
Articles
- Page Path
- HOME > Restor Dent Endod > Volume 44(1); 2019 > Article
- Research Article The push-out bond strength of BIOfactor mineral trioxide aggregate, a novel root repair material
-
Makbule Bilge Akbulut
 , Durmus Alperen Bozkurt, Arslan Terlemez, Melek Akman
, Durmus Alperen Bozkurt, Arslan Terlemez, Melek Akman -
Restor Dent Endod 2019;44(1):e5.
DOI: https://doi.org/10.5395/rde.2019.44.e5
Published online: January 28, 2019
Department of Endodontics, Faculty of Dentistry, Necmettin Erbakan University, Konya, Turkey.
- Correspondence to Makbule Bilge Akbulut, DDS, PhD. Assistant Professor, Department of Endodontics, Faculty of Dentistry, Necmettin Erbakan University, Ankara Street, Karatay, Konya 42050, Turkey. dt.bilge@yahoo.com
• Received: October 30, 2018 • Revised: January 11, 2019 • Accepted: January 12, 2019
Copyright © 2019. The Korean Academy of Conservative Dentistry
This is an Open Access article distributed under the terms of the Creative Commons Attribution Non-Commercial License (https://creativecommons.org/licenses/by-nc/4.0/) which permits unrestricted non-commercial use, distribution, and reproduction in any medium, provided the original work is properly cited.
- 2,779 Views
- 14 Download
- 25 Crossref
Abstract
-
Objectives The aim of this in vitro study was to evaluate the push-out bond strength of a novel calcium silicate-based root repair material-BIOfactor MTA to root canal dentin in comparison with white MTA-Angelus (Angelus) and Biodentine (Septodont).
-
Materials and Methods The coronal parts of 12 central incisors were removed and the roots were embedded in acrylic resin blocks. Midroot dentin of each sample was horizontally sectioned into 1.1 mm slices and 3 slices were obtained from each root. Three canal-like standardized holes having 1 mm in diameter were created parallel to the root canal on each dentin slice with a diamond bur. The holes were filled with MTA-Angelus, Biodentine, or BIOfactor MTA. Wet gauze was placed over the specimens and samples were stored in an incubator at 37°C for 7 days to allow complete setting. Then samples were subjected to the push-out test method using a universal test machine with the loading speed of 1 mm/min. Data was statistically analyzed using Friedman test and post hoc Wilcoxon signed rank test with Bonferroni correction.
-
Results There were no significant differences among the push-out bond strength values of MTA-Angelus, Biodentine, and BIOfactor MTA (p > 0.017). Most of the specimens exhibited cohesive failure in all groups, with the highest rate found in Biodentine group.
-
Conclusions Based on the results of this study, MTA-Angelus, Biodentine, and BIOfactor MTA showed similar resistances to the push-out testing.
INTRODUCTION
Root perforations due to mechanical, iatrogenic, or pathological causes can increase the failure risk of endodontic treatment, and they can even result in the extraction of the affected tooth. A greater than 70% success rate can be achieved by repairing a tooth nonsurgically with a variety of repair materials [1]. Additionally, the perforation repair treatment time and the size and location of the perforation are crucial factors that influence the treatment success rate [2]. Moreover, a good seal at the perforated site with a biocompatible root repair material can help maintain the health of the periodontal tissues [3].
Calcium silicate-based materials, with their many favorable properties, have become preferable for perforation repair. The traditional mineral trioxide aggregate (MTA), which is composed mainly of tricalcium silicate, dicalcium silicate, and bismuth oxide, has many advantages, including its biocompatibility, hard tissue induction capacity, and good sealing. However, MTA also has some major drawbacks, such as its long setting time, difficult handling characteristics, high cost, and tooth discoloration [4]. MTA-Angelus (Angelus Indústria de Produtos Odontológicos S/A, Londrina, PR, Brazil) is a commercial brand of MTA and has some advantages over ProRoot MTA (Dentsply Tulsa Dental, Tulsa, OK, USA) which is the first commercially available product of MTA. MTA-Angelus has been reported to be more economical than ProRoot MTA [5]. Additionally, the manufacturer of MTA-Angelus claims that this material has a setting time of 15 minutes which is shorter than ProRoot MTA's. However, other clinical problems like handling properties and tooth discoloration effects are still associated with clinical use of MTA-Angelus. The handling property of white MTA-Angelus has been reported to be grainy and sandy, making delivery to perforation cite and compacting difficult [6]. Furthermore, the teeth filled with white MTA-Angelus revealed a grayish discoloration with evident dentin staining due to bismuth oxide content [7].
Biodentine (Septodont, St-Maur-des-fosses, France), a dentin substitute, is composed primarily of tricalcium silicate, dicalcium silicate, calcium carbonate, and zirconium oxide [8]. It has been shown to have good biocompatibility and bioactivity, while the improved handling characteristics and reduced setting time make Biodentine a promising alternative to MTA.
A new type of MTA, called BIOfactor MTA (Imicryl Dental, Konya, Turkey) has recently been introduced for pulp capping, pulpotomies, apexification, root perforation repairs, root end filling, and apical plug procedures. The BIOfactor MTA powder is composed of tricalcium and dicalcium silicate, tricalcium aluminate, and ytterbium oxide as a radiopacifier agent. The liquid consists of 0.5%–3% hydrosoluble carboxylated polymer and demineralized water. This cement can be prepared in a flowing or thick consistency, based on the treatment type. The manufacturer claims that BIOfactor MTA has a finer powder for faster hydration, easier handling properties, stronger sealing, and a shorter setting time, and that it does not cause tooth discoloration. Additionally, BIOfactor MTA seems to be a lower costing product.
Calcium silicate-based materials can be exposed to masticatory or dislocating forces during the cement condensation period of a perforation repair. Thus, resistance to these dislocating forces and the marginal adaptation with dentin are crucial factors for the success of various endodontic procedures [9]. The bond strength of the cement to the dentin can be assessed by using a push-out test. Therefore, the objective of this in vitro study was to evaluate the push-out bond strength of a novel calcium silicate-based root repair material (BIOfactor MTA) to the root canal dentin and compare it with the more contemporary calcium silicate-based materials (white MTA-Angelus and Biodentine).
MATERIALS AND METHODS
According to a previous study [10], sample size was calculated based on effect size = 0.30, power b = 95%, and α = 5% input into an F-test family for analysis of variance repeated measures (G*Power 3.1 for Windows) and 27 samples were required to perform this study. However, 36 samples were included in order to account for possible exclusions like premature failure.
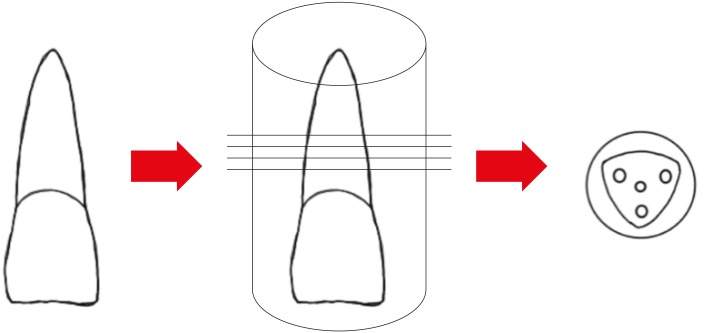
This study was approved by the Human Ethics Committee of the Institutional Review Board (protocol No. 2018/06). The study included 12 maxillary central incisors extracted for periodontal reasons. Teeth with dentin defects, previous endodontic treatment, calcification, internal resorption, or immature apexes were excluded from the study. The teeth were disinfected with a 2.5% sodium hypochlorite (NaOCl) solution and they were stored in distilled water until further processing. The apexes of the teeth were fixed on sticky wax; then, the teeth were embedded in self-curing acrylic resin. The upper middle third of each root was sectioned into 1.1 mm slices under water cooling, and three slices were obtained from each root (Figure 1). In total, 36 root slices underwent further processing.
The methodological set-up was adopted from a recent study, with minor modifications [10]. Briefly, three canal-like standardized holes of 1 mm in diameter were created parallel to the root canal in each dentin slice using a diamond bur. The holes were located at the corners of the triangular-shaped slices, and they were 1 mm from root canal lumen. The root slices were immersed in 2.5% NaOCl for 15 minutes, in 17% ethylenediaminetetraacetic acid for 3 minutes, and in 2.5% NaOCl for 1 minutes to remove the smear layer. Finally, they were rinsed with distilled water for 5 minutes to remove any solution remnants. The holes were dried with paper points, and dentin slices were placed on a glass slab and each cavity was filled with one of the test materials (MTA-Angelus, Biodentine, or BIOfactor MTA). The root repair materials were prepared according to each manufacturer's instructions (Table 1). For the BIOfactor MTA samples, 3 scoops of powder were mixed with 1 drop of liquid. Wet gauze was placed over the specimens, and the samples were stored in an incubator at 37°C for 7 days in order to allow complete setting.
Table 1
Compositions of tested root repair materials and instructions for use according to manufacturer
The samples were subjected to push-out testing using a universal testing machine (Devotrans Quality Control Test Equipment, Istanbul, Turkey) with a 0.6 mm in diameter cylindrical stainless-steel plunger tip and a loading speed of 1 mm/min until dislocation occurred. The maximum load applied for dislodging the cement was recorded in newtons (N) and transformed to megapascals (MPa) by dividing the load by the adhesion surface area of the root repair material. The bonded area was calculated using the following formula: 2 × π × r × h, where r is the root canal radius, h is the thickness of the root dentin slice in millimeters, and π is fixed at 3.14 [11].
After the push-out testing, the samples were examined under a stereomicroscope (SZTP; Olympus Optical Co., Tokyo, Japan) at ×25 magnification in order to evaluate the following failure modes: adhesive failure at the dentin-material interface, cohesive failure within the material, or mixed failure (a combination of adhesive and cohesive failures).
Two dentin slices were selected for the scanning electron microscopy (SEM) evaluation. After the push-out testing, the samples were air dried overnight at room temperature, and then they were sputter coated with gold/palladium for 3 minutes. The specimens were examined particularly with the intention to observe the interface between dentin and the root repair material. The observations were conducted using SEM (Hitachi SU-1510; Hitachi High-Technologies Corp., Tokyo, Japan) under 20 kV and 50× magnification.
Measurable push-out values could not be obtained from six of the specimens due to premature failure; therefore, only 30 specimens were involved in the statistical analyses. IBM SPSS Statistics for Windows version 22.0 (IBM Corp., Armonk, NY, USA) was used to analyze the results. The Shapiro-Wilks test indicated that the data was not normally distributed; therefore, a nonparametric Friedman analysis of variance was performed to compare the push-out values of the paired materials. The significance level was set at p < 0.05. Wilcoxon signed rank test with Bonferroni correction was performed as a post hoc test if the variance analysis test result was significant [12]. The level of statistical significance was set at p < 0.017 (0.05/3) after Bonferroni adjustment.
RESULTS
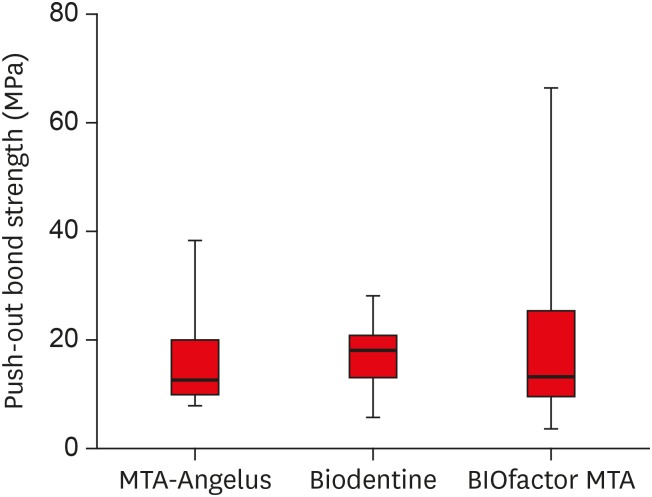
No statistically significant differences in the push-out bond strength were found between the three groups of materials (p > 0.017). The mean and standard deviation of push-out bond strength value was 15.77 ± 8.22 MPa for MTA-Angelus, 17.55 ± 5.67 MPa for Biodentine, and 18.24 ± 13.19 MPa for BIOfactor MTA (Figure 2).
Under the stereomicroscope, all of the groups showed cohesive failure majorities rather than mixed failures (Table 2 and Figure 3A). An adhesive failure was observed in only one specimen in the MTA-Angelus group.
Table 2
Failure mode distribution after the push-out test for root repair materials
| Failure type | MTA-Angelus | Biodentine | BIOfactor MTA |
|---|---|---|---|
| Adhesive | 1 (3.3) | 0 (0) | 0 (0) |
| Cohesive | 27 (90.0) | 29 (96.6) | 24 (80.0) |
| Mixed | 2 (6.6) | 1 (3.3) | 6 (20.0) |
Figure 3
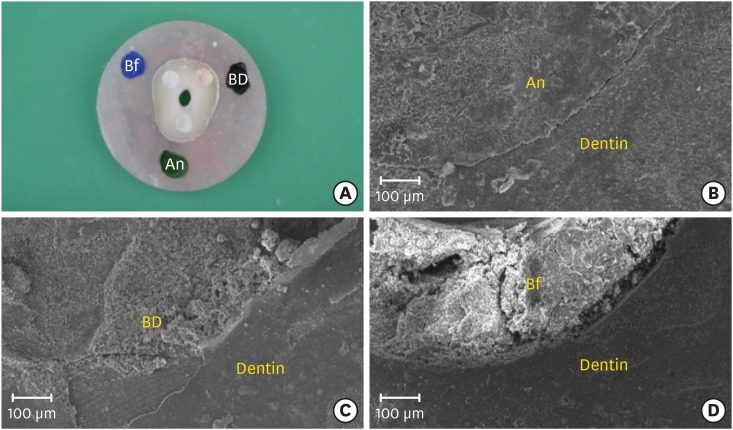
(A) Cohesive failure modes in randomly selected dentin disc (original magnification, ×25) and (B-D) representative scanning electron micrographs of root repair material-dentin interface after push-out testing; (B) MTA-Angelus (An), (C) Biodentine (BD), and (D) BIOfactor MTA (Bf) (original magnification, ×50).
Representative scanning electron microscopic images of root repair material–dentin interfaces were shown in Figure 3. After the push-out testing, no signs of debonding was observed at the MTA-Angelus/dentin (Figure 3B) and Biodentine/dentin interfaces (Figure 3C), indicating good adaptation of the materials. However, few interfacial gaps could be seen between dentin and BIOfactor MTA (Figure 3D).
DISCUSSION
The perforation repair material's adhesion to the root dentin is one of the major requirements of a repair, because providing a good seal maintains the integrity of the filling material-dentin interface, increasing the overall success rate of an endodontic treatment. However, the type of material can directly affect the quality of the dentin bonding. Therefore, this study was designed to evaluate and compare the bond strengths of three different calcium silicate-based materials used for perforation repairs.
In the present study, push-out testing was used to evaluate each calcium silicate-based material's resistance to dislocating forces. Previously, the push-out testing method has been shown to be efficient, reliable, and practical [13]. Furthermore, push-out testing exhibits certain advantages, including the fact that it more closely simulates clinical stress, permits accurate specimen standardization, and produces purer shear forces [14,15]. An innovative modification of the push-out test that was first presented by Scelza et al. [10] was chosen for this study. Because of its morphological and physical variations, human dentin is a complex bonding substrate [16], and thus, many variables related to the dentin substrate could alter the bond strength values. This new set-up enabled us to produce more reliable baseline values using the same dentin sample, while the confounding factors, such as the tooth age, mineralization, hardness, and elastic modulus, could be controlled better [10]. Some previous researches have applied this new methodology for testing root canal sealers and they have reported the reliability of this new set-up [17,18]. Other studies have also confirmed the usefulness of this method on determining push-out bond strength of calcium silicate-based cements [19,20].
The size of the cylindrical plunger used in the studies was adjusted to be closest fitting without touching the canal walls and mostly 3 sizes between 0.4 and 1.2 mm, usually in increasing increments of 0.2 mm were chosen [21]. As the hole diameter was 1 mm in the present study, 0.6 mm sized plunger was preferred. A previous study has investigated the effect of plunger diameter on push-out bond strength of different root filing materials and it has been showed that different plunger: canal size ratios (50%–83% of canal diameter) did not significantly affect the push-out bond strength [22]. More recent research has revealed lower push-out bond strength values when the plunger size was approximately 50% of the canal diameter [23]. According to these previous researches, the plunger size used in this study (60% of canal diameter) appears not to affect the push-out bond strength values. Additionally, 0.6 mm sized plunger could be easily positioned without contacting the dentin and maintained centralized.
The results of the present study indicated similar bond strength values for the MTA-Angelus, Biodentine, and BIOfactor MTA. Our findings are in agreement with previous research that revealed no significant differences between the bond strengths of the MTA-Angelus and Biodentine [24]. The similarities in the bond strengths among these calcium-silicate based materials may be due to the similarities in their basic composition, according to the manufacturers’ information. However, Biodentine's higher resistance to dislodgement has been demonstrated previously [10], and it could be attributed to Biodentine's high biomineralization ability. This may have caused the uptake of calcium and silicon ions into the dentin, leading to the formation of tag-like structures [25] and increasing the material's adaptation to the dentin. Besides, MTA-Angelus has been shown to release high levels of calcium [26]. This higher calcium ion release may lead to more calcium phosphate precipitates and tag-like structures, resulting in high dislodgement resistance.
The BIOfactor MTA displayed at least as high of a bond strength as the MTA-Angelus and Biodentine. The finer Biodentine and BIOfactor MTA particles could have contributed the formation of the tag-like microstructure, thus improving the cement's penetration into the dentin tubules and providing better micromechanical adhesion [27]. Unlike other calcium silicate-based materials, ytterbium oxide was added to the BIOfactor MTA as a radiopacifier agent. The effects of the addition of ytterbium oxide to the calcium silicate-based material on the material's physicochemical properties are unknown. However, ytterbium trifluoride has been incorporated into calcium silicate-based materials, and it was determined that the ytterbium trifluoride slightly increased the compressive strength of the portland cement, while enhancing the porosity of the material [28]. Further studies are required to determine whether the substitution of ytterbium oxide could affect the chemical bonding of the BIOfactor MTA to the dentin. Moreover, another BIOfactor MTA constituent, tricalcium aluminate, has been reported to be the most reactive component of portland cement [29]. Although tricalcium aluminate reacts vigorously with water, its contribution to the strength is minimal [29].
Our findings demonstrated that the bond failures observed in all the experimental groups were predominantly within the material (cohesive failure). These results are in accordance with a previous study that reported that the calcium silicate-dentin bond failures were usually cohesive [30]. The cohesive mode of fracture indicates that the bonding of these calcium silicate-based materials to the dentin was stronger than the cohesive strength of the materials. The cohesive failure percentage in the Biodentine group was the highest in our study, and previous studies have shown that the Biodentine-dentin bond failures were predominantly cohesive [31,32,33]. However, there are conflicting results for the MTA-Angelus; some previous studies reported adhesive failures [31,34], while other revealed mixed failures [24]. The differences in the MTA-Angelus failure modes could be attributed to the new methodological design used in the present study or different storage conditions. Incidentally, the BIOfactor MTA bond failure mode has not been determined in any other studies. Overall, the tubule penetration and micromechanical anchorage, which improve the retention of the material to the dentin, could explain the cohesive failure majorities in all of the groups [34].
One of the limitations of this in vitro study was that the samples were incubated in a moist environment for seven days before the push-out testing. However, in clinical conditions, the bond strengths of the perforation repair materials would be influenced by contamination with blood, irrigation solutions (including mostly NaOCl), and an acidic environment. Therefore, further long-term studies are suggested to evaluate the effects of both ageing and unavoidable environmental factors during setting on novel calcium silicate-based cements.
CONCLUSIONS
Within the limitations of this in vitro study, the MTA-Angelus, Biodentine, and BIOfactor MTA exhibited similar resistances to the push-out testing. All of the materials showed predominantly cohesive failures, with the highest rate found in the Biodentine samples. Overall, the BIOfactor MTA seemed appropriate for use as a root repair material with regard to its bond strength; however, its other characteristics, including its biocompatibility, bioactivity, and physicochemical properties, should be investigated further.
ACKNOWLEDGEMENTS
The authors thank Imicryl Dental (Konya, Turkey) and Gulsa Tibbi Cihazlar ve Malzeme Sanayi Ticaret (Izmir, Turkey) for the donation of some of the materials used in this project. This study was presented at TDB 24th International Dental Congress in Ankara, Turkey (September/2018). The authors deny any conflicts of interest related to this study.
-
Conflict of Interest: No potential conflict of interest relevant to this article was reported.
-
Author Contributions:
Conceptualization: Akbulut MB, Terlemez A.
Data curation: Akbulut MB, Bozkurt DA, Terlemez A.
Formal analysis: Bozkurt DA, Terlemez A.
Funding acquisition: Akman M.
Investigation: Akbulut MB, Bozkurt DA, Terlemez A, Akman M.
Methodology: Akbulut MB, Bozkurt DA, Terlemez A, Akman M.
Project administration: Akbulut MB.
Resources: Akbulut MB.
Software: Akman M.
Supervision: Akbulut MB, Akman M.
Validation: Bozkurt DA, Terlemez A, Akman M.
Visualization: Akbulut MB.
Writing - original draft: Akbulut MB.
Writing - review & editing: Akbulut MB, Bozkurt DA, Terlemez A, Akman M.
- 1. Siew K, Lee AH, Cheung GS. Treatment outcome of repaired root perforation: a systematic review and meta-analysis. J Endod 2015;41:1795-1804.ArticlePubMed
- 2. Fuss Z, Trope M. Root perforations: classification and treatment choices based on prognostic factors. Endod Dent Traumatol 1996;12:255-264.ArticlePubMed
- 3. Clauder T, Shin SJ. Repair of perforations with MTA: clinical applications and mechanisms of action. Endod Topics 2006;15:32-55.Article
- 4. Parirokh M, Torabinejad M. Mineral trioxide aggregate: a comprehensive literature review--Part I: chemical, physical, and antibacterial properties. J Endod 2010;36:16-27.ArticlePubMed
- 5. Srinivasan V, Waterhouse P, Whitworth J. Mineral trioxide aggregate in paediatric dentistry. Int J Paediatr Dent 2009;19:34-47.ArticlePubMed
- 6. Butt N, Talwar S, Chaudhry S, Nawal RR, Yadav S, Bali A. Comparison of physical and mechanical properties of mineral trioxide aggregate and Biodentine. Indian J Dent Res 2014;25:692-697.ArticlePubMed
- 7. Marciano MA, Costa RM, Camilleri J, Mondelli RF, Guimarães BM, Duarte MA. Assessment of color stability of white mineral trioxide aggregate angelus and bismuth oxide in contact with tooth structure. J Endod 2014;40:1235-1240.ArticlePubMed
- 8. Camilleri J. Investigation of Biodentine as dentine replacement material. J Dent 2013;41:600-610.ArticlePubMed
- 9. Reyes-Carmona JF, Felippe MS, Felippe WT. The biomineralization ability of mineral trioxide aggregate and Portland cement on dentin enhances the push-out strength. J Endod 2010;36:286-291.ArticlePubMed
- 10. Scelza MZ, da Silva D, Scelza P, de Noronha F, Barbosa IB, Souza E, De Deus G. Influence of a new push-out test method on the bond strength of three resin-based sealers. Int Endod J 2015;48:801-806.ArticlePubMed
- 11. Skidmore LJ, Berzins DW, Bahcall JK. An in vitro comparison of the intraradicular dentin bond strength of Resilon and gutta-percha. J Endod 2006;32:963-966.ArticlePubMed
- 12. Kim HY. Statistical notes for clinical researchers: nonparametric statistical methods: 2. Nonparametric methods for comparing three or more groups and repeated measures. Restor Dent Endod 2014;39:329-332.ArticlePubMedPMC
- 13. Goracci C, Tavares AU, Fabianelli A, Monticelli F, Raffaelli O, Cardoso PC, Tay F, Ferrari M. The adhesion between fiber posts and root canal walls: comparison between microtensile and push-out bond strength measurements. Eur J Oral Sci 2004;112:353-361.ArticlePubMed
- 14. Drummond JL, Sakaguchi RL, Racean DC, Wozny J, Steinberg AD. Testing mode and surface treatment effects on dentin bonding. J Biomed Mater Res 1996;32:533-541.ArticlePubMed
- 15. Sousa-Neto MD, Silva Coelho FI, Marchesan MA, Alfredo E, Silva-Sousa YT. Ex vivo study of the adhesion of an epoxy-based sealer to human dentine submitted to irradiation with Er : YAG and Nd : YAG lasers. Int Endod J 2005;38:866-870.ArticlePubMed
- 16. Perdigão J. Dentin bonding-variables related to the clinical situation and the substrate treatment. Dent Mater 2010;26:e24-e37.ArticlePubMed
- 17. Carvalho NK, Prado MC, Senna PM, Neves AA, Souza EM, Fidel SR, Sassone LM, Silva EJ. Do smear-layer removal agents affect the push-out bond strength of calcium silicate-based endodontic sealers? Int Endod J 2017;50:612-619.ArticlePubMedPDF
- 18. Silva EJ, Carvalho NK, Prado MC, Zanon M, Senna PM, Souza EM, De-Deus G. Push-out bond strength of injectable pozzolan-based root canal sealer. J Endod 2016;42:1656-1659.ArticlePubMed
- 19. Silva EJ, Carvalho NK, Guberman MR, Prado M, Senna PM, Souza EM, De-Deus G. Push-out bond strength of fast-setting mineral trioxide aggregate and pozzolan-based cements: ENDOCEM MTA and ENDOCEM Zr. J Endod 2017;43:801-804.ArticlePubMed
- 20. Silva EJ, Carvalho NK, Zanon M, Senna PM, DE-Deus G, Zuolo ML, Zaia AA. Push-out bond strength of MTA HP, a new high-plasticity calcium silicate-based cement. Braz Oral Res 2016;30:e84.Article
- 21. Brichko J, Burrow MF, Parashos P. Design variability of the push-out bond test in endodontic research: a systematic review. J Endod 2018;44:1237-1245.ArticlePubMed
- 22. Nagas E, Uyanik O, Durmaz V, Cehreli ZC. Effect of plunger diameter on the push-out bond values of different root filling materials. Int Endod J 2011;44:950-955.ArticlePubMed
- 23. Pane ES, Palamara JE, Messer HH. Critical evaluation of the push-out test for root canal filling materials. J Endod 2013;39:669-673.ArticlePubMed
- 24. Stefaneli Marques JH, Silva-Sousa YT, Rached-Júnior FJ, Macedo LM, Mazzi-Chaves JF, Camilleri J, Sousa-Neto MD. Push-out bond strength of different tricalcium silicate-based filling materials to root dentin. Braz Oral Res 2018;32:e18.PubMed
- 25. Han L, Okiji T. Uptake of calcium and silicon released from calcium silicate-based endodontic materials into root canal dentine. Int Endod J 2011;44:1081-1087.ArticlePubMed
- 26. Duarte MA, Demarchi AC, Yamashita JC, Kuga MC, Fraga SC. pH and calcium ion release of 2 root-end filling materials. Oral Surg Oral Med Oral Pathol Oral Radiol Endod 2003;95:345-347.ArticlePubMed
- 27. Atmeh AR, Chong EZ, Richard G, Festy F, Watson TF. Dentin-cement interfacial interaction: calcium silicates and polyalkenoates. J Dent Res 2012;91:454-459.ArticlePubMedPMCPDF
- 28. Antonijevic D, Medigovic I, Zrilic M, Jokic B, Vukovic Z, Todorovic L. The influence of different radiopacifying agents on the radiopacity, compressive strength, setting time, and porosity of Portland cement. Clin Oral Investig 2014;18:1597-1604.ArticlePubMedPDF
- 29. Bye GC. Portland cement: composition, production and properties. 2nd ed. London: Thomas Telford; 1999.
- 30. Alsubait SA. Effect of sodium hypochlorite on push-out bond strength of four calcium silicate-based endodontic materials when used for repairing perforations on human dentin: an in vitro evaluation. J Contemp Dent Pract 2017;18:289-294.ArticlePubMed
- 31. Dawood AE, Manton DJ, Parashos P, Wong RH, Palamara JE, Reynolds EC. Push-out bond strength of CPP-ACP-modified calcium silicate-based cements. Dent Mater J 2015;34:490-494.ArticlePubMed
- 32. Guneser MB, Akbulut MB, Eldeniz AU. Effect of various endodontic irrigants on the push-out bond strength of Biodentine and conventional root perforation repair materials. J Endod 2013;39:380-384.ArticlePubMed
- 33. Kadić S, Baraba A, Miletić I, Ionescu A, Brambilla E, Ivanišević Malčić A, Gabrić D. Push-out bond strength of three different calcium silicate-based root-end filling materials after ultrasonic retrograde cavity preparation. Clin Oral Investig 2018;22:1559-1565.ArticlePubMedPDF
- 34. Saghiri MA, Garcia-Godoy F, Gutmann JL, Lotfi M, Asatourian A, Ahmadi H. Push-out bond strength of a nano-modified mineral trioxide aggregate. Dent Traumatol 2013;29:323-327.ArticlePubMed
REFERENCES
Tables & Figures
REFERENCES
Citations
Citations to this article as recorded by 
- Evaluation of marginal adaptation and bond strength of apical root canal plugs using different bioceramic cements
Michel Sena Fernandes Faria Lima, Alberto Nogueira da Gama Antunes, Kênia Maria Pereira Soares de Toubes, Fábio Fernandes Borém Bruzinga, Camila de Sousa Caneschi, Luís Fernando dos Santos Alves Morgan, Frank Ferreira Silveira
BMC Oral Health.2026;[Epub] CrossRef - Examination of the Bond Strength of Retrograde Filling in Teeth with Failed Apical Resection After Retreatment
Sevda Tok, Leyla Benan Ayranci
Applied Sciences.2025; 15(7): 3441. CrossRef - Comparative Analysis of Physicocomechanical Properties of MTA and Biodentine with Addition of Graphene Oxide to MTA and Biodentine: An In-vitro Study
Tanvi Arvind Jagtap, Budhabhushan A. Sonvane, Guruprasad Handal, Jayashri Nimba Bhangare, Kedar Vilas Saraf, Abhishek Mulay
Journal of Pharmacy and Bioallied Sciences.2025; 17(Suppl 1): S608. CrossRef - Influence of Incubation Duration on Bond Strength and Microhardness of Calcium Silicate‐Based Materials
Emine Şimşek, Makbule Bilge Akbulut
Australian Endodontic Journal.2025; 51(2): 438. CrossRef - Comparative evaluation of push-out bond strength after root perforation repair using recently introduced bioceramic and calcium silicate-based materials – An in vitro study
Gurinder Kaur, Deepak Kurup, Deepyanti Dubey, Ajit Hindlekar, Ganesh Ranganath Jadhav, Priya Mittal, Siddharth Shinde
Endodontology.2025; 37(2): 194. CrossRef - Comparative Evaluation of Push-out Bond Strength of Conventional Mineral Trioxide Aggregate, Biodentine, and Two Novel Antibacterial-enhanced Mineral Trioxide Aggregates
Sanjeev Khanagar, Suman Panda, Prabhadevi C Maganur, Ganesh Jeevanandan, Satish Vishwanathaiah, Ather A Syed, Sara Kalagi, Arokia RS Merlin, Vignesh Ravindran, Aram AlShehri
The Journal of Contemporary Dental Practice.2024; 25(2): 168. CrossRef - Influence of Phase Composition and Morphology on the Calcium Ion Release of Several Classical and Hybrid Endodontic Cements
Ivanka Dimitrova, Galia Gentscheva, Ivanka Spassova, Daniela Kovacheva
Materials.2024; 17(22): 5568. CrossRef - The Effect of Two Different MTA (Mineral Trioxide Aggregate) On Thermal Insulation
Gizem Akkus, Ecem Salmaz, Didem Oner Ozdas
The Open Dentistry Journal.2024;[Epub] CrossRef - Comparison of push‐out bond strength and apical microleakage of different calcium silicate‐based cements after using EDTA, chitosan and phytic acid irrigations
Tutku Koçak Şahin, Murat Ünal
Microscopy Research and Technique.2024; 87(9): 2072. CrossRef - In vitro evaluation of the physical characteristics and push-out bond strength of new experimental nano-MTA
Nada Omar, Yousra Aly, Haidy N. Salem
Bulletin of the National Research Centre.2024;[Epub] CrossRef - Interfacial characteristics of BIOfactor MTA and Biodentine with dentin
Makbule Bilge Akbulut, Şeref Nur Mutlu, Mehmet Ali Soylu, Emine Şimşek
Microscopy Research and Technique.2023; 86(2): 258. CrossRef - Systemic effect of calcium silicate-based cements with different radiopacifiers-histopathological analysis in rats
Osman Ataş, Kubra Bılge, Semsettin Yıldız, Serkan Dundar, Ilknur Calik, Asime Gezer Ataş, Alihan Bozoglan
PeerJ.2023; 11: e15376. CrossRef - The push-out bond strength of three root canal materials used in primary teeth: in vitro study
Hazal Özer, Merve Abaklı İnci, Sevcihan Açar Tuzluca
Frontiers in Dental Medicine.2023;[Epub] CrossRef - Effects of different irrigation protocols on push-out bond strength of pre-mixed calcium silicate-based cements
Sabiha Ceren İlisulu, Aliye Tugce Gürcan, Soner Sismanoglu
Journal of the Australian Ceramic Society.2023; 59(5): 1381. CrossRef - Micro-Computed Tomographic Evaluation of the Sealing Quality and Bond Strength of Different MTA Apical Plugs
Taibe Tokgöz Kaplan, Murat Selim Botsalı
European Journal of Therapeutics.2023; 30(1): 29. CrossRef - Kan kontaminasyonunun farklı kök ucu dolgu materyallerinin dentine bağlanma dayanımına etkisi
Şeyma Nur GERÇEKCİOĞLU, Melike BAYRAM, Emre BAYRAM
Acta Odontologica Turcica.2023; 40(1): 9. CrossRef - Tooth Discoloration Effect of BIOfactor Mineral Trioxide Aggregate: A 6-Month In Vitro Study
Şeref Nur Mutlu, Makbule Bilge Akbulut
Applied Sciences.2023; 13(15): 8914. CrossRef - Comparative Evaluation of the Push-Out Bond Strength of Root-End Filling Materials by Using Different Condensation Methods
Pelin Tüfenkçi, Sevinç Sevgi, Ayşenur Öncü, Fatma Semra Sevimay, Berkan Çelikten
Cyprus Journal of Medical Sciences.2022; 7(7): 115. CrossRef - Effect of Different Adhesive Strategies on the Microshear Bond Strength of Calcium-Silicate-Based Materials
Aliye Tuğçe Gürcan, Soner Şişmanoğlu, Görkem Sengez
Journal of Advanced Oral Research.2022; 13(2): 191. CrossRef - BIOfactor MTA’nın Radyoopasitesinin Dijital Radyografi ile Değerlendirilmesi
Şeref Nur MUTLU, Makbule Bilge AKBULUT
Selcuk Dental Journal.2022; 9(2): 520. CrossRef - Morphological and Chemical Analysis of Different Types of Calcium Silicate‐Based Cements
Okba Mahmoud, Nashwan Abdullah Al-Afifi, Mohideen Salihu Farook, Maysara Adnan Ibrahim, Saaid Al Shehadat, Mohammed Amjed Alsaegh, Sandrine Bittencourt Berger
International Journal of Dentistry.2022;[Epub] CrossRef - Influence of Blood Contamination on Push-Out Bond Strength of Three Calcium Silicate-Based Materials to Root Dentin
Cristina Rodrigues Paulo, Joana A. Marques, Diana B. Sequeira, Patrícia Diogo, Rui Paiva, Paulo J. Palma, João Miguel Santos
Applied Sciences.2021; 11(15): 6849. CrossRef - An In vitro comparative evaluation of effect of novel irrigant Qmix and 17% ethylenediaminetetraacetic acid on the push-out bond strength of biodentine and endosequence bioceramic root repair material
VandanaJ Gade, Aparajita Gangrade, JaykumarR Gade, Neelam Rahul
Journal of the International Clinical Dental Research Organization.2021; 13(2): 124. CrossRef - A micro-computed tomographic study using a novel test model to assess the filling ability and volumetric changes of bioceramic root repair materials
Fernanda Ferrari Esteves Torres, Jader Camilo Pinto, Gabriella Oliveira Figueira, Juliane Maria Guerreiro-Tanomaru, Mario Tanomaru-Filho
Restorative Dentistry & Endodontics.2021;[Epub] CrossRef - Micro-computed tomographic evaluation of the flow and filling ability of endodontic materials using different test models
Fernanda Ferrari Esteves Torres, Juliane Maria Guerreiro-Tanomaru, Gisselle Moraima Chavez-Andrade, Jader Camilo Pinto, Fábio Luiz Camargo Villela Berbert, Mario Tanomaru-Filho
Restorative Dentistry & Endodontics.2020;[Epub] CrossRef
 ePub Link
ePub Link Cite
CiteThe push-out bond strength of BIOfactor mineral trioxide aggregate, a novel root repair material
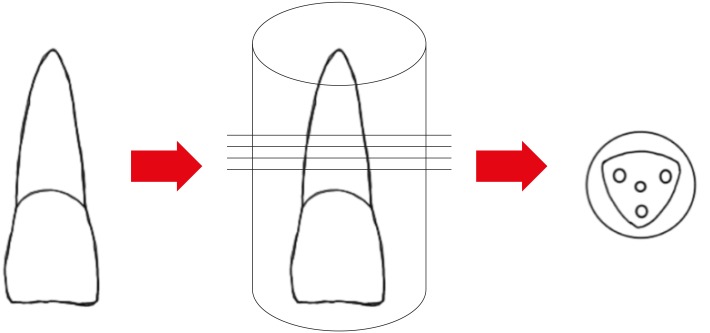

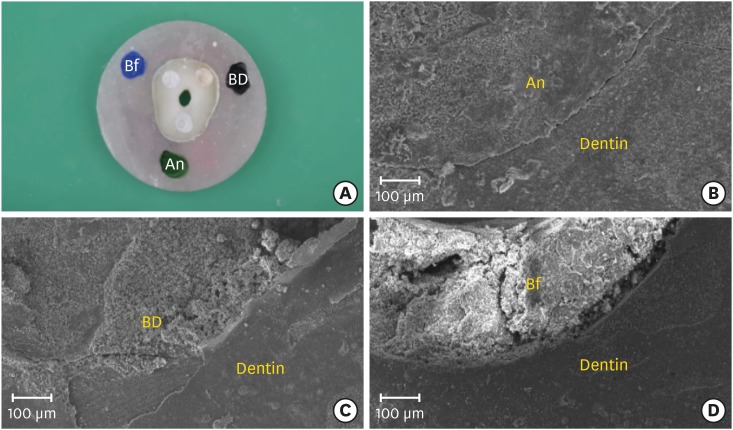
Figure 1 Schematic illustration of experimental design.
Figure 2 Push-out bond strength values for MTA-Angelus, Biodentine, and BIOfactor MTA.
Figure 3 (A) Cohesive failure modes in randomly selected dentin disc (original magnification, ×25) and (B-D) representative scanning electron micrographs of root repair material-dentin interface after push-out testing; (B) MTA-Angelus (An), (C) Biodentine (BD), and (D) BIOfactor MTA (Bf) (original magnification, ×50).
Figure 1
Figure 2
Figure 3
The push-out bond strength of BIOfactor mineral trioxide aggregate, a novel root repair material
Compositions of tested root repair materials and instructions for use according to manufacturer
| Product and manufacturer | Composition | Instructions for use |
|---|---|---|
| MTA-Angelus (Angelus Industria de Produtos Odontologicos, Londrina, Brazil) | Powder: tricalcium silicate, dicalcium silicate, tricalcium aluminate, calcium oxide, bismuth oxide | Mix 1 scoop of powder with 1 drop of distilled water for 30 seconds |
| Liquid: distilled water | ||
| Biodentine (Septodont, St-Maur-des-fosses, France) | Powder: tricalcium silicate, dicalcium silicate, calcium carbonate, calcium oxide, zirconium oxide as a radiopacifier | Mix 1 capsule of powder with 5 drops of liquid for 30 seconds using amalgam mixing machine |
| Liquid: water, calcium chloride, hydrosoluble polymer (plasticizing agent) | ||
| BIOfactor MTA (Imicryl Dental, Konya, Turkey) | Powder: tricalcium silicate, dicalcium silicate, tricalcium aluminate, ytterbium oxide as a radiopacifier | Mix 3 scoops of powder with 1 drop of liquid until having a homogeneous consistency |
| Liquid: 0.5%–3% hydrosoluble carboxylated polymer, demineralized water |
Failure mode distribution after the push-out test for root repair materials
| Failure type | MTA-Angelus | Biodentine | BIOfactor MTA |
|---|---|---|---|
| Adhesive | 1 (3.3) | 0 (0) | 0 (0) |
| Cohesive | 27 (90.0) | 29 (96.6) | 24 (80.0) |
| Mixed | 2 (6.6) | 1 (3.3) | 6 (20.0) |
Values are presented as number (%).
Table 1 Compositions of tested root repair materials and instructions for use according to manufacturer
Table 2 Failure mode distribution after the push-out test for root repair materials
Values are presented as number (%).

