
Articles
- Page Path
- HOME > Restor Dent Endod > Volume 49(4); 2024 > Article
- Research Article Effects of different curing methods on the color stability of composite resins
-
Massimo Pisano
 , Alfredo Iandolo, Dina Abdellatif, Andrea Chiacchio, Marzio Galdi, Stefano Martina
, Alfredo Iandolo, Dina Abdellatif, Andrea Chiacchio, Marzio Galdi, Stefano Martina -
Restor Dent Endod 2024;49(4):e33.
DOI: https://doi.org/10.5395/rde.2024.49.e33
Published online: September 5, 2024
Department of Medicine, Surgery and Dentistry ‘Scuola Medica Salernitana’, University of Salerno, Baronissi, Italy.
- Correspondence to Massimo Pisano, DDS. Department of Medicine, Surgery and Dentistry ‘Scuola Medica Salernitana’, University of Salerno, Via S. Allende, 84081 Baronissi, Italy. pisano.studio@virgilio.it
• Received: April 15, 2024 • Revised: June 5, 2024 • Accepted: June 24, 2024
Copyright © 2024. The Korean Academy of Conservative Dentistry
This is an Open Access article distributed under the terms of the Creative Commons Attribution Non-Commercial License (https://creativecommons.org/licenses/by-nc/4.0/) which permits unrestricted non-commercial use, distribution, and reproduction in any medium, provided the original work is properly cited.
Abstract
-
Objectives The aim of this study was to compare the effects of different polymerization strategies and the effectiveness of finishing and polishing procedures of composite resins on color stability.
-
Materials and Methods The samples were divided into 4 main groups according to the polymerization strategy, and all groups except the control group received surface treatment. Each group was subsequently divided into 3 subgroups respectively: Kuraray Clearfil Majesty ES-2 Classic, Premium and Universal. Approximately 24 hours after preparation of the samples, they were immersed for 7 days in a coffee solution. A first color measurement was performed after the preparation of the samples, the second measurement was performed after 7 days in the coffee solution. All measurements were carried out using a dental spectrophotometer to assess the CIE L* a* b* color parameters.
-
Results There was a statistically significant difference between ΔE values for different procedures (p = 0.003); in particular, the differences were found only between the groups that received surface treatment and the control group. In addition, a statistically significant difference was observed between the values of ΔE for different composites in the different procedure groups.
-
Conclusions Spectrophotometric analysis showed that the additional photopolymerization and oxygen inhibition procedures did not yield better results in relation to color stability. In addition, finishing and polishing provided better color stability compared to not performing these procedures.
INTRODUCTION
Composite resins are nowadays frequently used materials in everyday clinical dental practice. Thanks to the aesthetic, physical and mechanical properties that modern materials provide, they are widely used in the treatment of carious lesions, closing diastemas or camouflaging dental malpositions [1]. However, these materials need to be treated appropriately to avoid chemical degradation problems within the oral cavity, e.g. due to acid diets or extrinsic pigments, which would lead to aesthetic and functional failures of the restorative treatment [2].
It is well known that discolorations can have extrinsic causes and intrinsic causes. The former is represented by coloring substances such as coffee, tea, cola and red wine while intrinsic causes are related to the composition of the resin matrix, catalyst, mode and duration of polymerization, conversion of the monomer matrix, particle size and oxidation of the unconverted monomer [3]. The degradation of composite resins would lead the clinician to an early replacement of the restoration, which would then cause additional costs [3]. To date, despite advances in the properties of composite resins, the problem of discoloration still remains one of the most frequent causes of failure, especially in treatments in the aesthetic area. Several composite resins developed for aesthetic restorations are available on the market; these are classified according to the type, size and quantity of their filler particles, and according to the resin matrix [4].
Over time, many modifications have been applied that have made composites the materials of choice in conservative dentistry. Today, the composites can be of different types depending on the fillers included: microfilled composites, hybrid composites, nanofilled composites and universal composites [5].
Fillers play a main role in the reduction in shrinkage after polymerization and thermal expansion and play a crucial role in lowering water absorption and solubility [6]. These fillers are also important for the physical and the aesthetic properties of the composites, in addition to polishing abilities. Highly aesthetic and polished surfaces of resin composites can be achieved by minimizing the size of the filler. Improved filler qualities allow the material to withstand changes that are frequent in the oral cavity and, hence, help in the ability to withstand chewing while retaining aesthetics [7]. Another essential aspect is the adequate polymerization of composite resins to achieve optimal mechanical and optical properties. Insufficient curing processes and polymerization can lead to a decrease in the physical and mechanical properties of composite resins, which have been reported to be more susceptible to water absorption and dissolution of unreacted monomers, resulting in increased discoloration [8,9].
Composite resins in the oral cavity are continuously subjected to contact with different staining substances. Numerous studies have shown which substances, in common use, are capable of altering the qualities and in particular the color stability of composite resins [2,10,11,12,13,14]. The composition of the restoration, characteristics of the filler, oral hygiene, diet, smoking, finishing and polishing determine the surface roughness of the composite resin [15]. Surface roughness remaining from inappropriate polishing may result in excessive plaque adhesion with consequent irritation of the gingival tissues, as well as increased susceptibility of the restoration to surface pigmentation and progressive discoloration [16]. A surface roughness greater than 0.2 µm is considered a retention area for bacterial plaque, roughness is a variant that plays a key role in the aesthetic success of composite restorations [7].
Today, a wide variety of polishing protocols are available, ranging from multiple-step systems requiring the use of an orderly succession of tools, such as abrasive discs with decreasing grain size, to 1-step systems based on the use of a single medium, such as silicon carbide brushes or diamond powder-impregnated cups and tips [17]. High-quality finishing and polishing are important factors that improve both the aesthetics and longevity of composite restorations, while rough and poorly finished surfaces contribute to staining, plaque build-up, gingival irritation, recurrent caries and discoloration of the restoration over time [17,18,19]. Dental composite resin restorations should be polished to achieve as smooth a finish as possible to increase stain resistance [20].
Therefore, the aim of this study was to compare the effects of different polymerization strategies and the effectiveness of finishing and polishing procedures of composite resins on color stability using 3 different composites. The null hypothesis of the study is that polymerization and the surface treatment techniques guarantee the same results in terms of color stability.
MATERIALS AND METHODS
Three composites were tested:
• Clearfil Majesty ES-2 Universal (Kuraray Co. Ltd., Tokyo, Japan)
• Clearfil Majesty ES-2 Classic (Kuraray Co. Ltd.)
• Clearfil Majesty ES-2 Premium Dentin (Kuraray Co. Ltd.)
The total amount of filler is approximately 78 wt%, including inorganic filler of 40 vol%. The particle size of inorganic fillers ranges from 0.37 to 1.5 µm.
Cylindrical plexiglass molds with dimensions of 8 × 2 mm were used to test the composites. A total of 120 samples were produced. The composite was placed inside the molds using a stainless-steel instrument (Didier Dietschi CompoSculp; Hu-Friedy, Milano, Italy).
After the material was placed in the mold, a polyester strip was pressed onto the surface with a glass plate to obtain a flat surface.
The samples were divided into the following groups:
• Control group (Group C): A single light-cure was performed, and the composite resins were light-cured for 20 seconds.
• Single application of curing light + Polishing (Group 1): A single 20-second light curing and subsequent polishing was performed.
• Application of curing light + Polishing + Additional application of curing light (Group 2): After the first 20 seconds of photoactivation and subsequent polishing maneuvers, an additional 20 seconds of photo polishing was carried out.
• Glycerin + Single application of curing light + Polishing (Group 3): Before light-curing the samples for 20 seconds, the surface was sprinkled with glycerin (Liquid Strip - Glycerin Gel; Ivoclar Vivadent, Amherst, NY, USA) followed by polishing.
Photoactivation was carried out for 20 seconds with an LED lamp (VALO, Ultradent Italia Srl, Corsico, Italy) with a light intensity of 1,000 mW/cm2, perpendicularly and directly on top of the samples.
With the exception of the control group, the other groups were treated with polishing procedures, performed with the aid of an extra-fine diamond bur for 10 seconds to avoid the formation of micro-cracks followed by the use of a silicone rubber polisher and a polishing brush (Occlubrash Golden; Kerr Dental Italia, Scafati, Italy) for 10 seconds [13]. After the procedures, the specimens were washed with 70% alcohol with gauze to remove the glycerin (Group 3) and post-polishing compounds. The polishing and light curing procedures were carried out on the same side of the specimens. The same operator carried out the specimen preparation, finishing, and polishing procedures. The same clean protocol was used for the control group.
The sample was divided into 3 sub-groups for each group: Kuraray Majesty Classic, Kuraray Premium Dentin, and Kuraray Universal. Specifically, 2 types of nanohybrid composites (Kuraray ES-2 Classic and Kuraray ES-2 Premium) and a Universal composite were used. The division into groups and subgroups is shown in Table 1.
Table 1
Division of the sample into groups and sub-groups (n = 120)
*The samples were divided into the following groups: Group C, A single light-cure was performed, and the composite resins were light-cured for 20 seconds; Group 1, 20 seconds Photopolymerization + Polishing; Group 2, 20 seconds Photopolymerization + Polishing + 20 seconds Photopolymerization; and Group 3, Glycerin + 20 seconds Photopolymerization + Polishing.
Approximately 24 hours after the preparation of the samples, they were immersed for 7 days in a coffee solution (Caffè Motta Spa, Salerno, Italy) at a constant temperature of 37°C, the concentration used was 150 mg of caffeine in 100 mL of solution. The solution was changed daily. After the 7 days in the solution, the samples were rinsed for 2 minutes with distilled water and then dried.
A first color measurement was performed after the preparation of the samples, the measurement was carried out with the aid of a dental spectrophotometer (SpectroShade Micro, MHT S.P.A., Milan, Italy) (Figure 1), the second measurement was performed after 7 days in the coffee solution and after washing and drying the samples. The spectrophotometer was used to measure the CIE L* a* b* color parameters. The initial color of each sample was measured before immersion in the solutions. In the CIE L* a* b* color space, the brightness is indicated by L*, red-green by a*, and blue-yellow by b*) [21]. The device was calibrated before measurement, and the measurements were made 3 times for each sample. The mean values were considered the final value. Color difference (ΔE) was calculated using the following formula:
Figure 1
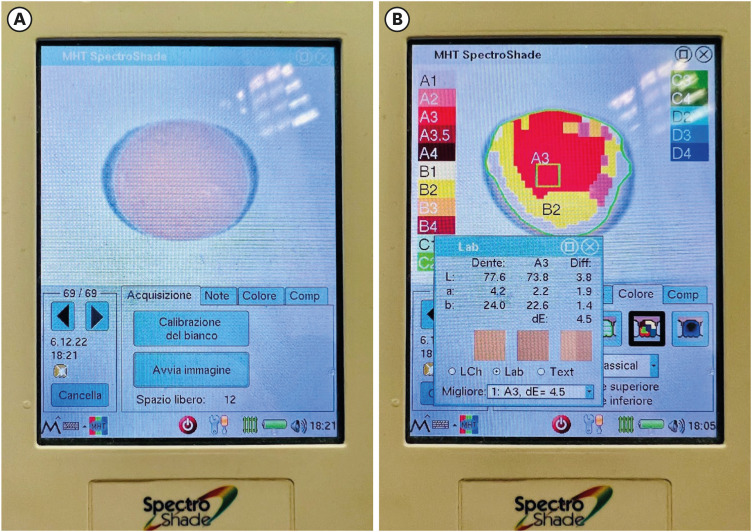
Procedure for using spectrophotometer on composite samples. A sample before (A) and during (B) the spectrophotometer measurement, the spectrophotometer was used to measure the CIE L* a* b* color parameters.
where:
• ΔE is a parameter used to evaluate the discoloration; therefore, it follows that the higher its value, the greater the degree of difference between the final and initial color of the sample examined.
• Δa is the difference between the red-green shades of the sample after and before coffee immersion.
• Δb is the difference between the blue-yellow shades of the sample after and before coffee immersion.
• ΔL is the difference between the brightness of the sample after and before coffee immersion.
A standard statistical software (Jamovi software, version 2.3.26; www.jamovi.org) was used to evaluate the data and the p value was set at 0.05. The means and standard deviations of each group were calculated. A Shapiro-Wilk test was used to assess if the sample was normally distributed. A 2-way analysis of variance (ANOVA) test was performed to compare groups and a post-hoc analysis (Tukey test) was used to perform dual comparisons between groups (p < 0.05).
RESULTS
A total of 120 samples were divided according to different groups (30 samples for each procedure) and into different sub-groups (10 samples for each composite), as shown in Table 1. Based on the Shapiro-Wilk test, ΔE was normally distributed in the general sample and in the different groups and sub-groups. The mean and standard deviations of ΔE were 5.5 ± 2.6; the statistical parameters for the groups and sub-groups are shown in Table 2. Based on the division of the groups, the lowest value of discoloration was observed in the subgroup “20 seconds Photopolymerization + Polishing” (ΔE: 4.3 ± 2.5) while the highest ΔE value was found in the control group (ΔE: 8.0 ± 2.8). By sub-groups division, the highest discoloration value was found in the Kuraray Universal composite (ΔE: 7.5 ± 2.5), while the lowest ΔE value was measured in the Kuraray Classic composite (ΔE: 3.3 ± 1.0).
Table 2
ΔE according to different procedure groups, and composite sub-groups
| Groups | ΔE | |
|---|---|---|
| Composites groups | ||
| Kuraray Universal | 7.5 ± 2.5 | |
| Kuraray Classic | 3.3 ± 1.0 | |
| Kuraray Premium | 5.6 ± 2.3 | |
| Procedures groups* | ||
| Group C | 8.0 ± 2.8 | |
| Group 1 | 4.3 ± 2.5 | |
| Group 2 | 4.8 ± 1.7 | |
| Group 3 | 4.8 ± 1.9 | |
Values are presented as mean ± standard deviation.
*The samples were divided into the following groups: Group C, A single light-cure was performed, and the composite resins were light-cured for 20 seconds; Group 1, 20 seconds Photopolymerization + Polishing; Group 2, 20 seconds Photopolymerization + Polishing + 20 seconds Photopolymerization; and Group 3, Glycerin + 20 seconds Photopolymerization + Polishing.
As a result of the ANOVA test, a statistically significant difference was found between ΔE values for different composites in the several procedure groups, as shown in Table 3. In particular, the p value of the comparison of ΔE values between the 3 different composite sub-groups in Group C was < 0.001, the same for Groups 2 and 3; while for Group 1, the p value of the comparison between the composite sub-groups was 0.011.
Table 3
ΔE according to different groups and sub-groups
The p value column is related to comparisons made between different composites subjected to the same procedure. Values are presented as mean ± standard deviation.
*The samples were divided into the following groups: Group C, A single light-cure was performed, and the composite resins were light-cured for 20 seconds; Group 1, 20 seconds Photopolymerization + Polishing; Group 2, 20 seconds Photopolymerization + Polishing + 20 seconds Photopolymerization; and Group 3, Glycerin + 20 seconds Photopolymerization + Polishing.
Depending on the division into groups and sub-groups, the highest discoloration value was found in the control group of Kuraray Universal (ΔE: 10.4 ± 1.5), while the lowest value of discoloration was seen in the Group 1 of Kuraray Premium (ΔE: 2.2 ± 0.8).
According to the ANOVA test, there was a statistically significant difference between ΔE values within the several groups divided according to the procedures (p = 0.003); Notably, with the post-hoc analysis, a statistically significant difference was found between Groups 1, 2, 3 and C (p = 0.004, p = 0.006 and p = 0.008, respectively), as shown in Table 4 and Figure 2.
Table 4
Comparison between the different procedures and the control group as a result of post-hoc analysis with Tukey test
| Comparison between groups* | p value | |
|---|---|---|
| Group 1 | Group C | 0.004 |
| Group 1 | Group 2 | 0.909 |
| Group 1 | Group 3 | 0.933 |
| Group 2 | Group C | 0.006 |
| Group 2 | Group 3 | 1.000 |
| Group 3 | Group C | 0.008 |
*The samples were divided into the following groups: Group C, A single light-cure was performed, and the composite resins were light-cured for 20 seconds; Group 1, 20 seconds Photopolymerization + Polishing; Group 2, 20 seconds Photopolymerization + Polishing + 20 seconds Photopolymerization; and Group 3, Glycerin + 20 seconds Photopolymerization + Polishing.
Figure 2
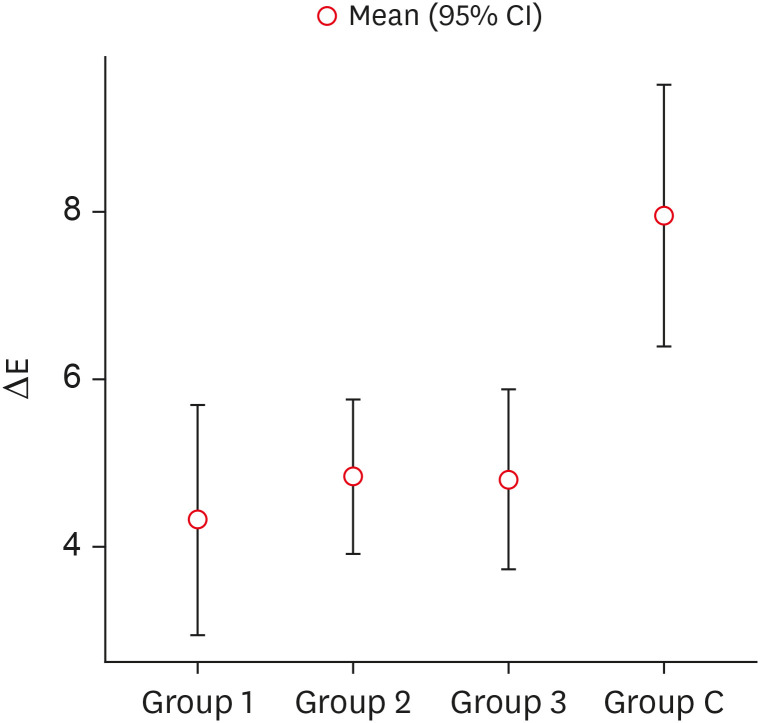
Comparison between the distribution of ΔE values in different procedure groups (Group 1: 20 seconds Photopolymerization + Polishing; Group 2: 20 seconds Photopolymerization + Polishing + 20 seconds Photopolymerization; Group 3: Glycerin + 20 seconds Photopolymerization + Polishing) and control group (Group C).
CI, confidence interval.
DISCUSSION
The aim of this study was to evaluate the color stability of composite resins immersed in a pigmenting substance such as coffee by comparing different composite curing approaches. Several factors can influence the discoloration process of composite resin materials by these substances, including incomplete polymerization, water absorption, food and drink staining, oral hygiene, tobacco smoking and surface roughness [22,23,24,25,26].
The color stability of materials can be measured objectively with instrumental methods such as the spectrophotometer [27]. To assess the color change, the CIE L* a* b* coordinate system was often used [28]. Several studies have reported that this system has advantages such as accuracy, repeatability, sensitivity and objectivity [29,30]. In the current study, all light curing techniques used in the different samples showed a color change after immersion in coffee. The color change (ΔE) was greater in the non-polished group (control group), mainly due to the rougher surface that contributed to the stain formation as reported in previous studies in the literature [2,20,31,32,33,34].
Finishing and polishing in restorative dentistry refers to the following steps: coarse contouring of the restoration to achieve the desired anatomy, reduction and smoothing of surface roughness and scratches created by the finishing instruments during the process of coarse reduction and initial polishing and finally a process that aims to produce a highly smooth surface that is able to reflect light, similar to enamel and is referred to as final polishing [35]. Various surface finishing and polishing treatments can affect stain resistance by altering the surface roughness of resins. In our study, the samples were finished using an extra-fine diamond burn for 10 seconds to avoid the formation of micro-cracks followed by the use of a silicone polisher and a polishing brush for 10 seconds [36]. All polishing groups showed less discoloration than the control group, in agreement with the results of the studies by Gönülol and Yilmaz [19], Barakah and Taher [20], and Gonulol and Patel et al. [33]. Discoloration of restorations could be removed by re-polishing, depending on the material and severity of the discoloration [35]. Re-polishing is a minimally invasive operative procedure that can remove extrinsic discoloration on restoration surfaces [28,37]. Ugurlu’s study [38] showed that although there was a clear improvement in discoloration after re-polishing, the nanohybrid and microhybrid composite resins used in the study still showed a significant ΔE after the procedure; this is because internal discoloration may not be completely removed by re-polishing.
Regarding the materials, the composites used in the present study were Kuraray Clearfil Majesty ES-2 Classic, a composite resin that contains a proprietary nano-filled filler and a high refractive matrix. It exhibits a light-diffusion property very similar to the natural tooth structure, this type of material is characterized by an intermediate translucency and a moderate opacity, which also makes it eligible for restorations in the aesthetic area. Another composite used was Kuraray Clearfil Majesty ES-2 Premium Dentin, a nano-filled material with a level of opacity that guarantees a certain degree of coverage, making it suitable for a technique involving layering of different masses in the aesthetic area. The third composite used was Kuraray Clearfil Majesty ES-2 Universal. This type of composite presented as ‘universal’ can be used without additional shades. Most of them follow the trend towards simplification with fewer shades and translucency as a result of some kind of chameleon effect [39]. These composite resins represent a simplified type of material with a regular viscosity consistency for which the layering technique is not necessary, due to the refractive and reflective properties that make the restorations diffuse light in a similar way to the tooth structure [39,40,41].
The polymerization process of composite resins plays an important role in color alterations and their optical properties. Residual unconverted methacrylate groups could cause increased water absorption of the resin matrix and color alterations. The degree of conversion depends on factors such as the composition of the resin material, type of photoinitiator, type and power density of the light-curing unit, inclination of the light rays with respect to the surface, intensity, and curing time [42]. The resin material contains the photo activator camphorquinone, which is activated at wavelengths of 420 to 470 nm. When these conditions are not met, polymerization is inhibited at various levels, leading to defects in the physical and chemical properties of the material [43,44]. According to the study by Hervás-García et al. [5] for optimal polymerization of composite resins, the thickness should be 1–2 mm, at room temperature, with a minimum distance of less than 1 mm and at an angle of 90° to the surface of the material. Previous studies report that the minimum light intensity required for adequate polymerization of 2 mm composite resin was approximately 400 mW/cm2 with an exposure time of 40 seconds [43,45]. In our study, photoactivation was performed for 20 seconds with LED light with a light intensity of 1,000 mW/cm2 perpendicularly and directly on top of the samples. In Group 3, an additional photo-activation was performed after the samples had been finished and polished, and in Group 4, a photo-activation was performed after the samples had been coated with glycerin. In our study, additive polymerization showed a statistically significant ΔE compared to the control group but showed no statistically significant differences compared to the other groups. On the contrary, Unsal and Karaman [44] showed how applying additive polymerization/additional light cure could improve the physical-mechanical properties of the materials while also reporting less color variation of the resins over time. In particular, by applying the additional polymerization, a statistically significant ΔE was reported in all tested samples compared to the group in which the procedure had not been applied, thus showing less discoloration in the samples treated with additional polymerization [44].
Furthermore, during the light-curing of composite resins, contact with oxygen produces a surface layer of uncured resin. Oxygen inhibits the polymerization reaction because its reactivity with free radicals is greater than that of the composite resin monomers, resulting in the formation of a polymer chain more prone to discoloration and wear [46,47]. Several authors have reported how oxygen inhibition, via substances such as glycerin gel, improves the degree of surface conversion of composite resins. In this study, it was decided to use glycerine before polymerization to prevent the formation of the oxidative inhibition layer [48].
The study by Borges et al. [49] showed that the use of glycerin alone did not improve the color stability of composite resins, but when combined with finishing and polishing techniques, it could significantly decrease the color variation of composite resins.
In our study, the use of glycerin showed a statistically significant difference compared to the control group but comparable to the other groups in which glycerin was not applied.
Further studies, in particular clinical studies with medium- and long-term follow-up, are needed to assess whether these polymerization techniques are able to achieve a real advantage compared with the other ones.
It should be noted that the present study has some limitations related to the design of the experimental study. There are extremely heterogeneous aspects between the various methodologies concerning: the effect of different curing times, different types of light sources, the degree of conversion of the composite resins or the heterogeneity of the different polishing protocols available, the lack of other tests, e.g. roughness or degree of conversion. In future studies, it will be necessary to include these aspects to verify and confirm the results of this study.
CONCLUSION
The different composite curing approaches investigated showed no statistically significant differences in color stability. On the other hand, the surface treatment of composite resins through finishing and polishing procedures provided better results in relation to color stability. Considering these findings, it could be concluded that finishing and polishing should be performed after restorative procedures to maintain the aesthetic properties by ensuring greater color stability and discoloration of composite resins regardless of light curing techniques.
-
Conflict of Interest: No potential conflict of interest relevant to this article was reported.
-
Author Contributions:
Conceptualization: Pisano M.
Data curation: Chiacchio A, Pisano M.
Formal analysis: Galdi M.
Investigation: Iandolo A, Martina S.
Methodology: Adbellatif D, Galdi M.
Project administration: Chiacchio A, Pisano M.
Software: Galdi M, Chiacchio A.
Supervision: Martina S.
Validation: Pisano M.
Visualization: Iandolo A.
Writing - original draft: Iandolo A, Pisano M,.
Writing - review & editing: Abdellatif D, Martina S.
- 1. Mante FK, Ozer F, Walter R, Atlas AM, Saleh N, Dietschi D, et al. The current state of adhesive dentistry: a guide for clinical practice. Compend Contin Educ Dent 2013;34 Spec 9:2-8.PubMed
- 2. Bagheri R, Burrow MF, Tyas M. Influence of food-simulating solutions and surface finish on susceptibility to staining of aesthetic restorative materials. J Dent 2005;33:389-398.ArticlePubMed
- 3. Bollen CM, Lambrechts P, Quirynen M. Comparison of surface roughness of oral hard materials to the threshold surface roughness for bacterial plaque retention: a review of the literature. Dent Mater 1997;13:258-269.ArticlePubMed
- 4. Sampath S. Survival times of restorative parameters vis-à-vis material combinations. J Res Dent 2015;3:14-20.Article
- 5. Hervás-García A, Martínez-Lozano MA, Cabanes-Vila J, Barjau-Escribano A, Fos-Galve P. Composite resins. A review of the materials and clinical indications. Med Oral Patol Oral Cir Bucal 2006;11:E215-E220.PubMed
- 6. Manhart J, Kunzelmann KH, Chen HY, Hickel R. Mechanical properties of new composite restorative materials. J Biomed Mater Res 2000;53:353-361.ArticlePubMed
- 7. dos Santos Bertoldo CE, Miranda DA, Souza-Junior EJ, Aguiar FHB, Lima DANL, Lovadino JR. Evaluation of surface roughness and color stability of direct resin composites after different polishing protocols. Int J Dent Clin 2011;3:4-7.
- 8. Zhu S, Platt JA. Curing efficiency of three different curing lights at different distances for a hybrid composite. Am J Dent 2009;22:381-386.PubMed
- 9. Price RBT. Light curing in dentistry. Dent Clin North Am 2017;61:751-778.ArticlePubMed
- 10. Guler AU, Yilmaz F, Kulunk T, Guler E, Kurt S. Effects of different drinks on stainability of resin composite provisional restorative materials. J Prosthet Dent 2005;94:118-124.ArticlePubMed
- 11. Sarembe S, Kiesow A, Pratten J, Webster C. The impact on dental staining caused by beverages in combination with chlorhexidine digluconate. Eur J Dent 2022;16:911-918.ArticlePubMedPMC
- 12. Kumari RV, Nagaraj H, Siddaraju K, Poluri RK. evaluation of the effect of surface polishing, oral beverages and food colorants on color stability and surface roughness of nanocomposite resins. J Int Oral Health 2015;7:63-70.
- 13. Tekçe N, Tuncer S, Demirci M, Serim ME, Baydemir C. The effect of different drinks on the color stability of different restorative materials after one month. Restor Dent Endod 2015;40:255-261.ArticlePubMedPMC
- 14. Villalta P, Lu H, Okte Z, Garcia-Godoy F, Powers JM. Effects of staining and bleaching on color change of dental composite resins. J Prosthet Dent 2006;95:137-142.ArticlePubMed
- 15. Kocaagaoglu H, Aslan T, Gürbulak A, Albayrak H, Taşdemir Z, Gumus H. Efficacy of polishing kits on the surface roughness and color stability of different composite resins. Niger J Clin Pract 2017;20:557-565.ArticlePubMed
- 16. Attar N. The effect of finishing and polishing procedures on the surface roughness of composite resin materials. J Contemp Dent Pract 2007;8:27-35.Article
- 17. Reis AF, Giannini M, Lovadino JR, Ambrosano GM. Effects of various finishing systems on the surface roughness and staining susceptibility of packable composite resins. Dent Mater 2003;19:12-18.ArticlePubMed
- 18. Başeren M. Surface roughness of nanofill and nanohybrid composite resin and ormocer-based tooth-colored restorative materials after several finishing and polishing procedures. J Biomater Appl 2004;19:121-134.ArticlePubMedPDF
- 19. Gönülol N, Yilmaz F. The effects of finishing and polishing techniques on surface roughness and color stability of nanocomposites. J Dent 2012;40(Supplement 2):e64-e70.Article
- 20. Barakah HM, Taher NM. Effect of polishing systems on stain susceptibility and surface roughness of nanocomposite resin material. J Prosthet Dent 2014;112:625-631.ArticlePubMed
- 21. International Commission on Illumination (CIE). CIE 142-2001. Improvement to industrial colour-difference evaluation. Vienna: CIE; 2001.
- 22. Asmussen E, Hansen EK. Surface discoloration of restorative resins in relation to surface softening and oral hygiene. Scand J Dent Res 1986;94:174-177.ArticlePubMed
- 23. Ferracane JL, Moser JB, Greener EH. Ultraviolet light-induced yellowing of dental restorative resins. J Prosthet Dent 1985;54:483-487.ArticlePubMed
- 24. Satou N, Khan AM, Matsumae I, Satou J, Shintani H. In vitro color change of composite-based resins. Dent Mater 1989;5:384-387.PubMed
- 25. Um CM, Ruyter IE. Staining of resin-based veneering materials with coffee and tea. Quintessence Int 1991;22:377-386.PubMed
- 26. D’Ambrosio F, Pisano M, Amato A, Iandolo A, Caggiano M, Martina S. Periodontal and peri-implant health status in traditional vs. heat-not-burn tobacco and electronic cigarettes smokers: a systematic review. Dent J 2022;10:103.ArticlePubMedPMC
- 27. Liberato WF, Barreto IC, Costa PP, de Almeida CC, Pimentel W, Tiossi R. A comparison between visual, intraoral scanner, and spectrophotometer shade matching: a clinical study. J Prosthet Dent 2019;121:271-275.ArticlePubMed
- 28. Saegusa M, Kurokawa H, Takahashi N, Takamizawa T, Ishii R, Shiratsuchi K, et al. Evaluation of color-matching ability of a structural colored resin composite. Oper Dent 2021;46:306-315.ArticlePubMedPDF
- 29. Mundim FM, Garcia LF, Pires-de-Souza FC. Effect of staining solutions and repolishing on color stability of direct composites. J Appl Oral Sci 2010;18:249-254.ArticlePubMedPMC
- 30. Alharbi A, Ardu S, Bortolotto T, Krejci I. Stain susceptibility of composite and ceramic CAD/CAM blocks versus direct resin composites with different resinous matrices. Odontology 2017;105:162-169.ArticlePubMedPDF
- 31. Ardu S, Duc O, Di Bella E, Krejci I, Daher R. Color stability of different composite resins after polishing. Odontology 2018;106:328-333.ArticlePubMedPDF
- 32. Alshehri A, Alhalabi F, Mustafa M, Awad MM, Alqhtani M, Almutairi M, et al. effects of accelerated aging on color stability and surface roughness of a biomimetic composite: an in vitro study. Biomimetics (Basel) 2022;7:158.PubMedPMC
- 33. Patel SB, Gordan VV, Barrett AA, Shen C. The effect of surface finishing and storage solutions on the color stability of resin-based composites. J Am Dent Assoc 2004;135:587-594.ArticlePubMed
- 34. Gaviria-Martinez A, Castro-Ramirez L, Ladera-Castañeda M, Cervantes-Ganoza L, Cachay-Criado H, Alvino-Vales M, et al. Surface roughness and oxygen inhibited layer control in bulk-fill and conventional nanohybrid resin composites with and without polishing: in vitro study. BMC Oral Health 2022;22:258.PubMedPMC
- 35. Seyidaliyeva A, Rues S, Evagorou Z, Hassel AJ, Rammelsberg P, Zenthöfer A. Color stability of polymer-infiltrated-ceramics compared with lithium disilicate ceramics and composite. J Esthet Restor Dent 2020;32:43-50.ArticlePubMedPDF
- 36. Marghalani HY. Effect of filler particles on surface roughness of experimental composite series. J Appl Oral Sci 2010;18:59-67.ArticlePubMedPMC
- 37. Mailart MC, Rocha RS, Contreras SCM, Torres CRG, Borges AB, Caneppele TMF. Effects of artificial staining on bulk-filled resin composites. Am J Dent 2018;31:144-148.PubMed
- 38. Ugurlu M. Effect of repolishing on the discoloration of indirect composite block, nanohybrid, and microhybrid resin composites. Eur Oral Res 2022;56:158-163.ArticlePubMedPMC
- 39. de Abreu JLB, Sampaio CS, Benalcázar Jalkh EB, Hirata R. Analysis of the color matching of universal resin composites in anterior restorations. J Esthet Restor Dent 2021;33:269-276.ArticlePubMedPDF
- 40. Silva MVMD, Batista JMN, Fraga MAA, Correr AB, Campos EA, Geraldeli S, et al. Surface analysis of a universal resin composite and effect of preheating on its physicochemical properties. Braz Dent J 2023;34:115-126.ArticlePubMedPMC
- 41. Hardan L, Bourgi R, Cuevas-Suárez CE, Lukomska-Szymanska M, Monjarás-Ávila AJ, Zarow M, et al. Novel trends in dental color match using different shade selection methods: a systematic review and meta-analysis. Materials (Basel) 2022;15:468.ArticlePubMedPMC
- 42. Sideridou I, Tserki V, Papanastasiou G. Effect of chemical structure on degree of conversion in light-cured dimethacrylate-based dental resins. Biomaterials 2002;23:1819-1829.ArticlePubMed
- 43. Rueggeberg FA, Caughman WF, Curtis JW Jr. Effect of light intensity and exposure duration on cure of resin composite. Oper Dent 1994;19:26-32.PubMed
- 44. Unsal KA, Karaman E. Effect of additional light curing on colour stability of composite resins. Int Dent J 2022;72:346-352.ArticlePubMed
- 45. Alkhudhairy F. Wear resistance of bulk-fill composite resin restorative materials polymerized under different curing intensities. J Contemp Dent Pract 2017;18:39-43.ArticlePubMed
- 46. Panchal AC, Asthana G. Oxygen inhibition layer: a dilemma to be solved. J Conserv Dent 2020;23:254-258.ArticlePubMedPMC
- 47. Rodrigues-Junior SA, Chemin P, Piaia PP, Ferracane JL. surface roughness and gloss of actual composites as polished with different polishing systems. Oper Dent 2015;40:418-429.ArticlePubMedPDF
- 48. Park HH, Lee IB. Effect of glycerin on the surface hardness of composites after curing. J Korean Acad Conserv Dent 2011;36:483-439.Article
- 49. Borges MG, Silva GR, Neves FT, Soares CJ, Faria-E-Silva AL, Carvalho RF, et al. Oxygen inhibition of surface composites and its correlation with degree of conversion and color stability. Braz Dent J 2021;32:91-97.ArticlePubMed
REFERENCES
Tables & Figures
REFERENCES
Citations
Citations to this article as recorded by 
- Color Stability Under Challenge: Effects of Thermo-Aging and Mouthrinse Exposure on Anterior Teeth and Esthetic Composites
Gökçe Keçeci, Zehra Güner, Süleyman Ziya Şenyurt, Kamile Erciyas
European Journal of Therapeutics.2026; 32(1): 94. CrossRef - Color stability and degree of conversion of conventional, amine-free, and self-adhesive resin cements polymerized under different conditions
Su Young Lee, Yasushi Shimada, Jaeyoung Edwin Han, Seung-Hoon Han
Dental Materials.2026;[Epub] CrossRef - Abrasiveness and Bleaching Level of Toothpastes on Composite Resins: A Quantitative Analysis Using a Novel Brushing Simulator
Simge Meseli, Elif Alkan, Bora Korkut, Ozlem Kanar, Dilek Tagtekin
Applied Sciences.2025; 15(5): 2314. CrossRef - Comparative Evaluation of Direct and Indirect Composite Restorations in Class II Tooth Preparations - An In vivo Study
Akshun Gupta, Garima Arora, Aprajita Mehta, Satish Sane, Siddhi Nevrekar, Apurva Nagrale
Advances in Human Biology.2025; 15(4): 550. CrossRef - Micro- and Nanoplastics and the Oral Cavity: Implications for Oral and Systemic Health, Dental Practice, and the Environment—A Narrative Review
Federica Di Spirito, Veronica Folliero, Maria Pia Di Palo, Giuseppina De Benedetto, Leonardo Aulisio, Stefano Martina, Luca Rinaldi, Gianluigi Franci
Journal of Functional Biomaterials.2025; 16(9): 332. CrossRef
 ePub Link
ePub Link Cite
CiteEffects of different curing methods on the color stability of composite resins
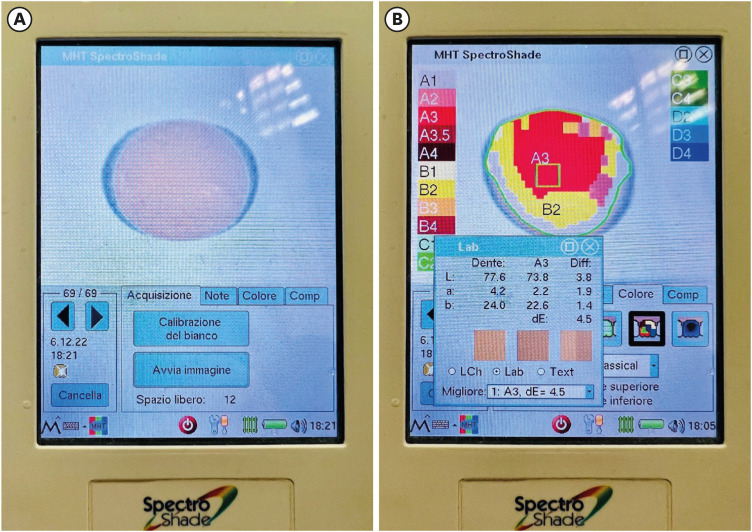
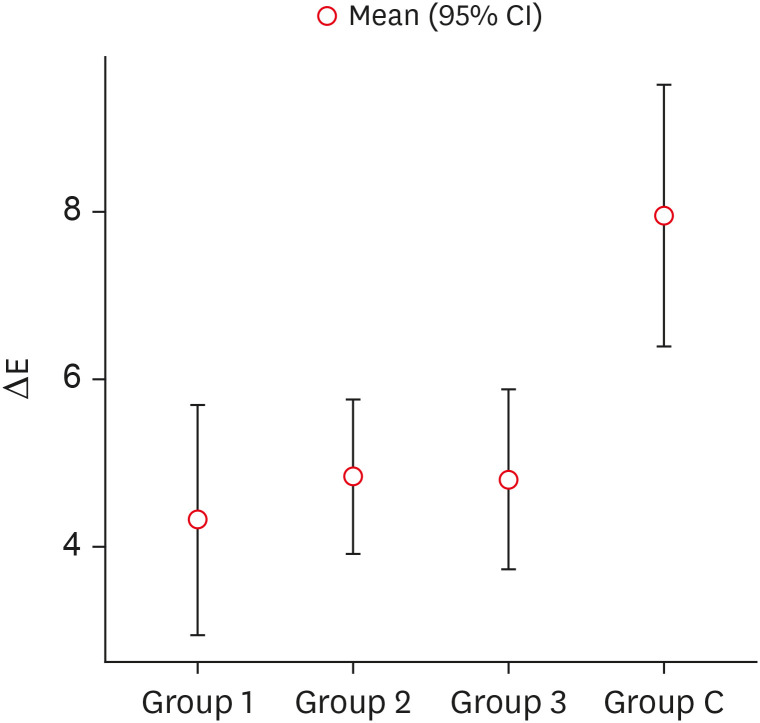
Figure 1 Procedure for using spectrophotometer on composite samples. A sample before (A) and during (B) the spectrophotometer measurement, the spectrophotometer was used to measure the CIE L* a* b* color parameters.
Figure 2 Comparison between the distribution of ΔE values in different procedure groups (Group 1: 20 seconds Photopolymerization + Polishing; Group 2: 20 seconds Photopolymerization + Polishing + 20 seconds Photopolymerization; Group 3: Glycerin + 20 seconds Photopolymerization + Polishing) and control group (Group C).CI, confidence interval.
Figure 1
Figure 2
Effects of different curing methods on the color stability of composite resins
Division of the sample into groups and sub-groups (n = 120)
| Composites groups | Procedures groups* | |||
|---|---|---|---|---|
| Group C | Group 1 | Group 2 | Group 3 | |
| Kuraray Universal | ||||
| Kuraray Classic | ||||
| Kuraray Premium | ||||
*The samples were divided into the following groups: Group C, A single light-cure was performed, and the composite resins were light-cured for 20 seconds; Group 1, 20 seconds Photopolymerization + Polishing; Group 2, 20 seconds Photopolymerization + Polishing + 20 seconds Photopolymerization; and Group 3, Glycerin + 20 seconds Photopolymerization + Polishing.
ΔE according to different procedure groups, and composite sub-groups
| Groups | ΔE | |
|---|---|---|
| Composites groups | ||
| Kuraray Universal | 7.5 ± 2.5 | |
| Kuraray Classic | 3.3 ± 1.0 | |
| Kuraray Premium | 5.6 ± 2.3 | |
| Procedures groups* | ||
| Group C | 8.0 ± 2.8 | |
| Group 1 | 4.3 ± 2.5 | |
| Group 2 | 4.8 ± 1.7 | |
| Group 3 | 4.8 ± 1.9 | |
Values are presented as mean ± standard deviation.
*The samples were divided into the following groups: Group C, A single light-cure was performed, and the composite resins were light-cured for 20 seconds; Group 1, 20 seconds Photopolymerization + Polishing; Group 2, 20 seconds Photopolymerization + Polishing + 20 seconds Photopolymerization; and Group 3, Glycerin + 20 seconds Photopolymerization + Polishing.
ΔE according to different groups and sub-groups
| Procedures* | Composite | ΔE | |
|---|---|---|---|
| Group C | Kuraray Universal | 10.4 ± 1.5 | < 0.001 |
| Kuraray Classic | 9.0 ± 0.6 | ||
| Kuraray Premium | 4.4 ± 0.8 | ||
| Group 1 | Kuraray Universal | 6.5 ± 2.7 | 0.011 |
| Kuraray Classic | 4.2 ± 1.4 | ||
| Kuraray Premium | 2.2 ± 0.8 | ||
| Group 2 | Kuraray Universal | 6.2 ± 1.3 | < 0.001 |
| Kuraray Classic | 5.3 ± 1.0 | ||
| Kuraray Premium | 3.0 ± 0.5 | ||
| Group 3 | Kuraray Universal | 7.0 ± 1.8 | < 0.001 |
| Kuraray Classic | 3.7 ± 0.8 | ||
| Kuraray Premium | 3.7 ± 0.5 |
The
*The samples were divided into the following groups: Group C, A single light-cure was performed, and the composite resins were light-cured for 20 seconds; Group 1, 20 seconds Photopolymerization + Polishing; Group 2, 20 seconds Photopolymerization + Polishing + 20 seconds Photopolymerization; and Group 3, Glycerin + 20 seconds Photopolymerization + Polishing.
Comparison between the different procedures and the control group as a result of post-hoc analysis with Tukey test
| Comparison between groups* | ||
|---|---|---|
| Group 1 | Group C | 0.004 |
| Group 1 | Group 2 | 0.909 |
| Group 1 | Group 3 | 0.933 |
| Group 2 | Group C | 0.006 |
| Group 2 | Group 3 | 1.000 |
| Group 3 | Group C | 0.008 |
*The samples were divided into the following groups: Group C, A single light-cure was performed, and the composite resins were light-cured for 20 seconds; Group 1, 20 seconds Photopolymerization + Polishing; Group 2, 20 seconds Photopolymerization + Polishing + 20 seconds Photopolymerization; and Group 3, Glycerin + 20 seconds Photopolymerization + Polishing.
Table 1 Division of the sample into groups and sub-groups (n = 120)
*The samples were divided into the following groups: Group C, A single light-cure was performed, and the composite resins were light-cured for 20 seconds; Group 1, 20 seconds Photopolymerization + Polishing; Group 2, 20 seconds Photopolymerization + Polishing + 20 seconds Photopolymerization; and Group 3, Glycerin + 20 seconds Photopolymerization + Polishing.
Table 2 ΔE according to different procedure groups, and composite sub-groups
Values are presented as mean ± standard deviation.
*The samples were divided into the following groups: Group C, A single light-cure was performed, and the composite resins were light-cured for 20 seconds; Group 1, 20 seconds Photopolymerization + Polishing; Group 2, 20 seconds Photopolymerization + Polishing + 20 seconds Photopolymerization; and Group 3, Glycerin + 20 seconds Photopolymerization + Polishing.
Table 3 ΔE according to different groups and sub-groups
The
*The samples were divided into the following groups: Group C, A single light-cure was performed, and the composite resins were light-cured for 20 seconds; Group 1, 20 seconds Photopolymerization + Polishing; Group 2, 20 seconds Photopolymerization + Polishing + 20 seconds Photopolymerization; and Group 3, Glycerin + 20 seconds Photopolymerization + Polishing.
Table 4 Comparison between the different procedures and the control group as a result of post-hoc analysis with Tukey test
*The samples were divided into the following groups: Group C, A single light-cure was performed, and the composite resins were light-cured for 20 seconds; Group 1, 20 seconds Photopolymerization + Polishing; Group 2, 20 seconds Photopolymerization + Polishing + 20 seconds Photopolymerization; and Group 3, Glycerin + 20 seconds Photopolymerization + Polishing.

