
Articles
- Page Path
- HOME > Restor Dent Endod > Volume 46(3); 2021 > Article
- Research Article Postoperative pain after endodontic treatment of necrotic teeth with large intentional foraminal enlargement
-
Ricardo Machado1
 , Daniel Comparin2, Sérgio Aparecido Ignácio3, Ulisses Xavier da Silva Neto3
, Daniel Comparin2, Sérgio Aparecido Ignácio3, Ulisses Xavier da Silva Neto3 -
Restor Dent Endod 2021;46(3):e31.
DOI: https://doi.org/10.5395/rde.2021.46.e31
Published online: May 31, 2021
1Department of Endodontics, School of Health and Bioscience, Pontifical Catholic University of Paraná – PUC/PR, Curitiba, Paraná, Brazil.
2Department of Endodontics, School of Dentistry, Paranaense University – UNIPAR, Francisco Beltrão, Paraná, Brazil.
3Department of Statistics, School of Health and Bioscience, Pontifical Catholic University of Paraná – PUC/PR, Curitiba, Paraná, Brazil.
- Correspondence to Ricardo Machado, DDS, MSc, PhD. Post-Doctorate Student, Department of Endodontics, School of Health and Bioscience, Pontifical Catholic University of Paraná, – PUC/PR, Rua Imaculada Conceição, 1155, Prado Velho, 80.215-901, Curitiba, Paraná, Brazil. ricardo.machado.endo@gmail.com
• Received: July 13, 2020 • Revised: December 17, 2020 • Accepted: December 31, 2020
Copyright © 2021. The Korean Academy of Conservative Dentistry
This is an Open Access article distributed under the terms of the Creative Commons Attribution Non-Commercial License (https://creativecommons.org/licenses/by-nc/4.0/) which permits unrestricted non-commercial use, distribution, and reproduction in any medium, provided the original work is properly cited.
Abstract
-
Objectives To evaluate postoperative pain after endodontic treatment of necrotic teeth using large intentional foraminal enlargement (LIFE).
-
Materials and Methods The sample included 60 asymptomatic necrotic teeth (with or without chronic apical periodontitis), and a periodontal probing depth of 3 mm, previously accessed and referred to perform endodontic treatment. After previous procedures, the position and approximate size of the apical foramen (AF) were determined by using an apex locator and K flexo-files, respectively. The chemomechanical preparation was performed with Profile 04 files 2 mm beyond the AF to achieve the LIFE, using 2.5 mL of 2.5% NaOCl at each file change. The filling was performed by Tagger's hybrid technique and EndoFill sealer. Phone calls were made to all the patients at 24, 48 and 72 hours after treatment, to classify postoperative pain. Statistical analysis was performed by different tests with a significance level of 5%.
-
Results Age, gender, periradicular status and tooth type did not influence postoperative pain (p > 0.05). Only 1 patient (1.66%) reported severe pain after 72 hours. Moderate pain was reported by 7, 4 and 3 patients after 24, 48 and 72 hours, respectively (p = 0.0001). However, paired analyses showed a statistically significant difference only between 24 and 72 hours (p = 0.04). Sealer extrusion did not influence the postoperative pain (p > 0.05).
-
Conclusions Acute or moderate postoperative pain was uncommon after endodontic treatment of necrotic teeth with LIFE.
-
Trial Registration The Brazilian Clinical Trials Registry Identifier: RBR-3r967t
INTRODUCTION
Endodontic treatment aims to maintain or reestablish the health of periapical tissues by cleaning and filling the root canals [1,2]. Biomechanical preparation and intracanal dressing (when used) are responsible for the disinfection process; however, they are not able to eliminate the content of the root canal system completely due to its anatomical and morphological complexity and to the resistance of some microorganisms involved in endodontic infection [3,4].
Molecular analysis has shown the presence of bacterial biofilms in apical foramen (AF) [5,6,7]. This is why the impact of intentional foraminal enlargement (IFE) on the success of endodontic treatment has been studied [8,9,10].
IFE is based on the mechanical enlargement of the AF to reduce the bacterial load by excising the infected cementum and dentin from this area [9,10]. However, a study performed by Tinaz et al. [11] showed that IFE caused greater debris extrusion, which is one of the main reasons for postoperative pain after endodontic treatment of necrotic teeth [12,13].
Several randomized clinical trials have evaluated postoperative pain after performing endodontic treatments of necrotic teeth using manual, rotary and reciprocating files to conduct IFE, and have found different results [14,15,16]. Silva et al. [16] carried out endodontic treatments of necrotic anterior teeth with or without IFE using hand files. The authors reported similar levels of postoperative pain between these groups. Cruz Junior et al. [15] conducted a similar analysis in the single-rooted necrotic tooth using a reciprocating system. Patients from the IFE group reported more pain after 24 hours.
It is noteworthy to mention that the AF frequently has an oval shape [17,18,19]. Therefore, it might be cleaned better with large IFE (LIFE) [10,20]. To the best of our knowledge, no study has yet been made to evaluate postoperative pain after performing endodontic treatment with LIFE in necrotic teeth (with or without chronic apical periodontitis). Therefore, this was the purpose of this study.
MATERIALS AND METHODS
This study received approval from the Human Research Ethics Committee of the Pontifical University of Paraná – PUC/PR (CAAE. 12449019.6.0000.0020), is reported in accordance with the Consolidated Standards of Reporting Trials Statement (CONSORT, 2010), and is registered at The Brazilian Registry of Clinical Trials (ReBEC; RBR-3r967t).
The sample size to validate the results of this research was determined by conducting a pilot study that showed that less than 5% of the patients reported significant postoperative pain (acute or moderate) after treatment. The proportion-sampling method was used to determine the sample size, which was set at 60 teeth, considering a confidence level of 95% and a maximum margin of error of 5.5%.
This study was conducted in patients ranging in age from 14 to 73 years, referred to the Centro de Especialidades Odontológicas de Navegantes, Santa Catarina, Brazil, to perform endodontic treatment, between September and October 2019. The patients were informed about the postoperative care, the clinical and radiographic examinations, and the available alternative treatment options. Information about the study and the treatment protocol were provided to all the patients or their caregivers (for patients under 18 years old), and written consent was obtained.
The inclusion criteria for this study were asymptomatic necrotic teeth (with and without chronic apical periodontitis), and a periodontal probing depth of 3 mm at most, as previously accessed at the Public Basic Health Units of the aforementioned city. The exclusion criteria were consumption of anti-inflammatories, analgesics of any type, or antibiotics within the last 10 days before treatment, presence of root resorption, sinus tracts, trismus, periodontal probing greater than 3 mm, systemic diseases, history of trauma, pregnancy, severe malocclusion associated with traumatic occlusion, lack of patient compliance and history of intolerance to nonsteroidal anti-inflammatory drugs.
After clinical and radiographic examination of the patients, and evaluation of their health status, the teeth were anesthetized using 2% mepivacaine with epinephrine 1:100,000 (Mepiadre; DFL Indústria e Comércio S.A., Rio de Janeiro, RJ, Brazil). After rubber dam placement and disinfection, the temporary restoration was removed using a 1014 or 1016 HL bur (KG Sorensen, Barueri, SP, Brazil). When reaching the pulp chamber, copious irrigation was performed with 5 mL 2.5% sodium hypochlorite (NaOCl) (Fórmula & Ação, São Paulo, SP, Brazil), and the canals were flooded continuously with irrigation solution from a NaviTip 31 G needle (Ultradent, South Jordan, UT, USA). Initial exploration was performed with a size 15 K Flexo-File (Dentsply-Maillefer, Ballaigues, Switzerland). Cervical and middle thirds were prepared with Orifice Shapers (Dentsply-Maillefer) driven by an X-Smart Plus motor (Dentsply-Maillefer). Afterward, the position of the AF was established by size 10 or larger K Flexo-Files (Dentsply-Maillefer) coupled to an apex locator (Root ZX II, J Morita, Kyoto, Japan), and confirmed by radiographs. The approximate size of the AF was determined by using K Flexo-Files size 10, 15, 20, 25 or 30 (Dentsply-Maillefer). This strategy was crucial for the instrumentation planning of similar LIFE procedures performed to treat different teeth (Table 1).
Table 1
Instrumentation planning for similar large intentional foraminal enlargement (LIFE) to treat different teeth
Chemomechanical preparation was performed by using Profile 04 files (Dentsply-Maillefer) driven by the same motor mentioned above, using a crown-down approach. A 2.5 mL aliquot of 2.5% NaOCl was used as an irrigating solution at each file change, applied with a NaviTip 31 G (Ultradent) needle up to 5 mm short of the AF, as established by rubber stops. All the teeth received the same amount of irrigant.
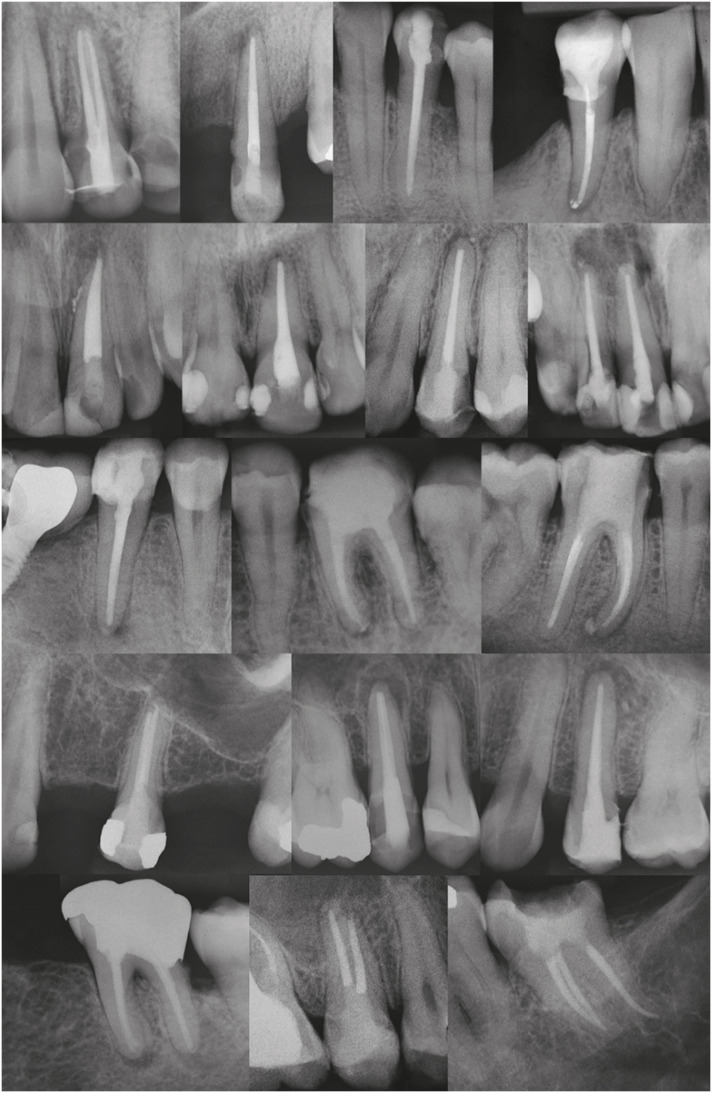
After instrumentation, the canals were flooded with 3 mL of 17% ethylenediaminetetraacetic acid (Fórmula & Ação) for 3 minutes. A final flush with 5 mL of saline solution was performed, and the canals were dried with absorbent paper points (Dentsply-Maillefer). For each canal, the main cone corresponding to the last instrument used during chemomechanical preparation was calibrated and stabilized to approximately 1.5 mm from the AF to avoid overextension. After radiographic analysis of the level of the main cone, the root canal filling was performed by Tagger's hybrid technique and Endofill sealer (Dentsply-Maillefer), and the temporary restoration, with Cavitec (Caitech, São José dos Pinhais, PR, Brazil) or Cimpat (Septodont, São Paulo, SP, Brazil). A final radiograph was taken after occlusal adjustment (Figure 1), after which the patients were referred back to the Public Basic Health Unit of origin to receive the definitive restorations. No medication was prescribed, and the patient was instructed to take either paracetamol (750 mg every 6 hours) or ibuprofen (600 mg every 6 hours) if feeling pain [15]. All the treatments were performed by a single and experienced operator (R.M).
The assessment of postoperative pain was conducted at 24, 48 and 72 hours after the treatments, as outlined below. Phone calls were made for all the patients to inquire into their pain. The postoperative pain was classified according to a score based on a verbal categorization (Table 2) [16,21].
Table 2
Scores and features of the pain
The findings were recorded on an Excel spreadsheet (Microsoft Corp., Redmond, WA, USA) for statistical evaluation with SPSS software version 25.0 (IBM Corp., Armonk, NY, USA). Kolmogorov-Smirnov's test was used to evaluate the normality of data. Kruskal-Wallis, Mann-Whitney U, χ2, Friedman's analysis of variance and Friedman's multiple 2 to 2 comparison tests were used to determine significant any difference among the variables (p < 0.05).
RESULTS
Demographic data are being shown in Table 3. General incidence and levels of postoperative pain at the time points are shown in Figure 2. There was a tendency for the postoperative pain to decrease over time (p = 0.0001). However, paired analyses showed a statistically significant difference only between 24 and 72 hours (p = 0.04). Age, gender, periradicular status, tooth type and sealer extrusion did not influence the postoperative pain, regardless of time (p > 0.05) (Tables 4, 5, 6).
Table 3
Demographic data
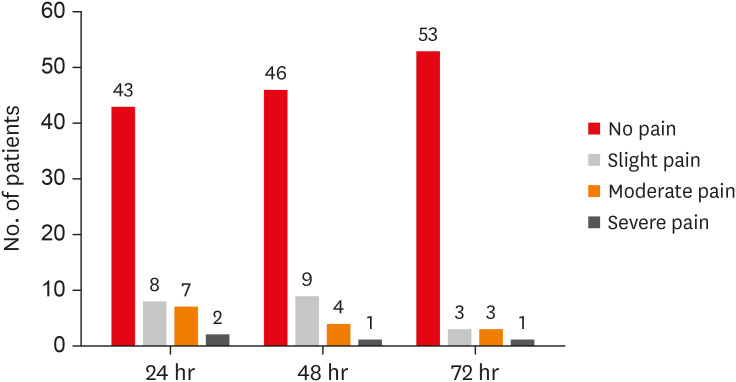
Table 4
Postoperative pain considering time and age, gender, periradicular status, and tooth type
Table 5
Postoperative pain considering time frame
Table 6
Postoperative pain considering sealer extrusion
DISCUSSION
The root canal system of necrotic teeth is contaminated, including the AF. Considering that the recommended treatment involves removing the cause of the disease, IFE could promote better cleaning by improving the condition for tissue repair [10]. However, it has been suggested that even small patency files used through the apex may cause an acute periapical inflammatory response and severe postoperative pain [22]. Therefore, a common concern regarding IFE is the postoperative pain related to physical iatrogenic trauma in the periapical region [14,15,16,23]. However, the AF in most dental groups is oval-shaped; consequently, better cleaning of this region could be achieved with LIFE [10,17,18,19,20]. Up to now, the incidence and levels of postoperative pain have been evaluated only after performing endodontic treatments of necrotic teeth with IFE [14,15,16]. Hence, the aim of this study was to perform the same analysis with LIFE.
Assessment of the incidence and levels of postoperative pain after performing endodontic treatment is a challenge due to the complexity of the intervention [13,24,25,26]. Assuming preoperative pain is a strong predictor of postoperative pain, only symptom-free patients were included in this study. Single-visit endodontic treatments have led to the same postoperative pain and healing of periapical tissues as 2-visit treatments [27,28,29,30,31]. Therefore, all treatments were completed in a single visit, to minimize the number of procedures and variations of intracanal medication used [14,15,29]. However, endodontic accesses had already been performed in previous appointments. Finally, it has been considered that operator experience may influence the incidence of postoperative pain [32]. For this reason, all treatments were performed by the same operator [14,15,24].
Different methods have been used to assess pain after endodontic therapy, such as visual analog scales (VAS), scores based on verbal categorizations or both [15,33,34,35,36,37,38]. The design of the method is crucial and must ensure that the questions will be fully understood by the patients and easily interpreted by the researchers [16,39]. In the present study, a score was used to classify postoperative pain, based on verbal categorizations, as follows: no, slight, moderate, and severe/acute pain. These categories were understood straightforwardly by patients. A similar strategy was used in other studies [16,34,35,36,40].
Our results pointed out that age did not influence postoperative pain, thus corroborating the findings by Ng et al. [41] and Polycarpou et al. [42]. On the other hand, Ali et al. [40] showed a higher postoperative pain in older (41 to 65 years) compared with younger (15 to 40 years) patients. The probable reasons could be lower pain tolerance, less blood flow, and delayed healing. However, a direct comparison between our results and those obtained by the 3 previously cited studies [40,41,42] should be made with caution. The age difference between the upper and lower limits of the age groupings of the cited studies [40,41,42] was 10 years and 25 years. Herein, the limit was about 15 years. In addition, the number of patients in the study groups was very discrepant. In the study by Ng et al. [41] for example, 119 (28.7%) of the 415 patients were ≥ 40 and < 50 years old, and 8 (1.9%) were ≥ 80 years old. In the present study, 21 patients were < 30 years old, 21 patients were ≥ 30 and ≤ 50 years old, and 18 patients were > 50 years old, that is, a similar distribution of patients occurred herein regarding age.
Several studies have shown a higher prevalence of postoperative pain in females than males [13,34,40]. The biological discrepancy between men and women could explain why [43,44]. Moreover, comparing the difference between male and female reproductive and pelvic anatomies, females have an additional portal of entry of infection, thereby leading to possible local and distant hyperalgesia. Moreover, fluctuating female hormonal levels might be associated with changing levels of serotonin and noradrenaline, thus leading to increased pain prevalence in females during the menstrual period, and when receiving hormonal replacement therapy or taking oral contraceptives [13,40,41]. However, our results pointed to no gender-related difference in postoperative pain. A plausible explanation is that a similar number of men and women (28/32) having similar ages (37.86 ± 18.55/38.38 ± 15.29, respectively) were treated herein. Healthy middle-aged women are likely to be less subject to the side effects associated with the above physical factors, and may therefore have responses to pain corresponding to those of men [41,42].
The nature of the pulp and periapical status could modulate postoperative pain in endodontics. Teeth with nonvital pulps associated with periapical lesions are densely contaminated, and have an 83.2% prevalence of foraminal resorption [45]. In addition, disruption of the apical constriction by IFE causes greater debris extrusion, which is an important factor associated with postoperative pain [11,17]. Nevertheless, our results showed that postoperative pain was not influenced by periradicular status. Marshall and Liesinger [46] observed that patients with periapical lesions that could not be detected by radiograph had more postoperative pain than those who had such lesions detected by radiograph. Ng et al. [41] indicated that postoperative pain was less in teeth having large periapical lesions (> 3 mm), compared with teeth having smaller or no periapical lesions. Genet et al. [47] showed that postoperative pain was greater in teeth with periapical radiolucency greater than 5 mm in diameter. A periapical lesion from an endodontic infection might exist without being visible in the radiograph [48]. It can be detected radiographically only when it attains nearly 30%–50% of the bone mineral loss [49,50]. Other conditions, such as apical morphologic variations, surrounding bone density, X-ray angulations and radiographic contrast, also influence radiographic interpretation [51]. These factors may explain the conflicting results of the studies cited above and also the present findings [41,46,47].
Some studies showed that postoperative pain was more frequent and higher in posterior teeth [13,33,41]. This could be attributed to their more complex root canal anatomy [36]. Conversely, other studies pointed out that postoperative pain was not influenced by the tooth type [28,52,53]. In this study, tooth type also did not influence postoperative pain. As mentioned previously, an experienced operator (R.M) performed all the treatments. This could have decreased the impact of the root canal anatomy, thus contributing to the low incidence and levels of postoperative pain.
Overall, mean pain scores were low, and just one patient reported severe/acute pain after 72 hours (1.66%). Similar results were obtained by Relvas et al. [35] in the group where the chemomechanical preparation was performed by a rotary system (ProTaper Universal). We believe that the low incidence and levels of postoperative pain observed in our study are probably related to the same reasons found by Relvas et al. [35] namely: a) only teeth with asymptomatic pulp necrosis were treated; b) all teeth suffered occlusal adjustment after the treatment; and c) in regard to the irrigation protocol, the same volume of irrigant was used, and the needle was inserted at a distance far enough from the apex to prevent extrusion.
Moderate pain was reported by 7, 4 and 3 patients after 24, 48 and 72 hours, respectively, implying that there was a tendency for pain to decrease over time (p = 0.0001). However, paired analyses showed a statistically significant difference only between 24 and 72 hours (p = 0.04). These results are in line with those obtained by a prospective, randomized, double-blind clinical trial performed by Shokraneh et al. [54] and a systematic review and meta-analysis conducted by Pak and White [55]. Nonetheless, Yaylali et al. [14] observed more pain in the 48-hour post-treatment period. This contradictory result may be attributed to the different methodological designs between the last cited study [14] and the current research. In the study by Yaylali et al. [14] only necrotic molars with radiographically visualized periradicular lesions were treated. Chemomechanical preparation was performed by using ProTaper Next files after establishing the working length (WL) at the AF. The irrigation consisted of 2.5% NaOCl using a Max-i-Probe needle up to 2 mm short of the WL, and the postoperative pain was evaluated by VAS. The authors did not report the approximate size of the AF. In our clinical protocol, the WL was determined at 2 mm beyond the AF. After measuring the approximate size of the AF with manual files, chemomechanical preparation was performed by using Profile 04 files to conduct the LIFE. Irrigation was performed with 2.5% NaOCl using a NaviTip needle up to 5 mm short of the AF, and the postoperative pain was evaluated with a score based on a verbal categorization.
Oxidative stress and, more specifically, reactive oxygen species (ROS) have been found to be linked to inflammatory pain in vivo [56,57]. A recent study showed that the production of ROS increased 4- to 7-fold when the human pulp cells were treated with root canal sealers in vitro [58]. This led the authors of the present study to evaluate the relationship between postoperative pain and sealer extrusion; however, no correlation was observed. According to Sadaf and Ahmad [28], clinical symptoms are associated with the composition and amount of the extruded sealer. Cintra et al. [59] showed that Endofill had the least favorable characteristics regarding cell viability, compared with Sealer Plus, AH Plus, Endofill, and SimpliSeal. Furthermore, in the histologic analysis, severe inflammation was observed at 7 days, characterized by multinucleated giant cells, and most specimens presented severe inflammation even after 30 days. These results can be explained by the presence of eugenol, which was also responsible for the strong antimicrobial action of this sealer [60]. Endofill was used in the present study, but only slight sealer extrusion occurred in 24 cases, and did not have a significant influence on postoperative pain over time (p > 0.05) [28].
CONCLUSIONS
The incidence and levels of postoperative pain after performing endodontic treatments in necrotic teeth with LIFE were low and not influenced by gender, age, tooth type, periradicular status or sealer extrusion. When postoperative pain did occur, it tended to decrease over time.
-
Conflict of Interest: No potential conflict of interest relevant to this article was reported.
-
Author Contributions:
Conceptualization: Machado R.
Data curation: Machado R, Comparin D.
Formal analysis: Ignácio SA.
Funding acquisition: Machado R.
Investigation: Machado R.
Methodology: Machado R.
Project administration: Silva Neto UX.
Resources: Machado R.
Software: Machado R, Ignácio SA.
Supervision: Silva Neto UX.
Validation: Ignácio SA.
Visualization: Machado R.
Writing - original draft: Machado R, Comparin D.
Writing - review & editing: Silva Neto UX.
- 1. Schilder H. Filling root canals in three dimensions. Dent Clin North Am 1967;723-744.ArticlePubMed
- 2. Schilder H. Cleaning and shaping the root canal. Dent Clin North Am 1974;18:269-296.ArticlePubMed
- 3. Üreyen Kaya B, Erik CE, Sesli Çetin E, Köle M, Maden M. Mechanical reduction in intracanal Enterococcus faecalis when using three different single-file systems: an ex vivo comparative study. Int Endod J 2019;52:77-85.ArticlePubMedPDF
- 4. Martinho FC, Gomes CC, Nascimento GG, Gomes AP, Leite FR. Clinical comparison of the effectiveness of 7- and 14-day intracanal medications in root canal disinfection and inflammatory cytokines. Clin Oral Investig 2018;22:523-530.ArticlePubMedPDF
- 5. Chavez de Paz LE. Redefining the persistent infection in root canals: possible role of biofilm communities. J Endod 2007;33:652-662.ArticlePubMed
- 6. Wang J, Chen W, Jiang Y, Liang J. Imaging of extraradicular biofilm using combined scanning electron microscopy and stereomicroscopy. Microsc Res Tech 2013;76:979-983.ArticlePubMed
- 7. Wang J, Jiang Y, Chen W, Zhu C, Liang J. Bacterial flora and extraradicular biofilm associated with the apical segment of teeth with post-treatment apical periodontitis. J Endod 2012;38:954-959.ArticlePubMed
- 8. Brandão PM, de Figueiredo JA, Morgental RD, Scarparo RK, Hartmann RC, Waltrick SB, Souza RA. Influence of foraminal enlargement on the healing of periapical lesions in rat molars. Clin Oral Investig 2019;23:1985-1991.ArticlePubMedPDF
- 9. Borlina SC, de Souza V, Holland R, Murata SS, Gomes-Filho JE, Dezan Junior E, Marion JJ, Neto DA. Influence of apical foramen widening and sealer on the healing of chronic periapical lesions induced in dogs' teeth. Oral Surg Oral Med Oral Pathol Oral Radiol Endod 2010;109:932-940.ArticlePubMed
- 10. de Souza Filho FJ, Benatti O, de Almeida OP. Influence of the enlargement of the apical foramen in periapical repair of contaminated teeth of dog. Oral Surg Oral Med Oral Pathol 1987;64:480-484.ArticlePubMed
- 11. Tinaz AC, Alacam T, Uzun O, Maden M, Kayaoglu G. The effect of disruption of apical constriction on periapical extrusion. J Endod 2005;31:533-535.ArticlePubMed
- 12. Mostafa MEHAA, El-Shrief YAI, Anous WIO, Hassan MW, Salamah FTA, El Boghdadi RM, El-Bayoumi MAA, Seyam RM, Abd-El-Kader KG, Amin SAW. Postoperative pain following endodontic irrigation using 1.3% versus 5.25% sodium hypochlorite in mandibular molars with necrotic pulps: a randomized double-blind clinical trial. Int Endod J 2020;53:154-166.ArticlePubMedPDF
- 13. Nagendrababu V, Gutmann JL. Factors associated with postobturation pain following single-visit nonsurgical root canal treatment: a systematic review. Quintessence Int 2017;48:193-208.PubMed
- 14. Yaylali IE, Teke A, Tunca YM. The effect of foraminal enlargement of necrotic teeth with a continuous rotary system on postoperative pain: a randomized controlled trial. J Endod 2017;43:359-363.ArticlePubMed
- 15. Cruz Junior JA, Coelho MS, Kato AS, Vivacqua-Gomes N, Fontana CE, Rocha DG, da Silveira Bueno CE. The effect of foraminal enlargement of necrotic teeth with the reciproc system on postoperative pain: a prospective and randomized clinical trial. J Endod 2016;42:8-11.ArticlePubMed
- 16. Silva EJ, Menaged K, Ajuz N, Monteiro MR, Coutinho-Filho TS. Postoperative pain after foraminal enlargement in anterior teeth with necrosis and apical periodontitis: a prospective and randomized clinical trial. J Endod 2013;39:173-176.ArticlePubMed
- 17. Kuttler Y. Microscopic investigation of root apexes. J Am Dent Assoc 1955;50:544-552.ArticlePubMed
- 18. Ponce EH, Vilar Fernández JA. The cemento-dentino-canal junction, the apical foramen, and the apical constriction: evaluation by optical microscopy. J Endod 2003;29:214-219.ArticlePubMed
- 19. Dummer PM, McGinn JH, Rees DG. The position and topography of the apical canal constriction and apical foramen. Int Endod J 1984;17:192-198.ArticlePubMed
- 20. Aminoshariae A, Kulild JC. Master apical file size - smaller or larger: a systematic review of healing outcomes. Int Endod J 2015;48:639-647.ArticlePubMed
- 21. Pasqualini D, Mollo L, Scotti N, Cantatore G, Castellucci A, Migliaretti G, Berutti E. Postoperative pain after manual and mechanical glide path: a randomized clinical trial. J Endod 2012;38:32-36.ArticlePubMed
- 22. Cailleteau JG, Mullaney TP. Prevalence of teaching apical patency and various instrumentation and obturation techniques in United States dental schools. J Endod 1997;23:394-396.ArticlePubMed
- 23. Kherlakian D, Cunha RS, Ehrhardt IC, Zuolo ML, Kishen A, da Silveira Bueno CE. Comparison of the incidence of postoperative pain after using 2 reciprocating systems and a continuous rotary system: a prospective randomized clinical trial. J Endod 2016;42:171-176.ArticlePubMed
- 24. Arias A, de la Macorra JC, Azabal M, Hidalgo JJ, Peters OA. Prospective case controlled clinical study of post-endodontic pain after rotary root canal preparation performed by a single operator. J Dent 2015;43:389-395.ArticlePubMed
- 25. Arias A, de la Macorra JC, Hidalgo JJ, Azabal M. Predictive models of pain following root canal treatment: a prospective clinical study. Int Endod J 2013;46:784-793.ArticlePubMed
- 26. Sun C, Sun J, Tan M, Hu B, Gao X, Song J. Pain after root canal treatment with different instruments: a systematic review and meta-analysis. Oral Dis 2018;24:908-919.ArticlePubMedPDF
- 27. Alí A, Olivieri JG, Duran-Sindreu F, Abella F, Roig M, García-Font M. Influence of preoperative pain intensity on postoperative pain after root canal treatment: A prospective clinical study. J Dent 2016;45:39-42.ArticlePubMed
- 28. Sadaf D, Ahmad MZ. Factors associated with postoperative pain in endodontic therapy. Int J Biomed Sci 2014;10:243-247.ArticlePubMedPMC
- 29. Patil AA, Joshi SB, Bhagwat SV, Patil SA. Incidence of postoperative pain after single visit and two visit root canal therapy: a randomized controlled trial. J Clin Diagn Res 2016;10:ZC09-ZC12.Article
- 30. El Mubarak AH, Abu-bakr NH, Ibrahim YE. Postoperative pain in multiple-visit and single-visit root canal treatment. J Endod 2010;36:36-39.ArticlePubMed
- 31. Paredes-Vieyra J, Enriquez FJ. Success rate of single- versus two-visit root canal treatment of teeth with apical periodontitis: a randomized controlled trial. J Endod 2012;38:1164-1169.ArticlePubMed
- 32. García-Font M, Duran-Sindreu F, Calvo C, Basilio J, Abella F, Ali A, Roig M, Olivieri JG. Comparison of postoperative pain after root canal treatment using reciprocating instruments based on operator's experience: a prospective clinical study. J Clin Exp Dent 2017;9:e869-e874.PubMedPMC
- 33. Graunaite I, Skucaite N, Lodiene G, Agentiene I, Machiulskiene V. Effect of resin-based and bioceramic root canal sealers on postoperative pain: a split-mouth randomized controlled trial. J Endod 2018;44:689-693.ArticlePubMed
- 34. Al-Negrish AR, Habahbeh R. Flare up rate related to root canal treatment of asymptomatic pulpally necrotic central incisor teeth in patients attending a military hospital. J Dent 2006;34:635-640.ArticlePubMed
- 35. Relvas JB, Bastos MM, Marques AA, Garrido AD, Sponchiado EC Jr. Assessment of postoperative pain after reciprocating or rotary NiTi instrumentation of root canals: a randomized, controlled clinical trial. Clin Oral Investig 2016;20:1987-1993.ArticlePubMedPDF
- 36. Çiçek E, Koçak MM, Koçak S, Sağlam BC, Türker SA. Postoperative pain intensity after using different instrumentation techniques: a randomized clinical study. J Appl Oral Sci 2017;25:20-26.ArticlePubMedPMC
- 37. Farzaneh S, Parirokh M, Nakhaee N, Abbott PV. Effect of two different concentrations of sodium hypochlorite on postoperative pain following single-visit root canal treatment: a triple-blind randomized clinical trial. Int Endod J 2018;51(Suppl 1):e2-e11.ArticlePubMedPDF
- 38. Attar S, Bowles WR, Baisden MK, Hodges JS, McClanahan SB. Evaluation of pretreatment analgesia and endodontic treatment for postoperative endodontic pain. J Endod 2008;34:652-655.ArticlePubMed
- 39. Arias A, Azabal M, Hidalgo JJ, de la Macorra JC. Relationship between postendodontic pain, tooth diagnostic factors, and apical patency. J Endod 2009;35:189-192.ArticlePubMed
- 40. Ali SG, Mulay S, Palekar A, Sejpal D, Joshi A, Gufran H. Prevalence of and factors affecting post-obturation pain following single visit root canal treatment in Indian population: a prospective, randomized clinical trial. Contemp Clin Dent 2012;3:459-463.ArticlePubMedPMC
- 41. Ng YL, Glennon JP, Setchell DJ, Gulabivala K. Prevalence of and factors affecting post-obturation pain in patients undergoing root canal treatment. Int Endod J 2004;37:381-391.ArticlePubMed
- 42. Polycarpou N, Ng YL, Canavan D, Moles DR, Gulabivala K. Prevalence of persistent pain after endodontic treatment and factors affecting its occurrence in cases with complete radiographic healing. Int Endod J 2005;38:169-178.ArticlePubMed
- 43. Unruh AM. Gender variations in clinical pain experience. Pain 1996;65:123-167.ArticlePubMed
- 44. Fillingim RB, Maixner W. Gender differences in the responses to noxious stimuli. Pain Forum 1995;4:209-221.Article
- 45. Vier FV, Figueiredo JA. Prevalence of different periapical lesions associated with human teeth and their correlation with the presence and extension of apical external root resorption. Int Endod J 2002;35:710-719.PubMed
- 46. Marshall JG, Liesinger AW. Factors associated with endodontic posttreatment pain. J Endod 1993;19:573-575.ArticlePubMed
- 47. Genet JM, Hart AA, Wesselink PR, Thoden van Velzen SK. Preoperative and operative factors associated with pain after the first endodontic visit. Int Endod J 1987;20:53-64.ArticlePubMed
- 48. Estrela C, Bueno MR, Leles CR, Azevedo B, Azevedo JR. Accuracy of cone beam computed tomography and panoramic and periapical radiography for detection of apical periodontitis. J Endod 2008;34:273-279.ArticlePubMed
- 49. Bender IB, Seltzer S. Roentgenographic and direct observation of experimental lesions in bone: II. 1961. J Endod 2003;29:707-712.PubMed
- 50. Bender IB, Seltzer S. Roentgenographic and direct observation of experimental lesions in bone: I. 1961. J Endod 2003;29:702-706.PubMed
- 51. Halse A, Molven O, Fristad I. Diagnosing periapical lesions--disagreement and borderline cases. Int Endod J 2002;35:703-709.ArticlePubMed
- 52. Yesilsoy C, Koren LZ, Morse DR, Rankow H, Bolanos OR, Furst ML. Post-endodontic obturation pain: a comparative evaluation. Quintessence Int 1988;19:431-438.PubMed
- 53. Liddell A, Locker D. Gender and age differences in attitudes to dental pain and dental control. Community Dent Oral Epidemiol 1997;25:314-318.ArticlePubMed
- 54. Shokraneh A, Ajami M, Farhadi N, Hosseini M, Rohani B. Postoperative endodontic pain of three different instrumentation techniques in asymptomatic necrotic mandibular molars with periapical lesion: a prospective, randomized, double-blind clinical trial. Clin Oral Investig 2017;21:413-418.ArticlePubMedPDF
- 55. Pak JG, White SN. Pain prevalence and severity before, during, and after root canal treatment: a systematic review. J Endod 2011;37:429-438.ArticlePubMed
- 56. Hackel D, Pflücke D, Neumann A, Viebahn J, Mousa S, Wischmeyer E, Roewer N, Brack A, Rittner HL. The connection of monocytes and reactive oxygen species in pain. PLoS One 2013;8:e63564.ArticlePubMedPMC
- 57. Vengerfeldt V, Mändar R, Saag M, Piir A, Kullisaar T. Oxidative stress in patients with endodontic pathologies. J Pain Res 2017;10:2031-2040.PubMedPMC
- 58. Camargo CH, Camargo SE, Valera MC, Hiller KA, Schmalz G, Schweikl H. The induction of cytotoxicity, oxidative stress, and genotoxicity by root canal sealers in mammalian cells. Oral Surg Oral Med Oral Pathol Oral Radiol Endod 2009;108:952-960.ArticlePubMed
- 59. Cintra LT, Benetti F, de Azevedo Queiroz IO, Ferreira LL, Massunari L, Bueno CR, de Oliveira SH, Gomes-Filho JE. Evaluation of the cytotoxicity and biocompatibility of new resin epoxy-based endodontic sealer containing calcium hydroxide. J Endod 2017;43:2088-2092.ArticlePubMed
- 60. Morgental RD, Vier-Pelisser FV, Oliveira SD, Antunes FC, Cogo DM, Kopper PM. Antibacterial activity of two MTA-based root canal sealers. Int Endod J 2011;44:1128-1133.ArticlePubMed
REFERENCES
Tables & Figures
REFERENCES
Citations
Citations to this article as recorded by 
- Postoperative Pain After Endodontic Treatment in HIV‐Positive Patients Under HAART: A Prospective Observational Cohort Study
Marcos Felipe Iparraguirre Nuñovero, Marco Antonio Hungaro Duarte, Luciana Reis Azevedo Alanis, Bruno Cavalini Cavenago, Ulisses Xavier da Silva Neto, Everdan Carneiro
International Endodontic Journal.2026; 59(5): 788. CrossRef - Does maintaining apical patency reduce early postoperative pain after root canal treatment? A randomized controlled trial in asymptomatic vital single-rooted teeth
Ozan Arda Deger, Sehnaz Yilmaz, Kübra Gürler
Clinical Oral Investigations.2026;[Epub] CrossRef - Evaluation of Postoperative Pain Frequency in Single‐Session Endodontic Treatments With Patency and Foraminal Enlargement
Viviane Barbosa Godoy, Ana Grasiela Limoeiro, Vanessa Sandini, Vini Mehta, Wayne Martins Nascimento, Marilia Fagury Videira Marceliano‐Alves, Marcos Frozoni
Clinical and Experimental Dental Research.2026;[Epub] CrossRef - Assessment of apical extrusion in regenerative endodontics: a comparative study of different irrigation methods using three-dimensional immature tooth models
Vahide Hazal Abat, Gökçen Deniz Bayrak, Mustafa Gündoğar
Odontology.2025; 113(1): 213. CrossRef - Clinical Advances in Calcium Phosphate for Maxillomandibular Bone Regeneration: From Bench to Bedside
Seyed Ali Mostafavi Moghaddam, Hamid Mojtahedi, Amirhossein Bahador, Lotfollah Kamali Hakim, Hamid Tebyaniyan
Ceramics.2025; 8(4): 129. CrossRef - Postoperative pain after single-visit root canal treatments in necrotic teeth comparing instruments’ kinematics and apical instrumentation limits – a prospective randomized multicenter clinical trial
Ricardo Machado, Guilherme Moreira, Daniel Comparin, Arthur Pimentel Barroso, Jaqueline Nascimento, Caio Cézar Randi Ferraz, Sérgio Aparecido Ignácio, Lucas da Fonseca Roberti Garcia, Rodrigo Rodrigues Amaral, David Shadid, Ulisses Xavier da Silva Neto
BMC Oral Health.2024;[Epub] CrossRef - Assessment of mechanical allodynia in healthy teeth adjacent and contralateral to endodontically diseased teeth: a clinical study
Vaishnavi Ratnakar Patankar, Ashish K Jain, Rahul D Rao, Prajakta R Rao
Restorative Dentistry & Endodontics.2024;[Epub] CrossRef - A systematic review and meta-analysis on the effects of phototherapy on postoperative pain in conventional endodontic reintervention
Larissa Pereira Nunes, Gabriel Pereira Nunes, Túlio Morandin Ferrisse, Henrico Badaoui Strazzi-Sahyon, Eloi Dezan-Júnior, Luciano Tavares Angelo Cintra, Gustavo Sivieri-Araujo
Clinical Oral Investigations.2024;[Epub] CrossRef - The effect of intracanal cryotherapy with and without foraminal enlargement on pain prevention after endodontic treatment: a randomized clinical trial
Marcos Felipe Iparraguirre Nuñovero, Marco Antonio Hungaro Duarte, André Vinícius Kaled Segato, Ulisses Xavier da Silva Neto, Vania Portela Ditzel Westphalen, Everdan Carneiro
Scientific Reports.2024;[Epub] CrossRef - Clinical determination of anatomical diameter in different dental groups correlating them with gender, age, tooth/canal and pulpoperiradicular diagnosis: an observational clinical study
Ricardo Machado, Gabriel Filipe Pamplona, Claudemir de Souza Júnior, Jaqueline Nascimento, Eduardo Donato Eing Elgelke Back, Daniel Comparin, Sérgio Aparecido Ignácio, Stella Maria Glaci Reinke, Ana Cristina Kovalik, Ulisses Xavier da Silva Neto
Scientific Reports.2023;[Epub] CrossRef - How much to enlarge? A letter to the editor
Krishnamachari Janani, Kavalipurapu Venkata Teja, Kumar Chandan Srivatsava
Saudi Endodontic Journal.2023; 13(3): 288. CrossRef - Efficiency of diode laser in control of post-endodontic pain: a randomized controlled trial
Hend H. Ismail, Maram Obeid, Ehab Hassanien
Clinical Oral Investigations.2023; 27(6): 2797. CrossRef - Periapical Healing following Root Canal Treatment Using Different Endodontic Sealers: A Systematic Review
Akshay Khandelwal, Krishnamachari Janani, KavalipurapuVenkata Teja, Jerry Jose, Gopi Battineni, Francesco Riccitiello, Alessandra Valletta, Ajitha Palanivelu, Gianrico Spagnuolo, Vincenzo Grassia
BioMed Research International.2022;[Epub] CrossRef
 ePub Link
ePub Link Cite
CitePostoperative pain after endodontic treatment of necrotic teeth with large intentional foraminal enlargement
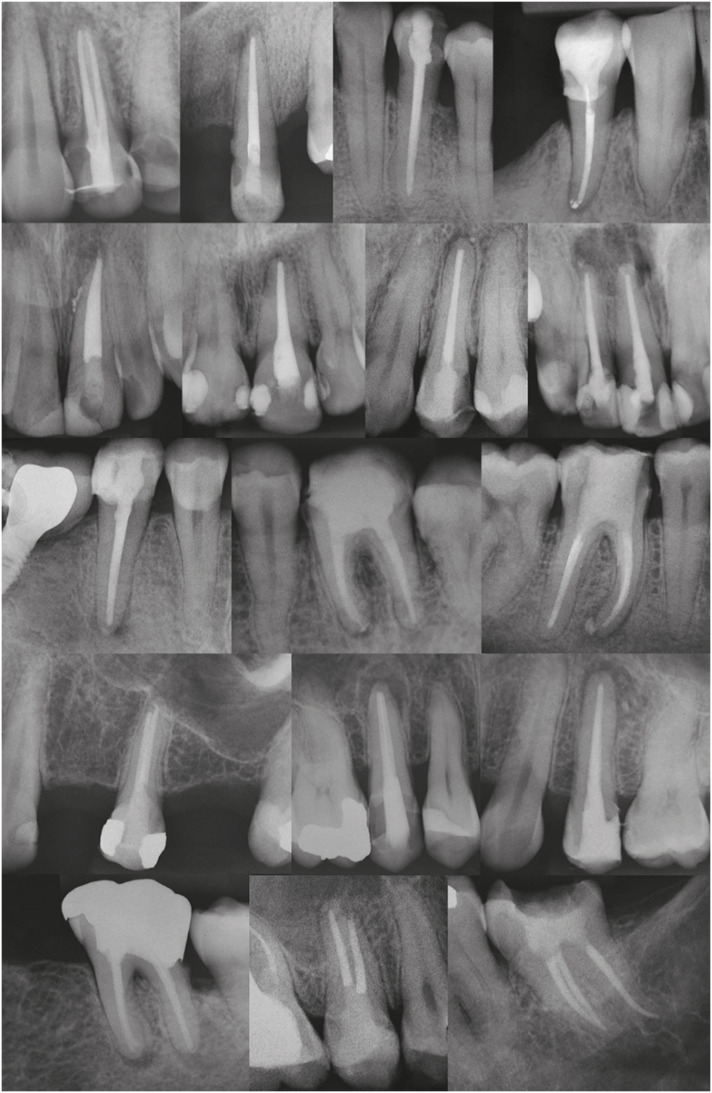
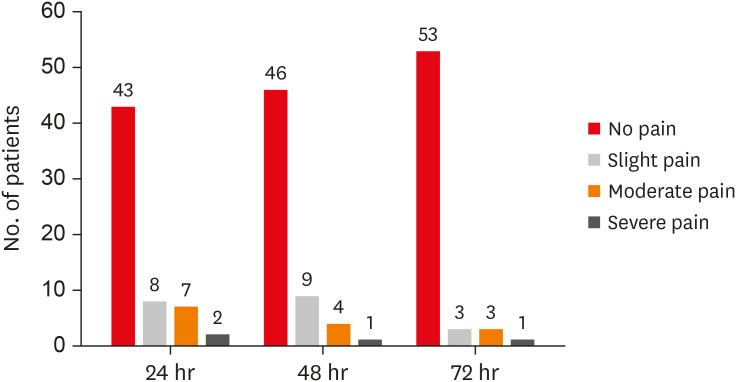
Figure 1 Examples of final radiographs.
Figure 2 Incidence and levels of postoperative pain after 24, 48 and 72 hours.
Figure 1
Figure 2
Postoperative pain after endodontic treatment of necrotic teeth with large intentional foraminal enlargement
Instrumentation planning for similar large intentional foraminal enlargement (LIFE) to treat different teeth
| Approximate size of AF before instrumentation (corresponding to the manual Flexo-File number) | Final file used 2mm beyond the AF (tip/taper) | Approximate size of AF after instrumentation (corresponding to D2 of the final file used) |
|---|---|---|
| 10 | 30.04 | 38 |
| 15 | 35.04 | 43 |
| 20 | 40.04 | 48 |
| 25 | 45.04 | 53 |
| 30 | 60.04 | 68 |
AF, apical foramen.
Scores and features of the pain
| Score | Pain | Features |
|---|---|---|
| 0 | No pain | The patient felt well. |
| 1 | Slight pain | The patient could be distracted from feeling pain, and no analgesic was required. |
| 2 | Moderate pain | The patient felt moderate pain even while concentrating on some other activity, and an analgesic was required. |
| 3 | Severe pain | The patient was no longer able to perform any type of activity, and needed to lie down and rest (analgesics had little or no effect on relieving the pain). |
Demographic data
| Characteristics | Men | Women | Total | |
|---|---|---|---|---|
| No. of patients | 28 | 32 | 60 | |
| Age (mean ± standard deviation) | 37.86 ± 18.55 | 38.38 ± 15.29 | - | |
| Periradicular status | Without lesion: 3 | Without lesion: 9 | 12 | |
| With lesion: 25 | With lesion: 23 | 48 | ||
| Tooth | ||||
| Maxillary canine | 1 | 2 | 3 | |
| Mandibular central incisor | 4 | 0 | 4 | |
| Maxillary central incisor | 3 | 4 | 7 | |
| Mandibular lateral incisor | 1 | 0 | 1 | |
| Maxillary lateral incisor | 0 | 1 | 1 | |
| First mandibular molar | 3 | 5 | 8 | |
| First maxillary molar | 2 | 3 | 5 | |
| First mandibular premolar | 1 | 1 | 2 | |
| First maxillary premolar | 3 | 3 | 6 | |
| Second mandibular molar | 0 | 1 | 1 | |
| Second maxillary molar | 4 | 0 | 4 | |
| Second mandibular premolar | 2 | 5 | 7 | |
| Second maxillary premolar | 4 | 7 | 11 | |
Postoperative pain considering time and age, gender, periradicular status, and tooth type
| Characteristics | Time (after; hr) | Subdivision | Number | Mean pain score | Standard deviation | p value |
|---|---|---|---|---|---|---|
| Age | 24 | < 30 years old | 21 | 0.52 | 0.873 | 0.10* |
| ≥ 30 and ≤ 50 years old | 21 | 0.71 | 1.007 | |||
| > 50 years old | 18 | 0.11 | 0.323 | |||
| 48 | < 30 years old | 21 | 0.43 | 0.811 | 0.30* | |
| ≥ 30 and ≤ 50 years old | 21 | 0.43 | 0.746 | |||
| > 50 years old | 18 | 0.11 | 0.323 | |||
| 72 | < 30 years old | 21 | 0.29 | 0.784 | 0.17* | |
| ≥ 30 and ≤ 50 years old | 21 | 0.29 | 0.644 | |||
| > 50 years old | 18 | 0.00 | 0.000 | |||
| Gender | 24 | Men | 28 | 0.32 | 0.612 | 0.40† |
| Women | 32 | 0.59 | 0.979 | |||
| 48 | Men | 28 | 0.25 | 0.518 | 0.62† | |
| Women | 32 | 0.41 | 0.798 | |||
| 72 | Men | 28 | 0.07 | 0.378 | 0.07† | |
| Women | 32 | 0.31 | 0.738 | |||
| Periradicular status | 24 | Without lesion | 12 | 0.50 | 0.790 | 0.72† |
| With lesion | 48 | 0.46 | 0.840 | |||
| 48 | Without lesion | 12 | 0.50 | 0.790 | 0.32† | |
| With lesion | 48 | 0.29 | 0.650 | |||
| 72 | Without lesion | 12 | 0.33 | 0.770 | 0.50† | |
| With lesion | 48 | 0.17 | 0.550 | |||
| Tooth type‡ | 24 | Maxillary canine | 3 | 0.00 | 0.000 | 0.87* |
| Mandibular central incisor | 4 | 0.50 | 1.000 | |||
| Maxillary central incisor | 7 | 0.71 | 0.951 | |||
| First mandibular molar | 8 | 0.50 | 1.069 | |||
| First maxillary molar | 5 | 0.60 | 0.894 | |||
| First maxillary premolar | 6 | 0.17 | 0.408 | |||
| Second maxillary molar | 4 | 0.50 | 0.577 | |||
| Second mandibular premolar | 7 | 0.71 | 1.254 | |||
| Second maxillary premolar | 11 | 0.27 | 0.647 | |||
| 48 | Maxillary canine | 3 | 0.00 | 0.000 | 0.81* | |
| Mandibular central incisor | 4 | 0.25 | 0.500 | |||
| Maxillary central incisor | 7 | 0.57 | 0.787 | |||
| First mandibular molar | 8 | 0.50 | 1.069 | |||
| First maxillary molar | 5 | 0.00 | 0.000 | |||
| First maxillary premolar | 6 | 0.17 | 0.408 | |||
| Second maxillary molar | 4 | 0.25 | 0.500 | |||
| Second mandibular premolar | 7 | 0.43 | 0.787 | |||
| Second maxillary premolar | 11 | 0.27 | 0.647 | |||
| 72 | Maxillary canine | 3 | 0.00 | 0.000 | 0.56* | |
| Mandibular central incisor | 4 | 0.00 | 0.000 | |||
| Maxillary central incisor | 7 | 0.43 | 0.787 | |||
| First mandibular molar | 8 | 0.38 | 1.061 | |||
| First maxillary molar | 5 | 0.00 | 0.000 | |||
| First maxillary premolar | 6 | 0.00 | 0.000 | |||
| Second maxillary molar | 4 | 0.00 | 0.000 | |||
| Second mandibular premolar | 7 | 0.43 | 0.787 | |||
| Second maxillary premolar | 11 | 0.18 | 0.603 |
*Value obtained from Kruskal-Wallis test; †Value obtained from Mann-Whitney U test; ‡Only tooth types with n. greater than 2 were used to analyze this variable.
Postoperative pain considering time frame
| Characteristics | Comparative analysis (hr) | Mean pain difference | Standard error | Test statistics | p value* |
|---|---|---|---|---|---|
| Time frame | 24 vs. 48 | 0.13 | 0.18 | 0.73 | 0.46 |
| 48 vs. 72 | 0.18 | 0.18 | 1.00 | 0.31 | |
| 24 vs. 72 | 0.37 | 0.18 | 2.02 | 0.04 |
*Value obtained by Friedman's multiple 2 to 2 comparisons test.
Postoperative pain considering sealer extrusion
| Characteristics | Time (after; hr) | Occurrence of the event | Number | Mean pain score | Standard deviation | p value* |
|---|---|---|---|---|---|---|
| Sealer extrusion | 24 | No | 36 | 0.25 | 0.50 | 0.07 |
| Yes | 24 | 0.79 | 1.10 | |||
| 48 | No | 36 | 0.19 | 0.46 | 0.10 | |
| Yes | 24 | 0.54 | 0.88 | |||
| 72 | No | 36 | 0.08 | 0.36 | 0.07 | |
| Yes | 24 | 0.38 | 0.82 |
*Value obtained from Mann-Whitney U test.
Table 1 Instrumentation planning for similar large intentional foraminal enlargement (LIFE) to treat different teeth
AF, apical foramen.
Table 2 Scores and features of the pain
Table 3 Demographic data
Table 4 Postoperative pain considering time and age, gender, periradicular status, and tooth type
*Value obtained from Kruskal-Wallis test; †Value obtained from Mann-Whitney
Table 5 Postoperative pain considering time frame
*Value obtained by Friedman's multiple 2 to 2 comparisons test.
Table 6 Postoperative pain considering sealer extrusion
*Value obtained from Mann-Whitney

