
Articles
- Page Path
- HOME > Restor Dent Endod > Volume 44(4); 2019 > Article
-
Research Article
The effect of individualization of fiberglass posts using bulk-fill resin-based composites on cementation: an
in vitro study -
Rodrigo Barros Esteves Lins1
 , Jairo Matozinho Cordeiro2, Carolina Perez Rangel1, Thiago Bessa Marconato Antunes1, Luís Roberto Marcondes Martins1
, Jairo Matozinho Cordeiro2, Carolina Perez Rangel1, Thiago Bessa Marconato Antunes1, Luís Roberto Marcondes Martins1 -
Restor Dent Endod 2019;44(4):e37.
DOI: https://doi.org/10.5395/rde.2019.44.e37
Published online: October 18, 2019
1Department of Restorative Dentistry, Piracicaba Dental School, State University of Campinas, Piracicaba, SP, Brazil.
2Department of Prosthodontics and Periodontology, Piracicaba Dental School, University of Campinas, Piracicaba, SP, Brazil.
- Correspondence to Rodrigo Barros Esteves Lins, DDS, MSc. PhD Student, Department of Restorative Dentistry, Piracicaba Dental School, State University of Campinas, Av. Limeira, 901 Areião, Piracicaba, SP 13414-903, Brazil. rodrigowlins@hotmail.com
• Received: February 12, 2019 • Revised: September 15, 2019 • Accepted: September 15, 2019
Copyright © 2019. The Korean Academy of Conservative Dentistry
This is an Open Access article distributed under the terms of the Creative Commons Attribution Non-Commercial License (https://creativecommons.org/licenses/by-nc/4.0/) which permits unrestricted non-commercial use, distribution, and reproduction in any medium, provided the original work is properly cited.
- 1,906 Views
- 12 Download
- 6 Crossref
Abstract
-
Objectives This study evaluated the bond strength of various fiberglass post cementation techniques using different resin-based composites.
-
Materials and Methods The roots from a total of 100 bovine incisors were randomly assigned to 5 treatment groups: G1, post + Scotchbond Multi-Purpose (SBMP) + RelyX ARC luting agent; G2, relined post (Filtek Z250) + SBMP + RelyX ARC; G3, individualized post (Filtek Z250) + SBMP; G4, individualized post (Filtek Bulk-Fill) + SBMP; G5, individualized post (Filtek Bulk-Fill Flow) + SBMP. The samples were subjected to the push-out (n = 10) and pull-out (n = 10) bond strength tests. Data from the push-out bond strength test were analyzed using 2-way analysis of variance (ANOVA) with the Bonferroni post hoc test, and data from the pull-out bond strength test were analyzed using 1-way ANOVA.
-
Results The data for push-out bond strength presented higher values for G2 and G5, mainly in the cervical and middle thirds, and the data from the apical third showed a lower mean push-out bond strength in all groups. No significant difference was noted for pull-out bond strength among all groups. The most frequent failure modes observed were adhesive failure between dentine and resin and mixed failure.
-
Conclusions Fiberglass post cementation using restorative and flowable bulk-fill composites with the individualization technique may be a promising alternative to existing methods of post cementation.
INTRODUCTION
The use of intraradicular retainers in endodontically treated teeth, despite great damage to the coronal tooth structure, is necessary to achieve superior longevity of restorative treatment [1,2]. Clinically, fiberglass posts are commonly used due to aesthetic issues, but they also increase the fracture strength and allow uniform distribution of masticatory forces over the root structure due to their modulus of elasticity, which is similar to that of dentine [3,4].
Currently, several fiberglass post cementation techniques are scientifically accepted, and these are associated with an auto- or dual-cure luting agent and a self-etch or etch-and-rinse adhesive system. In some challenging clinical situations, it may be necessary to use other techniques, such as in the cases of extensive and large roots, in which it is possible to reline the fiberglass post with a resin-based composite in order to decrease the thickness of the resin cement [3,5,6,7]. The scientifically recognized techniques that are commonly performed in dental clinics are 1) fiberglass post cementation using traditional methods with a dual-cure luting agent, using a conventional adhesive system and 2) relining with conventional resin-based composites [8,9]. However, the existence of multiple fiberglass post cementation techniques, as well as the considerable variation in clinical scenarios, requires a specific level of manual ability from the professional; although this factor can be limited or neglected at certain times, it does influence treatment success.
The failure of rehabilitation using fiberglass posts is associated with root characteristics that affect operator visibility and access, as well as with the instrumentation technique and irrigation solution used, endodontic contamination [10], resin composite characteristics (for instance, a high C-factor within the root canal), resin cement thickness [11], the presence of bubbles, and intraradicular retainers [3,7,12].
In this context, an innovative technique for relining the fiberglass post could involve a bulk-fill composite as an alternative material, since its main feature is lower shrinkage stress compared to conventional resin-based composites, as well as increased translucency, which improves light penetration [13]. Therefore, the individualized fiberglass post technique with bulk-fill composites used in this study enables the elimination of extensive cementation protocols. To the best of our knowledge, no previous studies have evaluated the role of bulk-fill composites in fiberglass post cementation; the use of these composites has been described only for relined fiberglass posts [8,9].
Thus, the aim of this in vitro study was to evaluate the bond strength of different fiberglass post cementation techniques using a conventional resin-based composite, as well as restorative and flowable bulk-fill composites, as a substitute for traditional cementation.
MATERIALS AND METHODS
In this study, 100 freshly extracted and intact young bovine incisors were selected, stored in a 0.1% thymol solution, and divided randomly across the mechanical tests (push-out and pull-out bond strength) and treatment groups. All of the roots of the bovine teeth were sectioned using a double-sided diamond disc (KG Sorensen, Barueri, SP, Brazil) at the cemento-enamel junction at a length of 18 mm and a cervical root canal width of 3.5 mm. The roots were endodontically instrumented at a working length of 17 mm with K-files (Dentsply Maillefer, Ballaigues, Switzerland) up to size 40 with 1% NaOCl between each preparation step, and they were filled using gutta-percha and AH 26 Root Canal Sealer (Dentsply Maillefer) as part of the lateral condensation technique [14]. After 24 hours, 12 mm of the endodontic material was removed with #2 Gates-Glidden and #5 and #6 Largo Peeso drills (Dentsply Maillefer), and the cementation protocols proceeded with a fiberglass post #3 (Whitepost DC, FGM, Joinville, SC, Brazil). Product specifications are presented in Table 1.
Table 1
Material information evaluated in this study
ARC, adhesive resin cement; Bis-EMA, ethoxylated bisphenol A dimethacrylate; UDMA, urethane dimethacrylate; Bis-GMA, bisphenol A diglycidyl ether dimethacrylate; TEGDMA, triethyleneglycol dimethacrylate; YbF3, ytterbium fluoride; DDDMA, 1,12-dodecane dimethacrylate; EDMAB, ethyl 4-(dimethylamino)benzoate; HEMA, 2-hydroxyethyl methacrylate; EDMAB, ethyl 4-(dimethylamino)benzoate; #, lot number.
The 100 bovine incisor roots were divided into 5 groups according to the cementation protocol (Table 2): G1, post + Scotchbond Multi-Purpose (SBMP; 3M ESPE, St. Paul, MN, USA) + RelyX ARC luting agent (3M ESPE); G2, relined post (Filtek Z250, 3M ESPE) + SBMP + RelyX ARC; G3, individualized post (Filtek Z250) + SBMP; G4, individualized post (Filtek Bulk-Fill, 3M ESPE) + SBMP; G5, individualized post (Filtek Bulk-Fill Flow, 3M ESPE) + SBMP. In G2, the resin composite was manipulated onto the fiberglass post, positioned into the canal, and photoactivated for 3 seconds. The relined post was then removed from the canal and light-cured completely for 40 seconds. To attain individualization of the fiberglass posts, in G3, a resin spatula was used with the incremental technique (with a thickness of 2 mm) to insert the conventional resin composite around the fiberglass post that was positioned in the canal. Each layer was photoactivated for 40 seconds from the occlusal end. In contrast, in G4 and G5, the bulk-fill resin composite or bulk-fill flowable resin composite was inserted around the fiberglass post using the bulk-fill technique (with a thickness of 4 mm) and was photoactivated for 20 seconds from the occlusal end. The samples were subjected to the push-out (n = 10) and pull-out (n = 10) bond strength tests.
Table 2
Cementation protocol of each treatment group
After storage for 7 days in relative humidity at 37°C, 50 roots were sectioned into nine 1-mm-thick slices (3 slices from each of the cervical, middle, and apical regions) cut perpendicularly to the long axis using a high-concentration diamond disc (Buehler, Lake Bluff, IL, USA) coupled with a precision cutting machine (Isomet 1000, Buehler). The push-out bond strengths (n = 10) were determined using a universal testing machine (Instron, Norwood, MA, USA) at a speed of 1.0 mm/min, and a cylindrical metal rod was used to exert a compressive load at the centre of the post in the apico-cervical direction until bond failure occurred [15].
The push-out bond strength value in newtons (N) was converted to megapascals (MPa) through the formula A = 2π (R2 + R1) × [h2 + (R2 − R1)]0.5, where π is a constant, h is the thickness of the slice, R2 is the cervical post radius, and R1 is the apical post radius, and was then divided by the bonded interface area (mm2) [16]. The fractured samples were subjected to scanning electron microscopy (SEM) analysis to determine the failure mode.
The 50 remaining treated roots underwent the same cementation protocol (n = 10). The roots were embedded in a polystyrene resin cylinder parallel to the long insertion axis, and the fiberglass post end was fixed in an acrylic resin sphere to enable retention in another polystyrene resin cylinder. Next, a metallic hook (2.2 mm × 31 mm, Fixtil, São Paulo, SP, Brazil) was threaded onto both cylinders in order to engage each in a universal testing machine (Instron). In this machine, each cylinder underwent a tensile force at a speed of 1.0 mm/min [17]. The pull-out bond strength value in newtons (N) was converted to megapascals (MPa).
SEM was used to analyse the fracture modes of the specimens after the push-out bond strength test. The fractured surfaces were sputter-coated with gold, analysed at 15 kV (JEOL JSM-T330A, JEOL Ltd., Tokyo, Japan), and evaluated at magnifications of ×75 and ×200. The fracture modes were classified into 5 types: 1) adhesive failure between the dentine and the adhesive resin cement/resin composite; 2) adhesive failure between the adhesive resin cement/resin composite and the fiberglass post; 3) cohesive failure of the adhesive resin cement/resin composite; 4) cohesive failure of the fiberglass post; 5) mixed failure (a combination of 2 or more failure types) [18].
One sample of each group was sectioned along the longitudinal axis (in the cervical-apical direction) using a high-concentration diamond disc (Buehler) coupled with a precision cutting machine (Isomet 1000, Buehler), allowing visualization of the adhesive interface. The internal side of the sectioned specimens was polished with a silicon carbide paper (4000 grit, Buehler) and placed in an ultrasonic machine for 10 minutes (Marconi, Piracicaba, SP, Brazil). The specimens were dried for 24 hours and were sputter-coated with gold, and the cervical adhesive interfaces resulting from the different cementation protocols were analysed at ×75 magnification using SEM.
Statistical analyses were performed using SPSS version 21.0 (IBM Corp., Armonk, NY, USA). The data were tested for a normal distribution (Shapiro-Wilk test, p > 0.05) followed by the 2-way analysis of variance (ANOVA) parametric statistical test and the Bonferroni post hoc test for push-out bond strength, and the 1-way ANOVA parametric statistical test for pull-out bond strength (α = 5%).
RESULTS
The results of the test for push-out bond strength for the experimental groups are presented in Table 3. G2 and G5 presented higher values in the cervical and middle regions when compared to other groups (p < 0.001), with significant differences observed in the cervical region (p = 0.003). G3 presented the lowest results for the middle and apical regions (p = 0.023). Regarding the dentine region, it was observed that the push-out values decreased when approaching the apical region, except for G1 and G4 (p = 0.254). Regarding pull-out bond strength (Table 3), none of the groups showed a statistically significant difference (1-way ANOVA, p = 0.502).
Table 3
Bond strength values obtained by push-out and pull-out bond strength tests
Failure modes as determined using SEM observation are presented in Figure 1. Type 1 was in the majority among the failure modes in all groups tested, followed by mixed failure. Types 2, 3, and 4 occurred rarely. Images obtained using SEM for the adhesive interfaces resulting from the different treatment protocols are shown in Figure 2.
Figure 1
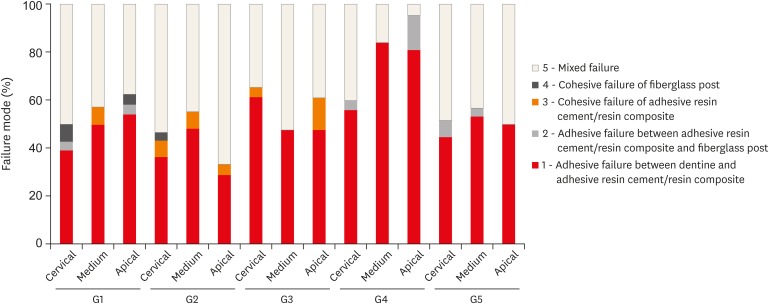
Distribution of failure modes (frequency, %) in 5 different cementation protocols and at 3 locations (the apical, middle, and cervical thirds) of the root canal dentin. The fracture modes were classified into 5 types.
G1, post + SBMP + RelyX ARC luting agent; G2, relined post (Filtek Z250) + SBMP + RelyX ARC; G3, individualized post (Filtek Z250) + SBMP; G4, individualized post (Filtek Bulk-Fill) + SBMP; G5, individualized post (Filtek Bulk-Fill-Flow) + SBMP; SBMP, Scotchbond Multi-Purpose.
Figure 2
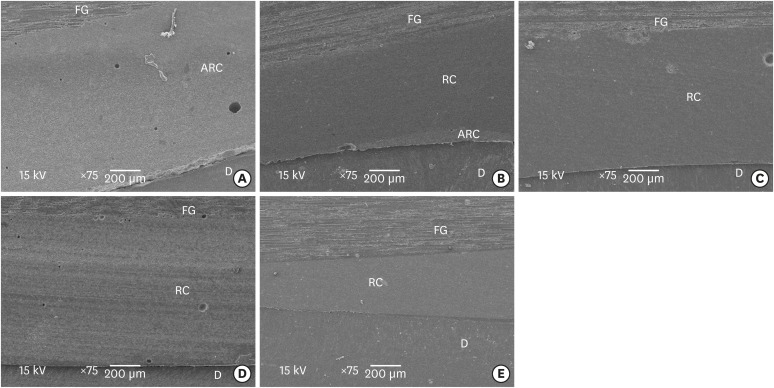
Scanning electron microscopic images of the adhesive interface present in each of the 5 groups (A, G1; B, G2; C, G3; D, G4; E, G5).
FG, fiberglass post; ARC, adhesive resin cement; RC, resin composite; D, dentin.
DISCUSSION
The present study evaluated the bond strength of fiberglass posts obtained with cementation techniques using a conventional resin-based composite, a bulk-fill composite, and adhesive resin cement. Individualization with bulk-fill composites may be a suitable alternative technique for performing fiberglass post cementation, as it replaces resin cement without affecting the bond strength when compared to conventional resin-based composite and dual-cure adhesive resin cement.
In current dentistry, the most commonly-used and scientifically accepted fiberglass post cementation technique uses a dual-cure luting agent and an etch-and-rinse adhesive system [19], and it was therefore characterized as the first control group for this study. Using a Fiberglass post for intraradicular retention in resin-based composite restorations is currently favoured as a technique for increasing fracture resistance and stress distribution across the dentin of the entire root [20]. However, in cases of a broad root canal, a relined fiberglass post technique with a resin composite is adopted in order to decrease the thickness of the adhesive resin cement layer, greatly influencing the bond strength [21], as observed in our results. However, these techniques require marked manual dexterity of the operator, implying that they could be replaced with more efficient and practical cementation techniques; apart from this issue, adhesion of different dental materials with root dentine is still challenging [16].
Gomes et al. [22] showed that cementation techniques of intraradicular retainers with fewer steps are more favourable for obtaining better bond strength between dentine and adhesive resin cement. For this reason, an innovative cementation technique using a fiberglass post with restorative or flowable bulk-fill composites was adopted, since it eliminates the necessity of using adhesive resin cement. This technique is also favoured by the adhesion characteristics of the SBMP adhesive system [23], and it serves as a simple way to introduce the resin material within the root canal. Resin-based composites present a challenge related to high polymerization shrinkage stress, characterized by the formation of polymer chains though the conversion of carbon-carbon double bonds into single bonds [24]. This transformation induces the accumulation of stress in the adhesive layer during the polymerization process, even apart from the technique of resin-based insertion promoting higher marginal tension [24]; however, the new generation of resin-based composites (bulk-fill composites) has promising properties, such as low polymerization shrinkage stress, suitability for high C-factor cavities, the possibility of inserting a single 4–5-mm layer, greater light penetration along the thickness of the resin cement, and shorter photopolymerization time [25]. In general, the differences in retention observed among the treatment groups for push-out bond strength indicate favourable results for these resin-based materials with low polymerization shrinkage stress. This mainly applies to the bulk fill flowable group (G5), which, due to its low viscosity and appealing mechanical properties [26,27], constitutes a promising technique for individualization of a fiberglass post with a resin composite, allowing it to reach the entire treated surface and induce higher bond strength along the root canal.
Evaluation of the bond strength of intraradicular retainers can be accomplished using various mechanical tests [16,17,28]. In the current study, the push-out and pull-out bond strength tests were conducted according to typical fiberglass post cementation protocols in order to evaluate the bond strength obtained through the different methodologies under study. Push-out bond strength is most commonly used for in vitro studies involving the evaluation of specific bond strength between different root canal regions [16]. In this study, the higher push-out bond strength of the cervical and middle thirds observed compared to the apical third, with significant differences for G2, G3, and G5, can potentially be explained by the radicular dentine morphology, since variation in tubular density directly influences hybrid layer thickness and, therefore, bond strength [29]. These structural variations, as well as the technical and operational limitations on fiberglass post cementation, can be suggested as reasons for failure mode occurrence for different root canal regions [3,7,10,11,12]. In our study, a prevalence of adhesive failure between dentine and adhesive resin cement or resin composite and mixed failure was observed, in accordance with the scientific literature [18,30]. Cohesive failure of the fiberglass post occurred rarely due to the post having similar mechanical properties to that of dentinal tissue, positively influencing its biomechanical behaviour [31]. Similarly, a low frequency of cohesive failure of the adhesive resin cement or resin composite was observed [32]. An interesting result was the absence of this failure pattern in G4 and G5, most likely due to the bulk-fill resin composite presenting a lower elastic modulus [25]. Another failure mode rarely observed was type 2, most likely because the push-out bond strength between the fiberglass post and the resin material was increased in all treatment groups due to application of a silane agent and adhesive, as observed by Machado et al. [33].
Pull-out bond strength has been used to quantify the fiberglass post bond strength in the entire root canal using parallel extrusion forces [17]. An important calculation that can be made using the pull-out test is frictional retention (the total contact area between the fiberglass post surface and the cementing material or radicular dentin), which has been adopted as a clinical measurement of the cementation technique because axial loading is the predominant form of load on clinical restorations and induces debonding as a failure mode [21,34]. Nevertheless, further long-term and clinical studies are required to validate this new technique.
CONCLUSIONS
Fiberglass post cementation using restorative and flowable bulk-fill composites via the individualization of the fiberglass post displayed similar bond strength to that of a conventional resin-based composite and an adhesive resin cement. The simplified technique achieved using bulk-fill composites may be a promising alternative to current dental clinical procedures.
-
Funding: The authors acknowledge the financial support of FAPESP (#2016/17701-0).
-
Conflict of Interest: No potential conflict of interest relevant to this article was reported.
-
Author Contributions:
Conceptualization: Lins RBE, Martins LRM.
Data curation: Rangel CP, Antunes TBM.
Formal analysis: Cordeiro JM.
Funding acquisition: Martins LRM.
Investigation: Lins RBE.
Methodology: Rangel C, Antunes TBM.
Project administration: Lins RBE.
Resources: Martins LRM.
Supervision: Lins RBE, Martins LRM.
Writing - original draft: Lins RBE.
Writing - review & editing: Cordeiro JM, Martins LRM.
- 1. Keul C, Köhler P, Hampe R, Roos M, Stawarczyk B. Glass fiber post/composite core systems bonded to human dentin: analysis of tensile load vs calculated tensile strength of various systems using pull-out tests. J Adhes Dent 2016;18:247-256.PubMed
- 2. Rezende EC, Gomes GM, Szesz AL, da Silveira Bueno CE, Reis A, Loguercio AD. Effects of dentin moisture on cementation of fiber posts to root canals. J Adhes Dent 2016;18:29-34.PubMed
- 3. Goracci C, Ferrari M. Current perspectives on post systems: a literature review. Aust Dent J 2011;56(Supplement 1):77-83.ArticlePubMed
- 4. Santos-Filho PC, Veríssimo C, Soares PV, Saltarelo RC, Soares CJ, Marcondes Martins LR. Influence of ferrule, post system, and length on biomechanical behavior of endodontically treated anterior teeth. J Endod 2014;40:119-123.ArticlePubMed
- 5. de Souza NC, Marcondes ML, da Silva D, Borges GA, Júnior LB, Spohr AM. Relined fiberglass post: effect of luting length, resin cement, and cyclic loading on the bond to weakened root dentin. Oper Dent 2016;41:e174-e182.ArticlePubMedPDF
- 6. Gruber YL, Bakaus TE, Gomes OM, Reis A, Gomes GM. Effect of dentin moisture and application mode of universal adhesives on the adhesion of glass fiber posts to root canal. J Adhes Dent 2017;19:385-393.PubMed
- 7. Zarpellon DC, Szesz AL, Loguercio AD, Arrais CA. Effect of sonic application of universal adhesive systems on bond strength of fiber posts to root canal. J Adhes Dent 2016;18:493-499.PubMed
- 8. Anchieta RB, Rocha EP, Almeida EO, Freitas AC Jr, Martin M Jr, Martini AP, Archangelo CM, Ko CC. Influence of customized composite resin fibreglass posts on the mechanics of restored treated teeth. Int Endod J 2012;45:146-155.ArticlePubMed
- 9. Conde DM, Rodrigues VP, Carvalho Souza SF, Bauer JR, Bramante FS, Linares Lima SN, Filho EM, Bandeca MC, de Mendonça AA, Lima DM. Influence of relining post on the bond strength of resin cements. J Contemp Dent Pract 2015;16:559-564.ArticlePubMed
- 10. Santana FR, Soares CJ, Silva JA, Alencar AH, Renovato SR, Lopes LG, Estrela C. Effect of instrumentation techniques, irrigant solutions and artificial accelerated aging on fiberglass post bond strength to intraradicular dentin. J Contemp Dent Pract 2015;16:523-530.ArticlePubMed
- 11. Grandini S, Goracci C, Monticelli F, Borracchini A, Ferrari M. SEM evaluation of the cement layer thickness after luting two different posts. J Adhes Dent 2005;7:235-240.PubMed
- 12. Fernandes AS, Shetty S, Coutinho I. Factors determining post selection: a literature review. J Prosthet Dent 2003;90:556-562.ArticlePubMed
- 13. Rosatto CM, Bicalho AA, Veríssimo C, Bragança GF, Rodrigues MP, Tantbirojn D, Versluis A, Soares CJ. Mechanical properties, shrinkage stress, cuspal strain and fracture resistance of molars restored with bulk-fill composites and incremental filling technique. J Dent 2015;43:1519-1528.ArticlePubMed
- 14. Marques EF, Bueno CE, Veloso HH, Almeida G, Pinheiro SL. Influence of instrumentation techniques and irrigating solutions on bond strength of glass fiber posts to root dentin. Gen Dent 2014;62:50-53.
- 15. Goracci C, Grandini S, Bossù M, Bertelli E, Ferrari M. Laboratory assessment of the retentive potential of adhesive posts: a review. J Dent 2007;35:827-835.ArticlePubMed
- 16. Shafiei F, Mohammadparast P, Jowkar Z. Adhesion performance of a universal adhesive in the root canal: effect of etch-and-rinse vs. self-etch mode. PLoS One 2018;13:e0195367.ArticlePubMedPMC
- 17. de Souza Batista VE, Vechiato-Filho AJ, Cesar PF, Coelho Goiato M, Cipriano Rangel E, Piza Pellizzer E, Ramos Verri F, Barão VA, Dos Santos DM. Surface characterization of a glass fiber post after nonthermal plasma treatment with hexamethyldisiloxane. J Adhes Dent 2017;19:525-533.
- 18. Mobarak E, Seyam R. Interfacial nanoleakage and bonding of self-adhesive systems cured with a modified-layering technique to dentin of weakened roots. Oper Dent 2013;38:E154-E165.ArticlePubMedPDF
- 19. Sarkis-Onofre R, Jacinto RC, Boscato N, Cenci MS, Pereira-Cenci T. Cast metal vs. glass fibre posts: a randomized controlled trial with up to 3 years of follow up. J Dent 2014;42:582-587.ArticlePubMed
- 20. Barcelos LM, Bicalho AA, Veríssimo C, Rodrigues MP, Soares CJ. Stress distribution, tooth remaining strain, and fracture resistance of endodontically treated molars restored without or with one or two fiberglass posts and direct composite resin. Oper Dent 2017;42:646-657.ArticlePubMedPDF
- 21. Macedo VC, Faria e Silva AL, Martins LR. Effect of cement type, relining procedure, and length of cementation on pull-out bond strength of fiber posts. J Endod 2010;36:1543-1546.ArticlePubMed
- 22. Gomes GM, Gomes OM, Reis A, Gomes JC, Loguercio AD, Calixto AL. Effect of operator experience on the outcome of fiber post cementation with different resin cements. Oper Dent 2013;38:555-564.ArticlePubMedPDF
- 23. Caixeta RV, Guiraldo RD, Kaneshima EN, Barbosa AS, Picolotto CP, Lima AE, Gonini Júnior A, Berger SB. Push-out bond strength of restorations with bulk-fill, flow, and conventional resin composites. Sci World J 2015;2015:452976.ArticlePubMedPMCPDF
- 24. Lins RB, Aristilde S, Osório JH, Cordeiro CM, Yanikian CR, Bicalho AA, Stape TH, Soares CJ, Martins LR. Biomechanical behaviour of bulk-fill resin composites in class II restorations. J Mech Behav Biomed Mater 2019;98:255-261.ArticlePubMed
- 25. Leprince JG, Palin WM, Vanacker J, Sabbagh J, Devaux J, Leloup G. Physico-mechanical characteristics of commercially available bulk-fill composites. J Dent 2014;42:993-1000.ArticlePubMed
- 26. Francis AV, Braxton AD, Ahmad W, Tantbirojn D, Simon JF, Versluis A. Cuspal flexure and extent of cure of a bulk-fill flowable base composite. Oper Dent 2015;40:515-523.ArticlePubMedPDF
- 27. Marovic D, Tauböck TT, Attin T, Panduric V, Tarle Z. Monomer conversion and shrinkage force kinetics of low-viscosity bulk-fill resin composites. Acta Odontol Scand 2015;73:474-480.ArticlePubMed
- 28. Castellan CS, Santos-Filho PC, Soares PV, Soares CJ, Cardoso PE. Measuring bond strength between fiber post and root dentin: a comparison of different tests. J Adhes Dent 2010;12:477-485.PubMed
- 29. Ferrari M, Mannocci F, Vichi A, Cagidiaco MC, Mjör IA. Bonding to root canal: structural characteristics of the substrate. Am J Dent 2000;13:255-260.PubMed
- 30. Park JS, Lee JS, Park JW, Chung WG, Choi EH, Lee Y. Comparison of push-out bond strength of fiber-reinforced composite resin posts according to cement thickness. J Prosthet Dent 2017;118:372-378.ArticlePubMed
- 31. Santos-Filho PC, Castro CG, Silva GR, Campos RE, Soares CJ. Effects of post system and length on the strain and fracture resistance of root filled bovine teeth. Int Endod J 2008;41:493-501.ArticlePubMed
- 32. de Assis FS, Lima SN, Tonetto MR, Bhandi SH, Pinto SC, Malaquias P, Loguercio AD, Bandéca MC. Evaluation of bond strength, marginal integrity, and fracture strength of bulk- vs incrementally-filled restorations. J Adhes Dent 2016;18:317-323.PubMed
- 33. Machado FW, Bossardi M, Ramos TS, Valente LL, Münchow EA, Piva E. Application of resin adhesive on the surface of a silanized glass fiber-reinforced post and its effect on the retention to root dentin. J Endod 2015;41:106-110.ArticlePubMed
- 34. Nova V, Karygianni L, Altenburger MJ, Wolkewitz M, Kielbassa AM, Wrbas KT. Pull-out bond strength of a fibre-reinforced composite post system luted with self-adhesive resin cements. J Dent 2013;41:1020-1026.ArticlePubMed
REFERENCES
Tables & Figures
REFERENCES
Citations
Citations to this article as recorded by 
- EVALUATION OF PUSH-OUT BOND STRENGTH OF GLASS FIBER POSTS USING DIFFERENT LUTING CEMENTS
Jannah Mohammed, Maha Agha
BULLETIN OF STOMATOLOGY AND MAXILLOFACIAL SURGERY.2025; : 274. CrossRef - Effects of a relined fiberglass post with conventional and self-adhesive resin cement
Wilton Lima dos Santos Junior, Marina Rodrigues Santi, Rodrigo Barros Esteves Lins, Luís Roberto Marcondes Martins
Restorative Dentistry & Endodontics.2024;[Epub] CrossRef - Fracture resistance of weakened roots restored with relined or milled CAD-CAM glass fiber posts
Belizane das Graças Oliveira MAIA, Thais da Silva Alves SANTOS, Cláudio Antonio Talge CARVALHO, Francielle Silvestre VERNER, Rafael Binato JUNQUEIRA
Dental Materials Journal.2023; 42(1): 92. CrossRef - Evaluation of pretreatments on intra‐radicular dentin bond strength of self‐adhesive resin cements
Marina Rodrigues Santi, Rodrigo Barros Esteves Lins, Beatriz Ometto Sahadi, Luís Roberto Marcondes Martins, Jorge Rodrigo Soto‐Montero
Journal of Esthetic and Restorative Dentistry.2022; 34(7): 1051. CrossRef - Comparison of the Mechanical Properties and Push-out Bond Strength of Self-adhesive and Conventional Resin Cements on Fiber Post Cementation
MR Santi, RBE Lins, BO Sahadi, JR Soto-Montero, LRM Martins
Operative Dentistry.2022; 47(3): 346. CrossRef - Glass fiber posts
Renata Pereira, Rodrigo Barros Esteves Lins, Victória Castelan Rodrigues, Débora Alves Nunes Leite Lima, Luís Roberto Marcondes Martins, Flávio Henrique Baggio Aguiar
Brazilian Journal of Oral Sciences.2020; 19: e207508. CrossRef
 ePub Link
ePub Link Cite
Cite- Figure
-
- Related articles
-
- Effect of high irradiance and short exposure curing time on the fracture toughness of bulk-fill resin-based composite: an in vitro study
- The influence of bioactive glass (BGS-7) on enamel remineralization: an in vitro study
- Cleaning protocols to enhance bond strength of fiberglass posts on root canals filled with bioceramic sealer: an in vitro comparative study
- The effect of limonene extract on the adhesion of different endodontic cements to root dentin: an in vitro experimental study
The effect of individualization of fiberglass posts using bulk-fill resin-based composites on cementation: an in vitro study
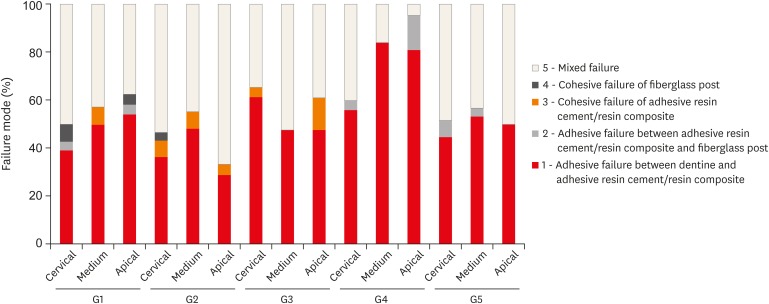
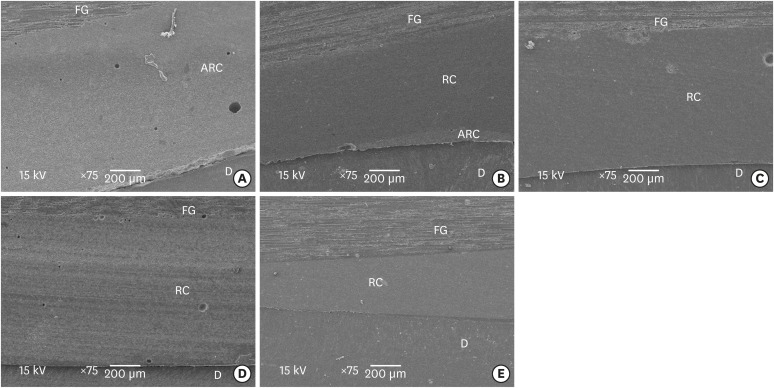
Figure 1 Distribution of failure modes (frequency, %) in 5 different cementation protocols and at 3 locations (the apical, middle, and cervical thirds) of the root canal dentin. The fracture modes were classified into 5 types.G1, post + SBMP + RelyX ARC luting agent; G2, relined post (Filtek Z250) + SBMP + RelyX ARC; G3, individualized post (Filtek Z250) + SBMP; G4, individualized post (Filtek Bulk-Fill) + SBMP; G5, individualized post (Filtek Bulk-Fill-Flow) + SBMP; SBMP, Scotchbond Multi-Purpose.
Figure 2 Scanning electron microscopic images of the adhesive interface present in each of the 5 groups (A, G1; B, G2; C, G3; D, G4; E, G5).FG, fiberglass post; ARC, adhesive resin cement; RC, resin composite; D, dentin.
Figure 1
Figure 2
The effect of individualization of fiberglass posts using bulk-fill resin-based composites on cementation: an in vitro study
Material information evaluated in this study
| Material | Description | Composition | Shade | Manufacturer |
|---|---|---|---|---|
| Filtek Z250 | Universal restorative resin composite | Bis-EMA, UDMA, Bis-GMA, TEGDMA, silane-treated ceramic, aluminum oxide (#81465) | A2 | 3M ESPE, St. Paul, MN, USA |
| Filtek Bulk Fill | Restorative bulk-fill resin composite | Aromatic urethane dimethacrylate, YbF3, UDMA, silane-treated ceramic, silica and zirconia, DDDMA, water, EDMAB, benzotriazole, titanium dioxide (#N685666) | A2 | |
| Filtek Bulk Fill Flow | Restorative flowable bulk-fill resin composite | UDMA, Bis-EMA, YbF3, Bis-GMA, TEGDMA, silane-treated ceramic, substituted dimethacrylate, benzotriazole, ethyl 4-(dimethylamino) benzoate (#N706754) | A2 | |
| Ceramic Primer | Silane agent | Ethyl alcohol, water, methacryloxypropyltrimethoxysilane (#N699035) | - | |
| Scotchbond Multi–Purpose | Activator | Ethyl alcohol (#N708060) | - | |
| Primer | Water, HEMA, copolymer of acrylic and itaconic acids (#1801700484) | - | ||
| Catalyst | Bis-GMA, HEMA, triphenylantimony, triphenylphosphine, hydroquinone (#N562953) | - | ||
| Adhesive | Bis-GMA, HEMA, triphenylantimony (#N808224) | - | ||
| RelyX ARC (ARC) | Adhesive resin cement | Paste A: Bis-GMA, TEGDMA, silane-treated ceramic and silica, reacted polycaprolactone polymer, 2-benzotriazolyl-4-methylphenol, EDMAB, 4-(dimethylamino)-benzeneethanol | A1 | |
| Paste B: Bis-GMA, TEGDMA, silane-treated ceramic and silica, reacted polycaprolactone polymer, 2-benzotriazolyl-4-methylphenol, benzoyl peroxide (#N696957) |
ARC, adhesive resin cement; Bis-EMA, ethoxylated bisphenol A dimethacrylate; UDMA, urethane dimethacrylate; Bis-GMA, bisphenol A diglycidyl ether dimethacrylate; TEGDMA, triethyleneglycol dimethacrylate; YbF3, ytterbium fluoride; DDDMA, 1,12-dodecane dimethacrylate; EDMAB, ethyl 4-(dimethylamino)benzoate; HEMA, 2-hydroxyethyl methacrylate; EDMAB, ethyl 4-(dimethylamino)benzoate; #, lot number.
Cementation protocol of each treatment group
| Group | Technique | Cementation protocol |
|---|---|---|
| G1 | Fiberglass post + SBMP + ARC | 1. Apply 35% phosphoric acid to the fiberglass post; |
| 2. Rinse with water, then dry; | ||
| 3. Apply Ceramic Primer, followed by a 5-minute wait; | ||
| 4. Apply bond with a disposable brush; perform strong volatilization and photoactivation for 20 seconds; | ||
| 5. Acid etch the canal with 35% phosphoric acid for 15 seconds; | ||
| 6. Rinse for 15 seconds with water; | ||
| 7. Dry with a paper point; | ||
| 8. Apply SBMP with a disposable brush for each material (activator, primer, and catalyst), followed by removable of any excess with a paper point; | ||
| 9. Manipulate and apply RelyX ARC into the canal with a Centrix syringe; | ||
| 10. Position the Fiberglass post into the canal with digital pressure; | ||
| 11. Wait for 5 minutes, then light-cure the resin (VALO, Ultradent, South Jordan, UT, USA) for 40 seconds for each side. | ||
| G2 | Relined fiberglass post (Filtek Z250 resin composite) + SBMP + ARC | 1. Apply 35% phosphoric acid to the fiberglass post; |
| 2. Rinse with water, then dry; | ||
| 3. Apply Ceramic Primer, followed by a 5-minute wait; | ||
| 4. Apply bond with a disposable brush; perform strong volatilization and photoactivation for 20 seconds; | ||
| 5. Apply water-soluble lubricant to the canal; | ||
| 6. Manipulate the resin composite onto the fiberglass post and position it into the canal; | ||
| 7. Perform photoactivation for 3 seconds, then remove from the canal for 40 seconds to complete the light-curing process; | ||
| 8. Rinse and dry the canal; | ||
| Repeat steps 5–11 from the G1 cementation protocol. | ||
| G3 | Individualized fiberglass post (Filtek Z250 resin composite) + SBMP | 1. Apply 35% phosphoric acid to the fiberglass post; |
| 2. Rinse with water, then dry; | ||
| 3. Apply Ceramic Primer, followed by a 5-minute wait; | ||
| 4. Apply bond with a disposable brush; perform strong volatilization and photoactivation for 20 seconds; | ||
| 5. Acid etch the canal with 35% phosphoric acid for 15 seconds; | ||
| 6. Rinse for 15 seconds with water; | ||
| 7. Dry with a paper point; | ||
| 8. Apply primer and adhesive with a disposable brush; perform volatilization and photoactivation for 20 seconds; | ||
| 9. Position the Fiberglass post into the canal and insert the conventional resin composite with a resin spatula using the incremental technique (with a thickness of 2 mm); | ||
| 10. Perform occlusal photoactivation of each layer for 40 seconds. | ||
| G4 | Individualized fiberglass post (Filtek Bulk Fill resin composite) + SBMP | Repeat the G3 cementation protocol (above), with the exception of: |
| 9. Position the Fiberglass post into the canal and insert the bulk-fill resin composite with a resin spatula using the bulk-fill technique (with a thickness of 4 mm); | ||
| 10. Perform occlusal photoactivation for 20 seconds from the occlusal end. | ||
| G5 | Individualized fiberglass post (Filtek Bulk Fill Flow resin composite) + SBMP | Repeat the G3 cementation protocol (above), with the exception of: |
| 9. Position the Fiberglass post into the canal and insert the bulk-fill flow resin composite using the bulk technique (with a thickness of 4 mm); | ||
| 10. Perform occlusal photoactivation for 20 seconds from the occlusal end. |
SBMP, Scotchbond Multi–Purpose; ARC, Adhesive resin cement.
Bond strength values obtained by push-out and pull-out bond strength tests
| Group | Push-out by canal root region | Pull-out | ||
|---|---|---|---|---|
| Cervical | Medium | Apical | ||
| 1 | 4.38 ± 1.13Ac | 4.62 ± 1.47Ab | 4.67 ± 2.08Aa | 4.77 ± 1.04a |
| 2 | 7.89 ± 2.68Aa | 7.06 ± 1.95Aa | 4.90 ± 1.80Ba | 4.94 ± 0.69a |
| 3 | 4.58 ± 2.34Ac | 3.01 ± 1.76Bc | 2.76 ± 1.38Bb | 4.94 ± 1.00a |
| 4 | 4.48 ± 1.41Ac | 4.53 ± 2.12Ab | 3.82 ± 2.25Aab | 5.59 ± 1.01a |
| 5 | 6.18 ± 2.61Ab | 6.26 ± 2.49Aa | 4.53 ± 2.98Ba | 4.83 ± 1.41a |
Data are presented as mean ± standard deviation (unit: MPa). Different uppercase letters indicate significant differences between root regions in the same row. Different lowercase letters indicate significant differences between groups in the same column (p < 0.05).
Table 1 Material information evaluated in this study
ARC, adhesive resin cement; Bis-EMA, ethoxylated bisphenol A dimethacrylate; UDMA, urethane dimethacrylate; Bis-GMA, bisphenol A diglycidyl ether dimethacrylate; TEGDMA, triethyleneglycol dimethacrylate; YbF3, ytterbium fluoride; DDDMA, 1,12-dodecane dimethacrylate; EDMAB, ethyl 4-(dimethylamino)benzoate; HEMA, 2-hydroxyethyl methacrylate; EDMAB, ethyl 4-(dimethylamino)benzoate; #, lot number.
Table 2 Cementation protocol of each treatment group
SBMP, Scotchbond Multi–Purpose; ARC, Adhesive resin cement.
Table 3 Bond strength values obtained by push-out and pull-out bond strength tests
Data are presented as mean ± standard deviation (unit: MPa). Different uppercase letters indicate significant differences between root regions in the same row. Different lowercase letters indicate significant differences between groups in the same column (

