
Articles
- Page Path
- HOME > Restor Dent Endod > Volume 39(2); 2014 > Article
- Case Report Endodontic management of a mandibular second molar with radix entomolaris: a case report
- Rosaline Hannah1, Deivanayagam Kandaswamy1, Nachimuthu Jayaprakash2
-
2014;39(2):-136.
DOI: https://doi.org/10.5395/rde.2014.39.2.132
Published online: March 21, 2014
1Department of Conservative Dentistry and Endodontics, Faculty of Dental Sciences, Sri Ramachandra University, Porur, Chennai, India.
2Department of Conservative Dentistry and Endodontics, JKK Nataraja Dental College, Komarapalayam, Erode, India.
- Correspondence to: Rosaline Hannah, MDS. Associate Professor, Department of Conservative Dentistry and Endodontics, Faculty of Dental Sciences, Sri Ramachandra University, Porur, Chennai, Tamilnadu, India. TEL, +9841825456; FAX, +914445928643; hannahrosaline@gmail.com
• Received: October 18, 2013 • Accepted: January 30, 2014
©Copyights 2014. The Korean Academy of Conservative Dentistry.
This is an Open Access article distributed under the terms of the Creative Commons Attribution Non-Commercial License (http://creativecommons.org/licenses/by-nc/3.0/) which permits unrestricted non-commercial use, distribution, and reproduction in any medium, provided the original work is properly cited.
- 3,165 Views
- 22 Download
- 5 Crossref
Abstract
- The presence of radix entomolaris (RE) in a mandibular first molar is a common occurrence in certain ethnic groups, but the presence of RE in a mandibular second molar is a rare occurrence. In the present case, RE was identified from preoperative radiographs and confirmed using cone-beam computed tomography (CBCT). The access cavity was modified to locate the RE. Cleaning and shaping were performed with nickel-titanium rotary instruments. Obturation was completed with gutta-percha cones using AH Plus (Dentsply Detrey GmbH) as sealer. From the CBCT axial images, the RE was determined to have a Type III curvature by the De Moor classification, Type B separate RE by the Carlsen and Alexandersen classification, and radiographically, a Type i image by the Wang classification. The presence of RE in the mandibular second molar makes it essential to anticipate and treat the distolingual root canal. This case report highlights the usefulness of CBCT for assessing RE in the mandibular second molar, which can help the clinician in making a confirmatory diagnosis and assessing the morphology of the root canal.
Introduction
The major cause of failure of root canal therapy is the complexity of the root canal system. Mandibular molars can manifest with several anatomical variations, based on the internal and external morphology of the tooth.1 The most common variation in the mandibular first molar is the presence of a distolingual supernumerary root called radix entomolaris (RE), mentioned first by Carabelli, or mesiobuccal root (radix paramolaris).2,3 According to Manning, 22% of mandibular second molars have one root, 76% have 2 roots, and 2% have 3 roots. It has been noted that a patient's age, sex, and race have a direct relationship with second molar anatomy.4
The most common root morphology in the second molars of Indians was found to be the two-rooted morphology with three canals and Type IV and Type I canals predominating in the mesial and distal roots. These teeth showed both Mongoloid and Caucasian traits, with 8.98% of the teeth having three roots.5 The number of roots on the mandibular first molar is related to certain ethnic groups.6 The prevalence of RE in the mandibular first molar is 40% in those with Mongolian traits, 3.4 - 4.2% in Europeans, 3% in Africans and less than 5% in Indians and Eurasians.7,8,9,10,11,12,13 The introduction of cone-beam computed tomography (CBCT) has proved to be a valuable aid in endodontics because of its noninvasive nature and the ability to reconstruct an image three-dimensionally.14,15,16 CBCT is an appropriate tool for investigating the prevalence and morphologic features of distolingual roots in molars.17
Identification and treatment of RE is important because a missed canal remains a nidus for infection and can compromise the treatment outcome. This is a case report of RE of a mandibular second molar with three roots and four canals confirmed with the help of CBCT.
Case report
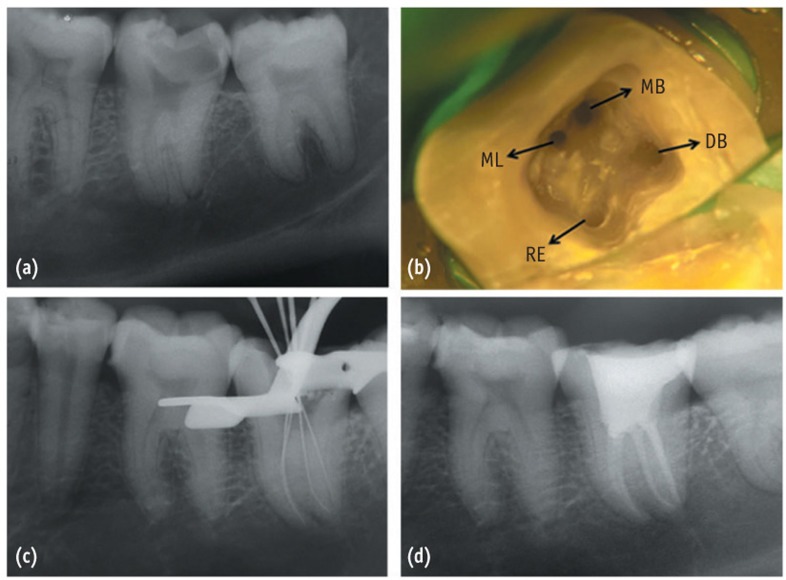
A 27-year-old male patient was referred to the Department of Conservative Dentistry and Endodontics with the complaint of spontaneous pain in the lower left posterior tooth for 3 days. The patient reported a history of intermittent pain for the past one month. On clinical examination, there was a carious mandibular left second molar (tooth #37). The tooth was tender to percussion and palpation did not reveal any tenderness. There was no mobility, and periodontal probing was within the physiological limits. A heat test resulted in intense lingering pain. The involved tooth showed a premature response to electronic pulp stimulation. The preoperative radiograph showed disto-occlusal radiolucency with pulpal involvement and periodontal space widening relative to the mesial and distal roots with an additional distolingual root (Figure 1a). Based on these findings, the tooth was diagnosed with dental caries with symptomatic irreversible pulpitis and apical periodontitis. Endodontic management was planned for the involved tooth.
An inferior alveolar nerve block was performed with 1.8 mL of 2% lidocaine containing 1 : 200,000 epinephrine (LOX 2%, Neon Laboratories Ltd., Mumbai, India) followed by buccal infiltration (1.8 mL) of the same anesthetic solution. The endodontic access cavity was prepared under rubber dam isolation. The conventional triangular outline form of the access cavity was modified into a trapezoidal form to place the distolingually located RE under the surgical operating microscope. A clinical examination was carried out with a DG16 endodontic explorer (Hu-Friedy, Chicago, IL, USA), and the surgical microscope (Seiler 600 series) revealed two mesial and two distal canal orifices. Coronal enlargements of the canals were performed with the nickel-titanium Protaper series orifice shaper (Dentsply Maillefer, Ballaigues, Switzerland) (Figure 1b). The canal length was determined with an electronic apex locator (Root ZX, Morita, Tokyo, Japan) and later confirmed using a radiograph (Figure 1c).
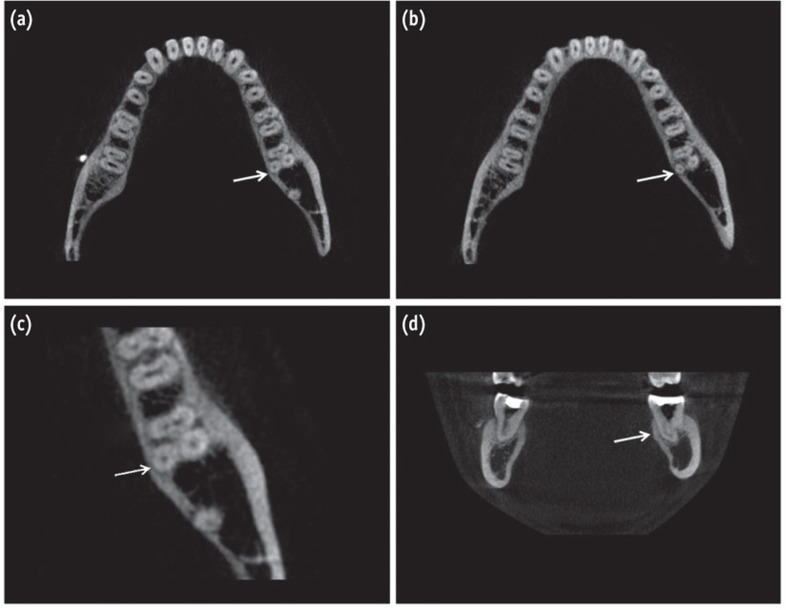
To confirm RE, CBCT imaging of the tooth (Kodak 9500, tube voltage: 90 kV, current: 10 mA, Carestream health Inc., Rochester, NY, USA) was performed after obtaining informed consent from the patient. The transverse, axial, and sagittal CBCT sections of the involved tooth were taken. The CBCT scan slices confirmed the presence of RE (Figures 2a - 2d). During the next visit, the patient was asymptomatic, and cleaning and shaping was done with Protaper nickel-titanium rotary instruments (Dentsply Maillefer) in a crown-down manner until F2. Irrigation was performed with 2.5% sodium hypochlorite solution, 17% EDTA, and 2% chlorhexidine digluconate solution as the final irrigant. Obturation was done with Protaper gutta-percha cones (Dentsply DeTrey Gmbh, Konstanz, Germany) and AH Plus resin sealer (Dentsply DeTrey Gmbh, Figure 1d). The access cavity was then restored with posterior composite resin, and the patient was advised to undergo full coverage restoration of the tooth.
Discussion
Accurate diagnosis of supernumerary roots like RE can contribute to the successful outcome of endodontic treatment.3 The presence of RE in the mandibular first molar has been extensively evaluated in the literature, but only a few studies have evaluated the morphology of mandibular second molars.4,5
Distolingually located RE varies from short conical extension to a mature root with normal length.3 Even though genetic factors may strongly influence the presence of RE, the etiology behind the formation of RE remains unknown.18 This unusual morphology of mandibular molars could be related to the penetrance of an atavistic gene or polygenetic system or due to external factors during odontogenesis.3,19
After identifying RE from the preoperative radiographs, the access cavity was modified into a trapezoidal outline in order to locate the distolingual RE, following previous studies in mandibular first molars.20,21
Based on the curvature of RE in the bucco-lingual orientation, De Moor et al. classified the RE into three types.21 A straight root/root canal refers to Type I. A root canal with initial curvature that continues as a straight root characterizes Type II, while a root canal with a curvature in the coronal third followed by a second curve from the middle third to the apical third forms Type III.21 The RE of our report has a Type III curve by the De Moor classification. CBCT sagittal images confirmed Type III curvature (Figure 2d). This Type III RE is more frequently found than any other anatomical type of RE in the mandibular first molar.22
To differentiate between separate and non-separate RE, Carlsen and Alexandersen classified RE into four types according to the location of the cervical part of the RE, Types A, B, C, and AC.23 In Type A, the distal part of the root has three cone-shaped macrostructures, a lingual, a medial, and a facial. Either the lingual structure is separate while the medial and facial structures are non-separate, or all three macrostructures are non-separate. In Type B, the distal part of the root has two cone-shaped macrostructures, lingual and facial ones of nearly the same size. The structures are either separate or non-separate. In Type C, the cervical part is located mesially. In Type AC, the cervical part is centrally located, between the mesial and distal root components.23 With the CBCT confirmation, our case comes under Type B RE (Figures 2a - 2c).
The recent radiographic classification of RE by Wang et al. comprises three types.22 Type i presents the most identifiable radiographic image. For a Type ii image, a large beam angulation is necessary mesially or distally for their identification. For a Type iii image, identification becomes extremely difficult because of the overlap of the adjacent distobuccal root.22 The present RE has a Type i image, as it can be identified from the preoperative radiograph (Figure 1a).
Type III RE can be detected most frequently in radiography as a Type i image. This is commonly mistaken as straight roots without any curvature leading to procedural errors.22 Furthermore, the limitations of periapical radiographs include anatomical noise, the two-dimensional nature of the resulting image and superimposition of structures.24,25 CBCT overcomes these limitations by enabling us to visualize the third dimension and also eliminating super-impositions. It also aids in-depth understanding of the true morphology of root canals.26,27 CBCT in the present case guides the assessment of severity of the curvature of the root canals, the number of roots and root canals, and identifying separated or unseparated root canals. Therefore, a cautious approach is required for clinicians in diagnosing and treating RE, which may present from mild to severe curvature leading to increased risk of shaping aberrations.
Conclusions
The presence of RE in the lower second molar makes it essential to anticipate and treat distolingual root canals to increase the longevity of the tooth. CBCT images can be used as an objective analytic tool to evaluate the nature of the root canal anatomy.
- 1. Schumacher C. Endodontic treatment of a mandibular first molar with radix entomolaris: a case report. ENDO (Lond Engl) 2008;2:301-304.
- 2. Carabelli G. Systematisches Handbuch Der Zahnheikunde. 2nd ed. Vienna: Braumuller and Seidel; 1844. p. 114.
- 3. Calberson FL, De Moor RJ, Deroose CA. The radix entomolaris and paramolaris: clinical approach in endodontics. J Endod 2007;33:58-63.ArticlePubMed
- 4. Manning SA. Root canal anatomy of mandibular second molars. Part I. Int Endod J 1990;23:34-39.ArticlePubMed
- 5. Neelakantan P, Subbarao C, Subbarao CV, Ravindranath M. Root and canal morphology of mandibular second molars in an Indian population. J Endod 2010;36:1319-1322.ArticlePubMed
- 6. Garg AK, Tewari RK, Kumar A, Hashmi SH, Agrawal N, Mishra SK. Prevalence of three-rooted mandibular permanent first molars among the Indian population. J Endod 2010;36:1302-1306.ArticlePubMed
- 7. Turner CG 2nd. Three-rooted mandibular first permanent molars and the question of American Indian origins. Am J Phys Anthropol 1971;34:229-241.ArticlePubMed
- 8. Loh HS. Incidence and features of three-rooted permanent mandibular molars. Aust Dent J 1990;35:434-437.ArticlePubMed
- 9. de Souza-Freitas JA, Lopes ES, Casati-Alvares L. Anatomic variations of lower first permanent molar roots in two ethnic groups. Oral Surg Oral Med Oral Pathol 1971;31:274-278.ArticlePubMed
- 10. Skidmore AE, Bjorndal AM. Root canal morphology of the human mandibular first molar. Oral Surg Oral Med Oral Pathol 1971;32:778-784.ArticlePubMed
- 11. Steelman R. Incidence of an accessory distal root on mandibular first permanent molars in Hispanic children. ASDC J Dent Child 1986;53:122-123.PubMed
- 12. Sperber GH, Moreau JL. Study of the number of roots and canals in Senegalese first permanent mandibular molars. Int Endod J 1998;31:117-122.ArticlePubMed
- 13. Tratman EK. Three-rooted lower molars in man and their racial distribution. Br Dent J 1938;64:264-274.
- 14. Tachibana H, Matsumoto K. Applicability of X-Ray computerized tomography in endodontics. Endod Dent Traumatol 1990;6:16-20.ArticlePubMed
- 15. Nair MK, Nair UP. Digital and advanced imaging in endodontics: a review. J Endod 2007;33:1-6.ArticlePubMed
- 16. Matherne RP, Angelopoulos C, Kulild JC, Tira D. Use of cone-beam computed tomography to identify root canal systems in vitro. J Endod 2008;34:87-89.ArticlePubMed
- 17. Song JS, Choi HJ, Jung IY, Jung HS, Kim SO. The prevalence and morphologic classification of distolingual roots in the mandibular molars in a Korean population. J Endod 2010;36:653-657.ArticlePubMed
- 18. Schäfer E, Breuer D, Janzen S. The prevalence of three-rooted mandibular permanent first molars in a German population. J Endod 2009;35:202-205.ArticlePubMed
- 19. Reichart PA, Metah D. Three-rooted permanent mandibular first molars in the Thai. Community Dent Oral Epidemiol 1981;9:191-192.ArticlePubMed
- 20. Gu Y, Lu Q, Wang H, Ding Y, Wang P, Ni L. Root canal morphology of permanent three-rooted mandibular first molars-part I: pulp floor and root canal system. J Endod 2010;36:990-994.ArticlePubMed
- 21. De Moor RJ, Deroose CA, Calberson FL. The radix entomolaris in mandibular first molars: an endodontic challenge. Int Endod J 2004;37:789-799.ArticlePubMed
- 22. Wang Q, Yu G, Zhou XD, Peters OA, Zheng QH, Huang DM. Evaluation of X-ray projection angulation for successful radix entomolaris diagnosis in mandibular first molars in vitro. J Endod 2011;37:1063-1068.ArticlePubMed
- 23. Carlsen O, Alexandersen V. Radix entomolaris: identification and morphology. Scand J Dent Res 1990;98:363-373.ArticlePubMed
- 24. Patel S, Dawood A, Whaites E, Pitt Ford T. New dimensions in endodontic imaging: part 1. Conventional and alternative radiographic systems. Int Endod J 2009;42:447-462.ArticlePubMed
- 25. Karanxha L, Kim HJ, Hong SO, Lee W, Kim PS, Min KS. Endodontic management of a C-shaped maxillary first molar with three independent buccal root canals by using cone-beam computed tomography. Restor Dent Endod 2012;37:175-179.ArticlePubMedPMC
- 26. Abella F, Patel S, Durán-Sindreu F, Mercadé M, Roig M. Mandibular first molars with disto-lingual roots: review and clinical management. Int Endod J 2012;45:963-978.ArticlePubMed
- 27. Lee MH, Ha JH, Jin MU, Kim YK, Kim SK. Endodontic treatment of maxillary lateral incisors with anatomical variations. Restor Dent Endod 2013;38:253-257.ArticlePubMedPMC
REFERENCES
Tables & Figures
REFERENCES
Citations
Citations to this article as recorded by 
- Three-Dimensional Observation and Classification of Root and Root Canal Morphology in Japanese Mandibular Third Molars
Tomoyuki Inose, Satoru Matsunaga, Norio Kasahara, Masashi Yamada, Shinichi Abe, Masahiro Furusawa
Journal of Hard Tissue Biology.2026; 35(1): 7. CrossRef - Endodontic Treatment of a Mandibular Second Molar Featuring Vertucci Type V Configuration in the Distal Root: A Case Report
He Liu, Ya Shen
Cureus.2024;[Epub] CrossRef - Endodontic management of a case of radix entomolaris: A case report
Priyanka Shorey, Kitty Sidhu
IP Indian Journal of Conservative and Endodontics.2022; 7(1): 39. CrossRef - Endodontic treatment of tooth with morphological anomalies using cone-beam computed tomography
Sung-Hyeon Choi, Na-Kyung Yoon, Ji-Hyun Jang, Young-Hoon Kim, Hoon-Sang Chang, Yun-Chan Hwang, In-Nam Hwang, Won-Mann Oh, Bin-Na Lee
Oral Biology Research.2018; 42(1): 53. CrossRef - Unusual root morphology in second mandibular molar with a radix entomolaris, and comparison between cone-beam computed tomography and digital periapical radiography: a case report
Elisardo López-Rosales, Pablo Castelo-Baz, Roland De Moor, Manuel Ruíz-Piñón, Benjamín Martín-Biedma, Purificación Varela-Patiño
Journal of Medical Case Reports.2015;[Epub] CrossRef
 ePub Link
ePub Link Cite
Cite- Figure
-
- Related articles
-
- Endodontic treatment of a molar-incisor malformation of the maxillary first molar: a case report
- An unusual case of dens invaginatus on a mandibular second molar: a case report
- Endodontic characteristics of mandibular premolar with dens evaginatus: a retrospective study
- Predictor factors of 1-rooted mandibular second molars on complicated root and canal anatomies of other mandibular teeth
Endodontic management of a mandibular second molar with radix entomolaris: a case report
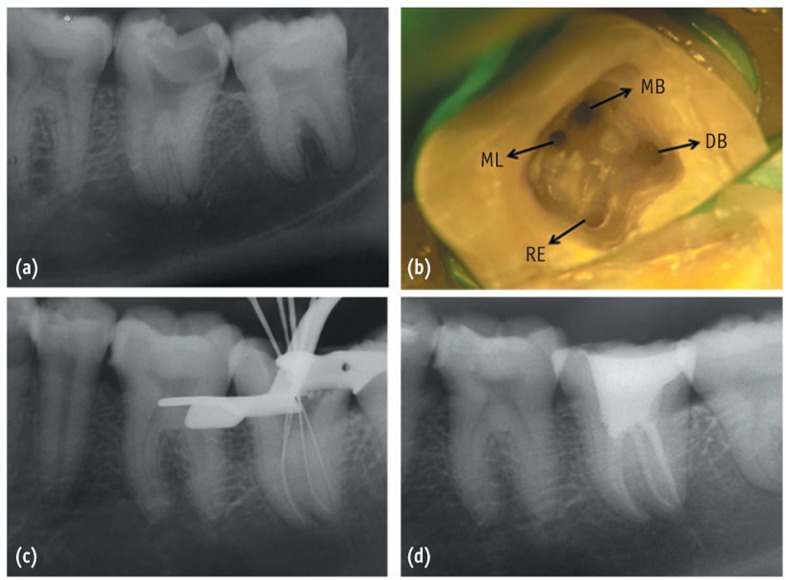
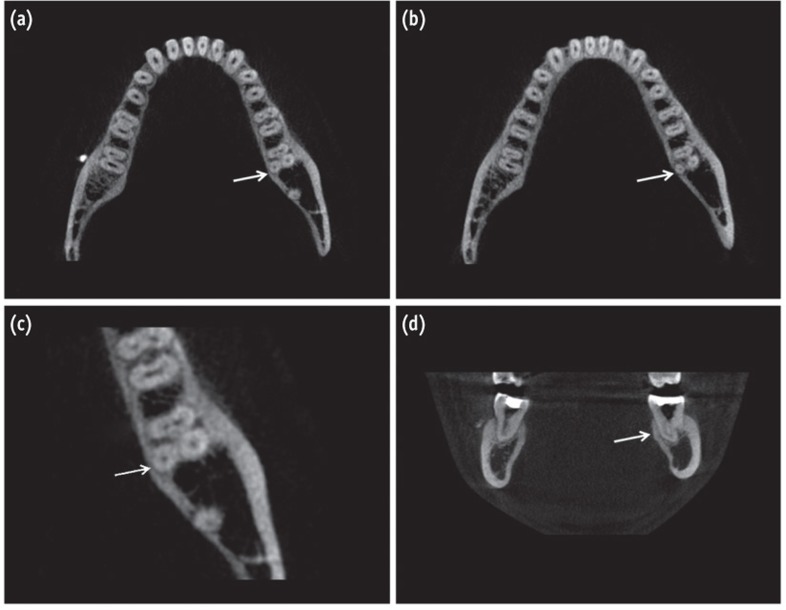
Figure 1 (a) Preoperative radiograph of #37; (b) Access opening showing the presence of RE, MB, ML, and DB canal orifices; (c) Working length radiograph; (d) Postoperative radiograph. RE, radix entomolaris; MB, mesio buccal; ML, mesio lingual; DB, disto buccal.
Figure 2 CBCT images of #37 confirming the presence of a separate RE (arrow) (a) At the cervical level; (b) At the apical level. (c) The CBCT enlarged section at cervical level. (d) CBCT sagittal section showing type III curvature.
Figure 1
Figure 2
Endodontic management of a mandibular second molar with radix entomolaris: a case report

