
Search
- Page Path
- HOME > Search
Research Articles
- Fracture resistance of regenerated immature teeth in different simulated stages of root development: an in vitro cyclic loading study
- Kyveli-Artemis Polydora, Konstantinos Kodonas, Anastasia Fardi, Christos Gogos
- Restor Dent Endod 2026;51(2):e21. Published online April 28, 2026
- DOI: https://doi.org/10.5395/rde.2026.51.e21
-
 Abstract
Abstract
 PDF
PDF Supplementary Material
Supplementary Material PubReader
PubReader ePub
ePub - Objectives
This in vitro study aimed to assess the fracture resistance of simulated stages of root maturation following regenerative endodontic treatment using a cyclic loading method.
Methods
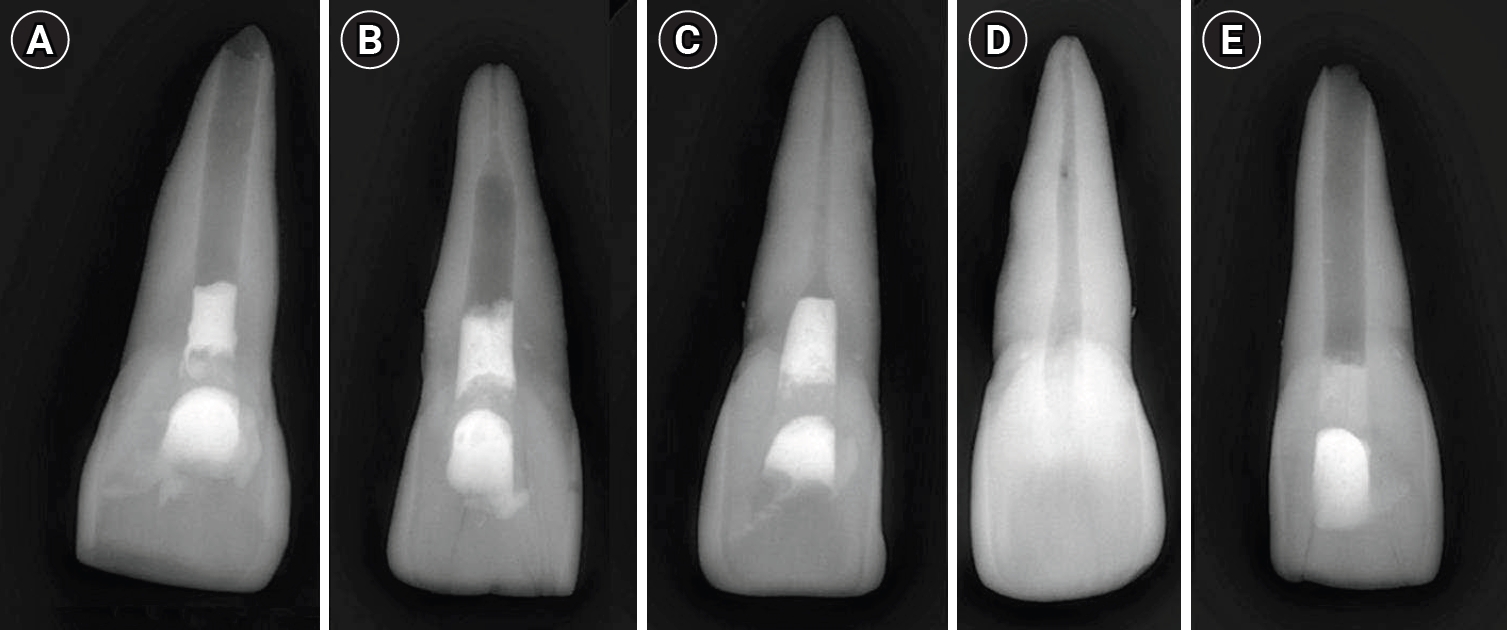
Ninety extracted maxillary central incisors were randomly allocated into three experimental groups representing different stages of root development, following revitalization: Group A for completely immature teeth immediately after treatment; Group B for teeth with apical closure, and Group C for teeth with apical closure and wall thickening. Two control groups were also included: Group D for intact teeth and Group E for simulated immature teeth without the bioceramic material. Following simulation of immature apices and treatment with a bioceramic material, all specimens were subjected to cyclic loading using a step-stress fatigue protocol until failure. The number of cycles to fracture and the peak load were recorded and statistically analyzed.
Results
Statistically significant differences in loading forces were observed between the negative control group (Group D) and Groups A, B, and E (p < 0.05). However, no statistically significant differences were detected among the experimental groups. These results indicate that apical closure and dentinal wall thickening alone did not substantially improve mechanical reinforcement under cyclic loading conditions.
Conclusions
Although intact teeth exhibited superior mechanical performance, apical closure and wall thickening alone were insufficient to enhance reinforcement under cyclic loading.
- 1,050 View
- 104 Download

- Fracture resistance and failure modes of endodontically-treated permanent teeth restored with Ribbond posts vs other post systems: a systematic review and meta-analysis of in vitro studies
- Meghana Aditya Vartak, Vibha Rahul Hegde, Sanitra Rahul Hegde, Ushaina Fanibunda
- Restor Dent Endod 2025;50(1):e5. Published online February 17, 2025
- DOI: https://doi.org/10.5395/rde.2025.50.e5

-
Abstract
PDFPubReaderePub
- Objectives
This systematic review aimed to investigate the fracture resistance and mode of failure of endodontically-treated permanent teeth restored with Ribbond posts (Ribbond, Inc.) compared with endodontically-treated permanent teeth restored with other post systems.
Methods
A comprehensive, systematic literature search was carried out using several electronic databases: MEDLINE/PubMed, Google Scholar, and Cochrane Library. Two separate researchers were appointed to identify the studies meeting the eligibility criteria, and to perform the data extraction, risk of bias, and quality assessment.
Results
Twelve studies were included in the quantitative analysis. Meta-analysis was performed with 11 of the 12 included articles. The meta-analysis showed that Ribbond posts have a fracture strength less than prefabricated metal posts, cast metal posts, and prefabricated fiber posts and greater than custom e-glass fiber posts. Mode of failure analysis revealed that Ribbond posts have the most favorable non-catastrophic fractures.
Conclusions
Although Ribbond posts have lower fracture resistance, their favorable mode of failure makes them potentially the most biomimetic post system. -
Citations
Citations to this article as recorded by
- Clinical Outcomes of Nonmetallic Customized Post-and-Core Systems: A Systematic Review
Jonathan Jun Xian Yuen, Yew Hin Beh, Zhi Kuan Saw, Hock Siang Chua
Journal of Endodontics.2026; 52(4): 525. CrossRef - Fracture Resistance of Extensively Compromised Anterior Teeth Restored With Fiberglass Posts and Biomimetic Protocols: An In Vitro Study
Chiu Tzyy Haur, Emanuel Ewerton Mendonça Vasconcelos, Natália Gomes de Oliveira, Gabriela Queiroz de Melo Monteiro, Luís Felipe Espíndola‐Castro
Journal of Esthetic and Restorative Dentistry.2026; 38(4): 874. CrossRef - Effect of Short and Long Fiber-Reinforced Composite Resins Used as Post and Core on Fracture Resistance of Premolars: An in vitro Study
Manal Hussian Abd-alla, Tuqa Jameel Ebrahim, Ahmed Sleibi Mustafa
Al-Rafidain Journal of Medical Sciences ( ISSN 2789-3219 ).2026; 10(1): 66. CrossRef - Study of the Effect of the Resin Matrix Type of Glass Fiber Posts on their Retention Within the Root Canal “An In Vitro Study”
Tarek Sheikh Salem, Maysam Khaddam, Nadim Sleman
The Open Dentistry Journal.2026;[Epub] CrossRef - Effect of three post systems on the fracture resistance of teeth with extensive coronal structure loss and internal resorption
Melis Oya Ateş, Esma Dinger, Kubra Degirmenci, Furkan Yılmaz, Dilaycan Uğureli
The Journal of Advanced Prosthodontics.2026; 18(2): 70. CrossRef - Polyethylene fiber reinforcement in resin composite restorations: A systematic review of clinical trials
Rim Bourgi, Ahmed A. Holiel, António HS Delgado, Abigailt Flores-Ledesma, Souheir Khafaja, Carlos Enrique Cuevas-Suárez
Dentistry Review.2026; 6(2): 100422. CrossRef - Fracture resistance of endodontically treated teeth restored with polyetheretherketone (PEEK) versus glass fiber posts: A comparative in vitro analysis
Manduwada Vishal, Neha Mehra, Mamta Kaushik, Prabakaran Saravanan
Endodontology.2026; 38(2): 172. CrossRef - Influence of Different Post-core Restorative Modalities on Fracture Characteristics of Immature Endodontically Treated Premolars
Wafa H Alaajam, Khalid M Abdelaziz, Malaz M Mustafa, Mohammed S Al-Ak'hali, Ashraf A Khalil, Mohammed M Al Moaleem, Hoda L Abouzeid
The Journal of Contemporary Dental Practice.2026; 27(4): 399. CrossRef - Biomimetic rehabilitation of a structurally compromised endodontically treated tooth using deep margin elevation and polyethylene fiber–reinforced post and core: a case report
Derek Shaji Pious, Chitharanjan M. Shetty, Maria Anna Geevarghis, Sunheri Bajpe, Rashi Shroff
Frontiers in Dental Medicine.2026;[Epub] CrossRef - Análise comparativa dos aspectos biomecânicos dos pinos de fibra de vidro e fibra de polietileno (RIBBOND) - revisão de literatura
Ana Kamily da Cunha Silva, Tânia Regina Carvalho de Sá, Livia Duarte Santos Lopes de Carvalho, Lilian Gomes Soares Pires, Marconi Raphael de Siqueira Rego, Matheus Araújo Brito Santos Lopes
RCMOS - Revista Científica Multidisciplinar O Saber.2025;[Epub] CrossRef - Biomimetic Strategies for the Rehabilitation of Compromised Anterior Teeth
Aakansha Puri, M.S. Prathap
Contemporary Clinical Dentistry.2025; 16(3): 218. CrossRef - Evaluation of fracture resistance and crack propensity of bulk-fill composite restorations reinforced by polyethylene fiber
Ayşe Aslı Şenol, Aybike Manav, Bengü Doğu Kaya, Pınar Yılmaz Atalı, Erkut Kahramanoğlu, Bilge Tarçın, Cafer Türkmen
BMC Oral Health.2025;[Epub] CrossRef - A Comparative Study on the Fracture Resistance of CAD/CAM–Fabricated Single‐Piece Post‐Crowns
Ali Erdem, Mehmet Selim Bilgin, Ibrahim Ersoy, Erhan Dilber, Ebru Nur Işık, Tan Fırat Eyüboğlu, Mutlu Özcan
Clinical and Experimental Dental Research.2025;[Epub] CrossRef - CAD/CAM Technologies in Post and Core Restoration of Endodontically Treated Teeth: Current Evidence, Clinical Applications, and Interdisciplinary Perspectives
Rawabi Abdulrahman Ahmed, Faris Ali Aseri, Ahmed Saleh Alammari, Zaher Saleh Asiri, Fahad Oudah Al Matir, Sami Safar Al Shahrani, Abdullah Ali Alharthi, Abdulaziz Ahmed Alfaifi, Hassan Yahya Hassan Asiri, Hassan Manea Ali Al Fotais, Amal Mali Almutairi, A
Journal of Clinical Practice and Medical Research.2025; 1(3): 178. CrossRef
- Clinical Outcomes of Nonmetallic Customized Post-and-Core Systems: A Systematic Review
- 15,339 View
- 671 Download
- 9 Web of Science
- 14 Crossref
- Effects of different calcium-silicate based materials on fracture resistance of immature permanent teeth with replacement root resorption and osteoclastogenesis
- Gabriela Leite de Souza, Gabrielle Alves Nunes Freitas, Maria Tereza Hordones Ribeiro, Nelly Xiomara Alvarado Lemus, Carlos José Soares, Camilla Christian Gomes Moura
- Restor Dent Endod 2023;48(2):e21. Published online May 5, 2023
- DOI: https://doi.org/10.5395/rde.2023.48.e21
-
Abstract
PDFSupplementary MaterialPubReaderePub
Objectives This study evaluated the effects of Biodentine (BD), Bio-C Repair (BCR), and mineral trioxide aggregate (MTA) plug on the fracture resistance of simulated immature teeth with replacement root resorption (RRR) and
in vitro -induced osteoclastogenesis.Materials and Methods Sixty bovine incisors simulating immature teeth and RRR were divided into 5 groups: BD and BCR groups, with samples completely filled with the respective materials; MTA group, which utilized a 3-mm apical MTA plug; RRR group, which received no root canal filling; and normal periodontal ligament (PL) group, which had no RRR and no root canal filling. All the teeth underwent cycling loading, and compression strength testing was performed using a universal testing machine. RAW 264.7 macrophages were treated with 1:16 extracts of BD, BCR, and MTA containing receptor activator of nuclear factor-kappa B ligand (RANKL) for 5 days. RANKL-induced osteoclast differentiation was assessed by staining with tartrate-resistant acid phosphatase. The fracture load and osteoclast number were analyzed using 1-way ANOVA and Tukey’s test (α = 0.05).
Results No significant difference in fracture resistance was observed among the groups (
p > 0.05). All materials similarly inhibited osteoclastogenesis (p > 0.05), except for BCR, which led to a lower percentage of osteoclasts than did MTA (p < 0.0001).Conclusions The treatment options for non-vital immature teeth with RRR did not strengthen the teeth and promoted a similar resistance to fractures in all cases. BD, MTA, and BCR showed inhibitory effects on osteoclast differentiation, with BCR yielding improved results compared to the other materials.
-
Citations
Citations to this article as recorded by- Effect of Restoration Strategy and Cavity Location on the Fracture Resistance of Teeth with External Cervical Resorption
Saadet Elpe, Öznur Sarıyılmaz
Journal of Endodontics.2026; 52(6): 980. CrossRef - Influence of Different Post-core Restorative Modalities on Fracture Characteristics of Immature Endodontically Treated Premolars
Wafa H Alaajam, Khalid M Abdelaziz, Malaz M Mustafa, Mohammed S Al-Ak'hali, Ashraf A Khalil, Mohammed M Al Moaleem, Hoda L Abouzeid
The Journal of Contemporary Dental Practice.2026; 27(4): 399. CrossRef - In vitro comparison of fracture strength of maxillary incisors with the simulated external root resorption cavities repaired with BioMTA or Biodentine
Tufan Ozasir, Birgul Ozasir, Nagihan Aribal, Derin Bugu Yuzer, Baris Kandemir, Kamran Gulsahi
Journal of Dental Sciences.2025; 20(3): 1532. CrossRef - Comparative Analysis of Gene Expression in Periodontal Ligament Stem Cells Exposed to Biodentine and Bio-C Repair: Implications for Cementogenesis—An In Vitro Study
Mahmoud M. Bakr, Mahmoud Al Ankily, Mohammed Meer, Mohamed Shamel
Oral.2025; 5(1): 19. CrossRef - Efficacy of Mineral Trioxide Aggregate Versus Biodentine as a Direct Pulp Capping Material in Carious Human Mature Permanent Teeth: A Systematic Review
Rashmi Misra, Nikita Toprani, Sumita Bhagwat, Aashaka Vaishnav, Aastha Dureja, Omkar Bhosale
Cureus.2025;[Epub] CrossRef - Evaluation of Different Techniques and Materials for Filling in 3-dimensional Printed Teeth Replicas with Perforating Internal Resorption by Means of Micro–Computed Tomography
Angelo J.S. Torres-Carrillo, Helena C. Assis, Rodrigo E. Salazar-Gamarra, Leonardo Moreira Teodosio, Alice C. Silva-Sousa, Jardel F. Mazzi-Chaves, Priscila B. Ferreira-Soares, Manoel D. Sousa-Neto, Fabiane C. Lopes-Olhê
Journal of Endodontics.2024; 50(2): 205. CrossRef
- Effect of Restoration Strategy and Cavity Location on the Fracture Resistance of Teeth with External Cervical Resorption
- 3,683 View
- 82 Download
- 4 Web of Science
- 6 Crossref
- Effect of glide path preparation with PathFile and ProGlider on the cyclic fatigue resistance of WaveOne nickel-titanium files
- Gülşah Uslu, Uğur İnan
- Restor Dent Endod 2019;44(2):e22. Published online May 9, 2019
- DOI: https://doi.org/10.5395/rde.2019.44.e22
-
Abstract
PDFPubReaderePub
Objectives The aim of this study was to investigate the effect of glide path preparation with PathFile and ProGlider nickel-titanium (NiTi) files on the cyclic fatigue resistance of WaveOne NiTi files.
Materials and Methods Forty-four WaveOne Primary files were used and divided into four groups (
n = 11). In the first group (0 WaveOne), the WaveOne Primary files served as a control group and were not used on acrylic blocks. In the 1 WaveOne Group, acrylic blocks were prepared using only WaveOne Primary files, and in the PF+WaveOne group and PG+WaveOne groups, acrylic blocks were first prepared with PathFile or ProGlider NiTi files, respectively, followed by the use of WaveOne Primary files. All the WaveOne Primary files were then subjected to cyclic fatigue testing. The number of cycles to failure was calculated and the data were statistically analyzed using one-way analysis of variance (ANOVA) and the Tukey honest significant difference multiple-comparison test at a 5% significance level.Results The highest number of cycles to failure was found in the control group, and the lowest numbers were found in the 1 WaveOne group and the PF+WaveOne group. Significant differences were found among the 1 WaveOne, PF+WaveOne, and control groups (
p < 0.05). No statistically significant differences were found between the PG+WaveOne group and the other three groups (p > 0.05).Conclusion Glide path preparation with NiTi rotary files did not affect the cyclic fatigue resistance of WaveOne Primary files used on acrylic blocks.
-
Citations
Citations to this article as recorded by- Screw-in force, torque generation, and performance of glide-path files with three rotation kinetics
Jee-Yeon Woo, Ji-Hyun Jang, Seok Woo Chang, Soram Oh
Odontology.2024; 112(3): 761. CrossRef - Glide Path in Endodontics: A Literature Review of Current Knowledge
Vlad Mircea Lup, Giulia Malvicini, Carlo Gaeta, Simone Grandini, Gabriela Ciavoi
Dentistry Journal.2024; 12(8): 257. CrossRef - Comparative Evaluation of the Cyclic Fatigue Resistance of WaveOne Gold in Reciprocation, ProGlider in Rotary Motion, and Manual Files in a Reciprocating Handpiece Within Simulated Curved Canals: An In Vitro Study
Shivangi M Pujara, Hardik B Shah, Leena H Jobanputra
Cureus.2024;[Epub] CrossRef - Effect of glide path instruments in cyclic fatigue resistance of reciprocating instruments after three uses
André Schroder Scherer, Carlos Alexandre Souza Bier, José Roberto Vanni
Brazilian Dental Journal.2023; 34(2): 27. CrossRef - An Investigation of the Accuracy and Reproducibility of 3D Printed Transparent Endodontic Blocks
Martin Smutný, Martin Kopeček, Aleš Bezrouk
Acta Medica (Hradec Kralove, Czech Republic).2022; 65(2): 59. CrossRef - Evaluation of Cyclic Fatigue of Hyflex EDM, Twisted Files, and ProTaper Gold Manufactured with Different Processes: An In Vitro Study
Pooja D. Khandagale, Prashant P. Shetty, Saleem D. Makandar, Pradeep A. Bapna, Mohmed Isaqali Karobari, Anand Marya, Pietro Messina, Giuseppe Alessandro Scardina, Antonino Lo Giudice
International Journal of Dentistry.2021; 2021: 1. CrossRef
- Screw-in force, torque generation, and performance of glide-path files with three rotation kinetics
- 2,638 View
- 11 Download
- 6 Crossref
- Critical evaluation of fracture strength testing for endodontically treated teeth: a finite element analysis study
- Emel Uzunoglu-Özyürek, Selen Küçükkaya Eren, Oğuz Eraslan, Sema Belli
- Restor Dent Endod 2019;44(2):e15. Published online April 18, 2019
- DOI: https://doi.org/10.5395/rde.2019.44.e15
-
Abstract
PDFPubReaderePub
Objectives The aim of this study was to investigate whether the diameter and direction of the plunger and simulation of the periodontal ligament (PDL) affected the stress distribution in endodontically treated premolars.
Methods A fracture strength test was simulated via finite element analysis. A base model was set up, and the following parameters were modified: plunger diameter (3 mm vs. 6 mm), plunger direction (vertical vs. 135° angular to the central fossa), and PDL simulation. The analysis was conducted using the CosmosWorks structural analysis program, and the results are presented in terms of von Mises stresses.
Results The smaller plunger increased the stresses at the contact area of the crown, but the plunger diameter had no effect on the stress distribution within the root. An angular plunger direction increased stresses within the root, as well as at the buccal cusp of the crown, compared with the vertical direction. Simulation of the PDL caused higher stress accumulation, especially in the cervical region of the root.
Conclusions The plunger diameter had no effect on the stress distribution in the roots, whereas the plunger direction and PDL simulation did affect the stress distribution. More stringent standards can be established by taking such parameters into account when performing fracture testing in future studies.
-
Citations
Citations to this article as recorded by- Fracture resistance of endodontically treated teeth restored with polyetheretherketone (PEEK) versus glass fiber posts: A comparative in vitro analysis
Manduwada Vishal, Neha Mehra, Mamta Kaushik, Prabakaran Saravanan
Endodontology.2026; 38(2): 172. CrossRef - Access cavity in endodontics: Balancing precision, preservation, and clinical needs
Dina Abdellatif, Ismail Davut Capar, De Fontaine Sarah, Alfredo Iandolo, Christophe Meyer, Davide Mancino
Journal of Conservative Dentistry and Endodontics.2025; 28(6): 573. CrossRef - Assessment of Stress Distribution with 3 Taper Design Preparation of Root Canal Using Finite Element Analysis
Tejasree Rathod, G. Durgabhavani, Pudu Tirupathi, Nusrath Parveen, Yelloji Paramesh, Prabhakar Dharavattu
Journal of Pharmacy and Bioallied Sciences.2024; 16(Suppl 1): S112. CrossRef - The impact of the filling technique with two sealers in bulk or associated with gutta-percha on the fatigue behavior and failure patterns of endodontically treated teeth
Isabella Marian Lena, Luiza Colpo Chiaratti, Rafaela Oliveira Pilecco, Renan Vaz Machry, João Paulo Mendes Tribst, Cornelis Johannes Kleverlaan, Gabriel Kalil Rocha Pereira, Renata Dornelles Morgental
PeerJ.2024; 12: e18221. CrossRef - Stronger than Ever: Multifilament Fiberglass Posts Boost Maxillary Premolar Fracture Resistance
Naji Kharouf, Eugenio Pedullà, Gianluca Plotino, Hamdi Jmal, Mohammed-El-Habib Alloui, Philippine Simonis, Patrice Laquerriere, Valentina Macaluso, Dina Abdellatif, Raphaël Richert, Youssef Haikel, Davide Mancino
Journal of Clinical Medicine.2023; 12(8): 2975. CrossRef - Neural network approach to evaluate the physical properties of dentin
Mohammad Ali Saghiri, Ali Mohammad Saghiri, Elham Samadi, Devyani Nath, Julia Vakhnovetsky, Steven M. Morgano
Odontology.2023; 111(1): 68. CrossRef - Modelling and evaluating periodontal ligament mechanical behaviour and properties: A scoping review of current approaches and limitations
Enaiyat Ghani Ovy, Dan L. Romanyk, Carlos Flores Mir, Lindsey Westover
Orthodontics & Craniofacial Research.2022; 25(2): 199. CrossRef - FEAr no more! Finite element analysis in orthodontics
Shilpa Chawla, Shailesh Deshmukh
Journal of the International Clinical Dental Research Organization.2022; 14(1): 6. CrossRef - Influence of Methodological Variables on Fracture Strength Tests Results of Premolars with Different Number of Residual Walls. A Systematic Review with Meta-Analysis
Carlo Gaeta, Crystal Marruganti, Emanuele Mignosa, Giovanni Franciosi, Edoardo Ferrari, Simone Grandini
Dentistry Journal.2021; 9(12): 146. CrossRef
- Fracture resistance of endodontically treated teeth restored with polyetheretherketone (PEEK) versus glass fiber posts: A comparative in vitro analysis
- 3,607 View
- 59 Download
- 9 Crossref
Basic Research
- The effects of short-term application of calcium hydroxide on dentin fracture strength
- Eun-Jung Shin, Yeong-Joon Park, Bin-Na Lee, Ji-Hyun Jang, Hoon-Sang Chang, In-Nam Hwang, Won-Mann Oh, Yun-Chan Hwang
- J Korean Acad Conserv Dent 2011;36(5):425-430. Published online September 30, 2011
- DOI: https://doi.org/10.5395/JKACD.2011.36.5.425
-
Abstract
PDFPubReaderePub
Objectives This
in vitro study investigated whether short-term application of calcium hydroxide in the root canal system for 1 and 4 wk affects the fracture strength of human permanent teeth.Materials and Methods Thirty two mature human single rooted mandibular premolars in similar size and dentin thickness without decay or restorations were hand and rotary instrumented and 16 teeth vertically packed with calcium hydroxide paste and sealed coronally with caviton to imitate the endodontic procedure and the other 16 teeth was left empty as a control group. The apicies of all the samples were sealed with resin, submerged in normal saline and put in a storage box at 37℃ to mimic the oral environment. After 1 and 4 wk, 8 samples out of 16 samples from each group were removed from the storage box and fracture strength test was performed. The maximum load required to fracture the samples was recorded and data were analysed statistically by the two way ANOVA test at 5% significance level.
Results The mean fracture strengths of two groups after 1 wk and 4 wk were similar. The intracanal placement of calcium hydroxide weakened the fracture strength of teeth by 8.2% after 4 wk: an average of 39.23 MPa for no treatment group and 36.01 MPa for CH group. However there was no statistically significant difference between experimental groups and between time intervals.
Conclusions These results suggest that short term calcium hydroxide application is available during endodontic treatment.
-
Citations
Citations to this article as recorded by- Effect of niobium pentoxide incorporated calcium hydroxide as an intracanal medicament on fracture resistance of root canal dentin
Nadimpalli Teja Varma, Venkatappan Sujatha, Kittappa Karthikeyan, Sekar Mahalaxmi
Journal of Conservative Dentistry and Endodontics.2025; 28(12): 1211. CrossRef - Effect of Calcium Hydroxide as an Intracanal Medication on Dentine Fracture Resistance: A Systematic Review and Network Meta-Analysis
Chayanit Sunlakawit, Chitpol Chaimanakarn, Natchalee Srimaneekarn, Sittichoke Osiri
Journal of Endodontics.2024; 50(12): 1714. CrossRef
- Effect of niobium pentoxide incorporated calcium hydroxide as an intracanal medicament on fracture resistance of root canal dentin
- 4,365 View
- 32 Download
- 2 Crossref
Original Articles
- Fracture resistance of the three types of undermined cavity filled with composite resin
- Hoon-Soo Choi, Dong-Hoon Shin
- J Korean Acad Conserv Dent 2008;33(3):177-183. Published online May 31, 2008
- DOI: https://doi.org/10.5395/JKACD.2008.33.3.177
-
Abstract
PDFPubReaderePub
It was reported that esthetic composite resin restoration reinforces the strength of remaining tooth structure with preserving the natural tooth structure. However, it is unknown how much the strength would be recovered. The purpose of this study was to compare the fracture resistance of three types of undermined cavity filled with composite resin with that of non-cavitated natural tooth.
Forty sound upper molars were allocated randomly into four groups of 10 teeth. After flattening occlusal enamel, undermined cavities were prepared in thirty teeth to make three types of specimens with various thickness of occlusal structure (Group 1 ~ 3). All the cavity have the 5 mm width mesiodistally and 7 mm depth bucco-lingually. Another natural 10 teeth (Group 4) were used as a control group. Teeth in group 1 have remaining occlusal structure about 1 mm thickness, which was composed of mainly enamel and small amount of dentin. In Group 2, remained thickness was about 1.5 mm, including 0.5 mm thickness dentin. In Group 3, thickness was about 2.0 mm, including 1 mm thickness dentin. Every effort was made to keep the remaining dentin thickness about 0.5 mm from the pulp space in cavitated groups. All the thickness was evaluated with radiographic Length Analyzer program.
After acid etching with 37% phosphoric acid, one-bottle adhesive (Single Bond™, 3M/ESPE, USA) was applied following the manufacturer's recommendation and cavities were incrementally filled with hybrid composite resin (Filtek Z-250™, 3M/ESPE, USA). Teeth were stored in distilled water for one day at room temperature, after then, they were finished and polished with Sof-Lex system.
All specimens were embedded in acrylic resin and static load was applied to the specimens with a 3 mm diameter stainless steel rod in an Universal testing machine and cross-head speed was 1 mm/min. Maximum load in case of fracture was recorded for each specimen.
The data were statistically analyzed using one-way analysis of variance (ANOVA) and a Tukey test at the 95% confidence level.
The results were as follows:
Fracture resistance of the undermined cavity filled with composite resin was about 75% of the natural tooth.
No significant difference in fracture loads of composite resin restoration was found among the three types of cavitated groups.
Within the limits of this study, it can be concluded the fracture resistance of the undermined cavity filled with composite resin was lower than that of natural teeth, however remaining tooth structure may be supported and saved by the reinforcement with adhesive restoration, even if that portion consists of mainly enamel and a little dentin structure.
-
Citations
Citations to this article as recorded by- Fracture resistance of crown-root fractured teeth repaired with dual-cured composite resin and horizontal posts
Seok-Woo Chang, Yong-Keun Lee, Seung-Hyun Kyung, Hyun-Mi Yoo, Tae-Seok Oh, Dong-Sung Park
Journal of Korean Academy of Conservative Dentistry.2009; 34(5): 383. CrossRef
- Fracture resistance of crown-root fractured teeth repaired with dual-cured composite resin and horizontal posts
- 2,181 View
- 6 Download
- 1 Crossref
- The effect of reinforcing methods on fracture strength of composite inlay bridge
- Chang-Won Byun, Sang-Hyuk Park, Sang-Jin Park, Kyoung-Kyu Choi
- J Korean Acad Conserv Dent 2007;32(2):111-120. Published online March 31, 2007
- DOI: https://doi.org/10.5395/JKACD.2007.32.2.111
-
Abstract
PDFPubReaderePub
The purpose of this study is to evaluate the effects of surface treatment and composition of reinforcement material on fracture strength of fiber reinforced composite inlay bridges.
The materials used for this study were I-beam, U-beam TESCERA ATL system and ONE STEP(Bisco, IL, USA). Two kinds of surface treatments were used; the silane and the sandblast. The specimens were divided into 11 groups through the composition of reinforcing materials and the surface treatments.
On the dentiform, supposing the missing of Maxillary second pre-molar and indirect composite inlay bridge cavities on adjacent first pre-molar disto-occlusal cavity, first molar mesio-occlusal cavity was prepared with conventional high-speed inlay bur.The reinforcing materials were placed on the proximal box space and build up the composite inlay bridge consequently. After the curing, specimen was set on the testing die with ZPC. Flexural force was applied with universal testing machine (EZ-tester; Shimadzu, Japan). at a cross-head speed of 1 mm/min until initial crack occurred. The data wasanalyzed using one-way ANOVA/Scheffes' post-hoc test at 95% significance level.
Groups using I-beam showed the highest fracture strengths (p < 0.05) and there were no significant differences between each surface treatment (p > 0.05). Most of the specimens in groups that used reinforcing material showed delamination.
The use of I-beam represented highest fracture strengths (p < 0.05).
In groups only using silane as a surface treatment showed highest fracture strength, but there were no significant differences between other surface treatments (p > 0.05).
The reinforcing materials affect the fracture strength and pattern of composites inlay bridge.
The holes at the U-beam did not increase the fracture strength of composites inlay bridge.
-
Citations
Citations to this article as recorded by- Esthetic rehabilitation of single anterior edentulous space using fiber-reinforced composite
Hyeon Kim, Min-Ju Song, Su-Jung Shin, Yoon Lee, Jeong-Won Park
Restorative Dentistry & Endodontics.2014; 39(3): 220. CrossRef
- Esthetic rehabilitation of single anterior edentulous space using fiber-reinforced composite
- 1,874 View
- 3 Download
- 1 Crossref
- The influence of different access cavity designs on the fracture strength in endodontically treated mandibular anterior teeth
- Young-Gyun Lee, Hye-Jin Shin, Se-Hee Park, Kyung-Mo Cho, Jin-Woo Kim
- J Korean Acad Conserv Dent 2004;29(6):515-519. Published online November 30, 2004
- DOI: https://doi.org/10.5395/JKACD.2004.29.6.515
-
Abstract
PDFPubReaderePub
Straight access cavity design allows the operator to locate all canals, helps in proper cleaning and shaping, ultimately facilitates the obturation of the canal system. However, change in the fracture strength according to the access cavity designs was not clearly demonstrated yet. The purpose of this study was to determine the influence of different access cavity designs on the fracture strength in endodontically treated mandibular anterior teeth.
Recently extracted mandibular anterior teeth that have no caries, cervical abrasion, and fracture were divided into three groups (Group 1 : conventional lingual access cavity, Group 2 : straight access cavity, Group 3 : extended straight access cavity) according to the cavity designs. After conventional endodontic treatment, cavities were filled with resin core material. Compressive loads parallel to the long axis of the teeth were applied at a crosshead speed of 2mm/min until the fracture occurred. The fracture strength analyzed with ANOVA and the Scheffe test at the 95% confidence level.
The results of this study were as follows :
1. The mean fracture strength decrease in following sequence Group 1 (558.90 ± 77.40 N), Group 2 (494.07 ± 123.98 N) and Group 3 (267.33 ± 27.02 N).
2. There was significant difference between Group 3 and other groups (P = 0.00).
Considering advantage of direct access to apical third and results of this study, straight access cavity is recommended for access cavity form of the mandibular anterior teeth.
-
Citations
Citations to this article as recorded by- Fracture resistance of crown-root fractured teeth repaired with dual-cured composite resin and horizontal posts
Seok-Woo Chang, Yong-Keun Lee, Seung-Hyun Kyung, Hyun-Mi Yoo, Tae-Seok Oh, Dong-Sung Park
Journal of Korean Academy of Conservative Dentistry.2009; 34(5): 383. CrossRef
- Fracture resistance of crown-root fractured teeth repaired with dual-cured composite resin and horizontal posts
- 1,714 View
- 3 Download
- 1 Crossref
 First
First Prev
Prev

