
Articles
- Page Path
- HOME > Restor Dent Endod > Volume 43(3); 2018 > Article
- Case Report Management of a permanent maxillary first molar with unusual crown and root anatomy: a case report
-
Prateeksha Chowdhry
 , Pallavi Reddy, Mamta Kaushik
, Pallavi Reddy, Mamta Kaushik -
Restor Dent Endod 2018;43(3):e35.
DOI: https://doi.org/10.5395/rde.2018.43.e35
Published online: August 7, 2018
Department of Conservative Dentistry and Endodontics, Army College of Dental Sciences, Secunderabad, TS, India.
- Correspondence to Prateeksha Chowdhry, BDS. Post Graduate Student, Department of Conservative Dentistry and Endodontics, Army College of Dental Sciences, Jai Jawahar Nagar, Chennapur, CRPF Road, Secunderabad, TS, 500087, India. ginnzz@gmail.com
• Received: April 25, 2018 • Accepted: July 4, 2018
Copyright © 2018. The Korean Academy of Conservative Dentistry
This is an Open Access article distributed under the terms of the Creative Commons Attribution Non-Commercial License (https://creativecommons.org/licenses/by-nc/4.0/) which permits unrestricted non-commercial use, distribution, and reproduction in any medium, provided the original work is properly cited.
- 2,268 Views
- 10 Download
- 2 Crossref
Abstract
- The aim of this article was to showcase the endodontic management of a maxillary first molar with an unusual crown and root anatomy. Clinical diagnosis of the roots and root canal configuration was confirmed by a cone-beam computed tomography (CBCT) and the detection of the canals was made using a dental operating microscope. CBCT images revealed the presence of 5 roots with Vertucci type I canal configuration in all, except, in the middle root which had 2 canals with type IV configuration. The 6 canal orifices were clinically visualized under the dental operating microscope. Clinicians should familiarize themselves with the latest technologies to get additional information in endodontic practice in order to enhance the outcomes of endodontic therapy.
INTRODUCTION
It is of utmost importance to have a thorough knowledge and understanding of the anatomical variations for a successful endodontic treatment outcome. Inability to detect and treat these variations is one of the reasons for failure of endodontic treatment because they pose a challenge for diagnosis and successful treatment outcome [1]. The morphology of permanent maxillary first molar has been reviewed extensively and reported in the literature. (Table1) [2,3,4,5,6,7,8,9,10,11,12]
Table 1
Summary of case reports of maxillary first molars with multiple canals
| Root configuration | No. of canals | Canal configuration | Reference | ||
|---|---|---|---|---|---|
| (MB) | (DB) | (P) | |||
| 3 | 7 | 3 | 2 | 2 | Kottor et al. (2010) [2] |
| 3 | 8 | 3 | 3 | 2 | Kottor et al. (2011) [3] |
| 3 | 6 | 2 | 2 | 2 | Kaushik and Mehra (2013) [4] |
| 6 | 6 | 3 | 1 | 2 | Kaushik and Mehra (2013) [4] |
| 3 | 5 | 2 | 1 | 2 | Shetty et al. (2014) [5] |
| 3 | 5 | 2 | 1 | 2 | Umer et al. (2014) [6] |
| 4 | 5 | 3 | 2 | 2 | Sharma et al. (2014) [7] |
| 3 | 7 | 3 | 2 | 2 | Kumar (2014) [8] |
| 3 | 7 | 3 | 2 | 2 | Munavalli et al. (2015) [9] |
| 3 | 8 | 3 | 3 | 2 | Almeida et al. (2015) [10] |
| 3 | 6 | 3 | 2 | 1 | Al-Habboubi and Al-Wasi (2016) [11] |
| 3 | 7 | 3 | 2 | 2 | Rodrigues et al. (2017) [12] |
Important variations may be either in the form of anomalous cusps or increased number of roots, or both [13]. The majority of variations occur in the crown of a tooth [14] and the concomitant occurrence of morphological variation in both the crown and roots of a tooth is rare [13]. The incidence of a second mesiobuccal canal in the maxillary first molar ranges from 18%–96.1% [15,16]. Other variations include 1 [17], 2 [18], and 5 [19] roots, and an unusual morphology of root canal systems within individual roots. The presence of such anomalies may be of functional and clinical significance. Formative variations in teeth are rare, with etiopathology being primarily polygenic along with secondary environmental influences [20].
To the best of authors' information, the present case is a unique corono-radicular variation of a maxillary first molar. The presence of 7 cusps, 5 roots, and 6 canals were confirmed with the help of a cone-beam computed tomography (CBCT).
CASE REPORT
A 35-year-old male patient reported to the Department of Conservative Dentistry and Endodontics, Army College of Dental Sciences, Telangana, India, with the chief complaint of mild intermittent pain in relation to left posterior tooth region in the maxilla for 10 days. The pain intensified mildly by thermal stimuli and on mastication. History revealed intermittent pain in relation to the same tooth with hot and cold stimuli for the past 2 months. No relevant medical history was elicited.
Clinical examination revealed a deep carious lesion on the mesial aspect of maxillary left first molar (tooth #26) whose crown had an abnormally large size with 7 cusps (Figure 1A). The tooth was tender to percussion. There was no tenderness on palpation of the buccal and palatal aspect of the tooth. There was no mobility and the periodontal probing all around the tooth was found to be well within the physiological limits. Vitality testing of tooth #26 with heat and cold elicited an intense lingering pain, and on using an electric pulp tester (Gentle Pulse Analog Pulp Tester, Parkell, Edgewood, NY, USA), it gave no response.
Figure 1
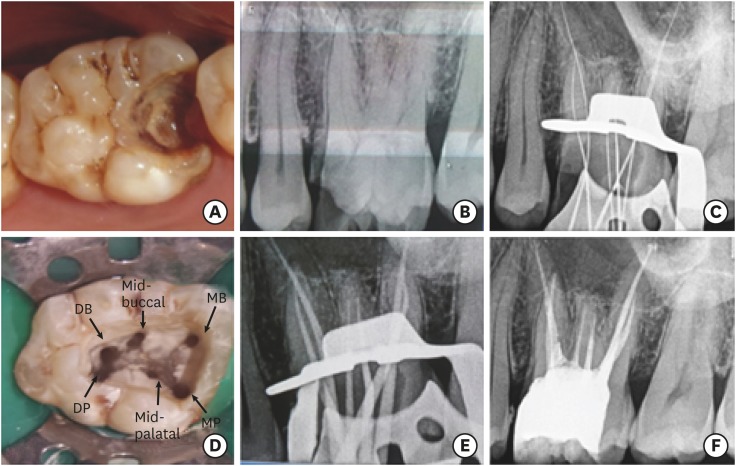
(A) Preoperative clinical view, abnormally large crown, with 7 cusps and mesio-occlusal caries; (B) Preoperative intraoral radiograph showing at least 5 roots; (C) Working length confirmed through radiograph; (D) Six canal orifices as seen under dental operating microscope; (E and F) master cone radiograph and obturation, respectively.
DB, distobuccal canal; DP, distopalatal canal; MB, mesiobuccal canal; MP, mesiopalatal canal.
A preoperative intraoral periapical radiograph revealed mesio-occlusal radiolucency approaching the pulp space and an unusual anatomic configuration of the root suggesting the presence of at least 5 roots, 3 buccal, and 2 palatal (Figure 1B). From the clinical and radiographic findings, a diagnosis of symptomatic irreversible pulpitis with symptomatic apical periodontitis in relation to tooth #26 was made and endodontic treatment was suggested to the patient.
Since the pre-operative radiograph did not clearly reveal the morphology of the root canal system, a single volume CBCT scan (NewTom 5G, Cefla S.C., Verona, Italy) was advised to confirm the number of roots and the internal canal morphology of the tooth before initiating the endodontic treatment. It was ascertained through the CBCT scans that the tooth had 5 roots (Figure 2A and 2B), 2 buccal, 2 palatal, and 1 middle root, extending buccolingually as a single flat and broad root.
Figure 2
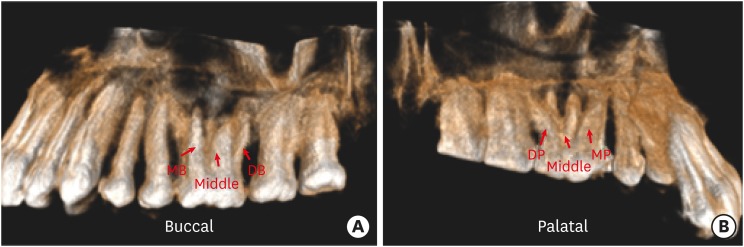
(A) Three-dimensional single volume cone-beam computed tomography images showing the (A) mesiobuccal, distobuccal, and middle root on the buccal aspect, and (B) mesiopalatal, distopalatal, and the middle root from the palatal aspect.
DB, distobuccal canal; MB, mesiobuccal canal; DP, distopalatal canal; MP, mesiopalatal canal.
Each root had one canal except in the middle root which had 2 canals. The root canals in the mesiobuccal, distobuccal, distopalatal, and mesiopalatal showed Vertucci's type I canal configuration, whereas the 2 canals in the middle root showed Vertucci's type IV canal configuration (Figure 3A-3F).
Figure 3
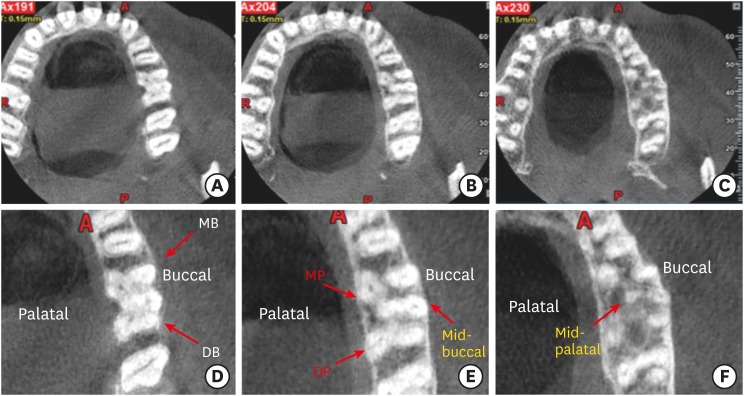
Cone-beam computed tomography (CBCT) images of tooth #26 showing the axial sections at the (A) cervical, (B) middle, and (C) apical level. Enlarged axial section CBCT images at the (D) cervical, (E) middle, and (F) apical level showing 5 roots and 6 canals.
DB, distobuccal canal; MB, mesiobuccal canal; DP, distopalatal canal; MP, mesiopalatal canal.
A posterior superior alveolar (PSA) block was administered by injecting 1.8 mL (52.3 mg) of 2% lignocaine containing 1:80,000 epinephrine (Lignox 2% ADR INJ, Indoco Remedies Ltd. (Warren, Pharma), Mumbai, MH, India) followed by rubber dam isolation. The caries was excavated using large BR #31 round bur (Mani, Inc., Utsunomiya, Japan) followed by a pre-endodontic buildup of the mesial wall using composite (Spectrum Composite, Dentsply, Weybridge, Surrey, United Kingdom). An endodontic access cavity was established using Endo Access bur #3 (Dentsply Maillefer, Tulsa, OK, USA). Clinical examination with a DG-16 endodontic explorer (GDC, CE, Hoshiarpur, PB, India) revealed 6 canal orifices. During examination under a dental operating microscope (600 Operating Microscope, Seiler, Seiler Precision Microscopes, St. Louis, MI, USA), the presence of 6 canal orifices, mesiobuccal, distobuccal, middle buccal, mesiopalatal, distopalatal, and middle palatal orifices, were confirmed (Figure 1D).
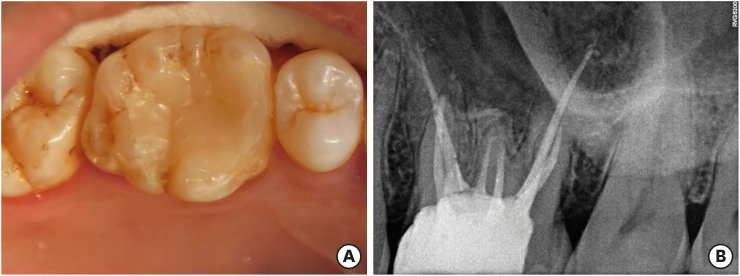
The working length was determined with the help of an electronic apex locator (Root ZX, Morita, Tokyo, Japan) and later confirmed using several working length radiographs taken at different angulations (Figure 1C). The access cavity was sealed with IRM cement (Dentsply De Trey GmbH, Konstanz, Germany). The patient was asymptomatic at the second appointment. Cleaning and shaping was performed under rubber dam isolation using M2 rotary system (VDW, Munich, Germany) in a crown down technique. An irrigation protocol with 5mL of 3% sodium hypochlorite solution (Vishal Dentocare Private Ltd., Ahmedabad, GJ, India) and then 5 mL 17% ethylenediaminetetraacetic acid (pH = 7.7, Dentwash, Prime Dental, Kalher, Bhiwandi, MH, India) followed by 5 mL of 2% chlorhexidine gluconate was followed. In between each of these irrigants, 5 mL of normal saline was used and lastly a final rinse was done with 5 mL normal saline. The canals were dried with absorbent paper points (Pearl Endopia, Pearl Dent Co., Ltd., Ho Chi Minh City, Vietnam). Obturation was performed using single cone obturation technique of gutta percha (Dentsply Maillefer Europe, Ballaigues, Switzerland) and AH Plus Resin sealer (Dentsply Maillefer), applied using lentulospiral (Dentsply Maillefer) (Figure 1E and 1F). A post-endodontic restoration with a posterior composite resin (Spectrum Composite, Dentsply) was done. Follow up radiograph and clinical photograph of tooth #26 at the end of 6 months were taken (Figure 4A and 4B). The patient was asymptomatic and was advised a full-coverage porcelain fused to metal (PFM) crown.
DISCUSSION
The development of formative variations such as the one in the present case, can be imagined as the lateral coalescence of the tooth with the independent formation paradentalis, which has been termed as a ‘paramolar’ [21]. Paramolar is a small and rudimentary, supernumerary molar. It is most commonly situated buccally or palatally to one of the maxillary molars [21].
In this case, the maxillary first molar had one extra middle buccal and middle palatal cusp with a corresponding middle root that is broad buccolingually and is fused as 1 root, with 2 distinct canals. Also, the cusp of Carabelli is in level with the other major cusps with an additional root (mesiopalatal root). Kallay [20] stated that the Carabelli's trait with an additional root is a formation supradentalis, and that a true Carabelli's cusp neither has a pulp nor is in level with the remaining major cusps. Kallay described another category of superstructures that represent coronal units, which are without a pulp and root [20]. Such anomalies are of immense clinical significance during the endodontic management as well as exodontia. Thus, diagnostic adjuncts such as CBCT, are mandatory. In the present case, the unusual anatomy of the crown, as well as the suspicion of the presence of extra roots in the preoperative intraoral periapical radiographs, prompted the referral for a CBCT scan to be carried out.
CBCT is a relatively new diagnostic imaging modality which offers several advantages over conventional CT such as X-ray beam limitation [22], rapid scan time [23], and effective dose reduction [24]. It is being successfully used in endodontics for effectively evaluating the root canal anatomy. Besides this, CBCT also aids in ascertaining the root and alveolar fractures, endodontic and non- endodontic pathosis, analysis of root resorptive lesions, pre-surgical management and assessment of root-end surgery [25,26,27]. In a study carried out by Matherne et al. [28], it was found that CBCT scans always revealed more number of unidentified root canal systems when compared with the images obtained by digital radiography. Baratto et al. [29] studied the internal morphology of the maxillary first molars by ex vivo as well as clinical assessments using operating microscope and CBCT scanning. He concluded that both, the operating microscope as well as CBCT scanning were equally important in identifying root canals, the latter being more important for the initial identification of the internal anatomy of the maxillary first molar.
In the present case, the CBCT scan revealed the presence of 5 roots. Each root had one canal each with Vertucci's type I canal configuration, except for the middle root which had 2 canals with Vertucci's type IV canal configuration. The success of the present case was also largely dependent on the use of the dental operating microscope which offered benefits such as providing a magnified image, increased precision, improved illumination and visualization.
CONCLUSIONS
The present case report discusses the endodontic management of a maxillary first molar (tooth #26) with 7 cusps, 5 roots, and 6 root canals, and highlights the role of the routine use of dental operating microscope and CBCT scanning while performing endodontic treatment which would help the clinician in identifying and successfully treating all root canal systems. Hence, clinicians should familiarize themselves with the latest technologies to get additional information in endodontic practice in order to enhance the outcomes of endodontic therapy.
-
Conflict of Interest: No potential conflict of interest relevant to this article was reported.
-
Author Contributions:
Conceptualization: Chowdhry P, Reddy P, Kaushik M.
Data curation: Chowdhry P, Reddy P, Kaushik M.
Formal analysis: Chowdhry P, Reddy P, Kaushik M.
Investigation: Chowdhry P, Reddy P, Kaushik M.
Methodology: Chowdhry P, Reddy P, Kaushik M.
Project administration: Chowdhry P, Reddy P, Kaushik M.
Resources: Chowdhry P, Reddy P, Kaushik M.
Supervision: Chowdhry P, Reddy P, Kaushik M.
Validation: Chowdhry P, Reddy P, Kaushik M.
Visualization: Chowdhry P, Reddy P, Kaushik M.
Writing - original draft: Chowdhry P.
Writing - review & editing: Chowdhry P, Reddy P, Kaushik M.
- 1. Wang Y, Zheng QH, Zhou XD, Tang L, Wang Q, Zheng GN, Huang DM. Evaluation of the root and canal morphology of mandibular first permanent molars in a western Chinese population by cone-beam computed tomography. J Endod 2010;36:1786-1789.ArticlePubMed
- 2. Kottoor J, Velmurugan N, Sudha R, Hemamalathi S. Maxillary first molar with seven root canals diagnosed with cone-beam computed tomography scanning: a case report. J Endod 2010;36:915-921.ArticlePubMed
- 3. Kottoor J, Velmurugan N, Surendran S. Endodontic management of a maxillary first molar with eight root canal systems evaluated using cone-beam computed tomography scanning: a case report. J Endod 2011;37:715-719.ArticlePubMed
- 4. Kaushik M, Mehra N. Maxillary first molars with six canals diagnosed with the aid of cone beam computed tomography: a report of two cases. Case Rep Dent 2013;2013:406923.ArticlePubMedPMCPDF
- 5. Shetty K, Yadav A, Babu VM. Endodontic management of maxillary first molar having five root canals with the aid of spiral computed tomography. Saudi Endod J 2014;4:149-153.Article
- 6. Umer F. Maxillary first molar with five canals. BMJ Case Rep 2014;2014:bcr2014205757.ArticlePubMedPMC
- 7. Sharma R, Maroli K, Sinha N, Singh B. An unusual maxillary molar with four roots and four buccal canals confirmed with the aid of spiral computed tomography: a case report. J Int Oral Health 2014;6:80-84.PubMedPMC
- 8. Kumar R. Report of a rare case: a maxillary first molar with seven canals confirmed with cone-beam computed tomography. Iran Endod J 2014;9:153-157.PubMedPMC
- 9. Munavalli A, Kambale S, Bandekar S, Ajgaonkar N. Maxillary first molar with seven root canals diagnosed with cone-beam computed tomography scanning. Indian J Dent Res 2015;26:82-85.ArticlePubMed
- 10. Almeida G, Machado R, Sanches Cunha R, Vansan LP, Neelakantan P. Maxillary first molar with 8 root canals detected by CBCT scanning: a case report. Gen Dent 2015;63:68-70.
- 11. Al-Habboubi TM, Al-Wasi KA. Maxillary first molars with six canals confirmed with the aid of cone-beam computed tomography. Saudi Endod J 2016;6:136-140.Article
- 12. Rodrigues E, Braitt AH, Galvão BF, da Silva EJ. Maxillary first molar with 7 root canals diagnosed using cone-beam computed tomography. Restor Dent Endod 2017;42:60-64.ArticlePubMedPDF
- 13. Shah DY, Jadhav GR. Endodontic management of a maxillary molar with formation supradentalis: a case report. J Conserv Dent 2014;17:481-482.ArticlePubMedPMC
- 14. Madhuram K, Dhanavel C, Naveen V, Anbu R. Corono radicular anomaly in a maxillary first molar – a rare case report. J Integr Dent 2012;1:41-44.
- 15. Kulild JC, Peters DD. Incidence and configuration of canal systems in the mesiobuccal root of maxillary first and second molars. J Endod 1990;16:311-317.ArticlePubMed
- 16. Buhrley LJ, Barrows MJ, BeGole EA, Wenckus CS. Effect of magnification on locating the MB2 canal in maxillary molars. J Endod 2002;28:324-327.ArticlePubMed
- 17. Gopikrishna V, Bhargavi N, Kandaswamy D. Endodontic management of a maxillary first molar with a single root and a single canal diagnosed with the aid of spiral CT: a case report. J Endod 2006;32:687-691.ArticlePubMed
- 18. Christie WH, Peikoff MD, Fogel HM. Maxillary molars with two palatal roots: a retrospective clinical study. J Endod 1991;17:80-84.ArticlePubMed
- 19. Barbizam JV, Ribeiro RG, Tanomaru Filho M. Unusual anatomy of permanent maxillary molars. J Endod 2004;30:668-671.ArticlePubMed
- 20. Kallay J. Extra cusp formation in the human dentition. J Dent Res 1966;45:1381-1394.ArticlePubMedPDF
- 21. Nayak G, Shetty S, Singh I, Pitalia D. Paramolar - A supernumerary molar: a case report and an overview. Dent Res J (Isfahan) 2012;9:797-803.PubMedPMC
- 22. Karamifar K, Azimi S, Dashti H. Root canal treatment of a maxillary second molar with two palatal roots: a case report. J Res Dent Sci 2009;1:37-41.
- 23. Lofthag-Hansen S, Huumonen S, Gröndahl K, Gröndahl HG. Limited cone-beam CT and intraoral radiography for the diagnosis of periapical pathology. Oral Surg Oral Med Oral Pathol Oral Radiol Endod 2007;103:114-119.ArticlePubMed
- 24. Cotton TP, Geisler TM, Holden DT, Schwartz SA, Schindler WG. Endodontic applications of cone-beam volumetric tomography. J Endod 2007;33:1121-1132.ArticlePubMed
- 25. Patel S, Dawood A, Ford TP, Whaites E. The potential applications of cone beam computed tomography in the management of endodontic problems. Int Endod J 2007;40:818-830.ArticlePubMed
- 26. Nair MK, Nair UP. Digital and advanced imaging in endodontics: a review. J Endod 2007;33:1-6.ArticlePubMed
- 27. Tyndall DA, Rathore S. Cone-beam CT diagnostic applications: caries, periodontal bone assessment, and endodontic applications. Dent Clin North Am 2008;52:825-841.ArticlePubMed
- 28. Matherne RP, Angelopoulos C, Kulild JC, Tira D. Use of cone-beam computed tomography to identify root canal systems in vitro . J Endod 2008;34:87-89.ArticlePubMed
- 29. Baratto Filho F, Zaitter S, Haragushiku GA, de Campos EA, Abuabara A, Correr GM. Analysis of the internal anatomy of maxillary first molars by using different methods. J Endod 2009;35:337-342.ArticlePubMed
REFERENCES
Tables & Figures
REFERENCES
Citations
Citations to this article as recorded by 
- Endodontic management of maxillary first molar with unusual anatomy
MadhuriSai Battula, Mamta Kaushik, Neha Mehra, Ankeeta Singh
Journal of Conservative Dentistry.2022; 25(5): 569. CrossRef - Diversity of root canal morphology of maxillary first molars
Juhász Kincső-Réka, Kovács Mónika, Pop Mihai, Pop Silvia, Kerekes-Máthé Bernadette
Bulletin of Medical Sciences.2021; 94(1): 63. CrossRef
 ePub Link
ePub Link Cite
CiteManagement of a permanent maxillary first molar with unusual crown and root anatomy: a case report
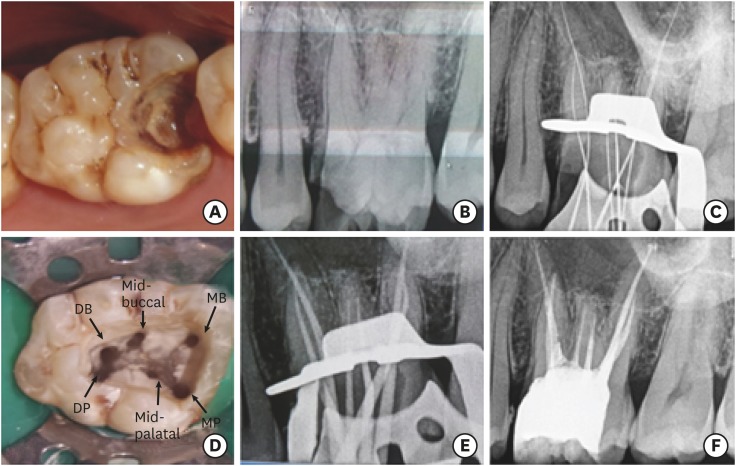
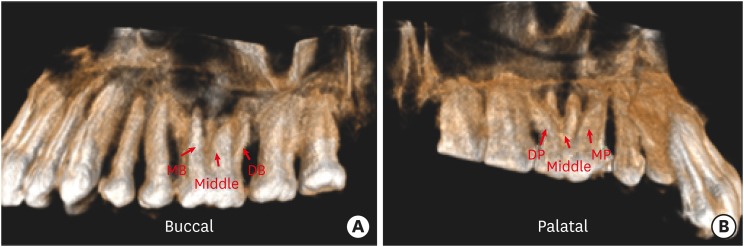
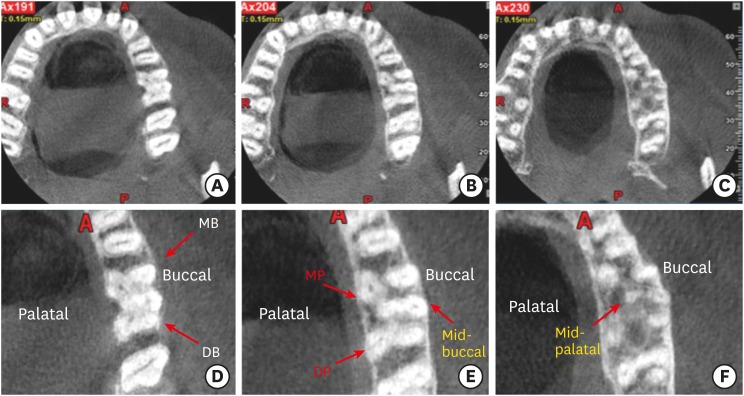
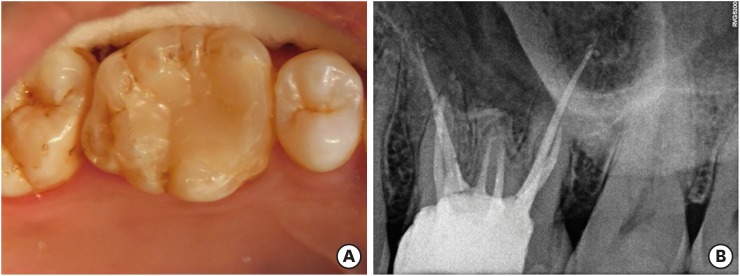
Figure 1 (A) Preoperative clinical view, abnormally large crown, with 7 cusps and mesio-occlusal caries; (B) Preoperative intraoral radiograph showing at least 5 roots; (C) Working length confirmed through radiograph; (D) Six canal orifices as seen under dental operating microscope; (E and F) master cone radiograph and obturation, respectively.DB, distobuccal canal; DP, distopalatal canal; MB, mesiobuccal canal; MP, mesiopalatal canal.
Figure 2 (A) Three-dimensional single volume cone-beam computed tomography images showing the (A) mesiobuccal, distobuccal, and middle root on the buccal aspect, and (B) mesiopalatal, distopalatal, and the middle root from the palatal aspect.DB, distobuccal canal; MB, mesiobuccal canal; DP, distopalatal canal; MP, mesiopalatal canal.
Figure 3 Cone-beam computed tomography (CBCT) images of tooth #26 showing the axial sections at the (A) cervical, (B) middle, and (C) apical level. Enlarged axial section CBCT images at the (D) cervical, (E) middle, and (F) apical level showing 5 roots and 6 canals.DB, distobuccal canal; MB, mesiobuccal canal; DP, distopalatal canal; MP, mesiopalatal canal.
Figure 4 Follow up of tooth #26 at the end of 6 months (A) clinical view and (B) radiograph.
Figure 1
Figure 2
Figure 3
Figure 4
Management of a permanent maxillary first molar with unusual crown and root anatomy: a case report
Summary of case reports of maxillary first molars with multiple canals
| Root configuration | No. of canals | Canal configuration | Reference | ||
|---|---|---|---|---|---|
| (MB) | (DB) | (P) | |||
| 3 | 7 | 3 | 2 | 2 | Kottor et al. (2010) [ |
| 3 | 8 | 3 | 3 | 2 | Kottor et al. (2011) [ |
| 3 | 6 | 2 | 2 | 2 | Kaushik and Mehra (2013) [ |
| 6 | 6 | 3 | 1 | 2 | Kaushik and Mehra (2013) [ |
| 3 | 5 | 2 | 1 | 2 | Shetty et al. (2014) [ |
| 3 | 5 | 2 | 1 | 2 | Umer et al. (2014) [ |
| 4 | 5 | 3 | 2 | 2 | Sharma et al. (2014) [ |
| 3 | 7 | 3 | 2 | 2 | Kumar (2014) [ |
| 3 | 7 | 3 | 2 | 2 | Munavalli et al. (2015) [ |
| 3 | 8 | 3 | 3 | 2 | Almeida et al. (2015) [ |
| 3 | 6 | 3 | 2 | 1 | Al-Habboubi and Al-Wasi (2016) [ |
| 3 | 7 | 3 | 2 | 2 | Rodrigues et al. (2017) [ |
MB, mesiobuccal canal; DB, distobuccal canal; P, palatal canal.
Table 1 Summary of case reports of maxillary first molars with multiple canals
MB, mesiobuccal canal; DB, distobuccal canal; P, palatal canal.

