J Endod 2013;39:1291-1295.ArticlePubMed
REFERENCES
Tables & Figures
REFERENCES
Citations
Citations to this article as recorded by 
- Effect of chitosan medicaments loaded with green-synthesized silver nanoparticles on basic fibroblast growth factor release from infected dentin
Dilek Hancerliogullari, Zehra Gun Gok, Nebahat Aytuna Cerci, Eray Ceylanoglu, Bengisu Ozturk, Ozum Hekim Harput, Sevda Durust Baris, Filiz Kiper, Ali Erdemir
Odontology.2026; 114(3): 1593. CrossRef - The Role and Efficacy of Scaffolds in Regenerative Endodontics: A Survey of Current Practices and Perspective among Clinicians: A Questionnaire-based Study
Minusha Mohanan, Shabna Moyin, Shamsheer Thayyil, Anju Balachandran, Mary Elizabeth Nellickapalley Jacob, Koroth Valappil Harsha
Conservative Dentistry and Endodontic Journal.2026; 8(1): 10. CrossRef - Evaluation of Regenerative Endodontic Therapy in Young Permanent Teeth with Pulp Necrosis: A Retrospective Study
Işıl Özgül Kalyoncu, Ayşe Nur Sadıkoğlu, Figen Eren Giray, Betul Kargul
Current Research in Dental Sciences.2026; 36(2): 163. CrossRef - Regeneration Versus Granulation Tissue Healing in a Hopeless Mature Mandibular Molar Post-Endodontic Management: A 40-Month Follow-Up Case Report
Elhassan Hassanein, Petra Gierthmuehlen, Almaha S. Algazlan, Dalia Kaisarly, Moataz Elgezawi
Dentistry Journal.2026; 14(4): 243. CrossRef - The outcome of pulp revascularization of necrotic mature permanent teeth with periapical lesions using platelet-rich fibrin versus induced bleeding: a prospective preliminary randomized clinical trial
Lama Awawdeh, Bushra Almesleh, Hanan Hammouri, Aladdin Al-Qudah
Clinical Oral Investigations.2026;[Epub] CrossRef - Regenerative potential of concentrated growth factor compared to platelet-rich fibrin in treatment of necrotic mature teeth: a randomized clinical trial
Taghreed Salah, Wael Hussein, Heba Abdelkafy
BDJ Open.2025;[Epub] CrossRef - Efficacy of Pulp Revascularization in the Treatment of Apical Periodontitis in Mature Necrotic Teeth: An Umbrella Review
Wanderson Limeira de Sousa Barbosa, Luiz Renato Paranhos, Márcia Valente de Brito Dantas, Rômulo Dias Jesuino, João Marcos da Costa Ribeiro, Walbert A. Vieira, Felipe de Souza Matos
Australian Endodontic Journal.2025; 51(2): 495. CrossRef - Clinical and radiographic outcomes of non-surgical retreatment of mature maxillary incisors using two regenerative endodontic techniques in adolescents: a 24-month randomized clinical trial
Ahmad Abdel Hamid Elheeny, Sherif Shafik EL Bahnasy, Yassmin Mohamed ElMakawi, Mohammed Turky, Eman Farouk Ahmed, Norhan Khaled Omar Wahba
BDJ Open.2025;[Epub] CrossRef - Revolutionizing Endodontics: Innovative Approaches for Treating Mature Teeth With Closed Apices and Apical Lesions: A Report of Two Cases
Claudia Brizuela, Gastón Meza, Maroun Khoury
Journal of Endodontics.2024; 50(5): 596. CrossRef - Current Aspects of Regenerative Endodontics: A Systematic Review
A. V. Mitronin, K. A. Archakov, D. A. Ostanina, Yu. A. Mitronin, T. V. Khizrieva
Endodontics Today.2024; 21(4): 287. CrossRef - Correlation between pulp sensibility and magnetic resonance signal intensity following regenerative endodontic procedures in mature necrotic teeth- a retrospective cohort study
Noha Mohamed El-Kateb, Amr Mohamed Abdallah, Rania Noaman ElBackly
BMC Oral Health.2024;[Epub] CrossRef - Influence of periapical lesion size on healing outcome following regenerative endodontic procedures: a clinical investigation
Noha Mohamed El Kateb, Mahmoud Mostafa Fata
Oral Radiology.2022; 38(4): 480. CrossRef - Do alternative scaffolds used in regenerative endodontics promote better root development than that achieved with blood clots?
Letícia de Araújo, Taynara Santos Goulart, Ana Clara Kuerten Gil, Daniela Peressoni Vieira Schuldt, Beatriz Serrato Coelho, Daniela de Rossi Figueiredo, Lucas da Fonseca Roberti Garcia, Josiane de Almeida
Brazilian Dental Journal.2022; 33(2): 22. CrossRef - Endodontic Regenerative Procedures in Necrotic Adult Teeth
Sara Garrido-Parada, Pablo Castelo-Baz, Nancy Feijoo-Pato, José Gaviño-Orduña, Benjamín Martín-Biedma
Applied Sciences.2022; 12(9): 4212. CrossRef - Combined conventional and regenerative treatment in molars with coexistent closed and open apices: A case series
Zafer C. Cehreli, Gizem Erbas Unverdi, Pinar Eymirli, Irem Mergen, Ezgihan Arslan, Gulce Esenturk
Australian Endodontic Journal.2022; 48(1): 197. CrossRef - Regenerative Endodontic Procedures for the Treatment of Necrotic Mature Teeth with Apical Periodontitis: A Systematic Review and Meta-analysis of Randomized Controlled Trials
Antonios Glynis, Federico Foschi, Ismini Kefalou, Despina Koletsi, Giorgos N. Tzanetakis
Journal of Endodontics.2021; 47(6): 873. CrossRef - Different Approaches to the Regeneration of Dental Tissues in Regenerative Endodontics
Anna M. Krupińska, Katarzyna Skośkiewicz-Malinowska, Tomasz Staniowski
Applied Sciences.2021; 11(4): 1699. CrossRef - Quantitative Assessment of Intracanal Regenerated Tissues after Regenerative Endodontic Procedures in Mature Teeth Using Magnetic Resonance Imaging: A Randomized Controlled Clinical Trial
Noha Mohamed El-Kateb, Rania Noaman El-Backly, Wessam Mohamed Amin, Amr Mohamed Abdalla
Journal of Endodontics.2020; 46(5): 563. CrossRef
 ePub Link
ePub Link Cite
CiteRevitalization of necrotic mature permanent incisors with apical periodontitis: a case report
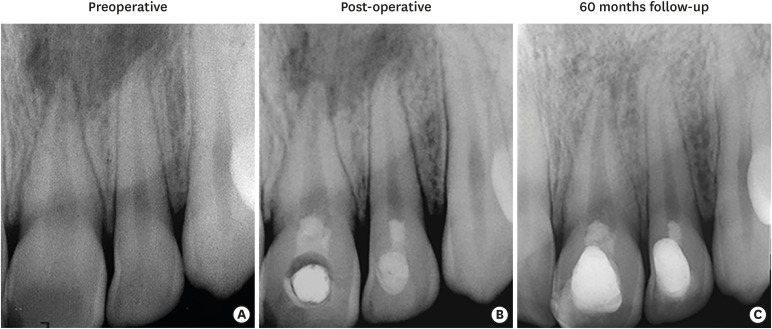
Figure 1 Preoperative (A), post-operative (B), and 60-month recall (C) radiographs of the patient. The post-operative and follow-up radiographs were corrected by using the TurboReg plug-in as a preparation for quantitative assessment of changes in root dimensions by using Image-J.
Figure 1
Revitalization of necrotic mature permanent incisors with apical periodontitis: a case report

