
Articles
- Page Path
- HOME > Restor Dent Endod > Volume 43(4); 2018 > Article
- Research Article Effects of the exposure site on histological pulpal responses after direct capping with 2 calcium-silicate based cements in a rat model
-
Panruethai Trongkij1
 , Supachai Sutimuntanakul1, Puangwan Lapthanasupkul2, Chitpol Chaimanakarn1, Rebecca Wong3, Danuchit Banomyong1
, Supachai Sutimuntanakul1, Puangwan Lapthanasupkul2, Chitpol Chaimanakarn1, Rebecca Wong3, Danuchit Banomyong1 -
Restor Dent Endod 2018;43(4):e36.
DOI: https://doi.org/10.5395/rde.2018.43.e36
Published online: August 22, 2018
1Department of Operative Dentistry and Endodontics, Faculty of Dentistry, Mahidol University, Bangkok, Thailand.
2Department of Oral and Maxillofacial Pathology, Faculty of Dentistry, Mahidol University, Bangkok, Thailand.
3Restorative Section, Melbourne Dental School, University of Melbourne, Melbourne, VIC, Australia.
- Correspondence to Danuchit Banomyong, DDS, PhD. Assistant Professor, Department of Operative Dentistry and Endodontics, Faculty of Dentistry, Mahidol University, 6 Yothi Street, Rachathewi, Bangkok 10400, Thailand. danuchit.ban@mahidol.ac.th
• Received: March 21, 2018 • Accepted: July 2, 2018
Copyright © 2018. The Korean Academy of Conservative Dentistry
This is an Open Access article distributed under the terms of the Creative Commons Attribution Non-Commercial License (https://creativecommons.org/licenses/by-nc/4.0/) which permits unrestricted non-commercial use, distribution, and reproduction in any medium, provided the original work is properly cited.
- 3,156 Views
- 30 Download
- 12 Crossref
Abstract
-
Objectives Direct pulp capping is a treatment for mechanically exposed pulp in which a biocompatible capping material is used to preserve pulpal vitality. Biocompatibility tests in animal studies have used a variety of experimental protocols, particularly with regard to the exposure site. In this study, pulp exposure on the occlusal and mesial surfaces of molar teeth was investigated in a rat model.
-
Materials and Methods A total of 58 maxillary first molars of Wistar rats were used. Forty molars were mechanically exposed and randomly assigned according to 3 factors: 1) the exposure site (occlusal or mesial), 2) the pulp-capping material (ProRoot White MTA or Bio-MA), and 3) 2 follow-up periods (1 day or 7 days) (n = 5 each). The pulp of 6 intact molars served as negative controls. The pulp of 12 molars was exposed without a capping material (n = 3 per exposure site for each period) and served as positive controls. Inflammatory cell infiltration and reparative dentin formation were histologically evaluated at 1 and 7 days using grading scores.
-
Results At 1 day, localized mild inflammation was detected in most teeth in all experimental groups. At 7 days, continuous/discontinuous calcified bridges were formed at exposure sites with no or few inflammatory cells. No significant differences in pulpal response according to the exposure site or calcium-silicate cement were observed.
-
Conclusions The location of the exposure site had no effect on rat pulpal healing. However, mesial exposures could be performed easily, with more consistent results. The pulpal responses were not significantly different between the 2 capping materials.
INTRODUCTION
Direct pulp capping is a procedure aimed at preserving the vitality of mechanically exposed pulp from a restorative procedure or dental trauma. The exposed pulp must be covered with a biocompatible capping material, followed by a coronal seal to protect the pulp from additional injury and to promote healing and repair. Healing of the pulp is characterized by the formation of reparative dentin at the exposure site with minimal pulpal inflammation in the absence of bacterial infection [1].
A variety of new biocompatible materials has been developed for use as pulp-capping agents. According to ISO 7405:2008 for dentistry, animal studies are recommended to assess the efficacy and biocompatibility of new pulp-capping materials or therapeutic medicaments [2]. Rat molars are usually selected as an experimental animal model due to their similarities to human molars in terms of anatomical, histological and biological features [3].
Nevertheless, experimental protocols in rat molars vary, particularly with regard to the site of pulpal exposure [4,5,6,7,8,9,10,11,12]. An approach via the occlusal surface has been reported to be superior to the mesial surface due to the ability to control the size and depth of pulpal exposure [13]. In contrast, other studies prepared exposure sites at the mesial aspects of the teeth in various positions, such as the cervical third (with gingivectomy) [4,5,6], the middle third [9,10], or the occlusal third (mesial marginal ridge) [11,12]. The preference for mesial exposure was due to the ease of access in cavity preparations [6], related to the space available between the incisors and the first molars. In addition to this, the mesial site is a non-stress bearing area. Occlusal forces may otherwise dislodge the temporary restoration during the observation period [4]. However, pulp exposure at the mesial surface may disrupt the blood supply from the radicular to the coronal pulp, or there may be an increased risk of contamination if the exposure site is at the cervical third. Therefore, pulpal healing after an exposure on the mesial surface may be delayed compared with an occlusal exposure. Thus, the effect of the exposure site on pulpal responses to direct pulp capping remains controversial.
Mineral trioxide aggregate (MTA) is a calcium-silicate based cement that is commercially available as ProRoot White MTA (WMTA; Tulsa Dental Products, Tulsa, OK, USA), with a setting time of 4 hours. MTA is highly compatible with living cells and tissues, provides an excellent seal to dentin, and promotes the proliferation of human dental pulp cells (hDPCs) and the differentiation of odontoblasts [14,15]. Many in vivo studies have demonstrated more favorable healing of the pulp-dentin complex after direct pulp capping with MTA than when the conventional pulp capping material, calcium hydroxide, was used. MTA stimulated fewer inflammatory reactions and was found to induce a thicker and more uniform mineralized-tissue bridge [16,17,18,19].
Recently, a new fast-setting calcium-silicate based material, Bio-MA (M-Dent/SCG, Bangkok, Thailand), has been developed. Bio-MA and WMTA contain similar main ingredients, which are tricalcium silicate, dicalcium silicate, and tricalcium aluminate [20], except that calcium chloride is added to Bio-MA to accelerate the setting reaction. The physiochemical and biological properties of Bio-MA are similar to those of WMTA [20,21,22]. The setting time of Bio-MA was reported to be shorter than that of WMTA [23,24], due to the presence of calcium chloride as an accelerator in the liquid component. Except for calcium chloride, the ingredients for Bio-MA are similar to those of WMTA. It is therefore speculated that the biocompatibility of both products will be similar.
The objective of this in vivo study was to evaluate the influence of different exposure sites (occlusal or mesial) on the pulpal tissue response at 1 and 7 days after direct pulp capping in mechanically exposed rat molars, using 2 calcium-silicate based cements, WMTA and Bio-MA.
MATERIALS AND METHODS
The study protocol was approved by the Faculty of Science, Mahidol University Animal Care and Use Committee (MUSC-ACUC), Bangkok, Thailand. Thirty-two 8-week-old male Wistar Albino rats (Nomura Siam International, Bangkok, Thailand) weighing 180–220 g were used in this study. The rats received general anesthesia through an intraperitoneal injection of 20 mg/kg of tiletamine hydrochloride and zolazepam (Zoletil 50, Virbac, Bangkok, Thailand) and 5 mg/kg of xylazine hydrochloride (X-Lazine, MacroPhar, Bangkok, Thailand).
Forty right and left maxillary first molars in 20 rats were randomly allocated into 8 experimental groups according to the 1) site of exposure (occlusal or mesial surface), 2) pulp capping material (WMTA [lot no. 0000144254] or Bio-MA [lot no. 01/2017)]), and 3) the observation period (1 or 7 days [n = 5 per group]). Six maxillary first molars served as negative controls (intact teeth with no preparation), while 12 maxillary first molars served as positive controls (pulp exposure without capping material) at the 2 follow-up periods (n = 3 per group). Each rat was fixed on the operating board in a supine position, and the mouth was kept open with a mouth prop. Teeth were cleaned with a micro applicator brush and disinfected with a cotton pellet soaked in 2% chlorhexidine gluconate. Under the aid of magnifying loupes attached with fiber-optic light (×2.5 magnification, Zeiss, Oberkochen, Germany), a sterile 0.8 mm slow-speed round diamond bur was used to prepare a cavity at the mesial half of the occlusal surface or the middle third of the mesial surface, according to the randomization. The depth of the cavity was approximately half the diameter of the bur. Each bur was changed after 2 cavity preparations. During the preparation, the cutting area was irrigated with copious saline solution (0.9% NaCl) to prevent heat generation.
Once the bur had penetrated the dentin, the dental pulp was then exposed with a sterile sharp endodontic explorer (DG16, Dental USA Inc., Mc Henry, IL, USA). Pulpal bleeding was controlled by pressing with a sterile saline-soaked cotton pellet and paper points. The exposure areas were directly capped with one of the pre-sterilized capping materials that was prepared according to the manufacturer's instructions and carried to the exposure sites using the tip of an endodontic explorer. In the contralateral tooth, the pulp was capped with the other pulp capping material. In the positive control groups, a sterile piece of polytetrafluoroethylene (PTFE; Teflon tape) was placed at the exposure site instead of a capping material, to prevent direct contact between pulpal tissue and the coronal restoration. All cavities were restored with light-cured glass-ionomer cement (GC Fuji II LC, GC, Tokyo, Japan), and the cusp tips of occluding teeth were ground to minimize occlusal forces.
At 1 and 7 days after direct pulp capping, the animals were sacrificed by an overdose of carbon dioxide gas. The whole maxilla was collected and fixed in 10% neutral buffered formalin for 24 hours at room temperature, and demineralized in 20% formic acid for 3 days. Then, the maxilla was vertically sectioned into 2 halves, washed in running tap water overnight, dehydrated through ascending concentrations of ethanol, and embedded in paraffin blocks. The 3-µm thick serial sections were cut through the molar area in the mesio-distal direction using a sliding microtome (RM2255, Leica Biosystems, Wetzlar, Germany) to include the entire pulp chamber and the exposed area. The slides were numbered, and the sections were stained with hematoxylin and eosin to evaluate the pulp tissue response and reparative dentin formation. Gram bacterial staining with the modified Brown and Brenn technique was used to confirm the absence or presence of bacteria in the capped pulp.
The stained sections were blindly evaluated by a trained investigator who was previously calibrated with an experienced pathologist. Then, the histopathological evaluation was performed twice at a 2-week interval to control intra-observer reliability (Cohen kappa ≥ 0.8). Under a light microscope (Olympus BX53, Olympus, Tokyo, Japan) at ×100, ×200, and ×400 magnifications, all samples were evaluated and scored in terms of: 1) inflammatory cell infiltration, 2) reparative dentin formation, 3) bacterial penetration, and 4) impaction of dentin fragments into the pulp, according to the criteria modified from Liu et al. [9], as presented in Table 1. In addition, the widest dimension of exposure was measured at ×40 magnification and recorded in micrometers as the pulp exposure size in each sample.
Table 1
Evaluation criteria for the histopathological analysis of pulpal tissue responses after mechanical pulp exposure and direct pulp capping in rats
The data were statistically analyzed with the level of significance set at 0.05 (IBM SPSS statistics software version 19, IBM, Armonk, NY, USA). The degree of inflammatory cell infiltration and reparative dentin formation between the two capping materials were compared using the Wilcoxon matched-pair signed rank test. Data from different exposure sites or observation periods were compared using the Mann-Whitney U test. The presence of dentin-fragment impaction was descriptively analyzed. The size of pulpal exposures was analyzed using the independent sample t-test.
RESULTS
Table 2 presents categorizations of the pulpal response, in terms of inflammatory cell infiltration and reparative dentin formation, to direct pulp capping with 2 calcium-silicate cements and positive controls. At 1 and 7 days, the intact teeth (negative control group) showed an intact odontoblastic layer and no inflammation of the pulp tissue. At 1 day, a mild to moderate acute inflammatory pulpal response was observed in the uncapped teeth (positive control group, Figure 1A, 1D, 1G, and 1J). Direct pulp capping with WMTA and Bio-MA showed a similar acute inflammatory response in the pulp tissue. Most pulps with either occlusal (Figure 1B-1C and 1E-1F) or mesial exposure (Figure 1H-1I and 1K-1L) exhibited a mild inflammatory response with a focal accumulation of polymorphonuclear leukocytes (PMNs) and congested blood vessels. Local disruption of the odontoblastic layer was observed at the exposure site in all samples.
Table 2
Grading of pulpal responses (inflammatory cell infiltration and reparative dentin formation) to direct pulp capping with 2 calcium-silicate cements and positive controls in rats
Figure 1
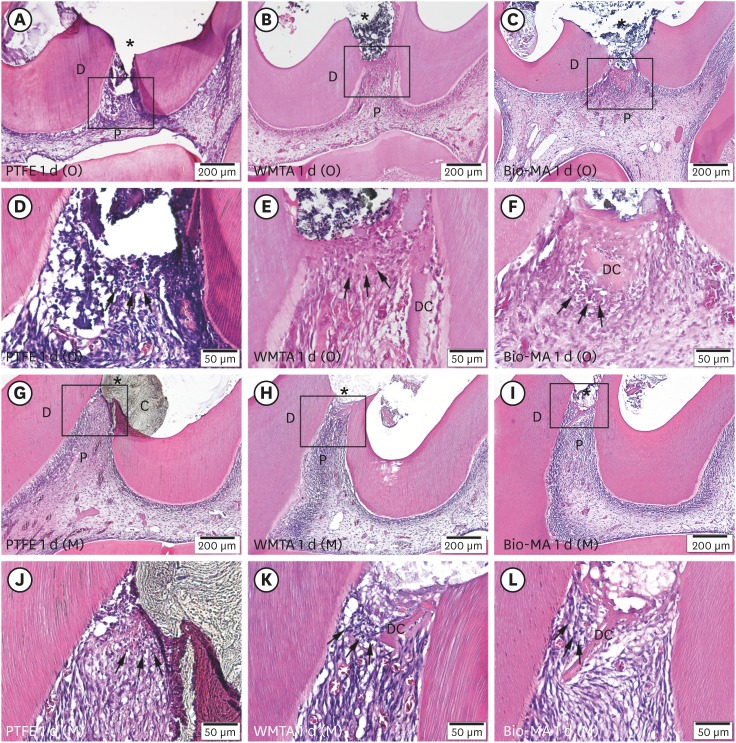
Effects of direct capping at 1 day on mechanically exposed pulp at occlusal (A-F) and mesial (G-L) sites. Mild inflammation with limited accumulation of polymorphonuclear leukocytes (black arrows) and congested blood vessels were observed at the exposure areas in the PTFE (positive control: A, D, G, and J), WMTA (B, E, H, and K), and Bio-MA (C, F, I, and L) groups. D-F and J-L present a high-magnification view (×400) of the areas demarcated by the black rectangles in A-C and G-I (×100), respectively.
P, pulp; D, dentin; DC, dentin chips; C, capping material.
Asterisk (*) indicates pulp exposure site.
At 7 days, a moderate to severe chronic inflammatory response was observed in the positive control groups (Figure 2A, 2D, 2G, and 2J). WMTA and Bio-MA capping on occlusal exposures showed variable pulpal responses, ranging from the absence of inflammation to moderate chronic inflammation (Figure 2B-2C and 2E-2F). WMTA and Bio-MA capping on mesial exposures mostly exhibited no inflammatory response or just a few inflammatory cells (Figure 2H-2I and 2K-2L), although a moderate inflammatory response was observed in a sample of each group.
Figure 2
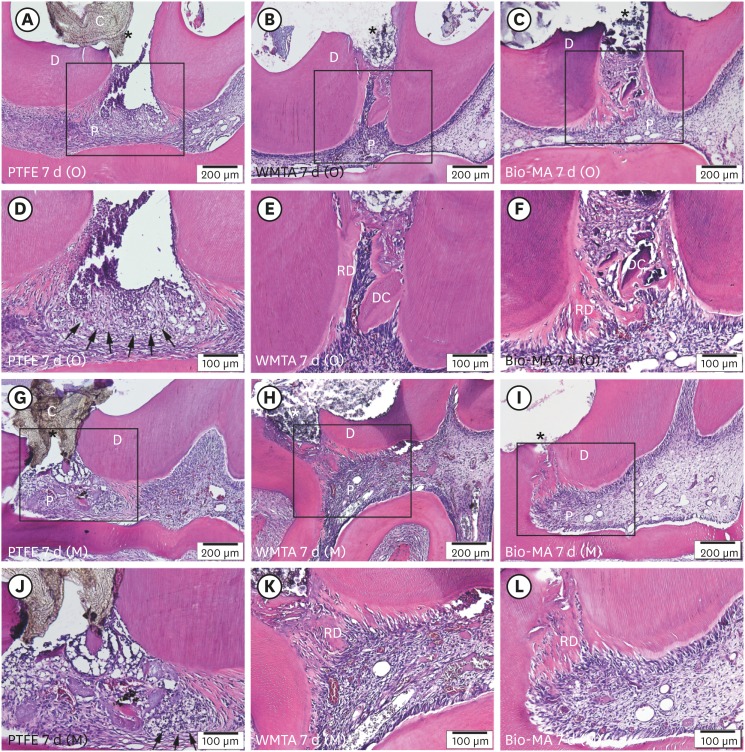
Effects of direct capping at 7 days on mechanically exposed pulp at occlusal (A-F) and mesial (G-L) sites. Moderate pulpal inflammation was observed, with extensive infiltration of inflammatory cells (arrows) and no hard tissue deposition at the exposure site in the positive control groups (A, D, G, and J). No inflammation with moderate hard tissue deposition was detected in the WMTA (B, E, H, and K) and Bio-MA (C, F, I, and L) groups. D-F and J-L present a high-magnification view (×200) of the areas demarcated by the black rectangles in A-C and G-I (×100), respectively.
P, pulp; D, dentin; DC, dentin chips; C, capping material; RD, reparative dentin.
Asterisk (*) indicates pulp exposure site.
No significant difference in the inflammatory response was observed between the 2 exposure sites or between the 2 calcium-silicate cements at either 1 day or 7 days (p > 0.05, Figure 3A). The inflammatory responses were also not significantly different between the 2 observation periods (p > 0.05, Figure 3A).
Figure 3
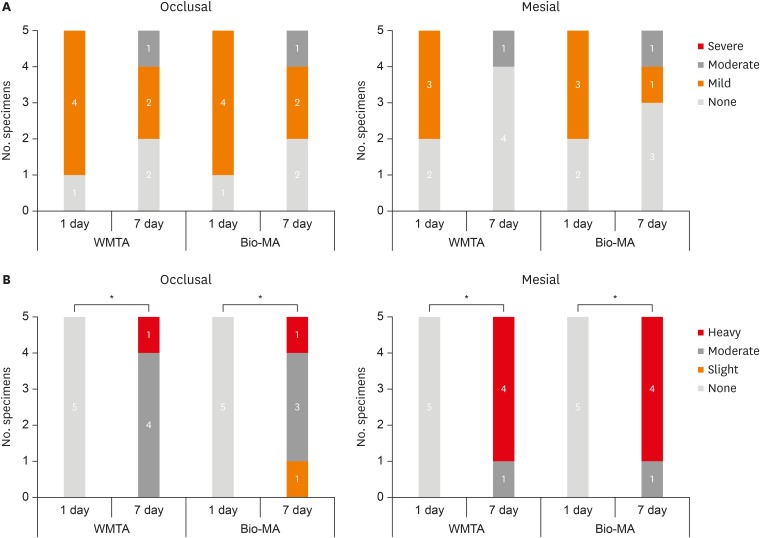
Comparison of (A) the inflammatory response and (B) reparative dentin formation in the experimental groups between the 2 observation periods. Asterisk (*) indicates a significant difference, with p < 0.01.
At 1 day, no hard tissue barrier was formed in any samples of the capped or uncapped (positive control) groups (Figure 1).
At 7 days, diffused calcification was observed at a distance below the exposure area in the positive control groups (Figure 2A, 2D, 2G, and 2J). The sites that were capped with WMTA and Bio-MA presented a layer of newly-generated mineralized matrix subjacent to the capping material. Four of the 5 samples with mesial exposure presented a continuous dentin bridge that completely covered the exposure site (Figure 2H-2I and 2K-2L). One sample showed moderate hard tissue deposition that incompletely covered the exposure. In contrast, only one sample with occlusal exposure in each of the WMTA or Bio-MA groups exhibited a continuous dentin bridge. The majority of samples in the WMTA and Bio-MA groups showed incomplete, moderate hard tissue deposition (Figure 2B-2C and 2E-2F). All dentin bridges in the experimental groups were formed with minor defects of cell inclusions and aligned with a layer of odontoblast-like cells underneath. The formation of hard tissue barriers at this observation period was significantly different from that observed at 1 day (p < 0.01). No significant difference was noted in reparative dentin formation between the 2 exposure sites, or between the 2 calcium-silicate cements (p > 0.05, Figure 3B).
At 1 day, all samples in the experimental and positive control groups exhibited no bacteria in the pulp or contained only few bacteria next to the exposure areas. At 7 days, most of the samples were free of bacteria, except 5 samples that contained bacteria in a limited area of coronal pulp below the dentin bridge.
Small dentin fragments were generally observed in most of the experimental and positive control groups in the 1-day samples, regardless of the site of exposure (Figure 1). At 7 days, the impacted dentin fragments were surrounded and merged with the newly mineralized bridge (Figure 2).
The pulp exposure sizes ranged from 207.5 ± 67.5 µm to 261.3 ± 104.4 µm in the occlusal exposure groups, and from 150.9 ± 41.2 µm to 181.2 ± 101.4 µm in the mesial exposure groups. The overall mean values for the occlusal and mesial groups were 234.5 and 166.8 µm, respectively. The difference in the exposure size between the 2 groups was 33.7%. However, there was no significant difference in the size of the pulp exposures among the experimental and positive control groups (p > 0.05, Table 3).
Table 3
Size of pulp exposure in the occlusal- and mesial-approach groups
DISCUSSION
The use of rat maxillary first molars in this study is a convenient and acceptable model for evaluating the biocompatibility of pulp-capping materials, as suggested by other studies [3,5,6]. The pulp in the rat molars responded to mechanical injury by stimulating the differentiation of odontoblast-like cells and then forming reparative dentin at the exposure site [25]. This process of pulpal repair in rats could be distinctly observed from 7 days onwards when the injured pulp was treated with calcium-silicate based cements [9,10]. In establishing exposure sites in the rat molar pulp, tooth isolation is impractical and difficult to achieve. As such, contamination with bacteria, if present, may have resulted in a delay in pulpal healing [26]. Using modified Gram bacterial staining, most samples in this study revealed no or minimal levels of bacteria, which were present only to a limited extent in the pulp exposure areas. Thus, the pulpal responses were likely to be a reaction to the mechanical injury and capping materials.
According to previous studies [4,5], rat molar pulp is expected to show a self-repair capacity, with auto-deposition of osteodentin-like matrix observed in the coronal pulp after pulp exposure, even in the absence of pulp capping material. To distinguish the biological effect of capping materials from the exceptional reparative capacity, a positive control was carried out using the same experimental protocol. This was achieved by replacing the capping material with PTFE tape, a chemically inert material [14]. At 7 days, pulp capping with PTFE tape led to a persistent chronic inflammatory response and incomplete dentin bridge formation at the exposure area, similar to results of previous studies [27,28]. Delayed resolution of pulpal inflammation was speculated to be a result of the inability of PTFE tape to regenerate and stimulate the differentiation of pulpal cells. PTFE tape was also ineffective in the promotion of pulpal healing or stimulation of a consistent dentin bridge formation at the exposure sites [28]. The consequences of this is an extended period for pulpal healing to be completed.
The results of this study indicated no significant difference in the inflammatory cell response and hard tissue formation in the pulp exposed at the occlusal surface compared with that exposed at the mesial surface at 1 day or 7 days. This potentially can be explained by the consistency of the experimental procedure and skills of the operator. Nevertheless, a trend for slightly delayed healing was observed in specimens in the occlusal group, and this tendency was likely due to the larger pulpal exposure size. In contrast to Berman and Massler [13], the size of exposure in the occlusal group in this study tended to be inconsistent and one-third larger than the mesial group. A larger surface area of pulpal tissue exposed would require a longer time period for repair [29]. The mesial approach provided more favorable access for cavity preparation and pulpal exposure due to the rat's anatomy. In agreement with a previous study [6], the distinct space between the incisors and first maxillary molars facilitated standardization and consistency in the size and location of pulp exposure. Samples with pulpal exposure at the middle level of the mesial surface also showed no to minimal risks of bacterial contamination, similarly to those exposed at the occlusal surface.
The presence of dentin fragments was investigated in this study, as it has previously been noted [4,5]. Unlike pulpal exposure, which occurs clinically during caries removal using rotary instruments, dentin fragments in the experimental animal model were accidentally pushed into the pulp when the tip of an endodontic explorer was used to create the exposure. These fragments could act as a stimulator for focal mineralization in the pulp [30]. Similar to the results of other studies [4,30], the presence of small scattered dentin fragments in this study did not induce pulpal inflammation. However, their effect on reparative dentin formation was not clearly observed.
At 1 day, local infiltration of PMNs and vascular proliferation were observed at the exposure sites in most of samples, indicating acute inflammatory responses to the injury. At 7 days, the inflammatory response in most of samples with mesial exposures subsided to none or very few inflammatory cell infiltrations. The inflammatory cells at 7 days were lymphocytes and plasma cells, with a few PMNs and macrophages, representing the chronic phase of inflammation. WMTA and Bio-MA induced an irregular band of calcified bridge that partially or completely covered the exposure site at 7 days. These findings are similar to those of the studies by Liu et al. [9] and Long et al. [10], who reported that pulp exposed at the mesial surface and capped with MTA had few or no inflammatory cells, and a thin layer of newly-mineralized bridge formation at 7 days. In those studies, a complete tubular dentin bridge with a well-organized odontoblast-like layer was observed at the exposure site at 30 days, with no pulp tissue inflammation. However, in our study, healing of pulpal tissues was already observed at 7 days. It is speculated that a thicker dentin bridge would be expected with a longer observation period.
Pulp capping with WMTA or Bio-MA did not show any significant differences. This can be explained by the presence of similar active ingredients, which are tricalcium silicate, dicalcium silicate, and tricalcium aluminate [20]. From the moisture within pulp tissue or dentinal tubules, these calcium-silicate based cements become hydrated and then release a calcium silicate hydrate gel and calcium hydroxide [31,32]. The release of calcium ions was found to up-regulate the levels of bone morphogenetic protein-2 mRNA expression and protein production, accelerating the odontoblastic-differentiation of hDPCs and then dentin bridge formation [33]. The pulpal responses to Bio-MA, a calcium silicate material with the addition of calcium chloride, were similar to those to WMTA, the material without calcium chloride. Thus, the calcium chloride added into Bio-MA did not interfere with pulpal healing.
CONCLUSIONS
Based on the findings of this study, the location of the exposure site did not affect pulp healing in direct pulp capping with 2 calcium-silicate cements. However, the mesial approach may be easier to perform, with better control and consistency than the occlusal approach. Bio-MA, the new calcium chloride containing pulp-capping material, exhibited biocompatibility with pulp tissues and stimulated reparative dentin formation with minimal pulpal inflammation at 7 days following mechanical exposure in rat molars, similar to WMTA.
ACKNOWLEDGEMENT
The authors thank Mr. Visut Rawiwet and the staff at the Central Animal Facilities, Faculty of Science, Mahidol University for their kind assistance in animal care during the experiment. The authors also thank the technicians from the Department of Oral and Maxillofacial Pathology, Faculty of Dentistry, Mahidol University who provided support in histological processing.
-
Conflict of Interest: No potential conflict of interest relevant to this article was reported.
-
Author Contributions:
Conceptualization: Trongkij P, Sutimuntanakul S, Lapthanasupkul P, Chaimanakarn C, Banomyong D.
Data curation: Trongkij P.
Formal analysis: Trongkij P.
Funding acquisition: Trongkij P.
Investigation: Trongkij P.
Methodology: Trongkij P.
Project administration: Sutimuntanakul S, Lapthanasupkul P, Chaimanakarn C, Banomyong D.
Resources: Sutimuntanakul S.
Software: Trongkij P.
Supervision: Sutimuntanakul S, Lapthanasupkul P, Chaimanakarn C, Banomyong D.
Validation: Trongkij P, Lapthanasupkul P, Banomyong D.
Visualization: Trongkij P, Lapthanasupkul P.
Writing - original draft: Trongkij P.
Writing - review & editing: Sutimuntanakul S, Lapthanasupkul P, Chaimanakarn C, Wong RH, Banomyong D.
- 1. Kakehashi S, Stanley HR, Fitzgerald RJ. The effects of surgical exposures of dental pulps in germ-free and conventional laboratory rats. Oral Surg Oral Med Oral Pathol 1965;20:340-349.ArticlePubMed
- 2. ISO. ISO 7405: 2008 Dentistry - Evaluation of biocompatibility of medical devices used in dentistry. Part 6: test procedures specific to dental materials. 2nd ed. New York (NY): International Organization for Standardization; 2008. p. 19-27.
- 3. Dammaschke T. Rat molar teeth as a study model for direct pulp capping research in dentistry. Lab Anim 2010;44:1-6.ArticlePubMedPDF
- 4. Decup F, Six N, Palmier B, Buch D, Lasfargues JJ, Salih E, Goldberg M. Bone sialoprotein-induced reparative dentinogenesis in the pulp of rat's molar. Clin Oral Investig 2000;4:110-119.ArticlePubMedPDF
- 5. Six N, Lasfargues JJ, Goldberg M. Differential repair responses in the coronal and radicular areas of the exposed rat molar pulp induced by recombinant human bone morphogenetic protein 7 (osteogenic protein 1). Arch Oral Biol 2002;47:177-187.ArticlePubMed
- 6. Louwakul P, Lertchirakarn V. Response of inflamed pulps of rat molars after capping with pulp-capping material containing fluocinolone acetonide. J Endod 2015;41:508-512.ArticlePubMed
- 7. Dammaschke T, Stratmann U, Fischer RJ, Sagheri D, Schäfer E. A histologic investigation of direct pulp capping in rodents with dentin adhesives and calcium hydroxide. Quintessence Int 2010;41:e62-e71.PubMed
- 8. Hayashi K, Handa K, Koike T, Saito T. The possibility of genistein as a new direct pulp capping agent. Dent Mater J 2013;32:976-985.ArticlePubMed
- 9. Liu S, Wang S, Dong Y. Evaluation of a bioceramic as a pulp capping agent in vitro and in vivo . J Endod 2015;41:652-657.ArticlePubMed
- 10. Long Y, Liu S, Zhu L, Liang Q, Chen X, Dong Y. Evaluation of pulp response to novel bioactive glass pulp capping materials. J Endod 2017;43:1647-1650.ArticlePubMed
- 11. Kawashima S, Shinkai K, Suzuki M. Effect of an experimental adhesive resin containing multi-ion releasing fillers on direct pulp-capping. Dent Mater J 2016;35:479-489.ArticlePubMed
- 12. Suzuki M, Taira Y, Kato C, Shinkai K, Katoh Y. Histological evaluation of direct pulp capping of rat pulp with experimentally developed low-viscosity adhesives containing reparative dentin-promoting agents. J Dent 2016;44:27-36.ArticlePubMed
- 13. Berman DS, Massler M. Experimental pulpotomies in rat molars. J Dent Res 1958;37:229-242.ArticlePubMedPDF
- 14. Paranjpe A, Zhang H, Johnson JD. Effects of mineral trioxide aggregate on human dental pulp cells after pulp-capping procedures. J Endod 2010;36:1042-1047.ArticlePubMed
- 15. Takita T, Hayashi M, Takeichi O, Ogiso B, Suzuki N, Otsuka K, Ito K. Effect of mineral trioxide aggregate on proliferation of cultured human dental pulp cells. Int Endod J 2006;39:415-422.ArticlePubMed
- 16. Ford TR, Torabinejad M, Abedi HR, Bakland LK, Kariyawasam SP. Using mineral trioxide aggregate as a pulp-capping material. J Am Dent Assoc 1996;127:1491-1494.ArticlePubMed
- 17. Faraco IM Jr, Holland R. Response of the pulp of dogs to capping with mineral trioxide aggregate or a calcium hydroxide cement. Dent Traumatol 2001;17:163-166.ArticlePubMedPDF
- 18. Nair PN, Duncan HF, Pitt Ford TR, Luder HU. Histological, ultrastructural and quantitative investigations on the response of healthy human pulps to experimental capping with mineral trioxide aggregate: a randomized controlled trial. Int Endod J 2008;41:128-150.ArticlePubMed
- 19. Yun YR, Yang IS, Hwang YC, Hwang IN, Choi HR, Yoon SJ, Kim SH, Oh WM. Pulp response of mineral trioxide aggregate, calcium sulfate or calcium hydroxide. J Korean Acad Conserv Dent 2007;32:95-101.Article
- 20. Settawacharawanich S, Sutimuntanakul S, Phuvaravan S, Plang-ngern S. The chemical compositions and physicochemical properties of a Thai white Portland cement [Master's thesis]. Bangkok: Mahidol University; 2006.
- 21. Pisalchaiyong N, Sutimuntanakul S, Korsuwannawong S, Vajrabhaya L. Evaluating cytotoxicity of Thai white Portland cement in cell culture using MTT assay. Mahidol Dent J 2010;30:17-26.
- 22. Chaimanakarn C, Sutimuntanakul S, Jantarat J. Subcutaneous tissue response to calcium silicate-based cement [Master's thesis]. Bangkok: Mahidol University; 2014.
- 23. Warotamawichaya S, Sutimuntanakul S. Effect of calcium chloride on setting time of Thai white Portland cement [Master's thesis]. Bangkok: Mahidol University; 2011.
- 24. Dentsply Maillefer. ProRoot® MTA (Mineral Trioxide Aggregate) Root canal repair material [Internet]. Johnson City (TN): DENTSPLY Tulsa Dental Specialties; 2005. updated 2017 Mar 16]. cited 2016 April 4]. Available from: http://www.dentsplymaillefer.com/wp-content/uploads/2016/10/Dentsply_Maillefer_PROROOT_MTA_0216_DFU_EN.pdf.
- 25. D'Souza RN, Bachman T, Baumgardner KR, Butler WT, Litz M. Characterization of cellular responses involved in reparative dentinogenesis in rat molars. J Dent Res 1995;74:702-709.ArticlePubMedPDF
- 26. Cotton WR. Bacterial contamination as a factor in healing of pulp exposures. Oral Surg Oral Med Oral Pathol 1974;38:441-450.ArticlePubMed
- 27. Heys DR, Fitzgerald M, Heys RJ, Chiego DJ Jr. Healing of primate dental pulps capped with Teflon. Oral Surg Oral Med Oral Pathol 1990;69:227-237.ArticlePubMed
- 28. Cvek M, Granath L, Cleaton-Jones P, Austin J. Hard tissue barrier formation in pulpotomized monkey teeth capped with cyanoacrylate or calcium hydroxide for 10 and 60 minutes. J Dent Res 1987;66:1166-1174.ArticlePubMedPDF
- 29. Pereira JC, Stanley HR. Pulp capping: influence of the exposure site on pulp healing--histologic and radiographic study in dogs' pulp. J Endod 1981;7:213-223.ArticlePubMed
- 30. Tziafas D, Kolokuris I, Alvanou A, Kaidoglou K. Short-term dentinogenic response of dog dental pulp tissue after its induction by demineralized or native dentine, or predentine. Arch Oral Biol 1992;37:119-128.ArticlePubMed
- 31. Camilleri J. Characterization of hydration products of mineral trioxide aggregate. Int Endod J 2008;41:408-417.ArticlePubMed
- 32. Chang SW. Chemical characteristics of mineral trioxide aggregate and its hydration reaction. Restor Dent Endod 2012;37:188-193.ArticlePubMedPMC
- 33. Yasuda Y, Ogawa M, Arakawa T, Kadowaki T, Saito T. The effect of mineral trioxide aggregate on the mineralization ability of rat dental pulp cells: an in vitro study. J Endod 2008;34:1057-1060.ArticlePubMed
REFERENCES
Tables & Figures
REFERENCES
Citations
Citations to this article as recorded by 
- Bioactivity and biocompatibility of bioceramic-based pulp capping materials in laboratory and animal models
Rafiqul Islam, Md. Refat Readul Islam, Kenta Tsuchiya, Yu Toida, Hidehiko Sano, Monica Yamauti, Hany Mohamed Aly Ahmed, Atsushi Tomokiyo
Journal of Materials Science: Materials in Medicine.2025;[Epub] CrossRef - The road map to proper dental pulp experiments in animal models
Nuha A Elmubarak
International Dental Journal of Student's Research.2024; 11(4): 163. CrossRef - Treatment outcomes of root perforations repaired by calcium silicate-based cements with or without an accelerator: A randomized controlled trial
Kanyarat Tungputsa, Danuchit Banomyong, Sittichoke Osiri, Supachai Sutimuntanakul
Endodontology.2024; 36(4): 315. CrossRef - Biological evaluation of novel phosphorylated pullulan‐based calcium hydroxide formulations as direct pulp capping materials: An in vivo study on a rat model
Md Refat Readul Islam, Rafiqul Islam, Yunqing Liu, Yu Toida, Yasuhiro Yoshida, Hidehiko Sano, Hany Mohamed Aly Ahmed, Atsushi Tomokiyo
International Endodontic Journal.2024; 57(9): 1247. CrossRef - 3D-printed microgels supplemented with dentin matrix molecules as a novel biomaterial for direct pulp capping
Diana Cunha, Nayara Souza, Manuela Moreira, Nara Rodrigues, Paulo Silva, Cristiane Franca, Sivaporn Horsophonphong, Ashley Sercia, Ramesh Subbiah, Anthony Tahayeri, Jack Ferracane, Pamela Yelick, Vicente Saboia, Luiz Bertassoni
Clinical Oral Investigations.2022; 27(3): 1215. CrossRef - Calcium silicate and calcium aluminate cements for dentistry reviewed
Carolyn Primus, James L. Gutmann, Franklin R. Tay, Anna B. Fuks
Journal of the American Ceramic Society.2022; 105(3): 1841. CrossRef - Pulpal response to mineral trioxide aggregate containing phosphorylated pullulan-based capping material
Yu TOIDA, Shimpei KAWANO, Rafiqul ISLAM, Fu JIALE, AFM A CHOWDHURY, Shuhei HOSHIKA, Yasushi SHIMADA, Junji TAGAMI, Masahiro YOSHIYAMA, Satoshi INOUE, Ricardo M. CARVALHO, Yasuhiro YOSHIDA, Hidehiko SANO
Dental Materials Journal.2022; 41(1): 126. CrossRef - The Effect of Calcium-Silicate Cements on Reparative Dentinogenesis Following Direct Pulp Capping on Animal Models
Mihai Andrei, Raluca Paula Vacaru, Anca Coricovac, Radu Ilinca, Andreea Cristiana Didilescu, Ioana Demetrescu
Molecules.2021; 26(9): 2725. CrossRef - Histological evaluation of a novel phosphorylated pullulan‐based pulp capping material: An in vivo study on rat molars
Rafiqul Islam, Yu Toida, Fei Chen, Toru Tanaka, Satoshi Inoue, Tetsuya Kitamura, Yasuhiro Yoshida, Abu Faem Mohammad Almas Chowdhury, Hany Mohamed Aly Ahmed, Hidehiko Sano
International Endodontic Journal.2021; 54(10): 1902. CrossRef - Effectiveness of Direct Pulp Capping Bioactive Materials in Dentin Regeneration: A Systematic Review
Ermin Nie, Jiali Yu, Rui Jiang, Xiangzhen Liu, Xiang Li, Rafiqul Islam, Mohammad Khursheed Alam
Materials.2021; 14(22): 6811. CrossRef - A strontium and amorphous calcium phosphate dipped premixed injectable calcium silicate-based ceramic for dental root canal sealing
Huimin Jin, Yuzhu Li, Qingqing Wang, Menglu Dong, Mengmeng Yang, Wendy Chen, Shengrui Wang, Heng Zhang, Shunli Zheng, Chris Ying Cao, Zheng Zhou, Quan-Li Li
Ceramics International.2021; 47(23): 33738. CrossRef - Bioactive tri/dicalcium silicate cements for treatment of pulpal and periapical tissues
Carolyn M. Primus, Franklin R. Tay, Li-na Niu
Acta Biomaterialia.2019; 96: 35. CrossRef
 ePub Link
ePub Link Cite
CiteEffects of the exposure site on histological pulpal responses after direct capping with 2 calcium-silicate based cements in a rat model

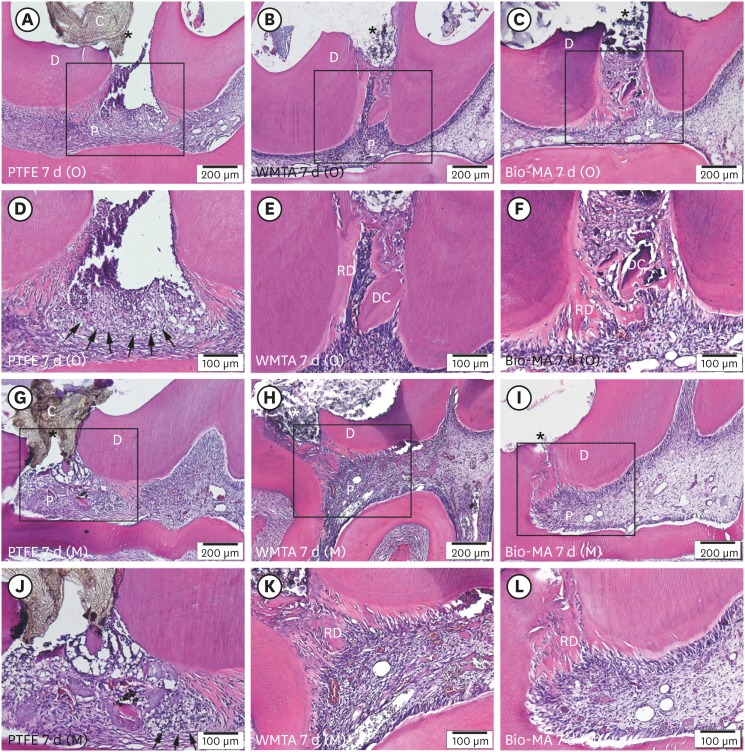
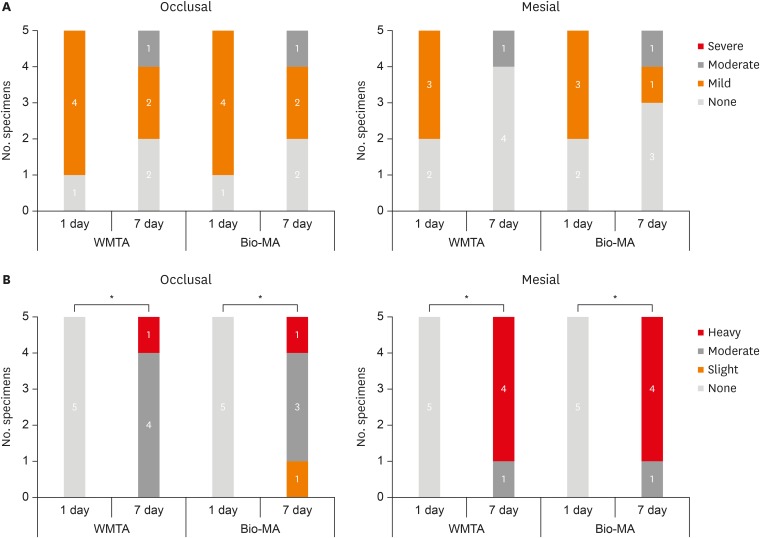
Figure 1 Effects of direct capping at 1 day on mechanically exposed pulp at occlusal (A-F) and mesial (G-L) sites. Mild inflammation with limited accumulation of polymorphonuclear leukocytes (black arrows) and congested blood vessels were observed at the exposure areas in the PTFE (positive control: A, D, G, and J), WMTA (B, E, H, and K), and Bio-MA (C, F, I, and L) groups. D-F and J-L present a high-magnification view (×400) of the areas demarcated by the black rectangles in A-C and G-I (×100), respectively.P, pulp; D, dentin; DC, dentin chips; C, capping material.Asterisk (*) indicates pulp exposure site.
Figure 2 Effects of direct capping at 7 days on mechanically exposed pulp at occlusal (A-F) and mesial (G-L) sites. Moderate pulpal inflammation was observed, with extensive infiltration of inflammatory cells (arrows) and no hard tissue deposition at the exposure site in the positive control groups (A, D, G, and J). No inflammation with moderate hard tissue deposition was detected in the WMTA (B, E, H, and K) and Bio-MA (C, F, I, and L) groups. D-F and J-L present a high-magnification view (×200) of the areas demarcated by the black rectangles in A-C and G-I (×100), respectively.P, pulp; D, dentin; DC, dentin chips; C, capping material; RD, reparative dentin.Asterisk (*) indicates pulp exposure site.
Figure 3 Comparison of (A) the inflammatory response and (B) reparative dentin formation in the experimental groups between the 2 observation periods. Asterisk (*) indicates a significant difference, with p < 0.01.
Figure 1
Figure 2
Figure 3
Effects of the exposure site on histological pulpal responses after direct capping with 2 calcium-silicate based cements in a rat model
Evaluation criteria for the histopathological analysis of pulpal tissue responses after mechanical pulp exposure and direct pulp capping in rats
| Inflammatory cell infiltration | |
| 0 | None: absent or few scattered inflammatory cells |
| 1 | Mild: inflammatory cells limited to the area of pulp exposure or dentin bridge |
| 2 | Moderate: inflammatory cell infiltration of more than one-third, but not all of the coronal pulp |
| 3 | Severe: all of the coronal pulp is infiltrated with inflammatory cells or necrotic |
| Reparative dentin formation | |
| 0 | None: no hard tissue deposition |
| 1 | Slight: scattered dentin bridge formation at less than 50% of the exposure site |
| 2 | Moderate: discontinuous dentin bridge formation at more than 50% of the exposure site, but not completely covering the exposure site |
| 3 | Heavy: a continuous dentin bridge completely covers the exposure site |
| Bacterial detection | |
| 0 | Absent or few scattered bacteria next to the area of pulp exposure or dentin bridge |
| 1 | Presence of bacteria with a clearly visible amount in the coronal pulp |
| Impaction of dentin fragments into the pulp | |
| 0 | No impaction |
| 1 | Impaction |
Grading of pulpal responses (inflammatory cell infiltration and reparative dentin formation) to direct pulp capping with 2 calcium-silicate cements and positive controls in rats
| Observation period | No. of specimens | Inflammatory cell response score | Reparative dentin formation score | |||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| 0 | 1 | 2 | 3 | Median | 0 | 1 | 2 | 3 | Median | |||
| 1 day | ||||||||||||
| PTFE (occlusal) | 3 | 0 | 2 | 1 | 0 | 1 | 3 | 0 | 0 | 0 | 0 | |
| PTFE (mesial) | 3 | 0 | 2 | 1 | 0 | 1 | 3 | 0 | 0 | 0 | 0 | |
| WMTA (occlusal) | 5 | 1 | 4 | 0 | 0 | 1 | 5 | 0 | 0 | 0 | 0 | |
| WMTA (mesial) | 5 | 2 | 3 | 0 | 0 | 1 | 5 | 0 | 0 | 0 | 0 | |
| Bio-MA (occlusal) | 5 | 1 | 4 | 0 | 0 | 1 | 5 | 0 | 0 | 0 | 0 | |
| Bio-MA (mesial) | 5 | 2 | 3 | 0 | 0 | 1 | 5 | 0 | 0 | 0 | 0 | |
| 7 days | ||||||||||||
| PTFE (occlusal) | 3 | 0 | 0 | 2 | 1 | 2 | 3 | 0 | 0 | 0 | 0 | |
| PTFE (mesial) | 3 | 0 | 0 | 3 | 0 | 2 | 3 | 0 | 0 | 0 | 0 | |
| WMTA (occlusal) | 5 | 2 | 2 | 1 | 0 | 1 | 0 | 0 | 4 | 1 | 2 | |
| WMTA (mesial) | 5 | 4 | 0 | 1 | 0 | 0 | 0 | 0 | 1 | 4 | 3 | |
| Bio-MA (occlusal) | 5 | 2 | 2 | 1 | 0 | 1 | 0 | 1 | 3 | 1 | 2 | |
| Bio-MA (mesial) | 5 | 3 | 1 | 1 | 0 | 0 | 0 | 0 | 1 | 4 | 3 | |
PTFE, polytetrafluoroethylene; WMTA, white mineral trioxide aggregate.
Size of pulp exposure in the occlusal- and mesial-approach groups
| Group | Size of pulp exposure (µm) | |
|---|---|---|
| Occlusal | ||
| Positive control (1 day) | 255.9 ± 58.2 | |
| WMTA (1 day) | 261.3 ± 104.4 | |
| Bio-MA (1 day) | 216.8 ± 83.8 | |
| Positive control (7 days) | 233.9 ± 32.4 | |
| WMTA (7 days) | 207.5 ± 67.5 | |
| Bio-MA (7 days) | 231.4 ± 88.4 | |
| Overall | 234.5 ± 72.5 | |
| Mesial | ||
| Positive control (1 day) | 161.2 ± 35.8 | |
| WMTA (1 day) | 179.4 ± 47.5 | |
| Bio-MA (1 day) | 159.8 ± 16.7 | |
| Positive control (7 days) | 168.1 ± 57.1 | |
| WMTA (7 days) | 150.9 ± 41.2 | |
| Bio-MA (7 days) | 181.2 ± 101.4 | |
| Overall | 166.8 ± 50.0 | |
WMTA, white mineral trioxide aggregate.
Table 1 Evaluation criteria for the histopathological analysis of pulpal tissue responses after mechanical pulp exposure and direct pulp capping in rats
Table 2 Grading of pulpal responses (inflammatory cell infiltration and reparative dentin formation) to direct pulp capping with 2 calcium-silicate cements and positive controls in rats
PTFE, polytetrafluoroethylene; WMTA, white mineral trioxide aggregate.
Table 3 Size of pulp exposure in the occlusal- and mesial-approach groups
WMTA, white mineral trioxide aggregate.

