
Articles
- Page Path
- HOME > Restor Dent Endod > Volume 46(3); 2021 > Article
- Research Article Effect of adhesive application method on repair bond strength of composite
-
Hee Kyeong Oh
 , Dong Hoon Shin
, Dong Hoon Shin -
Restor Dent Endod 2021;46(3):e32.
DOI: https://doi.org/10.5395/rde.2021.46.e32
Published online: June 4, 2021
Department of Conservative Dentistry, Graduate School, Dankook University College of Dentistry, Cheonan, Korea.
- Correspondence to Dong Hoon Shin, DDS, PhD. Professor, Department of Conservative Dentistry, Graduate School, Dankook University College of Dentistry, 119 Dandae-ro, Dongnam-gu, Cheonan, 31116, Korea. donyshin@dankook.ac.kr
• Received: July 20, 2020 • Revised: November 7, 2020 • Accepted: December 16, 2020
Copyright © 2021. The Korean Academy of Conservative Dentistry
This is an Open Access article distributed under the terms of the Creative Commons Attribution Non-Commercial License (https://creativecommons.org/licenses/by-nc/4.0/) which permits unrestricted non-commercial use, distribution, and reproduction in any medium, provided the original work is properly cited.
Abstract
-
Objectives This study aimed to evaluate the effect of the application method of universal adhesives on the shear bond strength (SBS) of repaired composites, applied with different thicknesses.
-
Materials and Methods The 84 specimens (Filtek Z350 XT) were prepared, stored in distilled water for a week and thermocycled (5,000 cycles, 5°C to 55°C). They were roughened using 400-grit sandpapers and etched with phosphoric acid. Then, specimens were equally divided into 2 groups; Single Bond Universal (SU) and Prime&Bond Universal (PB). Each group was subdivided into 3 subgroups according to application methods (n = 14); UC: 1 coat + uncuring, 1C: 1 coat + curing, 3C: 3 coats + curing. After storage of the repaired composite for 24 hours, specimens were subjected to the SBS test and the data were statistically analyzed by 2-way analysis of variance and independent t-tests. Specimens were examined with a stereomicroscope to analyze fracture mode and a scanning electron microscope to observe the interface.
-
Results Adhesive material was a significant factor (p = 0.001). Bond strengths with SU were higher than PB. The highest strength was obtained from the 1C group with SU. Bonding in multiple layers increased adhesive thicknesses, but there was no significant difference in SBS values (p = 0.255). Failure mode was predominantly cohesive in old composites.
-
Conclusions The application of an adequate bonding system plays an important role in repairing composite resin. SU showed higher SBS than PB and the additional layers increased the adhesive thickness without affecting SBS.
INTRODUCTION
An increasing focus on dental aesthetics and the development of new materials and techniques have led to an increase in resin restorations. When clinicians are faced with defective restorations, they need to decide whether to replace or repair the restorations. As part of the healthy tooth is removed together to replace the restoration, the size of the restoration increases and the likelihood of pulp irritation increases, which shortens the life of the tooth [1]. Due to the development of adhesive dentistry over the last few decades, repair, as opposed to replacement, may increase the clinical longevity of the restorations and prolong the long-term life of the tooth [2,3].
Bonding between aged and repaired resin composites is partly achieved by the critical amount of the unreacted monomer. However, aged composites have a diminished number of carbon double bonds to react with repaired composites [4]. A wide variety of methods have been proposed to increase the bond strength between aged and freshly added composites; surface roughening with burs, etching with phosphoric or hydrofluoric acid, air-borne particle abrasion with aluminum oxide particles, application of a silane coupling agent, and adhesive systems [5,6,7,8,9,10,11,12,13].
Universal adhesives have been developed and used in a large variety of restorative applications. They can be used to bond with metals, composites, ceramics as well as teeth and can be applied through total-etch, self-etch, and selective-etch modes according to the clinician's preference and specific clinical situation. Additionally, they are compatible with light-cure, self-cure, and dual-cure resin-based cements, so they can be used for the placement of both direct and indirect restorations [14,15]. In addition, some universal adhesives already contain a silane composition, although there is a controversy about the efficacy of the silane [16].
When considering the bond strength between dentin and composites, multiple applications of dental adhesives increase the thickness of the adhesive layer, which is related to high shear bond strength (SBS) [17,18]. However, in a repair, the thickness of the adhesive layer, which is considered the weakest part should be minimized. It has even been stated that not curing the adhesive before the composite placement allows for intimate contact between aged and repaired composite and a thinner adhesive layer renders higher bond strength [19,20].
The objectives of this study were to assess the SBS between aged and repaired composite with different application protocols, and to determine the effects of adhesives on the bond strength. The null hypothesis of the present study was that the SBS of repaired composite will not be affected by (i) different adhesives and (ii) application methods of adhesives.
MATERIALS AND METHODS
The materials are listed in Table 1 with associated components. This study was carried out in 2 main groups according to the adhesive system used. Each main group was further divided into 3 subgroups according to application methods. In all groups, the same composite was used as a repair material.
Table 1
Materials used in this study
SU, Single Bond Universal; PB, Prime&Bond Universal; 10-MDP, 10-methacryloyloxydecyl dihydrogen phosphate; bis-GMA, bisphenol A-glycidyl methacrylate; UDMA, urethane dimethacrylate; TEGDMA, triethylene glycol dimethacrylate; bis-EMA, ethoxylated bisphenol-A dimethacrylate; PEGDMA, poly(ethylene glycol) dimethacrylate; HEMA, 2-hydroxyethyl methacrylate.
Since there is no protocol for repairing resin restorations, the general protocol for direct resin restoration was used in the case of applying the adhesive once. The general application methods by manufacturers are shown in Table 2.
Table 2
General application protocol for direct resin restorations
A rectangular mold made of polypropylene was used to prepare 84 samples (10 × 10 × 2 mm) of Filtek Z350 XT composite. Each increment was light-polymerized with a light-curing device (Skylight, Dmetec, Bucheon, Korea) for 30 seconds. The wavelength was between 440 and 490 nm and the radiant emittance was 1,000 mW/cm2. The sample was removed from the mold and the specimens were then embedded in a cylinder-shaped mold (25 × 25 × 13 mm) and filled with self-cure acrylic resin (Ortho-Jet, Lang Dental Manufacturing Company, Wheeling, IL, USA).
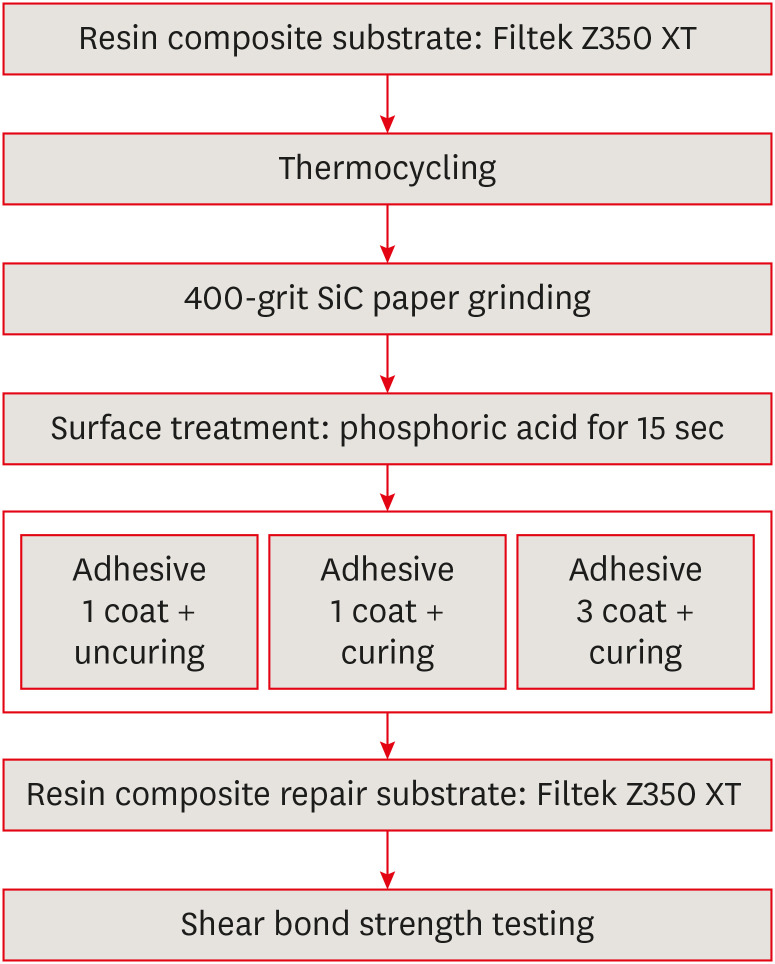
The specimens were aged by thermal cycling 5,000 times between 5°C and 55°C, with a dwell time of 10 seconds and transfer time of 10 seconds. Then, the specimens were all surfaced flat with a 400-grit silicon carbide sandpaper under running water to obtain a standardized roughness. The phosphoric acid (Etchant, Shinhung, Seoul, Korea) etching on each specimen was conducted for cleaning for 15 seconds. Subsequently, specimens were classified into 2 groups according to the adhesive systems; Single Bond Universal (SU) or Prime&Bond Universal (PB). Then, each group was subdivided into 3 subgroups according to the application methods; 1 coat + uncuring (UC), 1 coat + curing (1C), 3 coats + curing (3C). In the case of applying the adhesive, the protocol suggested by the manufacturer for bonding was used. When applying 3 times for 3C groups, air blow and light polymerization were separately performed for each layer. The experimental designs are shown in Figure 1. All samples were kept in distilled water for 2 weeks before carrying out the repair process.
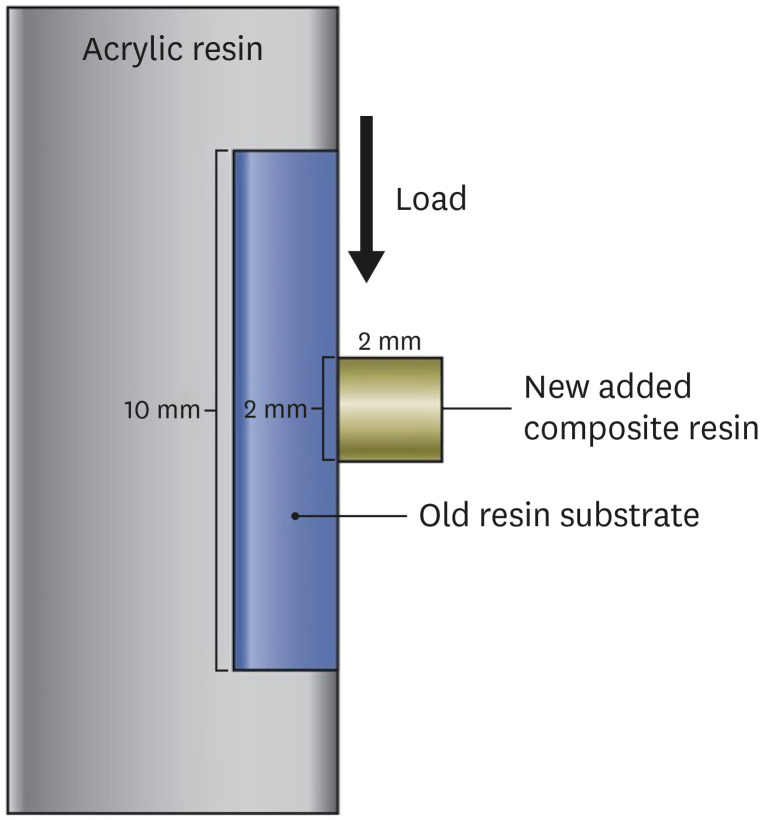
The 2 mm thick layer of composite resin was added into a plastic mold (Ultradent jig, Ultradent Products, South Jordan, UT, USA) and then light polymerized under 1,000 mW/cm2 power light gun for 20 seconds.
After 24-hour storage in distilled water, samples were submitted to the SBS test (Shear Bond Tester, Bisco Inc., Schaumburg, IL, USA) (Figure 2). The measured values were then divided by the area of the adhesive surface (4.34 mm2) and converted to units of MPa.
Failure modes were analyzed at a magnification of ×20 with a microscope. The results were classified as mixed, adhesive and cohesive failures.
One specimen of each group was made for the analysis of the interface, which was observed by a scanning electron microscope (SEM) at an accelerating voltage of 10 kV after sputter coating with gold powder.
Statistical analyses were conducted using commercial statistical software (SPSS Statistics 23, IBM, Armonk, NY, USA). The normality of data distribution was tested using the Shapiro-Wilk test. A 2-way analysis of variance (ANOVA) test was applied to SBS data with “adhesives” and “application methods” as factors. After verifying which factor causes the difference, an independent t-test was then used for comparisons of SBS data of 2 adhesive systems. All tests were run at the significance level of p < 0.05.
RESULTS
The mean bond strengths and average deviations are presented in Table 3. The results of the 2-way ANOVA test showed there was a significant difference according to the adhesives (p = 0.001) but no significant difference depending on the application methods (p = 0.255) and the interaction between these 2 factors (p = 0.900). It was observed through the independent t-test that the bond strengths of SU were higher than those of PB (p < 0.05).
Table 3
Shear bond strength values (MPa)
Analysis of the failure mode showed that the greatest number of failures found were cohesive in old resin (Table 4).
Table 4
Failure mode analysis
Figures 3 and 4 present SEM images of the bonding interface obtained after the application of the tested adhesives. They showed that multiple adhesive applications produced an increase in adhesive layer thickness for 2 adhesive systems. SU showed a thicker adhesive layer than PB. No clear adhesive layer could be observed in both adhesives without curing.
Figure 3
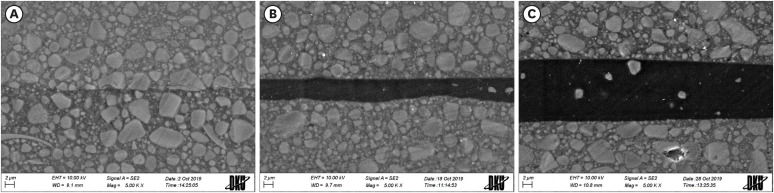
Scanning electron microscopy images of bonding interface obtained by application of Single Bond Universal (SU): (A) SU-UC, 1 coat + uncuring; (B) SU-1C, 1 coat + curing; (C) SU-3C, 3 coats + curing (×5,000).
WD, working distance; EHT, electron high tension.
Figure 4
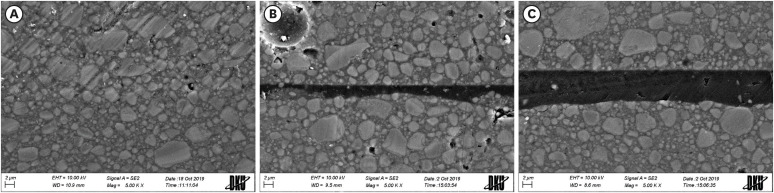
Scanning electron microscopy images of bonding interface obtained by application of Prime&Bond Universal (PB): (A) PB-UC, 1 coat + uncuring; (B) PB-1C, 1 coat + curing; (C) PB-3C, 3 coats + curing (×5,000).
WD, working distance; EHT, electron high tension.
At any of 3 points, the thickness of the adhesive layer was measured and averaged. The results are shown in Table 5.
Table 5
Thickness of adhesive layer (μm)
| Adhesives | Method of application | ||
|---|---|---|---|
| UC | 1C | 3C | |
| SU | Not measurable | 4.28 | 12.87 |
| PB | Not measurable | 2.47 | 7.30 |
DISCUSSION
This study evaluated the effect of different adhesives and application methods of adhesives on the SBS of repairs in a nanocomposite. The null hypothesis was partly rejected, as significant differences were found between different adhesives, but not between application methods.
When resin restorations fracture or secondary caries occur, repairs are known to benefit the life of the tooth rather than replacements. The replacement of the entire restoration will inevitably lead to a larger restoration as the healthy tooth substrates are removed [1]. In the repair process, it is important to obtain a high bond strength between the aged and repaired composite substrates. It is known that applying an adhesive on the underlying aged substrates improves the repair bond strength between the aged and repaired composite [21,22]. In this study, we investigated the influence of the application methods of universal adhesives on the repair SBS of a newly filled composite applied to the old composite substrates.
Universal adhesives were developed to simplify various dental restoration procedures. Previous studies have shown that universal adhesives have comparable bond strengths compared to previous generations of adhesive systems [14,23]. In this study, 2 universal adhesives were evaluated; SU and PB. Since SU was the first universal adhesive available after the patent for 10-methacryloyloxydecyl dihydrogen phosphate expired, it is widely used not only in clinics but also in various experimental studies [14]. Meanwhile, PB was launched later and features low film thickness. As the film thickness is expected to affect the repair bond strength, the 2 adhesives mentioned above were selected and tested in this experiment.
Unlike relying on micromechanical and chemical bonding between resin and tooth, the repair bond strength between aged and repaired composite substrates depends much more on the micromechanical bonding by surface roughening [21]. When a high viscosity composite is applied to this rough surface, it is difficult to achieve a mechanical interlocking. Therefore, the application of an adhesive with low viscosity prior to the repair is recommended in general to achieve a higher bond strength [22,24].
However, the adhesive layer in the repair process is regarded as the weakest part and the adhesive needs to act just as a wetting agent [19]. Contrary to the fact that the thick adhesive layer acts as a shock-absorbing layer between the tooth substrate and composites to thus disperse the stress at the interface, a minimally thin adhesive layer is required in the repair process, so that the substrates fit together as tightly as possible [25]. Eliasson et al. [20] reported that repairing composite restorations was enhanced by the use of an adhesive rendering a thin bonding layer and not curing the adhesive before placement of composite made an ideal situation for repairs between aged and repaired composites. Very intimate contact was observed between aged and repaired substrates under a light microscope when not curing the adhesive separately. It was believed that the repaired composite squeezed the uncured adhesive.
In this study, it was also found that if the adhesive was not cured, a clear adhesive layer did not appear on the SEM analysis, signifying intimate contact between substrates accomplished by squeezing pressure. However, this did not lead to an improvement in bond strength. The mean thickness of 1 layer of cured adhesive was measured at randomly selected 3 points and was approximately 4.28 μm for SU and 2.47 μm for PB, respectively. Each of the 3 layers applied increased the thickness accordingly, but there was no significant difference in the SBS. It was found that the multiple application of universal adhesives did not improve the repair bond strength. This is in contrast to the report showing higher bond strength between teeth and composite when applying bonding agents several times [18].
In the statistical analysis, SU, which contains silane in its composition, showed a higher SBS than that of PB. Although most of the bond strength is obtained from micromechanical bonds, some is achieved due to chemical bonds [21]. Silane may form siloxane bonds to promote chemical bonding between silicate-containing filler particles exposed on the surface and the resin matrix of the fresh resin layer [6]. It could be postulated that the silane contained in SU helps to improve the bond strength between aged and repaired composite. Yet more research would be needed to prove this effect because other studies show that the silane contained in the adhesive has no discernible effect on the bond strength. It was stated that only freshly mixed silane helped to improve the bond strength [16]. In addition, silane did not significantly affect the bond strength, depending on the substrates and thermocycling process [26]. Meanwhile, the group using PB showed a significantly lower SBS despite the comparatively thin film thickness. It could be inferred that the component itself had a significant influence on the bond strength rather than the thickness of the adhesive.
The bond strength is a force measured when the specimen fractures and when the adhesive failure occurs, it is the “true” bond strength. In this study, many of the test specimens showed cohesive failures in aged composite specimens. Della Bona and van Noort [27] suggested that the shear bond test measured the cohesive strength of the underlying composite. Cohesive failures in the underlying composite have been considered as evidence that the bond strength is superior to the cohesive strength of the parent substrate. It may also indicate that the underlying composite was weakened because of water sorption due to aging. However, the pull-out of substrates was partly due to the biomechanics of the test and did not indicate superior adhesive strength [28].
The composite substrate itself is also important to obtain a high repair bond strength. The nanocomposite used in this experiment, Filtek Z350 XT, consists of bisphenol A-glycidyl methacrylate (bis-GMA), ethoxylated bisphenol-A dimethacrylate (bis-EMA), urethane dimethacrylate (UDMA), and triethylene glycol dimethacrylate (TEGDMA). Hydrophilic TEGDMA absorbs greater amounts of water after thermocycling. It has a detrimental effect on the structural integrity of resin-based composites. The loose particles in the hydrolyzed Filtek Z350 XT resin matrix could easily detach. This would probably be the reason for the high percentage of cohesive failures.
Although the minimally required repair bond strength of the composite is unknown, repair bond strength was measured at a lower level that was far below that stated by the manufacturer even in the SU group with higher bond strength. The manufacturer of SU claims repair bond strengths above 20 MPa using their internal data [29]. The lower bond strength in this study may be due to the fact that repair was performed without mechanical roughening, such as air abrasion, which is recommended for the repair process.
There are a few limitations to this study. Clinicians perform surface preparation during resin repairing to remove surface contaminants and to form a rough surface [30]. In this experiment, 400-grit silicon carbide paper was used to obtain standardized surface coverage with smear layers similar to the surface created with a coarse diamond bur at a clinic [31]. However, it may be insufficient to simply prepare the surface to enhance micromechanical retention. Additional roughening, such as air abrasion, may need to be conducted during the preparation.
In this study, the SBS between the old and new composite substrates depends on the adhesive used, not on the application method. However, it is not yet possible to offer a universal repair protocol for all composites. Further studies are needed to assess the performance of these adhesives with different resin composites and over longer periods of time, allowing for aging.
CONCLUSIONS
The repair bond strength between aged and repaired composites depends on the adhesives used. However, application methods had no significant effect on the SBS between aged and repaired composites for the materials used in this study.
-
Conflict of Interest: No potential conflict of interest relevant to this article was reported.
-
Author Contributions:
- 1. Brantley CF, Bader JD, Shugars DA, Nesbit SP. Does the cycle of rerestoration lead to larger restorations? J Am Dent Assoc 1995;126:1407-1413.ArticlePubMed
- 2. Fernández E, Martín J, Vildósola P, Oliveira Junior OB, Gordan V, Mjor I, Bersezio C, Estay J, de Andrade MF, Moncada G. Can repair increase the longevity of composite resins? Results of a 10-year clinical trial. J Dent 2015;43:279-286.ArticlePubMed
- 3. Moncada G, Martin J, Fernández E, Hempel MC, Mjör IA, Gordan VV. Sealing, refurbishment and repair of class I and class II defective restorations: a three-year clinical trial. J Am Dent Assoc 2009;140:425-432.PubMed
- 4. Baur V, Ilie N. Repair of dental resin-based composites. Clin Oral Investig 2013;17:601-608.ArticlePubMedPDF
- 5. Rathke A, Tymina Y, Haller B. Effect of different surface treatments on the composite-composite repair bond strength. Clin Oral Investig 2009;13:317-323.ArticlePubMedPDF
- 6. Ahmadizenouz G, Esmaeili B, Taghvaei A, Jamali Z, Jafari T, Amiri Daneshvar F, Khafri S. Effect of different surface treatments on the shear bond strength of nanofilled composite repairs. J Dent Res Dent Clin Dent Prospect 2016;10:9-16.ArticlePubMedPMC
- 7. Loomans BA, Cardoso MV, Roeters FJ, Opdam NJ, De Munck J, Huysmans MC, Van Meerbeek B. Is there one optimal repair technique for all composites? Dent Mater 2011;27:701-709.ArticlePubMed
- 8. Loomans BA, Cardoso MV, Opdam NJ, Roeters FJ, De Munck J, Huysmans MC, Van Meerbeek B. Surface roughness of etched composite resin in light of composite repair. J Dent 2011;39:499-505.ArticlePubMed
- 9. Swift EJ Jr, LeValley BD, Boyer DB. Evaluation of new methods for composite repair. Dent Mater 1992;8:362-365.ArticlePubMed
- 10. Lucena-Martín C, González-López S, Navajas-Rodríguez de Mondelo JM. The effect of various surface treatments and bonding agents on the repaired strength of heat-treated composites. J Prosthet Dent 2001;86:481-488.ArticlePubMed
- 11. Fornazari IA, Wille I, Meda EM, Brum RT, Souza EM. Effect of surface treatment, silane, and universal adhesive on microshear bond strength of nanofilled composite repairs. Oper Dent 2017;42:367-374.ArticlePubMedPDF
- 12. Hisamatsu N, Atsuta M, Matsumura H. Effect of silane primers and unfilled resin bonding agents on repair bond strength of a prosthodontic microfilled composite. J Oral Rehabil 2002;29:644-648.ArticlePubMed
- 13. Söderholm KJ, Roberts MJ. Variables influencing the repair strength of dental composites. Scand J Dent Res 1991;99:173-180.ArticlePubMed
- 14. Alex G.. Universal adhesives: the next evolution in adhesive dentistry? Compend Contin Educ Dent 2015;36:15-26.PubMed
- 15. Nagarkar S, Theis-Mahon N, Perdigão J. Universal dental adhesives: current status, laboratory testing, and clinical performance. J Biomed Mater Res B Appl Biomater 2019;107:2121-2131.ArticlePubMedPDF
- 16. Yoshihara K, Nagaoka N, Sonoda A, Maruo Y, Makita Y, Okihara T, Irie M, Yoshida Y, Van Meerbeek B. Effectiveness and stability of silane coupling agent incorporated in ‘universal’ adhesives. Dent Mater 2016;32:1218-1225.ArticlePubMed
- 17. Chowdhury AF, Saikaew P, Alam A, Sun J, Carvalho RM, Sano H. Effects of double application of contemporary self-etch adhesives on their bonding performance to dentin with clinically relevant smear layers. J Adhes Dent 2019;21:59-66.PubMed
- 18. Zecin-Deren A, Sokolowski J, Szczesio-Wlodarczyk A, Piwonski I, Lukomska-Szymanska M, Lapinska B. Multi-layer application of self-etch and universal adhesives and the effect on dentin bond strength. Molecules 2019;24:345.ArticlePubMedPMC
- 19. Eliasson ST, Tibballs J, Dahl JE. Effect of different surface treatments and adhesives on repair bond strength of resin composites after one and 12 months of storage using an improved microtensile test method. Oper Dent 2014;39:E206-E216.ArticlePubMedPDF
- 20. Eliasson ST, Dahl JE. Effect of curing and silanizing on composite repair bond strength using an improved micro-tensile test method. Acta Biomater Odontol Scand 2017;3:21-29.ArticlePubMedPMCPDF
- 21. Brosh T, Pilo R, Bichacho N, Blutstein R. Effect of combinations of surface treatments and bonding agents on the bond strength of repaired composites. J Prosthet Dent 1997;77:122-126.ArticlePubMed
- 22. Imbery TA, Gray T, DeLatour F, Boxx C, Best AM, Moon PC. Evaluation of flexural, diametral tensile, and shear bond strength of composite repairs. Oper Dent 2014;39:E250-E260.ArticlePubMedPDF
- 23. Cardoso MV, de Almeida Neves A, Mine A, Coutinho E, Van Landuyt K, De Munck J, Van Meerbeek B. Current aspects on bonding effectiveness and stability in adhesive dentistry. Aust Dent J 2011;56(Suppl 1):31-44.ArticlePubMed
- 24. Valente LL, Sarkis-Onofre R, Goncalves AP, Fernandez E, Loomans B, Moraes RR. Repair bond strength of dental composites: systematic review and meta-analysis. Int J Adhes Adhes 2016;69:15-26.Article
- 25. Ausiello P, Apicella A, Davidson CL. Effect of adhesive layer properties on stress distribution in composite restorations--a 3D finite element analysis. Dent Mater 2002;18:295-303.ArticlePubMed
- 26. Wendler M, Belli R, Panzer R, Skibbe D, Petschelt A, Lohbauer U. Repair bond strength of aged resin composite after different surface and bonding treatments. Materials (Basel) 2016;9:547.ArticlePubMedPMC
- 27. Della Bona A, van Noort R. Shear vs. tensile bond strength of resin composite bonded to ceramic. J Dent Res 1995;74:1591-1596.ArticlePubMedPDF
- 28. Versluis A, Tantbirojn D, Douglas WH. Why do shear bond tests pull out dentin? J Dent Res 1997;76:1298-1307.ArticlePubMedPDF
- 29. 3M ESPE. Scotchbond Universal Technical Product Profile [Internet]. St. Paul, MN: 3M ESPE; 2013. cited 2019 Nov 25]. Available from: http://multimedia.3m.com/mws/media/754751O/scotchbond-universal-adhesive-technical-product-profile.
- 30. Ferracane JL. Resin composite--state of the art. Dent Mater 2011;27:29-38.ArticlePubMed
- 31. Ayar MK, Guven ME, Burduroglu HD, Erdemir F. Repair of aged bulk-fill composite with posterior composite: effect of different surface treatments. J Esthet Restor Dent 2019;31:246-252.ArticlePubMedPDF
REFERENCES
Tables & Figures
REFERENCES
Citations
Citations to this article as recorded by 
- The Effect of Adhesive Procedures on the Repair Bond Strength of Aged Universal Composites
Mehmet Semih Velioğlu, Merve Gürses, Fatma Sağ Güngör, Sinem Özdemir, Atiye Tuğba Kuzgun Türkmen, Nimet Ünlü
Selcuk Dental Journal.2026; 13(1): 129. CrossRef - The effect of different surface treatments and adhesive systems on shear bond strength in universal nanohybrid composite resin repair
Merve Kütük Ömeroğlu, Melek Çam, Işıl Doğruer, Zeynep Buket Kaynar
BMC Oral Health.2025;[Epub] CrossRef - Effect of Universal Adhesive Etching Mode on Shear Bond Strength of Pulp Capping Materials to Deep Dentin
Shahram Amirifar, Saba Tohidkhah, Seyedeh Mahsa Sheikh-Al-Eslamian, Mahdi Abbasi, Fatemeh Farshad, Elham Ahmadi, Carlos M. Ardila
BioMed Research International.2025;[Epub] CrossRef - Shear Bond Strength and Finite Element Stress Analysis of Composite Repair Using Various Adhesive Strategies With and Without Silane Application
Elif Ercan Devrimci, Hande Kemaloglu, Cem Peskersoy, Tijen Pamir, Murat Turkun
Applied Sciences.2025; 15(15): 8159. CrossRef
 ePub Link
ePub Link Cite
CiteEffect of adhesive application method on repair bond strength of composite
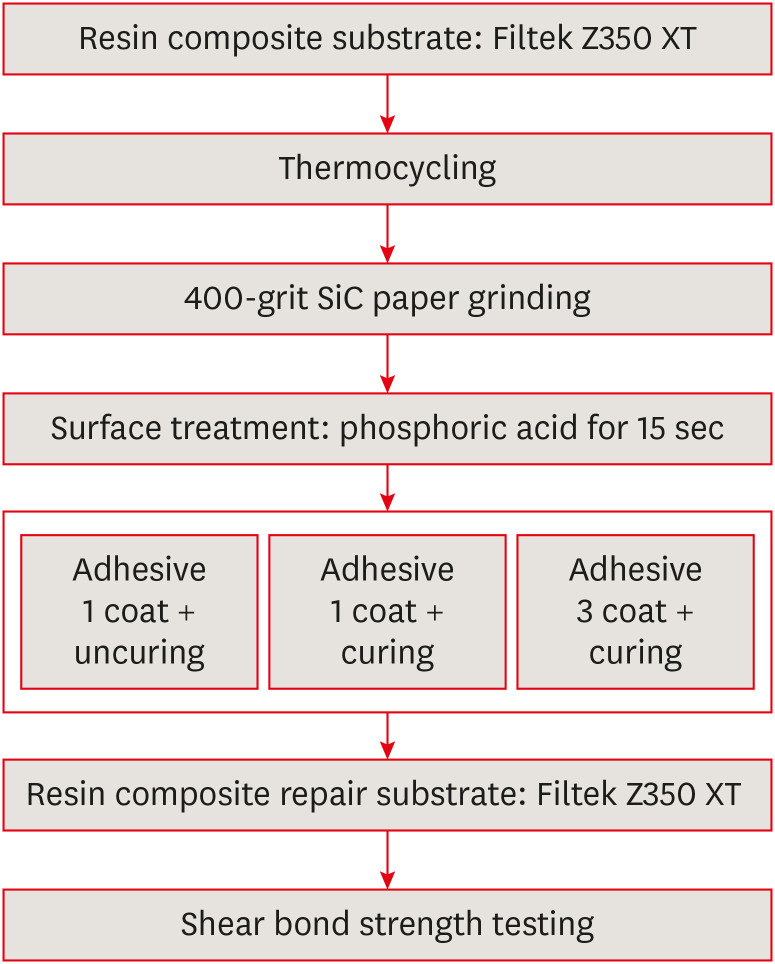
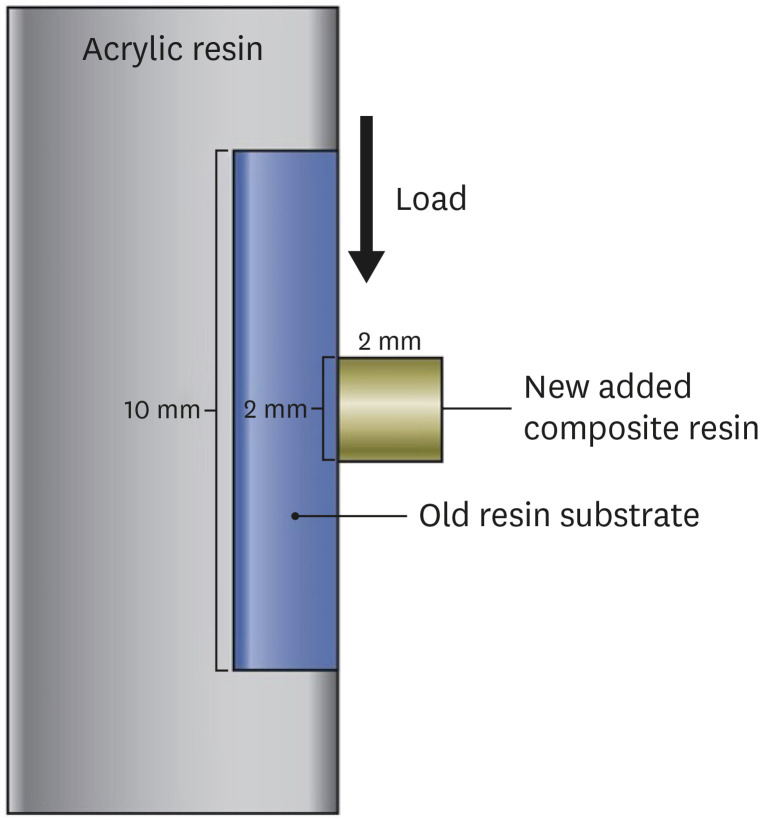
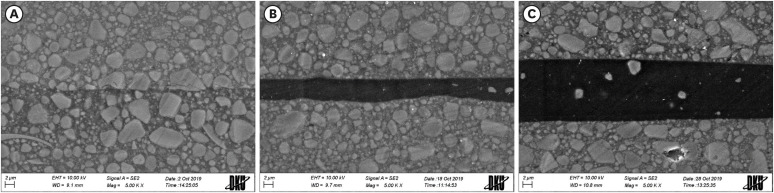
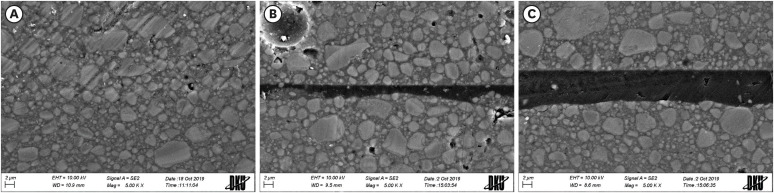
Figure 1 Experimental design of this study.
Figure 2 Schematic representation of the shear bond strength test.
Figure 3 Scanning electron microscopy images of bonding interface obtained by application of Single Bond Universal (SU): (A) SU-UC, 1 coat + uncuring; (B) SU-1C, 1 coat + curing; (C) SU-3C, 3 coats + curing (×5,000).WD, working distance; EHT, electron high tension.
Figure 4 Scanning electron microscopy images of bonding interface obtained by application of Prime&Bond Universal (PB): (A) PB-UC, 1 coat + uncuring; (B) PB-1C, 1 coat + curing; (C) PB-3C, 3 coats + curing (×5,000).WD, working distance; EHT, electron high tension.
Figure 1
Figure 2
Figure 3
Figure 4
Effect of adhesive application method on repair bond strength of composite
Materials used in this study
| Materials | Type of material | Component | Manufacturer |
|---|---|---|---|
| SU | Universal adhesive | 10-MDP, dimethacrylate resins, Vitrebond copolymer, HEMA, filler, ethanol, water, initiators, silane | 3M ESPE, St. Paul, MN, USA |
| PB | Universal adhesive | Phosphoric acid-modified acrylic resin, multifunctional acrylate, acid acrylate, bifunctional acrylate, isopranolol, water, initiators, stabilisators | Dentsply Caulk, Milford, DE, USA |
| Selection-K Etchant | Etchant | 37% phosphoric acid viscous gel, thickener | Shinhung, Seoul, Korea |
| Filtek Z350 XT Universal Restorative | Resin composite | bis-GMA, UDMA, TEGDMA, bis-EMA, PEDGMA, non-aggregated 4 to 10 nm zirconia, non-aggregated 20 nm silica and aggregated zirconia/silica cluster filler (63.3 vol%) | 3M ESPE, St. Paul, MN, USA |
SU, Single Bond Universal; PB, Prime&Bond Universal; 10-MDP, 10-methacryloyloxydecyl dihydrogen phosphate; bis-GMA, bisphenol A-glycidyl methacrylate; UDMA, urethane dimethacrylate; TEGDMA, triethylene glycol dimethacrylate; bis-EMA, ethoxylated bisphenol-A dimethacrylate; PEGDMA, poly(ethylene glycol) dimethacrylate; HEMA, 2-hydroxyethyl methacrylate.
General application protocol for direct resin restorations
| Adhesives | Application protocol |
|---|---|
| SU | 1. Apply SU to the prepared tooth and rub it for 20 sec. |
| 2. Gently air dry the adhesive for 5 sec to evaporate the solvent. | |
| 3. Light cure for 10 sec. | |
| PB | 1. Apply PB to all cavity surfaces. Avoid pooling. |
| 2. Keep PB slightly agitated for 20 sec. | |
| 3. Evaporate solvent with air for at least 5 sec. | |
| 4. Light cure for 10 sec. |
SU, Single Bond Universal; PB, Prime&Bond Universal.
Shear bond strength values (MPa)
| Application methods | Code | Adhesive | |
|---|---|---|---|
| SU | PB | ||
| 1 coat + uncuring | UC | 9.14 ± 3.94a | 6.40 ± 1.64b |
| 1 coat + curing | 1C | 10.03 ± 2.96a | 8.05 ± 1.80b |
| 3 coats + curing | 3C | 10.12 ± 3.48a | 7.67 ± 3.43b |
| 9.76 ± 3.42a | 7.37 ± 2.47b | ||
Values are presented as mean ± SD. The p < 0.05 was considered statistically significant.
SU, Single Bond Universal; PB, Prime&Bond Universal; SD, standard deviation.
Values followed by the same letter were not significantly different.
Failure mode analysis
| Adhesives | Group | Code | Type of fracture | ||
|---|---|---|---|---|---|
| A | M | C | |||
| SU | 1 coat + uncuring | UC | 2 | 5 | 6 |
| 1 coat + curing | 1C | 0 | 1 | 12 | |
| 3 coats + curing | 3C | 0 | 2 | 11 | |
| PB | 1 coat + uncuring | UC | 3 | 3 | 7 |
| 1 coat + curing | 1C | 0 | 4 | 9 | |
| 3 coats + curing | 3C | 1 | 4 | 8 | |
SU, Single Bond Universal; PB, Prime&Bond Universal; A, adhesive fracture; M, mixed fracture; C, cohesive fracture (in old composite substrate).
Thickness of adhesive layer (μm)
| Adhesives | Method of application | ||
|---|---|---|---|
| UC | 1C | 3C | |
| SU | Not measurable | 4.28 | 12.87 |
| PB | Not measurable | 2.47 | 7.30 |
SU, Single Bond Universal; PB, Prime&Bond Universal; UC, 1 coat + uncuring; 1C, 1 coat + curing; 3C, 3 coats + curing.
Table 1 Materials used in this study
SU, Single Bond Universal; PB, Prime&Bond Universal; 10-MDP, 10-methacryloyloxydecyl dihydrogen phosphate; bis-GMA, bisphenol A-glycidyl methacrylate; UDMA, urethane dimethacrylate; TEGDMA, triethylene glycol dimethacrylate; bis-EMA, ethoxylated bisphenol-A dimethacrylate; PEGDMA, poly(ethylene glycol) dimethacrylate; HEMA, 2-hydroxyethyl methacrylate.
Table 2 General application protocol for direct resin restorations
SU, Single Bond Universal; PB, Prime&Bond Universal.
Table 3 Shear bond strength values (MPa)
Values are presented as mean ± SD. The
SU, Single Bond Universal; PB, Prime&Bond Universal; SD, standard deviation.
Values followed by the same letter were not significantly different.
Table 4 Failure mode analysis
SU, Single Bond Universal; PB, Prime&Bond Universal; A, adhesive fracture; M, mixed fracture; C, cohesive fracture (in old composite substrate).
Table 5 Thickness of adhesive layer (μm)
SU, Single Bond Universal; PB, Prime&Bond Universal; UC, 1 coat + uncuring; 1C, 1 coat + curing; 3C, 3 coats + curing.

