
Articles
- Page Path
- HOME > Restor Dent Endod > Volume 44(4); 2019 > Article
- Case Report Guided endodontics: a case report of maxillary lateral incisors with multiple dens invaginatus
-
Afzal Ali1
 , Hakan Arslan2,3
, Hakan Arslan2,3 -
Restor Dent Endod 2019;44(4):e38.
DOI: https://doi.org/10.5395/rde.2019.44.e38
Published online: October 21, 2019
1Department of Conservative Dentistry and Endodontics, Pacific Dental College and Hospital, Udaipur, RJ, India.
2Department of Endodontics, Faculty of Dentistry, Istanbul Health Sciences University, Istanbul, Turkey.
3Department of Endodontics, Faculty of Dentistry, Eastern Mediterranean University, Famagusta, Northern Cyprus.
- Correspondence to Afzal Ali. Reader, Department of Conservative Dentistry and Endodontics, Pacific Dental College and Hospital, Udaipur, RJ 313024, India. abu.ali.4k@gmail.com
• Received: May 29, 2019 • Revised: July 19, 2019 • Accepted: September 3, 2019
Copyright © 2019. The Korean Academy of Conservative Dentistry
This is an Open Access article distributed under the terms of the Creative Commons Attribution Non-Commercial License (https://creativecommons.org/licenses/by-nc/4.0/) which permits unrestricted non-commercial use, distribution, and reproduction in any medium, provided the original work is properly cited.
- 4,323 Views
- 157 Download
- 23 Crossref
Abstract
- Navigation of the main root canal and dealing with a dens invaginatus (DI) is a challenging task in clinical practice. Recently, the guided endodontics technique has become an alternative method for accessing root canals, surgical cavities, and calcified root canals without causing iatrogenic damage to tissue. In this case report, the use of the guided endodontics technique for two maxillary lateral incisors with multiple DIs is described. A 16-year-old female patient was referred with the chief complaint of pain and discoloured upper front teeth. Based on clinical and radiographic findings, a diagnosis of pulp necrosis and chronic periapical abscess associated with double DI (Oehler's type II) was established for the upper left lateral maxillary incisor (tooth #22). Root canal treatment and the sealing of double DI with mineral trioxide aggregate was planned for tooth #22. For tooth #12 (Oehler's type II), preventive sealing of the DI was planned. Minimally invasive access to the double DI and the main root canal of tooth #22, and to the DI of tooth #12, was achieved using the guided endodontics technique. This technique can be a valuable tool because it reduces chair-time and, more importantly, the risk of iatrogenic damage to the tooth structure.
INTRODUCTION
Dens invaginatus (DI), an enamel-lined developmental malformation, occurs as an invagination in the surface of the crown during tooth development [1]. The exact aetiology of DI remains unclear. However, genetic factors, trauma, infection, focal growth retardation/acceleration on the tooth bud, and restriction of the dental arch on the enamel organ are considered to be causal elements [2,3,4].
DI is usually detected accidentally on a radiograph. Clinically, a deep foramen coecum and abnormal crown morphology can be the first sign of an invaginated tooth [4]. Oehler [5] suggested the following classification: type I, an enamel-lined minor invagination occurring within the crown and not extending beyond the cemento-enamel junction; type II, an enamel-lined invagination extending into the root, beyond the cemento-enamel junction, and terminating as a blind sac; type III, invagination penetrating through the root to form an additional apical or lateral foramen [6].
Recently, guided endodontics has gained popularity in the management of calcifications [7], anomalous tooth [8], dens evaginatus [9], access cavity preparations in the normal tooth [10], and micro-endodontic surgical procedures [11]. In the guided endodontics technique, a digital impression is taken and is superimposed onto cone-beam computed tomography (CBCT) data. A path for the drill is created, and a guide is designed to access the root canal using computer-aided design software. Finally, using a 3-dimensional (3D) printer, the guide is printed. The guided endodontics technique can reduce iatrogenic damage to the tooth while obtaining access to the main root canal or the DI, and can decrease the duration of the treatment [12,13,14,15,16]. The purpose of this case report is to describe the use of the guided endodontics technique for 2 lateral incisors with multiple DI.
CASE REPORT
A 16-year-old female patient was referred to the Department of Conservative Dentistry and Endodontics, with the chief complaint of pain and 2 discoloured teeth in the upper front tooth region. The patient was classified as score I according to the American Society of Anaesthesiologists physical status scoring system. The patient reported an intermittent purulent discharge from the gingival sulcus of teeth #21 and #22, starting approximately 1 year ago. The patient had visited the dentist 3 days previously with a complaint of extraoral swelling, and was offered emergency pain management with the initiation of endodontic treatment of tooth #21. A clinical examination revealed a prepared access cavity in relation to tooth #21 and discoloured maxillary left central (tooth #21) and lateral (tooth #22) incisors. The clinical crown of tooth #22 showed an increased labio-lingual dimension, and 2 deep palatal pits were found on tooth #22. There was also a deep palatal pit on tooth #12. Teeth #21, #22, and #23 did not respond to an electric pulp test (Analytic Pulp Tester; Analytic Technology Corp., Richmond, VA, USA) and a thermal test (Pulper G; C Corporation, Tokyo, Japan). However, tooth #12 responded. Teeth #21 and #23 had wide carious lesions. An initial periapical radiographic examination of teeth #12 and #22 revealed abnormal morphology, with an invagination that appeared narrow and enamel-lined, extending to the middle third of the root and a periapical radiolucency in relation to teeth #21, #22, and #23. However, there were 2 bulb-like enamel-lined structures noted, of which one was superficial and other extended to the middle third of the root in relation to tooth #22 (Figure 1A). Based on the clinical and radiographic findings, a diagnosis of pulp necrosis and chronic periapical abscess associated with double DI (Oehler's type II) was established for tooth #22. Root canal treatment and sealing of the double DI with mineral trioxide aggregate (MTA) was planned for tooth #22 (Figure 2). Tooth #12 had one DI (Oehler's type II) without symptoms or signs. Consequently, preventive sealing of DI on tooth #12 was decided upon (Figure 3A).
Figure 1
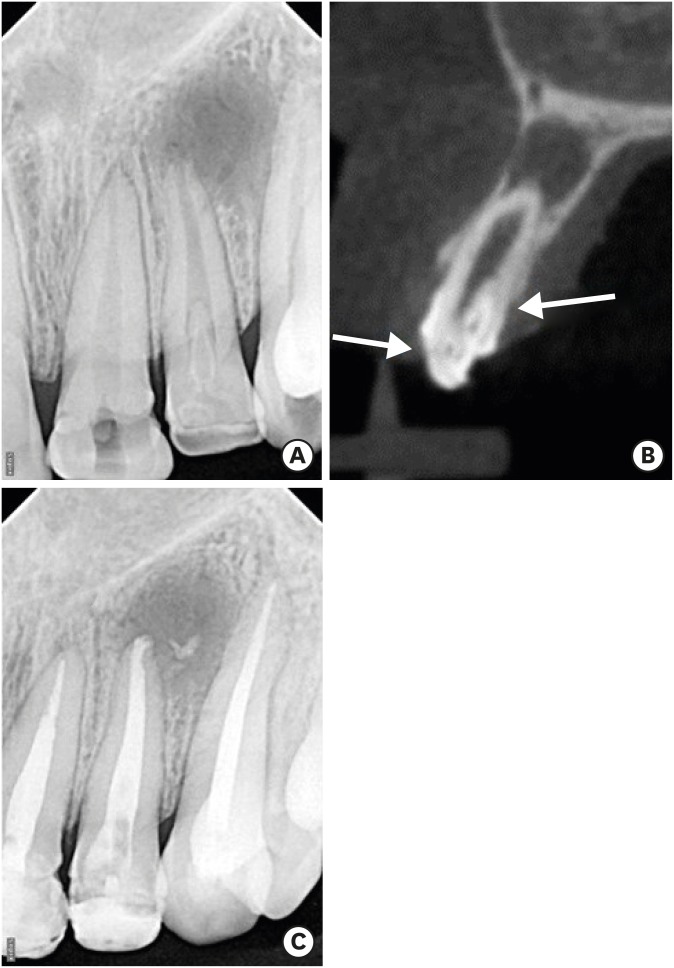
Representative radiographic images of the case. (A) Radiographic view of tooth #22 revealed a large periapical lesion, double dens invaginatus (DI), and a large root canal. (B) A cone-beam computed tomography image revealed that the double DI corresponded to a superficial one and a deep one extending to middle third of the root. (C) After sealing of the double DI and obturation of the root canal.
Figure 2
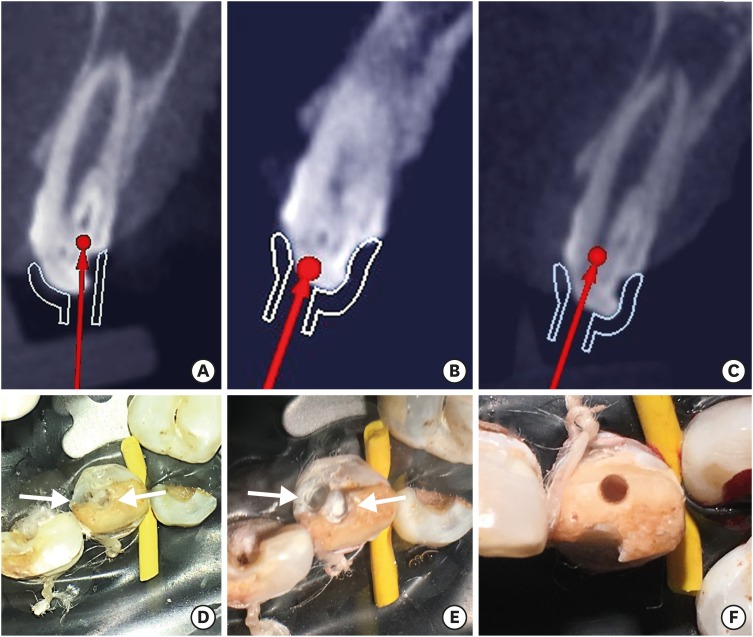
Radiographic and clinical images illustrating access to main canal and double dens followed by sealing of double dens with MTA. (A) Path of the bur to the deeply seated dens invaginatus (DI). (B) Path of the bur to the superficial DI. (C) Path for the bur to the main root canal. (D) Preparation of the DIs. (E) Sealing of the DIs with mineral trioxide aggregate. (F) Access to the main root canal of tooth #22.
Figure 3
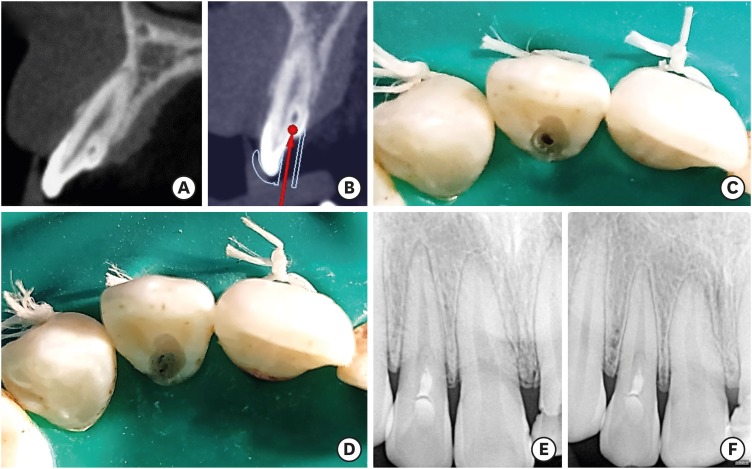
Illustrations showing the Guided prophylactic management of dens invaginatus (A) Tooth #12 with one dens invaginatus (DI). (B) Path of the bur. (C) Clinical view of guided access to the DI only. (D) Mineral trioxide aggregate obturation of the DI cavity. (E) Immediate radiographic view after the procedure. (F) One-year follow-up.
With consent of the patient, a CBCT (Carestream 9300; Carestream Health, Rochester, NY, USA) scan with a constant thickness of 0.65 mm per slice, and with exposure parameters of 84 kV, 6.0 mA, and 12 seconds, was taken of the area of interest. The scan revealed the presence of a periapical radiolucency larger than that revealed by the conventional radiograph (Figure 1B). The axial scan images demonstrated no communication with the main root canal.
Due to the difficulty and potentially high risk of iatrogenic damage to the tooth structure, 3D-printed guides were designed to aid the preparation of the access cavity and the DI cavities. Impressions were taken to obtain a study model of the maxillary teeth. An AutoScan-DS200 Dental 3D Scanner (Shining 3S Tech Co. Ltd., Hangzhou, China) was then used to obtain a stereolithography file of the arches to be used in computer-assisted designs of the splints. The 3D implant planning software (exocad Asia Ltd., Tsim Sha Tsui Kowloon, Hong Kong) was used to design the splints (Figure 4A and 4B) and a 3D printer (Formlabs Inc., Somerville, MA, USA) was used to fabricate the guides (Figure 5A–5D). Paths for the bur were created in order to maintain straight-line access up to the root canal and the DIs (Figures 2A–2C and 3B). The guides were made using dental SG resin (Formlabs Inc.). The length and the diameter of the guiding cylinder were 5 mm and 1.3 mm, respectively. We selected a MI-45F diamond bur (Mani Inc., Tokyo, Japan) with a length of 19.2 mm and a bur head diameter of 1 mm. We chose the milling depth on the basis of the CBCT images, ensuring access to the double dens part, the main root canal of tooth #22, and the dens part of tooth #12.
Figure 4

Illustration depicting 3-dimensional (3D) printed guide. (A) The 3D endodontic guide 1 design for the deeper dens invaginatus (DI) on tooth #22 and the DI on tooth #12. (B) The 3D endodontic guide 1 in the mouth. Arrows indicates the guide for tooth #12.
Figure 5
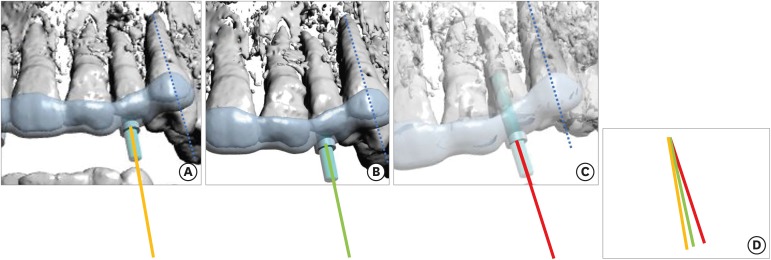
Three guides for tooth #22. The images shown in 5A-5C were rotated to make each canine tooth parallel (blue line). (A) 3D endodontic guide planning for the superficial dens invaginatus (DI) on tooth #22 (yellow line demonstrates the direction of access). (B) The 3-dimensional (3D) endodontic guide planning for the deeper DI on tooth #22 (green line demonstrates the direction of access). (C) 3D endodontic guide planning for the main canal (red line demonstrates the direction of access). (D) Comparison of the direction of each access.
Before placing the guides, multiple teeth were isolated using a rubber dam (Hygenic, Coltene Whaledent Inc., Akron, OH, USA). The 3D guide was placed on the maxillary teeth. Following access to the area of invagination using the guide for teeth #12 and #22, white MTA (ProRoot MTA; Dentsply Tulsa, Tulsa, OK, USA) was placed into the DI cavities (Figure 2D and 2E). MTA was chosen because of its superior tightness properties. The MTA was placed and ultrasonically activated with an Ultra-X device (Eighteeth Medical Technology Co. Ltd., Jiangsu, China), and after wet cotton placement, the teeth (#12 and #22) were temporized. The next day, the cavity was sealed with glass ionomer cement (tooth #22) (Vitrebond; 3M ESPE, Seefeld, Germany) and composite resin (tooth #12) (3M ESPE Dental Products, St. Paul, MN, USA) (Figure 3C–3E).
Using the guide, access was established to the main canal of tooth #22 (Figure 2F). Straight-line access was planned to the main canal, as labial access to the main canal enables the preservation of tooth structure. The root canal was negotiated with a size 15 K-file (Dentsply Maillefer, Ballaigues, Switzerland). The working length was determined using an apex locator (e-pex pro; Eighteeth Medical Technology Co. Ltd.) and was confirmed radiographically. Rotary instrumentation was performed with NiTi instruments (NeoNiti; Neolix, Châtres-la-Forêt, France) and K files up to a size 60. The canals were irrigated with 3% sodium hypochlorite (Novo Dental Product Pvt Ltd., Mumbai, MH, India) and saline, and dried with paper points. Calcium hydroxide paste was placed as an intracanal medicament. The tooth was temporized using Cavit G (3M ESPE) and the patient was recalled after a period of 1 week.
At the next appointment, the calcium hydroxide paste was removed using ultrasonically-activated 5% ethylenediaminetetraacetic acid. MTA was placed in the main root canal of tooth #22 and temporized (Figure 6A). The next day, the access cavity was restored with Filtek-Z250 composite resin (3M ESPE Dental Products) and conventional endodontic management of teeth #21 and #23 was completed (Figures 1C and 3E).
Figure 6
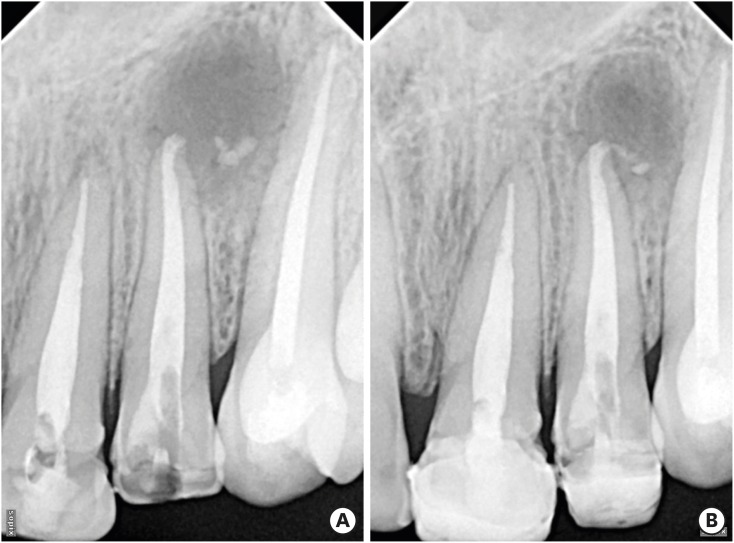
Intraoral periapical radiographs. (A) Immediate postoperative radiograph taken of tooth #22. (B) Radiographs taken at the follow-up visit (1 year later) showed regression of the periapical lesion in relation to tooth #22.
Radiographs taken at the follow-up visit showed regression of the periapical lesion in relation to teeth #21 and #22 (Figure 6B). Tooth #12 showed stable clinical parameters (Figure 3F).
DISCUSSION
Recently, the field of endodontics has begun to undergo an era of digitalization, as in other branches of dentistry. The guided endodontics technique is now applicable and increasingly used by clinicians. The guided endodontics technique was first described by Krastl et al. [17], who presented its use for teeth with pulp canal calcification that required root canal treatment. Up to the present, the technique has been used in a wide variety of cases in endodontics, such as calcification [7,18], dens evaginatus [9], an anomalous tooth [8], access cavity preparations [10] and micro-endodontic surgical procedures [11]. The present report is the first case report describing the use of the guided endodontics technique in two lateral incisors with multiple DIs.
The structural variations associated with DI make it difficult to undertake endodontic treatment. Endodontic treatment of a tooth with DI should only be initiated when the tooth presents relevant signs and symptoms [19]. According to the American Association of Endodontics (AAE) Endodontic Case Difficulty Assessment Guidelines [20], treating a tooth with DI is considered as being of high difficulty in endodontic practice. Management of a tooth with DI is expected to be difficult for even the most experienced clinicians. Furthermore, 3D navigation of DI and the main root canal while minimizing iatrogenic damage to the tooth structure is both time-consuming and challenging. Thus, conventional endodontic access can lead to iatrogenic damage to the tooth structure, resulting in an increase in treatment duration. In the present case report, tooth #22, which required endodontic treatment, had double DI, and tooth #12 had one DI. The aid of a 3D-printed guide facilitated the procedure.
The time needed to plan, design, and manufacture the guide was relatively long. However, the reduction in the duration of the treatment compensated for this. The possibility of iatrogenic damage to the tooth structure was also eliminated. After protocols are established, the planning period can be further shortened. A further advantage was that the use of a guide facilitated localization of the DI and the root canal, thereby making the root canal treatment easier [7].
If there are no teeth adjacent to the endodontic treatment-requiring tooth, the access cavity preparation must be prepared without rubber-dam isolation [16]. One of the strengths of this case report was that all the procedures were performed under rubber-dam isolation. Isolation of multiple teeth is needed to support the guide. A disadvantage of the guide is the limited visualization of the treatment under the guide. Thus, it may be necessary to disassemble the guide intermittently to ensure that the appropriate path is still being followed [3,18].
CONCLUSION
Minimally invasive access to both the DI and the main root canal was achieved in the teeth being treated using the guided endodontics technique. This technique can be a valuable tool for negotiation of the DI and the main root canal, reducing chair-time and, more importantly, the risk of iatrogenic damage to the tooth structure.
-
Conflict of Interest: No potential conflict of interest relevant to this article was reported.
-
Author Contributions:
Conceptualization: Ali A, Arslan H.
Data curation: Ali A, Arslan H.
Formal analysis: Ali A, Arslan H.
Funding acquisition: Ali A.
Investigation: Arslan H.
Methodology: Ali A.
Resources: Ali A.
Software: Ali A, Arslan H.
Supervision: Arslan H.
Validation: Ali A, Arslan H.
Visualization: Ali A.
Writing - original draft: Arslan H.
Writing - review & editing: Arslan H.
- 1. Hülsmann M. Dens invaginatus: aetiology, classification, prevalence, diagnosis, and treatment considerations. Int Endod J 1997;30:79-90.ArticlePubMed
- 2. Chen YH, Tseng CC, Harn WM. Dens invaginatus. Review of formation and morphology with 2 case reports. Oral Surg Oral Med Oral Pathol Oral Radiol Endod 1998;86:347-352.PubMed
- 3. Kumar H, Al-Ali M, Parashos P, Manton DJ. Management of 2 teeth diagnosed with dens invaginatus with regenerative endodontics and apexification in the same patient: a case report and review. J Endod 2014;40:725-731.ArticlePubMed
- 4. Kirzioğlu Z, Ceyhan D. The prevalence of anterior teeth with dens invaginatus in the western Mediterranean region of Turkey. Int Endod J 2009;42:727-734.ArticlePubMed
- 5. Oehlers FA. Dens invaginatus (dilated composite odontome): I. Variations of the invagination process and associated anterior crown forms. Oral Surg Oral Med Oral Pathol 1957;10:1204-1218.PubMed
- 6. Capar ID, Ertas H, Arslan H, Tarim Ertas E. A retrospective comparative study of cone-beam computed tomography versus rendered panoramic images in identifying the presence, types, and characteristics of dens invaginatus in a Turkish population. J Endod 2015;41:473-478.ArticlePubMed
- 7. Torres A, Shaheen E, Lambrechts P, Politis C, Jacobs R. Microguided Endodontics: a case report of a maxillary lateral incisor with pulp canal obliteration and apical periodontitis. Int Endod J 2019;52:540-549.ArticlePubMedPDF
- 8. Byun C, Kim C, Cho S, Baek SH, Kim G, Kim SG, Kim SY. Endodontic treatment of an anomalous anterior tooth with the aid of a 3-dimensional printed physical tooth model. J Endod 2015;41:961-965.ArticlePubMed
- 9. Mena-Álvarez J, Rico-Romano C, Lobo-Galindo AB, Zubizarreta-Macho Á. Endodontic treatment of dens evaginatus by performing a splint guided access cavity. J Esthet Restor Dent 2017;29:396-402.ArticlePubMedPDF
- 10. Connert T, Zehnder MS, Amato M, Weiger R, Kühl S, Krastl G. Microguided Endodontics: a method to achieve minimally invasive access cavity preparation and root canal location in mandibular incisors using a novel computer-guided technique. Int Endod J 2018;51:247-255.ArticlePubMedPDF
- 11. Strbac GD, Schnappauf A, Giannis K, Moritz A, Ulm C. Guided modern endodontic surgery: a novel approach for guided osteotomy and root resection. J Endod 2017;43:496-501.ArticlePubMed
- 12. Ackerman S, Aguilera FC, Buie JM, Glickman GN, Umorin M, Wang Q, Jalali P. Accuracy of 3-dimensional-printed endodontic surgical guide: a human cadaver study. J Endod 2019;45:615-618.ArticlePubMed
- 13. Chong BS, Dhesi M, Makdissi J. Computer-aided dynamic navigation: a novel method for guided endodontics. Quintessence Int 2019;50:196-202.PubMed
- 14. Connert T, Krug R, Eggmann F, Emsermann I, ElAyouti A, Weiger R, Kühl S, Krastl G. Guided endodontics versus conventional access cavity preparation: a comparative study on substance loss using 3-dimensional-printed teeth. J Endod 2019;45:327-331.ArticlePubMed
- 15. Fan Y, Glickman GN, Umorin M, Nair MK, Jalali P. A novel prefabricated grid for guided endodontic microsurgery. J Endod 2019;45:606-610.ArticlePubMed
- 16. Maia LM, de Carvalho Machado V, da Silva NR, Brito Júnior M, da Silveira RR, Moreira Júnior G, Ribeiro Sobrinho AP. Case reports in maxillary posterior teeth by guided endodontic access. J Endod 2019;45:214-218.ArticlePubMed
- 17. Krastl G, Zehnder MS, Connert T, Weiger R, Kühl S. Guided Endodontics: a novel treatment approach for teeth with pulp canal calcification and apical pathology. Dent Traumatol 2016;32:240-246.ArticlePubMed
- 18. van der Meer WJ, Vissink A, Ng YL, Gulabivala K 3rd. 3D computer aided treatment planning in endodontics. J Dent 2016;45:67-72.ArticlePubMed
- 19. Bishop K, Alani A. Dens invaginatus. Part 2: clinical, radiographic features and management options. Int Endod J 2008;41:1137-1154.ArticlePubMed
- 20. American Association of Endodontists. AAE endodontic case difficulty assessment form and guidelines [Internet]. Chicago (IL): American Association of Endodontists; cited 2019 Feb 21]. Available from: https://www.aae.org/specialty/wp-content/uploads/sites/2/2017/10/2006casedifficultyassessmentformb_edited2010.pdf.
REFERENCES
Tables & Figures
REFERENCES
Citations
Citations to this article as recorded by 
- Guided Cavity Preparation to Access an Invagination and Preserve Pulp Vitality of an Immature Maxillary Lateral Incisor With Type IIIa Dens Invaginatus: Technical Overview and a Case Report With 3‐Year Follow‐Up
Francesc Abella Sans, Venkateshbabu Nagendrababu, Nandini Suresh, Marc Garcia‐Font, Paul M. H. Dummer
International Endodontic Journal.2026; 59(4): 737. CrossRef - Cone-Beam Computed Tomography (CBCT)-Guided Non-surgical Management of Type II Dens Invaginatus in Maxillary Lateral Incisors Using Calcium Silicate-Based Materials: A Case Series
Prerna Priya
Cureus.2026;[Epub] CrossRef - A novel approach in management of Ohler’s type III dens invaginatus in maxillary lateral incisor with guided endodontics and three-dimensional printing
Jatin Gupta, Shikha Jaiswal, Shefali Sawani, Sachin Gupta
Endodontology.2026; 38(1): 103. CrossRef - Guided endodontics in the application of personalized mini-invasive treatment in clinical cases: a literature review
Shuangshuang Ren, Wanping Wang, Mingyue Cheng, Wenyue Tang, Yue Zhao, Leiying Miao
The Saudi Dental Journal.2025;[Epub] CrossRef - Navigating Calcified Challenges: Guided Endodontic Treatment of a Maxillary Central Incisor
Saide Nabavi, Sara Navabi, Iman Shiezadeh, SeyedehZahra JamaliMotlagh
Clinical Case Reports.2025;[Epub] CrossRef - Successful nonsurgical management of Oehler’s type III dens invaginatus in maxillary lateral incisor: A case report as per CARE guidelines
Anshul Sachdeva, Gurdeep Singh Gill, Adel Al Obied, Suraj Arora, Ali Y. Alsaeed, Waled Abdulmalek Alanesi, Gotam Das
Medicine.2025; 104(31): e42725. CrossRef - Guided Endodontics in Managing Root Canal Treatment for Anomalous Teeth—A Narrative Review
Pouya Sabanik, Mohammad Samiei, Shiva Tavakkoli Avval, Bruno Cavalcanti
Australian Endodontic Journal.2025; 51(3): 836. CrossRef - Efficacy of Computer-aided Static Navigation on Accuracy of Guided Endodontic Root Canal Treatment: A Systematic Review and Meta-analysis
Ashish Jain, Rahul D Rao, Meenakshi R Verma, Rishabhkumar N Jain, Shreya Sivasailam, Anandita Sinha
World Journal of Dentistry.2024; 14(11): 1004. CrossRef - Application of personalized templates in minimally invasive management of coronal dens invaginatus: a report of two cases
Mingming Li, Guosong Wang, Fangzhi Zhu, Han Jiang, Yingming Yang, Ran Cheng, Tao Hu, Ru Zhang
BMC Oral Health.2024;[Epub] CrossRef - Endodontic management of severely calcified mandibular anterior teeth using guided endodontics: A report of a case and a review of the literature
Mina Davaji, Sahar Karimpour
Saudi Endodontic Journal.2024; 14(2): 245. CrossRef - Application of an Endodontic Static Guide in Fiber Post Removal from a Compromised Tooth
Mehran Farajollahi, Omid Dianat, Samaneh Gholami, Shima Saber Tahan, Sivakumar Nuvvula
Case Reports in Dentistry.2023;[Epub] CrossRef - The Impact of the Preferred Reporting Items for Case Reports in Endodontics (PRICE) 2020 Guidelines on the Reporting of Endodontic Case Reports
Sofian Youssef, Phillip Tomson, Amir Reza Akbari, Natalie Archer, Fayjel Shah, Jasmeet Heran, Sunmeet Kandhari, Sandeep Pai, Shivakar Mehrotra, Joanna M Batt
Cureus.2023;[Epub] CrossRef - Effectiveness of guided endodontics in locating calcified root canals: a systematic review
F. Peña-Bengoa, M. Valenzuela, M. J. Flores, N. Dufey, K. P. Pinto, E. J. N. L. Silva
Clinical Oral Investigations.2023; 27(5): 2359. CrossRef - Expert consensus on digital guided therapy for endodontic diseases
Xi Wei, Yu Du, Xuedong Zhou, Lin Yue, Qing Yu, Benxiang Hou, Zhi Chen, Jingping Liang, Wenxia Chen, Lihong Qiu, Xiangya Huang, Liuyan Meng, Dingming Huang, Xiaoyan Wang, Yu Tian, Zisheng Tang, Qi Zhang, Leiying Miao, Jin Zhao, Deqin Yang, Jian Yang, Junqi
International Journal of Oral Science.2023;[Epub] CrossRef - Prevalence and morphological analysis of dens invaginatus in anterior teeth using cone beam computed tomography: A systematic review and meta-analysis
Guilherme Nilson Alves dos Santos, Manoel Damião Sousa-Neto, Helena Cristina Assis, Fabiane Carneiro Lopes-Olhê, André L. Faria-e-Silva, Matheus L. Oliveira, Jardel Francisco Mazzi-Chaves, Amanda Pelegrin Candemil
Archives of Oral Biology.2023; 151: 105715. CrossRef - Root Maturation of an Immature Dens Invaginatus Despite Unsuccessful Revitalization Procedure: A Case Report and Recommendations for Educational Purposes
Julia Ludwig, Marcel Reymus, Alexander Winkler, Sebastian Soliman, Ralf Krug, Gabriel Krastl
Dentistry Journal.2023; 11(2): 47. CrossRef - Guided Endodontics as a Personalized Tool for Complicated Clinical Cases
Wojciech Dąbrowski, Wiesława Puchalska, Adam Ziemlewski, Iwona Ordyniec-Kwaśnica
International Journal of Environmental Research and Public Health.2022; 19(16): 9958. CrossRef - Present status and future directions – Guided endodontics
Thomas Connert, Roland Weiger, Gabriel Krastl
International Endodontic Journal.2022; 55(S4): 995. CrossRef - Treatment options for dens in dente: state-of-art literature review
Volodymyr Fedak
Ukrainian Dental Journal.2022; 1(1): 37. CrossRef - Dens Invaginatus: Clinical Implications and Antimicrobial Endodontic Treatment Considerations
José F. Siqueira, Isabela N. Rôças, Sandra R. Hernández, Karen Brisson-Suárez, Alessandra C. Baasch, Alejandro R. Pérez, Flávio R.F. Alves
Journal of Endodontics.2022; 48(2): 161. CrossRef - Guided Endodontics: Static vs. Dynamic Computer-Aided Techniques—A Literature Review
Diana Ribeiro, Eva Reis, Joana A. Marques, Rui I. Falacho, Paulo J. Palma
Journal of Personalized Medicine.2022; 12(9): 1516. CrossRef - Application of CBCT Data and Three-Dimensional Printing for Endodontic Diagnosis and Treatment
Srinidhi Vishnu Ballulaya, Neha Taufin, Nenavath Deepthi, Venu Babu Devella
Nigerian Journal of Experimental and Clinical Biosciences.2021; 9(3): 206. CrossRef - When to consider the use of CBCT in endodontic treatment planning in adults
Nisha Patel, Andrew Gemmell, David Edwards
Dental Update.2021; 48(11): 932. CrossRef
 ePub Link
ePub Link Cite
CiteGuided endodontics: a case report of maxillary lateral incisors with multiple dens invaginatus
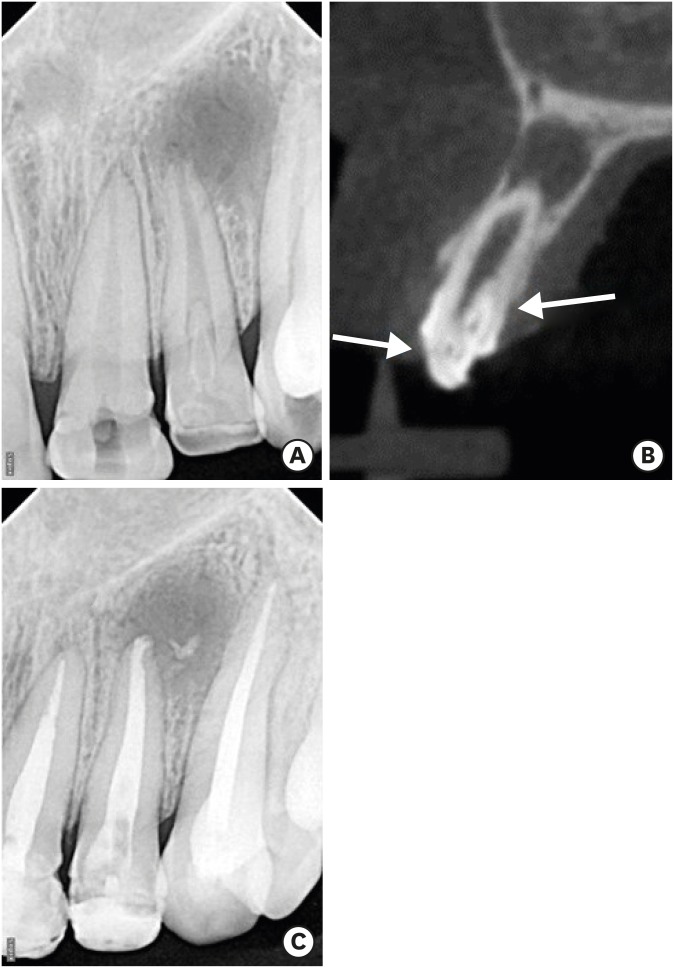
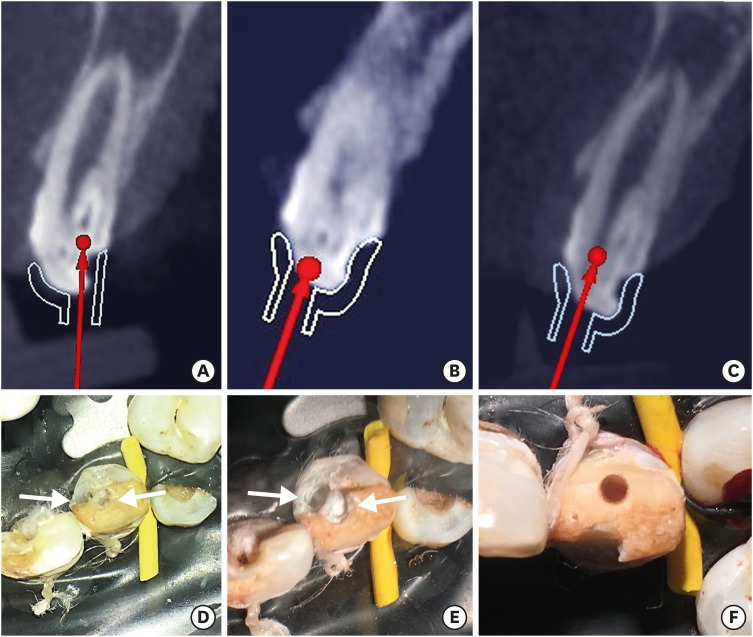
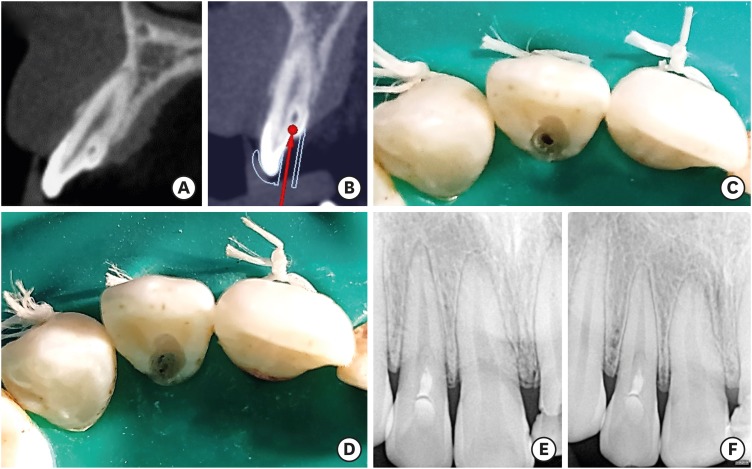

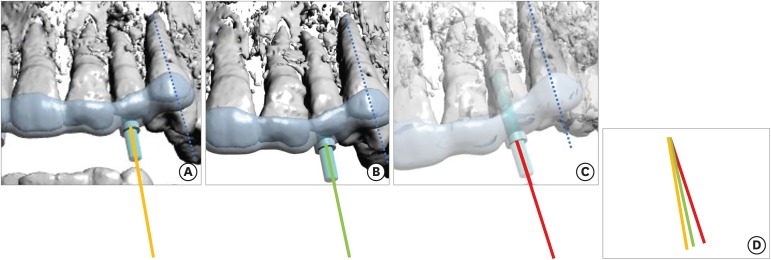
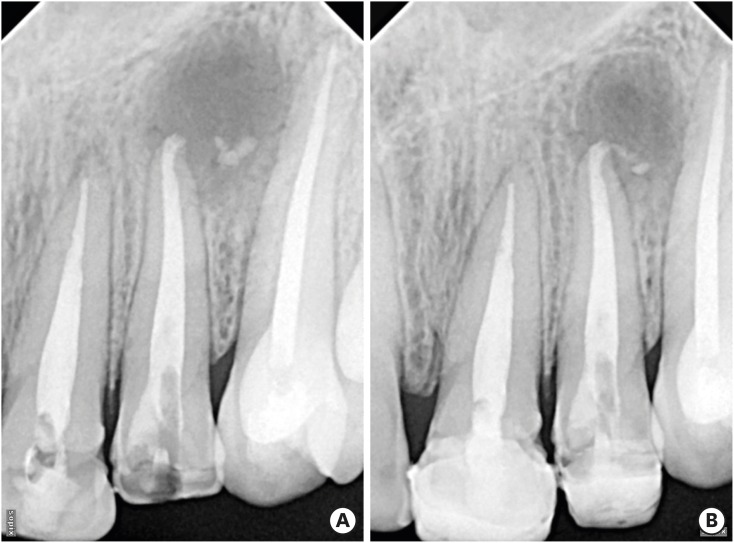
Figure 1 Representative radiographic images of the case. (A) Radiographic view of tooth #22 revealed a large periapical lesion, double dens invaginatus (DI), and a large root canal. (B) A cone-beam computed tomography image revealed that the double DI corresponded to a superficial one and a deep one extending to middle third of the root. (C) After sealing of the double DI and obturation of the root canal.
Figure 2 Radiographic and clinical images illustrating access to main canal and double dens followed by sealing of double dens with MTA. (A) Path of the bur to the deeply seated dens invaginatus (DI). (B) Path of the bur to the superficial DI. (C) Path for the bur to the main root canal. (D) Preparation of the DIs. (E) Sealing of the DIs with mineral trioxide aggregate. (F) Access to the main root canal of tooth #22.
Figure 3 Illustrations showing the Guided prophylactic management of dens invaginatus (A) Tooth #12 with one dens invaginatus (DI). (B) Path of the bur. (C) Clinical view of guided access to the DI only. (D) Mineral trioxide aggregate obturation of the DI cavity. (E) Immediate radiographic view after the procedure. (F) One-year follow-up.
Figure 4 Illustration depicting 3-dimensional (3D) printed guide. (A) The 3D endodontic guide 1 design for the deeper dens invaginatus (DI) on tooth #22 and the DI on tooth #12. (B) The 3D endodontic guide 1 in the mouth. Arrows indicates the guide for tooth #12.
Figure 5 Three guides for tooth #22. The images shown in 5A-5C were rotated to make each canine tooth parallel (blue line). (A) 3D endodontic guide planning for the superficial dens invaginatus (DI) on tooth #22 (yellow line demonstrates the direction of access). (B) The 3-dimensional (3D) endodontic guide planning for the deeper DI on tooth #22 (green line demonstrates the direction of access). (C) 3D endodontic guide planning for the main canal (red line demonstrates the direction of access). (D) Comparison of the direction of each access.
Figure 6 Intraoral periapical radiographs. (A) Immediate postoperative radiograph taken of tooth #22. (B) Radiographs taken at the follow-up visit (1 year later) showed regression of the periapical lesion in relation to tooth #22.
Figure 1
Figure 2
Figure 3
Figure 4
Figure 5
Figure 6
Guided endodontics: a case report of maxillary lateral incisors with multiple dens invaginatus

