
Articles
- Page Path
- HOME > Restor Dent Endod > Volume 33(1); 2008 > Article
- Original Article Stress distribution of Class V composite resin restorations: A three-dimensional finite element study
- Jeong-Kil Park1, Bock Hur1, Sung-Kyo Kim2
-
2008;33(1):-38.
DOI: https://doi.org/10.5395/JKACD.2008.33.1.028
Published online: January 31, 2008
1Department of Conservative Dentistry, School of Dentistry, Pusan National University, Busan, Korea.
2Department of Conservative Dentistry, School of Dentistry, Kyungpook National University, Daegu, Korea.
- Corresponding Author: Sung-Kyo Kim. Department of Conservative Dentistry, School of Dentistry, Kyoungpook National University, 188-1, Samduk-dong 2ga, Jung-gu, Daegu, 700-412, Korea. Tel: 82-53-420-5935, skykim@knu.ac.kr
• Received: October 8, 2007 • Revised: November 5, 2007 • Accepted: January 3, 2008
Copyright © 2008 The Korean Academy of Conservative Dentistry
- 2,825 Views
- 15 Download
- 10 Crossref
Abstract
-
This study was to investigate the influence of composite resins with different elastic modulus, cavity modification and occlusal loading condition on the stress distribution of restored notch-shaped noncarious cervical lesion using 3-dimensional (3D) finite element (FE) analysis.The extracted maxillary second premolar was scanned serially with Micro-CT. The 3D images were processed by 3D-DOCTOR. ANSYS was used to mesh and analyze 3D FE model. A notch-shaped cavity and a modified cavity with a rounded apex were modeled. Unmodified and modified cavities were filled with hybrid or flowable resin. After restoration, a static load of 500N was applied in a point-load condition at buccal cusp and palatal cusp. The stress data were analyzed using analysis of principal stress.The results were as follows:
In the unrestored cavity, the stresses were highly concentrated at mesial CEJ and lesion apex and the peak stress was observed at the mesial point angle under both loading conditions.
After restoration of the cavity, stresses were significantly reduced at the lesion apex, however cervical cavosurface margin, stresses were more increased than before restoration under both loading conditions.
When restoring the notch-shaped lesion, material with high elastic modulus worked well at the lesion apex and material with low elastic modulus worked well at the cervical cavosurface margin.
Cavity modification the rounding apex did not reduce compressive stress, but tensile stress was reduced.
I. INTRODUCTION
Noncarious cervical lesions (NCCLs) are characterized as structural defects found on the tooth surface of the cemento-enamel junction (CEJ)1). Loss of tooth structure through noncarious mechanisms may vary in etiology and clinical presentation for each individual and may be associated with physiological or pathological processes2).
Clinically, these lesions have sharp, angular, wedge-shaped defects principally found on the buccal and labial aspects of the teeth. According to Telles et al.3), the most commonly affected teeth are the maxillary premolars. The most important cause of formation of wedge-shaped lesion is the stress applied in the cervical area of the tooth under oral physiological and pathological loads4). Lee and Eakle5) have proposed a mechanical theory of cervical lesion formation and Grippo6) defined pathological loss of hard tissues at the CEJ caused by flexure and ultimate fatigue of enamel at a location away from the point of loading as abfraction.
These lesions may affect either a single tooth or many ones depending on the occlusal forces concentrated. The extent of stress of a cervical lesion, as shown by one study7), is directly related to the area of the periodontal ligament and the amount of tooth mobility under loading. Another study also showed that the lesions were increased as the loads on the tooth moved further away from the long axis8).
Loss of tooth structure in the cervical area of a NCCL may cause esthetic problems and discomfort due to dentinal hypersensitivity3,6). NCCLs occur in a variety of forms depending on the type and severity of the etiological factor, but not all lesions require restorations9). The decision to restore NCCLs is based on the desire to strengthen the tooth and decrease the theoretical stress concentration and flexure, mitigate lesion progression, prevent hypersensitivity and pulp involvement, improve oral hygiene and enhance esthetics9,10). Treatment materials have included the restoration with resin-based composites, glass ionomers11).
In the restoration of NCCLs, restorative materials with esthetic and bonding characteristics are required. Composite restorations are appreciated for their esthetic qualities, relative wear resistance, and smooth surface texture. Recently, flowable resin was introduced. Due to the flexibility of this material, it can be used to restore NCCLs.
A number of studies of modification of cavity design have been conducted. Modified designs of cavity preparation have been proposed as a way of reducing residual shrinkage stresses and margin opening12,13). Osborne-Smith et al.10) and Lee et al.14) proposed that preparation design may need to be changed, depending on whether adhesive retention is adequate or if mechanical retention is necessary. Leinfelder15) suggested reshaping the axial wall to reduce the stress distribution of the notch-shaped lesion. In recent years, there has been increasing interest in understanding the effect of minimal cavity preparation by retaining the V-shape and alternative approaches of preparing the cavity to U-shape for improved retention16).
In the oral cavity, teeth and restorations are exposed to various overloads as a result of biting forces that cause variable patterns of stress in dental tissues. The durability of the restored teeth largely depends on various factors such as tooth flexure, occlusal stress, the sclerosis of the dentinal surface and elastic modulus of the restorative materials.
Three dimensional (3D) finite element (FE) stress analysis is a particularly useful method for examining the stress distribution in teeth because it can cope with the complex geometric shape of a tooth and the large variations in the physical properties of the materials which make up a tooth and its supporting structures7).
The purpose of this study was to investigate the influence of composite resins with different elastic modulus, cavity modification and occlusal loading condition on the stress distribution of the restored notch-shaped NCCL using 3D FE analysis.
II. MATERIALS & METHODS
To develop a 3D FE model, an intact normal extracted human maxillary second premolar was used. The extracted premolar was scanned serially with Micro-CT (SkyScan1072; SkyScan, Aartselaar, Belgium) to expose the tooth sections perpendicular to the long axis of the tooth (58 µm in thickness) and parallel to the occlusal plane. Image processing software, 3D-DOCTOR (Able Software Co., Lexington, MA, USA), was employed to make the boundaries of enamel, dentin and pulp and to construct a surface model of tooth from the sectioned two dimensional images. ANSYS (Swanson Analysis Systems, Inc., Houston, USA) was used to mesh and analyze 3D FE model.
In this study, the final model consisted of 16,668 elements with 18,245 nodes. A notch-shaped lesion with a 4.28 mm vertical height and a 5.31 mm mesiodistal width was modeled. The modified notch model was the same shaped lesion except for the rounded lesion apex (Figure 1).
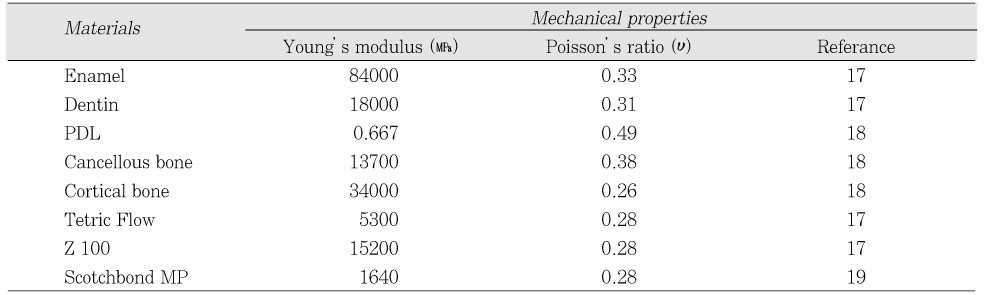
Unmodified and modified notch cavities were filled with hybrid or flowable. Z100 (3M Dental Products, St. Paul, MN, USA) and The Tetric Flow (Vivadent Ets., FL-9494-Schaan, Liechtenstein) were used as representatives of hybrid and flowable resin. The dentin bonding system used in this study was Scotchbond MP (3M Dental Products, St. Paul, MN, USA) and the adhesive layer thickness was 40 µm. The physical properties of the tooth, supporting structures and materials used in this study are given in Table 1.
The model was loaded with two vertical loads of 500 N each, shown in Figure 2. Perpendicular load on the upper third of the palatal slope of the buccal cusp (Load A) and perpendicular load on the upper third of the buccal slope of the palatal cusp (Load B) were used.
The variables were cavity designs (Unmodified cavity; U or Modified cavity; M), restoration methods (Tetric Flow; T, Z100; Z), and loading conditions (Load A; A or Load B; B). The tested groups were classified as 8 situations (Table 2).
To explore the stress condition of the element, the principal stresses presented at the buccal cervical area were used. Under Load A, minimum principal stress was analyzed and under load B maximum principal stress was analyzed. The principal stresses of five nodes {Mesial point angle (MP), Mesial node (Mes), Middle node (Mid), Distal node (Dist), Distal point angle (DP)} in the lesion apex, and cavosurface margin of cervical wall were analyzed using ANSYS. At the initial pilot study, after the cavity was restored with composite resin, the peak stress was moved to more mesial proximal node than MP. Thus, an additional M1 node was selected.
III. RESULTS
The lesion apex line stresses showed the largest stress value and larger apex stresses were observed in the mesial area than in the distal area (Figure 3).
The peak compressive stress of 588.0 MPa was concentrated at MP under Load A and the peak tensile stress of 193.3 MPa was concentrated at MP under Load B and these peak stresses were over the stress limit of teeth20) (Figure 4).
General compressive and tensile stress distributions were shown in Figure 5. After restoration, significant stress relief was shown in the all cavity areas, especially at the lesion apex. however, cervical cavosurface margin, stresses were more increased than before restoration under both loading conditions. And stress concentration at the mesial corner was still observed as unrestored cavity.
Under Load A, similar stress relief was observed regardless of cavity design or restorations, but at the lesion apex, stress relief was smaller when the cavity was restored by Tetric Flow than Z100.
Under Load B, stress values were smaller than Load A. However, larger tensile stress concentrations were observed in the mesial root dentin as well as at the lesion apex in UZB.
1) Lesion apex and CEJ
On the lesion apex and CEJ, similar compressive stresses except peak stress value were observed in all restorations under Load A. The peak stress site shifted from MP to M1 (Figure 6). The highest compressive stress of 310.7 MPa was concentrated at M1 in MTA under Load A. In UZA, the lowest compressive stress of 232.0 MPa was concentrated at M1.
Under Load B, the peak stress site also moved from MP to M1. The highest tensile stress of 101.6 MPa was concentrated at M1 in UTB. Tensile stresses were more reduced in the modified cavity than in the unmodified cavity.
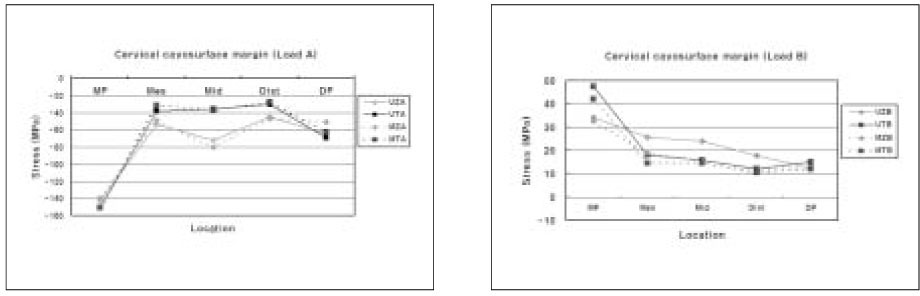
2) Cervical cavosurface margin
On cervical cavosurface margin, the highest compressive stress of 150.7 MPa was concentrated at MP in UTA under Load A. In MZA, the lowest compressive stress of 137.1 MPa was concentrated at MP. At the most site, in Z100 restoarations, compressive stresses were larger than Tetric Flow restoration except MP and DP (Figure 7).
Under Load B, the stresses were reduced moving from the MP to DP. The highest tensile stress of 47.5 MPa was concentrated at MP in UTB under Load B. In MZB, the lowest tensile stress of 32.5 MPa was concentrated at MP. At the most site, in Z100 restoarations, tensile stresses were also larger than Tetric Flow restoration except MP and DP. Similarly, at the lesion apex and CEJ, tensile stresses were more reduced in the modified cavity than in the unmodified cavity.
IV. DISCUSSION
In the current study, 500 N oblique loads were applied to the inner aspects of the buccal or lingual cusp slopes to reproduce of the lateral force that causes NCCL. The highest maximum and minimum principal stress values of between 193.3 and 588 MPa were found in the unrestored cavity. These values were all beyond the potential limit stress value of teeth20). These types of stress concentrations may contribute to fatigue of the tooth structure and accelerate the progression of NCCLs.
Once the lesion was formed, the highest stress concentration was observed around the apex of the wedge-shaped lesion. The discontinuity of the enamel and dentin may cause increased stress and damage in the enamel. In our experiment, the stresses converged in the apex line with more mesial side under both loading conditions. These asymmetric patterns of mesial stress distribution were related to the anatomical asymmetry of the teeth.
Restoring these lesions also will change the stress distribution within the tooth. Grippo6) suggested that if the lesions were left unrestored, the stress concentration caused by the cervical lesion would facilitate further deterioration of the tooth structure. Kuroe et al.21) demonstrated that resin composite restoration of these lesions leads to substantial improvement in the internal stresses within the tooth. Similarly, in the current study, the stresses were greatly reduced after restoration, especially in the lesion apex.
In the clinical assessment of this lesion type, dental practitioners must consider whether the cervical defect requires restoration and choose proper restorative material that will provide the best outcome. The choice of material to restore these lesions is crucial. Glass ionomer may be used, especially in patients with high caries rates. Recently resin composites with dentin bonding agents have become a popular alternative to glass ionomer cement for the restoration of NCCLs. In the current experiment, lesions were restored by conventional hybrid resin and flowable resin.
After restoration of these cavities, restored teeth are also subjected to the physical forces of mastication with their attendant compressive, tensile, shear and bending forces. Concentration of compressive and tensile stresses at the cervical area induced by eccentric or heavy centric occlusal forces may progressively dislodge and eventually debond resin restorations.
Another factor affecting retention failure is the elastic modulus of the restorative materials. It has been demonstrated that a strong correlation exists between marginal failure and Young's modulus of the composite restoration material in the class V situation22). Yaman et al.23) concluded that for class V applications Z 100 gives the most promising results. According to Nakayama et al.24) a Young's modulus equal to or greater than that of the dentine is required for resin composite to resist deformation by occlusal stress. In addition, resin composite Z 100 has a high Young's modulus and a high percentage of volume fraction filler, which increases resistance to deformation by occlusal force25). When use a hard material, the stiffest restoration-tooth interface resulted in the lowest restoration displacement.
In contrast, some researchers contend that one of the methods used to maximize the retention rates of class V restorations is the placement of low elastic modulus materials. Heymann and colleagues26) reported that the retention rates for restorations of a material with lower elastic modulus were significantly higher than those of a material with higher elastic modulus. The rationale behind this is that high modulus materials are unable to flex when the tooth structure is deformed under load and therefore they are displaced from the cavity.
On the other hand, there is an investigation found no differences between a microfilled and a hybrid resin, although the two materials have widely different moduli of elasticity27).
In the current study, two different elastic modulus materials were used. The highest stress reduction was observed at the apex in the Z100 restoration which had the higher elastic modulus. In the cervical cavosurface margin, Tetric Flow restoration showed a smaller stress value compared with Z100. It was hypothesized that Z100 composites used as a strut would improve the reduction rates of stress in the apex. This hypothesis was based on earlier studies23) showing that restoration using Z100 worked as a strut to prevent stress concentration of the lesion.
Under Load A, similar compressive stress was observed independently of kind of restorations. However, under Load B, different stress values appeared. In Tetric Flow restoration, stresses were greater at the apex, but stresses were smaller at the cervical margin. Z100 was reversed. These results show that high elastic modulus materials work well at the lesion apex. This is also involved with special feature of notch-shaped cavity. Due to its sharpest geometrical discontinuity, stress was focused on the lesion apex in the notch-shaped cavity. When biting force is applied, a high elastic modulus material like as a strut can sustain the stress at the apex. This is especially true under Load B when tensile stress occurs.
Stress also depends on geometry of the cavity as well as the mechanical properties of restorative material. According to Hubsch et al.28), stress can be reduced by modifying the cavity design. Additionally, Leinfelder15) suggested that the problem of stress concentrations can be reduced dramatically by modifying the axial wall from V-shaped configuration to one that is somewhat more concave in design and the proper shaping can be accomplished with a No 4 or in some instances a No 6 round bur.
In the present study, stresses were compared with a modified cavity form. Because the notch-shaped lesion had the highest stress concentration corresponded with sharpest geometric discontinuity at the apex of lesion, so the apex was remodeled by rounding. Contrary our expectations, in the modified cavity, the stresses of lesion apex did not decrease under Load A as compressive force. On the other hand, under Load B as tensile force, the stresses decreased much more than in the unmodified cavity.
So considered, it is assumed that in compressive stress, the change of geometrical shape of modified cavity is not significant, similar stress concentration was observed. However, in tensile stress, from the point of view of fracture mechanics, stress was acted as a crack course in the unmodified cavity. On the other hand, in the modified cavity, the stress concentration was dispersed through crack retardation by a rounding effect29,30). For these stress characters, further study is necessary. Although compressive stress did not decreased, apex modification has a significant meaning for tensile stress which damage teeth seriously was decreased.
In general, the compressive strength of enamel is greater than that of dentin, while the tensile strength of dentin is greater than that of enamel. As the tensile strengths of enamel and dentin are much lower than their respective compressive strengths31,32), tensile stress is much more destructive than compressive stress. In terms of restoration retention in dentin bonding agent trials, tensile stresses appear to be the most destructive, at least short-term. Therefore, the developments of methods and materials that may reduce tensile stress are important.
In this experiment, the cavity modification method that cavity apex was modified by rounding was the profitable method for tensile stress reduction. Thus, this method is recommended for restoration of notch-shaped lesion because it showed the favorable effect in tensile stress.
V. CONCLUSIONS
Within the limitations of this study, it is suggested that when restoring the notch-shaped lesion, material with high elastic modulus worked well at the lesion apex and material with low elastic modulus worked well at the cervical cavosurface margin. Cavity modification of the rounding apex did not reduce compressive stress, but tensile stress was reduced.
- 1. Levitch LC, Bader JD, Shugars DA, Heymann HO. Non-carious cervical lesion. J Dent. 1994;22: 195-207.PubMed
- 2. Litonjua LA, Bush PJ, Andreana S, Tobias TS. Effects of occlusal load on cervical lesion. J Oral Rehabil. 2004;31: 225-232.PubMed
- 3. Telles D, Pegoraro LF, Pereira JC. Prevalence of non-carions cervical lesions and their relation to occlusal aspects: a clinical study. J Esthet Dent. 2000;12: 10-15.PubMed
- 4. Palamara D, Palamara JE, Tyas MJ, Messer HH. Strain patterns in cervical enamel of teeth subjected to occlusal loading. Dent Mater. 2000;16: 412-419.ArticlePubMed
- 5. Lee WC, Eakle WS. Possible role of tensile stress in etiology of cervical erosive lesions of teeth. J Prosthet Dent. 1984;52: 374-380.PubMed
- 6. Grippo JO. Abfractions: A new classification of hard tissue lesions of tooth. J Esthet Dent. 1991;3: 14-19.PubMed
- 7. Rees JS. An investigation into the importance of the periodontal ligament and alveolar bone as supporting structures in finite element studies. J Oral Rehabil. 2001;28: 425-432.ArticlePubMed
- 8. Rees JS. The effect of variation in occlusal loading on the development of abfraction lesions: a finite element study. J Oral Rehabil. 2002;29: 188-193.ArticlePubMed
- 9. King PA. Adhesive techniques. Br Dent J. 1999;186: 321-326.ArticlePubMed
- 10. Osborne-Smith KL, Burke FJ, Wilson NH. The aetiology of the non-carious cervical lesion. Int Dent J. 1999;49: 139-143.ArticlePubMed
- 11. Vandewalle KS, Vigil G. Guidelines for the restoration of class V lesions. Gen Dent. 1997;45: 254-260.PubMed
- 12. Marzouk MA, Bhaiji AH. Influence of enamel cavosurface configuration on marginal leakage in class V composite resin restorations. Am J Dent. 1989;2: 165-169.PubMed
- 13. Saunders WP, Muirhead JM. Microleakage of composite restorations with Syntac Bond and Denthesive. Am J Dent. 1992;5: 255-257.PubMed
- 14. Lee WC, Eakle WS. Stress-induced cervical lesions: review of advances in the past 10 years. J Prosthet Dent. 1996;75: 487-494.ArticlePubMed
- 15. Leinfelder KF. Restoration of abfracted lesions. Compendium. 1994;15: 1396-1400.PubMed
- 16. Hakimeh S, Vaidyanathan J, Houpt ML, Vaidyanathan TK, Von Hagen S. Microleakage of compomer class V restorations: effect of load cycling, thermal cycling, and cavity shape differences. J Prosthet Dent. 2000;83: 194-203.ArticlePubMed
- 17. Katona TR, Winkler MM. Stress analysis of a bulk-filled class V light-cured composite restoration. J Dent Res. 1994;73: 1470-1477.ArticlePubMedPDF
- 18. Geramy A, Sharafoddin F. Abfraction: 3D analysis by means of the finite element method. Quintessence Int. 2003;34: 526-533.PubMed
- 19. Le SY, Chiang HC, Huang HM, Shih YH, Chen HC, Dong DR, Lin CT. Thermo-debonding mechanisms in dentin bonding systems using finite element analysis. Biomaterials. 2001;22: 113-123.ArticlePubMed
- 20. Litonjua LA, Andreana S, Patra AK, Cohen RE. An assessment of stress analyses in the theory of abfraction. Biomed Mater Eng. 2004;14: 311-321.PubMed
- 21. Kuroe T, Itoh H, Caputo AA, Konuma M. Biomechanics of cervical tooth structure lesions and their restoration. Quintessence Int. 2000;31: 267-274.PubMed
- 22. Kemp-Scholte CM, Davidson CL. Marginal integrity related to bond strength and strain capacity of composite resin restorative systems. J Prosthet Dent. 1990;64: 658-664.ArticlePubMed
- 23. Yaman SD, Sahin M, Aydin C. Finite element analysis of strength characteristics of various resin based restorative materials in class V cavities. J Oral Rehabil. 2003;30: 630-641.ArticlePubMedPDF
- 24. Nakayama WT, Hall DR, Grenoble DE, Katz JL. Elastic properties of dental resin restorative materials. J Dent Res. 1974;53: 1121-1126.ArticlePubMedPDF
- 25. Willems G, Lambrechts P, Braem M, Celis JP, Vanherle G. A classification of dental composites according to their morphological and mechanical characteristics. Dent Mater. 1992;8: 310-319.ArticlePubMed
- 26. Heymann HO, Sturdevant JR, Bayne S, Wilder AD, Sluder TB, Brunson WD. Examining tooth flexure effects on cervical restorations: a two-year clinical study. J Am Dent Assoc. 1991;122: 41-47.Article
- 27. Browning WD, Brackett WW, Gilpatrick RO. Retention of microfilled and hybrid resin-based composite in non-carious class 5 lesions: a double-blind, randomized clinical trial. Oper Dent. 1999;24: 26-30.PubMed
- 28. Hubsch PF, Middleton J. Asymptotic analysis of the stress field in adhering dental restorations. J Biomech Eng. 2000;122: 408-415.ArticlePubMedPDF
- 29. Ugural AC, Fenster SK. Advanced strength and applied elasticity. 2003;4th ed. New Jersey: Pearson Education Inc.; 163-168.
- 30. Ghfiri R, Amrouche A, Imad A, Mesmacque G. Fatigue life estimation after crack repair in 6005 A-T6 aluminium alloy using the cold expansion hole technique. Fatigue Fract Engng Mater Struct. 2000;23: 911-916.Article
- 31. Bowen RL, Rodriguez MS. Tensile strength and modulus of elasticity of tooth structure and several restorative materials. J Am Dent Assoc. 1962;64: 378-387.ArticlePubMed
- 32. Lehman ML. Tensile strength of human dentin. J Dent Res. 1967;46: 197-201.ArticlePubMedPDF
REFERENCES
Figure 1
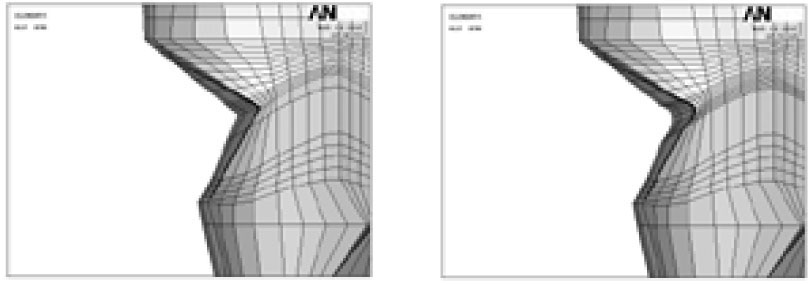
Schematic diagram represents unmodified and modified cavity configuration (Left; Unmodified cavity, Right; Modified cavity).
Figure 2
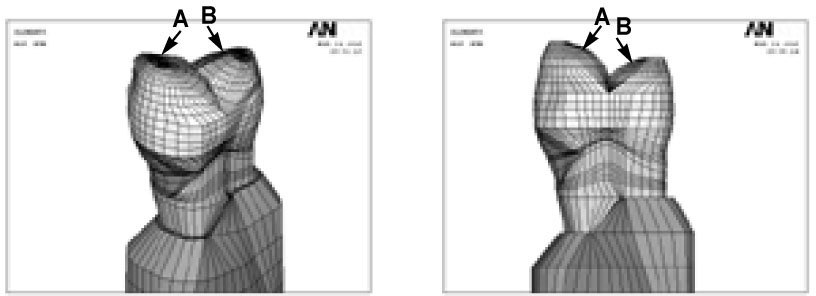
Schematic diagram of loading points (A; Perpendicular load on the upper third of the palatal slope of the buccal cusp, B; perpendicular load on the upper third of the buccal slope of the palatal cusp).
Figure 3
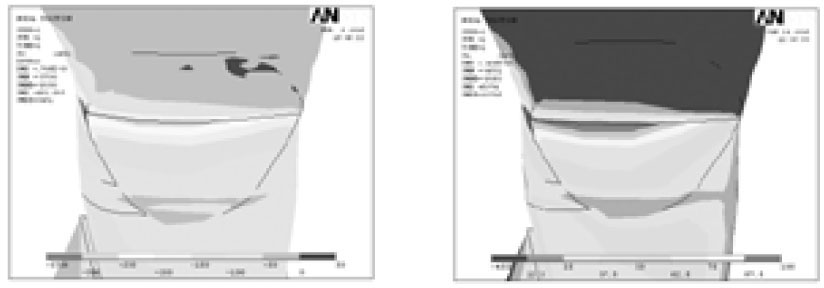
The principal stress distribution of notch-shaped cavity before restoration (Left; Minimum principal stress-Compressive stress, Right; Maximum principal stress-Tensile stress. Upper and lower view's scales were different each other).
Figure 4
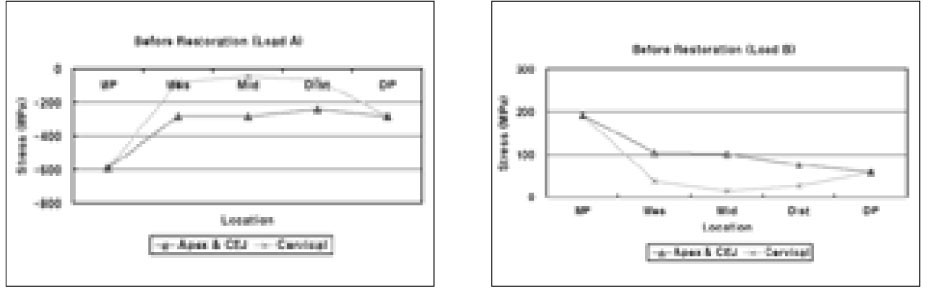
Before restoration, the principal stress distribution on the lesion apex and CEJ (Apex & CEJ), cervical cavosurface margin (Cervical) under Load A and B (MP: Mesial point angle, DP: Distal point angle, Mes: Mesial node, Mid: Middle node, Dist: Distal node).
Figure 5
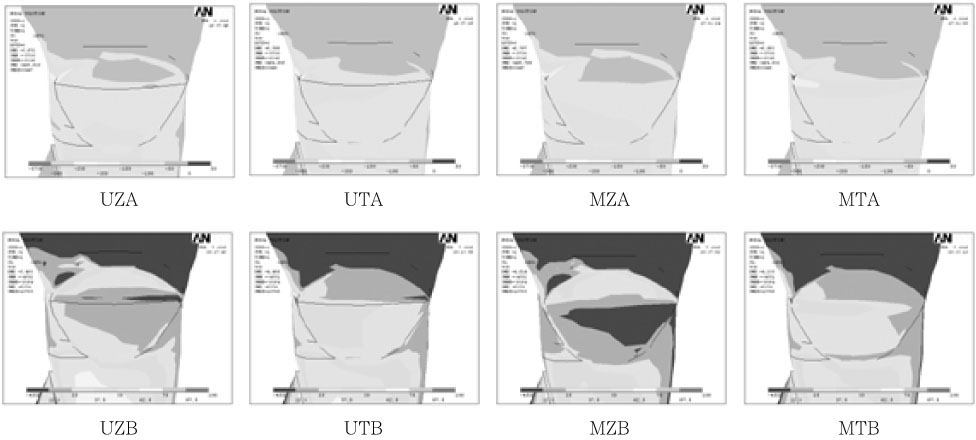
After restoration, the principal stress distribution in cervical cavity wall under Load A and B.
Figure 6
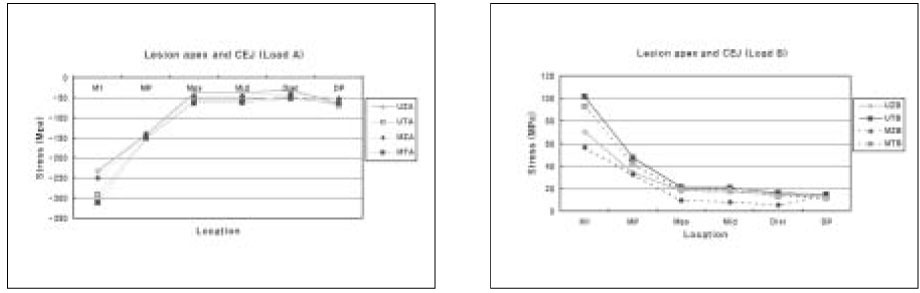
The principal stress distribution on lesion apex and CEJ after restoration under Load A and B (MP: Mesial point angle, DP: Distal point angle, Mes: Mesial node, Mid: Middle node, Dist: Distal node, M1: more mesial proximal point than MP).

Tables & Figures
REFERENCES
Citations
Citations to this article as recorded by 
- Effect of Loading and Restoration on the Biomechanical Behavior of Premolars with Simulated Abfraction Lesions
Deepa N Thangaraj, Sebeena Mathew, Karthick Kumaravadivel, Kerena Joseline, Boopathi Thangavel, Manimaran Sekar
World Journal of Dentistry.2025; 15(12): 1076. CrossRef - A Comparative Evaluation of Fiber-Reinforced Composite and Conventional Composite Restorations in Non-Carious Cervical Lesions: A Randomized Clinical Trial
Vinutha Manjunath, Aparna Nair, Vidya G. Doddawad
Journal of International Oral Health.2025; 17(2): 145. CrossRef - Numerical investigation of stress concentration at the tip of the V-notch partially filled with material
V.P. Matveenko, A.Y. Fedorov, E.B. Galkina
Computational Continuum Mechanics.2022; 15(3): 333. CrossRef - Clinical Evaluation of Bioactive Restorative Material versus Resin Modified Glass Ionomer in Cervical Restorations: A Randomized Controlled Clinical Trial
Yehia Hafez Yehia, Amir Hafez Ibrahim, Eman Abou-auf, Amira Farid Elzogbhi
Open Access Macedonian Journal of Medical Sciences.2022; 10(D): 33. CrossRef - Effects of Root Maturation and Thickness Variation in Coronal Mineral Trioxide Aggregate Plugs Under Traumatic Load on Stress Distribution in Regenerative Endodontic Procedures: A 3-dimensional Finite Element Analysis Study
Akif Demirel, Tuğba Bezgin, Şaziye Sarı
Journal of Endodontics.2021; 47(3): 492. CrossRef - Finite element analysis of V-shaped tooth defects filled with universal nanohybrid composite using incremental technique
Tsanka Dikova, Tihomir Vasilev, Vesela Hristova, Vladimir Panov
Journal of the Mechanical Behavior of Biomedical Materials.2021; 118: 104425. CrossRef - Are Increased Masticatory Forces Risk for Primary 2nd Molars without Successors? A 3D FEA Study
Akif Demirel, Şaziye Sarı
Journal of Clinical Pediatric Dentistry.2019; 43(1): 64. CrossRef - Finite element analysis of maxillary central incisors restored with various post-and-core applications
MinSeock Seo, WonJun Shon, WooCheol Lee, Hyun-Mi Yoo, Byeong-Hoon Cho, Seung-Ho Baek
Journal of Korean Academy of Conservative Dentistry.2009; 34(4): 324. CrossRef - The influence of combining composite resins with different elastic modulus on the stress distribution of Class V restoration: a three-dimensional finite element study
Jeong-Kil Park, Bock Hur, Sung-Kyo Kim
Journal of Korean Academy of Conservative Dentistry.2008; 33(3): 184. CrossRef - Stress analysis of maxillary premolars with composite resin restoration of notch-shaped class V cavity and access cavity; Three-dimensional finite element study
Seon-Hwa Lee, Hyeon-Cheol Kim, Bock Hur, Kwang-Hoon Kim, Kwon Son, Jeong-Kil Park
Journal of Korean Academy of Conservative Dentistry.2008; 33(6): 570. CrossRef
 ePub Link
ePub Link Cite
CiteStress distribution of Class V composite resin restorations: A three-dimensional finite element study
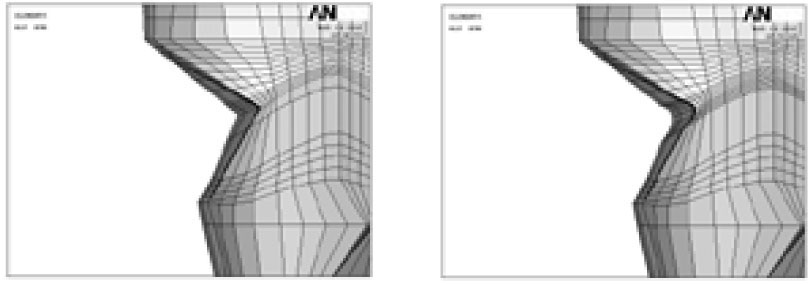
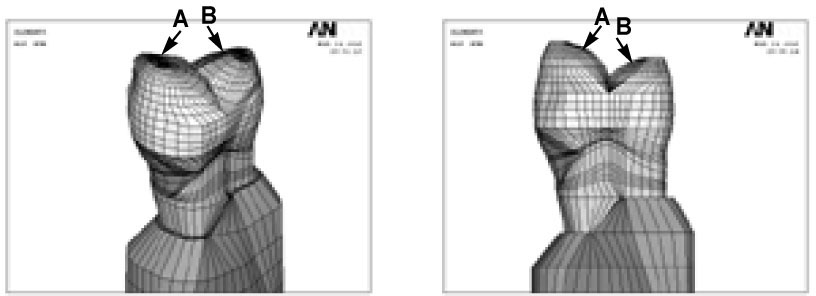
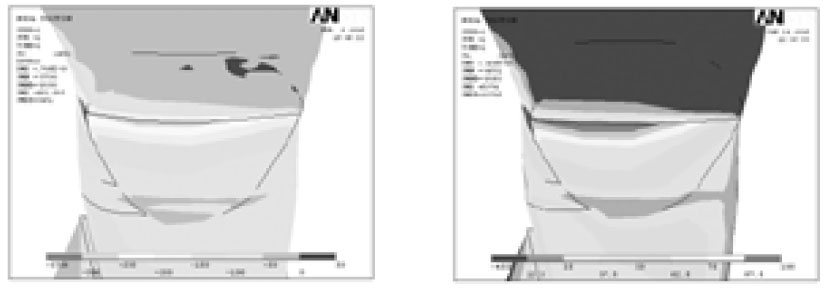
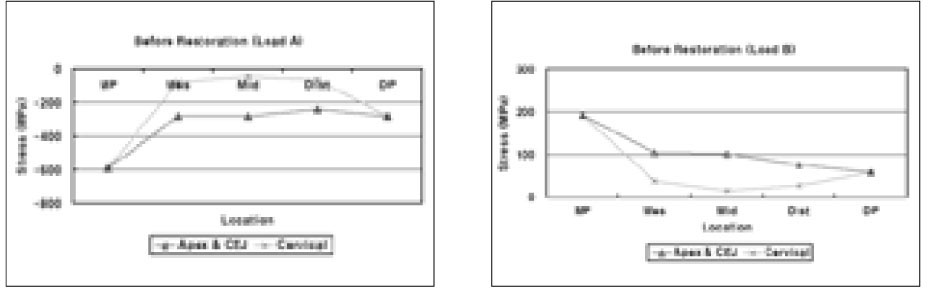
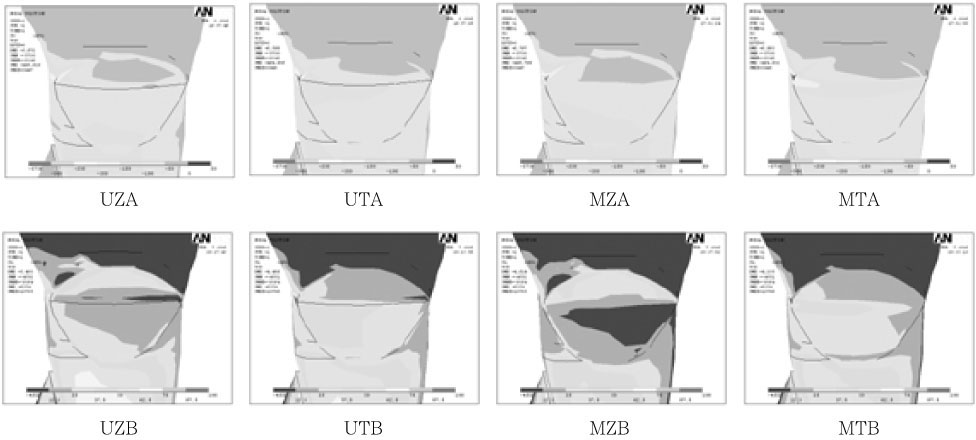
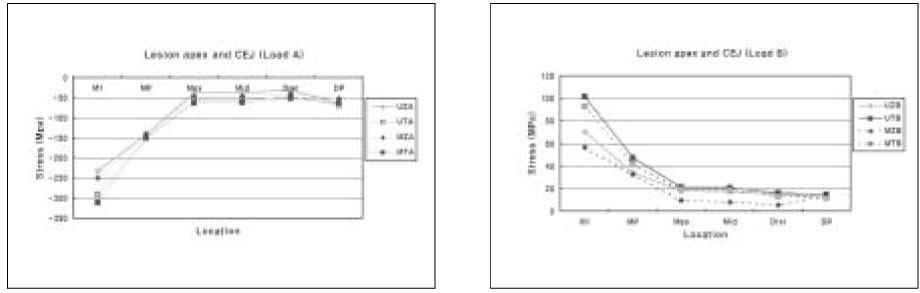

Figure 1
Schematic diagram represents unmodified and modified cavity configuration (Left; Unmodified cavity, Right; Modified cavity).
Figure 2
Schematic diagram of loading points (A; Perpendicular load on the upper third of the palatal slope of the buccal cusp, B; perpendicular load on the upper third of the buccal slope of the palatal cusp).
Figure 3
The principal stress distribution of notch-shaped cavity before restoration (Left; Minimum principal stress-Compressive stress, Right; Maximum principal stress-Tensile stress. Upper and lower view's scales were different each other).
Figure 4
Before restoration, the principal stress distribution on the lesion apex and CEJ (Apex & CEJ), cervical cavosurface margin (Cervical) under Load A and B (MP: Mesial point angle, DP: Distal point angle, Mes: Mesial node, Mid: Middle node, Dist: Distal node).
Figure 5
After restoration, the principal stress distribution in cervical cavity wall under Load A and B.
Figure 6
The principal stress distribution on lesion apex and CEJ after restoration under Load A and B (MP: Mesial point angle, DP: Distal point angle, Mes: Mesial node, Mid: Middle node, Dist: Distal node, M1: more mesial proximal point than MP).
Figure 7
The principal stress distribution on cervical cavosurface margin after restoration under Load A and B (MP: Mesial point angle, DP: Distal point angle, Mes: Mesial node, Mid: Middle node, Dist: Distal node).
Figure 1
Figure 2
Figure 3
Figure 4
Figure 5
Figure 6
Figure 7
Stress distribution of Class V composite resin restorations: A three-dimensional finite element study
Mechanical properties of the tooth and supporting structures used in the study
Simulated groups according to cavity designs, restoration materials and loading conditions
Table 1
Mechanical properties of the tooth and supporting structures used in the study
Table 2
Simulated groups according to cavity designs, restoration materials and loading conditions

