
Search
- Page Path
- HOME > Search
Research Articles
- Magnitude of pulp space narrowing over time and contributing factors in teeth with vital pulp therapy: a retrospective cohort study
- Akarapong Boontankun, Papimon Chompu‑inwai, Chanika Manmontri, Nattakan Chaipattanawan, Areerat Nirunsittirat, Phichayut Phinyo, Trasapong Thaiupathump
- Restor Dent Endod 2026;51(2):e24. Published online May 13, 2026
- DOI: https://doi.org/10.5395/rde.2026.51.e24
-
 Abstract
Abstract
 PDF
PDF Supplementary Material
Supplementary Material PubReader
PubReader ePub
ePub - Objectives
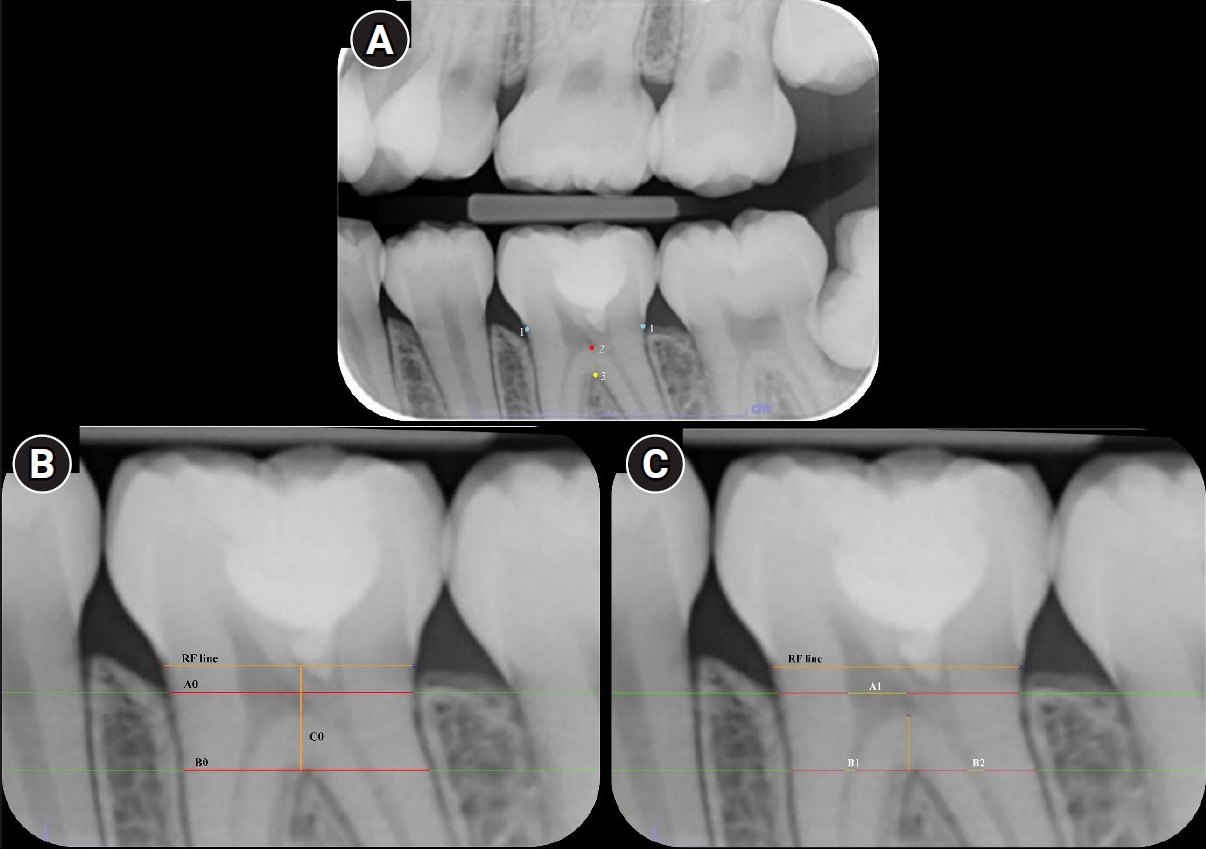
This study aimed to compare the magnitude of pulp space narrowing over time—measured as the change in pulp/tooth proportion from baseline—between mandibular molars treated with different types of vital pulp therapy (VPT) and their contralateral sound molars (controls). This study also investigated factors influencing the magnitude of pulp space narrowing in molars that have undergone VPT.
Methods
This retrospective cohort study involved the assessment of bitewing radiographs of VPT-treated molars and controls at baseline and follow-up. Using reference points and lines on the radiograph, pulp/tooth proportions were measured by examiners. The intraclass correlation coefficient (ICC) was used to report examiner reliability. The changes in pulp/tooth proportions from baselines were compared between subgroups using multilevel mixed effect linear regression and the Wald test.
Results
A total of 382 bitewing radiographs from 134 teeth were included. The follow-up period ranged from 6 to 84 months (mean, 27.12 ± 17.67 months). ICC values indicated good to excellent examiner reliability. Compared to the controls, changes in pulp/tooth proportion from baselines, indicating pulp space narrowing, were significantly greater in teeth with partial pulpotomy (at pulp chamber width) and coronal pulpotomy (at pulp canal width). Factors affecting the magnitude of pulp space narrowing included the more invasive type of VPT and the more severe preoperative diagnosis.
Conclusions
The magnitude of pulp space narrowing was greater in VPT-treated molars than in controls. The more invasive type of VPT and severe preoperative diagnosis were factors contributing to the magnitude of pulp space narrowing.
- 1,060 View
- 61 Download

- Concentrated growth factor scaffold-based pulpotomy of permanent molars with symptomatic irreversible pulpitis
- Arthi K. Harith, Vishnupriya Koteeswaran, Dinesh Kowsky, Natanasabapathy Velmurugan, Suresh Nandini
- Restor Dent Endod 2025;50(1):e1. Published online January 17, 2025
- DOI: https://doi.org/10.5395/rde.2025.50.e1
-
Abstract
PDFPubReaderePub
- Objectives
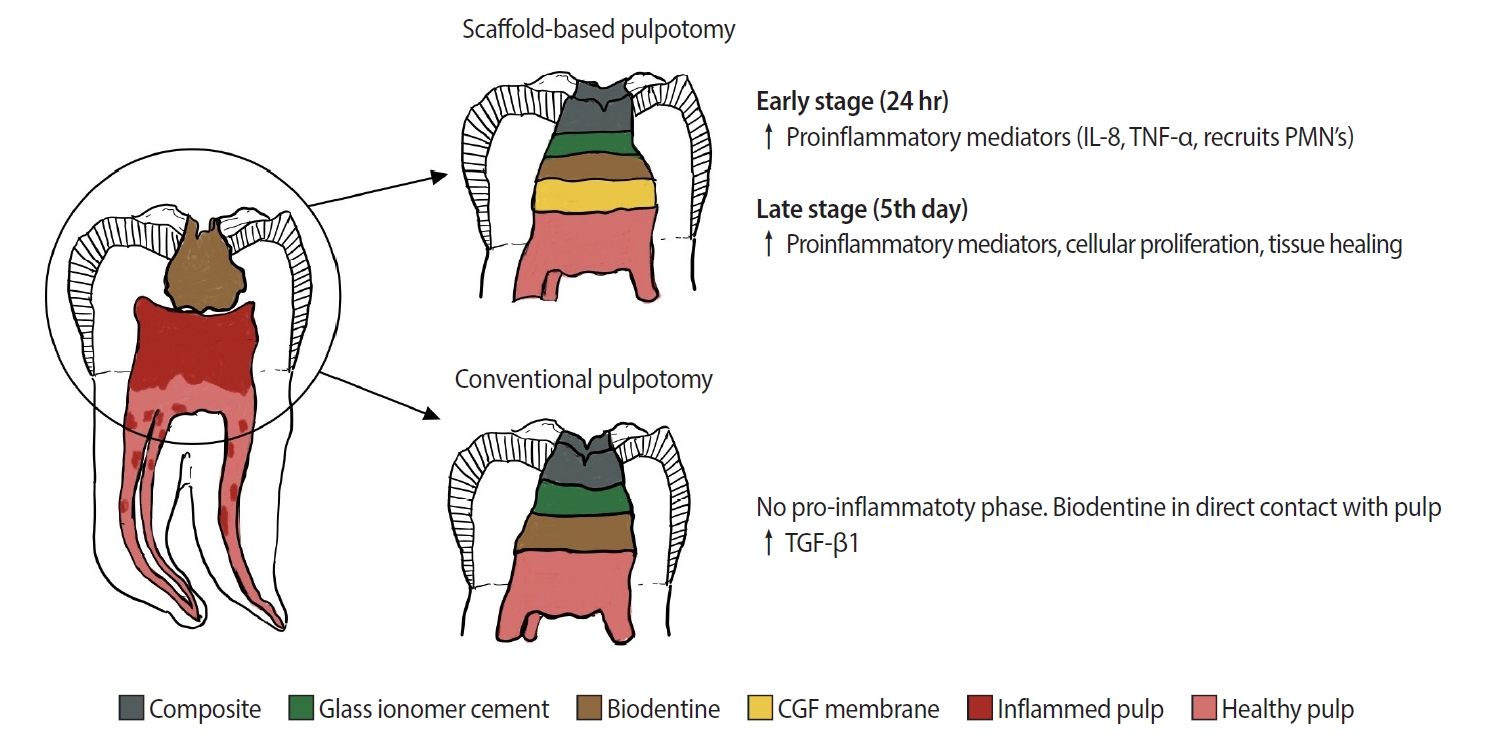
Pulpotomy is a minimally invasive procedure that aims to retain the vitality of the radicular pulp by removing the inflamed coronal pulp tissue. This case series presents the successful management of symptomatic irreversible pulpitis by pulpotomy with concentrated growth factor (CGF) scaffolds.
Methods
Six permanent mandibular molars with a diagnosis of symptomatic irreversible pulpitis were included. Under Local anesthesia and rubber dam isolation, caries were excavated using high-speed bur under coolant. Full coronal pulpotomy was done and hemostasis was achieved. CGF membrane was prepared and placed over the radicular pulp and layered with Biodentine (Septodont). Final restoration of type IX glass ionomer cement and bulk fill composite resin was placed. Patients were assessed for various clinical and radiographic parameters at intervals of 1 week and 3, 6, and 12 months. Five patients fulfilled the success criteria at the end of 1 year.
Results
Pulpotomy is considered an alternative treatment modality for root canal treatment in symptomatic irreversible pulpitis aiming at alleviating symptoms and maintaining vitality. CGF scaffold when used as a capping material acts as a reservoir for growth factors with anti-inflammatory properties and enhances healing.
Conclusions
Scaffold-based pulpotomy can be considered a biological approach to healing inflamed pulp.
- 5,537 View
- 541 Download
-
Evaluation of mineral induction ability and cytotoxicity of carbonated hydroxyapatite for pulp tissue regeneration: an
in vitro study - S. Swathi Priyadharshini, Chinnasamy Ragavendran, Anand Sherwood, J. Ramana Ramya, Jogikalmat Krithikadatta
- Restor Dent Endod 2024;49(4):e40. Published online October 29, 2024
- DOI: https://doi.org/10.5395/rde.2024.49.e40
-
Abstract
PDFPubReaderePub
Objectives This study aimed to evaluate carbonated hydroxyapatite (CHA)’s ability for mineral induction and its
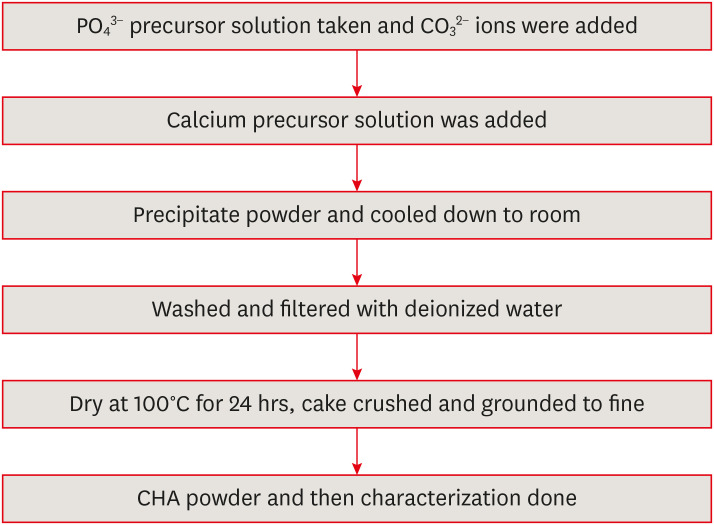
in vitro cytotoxicity with human dental pulp cells.Materials and Methods Precursors for the study include di-ammonium hydrogen phosphate and calcium nitrate tetrahydrate, with sodium hydrogen carbonate added to achieve different levels of carbonate substitution. The synthesized CHA samples are characterized using X-ray diffraction, Fourier transform infrared spectroscopy, and Raman spectroscopy. Scanning electron microscopy (SEM) was used to observe morphology. For 14 days at 37°C, samples were submerged in simulated body fluid to assess their mineral induction capabilities. SEM was used to confirm apatite formation on sample surfaces. The cytotoxicity assay was used to assess the vitality of the cells following their exposure to various concentrations of CHA.
Results The Joint Committee on Powder Diffraction Standards data for HA aligned well with the results from X-ray diffraction analysis of CHA across 3 different concentrations, indicating strong agreement. Fourier transform infrared spectra indicated the presence of phosphate, hydroxyl, and carbonate groups within the samples. SEM and Energy-dispersive X-ray analysis show agglomerated and flaky nanoparticles. All the samples are bioactive, but the formation of apatite differs from one another.
In vitro cytotoxicity assay showed that over 70% of cells maintain viability.Conclusions The results of this study may provide insight into the potential use of carbonated HA as a dental pulp-capping material for vital pulp therapy.
-
Citations
Citations to this article as recorded by
- Smart Nanomaterials: Current State and Future Prospects in Drug Delivery and Tissue Engineering
E. Elizabeth Rani, D. Sakthi Sanjana, E. Karthikeyan, J. Nandhini
Biomedical Materials & Devices.2026; 4(2): 1455. CrossRef - Thermoresponsive Nanomaterials: Revolutionizing Cancer Theranostics
Bellarmin Michael, Mohanakrishnan Srinivasan, Karthikeyan Elumalai, Lokeshwar Ravikumar, Sivaprakash Kathiresan, Nandhini Jayaprakash
Biomedical Materials & Devices.2026; 4(3): 2697. CrossRef - Physicochemical and antibacterial evaluation of novel nano α-TCP–AgNPs biocomposites for direct pulp-capping applications
Selviana Wulansari, Hendra Dian Adhita Dharsono, Nasrul Wathoni, Rosalina Tjandrawinata, Arief Cahyanto, Moehamad Orliando Roeslan
Frontiers in Oral Health.2026;[Epub] CrossRef - Physicochemical effects of nano type-B bone substitute on pulp protective cement formulations
Njwan Fadhel SHEHAB
Dental Materials Journal.2026; 45(1): 92. CrossRef - Recycling waste for sustainability: The green synthesis of silver nanoparticles from Bougainvillea glabra green waste, and the evaluation of their antioxidant, cytotoxic, catalytic, antibacterial and in-silico molecular docking properties
Hafsa Naleem, Mathivathani Kandiah, Beneli Gunaratne, Ominda Perera
Next Research.2026; 11: 101990. CrossRef - Comparative evaluation of compressive strength and morphological interface of carbonated hydroxyapatite with other pulp capping materials: An in vitro analysis
S. Swathi Priyadharshini, Chinnasamy Ragavendran, I. Anand Sherwood, Ramanaramya Jeyapalan
Endodontology.2025; 37(1): 90. CrossRef - Bioactive Dioxo-Phosphobetaines derived from the reaction of Dichlorodinitrobenzofuroxane with various phosphines
Irina V. Galkina, Haiyan Fan, Semen R. Romanov, Dmitriy I. Bakhtiyarov, Luisa M. Usupova, Svetlana N. Egorova, Yulia V. Bakhtiyarova, Enrico Benassi
Bioorganic Chemistry.2025; 163: 108695. CrossRef - Near-infrared laser-activated PLGA-PDA core-shell nanohybrids for synergistic photothermal antibacterial therapy and sustained ion release in orthodontic white spot lesions prevention
Zezhou Feng, Yujiang Liu, Silu Sun, Minmin Si, Di Huang, Zhiyuan Feng
Journal of Dentistry.2025; 162: 106078. CrossRef - Formation and utilization of soluble microbial products in denitrifying biofilters at different carbon-to-nitrogen ratios: Microbial community characteristics
Fangyuan Jiang, Xianyang Shi
Journal of Environmental Chemical Engineering.2025; 13(6): 119554. CrossRef - Bioactivity and biocompatibility of bioceramic-based pulp capping materials in laboratory and animal models
Rafiqul Islam, Md. Refat Readul Islam, Kenta Tsuchiya, Yu Toida, Hidehiko Sano, Monica Yamauti, Hany Mohamed Aly Ahmed, Atsushi Tomokiyo
Journal of Materials Science: Materials in Medicine.2025;[Epub] CrossRef - Physical, Chemical, and Biological Properties of Graphene Nanoparticle-added Tricalcium Silicate Formulations: A Systematic Review
Soundaria Srinivasan, Deepa Gurunathan, Lakshmi Thangavelu
Journal of International Oral Health.2025; 17(6): 453. CrossRef - Advanced structural and compositional profiling of mineral trioxide aggregate incorporated with nano-carbonated hydroxyapatite: a comprehensive X-ray diffraction and energy dispersive X-ray investigation
Njwan Fadhel Shehab, Nadia Hameed Hasan, Alaa Edrees Dawood, Nawal Atiya Khalaf
Biomaterial Investigations in Dentistry.2025; 12: 216. CrossRef
- Smart Nanomaterials: Current State and Future Prospects in Drug Delivery and Tissue Engineering
- 4,780 View
- 156 Download
- 9 Web of Science
- 12 Crossref
-
The influence of sodium hypochlorite concentration on the fibrin structure of human blood clots and transforming growth factor-beta 1 release: an
ex vivo study - Anisha Mishra, Velmurugan Natanasabapathy, Nandini Suresh
- Restor Dent Endod 2022;47(4):e42. Published online October 31, 2022
- DOI: https://doi.org/10.5395/rde.2022.47.e42
-
Abstract
PDFSupplementary MaterialPubReaderePub
Objective This study investigated the effects of various concentrations of sodium hypochlorite (NaOCl) on human whole-blood clotting kinetics, the structure of the blood clots formed, and transforming growth factor (TGF)-β1 release.
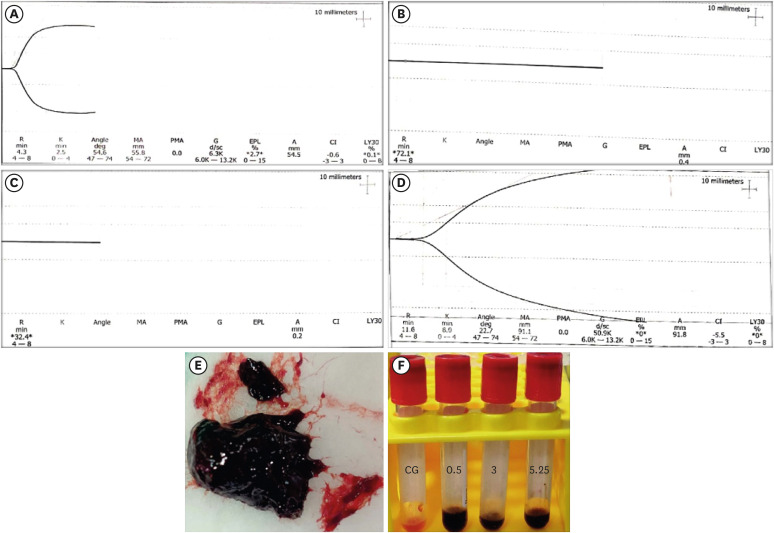
Materials and Methods Human whole blood was collected from 5 healthy volunteers and divided into 4 groups: CG (control, 0.5 mL of blood), BN0.5 (0.5 mL of blood with 0.5 mL of 0.5% NaOCl), BN3 (0.5 mL of blood with 0.5 mL of 3% NaOCl), and BN5.25 (0.5 mL of blood with 0.5 mL of 5.25% NaOCl). The effects of NaOCl on clotting kinetics, structure of fibrin and cells, and release of TGF-β1 were assessed using thromboelastography (TEG), scanning electron microscopy (SEM), and enzyme-linked immunosobent assay, respectively. Statistical analysis was conducted using the Kruskal Wallis and Mann-Whitney
U tests, followed by thepost hoc Dunn test. Ap value < 0.05 indicated statistical significance.Results The blood samples in BN0.5 and BN3 did not clot, whereas the TEG of BN5.25 showed altered clot formation. Samples from the CG and BN3 groups could only be processed with SEM, which showed that the latter lacked fibrin formation and branching of fibers, as well as clumping of red blood cells with surface roughening and distortion. TGF-β1 release was significantly highest in BN3 when all groups were compared to CG (
p < 0.05).Conclusions Each concentration of NaOCl affected the release of TGF-β1 from blood clots and altered the clotting mechanism of blood by affecting clotting kinetics and cell structure.
-
Citations
Citations to this article as recorded by- Evaluation of the cytotoxicity of a broad-spectrum antiseptic using a model of erythrocyte hemolysis in an in vitro experiment
S. P. Rubnikovich, O. E. Bekjanova, L. E. Khasanova, Sh. F. Shamsieva, S. X. Alimova, M. M. Astanakulova, N. T. Babadjanova, X. Sh. Mirzaev
Proceedings of the National Academy of Sciences of Belarus, Medical series.2026; 23(2): 95. CrossRef - Effect of Adjunctive Ozone Application Protocols on Dentin-Derived Growth Factor Release: An In Vitro Study
Sude Göbüt, Melis Oya Ateş, Ali Keleş, Fatma Avcıoğlu
Journal of Clinical Medicine.2026; 15(11): 4277. CrossRef - Cytotoxic Effects of Synthetic and Herbal Endodontic Irrigants on Human Red Blood Cells: An In Vitro Study
Panna Mangat, Bhaviya Chandel, Mampi Biswas, Sara Trivedy, Akshata Gupta, Nayan Shree, Seema Gupta
Cureus.2025;[Epub] CrossRef
- Evaluation of the cytotoxicity of a broad-spectrum antiseptic using a model of erythrocyte hemolysis in an in vitro experiment
- 3,079 View
- 39 Download
- 1 Web of Science
- 3 Crossref
- Clinical and radiographical evaluation of mineral trioxide aggregate, biodentine and propolis as pulpotomy medicaments in primary teeth
- Bharti Kusum, Kumar Rakesh, Khanna Richa
- Restor Dent Endod 2015;40(4):276-285. Published online September 9, 2015
- DOI: https://doi.org/10.5395/rde.2015.40.4.276
-
Abstract
PDFPubReaderePub
Objectives The purpose of this study was to evaluate the efficacy of mineral trioxide aggregate (MTA), Biodentine and Propolis as pulpotomy medicaments in primary dentition, both clinically and radiographically.
Materials and Methods A total of 75 healthy 3 to 10 yr old children each having at least one carious primary molar tooth were selected. Random assignment of the pulpotomy medicaments was done as follows: Group I, MTA; Group II, Biodentine; Group III, Propolis. All the pulpotomized teeth were evaluated at 3, 6, and 9 mon clinically and radiographically, based on the scoring criteria system.
Results The clinical success rates were found to be similar among the three groups at 3 and 6 mon where as a significant decrease in success rate was observed in Group III (84%) compared to both Group I (100%) and Group II (100%) at 9 mon. Radiographic success rates over a period of 9 mon in Groups I, II, and III were 92, 80, and 72%, respectively.
Conclusions Teeth treated with MTA and Biodentine showed more favorable clinical and radiographic success as compared to Propolis at 9 mon follow-up.
-
Citations
Citations to this article as recorded by- Histological Tissue Response to Calcium Silicate-Based Cements Assessed in Human Tooth Culture Models: A Systematic Review
Alberto Cabrera-Fernández, Hebertt Gonzaga dos Santos Chaves, Aránzazu Díaz-Cuenca, Juan J. Segura-Egea, Jenifer Martín-González, João Peça, Diana B. Sequeira, João Miguel Marques dos Santos
Journal of Functional Biomaterials.2026; 17(2): 78. CrossRef - The Clinical Effectiveness of Propolis on the Endodontic Treatment of Permanent Teeth: A Systematic Review of Randomized Clinical Trials and Updates
Amirah Y Aldosari, Amira M Aljared, Hanin S Alqurshy, Abdullah M Alfarran, Mohanad G Alnahdi, Sarah S Alharbi, Wed S Alharbi, Faisal T Alghamdi
Cureus.2025;[Epub] CrossRef - Natural nanoparticles versus the gold standard in direct pulp capping: a randomized clinical trial
Dalia M. Elasser, Sabah M. Sobhy, Rania Rashad Omar Taha, Nevin A. Gad, Dina M. Abdel-Ghany
The Saudi Dental Journal.2025;[Epub] CrossRef - Systematic review and meta analysis of first and second generation bioceramic materials in primary dentition pulpotomies
João Albernaz Neves, Luísa Bandeira Lopes, Marta Alves Duarte, José João Mendes, Tiago Pimentel
Scientific Reports.2025;[Epub] CrossRef - EFFICACY OF BIODENTINE VERSUS MINERAL TRIOXIDE AGGREGATE IN PULPOTOMY FOR PRIMARY TEETH: A SYSTEMATIC REVIEW AND META-ANALYSIS OF RANDOMIZED CONTROLLED TRIALS
KORINA YUN-FAN LU, JENNIFER L. GIBBS, CHENG-YU WU, MARKUS B. BLATZ, XUEHAO MA, MIN-WEN FU, KEVIN SHENG-KAI MA
Journal of Evidence-Based Dental Practice.2025; 25(4): 102191. CrossRef - Calcium Silicate-Based Cements in Restorative Dentistry: Vital Pulp Therapy Clinical, Radiographic, and Histological Outcomes on Deciduous and Permanent Dentition—A Systematic Review and Meta-Analysis
Maria Teresa Xavier, Ana Luísa Costa, João Carlos Ramos, João Caramês, Duarte Marques, Jorge N. R. Martins
Materials.2024; 17(17): 4264. CrossRef - Outcome assessment methods of bioactive and biodegradable materials as pulpotomy agents in primary and permanent teeth: a scoping review
Yasmine Elhamouly, May M. Adham, Karin M L Dowidar, Rania M. El Backly
BMC Oral Health.2024;[Epub] CrossRef - Comparative Evaluation of the Efficacy of Theracal Lc, Mineral Trioxide Aggregate, and Biodentine As Direct Pulp Capping Materials in Patients With Pulpal Exposure in Posterior Teeth: A Triple Blinded Randomized Parallel Group Clinical Trial
Joyeeta Mahapatra, Pradnya P Nikhade, Aditya Patel, Nikhil Mankar, Prachi Taori
Cureus.2024;[Epub] CrossRef - Efficacy of different endodontic irrigants in the lesion sterilization and tissue repair technique in primary molars: A randomized controlled clinical trial
Anukriti Dimri, Nikhil Srivastava, Vivek Rana, Noopur Kaushik
Journal of Indian Society of Pedodontics and Preventive Dentistry.2024; 42(4): 294. CrossRef - Clinical and Radiographic Success Rates of Pulpotomies in Primary Molars Treated with Formocresol, BiodentineTM, and Endo Repair: A Randomized Clinical Trial
Elham Farokh Gisour, Farzaneh Jalali, Fatemeh Jahanimoghadam, Tania Dehesh
Pesquisa Brasileira em Odontopediatria e Clínica Integrada.2023;[Epub] CrossRef - Evaluation and comparison of mineral trioxide aggregate and cold ceramic in primary tooth pulpotomy: Clinical and radiographic study
Bita Rasteh, Leila Basir, Shirin Taravati, Masoumeh Khataminia
Journal of Family Medicine and Primary Care.2023; 12(12): 3068. CrossRef - Comparison between the Radiographic and Clinical Rates of Success for TheraCal and MTA in Primary Tooth Pulpotomy within a 12‐Month Follow‐Up: A Split‐Mouth Clinical Trial
Sedigheh Hassanpour, Naser Asl Aminabadi, Mahdi Rahbar, Leila Erfanparast, Iole Vozza
BioMed Research International.2023;[Epub] CrossRef - Biodentine™ Pulpotomy in Stage I Primary Molars: A 12-month Follow-up
Hitaf Nasrallah, Balsam Noueiri
International Journal of Clinical Pediatric Dentistry.2023; 15(6): 660. CrossRef - Omega 3 based formulations as new possible pulpotomy agents for primary teeth
Nancy M. Metwally, Amina M. El Hosary, Gamal M. El Maghraby, Maha A. El Demellawy, Mohamed Nabil, Elsayed M. Deraz
Tanta Dental Journal.2022; 19(4): 287. CrossRef - Clinical efficacy of Er:YAG laser application in pulpotomy of primary molars: a 2-year follow-up study
Junhui Wang, Yujiang Chen, Baize Zhang, Xin Ge, Xiaojing Wang
Lasers in Medical Science.2022; 37(9): 3705. CrossRef - Comparative efficacy of medicaments or techniques for pulpotomy of primary molars: a network meta-analysis
Jiehua Guo, Na Zhang, Yuzhao Cheng
Clinical Oral Investigations.2022; 27(1): 91. CrossRef - Comparative evaluation of zinc oxide-eugenol and zinc oxide with Neem oil in root canal treatment of primary teeth
Dhvani Gordhanbhai Patel, Shoba Fernandes, Yash Bafna, Krunal Choksi, Shaila Chaudhary, Priya Mishra
AYU (An International Quarterly Journal of Research in Ayurveda).2022; 43(1): 8. CrossRef - Treatment Outcomes of Pulpotomy with Propolis in Comparison with MTA in Human Primary Molars: A 24-month Follow-up Randomized Controlled Trial
Kakarla Sri RojaRamya, Rayala Chandrasekhar, KS Uloopi, C Vinay
International Journal of Clinical Pediatric Dentistry.2022; 15(S1): S3. CrossRef - Comparison of Clinical and Radiographic Success between MTA and Biodentine in Pulpotomy of Primary Mandibular Second Molars with Irreversible Pulpitis: A Randomized Double‐Blind Clinical Trial
Alireza Eshghi, Maryam Hajiahmadi, Mohammad Hossein Nikbakht, Mona Esmaeili, Murilo Baena Lopes
International Journal of Dentistry.2022;[Epub] CrossRef - Does the use of natural products for endodontic therapy in primary teeth have sufficient evidence for clinical practice? A scoping review
Filipe Colombo Vitali, Ana Cristina Andrada, Helhen Cristina da Luz Cardoso, Gesner Francisco Xavier-Junior, Cleonice da Silveira Teixeira, Loise Pedrosa Salles, Erica Negrini Lia, Carla Massignan
Clinical Oral Investigations.2022; 26(10): 6043. CrossRef - Prevalence of pain following single-visit pulpectomy with stainless steel crown done by postgraduate students in a university sitting
Ashwin Shravan Kumar, Mahesh Ramakrishnan
Journal of Advanced Pharmaceutical Technology & Research.2022; 13(Suppl 1): S177. CrossRef - Clinical and histological response of human pulp tissue to direct pulp capping with mineral trioxide aggregate, Biodentine and propolis
Zahra Nasri, MaryamZare Jahromi, Atousa Aminzadeh
Dental Research Journal.2022; 19(1): 40. CrossRef - Long-term evaluation of primary teeth molar pulpotomies with Biodentine and MTA: a CONSORT randomized clinical trial
S. Vilella-Pastor, S. Sáez, A. Veloso, F. Guinot-Jimeno, M. Mercadé
European Archives of Paediatric Dentistry.2021; 22(4): 685. CrossRef - Tailored 70S30C Bioactive glass induces severe inflammation as pulpotomy agent in primary teeth: an interim analysis of a randomised controlled trial
Yasmine Elhamouly, Rania M. El Backly, Dalia M. Talaat, Samia S. Omar, Maha El Tantawi, Karin M. L. Dowidar
Clinical Oral Investigations.2021; 25(6): 3775. CrossRef - Efficacy of laser photobiomodulation pulpotomy in human primary teeth
Chandrashekar Murugesh Yavagal, Akshaya Lal, Viplavi Vijaysinh Chavan Patil, Puja C. Yavagal, Kiran Kumar Neelakantappa, Madhu Hariharan
Journal of Indian Society of Pedodontics and Preventive Dentistry.2021; 39(4): 436. CrossRef - SÜT DİŞİ AMPUTASYON TEDAVİSİNDE GÜNCEL YAKLAŞIMLAR
Necibe Damla ŞAHİN, Volkan ARIKAN
Atatürk Üniversitesi Diş Hekimliği Fakültesi Dergisi.2021; : 1. CrossRef - The use of propolis in dentistry, oral health, and medicine: A review
Felix Zulhendri, Rafael Felitti, James Fearnley, Munir Ravalia
Journal of Oral Biosciences.2021; 63(1): 23. CrossRef - Clinical and radiographic evaluation of pulpotomy using MTA, Biodentine and Er,Cr:YSGG laser in primary teeth. A clinical study
Pandiyan Ramanandvignesh, Kumar Gyanendra, Dhillon Jatinder Kaur Goswami Mridula
Laser Therapy.2020; 29(1): 29. CrossRef - Comparative Evaluation of Success of Biodentine and Mineral Trioxide Aggregate with Formocresol as Pulpotomy Medicaments in Primary Molars: An In Vivo Study
Ritika Malhotra, Shilpa Ahuja, Dipanshu Kumar, Kapil Gandhi, Rishabh Kapoor, Kumari Surabhi
International Journal of Clinical Pediatric Dentistry.2020; 13(2): 167. CrossRef - Comparison of Partial Pulpotomy in Permanent Molars Using Different Pulp Capping Agents and Restoration Materials
Jimi Lee, Nanyoung Lee, Sangho Lee, Myeongkwan Jih
THE JOURNAL OF THE KOREAN ACADEMY OF PEDTATRIC DENTISTRY.2020; 47(2): 148. CrossRef - A Comparative Evaluation between Propolis and Mineral Trioxide Aggregate as Pulpotomy Medicaments in Primary Molars
Kavita Madan, Sudhindra Baliga, Pranjali Deulkar, Nilima Thosar, Nilesh Rathi, Meghana Deshpande, Sphurti Bane
Journal of Evolution of Medical and Dental Sciences.2020; 9(15): 1256. CrossRef - Efficacy of Biodentine and Mineral Trioxide Aggregate in Primary Molar Pulpotomies—A Systematic Review and Meta-Analysis With Trial Sequential Analysis of Randomized Clinical Trials
Venkateshbabu Nagendrababu, Shaju Jacob Pulikkotil, Sajesh K. Veettil, Peerawat Jinatongthai, James L. Gutmann
Journal of Evidence Based Dental Practice.2019; 19(1): 17. CrossRef - Efficacy of Alternative Medicaments for Pulp Treatment in Primary Teeth in the Short Term: A Meta-analysis
Joon Soo Park, Bosky Jasani, Jilen Patel, Robert P. Anthonappa, Nigel M. King
Journal of Evidence Based Dental Practice.2019; 19(4): 101309. CrossRef - The evaluation of MTA and Biodentine as a pulpotomy materials for carious exposures in primary teeth
Burcu Nihan Çelik, Merve Safa Mutluay, Volkan Arıkan, Şaziye Sarı
Clinical Oral Investigations.2019; 23(2): 661. CrossRef - Effects of MTA and Brazilian propolis on the biological properties of dental pulp cells
Bingqing Shi, Yuming Zhao, Xiaojing Yuan
Brazilian Oral Research.2019;[Epub] CrossRef - MTA and biodentine for primary teeth pulpotomy: a systematic review and meta-analysis of clinical trials
Emyr Stringhini Junior, Manuela Gouvêa Campêlo dos Santos, Luciana Butini Oliveira, Montse Mercadé
Clinical Oral Investigations.2019; 23(4): 1967. CrossRef - Comparison of the success rate of a bioactive dentin substitute with those of other root restoration materials in pulpotomy of primary teeth
Hooman Shafaee, Mehrnoosh Alirezaie, Abdolrasoul Rangrazi, Erfan Bardideh
The Journal of the American Dental Association.2019; 150(8): 676. CrossRef - BiodentineTM versus formocresol pulpotomy technique in primary molars: a 12–month randomized controlled clinical trial
Omar Abd El Sadek El Meligy, Najlaa Mohamed Alamoudi, Sulaiman Mohamed Allazzam, Azza Abdel Mohsen El-Housseiny
BMC Oral Health.2019;[Epub] CrossRef - Randomized Controlled Trial of Pulpotomy in Primary Molars using MTA and Formocresol Compared to 3Mixtatin: A Novel Biomaterial
Zahra Jamali, Vajiheh Alavi, Ebrahim Najafpour, Naser Asl Aminabadi, Sajjad Shirazi
Journal of Clinical Pediatric Dentistry.2018; 42(5): 361. CrossRef - Recent Trends in Tricalcium Silicates for Vital Pulp Therapy
Imad About
Current Oral Health Reports.2018; 5(3): 178. CrossRef - Clinical and Radiographic Evaluations of Biodentine™ Pulpotomies in Mature Primary Molars (Stage 2)
Fouad Ayoub, Hitaf Nasrallah, Balsam El Noueiri, Charles Pilipili
International Journal of Clinical Pediatric Dentistry.2018; 11(6): 496. CrossRef - Clinical and radiographic evaluation of biodentine versus calcium hydroxide in primary teeth pulpotomies: a retrospective study
Silvia Caruso, Teresa Dinoi, Giuseppe Marzo, Vincenzo Campanella, Maria Rita Giuca, Roberto Gatto, Marco Pasini
BMC Oral Health.2018;[Epub] CrossRef - How does the pulpal response to Biodentine and ProRoot mineral trioxide aggregate compare in the laboratory and clinic?
R. Careddu, H. F. Duncan
British Dental Journal.2018; 225(8): 743. CrossRef - Mineral trioxide aggregate and other bioactive endodontic cements: an updated overview – part I: vital pulp therapy
M. Parirokh, M. Torabinejad, P. M. H. Dummer
International Endodontic Journal.2018; 51(2): 177. CrossRef - Pulp treatment for extensive decay in primary teeth
Violaine Smaïl-Faugeron, Anne-Marie Glenny, Frédéric Courson, Pierre Durieux, Michele Muller-Bolla, Helene Fron Chabouis
Cochrane Database of Systematic Reviews.2018;[Epub] CrossRef - Biodentine™ material characteristics and clinical applications: a 3 year literature review and update
S. Rajasekharan, L. C. Martens, R. G. E. C. Cauwels, R. P. Anthonappa
European Archives of Paediatric Dentistry.2018; 19(1): 1. CrossRef - Microleakage and Shear Bond Strength of Biodentine at Different Setting Time
Yong Ho Song, Nanyoung Lee, Sangho Lee, Myeongkwan Jih
THE JOURNAL OF THE KOREAN ACADEMY OF PEDTATRIC DENTISTRY.2018; 45(3): 344. CrossRef - Evaluation of Biodentine Pulpotomies in Deciduous Molars with Physiological Root Resorption (Stage 3)
Fouad Ayoub, Hitaf Nasrallah, Balsam El Noueiri, Charles Pilipili
International Journal of Clinical Pediatric Dentistry.2018; 11(5): 393. CrossRef - Clinical and radiographic comparison of biodentine, mineral trioxide aggregate and formocresol as pulpotomy agents in primary molars
P. Juneja, S. Kulkarni
European Archives of Paediatric Dentistry.2017; 18(4): 271. CrossRef - Success Rates of Pulpotomies in Primary Molars Using Calcium Silicate-Based Materials: A Randomized Control Trial
Yeliz Guven, Sermin Dicle Aksakal, Nilufer Avcu, Gulcan Unsal, Elif Bahar Tuna, Oya Aktoren
BioMed Research International.2017; 2017: 1. CrossRef - Biodentine: from biochemical and bioactive properties to clinical applications
Imad About
Giornale Italiano di Endodonzia.2016; 30(2): 81. CrossRef
- Histological Tissue Response to Calcium Silicate-Based Cements Assessed in Human Tooth Culture Models: A Systematic Review
- 3,670 View
- 36 Download
- 51 Crossref
- A preliminary report on histological outcome of pulpotomy with endodontic biomaterials vs calcium hydroxide
- Ali Nosrat, Ali Peimani, Saeed Asgary
- Restor Dent Endod 2013;38(4):227-233. Published online November 12, 2013
- DOI: https://doi.org/10.5395/rde.2013.38.4.227
-
Abstract
PDFPubReaderePub
Objectives The purpose of the study was to evaluate human dental pulp response to pulpotomy with calcium hydroxide (CH), mineral trioxide aggregate (MTA), and calcium enriched mixture (CEM) cement.
Materials and Methods A total of nine erupted third molars were randomly assigned to each pulpotomy group. The same clinician performed full pulpotomies and coronal restorations. The patients were followed clinically for six months; the teeth were then extracted and prepared for histological assessments. The samples were blindly assessed by an independent observer for pulp vitality, pulp inflammation, and calcified bridge formation.
Results All patients were free of clinical signs/symptoms of pulpal/periradicular diseases during the follow up period. In CH group, one tooth had necrotic radicular pulp; other two teeth in this group had vital uninflamed pulps with complete dentinal bridge formation. In CEM cement and MTA groups all teeth had vital uninflamed radicular pulps. A complete dentinal bridge was formed beneath CEM cement and MTA in all roots. Odontoblast-like cells were present beneath CEM cement and MTA in all samples.
Conclusions This study revealed that CEM cement and MTA were reliable endodontic biomaterials in full pulpotomy treatment. In contrast, the human dental pulp response to CH might be unpredictable.
-
Citations
Citations to this article as recorded by- Long-term Outcome of Vital Pulp Therapy and Regenerative Endodontic Procedures in Immature Permanent Maxillary Incisors: A 7-year Follow-up Case Report
Mulham Almaliki, Motaz Almaghraby, Abdulaziz Bakhsh
International Journal of Clinical Pediatric Dentistry.2026; 19(3): 403. CrossRef - A meta‐analysis of calcium silicate‐based cements and calcium hydroxide as promoters of hard tissue bridge formation
Emmanuel J. N. L. Silva, Karem P. Pinto, Fernanda N. S. J. Riche, Maristela G. H. Carestiato, Jorge N. R. Martins, Henry F. Duncan, Marco A. Versiani, Gustavo De‐Deus
International Endodontic Journal.2025; 58(5): 685. CrossRef - Clinical and radiographic outcomes of pulpotomy materials in permanent teeth: a systematic review of calcium hydroxide, MTA, biodentine, and iRoot BP plus
Anggi Putri Riandani, Arief Cahyanto, Rana Abdelbaset Lotfy Diab, Ratih Widyasari, Atia Nurul Sidiqa, Hendra Dian Adhita Dharsono, Myrna Nurlatifah Zakaria
BMC Oral Health.2025;[Epub] CrossRef - Comprehensive review of composition, properties, clinical applications, and future perspectives of calcium-enriched mixture (CEM) cement: a systematic analysis
Saeed Asgary, Mahtab Aram, Mahta Fazlyab
BioMedical Engineering OnLine.2024;[Epub] CrossRef - Hard tissue formation in pulpotomized primary teeth in dogs with nanomaterials MCM-48 and MCM-48/hydroxyapatite: an in vivo animal study
Sahar Talebi, Nosrat Nourbakhsh, Ardeshir Talebi, Amir Abbas Nourbakhsh, Abbas Haghighat, Maziar Manshayi, Hamid Reza Bakhsheshi, Razieh Karimi, Rahman Nazeri, Kenneth J.D. Mackenzie
BMC Oral Health.2024;[Epub] CrossRef - The Role of Growth Factor Delivery Systems on Cellular Activities of Dental
Stem Cells: A Systematic Review (Part II)
Sayna Shamszadeh, Armin Shirvani, Saeed Asgary
Current Stem Cell Research & Therapy.2024; 19(4): 587. CrossRef - Calcium Silicate-Based Cements in Restorative Dentistry: Vital Pulp Therapy Clinical, Radiographic, and Histological Outcomes on Deciduous and Permanent Dentition—A Systematic Review and Meta-Analysis
Maria Teresa Xavier, Ana Luísa Costa, João Carlos Ramos, João Caramês, Duarte Marques, Jorge N. R. Martins
Materials.2024; 17(17): 4264. CrossRef - Pulpotomy: An alternative treatment modality to conventional root canal treatment
Günther Streit, Martin Vorster, Peet J Van der Vyver
South African Dental Journal.2023; 78(06): 309. CrossRef - A Comparative Histological Analysis of Human Pulp Following Direct Pulp Capping with Propolis or Biodentine
Nehad A Ahmad, Nevin A. Gad, Marwa H. Abdulmonaem
Journal of Nature and Science of Medicine.2022; 5(3): 281. CrossRef - Expression of Matrix Metalloproteinases-8 and Myeloperoxidase in Pulp Tissue after Pulpotomy with Calcium Silicate Cements
Nayara Nery de Oliveira Cunha, Marina Azevedo Junqueira, Leopoldo Cosme-Silva, Laís da Silveira Terra Santos, George Augusto Veloso de Oliveira, Rafael Tobias Moretti Neto, Denismar Alves Nogueira, Maísa Ribeiro Pereira Lima Brigagão, Ana Beatriz da Silve
Pesquisa Brasileira em Odontopediatria e Clínica Integrada.2021;[Epub] CrossRef - Long-term Outcomes of Full Pulpotomy in Permanent Molars for Patients Treated in a Single, Short Session under Special Conditions
Natacha Linas, Nicolas Decerle, Marie-Laure Munoz-Sanchez, Denise Faulks, Valérie Collado, Emmanuel Nicolas, Martine Hennequin, Pierre-Yves Cousson
Journal of Endodontics.2020; 46(11): 1597. CrossRef - Quantitative Assessment of Root Development after Regenerative Endodontic Therapy: A Systematic Review and Meta-Analysis
Teng Kai Ong, Ghee Seong Lim, Maharaj Singh, Alissa V. Fial
Journal of Endodontics.2020; 46(12): 1856. CrossRef - Dexamethasone- loaded polymeric porous sponge as a direct pulp capping agent
Amjad Alagha, Abdulwahab Nourallah, Sahar Alhariri
Journal of Biomaterials Science, Polymer Edition.2020; 31(13): 1689. CrossRef - Postendodontic Pain after Pulpotomy or Root Canal Treatment in Mature Teeth with Carious Pulp Exposure: A Multicenter Randomized Controlled Trial
Mohammad Jafar Eghbal, Ali Haeri, Arash Shahravan, Ali Kazemi, Fariborz Moazami, Mohammad Ali Mozayeni, Eshaghali Saberi, Mohammad Samiei, Mehdi Vatanpour, Alireza Akbarzade Baghban, Mahta Fazlyab, Ardavan Parhizkar, Mahboobe Ahmadi, Nazila Akbarian Rad,
Pain Research and Management.2020; 2020: 1. CrossRef - Vital Pulp Therapy as a Conservative Approach for Management of Invasive Cervical Root Resorption: A Case Series
Saeed Asgary, Mahdieh Nourzadeh, Prashant Verma, M. Lamar Hicks, Ali Nosrat
Journal of Endodontics.2019; 45(9): 1161. CrossRef - Which procedures and materials could be applied for full pulpotomy in permanent mature teeth? A systematic review
M. Zanini, M. Hennequin, PY. Cousson
Acta Odontologica Scandinavica.2019; 77(7): 541. CrossRef - Periodontal healing following non-surgical repair of an old perforation with pocket formation and oral communication
Saeed Asgary, Prashant Verma, Ali Nosrat
Restorative Dentistry & Endodontics.2018;[Epub] CrossRef - Mineral trioxide aggregate and other bioactive endodontic cements: an updated overview – part I: vital pulp therapy
M. Parirokh, M. Torabinejad, P. M. H. Dummer
International Endodontic Journal.2018; 51(2): 177. CrossRef - Treatment Outcomes of 4 Vital Pulp Therapies in Mature Molars
Saeed Asgary, Raheleh Hassanizadeh, Hassan Torabzadeh, Mohammad Jafar Eghbal
Journal of Endodontics.2018; 44(4): 529. CrossRef - A Review of Criteria for the Evaluation of Pulpotomy Outcomes in Mature Permanent Teeth
Marjorie Zanini, Martine Hennequin, Pierre-Yves Cousson
Journal of Endodontics.2016; 42(8): 1167. CrossRef - Calcium-Enriched Mixture Pulpotomy of Primary Molar Teeth with Irreversible Pulpitis. A Clinical Study
Mahtab Memarpour, Soleiman Fijan, Saeed Asgary, Marzieh Keikhaee
The Open Dentistry Journal.2016; 10(1): 43. CrossRef - Endodontie in der unreifen bleibenden Dentition — Maßnahmen zur Vitalerhaltung, Apexifikation und Regeneration der Pulpa
Martin Jung
Oralprophylaxe & Kinderzahnheilkunde.2016; 38(1): 29. CrossRef - Conservative Management of Class 4 Invasive Cervical Root Resorption Using Calcium-enriched Mixture Cement
Saeed Asgary, Ali Nosrat
Journal of Endodontics.2016; 42(8): 1291. CrossRef - Permanent teeth pulpotomy survival analysis: retrospective follow-up
Gustavo Golgo Kunert, Itaborai Revoredo Kunert, Luiz Cesar da Costa Filho, José Antônio Poli de Figueiredo
Journal of Dentistry.2015; 43(9): 1125. CrossRef - Cytocompatibility and Antibacterial Properties of Capping Materials
Claudio Poggio, Carla Renata Arciola, Riccardo Beltrami, Annachiara Monaco, Alberto Dagna, Marco Lombardini, Livia Visai
The Scientific World Journal.2014; 2014: 1. CrossRef - Surgical management of a failed internal root resorption treatment: a histological and clinical report
Saeed Asgary, Mohammad Jafar Eghbal, Leili Mehrdad, Sanam Kheirieh, Ali Nosrat
Restorative Dentistry & Endodontics.2014; 39(2): 137. CrossRef - Effect of Mineral Trioxide Aggregate Surface Treatments on Morphology and Bond Strength to Composite Resin
Joo-Hee Shin, Ji-Hyun Jang, Sang Hyuk Park, Euiseong Kim
Journal of Endodontics.2014; 40(8): 1210. CrossRef
- Long-term Outcome of Vital Pulp Therapy and Regenerative Endodontic Procedures in Immature Permanent Maxillary Incisors: A 7-year Follow-up Case Report
- 3,034 View
- 18 Download
- 27 Crossref
 First
First Prev
Prev

