
Articles
- Page Path
- HOME > Restor Dent Endod > Volume 44(1); 2019 > Article
- Research Article Evaluation of the effects of whitening mouth rinses combined with conventional tooth bleaching treatments
-
Jaqueline Costa Favaro1
 , Omar Geha1, Ricardo Danil Guiraldo1, Murilo Baena Lopes1, Andreza Maria Fábio Aranha2, Sandrine Bittencourt Berger1
, Omar Geha1, Ricardo Danil Guiraldo1, Murilo Baena Lopes1, Andreza Maria Fábio Aranha2, Sandrine Bittencourt Berger1 -
Restor Dent Endod 2019;44(1):e6.
DOI: https://doi.org/10.5395/rde.2019.44.e6
Published online: January 30, 2019
1Department of Restorative Dentistry, School of Dentistry, University of North Parana, Londrina, PR, Brazil.
2Department of Dental Sciences, School of Dentistry, University of Cuiabá, Cuiabá, MT, Brazil.
- Correspondence to Sandrine Bittencourt Berger, DDS, MS, PhD. Associate Professor, Department of Restorative Dentistry, School of Dentistry, University of North Parana, Rua Marselha, 183, Londrina, PR 86041-140, Brazil. berger.sandrine@gmail.com
• Received: September 24, 2018 • Revised: December 8, 2018 • Accepted: January 12, 2019
Copyright © 2019. The Korean Academy of Conservative Dentistry
This is an Open Access article distributed under the terms of the Creative Commons Attribution Non-Commercial License (https://creativecommons.org/licenses/by-nc/4.0/) which permits unrestricted non-commercial use, distribution, and reproduction in any medium, provided the original work is properly cited.
- 2,385 Views
- 17 Download
- 10 Crossref
Abstract
-
Objectives The aim of the present study was to evaluate the effect of whitening mouth rinses alone and in combination with conventional whitening treatments on color, microhardness, and surface roughness changes in enamel specimens.
-
Materials and Methods A total of 108 enamel specimens were collected from human third molars and divided into 9 groups (n = 12): 38% hydrogen peroxide (HP), 10% carbamide peroxide (CP), 38% HP + Listerine Whitening (LW), 10% CP + LW, 38% HP + Colgate Plax Whitening (CPW), 10% CP + CPW, LW, CPW, and the control group (CG). The initial color of the specimens was measured, followed by microhardness and roughness tests. Next, the samples were bleached, and their color, microhardness, and roughness were assessed. Data were analyzed through 2-way analysis of variance (ANOVA; microhardness and roughness) and 1-way ANOVA (color change), followed by the Tukey post hoc test. The Dunnett test was used to compare the roughness and microhardness data of the CG to those of the treated groups.
-
Results Statistically significant color change was observed in all groups compared to the CG. All groups, except the LW group, showed statistically significant decreases in microhardness. Roughness showed a statistically significant increase after the treatments, except for the 38% HP group.
-
Conclusions Whitening mouth rinses led to a whitening effect when they were used after conventional treatments; however, this process caused major changes on the surface of the enamel specimens.
INTRODUCTION
The search for ways to combine dental aesthetics and functional features has boosted the development and enhancement of protocols to improve the appearance of teeth [1]. Extrinsic and intrinsic factors, both congenital and acquired, can darken vital and non-vital teeth and compromise smile aesthetics. Intrinsic color changes are often systemic or pulpal; they are caused by pigments incorporated into the tooth structure, enamel and dentin, whereas extrinsic changes result from the deposition of external pigments (such as food, drinks, or chromogenic bacteria) on the tooth surface, or from biofilms [2].
The demand for dental bleaching treatments to correct tooth discoloration has grown considerably. Tooth bleaching is a minimally-invasive, conservative, and efficient option for patients under proper supervision by a dentist [1], and furthermore, it is relatively easy to apply [3]. Haywood and Heymann [3] suggested using 10% carbamide peroxide as a bleaching agent for at-home tooth bleaching because of its safety and effectiveness. As a result, this protocol emerged as the most widely-accepted dental bleaching technique due to its simplicity and rapid effect on tooth color.
There are three protocols available for vital-teeth bleaching, namely: at-home bleaching supervised by a dentist, in-office bleaching, and the treatment with over-the-counter (OTC) products. Supervised at-home treatment involves using 10% carbamide peroxide (CP) for 8 hours on a daily basis for 2 to 6 weeks [3]. In-office bleaching consists in the application of 35% to 40% hydrogen peroxide (HP) for 30 minutes (two 15-minute applications) at 2 or 3 weekly sessions, for as long as necessary [4]. Both protocols are capable of bleaching intrinsic stains [5]. The third bleaching protocol utilizes OTC products, which are sold freely in supermarkets and pharmacies and on the Internet. OTC treatments do not require any professional prescription or supervision [2,4,6,7], because they involve self-application through the use of whitening chewing gum, whitening strips, paint-on films, whitening toothpaste, or whitening mouth rinses. Some of these products, such as whitening mouth rinses [8], contain low concentrations of bleaching agents (3%–6% hydrogen peroxide, on average).
The wide variety of OTC products available on the market and their ease of use can lead consumers to overuse these products, since they can be applied on a daily basis. Sometimes OTC products are used along with conventional bleaching treatments, without dentists being aware that their patients are doing so. Moreover, they can be used during or after the supervised treatments in order to maximize the expected effects [4]. Shorter-duration bleaching treatments and higher application frequencies limit the time the teeth stay in contact with saliva, which can reduce remineralization. This reduction significantly increases the chances of damaging the enamel [9], since bleaching agents trigger morphological changes on the surface of enamel [1,10,11]. Therefore, professionals must pay close attention when choosing a bleaching protocol in order to avoid such changes [12,13].
Given the wide availability of OTC products on the market and the lack of studies of the effects of their use, either alone or in combination with conventional bleaching procedures, this study was conducted to evaluate the bleaching effect of OTCs on color, microhardness, and enamel roughness changes after treatment completion. The null hypotheses to be herein tested are that the combined effect of mouth rinses and conventional bleaching would not promote color change and would not damage the enamel structure.
MATERIALS AND METHODS
The sample size was determined based on microhardness data collected in the study by Berger et al., 2010 [14]. Based on the power analysis, it was determined that at least 9 teeth per group (80%) would be needed to reach a significance level of 0.05.
The present study was approved by the local Ethics Committee (protocol #579.916). A total of 120 human third molars, without cavities or enamel defects, were selected for therapeutic purposes. The specimens were cleaned and stored in 0.5% chloramine T solution for 7 days after extraction, and then stored in distilled water at 4°C until the experiment.
Enamel specimens were collected from the buccal surface of each tooth (7 mm width × 4 mm thickness × 7 mm height). The enamel specimens were fixed with wax on acrylic discs. The enamel surfaces were abraded with 600, 1,200, and 2,000 grit silicon carbide paper, and polished with abrasive paper and 1 µm diamond paste in electric polisher (Arotec S/A Ind. e Comércio, Cotia, SP, Brazil). The specimens were subjected to an ultrasonic bath in deionized water for 10 minutes (Ultrasonic Cleaner, Odontobras, Ribeirão Preto, SP, Brazil) to remove debris. The prepared specimens were examined under a stereomicroscope (Bel Photonics STM Pro, Bel Microimage Analyzer, Monza, Italy) to verify the absence of cracks or other surface defects. The specimens were then stored in deionized water until use to avoid dehydration.
Surface microhardness was determined using a Shimadzu Micro Hardness Tester (HMV-G 21S, Shimadzu Corporation, Kyoto, Japan) equipped with a Knoop-type indenter, adjusted to a static charge of 25 g for 10 seconds, based on Araújo et al. [1]. Three indentations were made 100 μm from each other, moving outwards from the center of the fragments. The means of the three measures were calculated and the results were used to represent the sample. The initial mark indentation was made in the upper left corner, measuring 1,500 μm on the horizontal plane and 1,500 μm on the vertical plane.
The mean hardness of all enamel specimens was calculated, and specimens showing values less than or equal to 10% were excluded from the study. Finally, 108 dental enamel specimens were selected and randomly allocated into 9 experimental groups (n = 12). One-way analysis of variance (ANOVA) was performed to verify whether samples were statistically equivalent at baseline (p > 0.05). Each sample was measured at 2 time points: at the beginning of the study (T0, baseline) and after treatment (T1).
Table 1 shows the experimental groups and the composition of the bleaching agents used in the study. Microhardness (Knoop), color, and surface roughness (Ra) of each enamel sample were evaluated based on the T0 values (i.e., prior to the bleaching treatment).
Table 1
Information about the materials used in the present study
Samples were dried with absorbent paper before the color evaluation. A trained examiner measured the samples under standardized environmental conditions. An acrylic positioner with a 3 mm hole at the center was used to position the specimen under a digital spectrophotometer (Vita Easyshade Advance, Vita Zahnfabrik, Bad Sackingen, Germany). The spectrophotometer was calibrated on a calibration plate after every 3 measurements, according to the manufacturer's recommendations. The following coordinates were recorded for each sample: L*, a*, and b*. L* represented the degree of lightness, which could vary from black (0) to white (100). a* represented the degree of color in the red (+a*) -green (−a*) axis, and b* corresponded to the same variable in the yellow (+b*) -blue (−b*) axis of the samples [15,16,17]. Each sample was measured at 2 time points: at the beginning of the study (T0, baseline) and after treatment (T1). The total color change, or the distance between 2 color coordinates (ΔE), was calculated using the following formula: ΔE* = (ΔL∗)2 + (Δa∗)2 + (Δb∗)]1/2.
Surface roughness (Ra; mean surface roughness) was measured with a profilometer (SJ-410, Mitutoyo, Tokyo, Japan). Three measurements were taken of each sample, in 3 different directions (vertical, horizontal, and transversal), at different time points, with a length of 0.25 mm [18] and a speed of 0.01 mm/sec. Each sample was measured at 2 time points: at the beginning of the study (T0, baseline) and after treatment (T1). The mean values at each time point were calculated and used in the statistical analysis.
Figure 1 shows the study design. The specimens in the single-agent groups (38% hydrogen peroxide [38% HP; Opalescence Boost, Ultradent Products Inc., South Jordan, UT, USA], 10% carbamide peroxide [10% CP; Opalescence 10% PF, Ultradent Products Inc.], Listerine Whitening [LW; Johnson & Johnson do Brasil Indústria e Comércio de Produtos para Saúde Ltda, São Paulo, SP, Brazil], and Colgate Plax Whitening [CPW; Colgate-Palmolive Ind. Ltda., São Paulo, SP, Brazil]) and the combination groups (38% HP + LW, 10% CP + LW, 38% HP + CPW, 10% CP + CPW) were subjected to bleaching procedures according to the recommendations of the manufacturers.
Figure 1
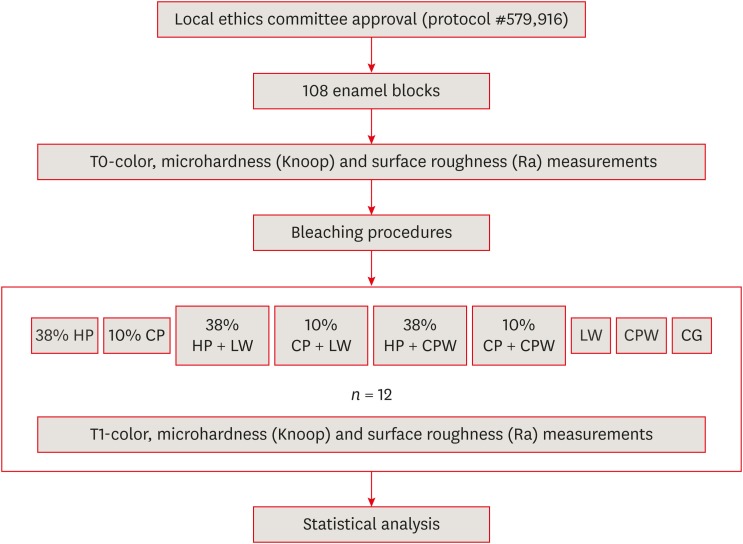
Schematic illustration of the experimental design.
T0, at the beginning of the study (baseline); T1, after bleaching treatment; HP, hydrogen peroxide (38% HP; Opalescence Boost, Ultradent Products Inc., South Jordan, UT, USA); CP, carbamide peroxide (10% CP; Opalescence 10% PF, Ultradent Products Inc.); LW, Listerine Whitening (Johnson & Johnson do Brasil Indústria e Comércio de Produtos para Saúde Ltda, São Paulo, SP, Brazil); CPW, Colgate Plax Whitening (Colgate-Palmolive Ind. Ltda., São Paulo, SP, Brazil); CG, control group.
A 2-mm-thick layer (approximately 0.1 g) of bleaching gel was applied over the surface of specimens in the groups treated with bleaching agents (38% HP and 10% CP) for the times specified in Table 2. The gel layer was thoroughly removed with running water and the specimens were dried with absorbent paper. Specimens in the groups treated with OTC products (LW and CPW) were immersed in mouth rinses, according to recommendations of the manufacturers (Table 2), under constant agitation. Samples in the combination groups (38% HP + LW, 10% CP + LW, 38% HP + CPW, 10% CP + CPW) were treated with conventional bleaching agents and subjected to mouth rinses after 24 hours, since they were treated based on the same protocol described above. All specimens were stored in distilled water at 37°C between applications [13]. The bleaching protocols used in this study are presented in Table 2. Distilled water was replaced daily in all groups. Surface color, microhardness, and roughness were evaluated at 24 hours after the last application and/or immersion.
Table 2
Application protocols of the bleaching agents in the experimental groups depending on treatment and application time
HP, hydrogen peroxide (38% HP; Opalescence Boost, Ultradent Products Inc., South Jordan, UT, USA); CP, carbamide peroxide (10% CP; Opalescence 10% PF, Ultradent Products Inc.); LW, Listerine Whitening (Johnson & Johnson do Brasil Indústria e Comércio de Produtos para Saúde Ltda, São Paulo, SP, Brazil); CPW, Colgate Plax Whitening (Colgate-Palmolive Ind. Ltda., São Paulo, SP, Brazil); CG, control group.
*According to the manufacturer's instructions.
Statistical analyses were performed in the Minitab 16 for Windows 8 software (Minitab Inc., Pennsylvania State College, Philadelphia, PA, USA). Data were tabulated and their normality was assessed through the Kolmogorov-Smirnov test. Next, 2-way ANOVA was used to determine differences in microhardness and roughness. One-way ANOVA followed by the Tukey test, at a 5% significance level, was applied to the color change data. The Dunnett test was adopted to compare the roughness and microhardness data of the treated groups to those of the control group.
RESULTS
Table 3 presents the ΔE values for each tested bleaching protocol. Data were assessed through 1-way ANOVA, followed by the Tukey post hoc test, which indicated significant differences among the treatments (p < 0.05). The mean ΔE of each group was statistically different from that of the control group (p < 0.05).
Table 3
Color changes (ΔE) of the enamel specimens after various experimental bleaching protocols
Data are presented as means ± standard deviations. Values with different superscript letters were statistically different according to the Tukey test (p < 0.05).
HP, hydrogen peroxide (38% HP; Opalescence Boost, Ultradent Products Inc., South Jordan, UT, USA); CP, carbamide peroxide (10% CP; Opalescence 10% PF, Ultradent Products Inc.); LW, Listerine Whitening (Johnson & Johnson do Brasil Indústria e Comércio de Produtos para Saúde Ltda, São Paulo, SP, Brazil); CPW, Colgate Plax Whitening (Colgate-Palmolive Ind. Ltda., São Paulo, SP, Brazil); CG, control group.
*Asterisk means that the value is statistically significantly different from the corresponding value in the control group according to the Dunnett test (p < 0.05).
The bleaching effect observed in the treatment group with 38% HP + CPW, which was statistically equivalent to the result observed for treatment groups with 10% CP and 10% CP + CPW, was greater in comparison to the ΔE values recorded for other treatment groups (Table 3). The CPW group showed less color change and was statistically equivalent to the LW group. However, all groups showed statistically significant differences from the control group in the Dunnett test (p < 0.05).
Microhardness data were used to calculate power, which was determined to be 0.956 when the greatest difference between groups was adopted (a Knoop microhardness [KHN] of 199.19 ± 21.72). Table 4 presents the KHN values at T0 and T1. Significant differences were found across treatments (p < 0.05) and between time points (p < 0.05), and a significant interaction effect was found between these 2 variables (p < 0.05).
Table 4
Microhardness (KHN) values of the enamel specimens at baseline (T0), and after the bleaching treatments (T1), based on the bleaching protocols and evaluation time point (n = 12)
Data are presented as means ± standard deviations. Values with different uppercase superscript letters in each row were statistically significantly different for each treatment between the time points before (T0) and after (T1) treatment based on the Tukey test (p < 0.05). Values with different lowercase superscript letters in each column were statistically significantly different at each time point between the experimental treatment groups based on the Tukey test (p < 0.05).
HP, hydrogen peroxide (38% HP; Opalescence Boost, Ultradent Products Inc., South Jordan, UT, USA); CP, carbamide peroxide (10% CP; Opalescence 10% PF, Ultradent Products Inc.); LW, Listerine Whitening (Johnson & Johnson do Brasil Indústria e Comércio de Produtos para Saúde Ltda, São Paulo, SP, Brazil); CPW, Colgate Plax Whitening (Colgate-Palmolive Ind. Ltda., São Paulo, SP, Brazil); CG, control group.
*Asterisk means that the value is statistically significantly different from the corresponding value in the control group according to the Dunnett test (p < 0.05).
After all protocols were completed, only the LW group showed no statistically significant microhardness changes. No statistically significant difference in KHN was found when groups were compared at T0; however, the groups were significantly different when they were compared at T1. The specimens treated with LW mouth rinse recorded the highest microhardness values. However, based on the Dunnett test, all groups showed statistically significant changes in KHN compared to the control group after treatment was completed (p < 0.05). The 38% HP + CPW and 10% CP + CPW groups presented the lowest microhardness values.
The surface roughness values at T0 and T1 are shown in Table 5. There were significant differences across the treatments (p < 0.05) and between the time points (p < 0.05), as well as a significant interaction effect between these 2 variables (p < 0.05).
Table 5
Surface roughness (Ra; in μm) values of the enamel specimens at baseline (T0) and after the bleaching treatments (T1) according to the experimental bleaching protocol and the evaluation time point (n = 12)
Data are presented as means ± standard deviations. Values with different uppercase superscript letters in each row were statistically significantly different for each treatment between the time points before (T0) and after (T1) treatment based on the Tukey test (p < 0.05). Values with different lowercase superscript letters in each column were statistically significantly different at each time point between the experimental treatment groups based on the Tukey test (p < 0.05).
HP, hydrogen peroxide (38% HP; Opalescence Boost, Ultradent Products Inc., South Jordan, UT, USA); CP, carbamide peroxide (10% CP; Opalescence 10% PF, Ultradent Products Inc.); LW, Listerine Whitening (Johnson & Johnson do Brasil Indústria e Comércio de Produtos para Saúde Ltda, São Paulo, SP, Brazil); CPW, Colgate Plax Whitening (Colgate-Palmolive Ind. Ltda., São Paulo, SP, Brazil); CG, control group.
*Asterisk means that the value is statistically significantly different from the corresponding value in the control group according to the Dunnett test (p < 0.05).
All groups were statistically equivalent at T0, highlighting the random allocation of samples between groups. Although various bleaching treatments changed the roughness of the enamel surface (p < 0.05), only the 38% HP group showed no statistically significant change in surface roughness after the bleaching treatment. However, based on the Dunnett test (p < 0.05), only the 38% HP and 10% CP groups were statistically equivalent to the control group.
DISCUSSION
The current study investigated the combined effect of various bleaching treatments on color and surface properties (microhardness and surface roughness) of human dental enamel. This study analyzed both bleaching treatments performed and supervised by professionals with hydrogen or carbamide peroxide gels, and those done by patients themselves with OTC products (mouth rinses containing hydrogen peroxide). OTC products are freely sold and they can be self-applied by patients. Based on our results, the groups that received conventional treatments using 38% HP and 10% CP gels showed significantly greater color changes than those treated with mouth rinses (LW and CPW) and the control group. Therefore, the conventional treatments, whether in-office or at-home, promoted color changes of dental enamel in the short term. The present results are consistent with those of previous studies [8,17], which showed that these treatments were more effective for color change than whitening mouth rinses alone.
Based on the literature, the hydrogen peroxide present in bleaching mouth rinse formulations could have a bleaching effect on the enamel [4], but low concentrations of the bleaching agent could limit the clinical effectiveness of such changes, as in the present study. However, Torres et al. [7] reported that mouth rinses with LW and CPW for 12 weeks had similar results to those of treatment with 10% carbamide peroxide applied for 14 days. Nonetheless, they pointed out that dilution of the mouth rinse in saliva might have influenced the bleaching effect, although the mouth rinses showed clinically similar effectiveness. The combined effect of conventional techniques and bleaching mouth rinses was investigated in this study. This combination led to significant color change in comparison to the samples treated with whitening mouth rinses alone, or in association with CPW, leading to a stronger bleaching effect on the tooth surface; thus, the first null hypothesis tested herein was rejected. The synergistic effect in the 38% HP + CPW group may have occurred due to the acidic behavior of whitening mouth rinses, particularly of CPW (pH 3.42). This finding is consistent with that reported by Lima et al. [6], who assessed the effect of LW and CPW whitening mouth rinses on enamel specimens. According to their study, the CPW whitening mouth rinse led to greater color change, and the effect was ascribed to the low pH. Araújo et al. [1] raised the concern that the association between bleaching treatments and CPW whitening mouth rinse may have been related to patients' personal habits, since these acid products could have a negative effect on the enamel surface.
The combinations of conventional techniques and mouth rinses led to severe changes in the microhardness and surface roughness of the enamel specimens. In this study, microhardness decreased and surface roughness increased. Therefore, the second null hypothesis was also rejected. These findings are consistent with those of previous reports on combinations of carbamide peroxide-based bleaching agents and acidic or abrasive substances, which caused significant changes in the enamel structure [1,2,13,18,19]. Accordingly, these substances should be used with caution [7] due to the possibility of a synergistic effect between bleaching treatments and whitening mouth rinses, which may have deleterious effects on tooth enamel. It is extremely important for clinicians to be aware of patients' personal habits, so that they can provide warnings of the risks posed by the synergistic effect between these protocols and prevent their undesirable effects on the tooth surface [2,13,18,19]. The enamel surface in the group treated with CPW whitening mouth rinse also suffered damage, because this treatment caused microhardness and surface roughness changes. The present results are supported by the study by Lima et al. [6], who claimed that continuous tooth exposure to acid products can result in numerous complications. According to the authors, the color change triggered by CPW was ascribed to enamel surface demineralization resulting from its low pH. However, the storage of samples in artificial saliva between protocols could have stimulated the formation of a salivary pellicle [20], which might have influenced microhardness and roughness changes.
In contrast, the treatment with LW whitening mouth rinse did not cause any changes in enamel hardness, which might be attributed to its higher pH (5.38). Although a high concentration of HP bleaching gel (38%) used for shorter application periods (3 sessions, 45-minutes long) did not have any effect on the surface roughness of enamel (Table 5), this product led to microhardness changes of the enamel surface. However, its effect was milder than those caused by the combined treatments. These findings corroborate those of Cvikl et al. [12], who claimed that higher concentrations of bleaching agents applied for shorter periods of time may be less harmful to enamel. Therefore, the longer the enamel is exposed to the bleaching agent, the worse the damage caused by the agent is [9,10]. For this reason, high gel concentrations have been recommended in order to achieve rapid results [11,21]. However, Soares et al. [11], presented opposite findings, according to which the higher the concentration of the bleaching agent, the worse the damage. These issues need to be studied further in the future.
Based on the present results, conventional treatments are more effective than whitening mouth rinses. The combination of protocols (conventional and whitening mouth rinse) accelerated the lightening effect, but also worsened enamel damage. This stronger lightening effect may have resulted from the successive use of both protocols and through the synergistic effect between conventional treatments (peroxide-based bleaching agents) and whitening mouth rinses. The use of higher concentrations of a bleaching agent with fewer applications and for shorter periods of time could be an interesting alternative, since this treatment model could cause less deleterious effects on enamel and reduce treatment time and costs.
The present results must be cautiously interpreted, since the research was performed in a laboratory environment and evaluated the action of bleaching agents outside the oral environment (i.e., samples were stored in distilled water, not artificial saliva). Saliva might favor enamel surface remineralization [22] and the oral environment could influence the action of bleaching agents in a clinical setting.
CONCLUSIONS
Whitening mouth rinses had a bleaching effect only when they were used with conventional treatments. The combined protocols involving conventional treatments and whitening mouth rinses led to significant changes of the enamel surface. Furthermore, bleaching agents and acidic substances, such as whitening mouth rinses, should be used with caution, and the risks of using such combinations must be explained to prospective patients to prevent their undesirable effects on the tooth surface.
-
Conflict of Interest: No potential conflict of interest relevant to this article was reported.
-
Author Contributions:
Conceptualization: Berger SB.
Data curation: Favaro JC, Geha O.
Formal analysis: Favaro JC, Geha O, Guiraldo RD, Lopes MB, Berger SB.
Funding acquisition: Lopes MB.
Investigation: Favaro JC, Geha O, Guiraldo RD, Aranha AMF.
Methodology: Favaro JC, Geha O, Guiraldo RD, Lopes MB.
Project administration: Berger SB.
Resources: Guiraldo RD.
Supervision: Berger SB.
Validation: Favaro JC, Geha O, Aranha AMF.
Visualization: Favaro JC, Geha O.
Writing - original draft: Favaro JC.
Writing - review & editing: Favaro JC, Geha O, Guiraldo RD, Lopes MB, Aranha AMF, Berger SB.
- 1. de Araújo LS, dos Santos PH, Anchieta RB, Catelan A, Fraga Briso AL, Fraga Zaze AC, Sundfeld RH. Mineral loss and color change of enamel after bleaching and staining solutions combination. J Biomed Opt 2013;18:108004.ArticlePubMed
- 2. Kishta-Derani M, Neiva G, Yaman P, Dennison J. In vitro evaluation of tooth-color change using four paint-on tooth whiteners. Oper Dent 2007;32:394-398.ArticlePubMedPDF
- 3. Haywood VB, Heymann HO. Nightguard vital bleaching. Quintessence Int 1989;20:173-176.PubMed
- 4. Demarco FF, Meireles SS, Masotti AS. Over-the-counter whitening agents: a concise review. Braz Oral Res 2009;23(Supplement 1):64-70.ArticlePubMed
- 5. Hilgenberg SP, Pinto SC, Farago PV, Santos FA, Wambier DS. Physical-chemical characteristics of whitening toothpaste and evaluation of its effects on enamel roughness. Braz Oral Res 2011;25:288-294.ArticlePubMed
- 6. Lima FG, Rotta TA, Penso S, Meireles SS, Demarco FF. In vitro evaluation of the whitening effect of mouth rinses containing hydrogen peroxide. Braz Oral Res 2012;26:269-274.ArticlePubMed
- 7. Torres CR, Perote LC, Gutierrez NC, Pucci CR, Borges AB. Efficacy of mouth rinses and toothpaste on tooth whitening. Oper Dent 2013;38:57-62.ArticlePubMedPDF
- 8. Jaime IM, França FM, Basting RT, Turssi CP, Amaral FL. Efficacy of hydrogen-peroxide-based mouthwash in altering enamel color. Am J Dent 2014;27:47-50.PubMed
- 9. Potgieter E, Osman Y, Grobler SR. The effect of three whitening oral rinses on enamel micro-hardness. SADJ 2014;69:152. 154-156.PubMed
- 10. Bistey T, Nagy IP, Simó A, Hegedus C. In vitro FT-IR study of the effects of hydrogen peroxide on superficial tooth enamel. J Dent 2007;35:325-330.ArticlePubMed
- 11. Soares DG, Ribeiro AP, Sacono NT, Loguércio AD, Hebling J, Costa CA. Mineral loss and morphological changes in dental enamel induced by a 16% carbamide peroxide bleaching gel. Braz Dent J 2013;24:517-521.ArticlePubMed
- 12. Cvikl B, Lussi A, Moritz A, Flury S. Enamel surface changes after exposure to bleaching gels containing carbamide peroxide or hydrogen peroxide. Oper Dent 2016;41:E39-E47.ArticlePubMedPDF
- 13. Özkan P, Kansu G, Özak ST, Kurtulmuş-Yilmaz S, Kansu P. Effect of bleaching agents and whitening dentifrices on the surface roughness of human teeth enamel. Acta Odontol Scand 2013;71:488-497.PubMed
- 14. Berger SB, Cavalli V, Ambrosano GM, Giannini M. Changes in surface morphology and mineralization level of human enamel following in-office bleaching with 35% hydrogen peroxide and light irradiation. Gen Dent 2010;58:e74-e79.PubMed
- 15. Yasa B, Arslan H, Akcay M, Kavrik F, Hatirli H, Ozkan B. Comparison of bleaching efficacy of two bleaching agents on teeth discoloured by different antibiotic combinations used in revascularization. Clin Oral Investig 2015;19:1437-1442.ArticlePubMedPDF
- 16. Horuztepe SA, Baseren M. Effect of resin infiltration on the color and microhardness of bleached white-spot lesions in bovine enamel (an in vitro study). J Esthet Restor Dent 2017;29:378-385.ArticlePubMedPDF
- 17. Karadas M, Hatipoglu O. Efficacy of mouthwashes containing hydrogen peroxide on tooth whitening. Sci World J 2015;2015:961403.ArticlePubMedPMCPDF
- 18. Melo CF, Manfroi FB, Spohr AM. Microhardness and roughness of enamel bleached with 10% carbamide peroxide and brushed with different toothpastes: an in situ study. J Int Oral Health 2014;6:18-24.
- 19. Bolay S, Cakir FY, Gurgan S. Effects of toothbrushing with fluoride abrasive and whitening dentifrices on both unbleached and bleached human enamel surface in terms of roughness and hardness: an in vitro study. J Contemp Dent Pract 2012;13:584-589.ArticlePubMed
- 20. Joiner A. Review of the effects of peroxide on enamel and dentine properties. J Dent 2007;35:889-896.ArticlePubMed
- 21. Matis BA, Cochran MA, Eckert G. Review of the effectiveness of various tooth whitening systems. Oper Dent 2009;34:230-235.ArticlePubMedPDF
- 22. Faraoni-Romano JJ, Da Silveira AG, Turssi CP, Serra MC. Bleaching agents with varying concentrations of carbamide and/or hydrogen peroxides: effect on dental microhardness and roughness. J Esthet Restor Dent 2008;20:395-402.ArticlePubMed
REFERENCES
Tables & Figures
REFERENCES
Citations
Citations to this article as recorded by 
- Property changes in resin composite exposed to mouth rinses during 10% carbamide peroxide bleaching
Mariana Ferreira da Silva, Giovana Contin Germinari, Carolina Meneghin Barbosa, Tatiane Cristina Dotta, Renata Siqueira Scatolin, Waldemir Francisco Vieira Júnior, Laura Nobre Ferraz
Brazilian Journal of Oral Sciences.2026; 25: e260366. CrossRef - Effect of Over-the-counter Whitening Products on Postbleaching Enamel Surface Roughness and Shade Recovery: An In Vitro Study
Rocío Llancari-Alonzo, Jorge Manrique-Guzmán, Jorge Manrique-Chávez, Leonor Castro-Ramirez, Carlos López-Gurreonero, Alberto Cornejo-Pinto, César Cayo-Rojas
The Journal of Contemporary Dental Practice.2026; 27(2): 148. CrossRef - Influence of commercial mouth rinses with different formulations on enamel properties during at-home bleaching
Thalita Novello Coelho, Ana Júlia Gil, Marcos Roberto Lima Benati, Carolina Meneghin Barbosa, Tatiane Cristina Dotta, Waldemir Francisco Vieira-Junior, Renata Siqueira Scatolin, Laura Nobre Ferraz
Odontology.2026;[Epub] CrossRef - Which Whitening Mouthwash With Different Ingredients Is More Effective on Color and Bond Strength of Enamel?
Elif Varli Tekingur, Fatih Bedir, Muhammet Karadas, Rahime Zeynep Erdem
Journal of Esthetic and Restorative Dentistry.2025; 37(4): 960. CrossRef - Do Different Tooth Bleaching–Remineralizing Regimens Affect the Bleaching Effectiveness and Enamel Microhardness In Vitro?
Hamideh Sadat Mohammadipour, Parnian Shokrollahi, Sima Gholami, Hosein Bagheri, Fatemeh Namdar, Salehe Sekandari, Cesar Rogério Pucci
International Journal of Dentistry.2024;[Epub] CrossRef - Effect of hydrogen peroxide versus charcoal-based whitening mouthwashes on color, surface roughness, and color stability of enamel
Mayada S. Sultan
BMC Oral Health.2024;[Epub] CrossRef - Effects of online marketplace-sourced over-the-counter tooth whitening products on the colour, microhardness, and surface topography of enamel: an in vitro study
Radhika Agarwal, Nikki Vasani, Urmila Sachin Mense, Niharika Prasad, Aditya Shetty, Srikant Natarajan, Arindam Dutta, Manuel S. Thomas
BDJ Open.2024;[Epub] CrossRef - Effect of Whitening Mouthwashes on Color Change and Enamel Mineralization: An In Vitro Study
Rosa Josefina Roncal Espinoza, José Alberto Castañeda Vía, Alexandra Mena-Serrano, Lidia Yileng Tay
World Journal of Dentistry.2023; 14(9): 739. CrossRef - Effectiveness and Adverse Effects of Over-the-Counter Whitening Products on Dental Tissues
Maiara Rodrigues de Freitas, Marynara Mathias de Carvalho, Priscila Christiane Suzy Liporoni, Ana Clara Borges Fort, Rodrigo de Morais e Moura, Rayssa Ferreira Zanatta
Frontiers in Dental Medicine.2021;[Epub] CrossRef - Renklendirilmiş kompozit rezinin renk değişimine ve yüzey pürüzlülüğüne beyazlatıcı ağız gargarasının etkisi
Şeref Nur MUTLU, Makbule Tuğba TUNCDEMIR
Selcuk Dental Journal.2020; 7(3): 435. CrossRef
 ePub Link
ePub Link Cite
CiteEvaluation of the effects of whitening mouth rinses combined with conventional tooth bleaching treatments
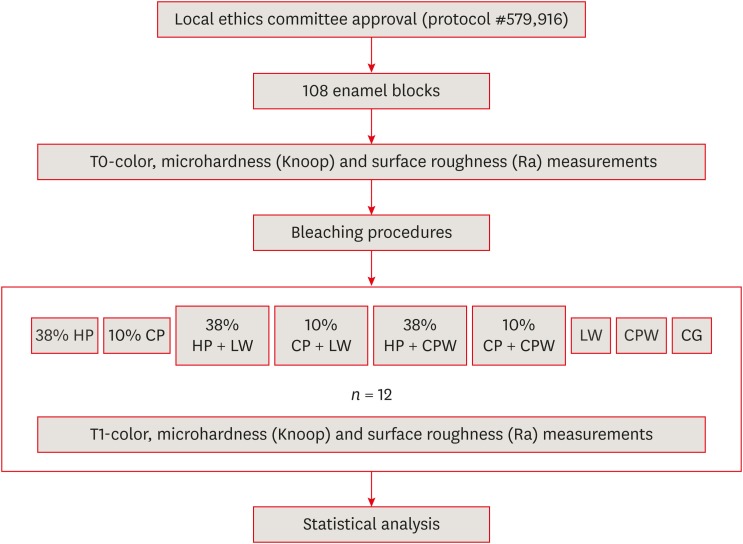
Figure 1 Schematic illustration of the experimental design.T0, at the beginning of the study (baseline); T1, after bleaching treatment; HP, hydrogen peroxide (38% HP; Opalescence Boost, Ultradent Products Inc., South Jordan, UT, USA); CP, carbamide peroxide (10% CP; Opalescence 10% PF, Ultradent Products Inc.); LW, Listerine Whitening (Johnson & Johnson do Brasil Indústria e Comércio de Produtos para Saúde Ltda, São Paulo, SP, Brazil); CPW, Colgate Plax Whitening (Colgate-Palmolive Ind. Ltda., São Paulo, SP, Brazil); CG, control group.
Figure 1
Evaluation of the effects of whitening mouth rinses combined with conventional tooth bleaching treatments
Information about the materials used in the present study
| Product | Manufacturer/batch | Composition | Classification | pH |
|---|---|---|---|---|
| Opalescence Boost (38% HP) | Ultradent Products Inc., South Jordan, UT, USA/DO 19U | Gel: Hydrogen peroxide | Whitening gel | 6.88 |
| Activator: Potassium hydroxide, 1.1% fluoride, and 3% potassium nitrate | ||||
| Opalescence 10% PF (10% CP) | Ultradent Products Inc., South Jordan, UT, USA/D014W | Carbamide peroxide, potassium nitrate, 0.11% fluoride ion, carbopol, glycerin, flavor | Whitening gel | 6.5 |
| Listerine Whitening (LW) | Johnson & Johnson do Brasil Indústria e Comércio de Produtos para Saúde Ltda, São Paulo City, São Paulo, Brazil/0285C | Water, alcohol (8%), hydrogen peroxide, sodium phosphate, poloxamer 407, sodium lauryl sulfate, sodium citrate, mint flavor, menthol, eucalyptol, sodium saccharin, sucralose | Mouth rinse | 5.38 |
| Colgate Plax Whitening (CPW) | Colgate-Palmolive Ind. Ltda. São Paulo City, São Paulo, Brazil/5260BR121C | Water, ethyl alcohol, hydrogen peroxide, sorbitol, poloxamer 338, polysorbate 20, methyl salicylate, menthol, sodium saccharin, CL 42090 | Mouth rinse | 3.42 |
| Control group | - | Distilled water | - | 7.0 |
Application protocols of the bleaching agents in the experimental groups depending on treatment and application time
| Group | Bleaching agent | Application protocol* |
|---|---|---|
| 38% HP | Opalescence Boost | 3 sessions (3 applications, 15 min each), 1-week interval between sessions |
| 10% CP | Opalescence 10% PF | 6 hr/day, 15 days |
| 38% HP + LW | Opalescence Boost + Listerine Whitening | 3 sessions 38% HP + LW: 1 min × 2 times/day, 12 weeks* |
| 10% CP + LW | Opalescence 10% PF + Listerine Whitening | 10% CP, 6 hr/day, 15 days; LW, 1 min × 2 times/day, 12 weeks |
| 38% HP + CPW | Opalescence Boost + Colgate Plax Whitening | 3 sessions with 38% HP; CPW, 2 min × 2 times/day, 12 weeks |
| 10% CP + CPW | Opalescence 10% PF + Colgate Plax Whitening | 10% CP, 6 hr/day, 15 days; CPW, 2 min × 2 times/day, 12 weeks |
| LW | Listerine Whitening | 1 min × 2 times/day, 12 weeks |
| CPW | Colgate Plax Whitening | 2 min × 2 times/day, 12 weeks |
| CG | Distilled water | Immersion for 12 weeks |
HP, hydrogen peroxide (38% HP; Opalescence Boost, Ultradent Products Inc., South Jordan, UT, USA); CP, carbamide peroxide (10% CP; Opalescence 10% PF, Ultradent Products Inc.); LW, Listerine Whitening (Johnson & Johnson do Brasil Indústria e Comércio de Produtos para Saúde Ltda, São Paulo, SP, Brazil); CPW, Colgate Plax Whitening (Colgate-Palmolive Ind. Ltda., São Paulo, SP, Brazil); CG, control group.
*According to the manufacturer's instructions.
Color changes (ΔE) of the enamel specimens after various experimental bleaching protocols
| Treatment | ΔL | Δa | Δb | ΔE |
|---|---|---|---|---|
| 38% HP | 6.74 ±; 2.35 | −1.44 ±; 0.82 | −5.98 ±; 2.38 | 9.51 ±; 2.20bc* |
| 10% CP | 8.86 ±; 3.67 | −1.72 ±; 0.95 | −8.95 ±; 4.27 | 13.15 ±; 4.5ab* |
| 38% HP + LW | 4.66 ±; 3.28 | −2.13 ±; 1.42 | −10.10 ±; 5.25 | 12.02 ±; 4.70b* |
| 10% CP + LW | 3.11 ±; 2.98 | −2.05 ±; 1.03 | −7.86 ±; 5.87 | 9.75 ±; 4.70bc* |
| 38% HP + CPW | 5.02 ±; 6.67 | −3.03 ±; 1,86 | −15.17 ±; 3.49 | 17.84 ±; 4.30a* |
| 10% CP + CPW | 7.75 ±; 4.91 | −1.81 ±; 1.40 | −10.72 ±; 4.03 | 14.20 ±; 4.40ab* |
| LW | 3.48 ±; 3.66 | −1.40 ±; 0.82 | −1.73 ±; 3.50 | 6.08 ±; 2.50cd* |
| CPW | 3.48 ±; 3.66 | −1.40 ±; 0.82 | −1,73 ±; 3.50 | 3.66 ±; 2.00d* |
| CG | 0.88 ±; 0.59 | 0.25 ±; 0.52 | 0.44 ±; 0.58 | 1.30 ±; 0.59 |
Data are presented as means ± standard deviations. Values with different superscript letters were statistically different according to the Tukey test (p < 0.05).
HP, hydrogen peroxide (38% HP; Opalescence Boost, Ultradent Products Inc., South Jordan, UT, USA); CP, carbamide peroxide (10% CP; Opalescence 10% PF, Ultradent Products Inc.); LW, Listerine Whitening (Johnson & Johnson do Brasil Indústria e Comércio de Produtos para Saúde Ltda, São Paulo, SP, Brazil); CPW, Colgate Plax Whitening (Colgate-Palmolive Ind. Ltda., São Paulo, SP, Brazil); CG, control group.
*Asterisk means that the value is statistically significantly different from the corresponding value in the control group according to the Dunnett test (p < 0.05).
Microhardness (KHN) values of the enamel specimens at baseline (T0), and after the bleaching treatments (T1), based on the bleaching protocols and evaluation time point (n = 12)
| Treatment | Evaluation time point | Hardness loss (%) | |
|---|---|---|---|
| T0 | T1 | ||
| 38% HP | 328.33 ±; 7.16Aa | 252.64 ±; 23.18Bb* | 23.05 |
| 10% CP | 324.65 ±; 11.56Aa | 234.57 ±; 7.68Bbc* | 27.75 |
| 38% HP + LW | 320.59 ±; 27.68Aa | 208.75 ±; 25.01Bc* | 12.43 |
| 10% CP + LW | 314.69 ±; 26.51Aa | 226.75 ±; 34.57Bbc* | 27.94 |
| 38% HP + CPW | 315.94 ±; 19.69Aa | 129.53 ±; 21.48Bd* | 59.00 |
| 10% CP + CPW | 328.72 ±; 13.86Aa | 148.66 ±; 36.66Bd* | 54.78 |
| LW | 318.52 ±; 29.15Aa | 298.42 ±; 21.56Aa* | 6.31 |
| CPW | 325.57 ±; 15.06Aa | 242.28 ±; 36.46Bbc* | 25.58 |
| CG | 326.46 ±; 12.06 | ||
Data are presented as means ± standard deviations. Values with different uppercase superscript letters in each row were statistically significantly different for each treatment between the time points before (T0) and after (T1) treatment based on the Tukey test (p < 0.05). Values with different lowercase superscript letters in each column were statistically significantly different at each time point between the experimental treatment groups based on the Tukey test (p < 0.05).
HP, hydrogen peroxide (38% HP; Opalescence Boost, Ultradent Products Inc., South Jordan, UT, USA); CP, carbamide peroxide (10% CP; Opalescence 10% PF, Ultradent Products Inc.); LW, Listerine Whitening (Johnson & Johnson do Brasil Indústria e Comércio de Produtos para Saúde Ltda, São Paulo, SP, Brazil); CPW, Colgate Plax Whitening (Colgate-Palmolive Ind. Ltda., São Paulo, SP, Brazil); CG, control group.
*Asterisk means that the value is statistically significantly different from the corresponding value in the control group according to the Dunnett test (p < 0.05).
Surface roughness (Ra; in μm) values of the enamel specimens at baseline (T0) and after the bleaching treatments (T1) according to the experimental bleaching protocol and the evaluation time point (n = 12)
| Treatment | Evaluation time point | Roughness change (%) | |
|---|---|---|---|
| T0 | T1 | ||
| 38% HP | 0.037 ±; 0.014Aa | 0.047 ±; 0.024Ac | 127.03 |
| 10% CP | 0.030 ±; 0.008Ba | 0.050 ±; 0.012Ac | 166.67 |
| 38% HP + LW | 0.029 ±; 0.008Ba | 0.183 ±; 0.033Aab* | 631.03 |
| 10% CP + LW | 0.027 ±; 0.010Ba | 0.163 ±; 0.037Aab* | 603.70 |
| 38% HP + CPW | 0.031 ±; 0.013Ba | 0.208 ±; 0.115Aa* | 670.97 |
| 10% CP + CPW | 0.044 ±; 0.033Ba | 0.201 ±; 0.019Aab* | 456.82 |
| LW | 0.025 ±; 0.012Ba | 0.133 ±; 0.027Ab* | 532.00 |
| CPW | 0.033 ±; 0.021Ba | 0.194 ±; 0.023Aab* | 587.88 |
| CG | 0.031 ±; 0.0130 | ||
Data are presented as means ± standard deviations. Values with different uppercase superscript letters in each row were statistically significantly different for each treatment between the time points before (T0) and after (T1) treatment based on the Tukey test (p < 0.05). Values with different lowercase superscript letters in each column were statistically significantly different at each time point between the experimental treatment groups based on the Tukey test (p < 0.05).
HP, hydrogen peroxide (38% HP; Opalescence Boost, Ultradent Products Inc., South Jordan, UT, USA); CP, carbamide peroxide (10% CP; Opalescence 10% PF, Ultradent Products Inc.); LW, Listerine Whitening (Johnson & Johnson do Brasil Indústria e Comércio de Produtos para Saúde Ltda, São Paulo, SP, Brazil); CPW, Colgate Plax Whitening (Colgate-Palmolive Ind. Ltda., São Paulo, SP, Brazil); CG, control group.
*Asterisk means that the value is statistically significantly different from the corresponding value in the control group according to the Dunnett test (p < 0.05).
Table 1 Information about the materials used in the present study
Table 2 Application protocols of the bleaching agents in the experimental groups depending on treatment and application time
HP, hydrogen peroxide (38% HP; Opalescence Boost, Ultradent Products Inc., South Jordan, UT, USA); CP, carbamide peroxide (10% CP; Opalescence 10% PF, Ultradent Products Inc.); LW, Listerine Whitening (Johnson & Johnson do Brasil Indústria e Comércio de Produtos para Saúde Ltda, São Paulo, SP, Brazil); CPW, Colgate Plax Whitening (Colgate-Palmolive Ind. Ltda., São Paulo, SP, Brazil); CG, control group.
*According to the manufacturer's instructions.
Table 3 Color changes (ΔE) of the enamel specimens after various experimental bleaching protocols
Data are presented as means ± standard deviations. Values with different superscript letters were statistically different according to the Tukey test (
HP, hydrogen peroxide (38% HP; Opalescence Boost, Ultradent Products Inc., South Jordan, UT, USA); CP, carbamide peroxide (10% CP; Opalescence 10% PF, Ultradent Products Inc.); LW, Listerine Whitening (Johnson & Johnson do Brasil Indústria e Comércio de Produtos para Saúde Ltda, São Paulo, SP, Brazil); CPW, Colgate Plax Whitening (Colgate-Palmolive Ind. Ltda., São Paulo, SP, Brazil); CG, control group.
*Asterisk means that the value is statistically significantly different from the corresponding value in the control group according to the Dunnett test (
Table 4 Microhardness (KHN) values of the enamel specimens at baseline (T0), and after the bleaching treatments (T1), based on the bleaching protocols and evaluation time point (n = 12)
Data are presented as means ± standard deviations. Values with different uppercase superscript letters in each row were statistically significantly different for each treatment between the time points before (T0) and after (T1) treatment based on the Tukey test (
HP, hydrogen peroxide (38% HP; Opalescence Boost, Ultradent Products Inc., South Jordan, UT, USA); CP, carbamide peroxide (10% CP; Opalescence 10% PF, Ultradent Products Inc.); LW, Listerine Whitening (Johnson & Johnson do Brasil Indústria e Comércio de Produtos para Saúde Ltda, São Paulo, SP, Brazil); CPW, Colgate Plax Whitening (Colgate-Palmolive Ind. Ltda., São Paulo, SP, Brazil); CG, control group.
*Asterisk means that the value is statistically significantly different from the corresponding value in the control group according to the Dunnett test (
Table 5 Surface roughness (Ra; in μm) values of the enamel specimens at baseline (T0) and after the bleaching treatments (T1) according to the experimental bleaching protocol and the evaluation time point (n = 12)
Data are presented as means ± standard deviations. Values with different uppercase superscript letters in each row were statistically significantly different for each treatment between the time points before (T0) and after (T1) treatment based on the Tukey test (
HP, hydrogen peroxide (38% HP; Opalescence Boost, Ultradent Products Inc., South Jordan, UT, USA); CP, carbamide peroxide (10% CP; Opalescence 10% PF, Ultradent Products Inc.); LW, Listerine Whitening (Johnson & Johnson do Brasil Indústria e Comércio de Produtos para Saúde Ltda, São Paulo, SP, Brazil); CPW, Colgate Plax Whitening (Colgate-Palmolive Ind. Ltda., São Paulo, SP, Brazil); CG, control group.
*Asterisk means that the value is statistically significantly different from the corresponding value in the control group according to the Dunnett test (

