
Articles
- Page Path
- HOME > Restor Dent Endod > Volume 46(1); 2021 > Article
- Research Article Impact of root canal curvature and instrument type on the amount of extruded debris during retreatment
-
Burcu Serefoglu1
 , Gözde Kandemir Demirci1, Seniha Miçooğulları Kurt1, İlknur Kaşıkçı Bilgi2, Mehmet Kemal Çalışkan1
, Gözde Kandemir Demirci1, Seniha Miçooğulları Kurt1, İlknur Kaşıkçı Bilgi2, Mehmet Kemal Çalışkan1 -
Restor Dent Endod 2020;46(1):e5.
DOI: https://doi.org/10.5395/rde.2021.46.e5
Published online: December 17, 2020
1Department of Endodontics, Faculty of Dentistry, Ege University, Bornova, İzmir, Turkey.
2Bornova Oral Health Center, Bornova, İzmir, Turkey.
- Correspondence to Burcu Serefoglu, DDS, PhD. Research Assistant, Department of Endodontics, Faculty of Dentistry, Ege University, Erzene Street, Bornova, İzmir 35040, Turkey. burcuseref@yahoo.com
• Received: March 9, 2020 • Revised: May 3, 2020 • Accepted: May 15, 2020
Copyright © 2021. The Korean Academy of Conservative Dentistry
This is an Open Access article distributed under the terms of the Creative Commons Attribution Non-Commercial License (https://creativecommons.org/licenses/by-nc/4.0/) which permits unrestricted non-commercial use, distribution, and reproduction in any medium, provided the original work is properly cited.
Abstract
-
Objectives The aim of the current study was to assess whether the amount of extruded debris differs for straight and severely curved root canals during retreatment using H-files, R-Endo, Reciproc and ProTaper Universal Retreatment (PTU-R) files. Additionally, the area of residual filling material was evaluated.
-
Materials and Methods Severely curved (n = 104) and straight (n = 104) root canals of maxillary molar teeth were prepared with WaveOne Primary file and obturated with gutta-percha and AH Plus sealer. Root canal filling materials were removed with one of the preparation techniques: group 1: H-file; group 2: R-Endo; group 3: Reciproc; group 4: PTU-R (n = 26). The amount of extruded material and the area of the residual filling material was measured. The data were analyzed with 2-way analysis of variance (ANOVA) and 1-way ANOVA at the 0.05 significance level.
-
Results Except for Reciproc group (p > 0.05), PTU-R, R-Endo, and H-file systems extruded significantly more debris in severely curved canals (p < 0.05). Each file system caused more residual filling material in severely curved canals than in straight ones (p < 0.05).
-
Conclusions All instruments used in this study caused apical debris extrusion. Root canal curvature had an effect on extruded debris, except for Reciproc system. Clinicians should be aware that the difficult morphology of the severely curved root canals is a factor increasing the amount of extruded debris during the retreatment procedure.
INTRODUCTION
The insufficiency of the root canal treatment can be considered as one of the major factors in persistent or newly developed periradicular inflammatory lesions following primary endodontic treatment [1]. In such cases, while teeth may be preserved by nonsurgical retreatment or endodontic surgery, the complicated nature of preoperative and intraoperative factors may influence the outcome [2,3]. Retreatment procedures require complete removal of pre-existent root canal filling material, along with re-instrumentation, re-disinfection, and re-filling of the root canals [2,4]. Removal of gutta-percha and sealer from the root canal system can be performed in several ways, including the use of stainless steel hand files, heat-bearing instruments, and ultrasonic and nickel-titanium (Ni-Ti) retreatment systems [5,6,7]. During the retreatment procedure, sealers and gutta-percha may extrude from the root canal into the periapical tissues. Additionally, the presence of residual filling materials, necrotic tissue, and bacteria, especially within the apical third of the root canal, is considered as the primary cause of postoperative inflammation, flare-ups, and retreatment failure [8]. For that reason, it is important to select the most appropriate retreatment system to remove obturation material as completely as possible in order to reduce the amount of extruded debris [9]. However, in vitro studies have consistently shown that all retreatment techniques produce varying degrees of debris extrusion, with significant amounts of root canal filling residue adhering to the canal walls [7,9,10,11].
In the literature, the efficacy of Ni-Ti retreatment systems in terms of the amount of extruded debris has been evaluated mainly in straight root canals, with only limited data on their efficacy in severely curved canals [9,10,12]. Retreatment is especially challenging in curved root canals, as procedural errors such as alteration of root canal morphology or instrument fracture are more likely to occur [13]. On that basis, the primary aim of the current study was to assess whether the amount of extruded debris and the area of residual filling material differ for straight and severely curved root canals during retreatment using H-files, R-Endo, Reciproc and PTU-R files. The second aim was to compare the file systems in terms of the amount of extruded debris and the area of residual filling material for the entire root canal length and each section, both in straight and severely curved root canals.
MATERIALS AND METHODS
The present study protocol was reviewed and approved by the Ethical Committee of Ege University, School of Medicine (Approval No. 16-8.1/3). Following Kaşıkçı Bilgi et al. [12], the minimum sample size at an alpha level of 0.10 was determined as 24 samples for each group. To prevent possible sample loss, 26 samples were included in each group. In total, the sample included 208 extracted human maxillary first molar teeth without previous endodontic treatment apical resorption, vertical or horizontal cracks, visibly immature apices, or calcified root canals. Disto-buccal or mesio-buccal roots of the maxillary first molar teeth, into which a 15 K file could not reach but a 10 K file fitted tightly at the apical foramen, were separated at the furcation with high-speed diamond burs to prevent superposition. Digital radiographs were then taken in bucco-palatal and mesio-distal projection to measure root canal curvature and radius, using AutoCAD 2013 software (Autodesk Inc., San Rafael, CA, USA) as described by Pruett et al. [14]. Teeth with root canal curvature between 0°–5° and 30°–45o and radius 8–10 mm were enrolled in the study. Overall, 104 teeth of curvature < 5o were allocated to the straight root canal group (Figure 1A), 104 roots of curvature 30°–45° were assigned to the curved root canal group (Figure 1B).
Figure 1
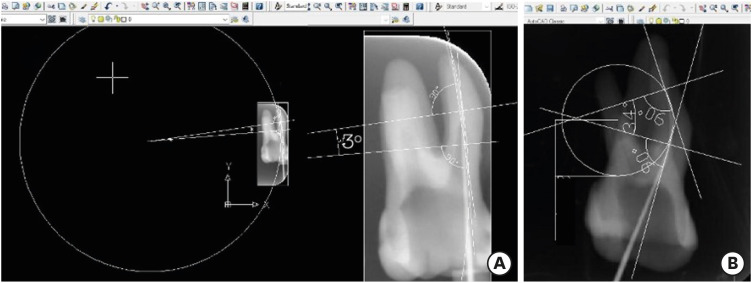
The root canal curvature and radius measurement according to Pruett et al. [14] using AutoCAD software. (A) Straight canal, (B) severely curved root canal.
Access cavities were prepared, and each root length was standardized to 17 mm in both curved and straight root canal groups by flattening the buccal cusp edges. Working length was determined as 1 mm short of the major apical foramen. After creating a glide path with size 20 K-files, root canal preparation was performed using the Wave One Primary (Dentsply Maillefer, Ballaigues, Switzerland) Ni-Ti instrument (size 25/0.08). Root canals were irrigated with a total 5 mL 2.5% sodium hypochlorite (NaOCl) (Merck, Darmstadt, Germany) during root canal preparation, and final irrigation was performed with 5 mL 17% ethylenediaminetetraacetic acid (EDTA) (Merck) and 5 mL 2.5% NaOCl solutions. Root canals were then dried with paper points and obturated with a Wave One Primary gutta-percha cone (Dentsply Maillefer) and AH Plus sealer (Dentsply Sirona, Tulsa, OK, USA) in a single-cone technique by one experienced operator. The obturations were confirmed to have no voids by radiographs in the bucco-lingual and mesio-distal directions. Finally, Cavit (3M ESPE, Seefeld, Germany) was placed into the access cavities, and all teeth were stored at 37°C in 100% humidity for 30 days for sealer set.
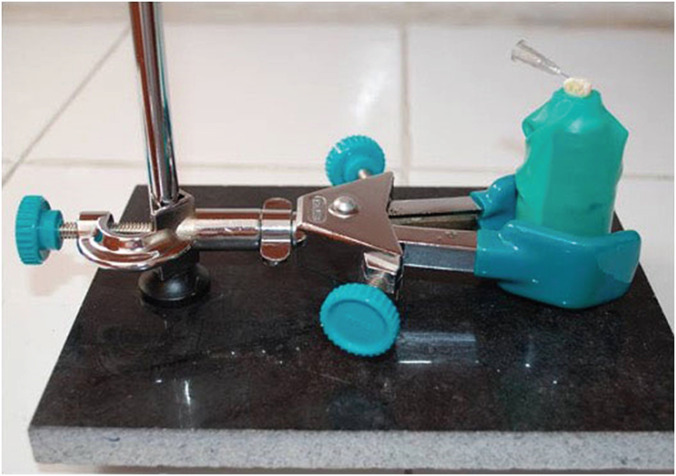
To randomly allocate the curved root canals to the experimental groups, the teeth were first divided into sub-groups with respect to their root canal curvature angles (30°–35°; 36°–40°; 41°–45°). Roots from each subgroup were then randomly assigned to 4 experimental groups defined by preparation technique (group 1: H-file [VDW, Munich, Germany]; group 2: R-Endo [Micro-Mega, Besancon, France]; group 3: Reciproc [VDW]; group 4: ProTaper Universal Retreatment [PTU-R; Dentsply Maillefer] [n = 26]). In this way, mean curvature values for each group remained stable within the range 36°–37° (36.65° ± 6.5°). Similarly, teeth in the straight root canal group were randomly divided into 4 experimental groups (n = 26). The method of Myers and Montgomery [15] was used when collecting the extruded material. Before attaching the teeth to the glass vials as described by Kaşıkçı Bilgi et al. [12] (Figure 2), all vials were measured using a microbalance (10−5 g) (Sartorius, Göttingen, Germany), and their weight was recorded.
All of the tested instruments and Gates Glidden drills (VDW) were operated using the X Smart plus endodontic motor (Dentsply Sirona) according to the manufacturer's instructions concerning speed and torque. All retreatment protocols were performed by a single qualified operator. With the exception of the PTU-R group, a size 3 Gates Glidden drill was used at 1,200 rpm to remove the coronal 3 mm. Retreatment procedures were performed in experimental groups as follows:
Group 1 H-file: H-files (sizes 35, 30, 25, 20 and 15) were used to remove the gutta-percha, employing the crown-down technique. When the working length was reached, root canals were re-instrumented with size 20, 25, 30, 35 and 40 H-files respectively used at working length.
Group 2 R-Endo: R1 (25, 0.08 taper) and R2 (25, 0.06 taper) files were used at the coronal and middle thirds, and R3 (25, 0.04 taper) was used at the working length at 350 rpm and 1.6 Ncm while removing the root canal filling material. For final apical preparation, AS30, AS35, AS40 (40, 0.06 taper) of Revo-S instruments were then utilized at working length.
Group 3 Reciproc: The R25 (tip size 25, 0.08 taper) instrument was used in a slow in-and-out motion to remove the root canal filling material. Following 3 pecking movements, the root canals were irrigated, and the same protocol continued to reach the working length. The Reciproc R40 (40, 0.06 taper for the first 3 mm) instrument was then utilized for final preparation.
Group 4 PTU-R: Filling material was removed from the coronal, middle, and apical thirds of the root canal using the D1 (size 30, 0.09 taper), D2 (25, 0.08 taper), and D3 (20, 0.07 taper) files at 500 rpm and 2.5 Ncm, respectively. Following the completion of gutta-percha removal, root canals were prepared with the ProTaper Next X2, X3 and X4 (40, 0.06 taper) instruments.
Root canal preparation was stopped when the working length was reached and gutta-percha was not observed on the surface of the instruments. Any procedural errors such as blockage, instrument fractures, or apical perforations were recorded. No solvents were used to remove the root filling materials in any of the experimental groups. A 30 G side-vented irrigation needle was inserted into the canal 2 mm short of the working length, and 10 mL distilled water was used for irrigation during the instrumentation procedure. Before the vials were stored in a dry-heat oven at a stable temperature of 95°C for 48 hours, the apex was irrigated into the vials, with an extra 1 mL of distilled water for collecting the debris adhering to the external part of the root. In total, 11 mL of distilled water was used. Following evaporation of the irrigant, each vial was measured 3 times by an examiner, who was blinded to groups. The amount of extruded debris was obtained by subtracting the empty weight of the vial from the post-instrumentation weight. The total area of the residual filling material was calculated from mesio-distal and bucco-lingual projections of the periapical radiographs (Figure 3), using Image J software (National Institute of Health, Bethesda, MD, USA). Before taking digital radiographs, a 10 × 10 mm wire was positioned on the phosphor plates to calibrate the measurement. The total area was calculated without distinguishing between gutta-percha and sealer remnants during measurement. Standard radiographic exposure conditions were employed to obtain the digital radiographs, and the X-ray source was placed 10 cm away from the periapical film.
Figure 3
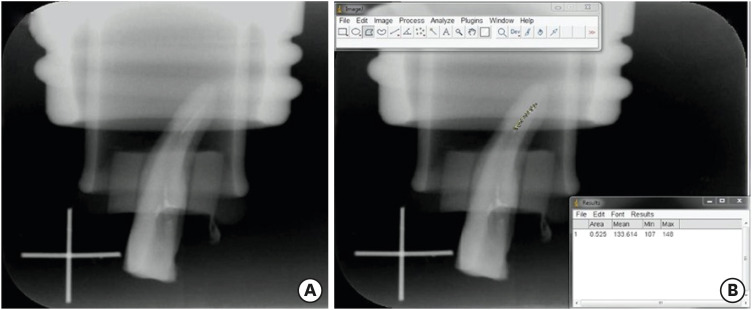
(A) An image showing the residual filling material on the root canal walls (B) calculation of the area of residual filling material using Image J software.
Data were analyzed using GraphPad statistical package software program (GraphPad Software, LA Jolla, CA, USA). Shapiro Wilk test was used to evaluate the distribution of the variables in each group in terms of both extruded debris and residual filling material. As parametric distribution was assessed by the Shapiro-Wilk test, the influence of curvature and the instrument type (independent variables) on the amount of extruded debris and the residual filling material (dependent variables) were analyzed with 2-way at the 0.05 significance level. Post hoc comparisons were completed by Bonferroni test. Since the 2-way analysis of variance (ANOVA) test showed an interaction between curvature and instrument type on the area of residual filling material, one-way ANOVA was performed to compare the effect of either curvature or instrument type on the area of residual filling material for the entire and each section of the root canals. Likewise, the correlation between the amount of extruded debris and the residual filling material was investigated using Pearson correlation analysis.
RESULTS
No procedural errors occurred during the experiment. The mean amount of extruded debris for each experimental group is shown in Table 1. The 2-way ANOVA test revealed that the curvature had a significant impact (p < 0.001), whereas the instrument type had no influence on the amount of extruded debris (p = 0.947). According to the data obtained through post hoc analysis of 2-way ANOVA, PTU-R, R-Endo, and H-file systems extruded significantly more debris in severely curved root canals than straight ones (PPTR-U < 0.001, PR-ENDO= 0.013, PH-FILE < 0.001). However, there was no significant difference between the severely curved and straight root canals in terms of the amount of extruded debris caused by Reciproc system (p = 0.246).
Table 1
Amount of extruded debris (g) associated with the 4 nickel-titanium (Ni-Ti) file systems in severely curved and straight canals
When each file system was compared with respect to the extruded debris in severely curved root canals, the differences were not statistically significant between the file systems (PRECIPROC-PTR-U = 0.574, PRECIPROC-R-ENDO = 0.852, PRECIPROC-H-FILE = 0.272, PPTR-U-R-ENDO = 0.964, PPTR-U-H-FILE = 0.953, PR-ENDO-H-FILE = 0.747). Moreover, regarding the amount of the extruded debris, 4 groups ranked as follows: Reciproc < R-Endo < PTU-R < H-file.
In straight root canals, 4 file systems caused a statistically similar amount of extruded debris during removal of the root canal filling material (PRECIPROC-PTR-U = 0.807, PRECIPROC-R-ENDO > 0.999, PRECIPROC-H-FILE = 0.685, PPTR-U-R-ENDO = 0.829, PPTR-U-H-FILE = 0.997, PR-ENDO-H-FILE = 0.711), and the ranking order of the file systems were as follows: H-file < PTU-R < R-Endo < Reciproc.
The mean areas of residual filling material (mm2) are summarized in Table 2. Both curvature (p < 0.001) and the instrument type (p = 0.021) had an influence on residual filling material. Each file system caused more residual filling material in severely curved canals than straight ones (PPTR-U = 0.012, PR-ENDO < 0.001, PH-FILE < 0.001, PRECIPROC < 0.001).
Table 2
Radiographic assessment of the area of residual filling material (mm2)
In severely curved canals, the Reciproc system was associated with significantly more residual filling material than the H-files for entire root canal length (p = 0.027). Considering each third of the root canal, there were no significant differences among the file systems in apical (p = 0.408) and coronal thirds (p = 0.246), but at the middle third, Reciproc system resulted in more residual filling material than both PTU-R (p = 0.015) and H-file (p = 0.004).
On the other hand, in straight canals, significantly more filling material remained for the PTU-R than for the R-Endo system (p = 0.002) and the Hand File (p = 0.033) for the entire root canal length. When each third of the root canal was considered, PTU-R system left more residual filling material than the H-file (p = 0.006) and R-Endo (p = 0.034) system at the apical and coronal third of the root canals, respectively.
The correlation between the amount of extruded debris and residual filling material was insignificant both in severely curved (PPTR-U = 0.429, PR-ENDO = 0.157, PH-FILE = 0.085, PRECIPROC = 0.299) and straight canals (PPTR-U = 0.211, PR-ENDO = 0.478, PH-FILE = 0.590, PRECIPROC = 0.898) for each file system (Table 3).
Table 3
Correlation between extruded debris and residual filling material
DISCUSSION
It is known that apical debris extrusion may lead to postoperative pain and flare-up, and diminish the success rate of nonsurgical retreatment [16,17]. This may occur during endodontic retreatment using current preparation techniques and instruments, as well as during primary root canal treatment [5,18].
Apical debris extrusion during endodontic retreatment has previously been studied separately for straight and curved root canals, but a few studies addressed severely curved root canals [9,10,12,19,20]. As no previous study has evaluated the impact of root canal curvature on the amount of extruded debris in retreatment procedures, we aimed to assess this issue was in the current study. To prevent heterogeneity between experimental groups, only teeth of similar length and angle of curvature (< 5° and 30°–45° with radius 8–10 mm) and teeth in which the 15 K file could not reach the apex and the 10 K file could be tightly fitted at the apical foramen were included.
The method of Myers and Montgomery [15] was used during the retreatment procedure since the most commonly preferred technique to collect extruded debris. In clinical settings, irrigation solutions such as NaOCl and EDTA are routinely used to enhance the removal of gutta-percha and sealer [21]. However, because a constant temperature was necessary for evaporation of the irrigant, distilled water was used in the present study to prevent possible crystallization of both solutions and to avoid affecting the amount of extruded debris as in previous studies [9,10,18].
The finding of the current study revealed that curvature had a significant impact on the amount of extruded debris. Due to the lack of data about retreatment, the results of this study could only be compared with primer debris extrusion studies. Both Hinrichs et al. [22] and Leonardi et al. [23] reported that curvature had no effect on the amount of extruded debris, but in contrast to our study, both of those studies compared only straight and moderately curved root canals. On the other hand, Karataslioglu et al. [24] reported that root canal curvature played a significant role in debris extrusion, and our results are in accordance with that finding. It may be speculated that in straight root canals, debris could be easily transported coronally, but in severely curved canals, more pecking motion would be required to reach the apical area as noted previously by Karataslioglu et al. [24] and that may result in more debris extrusion.
In the current study, 2 multi-file retreatment systems and 1 single file system, with different kinematics were used to evaluate the amount of extruded debris during the retreatment procedure. In the previous studies, there has been no consensus about which kinematics may increase debris extrusion [18,25,26,27]. There are several investigators who reported that the debris extrusion is more in the rotational movement or reciprocal movement [18,26,27,28]. On the other hand, Kirchhoff et al. [25] compared reciprocal, rotary and adaptive movement to evaluate the amount of extruded debris during the primary root canal treatment and reported that there was no difference among the used kinematics. Similarly, Silva et al. [29] used the PTU-R, Reciproc and WaveOne systems during endodontic retreatment while evaluating the extruded debris and stated that there was no difference between the rotary and reciprocal movement. The present study showed that the Reciprocal movement had a comparable effect with rotary movement both in straight and severely curved root canals and this result is consistent with the previous studies [25,29]. The present study also revealed that both H-file and 3 Ni-Ti file systems caused a similar amount of extruded debris both in severely curved and straight root canals. Even though the difference was not significant, H-file caused more extruded debris in severely curved root canals. In contrast, the least extruded debris was observed with H-file in straight root canals. Whereas the Ni-Ti files tend to displace the debris or filling material coronally due to their design, hand files push the debris to the periapical area in crown-down shaping. However, increased taper of Ni-Ti instruments in the present study might have had an influence in increasing the amount of extruded debris in straight canals as it was previously reported by Bürklein et al. [30]. On the other hand, in severely curved root canals, H-file might have removed excessive dentin along the outer surface of the severely curved canals in order to shape the curved area and consequently, this might have increased the extruded debris.
In clinical conditions, gutta-percha should be removed completely from the root canal during the retreatment procedure because the bacteria may be concealed between the filling material and the recesses of the root canal walls. Where total removal of gutta-percha is not achieved, apical inflammation may persist, reducing the likelihood of success [17]. Therefore, the residual filling material should be checked by a radiograph during the process in order to make sure that no gutta-percha is observed on the instrument. If any residual filling material is seen on the radiographs especially at the apical area of the root canal, the shaping procedure has to be continued until the residual filling material is completely eliminated. However, in laboratory studies, maintaining the shaping process to completely remove the root canal filling residue adhering to the canal wall may influence the standardization among the experimental groups. Therefore, in the current study, after using the retreatment systems, final root canal preparation was performed up to 2 large files from the initial instrumentation size in order to reduce the amount of residual filling material as suggested by previous studies [12,31].
However, in the previous debris extrusion studies in retreatment procedure, the amount of residual filling material was not evaluated except for 2 studies [10,12,20,32]. Depending on the gutta-percha removing ability of the instrument, the area of residual filling material on root canal walls would influence the amount of extruded debris. Although the primary aim in the current study was to assess whether the amount of extruded debris differs for straight and severely curved root canals, the area of residual filling material was also evaluated as done previously, because the evaluation of these 2 factors concurrently and assessment of their correlation is necessary to get a consistent data [12,32].
Regarding the evaluation of the amount of residual filling material, conventional radiography, cone beam computed tomography and micro-computed tomography have been utilized in the literature [33,34,35,36,37,38]. Although 3D analysis provides more detailed results [34,36,37], these methods do not precisely reflect the clinical conditions for daily routine retreatment procedures. Moreover, using 2-dimensional radiographs in similar studies is still considered relevant, as stated previously [39]. Thus, as done in a former study the area of the residual filling material was evaluated using conventional radiographic images in the present study [12].
In order to remove the root canal filling material, H-files, R-Endo, Reciproc and PTU-R instruments were used in this study. In straight canals, the PTU-R system left significantly more residual filling material than either the R-Endo system or Hand file; in contrast, Gergi and Sabbagh [40] reported no significant difference between the H-file, PTU-R, and R-Endo systems. Among the tested instruments, as the only D1 file of PTU-R system has an active working tip, which simplifies penetration into the gutta-percha, Gates Glidden drill was not used for PTU-R group [41]. It can be concluded that this may account for the reduced effectiveness of the PTU-R instrument. Although previous studies have reported no statistical difference between Reciproc and H-file in terms of residual filling material, their results align with the current study's finding that the Reciproc system removed less material than H-file [12,36]. This may be due to subjective factors such as brushing and pecking motions associated with the operator.
In the present study, each file system remained more filling material in severely curved root canals. Instrumentation, especially in curved root canals, could cause procedural errors and also files result in excessive dentin removal. Similarly, removing the root canal filling material from the curved root canals could lead to introducing complexity to the Ni-Ti instruments for removing the root canal filling material. A pilot hole created inside the gutta-percha allows the files to go through inside the filling material. However, the cutting action of the instruments could have concentrated more along the curved area. Consequently, this could prevent the centering ability of the files as it was previously reported [42]. In addition, it could be attributed that the presence of severe curvature could have increased the residual filling material due to the curvature limits the access of the file to one aspect of the canal, whereas other parts of the canal remain untouched.
In the literature, either primer root canal treatment or retreatment studies related to extruded debris caused by Reciproc system reported contradicting results. It was reported that Reciproc system caused less or more debris extrusion in primer root canal treatment [18,29,43]. Similarly, Reciproc system resulted in less or more debris extrusion during retreatment studies [12,19,44]. In the present study, even though PTU-R, R-Endo, and H-file systems extruded significantly more debris in severely curved root canals, curvature did not have a statistically significant impact on the amount of extruded debris caused by Reciproc system. Moreover, Reciproc system removed less filling material both in straight and curved root canals.
Although Reciproc system was assessed in the current study during the retreatment procedure in terms of the debris extrusion and residual filling material, it was developed for primer root canal treatment purposes. Contrary to the primer root canal treatment, files encounter a restriction within the root canal filling material during the retreatment procedure. Therefore, it could not be anticipated for Reciproc system to remove the root canal filling material as effective as the Ni-Ti files that were designed especially for retreatment purposes. The results associated with the Reciproc system could be explained by its ineffectiveness of removing the root canal filling material during the retreatment procedure.
While there was more residual filling material on the root canal walls, it could be anticipated that there would be less extruded debris. However, aligning with Kaşıkçı Bilgi et al. [12] and Azim et al. [32], the present study revealed that the correlation between the amount of extruded debris and residual filling material was insignificant. Both of these parameters were more accentuated in severely curved root canals, and it is reasonable to speculate that this is a consequence of the difficult morphology of severely curved root canal.
CONCLUSIONS
All instruments used in this study caused apical debris extrusion and none of them could completely remove the filling material. Although the instrument type affected only the residual filling material, root canal curvature had an effect both on extruded debris except for Reciproc, and residual filling material. Clinicians should be aware that the difficult morphology of the severely curved root canals is a factor increasing the amount of extruded debris during the retreatment procedure.
ACKNOWLEDGEMENT
The authors thank Professor Dr. Pelin Güneri and Associate Professor Timur Köse for their valuable suggestions.
-
Funding: This study was funded and supported by Ege University Scientific Research Project Fund (project number 2016/DIS/015).
-
Conflict of Interest: No potential conflict of interest relevant to this article was reported.
-
Author Contributions:
Conceptualization: Serefoglu B, Çalışkan MK.
Data curation: Serefoglu B, Kandemir Demirci G, Miçooğulları Kurt S.
Formal analysis: Serefoglu B.
Investigation: Serefoglu B, Demirci G, Miçooğulları Kurt S, Kaşıkçı Bilgi I.
Methodology: Serefoglu B, Çalışkan MK.
Project administration: Serefoglu B.
Resources: Serefoglu B.
Supervision: Çalışkan MK.
Validation: Çalışkan MK.
Visualization: Demirci G, Miçooğulları Kurt S, Kaşıkçı Bilgi I.
Writing - original draft: Serefoglu B, Çalışkan MK.
Writing - review & editing: Serefoglu B, Demirci G, Miçooğulları Kurt S, Kaşıkçı Bilgi I, Çalışkan MK.
- 1. Machtou P, Reit C. Non-surgical retreatment. In: Bergenholtz G, Hørsted-Bindslev P, Reit C, editors. Textbook of endodontology. 1st ed. Oxford: Blackwell Munksgaard; 2003. p. 300-310.
- 2. Bergenholtz G, Lekholm U, Milthon R, Heden G, Odesjö B, Engström B. Retreatment of endodontic fillings. Scand J Dent Res 1979;87:217-224.ArticlePubMed
- 3. Çalışkan MK. Nonsurgical retreatment of teeth with periapical lesions previously managed by either endodontic or surgical intervention. Oral Surg Oral Med Oral Pathol Oral Radiol Endod 2005;100:242-248.ArticlePubMed
- 4. Hülsmann M, Drebenstedt S, Holscher C. Shaping and filling root canals during root canal re-treatment. Endod Topics 2008;19:74-124.Article
- 5. Betti LV, Bramante CM. Quantec SC rotary instruments versus hand files for gutta-percha removal in root canal retreatment. Int Endod J 2001;34:514-519.ArticlePubMedPDF
- 6. Bernardes RA, Duarte MA, Vivan RR, Alcalde MP, Vasconcelos BC, Bramante CM. Comparison of three retreatment techniques with ultrasonic activation in flattened canals using micro-computed tomography and scanning electron microscopy. Int Endod J 2016;49:890-897.ArticlePubMedPDF
- 7. Hülsmann M, Bluhm V. Efficacy, cleaning ability and safety of different rotary NiTi instruments in root canal retreatment. Int Endod J 2004;37:468-476.ArticlePubMed
- 8. Siqueira JF Jr, Rôças IN, Ricucci D, Hülsmann M. Causes and management of post-treatment apical periodontitis. Br Dent J 2014;216:305-312.ArticlePubMedPDF
- 9. Huang X, Ling J, Wei X, Gu L. Quantitative evaluation of debris extruded apically by using ProTaper Universal Tulsa rotary system in endodontic retreatment. J Endod 2007;33:1102-1105.ArticlePubMed
- 10. Topçuoğlu HS, Aktı A, Tuncay Ö, Dinçer AN, Düzgün S, Topçuoğlu G. Evaluation of debris extruded apically during the removal of root canal filling material using ProTaper, D-RaCe, and R-Endo rotary nickel-titanium retreatment instruments and hand files. J Endod 2014;40:2066-2069.ArticlePubMed
- 11. Sae-Lim V, Rajamanickam I, Lim BK, Lee HL. Effectiveness of ProFile. 04 taper rotary instruments in endodontic retreatment. J Endod 2000;26:100-104.ArticlePubMed
- 12. Kaşıkçı Bilgi I, Köseler I, Güneri P, Hülsmann M, Çalışkan MK. Efficiency and apical extrusion of debris: a comparative ex vivo study of four retreatment techniques in severely curved root canals. Int Endod J 2017;50:910-918.ArticlePubMedPDF
- 13. Schirrmeister JF, Wrbas KT, Meyer KM, Altenburger MJ, Hellwig E. Efficacy of different rotary instruments for gutta-percha removal in root canal retreatment. J Endod 2006;32:469-472.ArticlePubMed
- 14. Pruett JP, Clement DJ, Carnes DL Jr. Cyclic fatigue testing of nickel-titanium endodontic instruments. J Endod 1997;23:77-85.ArticlePubMed
- 15. Myers GL, Montgomery S. A comparison of weights of debris extruded apically by conventional filing and Canal Master techniques. J Endod 1991;17:275-279.ArticlePubMed
- 16. Ruiz-Hubard EE, Gutmann JL, Wagner MJ. A quantitative assessment of canal debris forced periapically during root canal instrumentation using two different techniques. J Endod 1987;13:554-558.ArticlePubMed
- 17. Fukushima H, Yamamoto K, Hirohata K, Sagawa H, Leung KP, Walker CB. Localization and identification of root canal bacteria in clinically asymptomatic periapical pathosis. J Endod 1990;16:534-538.ArticlePubMed
- 18. Bürklein S, Schäfer E. Apically extruded debris with reciprocating single-file and full-sequence rotary instrumentation systems. J Endod 2012;38:850-852.ArticlePubMed
- 19. Çanakçi BC, Ustun Y, Er O, Genc Sen O. Evaluation of apically extruded debris from curved root canal filling removal using 5 nickel-titanium systems. J Endod 2016;42:1101-1104.ArticlePubMed
- 20. Delai D, Boijink D, Hoppe CB, Grecca AS, Kopper PM. Apically extruded debris in filling removal of curved canals using 3 NiTi systems and hand files. Braz Dent J 2018;29:54-59.ArticlePubMed
- 21. Friedman S, Stabholz A, Tamse A. Endodontic retreatment--case selection and technique. 3. Retreatment techniques. J Endod 1990;16:543-549.PubMed
- 22. Hinrichs RE, Walker WA 3rd, Schindler WG. A comparison of amounts of apically extruded debris using handpiece-driven nickel-titanium instrument systems. J Endod 1998;24:102-106.ArticlePubMed
- 23. Leonardi LE, Atlas DM, Raiden G. Apical extrusion of debris by manual and mechanical instrumentation. Braz Dent J 2007;18:16-19.ArticlePubMed
- 24. Karataslioglu E, Arslan H, Er G, Avci E. Influence of canal curvature on the amount of apically extruded debris determined by using three-dimensional determination method. Aust Endod J 2019;45:216-224.ArticlePubMedPDF
- 25. Kirchhoff AL, Fariniuk LF, Mello I. Apical extrusion of debris in flat-oval root canals after using different instrumentation systems. J Endod 2015;41:237-241.ArticlePubMed
- 26. Arslan H, Doğanay E, Alsancak M, Çapar ID, Karataş E, Gündüz HA. Comparison of apically extruded debris after root canal instrumentation using Reciproc® instruments with various kinematics. Int Endod J 2016;49:307-310.ArticlePubMed
- 27. Toyoğlu M, Altunbaş D. Influence of different kinematics on apical extrusion of irrigant and debris during canal preparation using K3XF instruments. J Endod 2017;43:1565-1568.ArticlePubMed
- 28. Üstün Y, Çanakçi BC, Dinçer AN, Er O, Düzgün S. Evaluation of apically extruded debris associated with several Ni-Ti systems. Int Endod J 2015;48:701-704.ArticlePubMed
- 29. Silva EJ, Carapiá MF, Lopes RM, Belladonna FG, Senna PM, Souza EM, De-Deus G. Comparison of apically extruded debris after large apical preparations by full-sequence rotary and single-file reciprocating systems. Int Endod J 2016;49:700-705.ArticlePubMed
- 30. Bürklein S, Benten S, Schäfer E. Quantitative evaluation of apically extruded debris with different single-file systems: Reciproc, F360 and OneShape versus Mtwo. Int Endod J 2014;47:405-409.PubMed
- 31. Hassanloo A, Watson P, Finer Y, Friedman S. Retreatment efficacy of the Epiphany soft resin obturation system. Int Endod J 2007;40:633-643.ArticlePubMed
- 32. Azim AA, Wang HH, Tarrosh M, Azim KA, Piasecki L. Comparison between single-file rotary systems: part 1-efficiency, effectiveness, and adverse effects in endodontic retreatment. J Endod 2018;44:1720-1724.ArticlePubMed
- 33. Taşdemir T, Er K, Yildirim T, Çelik D. Efficacy of three rotary NiTi instruments in removing gutta-percha from root canals. Int Endod J 2008;41:191-196.ArticlePubMed
- 34. Abramovitz I, Relles-Bonar S, Baransi B, Kfir A. The effectiveness of a self-adjusting file to remove residual gutta-percha after retreatment with rotary files. Int Endod J 2012;45:386-392.ArticlePubMed
- 35. Akbulut MB, Akman M, Terlemez A, Magat G, Sener S, Shetty H. Efficacy of Twisted File Adaptive, Reciproc and ProTaper Universal Retreatment instruments for root-canal-filling removal: a cone-beam computed tomography study. Dent Mater J 2016;35:126-131.ArticlePubMed
- 36. Rödig T, Reicherts P, Konietschke F, Dullin C, Hahn W, Hülsmann M. Efficacy of reciprocating and rotary NiTi instruments for retreatment of curved root canals assessed by micro-CT. Int Endod J 2014;47:942-948.PubMed
- 37. Keleş A, Alcin H, Kamalak A, Versiani MA. Oval-shaped canal retreatment with self-adjusting file: a micro-computed tomography study. Clin Oral Investig 2014;18:1147-1153.ArticlePubMedPDF
- 38. Monguilhott Crozeta B, Damião de Sousa-Neto M, Bianchi Leoni G, Francisco Mazzi-Chaves J, Terezinha Corrêa Silva-Sousa Y, Baratto-Filho F. A micro-computed tomography assessment of the efficacy of rotary and reciprocating techniques for filling material removal in root canal retreatment. Clin Oral Investig 2016;20:2235-2240.ArticlePubMedPDF
- 39. Hülsmann M. Research that matters - canal preparation, retreatment and working length studies. Int Endod J 2013;46:293-295.ArticlePubMed
- 40. Gergi R, Sabbagh C. Effectiveness of two nickel-titanium rotary instruments and a hand file for removing gutta-percha in severely curved root canals during retreatment: an ex vivo study. Int Endod J 2007;40:532-537.ArticlePubMed
- 41. Takahashi CM, Cunha RS, de Martin AS, Fontana CE, Silveira CF, da Silveira Bueno CE. In vitro evaluation of the effectiveness of ProTaper universal rotary retreatment system for gutta-percha removal with or without a solvent. J Endod 2009;35:1580-1583.ArticlePubMed
- 42. Gogulnath D, Rajan RM, Arathy G, Kandaswamy D. A comparative evaluation of the canal centering ability of three rotary nickel-titanium retreatment systems in the mesio-buccal canals of mandibular first molars using computed tomography. J Conserv Dent 2015;18:310-314.ArticlePubMedPMC
- 43. Topçuoğlu HS, Zan R, Akpek F, Topçuoğlu G, Ulusan Ö, Aktı A, Düzgün S, Ağırnaslıgil M. Apically extruded debris during root canal preparation using Vortex Blue, K3XF, ProTaper Next and Reciproc instruments. Int Endod J 2016;49:1183-1187.PubMed
- 44. Dincer AN, Er O, Canakci BC. Evaluation of apically extruded debris during root canal retreatment with several NiTi systems. Int Endod J 2015;48:1194-1198.ArticlePubMed
REFERENCES
Tables & Figures
REFERENCES
Citations
Citations to this article as recorded by 
- Evaluation of the Effectiveness of MicroMega Remover, ProTaper Universal Retreatment, Reciproc, and Hedstrom Files in the Retreatment of Curved Root Canals Obturated with Different Techniques: A Micro-Computed Tomography Study
Pınar Hava Dursun, Fatma Semra Sevimay, Arda Buyuksungur, Berkan Celikten
Medicina.2026; 62(1): 188. CrossRef - Remaining Root Filling Material in Oval Canals After Retreatment Using MicroMega Remover and Reciproc Blue Systems with and Without Passive Ultrasonic Irrigation: A Micro-CT Study
Furkan Konus, Faruk Oztekin
Journal of Clinical Medicine.2026; 15(12): 4822. CrossRef - Comparative Analysis of Root Canal Curvature Measurement Methods for Permanent Mandibular Molars Distal Root: An Observational Study
Tanu Singh, Saurav Bathla, Anuraag Gurtu, Shubhi Gupta, Sana Saifi, Madhusudan Astekar
The Journal of Contemporary Dental Practice.2025; 26(10): 945. CrossRef - Do Continuous Rotating Endodontic Instruments Extrude Fewer Apical Debris Than Reciprocating Instruments in Non-Surgical Endodontic Retreatments? A Systematic Review
Francesco Puleio, Francesco Giordano, Ugo Bellezza, David Rizzo, Valentina Coppini, Roberto Lo Giudice
Applied Sciences.2024; 14(4): 1621. CrossRef - Intracanal removal and apical extrusion of filling material after retreatment using rotary or reciprocating instruments: A new approach using human cadavers
Thamyres M. Monteiro, Victor O. Cortes‐Cid, Marilia F. V. Marceliano‐Alves, Andrea F. Campello, Luan F. Bastos, Ricardo T. Lopes, José F. Siqueira, Flávio R. F. Alves
International Endodontic Journal.2024; 57(1): 100. CrossRef - Comparative analysis of methods for measuring root canal curvature based on periapical radiography: A laboratory study
Rafael Chies Hartmann, Eduardo Silva Ferraz, Theodoro Weissheimer, Jose Antônio Poli de Figueiredo, Giampiero Rossi‐Fedele, Maximiliano Schünke Gomes
International Endodontic Journal.2024; 57(12): 1848. CrossRef - Evaluation of apically extruded debris during root canal filling material removal in teeth with external apical root resorption: a comparison of different obturation techniques
Büşra Melike Çağlar, İsmail Uzun
BMC Oral Health.2024;[Epub] CrossRef - Evaluation of apically extruded debris using protaper universal, protaper next, one curve, Xp shaper, and edge file: An in vitro study
Murtada Qadir Muhaibes, Shatha Abdulkareem Alwakeel
Saudi Endodontic Journal.2024; 14(1): 31. CrossRef - A quantitative comparison of apically extruded debris during root canal preparation using NiTi full-sequence rotary and single-file rotary systems: An in vitro study
Pallavi Goel, R. Vikram, R. Anithakumari, M. S. Adarsha, M. E. Sudhanva
Endodontology.2024; 36(3): 235. CrossRef - In vitro evaluation of filling material removal and apical debris extrusion after retreatment using Reciproc blue, Hyflex EDM and ProTaper retreatment files
Passent Abdelnaby, Mohamed Ibrahim, Rania ElBackly
BMC Oral Health.2023;[Epub] CrossRef - A Comparative Study on the Shaping Ability and Cleaning Efficiency of Two Different Single-File Systems, Reciprocating Wave One Versus Continuous Rotation F360, Evaluated by Scanning Electron Microscope: An In Vitro Study
Arunkumar Samudrala, Chandrakanth Majeti, Kommineni Harika Chowdary, Lakshmi Bhavani Potru, Anusha Yaragani, Yata Prashanth Kumar, Gagandeep K Sidhu, Navneet S Kathuria
Cureus.2023;[Epub] CrossRef - COMPARATIVE EVALUATION OF THE EFFECT OF DIFFERENT ROTARY INSTRUMENT SYSTEMS ON THE AMOUNT OF APICALLY EXTRUDED DEBRIS
Recai ZAN, Bilge LENGER
Cumhuriyet Dental Journal.2022; 25(2): 172. CrossRef - A critical analysis of research methods and experimental models to study apical extrusion of debris and irrigants
Jale Tanalp
International Endodontic Journal.2022; 55(S1): 153. CrossRef - Critical analysis of research methods and experimental models to study removal of root filling materials
Mahdi A. Ajina, Pratik K. Shah, Bun San Chong
International Endodontic Journal.2022; 55(S1): 119. CrossRef
 ePub Link
ePub Link Cite
CiteImpact of root canal curvature and instrument type on the amount of extruded debris during retreatment
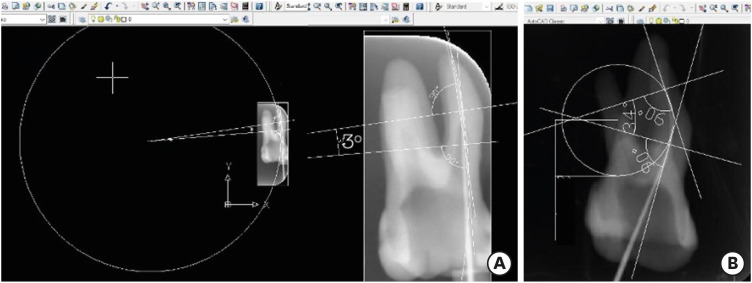
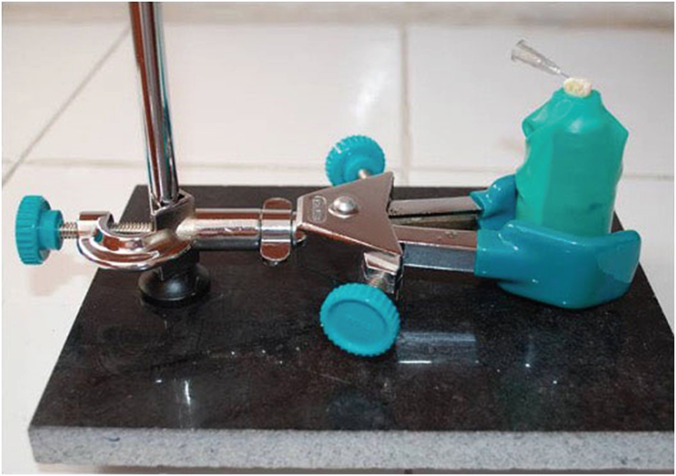
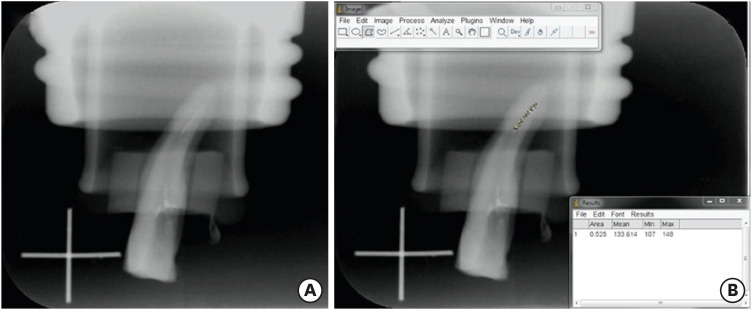
Figure 1 The root canal curvature and radius measurement according to Pruett et al. [14] using AutoCAD software. (A) Straight canal, (B) severely curved root canal.
Figure 2 The experimental set-up for the collection of the extruded debris.
Figure 3 (A) An image showing the residual filling material on the root canal walls (B) calculation of the area of residual filling material using Image J software.
Figure 1
Figure 2
Figure 3
Impact of root canal curvature and instrument type on the amount of extruded debris during retreatment
Amount of extruded debris (g) associated with the 4 nickel-titanium (Ni-Ti) file systems in severely curved and straight canals
| Instrument type | Extruded material (g) | p value | |
|---|---|---|---|
| Severely curved canals | Straight canals | ||
| H-file | 0.00203 ± 0.00090 | 0.000623 ± 0.00045 | < 0.001 |
| R-Endo | 0.00173 ± 0.00124 | 0.00093 ± 0.00098 | 0.013 |
| Reciproc | 0.00149 ± 0.00171 | 0.00095 ± 0.00090 | 0.246 |
| PTU-R | 0.00187 ± 0.00115 | 0.00068 ± 0.00073 | < 0.001 |
Values are presented as mean ± standard deviation.
PTU-R, ProTaper Universal Retreatment.
Radiographic assessment of the area of residual filling material (mm2)
| Canal thirds | Instrument type | |||||||
|---|---|---|---|---|---|---|---|---|
| Severely curved canals | Straight canals | |||||||
| H file | R-Endo | Reciproc | PTU-R | H file | R-Endo | Reciproc | PTU-R | |
| Coronal | 0.522 ± 0.403 | 0.600 ± 0.506 | 0.694 ± 0.393 | 0.522 ± 0.483 | 0.113 ± 0.211 | 0.025 ± 0.044 | 0.084 ± 0.164 | 0.145 ± 0.256 |
| Middle | 0.295 ± 0.341 | 0.523 ± 0.680 | 0.915 ± 0.952 | 0.369 ± 0.430 | 0.107 ± 0.138 | 0.063 ± 0.130 | 0.116 ± 0.233 | 0.219 ± 0.274 |
| Apical | 0.180 ± 0.332 | 0.380 ± 0.418 | 0.193 ± 0.277 | 0.345 ± 0.500 | 0.068 ± 0.079 | 0.108 ± 0.146 | 0.181 ± 0.200 | 0.238 ± 0.260 |
| Total | 0.998 ± 0.697 | 1.505 ± 1.164 | 1.799 ± 1.019 | 1.237 ± 1.117 | 0.289 ± 0.304 | 0.197 ± 0.248 | 0.433 ± 0.435 | 0.599 ± 0.556 |
Values are presented as mean ± standard deviation.
SD, standard deviation; PTU-R, ProTaper Universal Retreatment.
Correlation between extruded debris and residual filling material
| Curvature type | Residual filling material | ||||||
|---|---|---|---|---|---|---|---|
| Value | H-file | R-Endo | Reciproc | PTU-R | |||
| Severely curved canals | |||||||
| Extruded debris | |||||||
| H-file | r | 0.344 | |||||
| p | 0.085 | ||||||
| R-Endo | r | −0.286 | |||||
| p | 0.157 | ||||||
| Reciproc | r | −0.212 | |||||
| p | 0.299 | ||||||
| PTU-R | r | −0.162 | |||||
| p | 0.429 | ||||||
| Straight canals | |||||||
| Extruded debris | |||||||
| H-file | r | 0.111 | |||||
| p | 0.590 | ||||||
| R-Endo | r | 0.146 | |||||
| p | 0.478 | ||||||
| Reciproc | r | 0.026 | |||||
| p | 0.898 | ||||||
| PTU-R | r | −0.254 | |||||
| p | 0.211 | ||||||
PTU-R, ProTaper Universal Retreatment.
Table 1 Amount of extruded debris (g) associated with the 4 nickel-titanium (Ni-Ti) file systems in severely curved and straight canals
Values are presented as mean ± standard deviation.
PTU-R, ProTaper Universal Retreatment.
Table 2 Radiographic assessment of the area of residual filling material (mm2)
Values are presented as mean ± standard deviation.
SD, standard deviation; PTU-R, ProTaper Universal Retreatment.
Table 3 Correlation between extruded debris and residual filling material
PTU-R, ProTaper Universal Retreatment.

