
Articles
- Page Path
- HOME > Restor Dent Endod > Volume 42(3); 2017 > Article
- Research Article Comparing the effect of a desensitizing material and a self-etch adhesive on dentin sensitivity after periodontal surgery: a randomized clinical trial
-
Hila Hajizadeh1,2, Atefeh Nemati-Karimooy2
 , Sara Majidinia1,2, Amir Moeintaghavi3, Marjaneh Ghavamnasiri1
, Sara Majidinia1,2, Amir Moeintaghavi3, Marjaneh Ghavamnasiri1 -
2017;42(3):-175.
DOI: https://doi.org/10.5395/rde.2017.42.3.168
Published online: July 21, 2017
1Dental Research Center, Mashhad University of Medical Sciences, Mashhad, Iran.
2Department of Restorative and Cosmetic Dentistry, School of Dentistry, Mashhad University of Medical Sciences, Mashhad, Iran.
3Department of Periodontics, School of Dentistry, Mashhad University of Medical Sciences, Mashhad, Iran.
- Correspondence to Atefeh Nemati-Karimooy, DDS, MS. Assistant Professor, Department of Restorative and Cosmetic Dentistry, Mashhad University of Medical Sciences School of Dentistry, Vakil-Abad Blvd., Mashhad 91735, Iran. Tel: +98-9151098060, Fax: +98-51-38832300, Nematika@mums.ac.ir
• Received: November 28, 2016 • Accepted: June 22, 2017
Copyright © 2017. The Korean Academy of Conservative Dentistry
This is an Open Access article distributed under the terms of the Creative Commons Attribution Non-Commercial License (https://creativecommons.org/licenses/by-nc/3.0/) which permits unrestricted non-commercial use, distribution, and reproduction in any medium, provided the original work is properly cited.
- 3,688 Views
- 11 Download
- 11 Crossref
Abstract
-
Objectives This double-blind randomized placebo-controlled clinical trial evaluated the ability of a desensitizing agent and a self-etch adhesive on cervical dentin sensitivity (CDS) after periodontal surgery.
-
Materials and Methods Ninety hypersensitive teeth of 13 subjects were included in the study. After periodontal surgery, the teeth of each posterior sextant treated with one of the following materials: G1: Clearfil S3 Bond (Kuraray Dental), G2: Gluma Desensitizer (Heraeus Kulzer), and G3: placebo (water). The sensitivity was assessed using evaporative stimuli before treatment (baseline, T0), 1 day after treatment (T1), after 1 week (T2), and after 1 month (T3) according to visual analog scale (VAS).
-
Results Following the treatment, all the 3 groups showed significant reduction of CDS in T1 compared to T0. Reduction of CDS between T1 and T2 was observed only in G1 but there was no significant difference between T2 and T3 in this group. Although we observed a significant difference in T3 compared to T1 and T2 in G2 and G3, comparison of treatment groups in each assessment time showed a significant difference only in T3. According to paired comparison, this was due to the difference between G2 and G3.
-
Conclusions Dentin sensitivity following periodontal surgery will decrease spontaneously over time, but treating the sensitive teeth with Gluma Desensitizer and Clearfil S3 Bond can have some benefits.
INTRODUCTION
Cervical dentin sensitivity (CDS) is one of the most common painful conditions affecting oral comfort and function and can be defined as a painful symptom of the exposed dentin in response to chemical, thermal, tactile or osmotic stimuli which cannot be explained by any other dental defect or pathology [1,2]. The occurrence of CDS ranges from 3 up to 98%. This vast range can be explained by the differences in the selection criteria for the study sample and also the variety in diagnostic approaches or time frames. Women are slightly more affected than men with an age peak of 30 to 40 years [3]. Exposure of root surface by loss of the overlying cementum and periodontal tissues is one of the most common etiological factors related to CDS [4].
The most widely accepted explanation for tooth sensitivity is Brännström and Åström's hydrodynamic theory [5]. According to this theory, the exogenous stimuli applied to the exposed dentinal tubules result in the flow of dentinal tubular fluid, activate the intratubular nerve endings, and create pain. The number, size, and diameter of the open dentinal tubules are important factors that determine the degree of hypersensitivity in the subjects [6]. Recently, two strategies are used for the treatment of CDS. One is occluding the dentine tubules and the other is interfering with the sensitivity of the mechanoreceptors [7]. A variety of products have been developed with the aim of alleviating the discomfort arising from the CDS [8].
Some researchers believe that self-etch adhesives can reduce dentin sensitivity by decreasing dentin permeability [9,10] due to production of an acid-resistant hybrid layer [11]. This acid-base resistance zone may result in longer lasting clinical effectiveness. Yu et al. [12] showed that the one-bottle self-etching adhesives and dentin desensitizers could significantly relieve CDS (which was not due to periodontal surgery) immediately and over the course of a month after treatment.
The aim of the current clinical study was to compare the clinical effectiveness of a dentin desensitizer, a one-bottle self-etching adhesive, and a placebo for CDS treatment after periodontal surgery and the null hypotheses of the present study was that all three methods have the same clinical effectiveness at different interval times.
MATERIALS AND METHODS
According to the study of Yu et al. [12], 14 patients who were planned to undergo surgical periodontal treatment in at least three posterior sextants were recruited into this randomized, double-blinded, placebo-controlled, split-mouth study.
These patients were referred to the Department of Restorative and Cosmetic Dentistry of Mashhad University of Medical Sciences for desensitizing treatment if they had complained about CDS after removing the periodontal pack of the first sextant. Participants were given a brief explanation about the investigation and all consented to participate and signed a consent form approved by the Committee on Ethics in Research, Mashhad University of Medical Sciences. This trial was registered at: http://www.IRCT.ir and its identification number is IRCT201408176267N2.
The inclusion and exclusion criteria are stated in Figure 1.
Figure 1
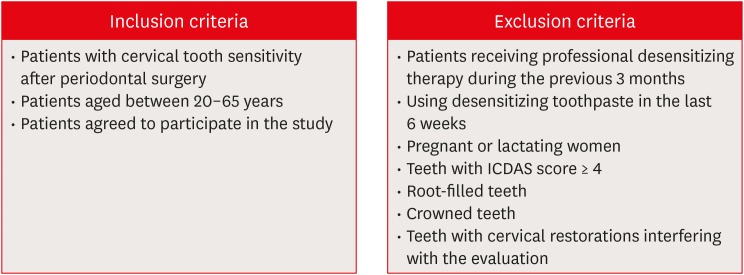
Inclusion and exclusion criteria.
ICDAS, International Caries Detection and Assessment System.
All the patients had moderate to severe chronic periodontitis. This means that all of them had more than 4 mm attachment loss and more than 5 mm periodontal pockets, so all of them needed periodontal surgery which was contained flap debridement, scaling and root planning and respective osseous surgery as needed, suturing, and covering the area with dressing. Generally, patients with periodontal diseases suffer from some degrees of dental hypersensitivity which usually increases after scaling and root planning or periodontal surgery. Because the periodontal pack was removed between 1 to 2 weeks after the surgery, the first treatment session was scheduled 10–20 days after the surgery of the first sextant.
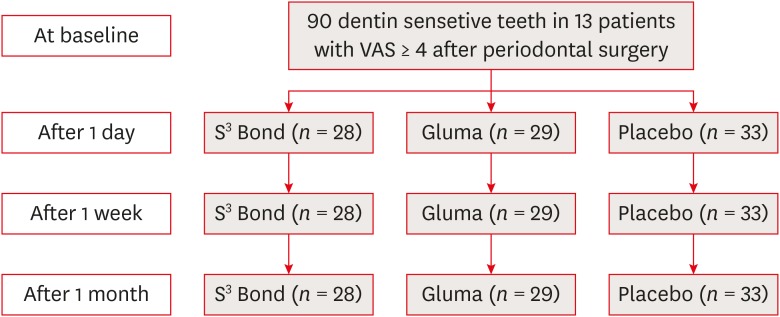
A total of 96 teeth with CDS after periodontal surgery were considered suitable for the study and the rate of sensitivity to the cold air stimulation was recorded at baseline (T0) for each tooth according to visual analog scale (VAS). To produce the stimuli, 2-second air blast (45 psi, 19°C–24°C) was applied using an air syringe held 2 mm away, and perpendicular to the tooth surface whilst shielding adjacent teeth with the operator's fingers. In this step only teeth with VAS score of 4 and more (teeth with moderate to severe sensitivity) were selected for study. In order to avoid bias, each sextant was randomly allocated to one of 3 treatment groups by choosing an envelope containing the order of treatment options which were placebo (distilled water), Gluma Desensitizer (Heraeus Kulzer, Hanau, Germany), and Clearfil S3 Bond (Kuraray Dental, Okayama, Japan). The teeth of the different sextants received different treatment and the adjacent teeth received the same material. By using a split mouth study design, three study groups, had the advantages of similar pain perception, oral hygiene habits, dietary habits, and psychosomatic factors in the same patient. Allocating the samples in each group is showed in Figure 2.
After anesthetizing each sextant, the teeth were cleaned very gently using cotton swap, microbrush, and supper floss. The area was isolated with cotton rolls and the selected material was applied basically according to the manufacture's instruction. In the first group (G1, n = 28), the self-etch adhesive, Clearfil S3 Bond was applied for 20 seconds, dried with high-pressure air flow for 5 seconds and light cured for 10 seconds according to manufacture. Then in order to assimilate with the Gluma material, the area was rinsed with water. In the second group (G2, n = 29), Gluma Desensitizer was applied for 30–60 seconds on the sensitive area, the solvent evaporated gently, then, the tip of an off light cure unit was positioned on the area for 10 seconds in order to assimilate with adhesive group, so, the patient remained blind about the treatment procedure. Finally, the area was rinsed with water. In the third group (G3, n = 33), the placebo (distilled water) was applied the same as Gluma Desensitizer. All subjects were instructed not to brush their teeth, eat, drink or rinse their mouth for at least 2 hours after each treatment.
A clinical evaluation of each tooth was assessed by another investigator who was not involved with the treatment procedure. Air stimulation response measurement was done via VAS as the baseline evaluation (T0) and data were collected on each tooth, 1 day (T1), 1 week (T2), and 1 month after treatment (T3). The same examiner calculated the total VAS score of each study group at each follow-up time from the mean of the VAS scores of all the treated teeth of every subject in the same group.
All the data were analyzed using the SPSS software package (version 16.0, SPSS Inc., Chicago, IL, USA). The normality of the data was checked using Kolmogorov-Smirnov test. Repeated measurement analysis assessed the interaction of follow-up time and treatment group. Hotelling's Trace test was used to analyze the efficacy of all the materials in each of the follow-up times. Analysis of variance (ANOVA) test followed by Tukey test as its post hoc was used to assess each material in different investigation times (baseline, 1 day, 1 week, and 1 month after treatment). The level of significance was set at α = 0.05.
RESULTS
At the beginning of the survey, 6 males and 8 females between the ages of 20 and 65 years recruited in the study but one of the patients excluded, because all his teeth in the last sextant undergone surgery showed VAS scores less than 4, so we had not 3 sensitive sextants to treat. Therefore, a total of 52 premolars and 38 molars remained in the three study groups.
First, the normality of the data was confirmed with Kolmogorov-Smirnov test. There was no significant difference between all groups in base line sensitivity (p = 0.83).
Repeated measurement analysis considering follow-up time and treatment group showed the interaction of this 2 variables. So, Hotelling's Trace test showed a significant difference between all assessment times in all 3 groups. Therefore, paired comparison of groups according to the assessment times was done. The results have been shown in Table 1.
Table 1
Mean visual analog scale (VAS) scores for each treatment group within each assessment time
The data were presented as mean ± standard deviation.
Same superscript letter indicates no significant differences between groups as per the results of pairwise multiple comparisons (p < 0.05). Lowercase superscripts denote differences in each row (horizontal). Uppercase superscripts denote differences in each column (vertical).
ANOVA test was used to assess each treatment group in different investigation times (baseline, 1 day, 1 week, and 1 month after treatment). The results of this test showed a significant difference only in the last follow-up time (T3, p = 0.029). Accordingly, Tukey test was used for paired comparison of treatment groups in the last follow-up time and showed a significant difference between G2 and G3 (p < 0.05).
DISCUSSION
The current clinical study tried to compare the clinical effectiveness of Gluma Desensitizer, Clearfil S3 Bond (one-bottle self-etching adhesive), and placebo (distilled water) for CDS treatment after periodontal surgery in different evaluation times by using VAS. Several studies noted that the patient may encounter abrupt and severe dentin sensitivity after periodontal therapies [13,14]. Also, the occurrence and severity of CDS directly depend on the type of periodontal treatment and are greater after surgical procedures [15]. The main reason for sensitivity is exposing dentinal tubules to the oral environment [16]. Thus, the basis of most desensitizing treatments is to block these tubules.
To date, only few studies have evaluated the effect of dentin bonding agents in reducing CDS [17,18,19,20,21]. Even these studies rarely assessed all-in-one adhesives and CDS following periodontal surgery [12,22]. The results of this study showed that in the group treated with Clearfil S3 Bond, CDS values reduced 1 day after treatment and the reduction continued for 1 week after treatment. This may be due to the concurrent effect of natural tubule blocking factors over time and blocking effect of adhesive material. According to microscopic findings, topical application of these adhesives on the sensitive dentinal areas resulted in occlusion of the patent tubules and produced an acid-base resistant hybrid layer on the dentin surface [23]. This acid-base resistant zone is a combination of dentin and the adjacent hybrid layer. Since this layer is mechanically, chemically, and biologically more resistant than normal dentin, it is also called ‘Super Dentin’ [23]. One of the functional monomers with the ability to create Super Dentin is 10-methacryloyloxydecyl dihydrogen phosphate (10-MDP) [24]. Clearfil S3 Bond contains 10-MDP.
On the other hand, Yu et al. [12] showed that some occluded dentinal tubules partly reopened 1 month after treatment and so some sensitivity returned after 1 month. The reason might be the fact that all-in-one adhesives contain mixtures of more hydrophilic monomers, and thus, are permeable to water after application to the dentinal surface [9]. However, our study showed reduction of CDS over time after applying Clearfil S3 Bond. It seems that time factor could add some positive effect during 1 month.
According to this study, as there were significant difference between T1 and T2 with T3, Gluma can reduce CDS 1 day after treatment. Moreover, gradual reduction of CDS happened in this treatment group over the investigation period. These results are consistent with the results of other studies, which have shown the same reduction [12,22,25,26]. It has been noted that the effect of Gluma (5% glutaraldehyde and 35% hydroxyethyl methacrylate [HEMA] marketed as Gluma Desitizer) as a desensitizer to block dentinal tubules occurs through 2 mechanisms: first, through denaturation of dentinal fluid proteins by glutaraldehyde and second, through polymerization of HEMA. Both of them result in decrease in dentin permeability [27].
The present study showed that placebo can significantly reduce CDS one day after treatment. Patient's supposition of receiving a treatment can be effective on decreasing CDS, because pain is a subjective phenomenon. This mechanism is undeniable and is shown by many investigations. Therefore, the efficacy of placebo in one day after treatment can be explained by its psychological effects [12,18,22]. Additionally, the mean of VAS in placebo group decreased gradually over time. This is not in line with the results of the study by Yu et al. [12], which showed that some of the CDS will return during one month. This difference may be explained by the various conditions of studies. The present study was implemented on CDS following periodontal surgery, but in the study by Yu et al. [12], it was performed on sensitive teeth which did not passed any surgical procedure. Therefore, in this study, cervical dentin had been suddenly exposed to oral environment and the natural factors such as saliva protein precipitation, smear layer formation, and remineralization, did not have enough time to block tubules and decrease CDS. While, in the study by Yu et al. [12], cervical dentin have been exposed to oral environment for long a time and those natural processes would not meet any additional effect even if they had more time. Studies have shown that some natural factors, can decrease dentin permeability and therefore decrease CDS over time [28,29,30].
This study noted that Gluma was the most effective and placebo the least effective treatment of CDS among three groups in the last follow up time. The effectiveness of Gluma may be due to its dual effect of HEMA and glutaraldehyde. Since Gluma has low viscosity and does not need light curing, it is more user-friendly and less technique sensitive than Clearfil S3 Bond, especially in interproximal areas. Also, our investigation showed that the effectiveness of Clearfil S3 Bond is the same as Gluma and placebo in 1 day and 1 week follow-up times and have significant difference with Gluma after 1 month. Since this adhesive affects CDS reduction only by polymerization into the dentinal tubules, it seems that it can merely meet just one of the action mechanisms of Gluma Desensitizer. The problem of not being sure of the successful light curing of resin in more difficult accessible areas might also reduce its effectiveness in CDS treatment. Although, the all-in-one adhesive tested in the current study did not perform better than the dentin desensitizer, but it could reduce the CDS to some degree.
CONCLUSIONS
According to the limitations of this study, it was shown that also dentin sensitivity following periodontal surgery will decrease spontaneously over time, but treating the sensitive teeth with Gluma Desensitizer and Clearfil S3 Bond can have some benefits.
ACKNOWLEDGEMENT
The results of presented study have been taken from a post-graduate thesis (no: 930240) approved and supported by Mashhad University of Medical Sciences.
-
Conflict of Interest: No potential conflict of interest relevant to this article was reported.
-
Author Contributions:
Conceptualization: Ghavamnasiri M.
Data curation: Hajizadeh H.
Formal analysis: Moeintaghavi A.
Funding acquisition: Hajizadeh H.
Investigation: Nemati-Karimooy A.
Methodology: Moeintaghavi A.
Project administration: Hajizadeh H.
Software: Hajizadeh H.
Supervision: Ghavamnasiri M.
Validation: Majidinia S.
Visualization: Ghavamnasiri M.
Writing - original draft: Nemati-Karimooy A, Hajizadeh H.
Writing - review & editing: Nemati-Karimooy A, Majidinia S, Ghavamnasiri M.
- 1. Davari A, Ataei E, Assarzadeh H. Dentin hypersensitivity: etiology, diagnosis and treatment; a literature review. J Dent (Shiraz) 2013;14:136-145.PubMedPMC
- 2. Canadian Advisory Board on Dentin Hypersensitivity. Consensus-based recommendations for the diagnosis and management of dentin hypersensitivity. J Can Dent Assoc 2003;69:221-226.PubMed
- 3. Splieth CH, Tachou A. Epidemiology of dentin hypersensitivity. Clin Oral Investig 2013;17(Supplement 1):S3-S8.ArticlePubMedPDF
- 4. Walters PA. Dentinal hypersensitivity: a review. J Contemp Dent Pract 2005;6:107-117.Article
- 5. Brännström M, Åström A. A study on the mechanism of pain elicited from the dentin. J Dent Res 1964;43:619-625.ArticlePubMedPDF
- 6. Yoshiyama M, Suge T, Kawasaki A, Ebisu S. Morphological characterization of tube-like structures in hypersensitive human radicular dentine. J Dent 1996;24:57-63.PubMed
- 7. Ling TY, Gillam DG. The effectiveness of desensitizing agents for the treatment of cervical dentine sensitivity (CDS)--a review. J West Soc Periodontol Periodontal Abstr 1996;44:5-12.PubMed
- 8. Lin PY, Cheng YW, Chu CY, Chien KL, Lin CP, Tu YK. In-office treatment for dentin hypersensitivity: a systematic review and network meta-analysis. J Clin Periodontol 2013;40:53-64.ArticlePubMedPDF
- 9. Fu B, Shen Y, Wang H, Hannig M. Sealing ability of dentin adhesives/desensitizer. Oper Dent 2007;32:496-503.ArticlePubMedPDF
- 10. Grégoire G, Joniot S, Guignes P, Millas A. Dentin permeability: self-etching and one-bottle dentin bonding systems. J Prosthet Dent 2003;90:42-49.ArticlePubMed
- 11. Tsuchiya S, Nikaido T, Sonoda H, Foxton RM, Tagami J. Ultrastructure of the dentin-adhesive interface after acid-base challenge. J Adhes Dent 2004;6:183-190.PubMed
- 12. Yu X, Liang B, Jin X, Fu B, Hannig M. Comparative in vivo study on the desensitizing efficacy of dentin desensitizers and one-bottle self-etching adhesives. Oper Dent 2010;35:279-286.ArticlePubMedPDF
- 13. Al-Sabbagh M, Beneduce C, Andreana S, Ciancio SG. Incidence and time course of dentinal hypersensitivity after periodontal surgery. Gen Dent 2010;58:e14-e19.PubMed
- 14. Nishida M, Murayama Y, Nomura Y, Asano K, Ujimoto F, Shinoda S, Sakan J, Uchida A, Katamsi D, Yokomizo I. Hypersensitivity of the exposed root surface after the surgical periodontal treatment. Nippon Shishubyo Gakkai Kaishi 1976;18:502-510.
- 15. Lin YH, Gillam DG. The prevalence of root sensitivity following periodontal therapy: a systematic review. Int J Dent 2012;2012:407023.ArticlePubMedPMCPDF
- 16. Absi EG, Addy M, Adams D. Dentine hypersensitivity. A study of the patency of dentinal tubules in sensitive and non-sensitive cervical dentine. J Clin Periodontol 1987;14:280-284.PubMed
- 17. Duran I, Sengun A. The long-term effectiveness of five current desensitizing products on cervical dentine sensitivity. J Oral Rehabil 2004;31:351-356.ArticlePubMed
- 18. Gillam DG, Coventry JF, Manning RH, Newman HN, Bulman JS. Comparison of two desensitizing agents for the treatment of cervical dentine sensitivity. Endod Dent Traumatol 1997;13:36-39.ArticlePubMed
- 19. Ide M, Morel AD, Wilson RF, Ashley FP. The role of a dentine-bonding agent in reducing cervical dentine sensitivity. J Clin Periodontol 1998;25:286-290.PubMed
- 20. Prati C, Cervellati F, Sanasi V, Montebugnoli L. Treatment of cervical dentin hypersensitivity with resin adhesives: 4-week evaluation. Am J Dent 2001;14:378-382.PubMed
- 21. Swift EJ Jr, May KN Jr, Mitchell S. Clinical evaluation of Prime & Bond 2.1 for treating cervical dentin hypersensitivity. Am J Dent 2001;14:13-16.PubMed
- 22. Kakaboura A, Rahiotis C, Thomaidis S, Doukoudakis S. Clinical effectiveness of two agents on the treatment of tooth cervical hypersensitivity. Am J Dent 2005;18:291-295.PubMed
- 23. Inoue G, Tsuchiya S, Nikaido T, Foxton RM, Tagami J. Morphological and mechanical characterization of the acid-base resistant zone at the adhesive-dentin interface of intact and caries-affected dentin. Oper Dent 2006;31:466-472.ArticlePubMedPDF
- 24. Nikaido T, Inoue G, Takagaki T, Waidyasekera K, Iida Y, Shinohara MS, Sadr A, Tagami J. New strategy to create “Super Dentin” using adhesive technology: reinforcement of adhesive–dentin interface and protection of tooth structures. Jpn Dent Sci Rev 2011;47:31-42.Article
- 25. Polderman RN, Frencken JE. Comparison between effectiveness of a low-viscosity glass ionomer and a resin-based glutaraldehyde containing primer in treating dentine hypersensitivity--a 25.2-month evaluation. J Dent 2007;35:144-149.ArticlePubMed
- 26. Aranha AC, Pimenta LA, Marchi GM. Clinical evaluation of desensitizing treatments for cervical dentin hypersensitivity. Braz Oral Res 2009;23:333-339.ArticlePubMed
- 27. Qin C, Xu J, Zhang Y. Spectroscopic investigation of the function of aqueous 2-hydroxyethylmethacrylate/glutaraldehyde solution as a dentin desensitizer. Eur J Oral Sci 2006;114:354-359.ArticlePubMed
- 28. Kawasaki A, Ishikawa K, Suge T, Shimizu H, Suzuki K, Matsuo T, Ebisu S. Effects of plaque control on the patency and occlusion of dentine tubules in situ . J Oral Rehabil 2001;28:439-449.ArticlePubMed
- 29. Pashley DH. Dentin permeability, dentin sensitivity, and treatment through tubule occlusion. J Endod 1986;12:465-474.ArticlePubMed
- 30. Pashley DH, Nelson R, Kepler EE. The effects of plasma and salivary constituents on dentin permeability. J Dent Res 1982;61:978-981.ArticlePubMedPDF
REFERENCES
Tables & Figures
REFERENCES
Citations
Citations to this article as recorded by 
- Effect of different material protocols on the control of dentin hypersensitivity: a split-mouth randomized controlled clinical trial
Júlia Marques Martins, Maria Fernanda Ferreira Nogueira, Guilherme José Pimentel Lopes de Oliveira, Alexandre Coelho Machado, Paulo César de Freitas Santos Filho, Hugo Lemes Carlo, Carlos José Soares, Gisele Rodrigues da Silva
Clinical Oral Investigations.2026;[Epub] CrossRef - Biomineralization reaction from nanosized calcium silicate: A new method for reducing dentin hypersensitivity
Mi-Jeong Jeon, Yu-Sung Choi, Jeong-Kil Park, Jin-Soo Ahn, Yu-Chih Chiang, Deog-Gyu Seo
Journal of Dental Sciences.2025; 20(1): 428. CrossRef - Effectiveness of Self-etching Adhesive Only Versus in Combination with Gluma Desensitizer for Preventing Post-composite Sensitivity - A Prospective Study
Hemamalini Rath, Shilpa Mahapatra, Sri Priya Narayanan
Indian Journal of Dental Research.2025; 36(1): 32. CrossRef - Efficacy of seventh generation bonding agents as desensitizers in patients with dentin hypersensitivity: a randomized clinical trial
Sumaiya Shabbir, Shahbaz Ahmed, Syed Jaffar Abbas Zaidi, Sania Riaz, Huma Sarwar, Muhammad Taqi, Zia ur Rahman Khan
BMC Oral Health.2024;[Epub] CrossRef - Investigation of the crystal formation from calcium silicate in human dentinal tubules and the effect of phosphate buffer saline concentration
Mi-Jeong Jeon, Jin-Soo Ahn, Jeong-Kil Park, Deog-Gyu Seo
Journal of Dental Sciences.2024; 19(4): 2278. CrossRef - The effect of fluoride iontophoresis on seal ability of self-etch adhesive in human dentin in vitro
Kanittha Kijsamanmith, Parintorn Wallanon, Chanya Pitchayasatit, Poonnapha Kittiratanaviwat
BMC Oral Health.2022;[Epub] CrossRef - The study of toothpaste desensitizing properties
S. B. Ulitovskiy, O. V. Kalinina, A. A. Leontev, O. V. Khabarova, L. I. Pankrateva, E. S. Soloveva, N. K. Fok
Parodontologiya.2022; 27(1): 81. CrossRef - Effectiveness and cytotoxicity of two desensitizing agents: a dentin permeability measurement and dentin barrier testing in vitro study
Ruodan Jiang, Yongxiang Xu, Feilong Wang, Hong Lin
BMC Oral Health.2022;[Epub] CrossRef - A randomized clinical trial of dentin hypersensitivity reduction over one month after a single topical application of comparable materials
Samar Hatem Abuzinadah, Abdulrahman Jafar Alhaddad
Scientific Reports.2021;[Epub] CrossRef - Comparison between effectiveness of dentine desensitizer and one bottle self-etch adhesive on dentine hypersensitivity
Muhammad Zohaib Younus, Muhammad Adeel Ahmed, Azeem Ul Yaqin Syed, Jiand Malik Baloch, Muhammad Ali, Abubakar Sheikh
Technology and Health Care.2021; 29(6): 1153. CrossRef - A long-term evaluation of experimental potassium oxalate concentrations on dentin hypersensitivity reduction: A triple-blind randomized clinical trial
Alexia da Mata Galvão, Livia Fávaro Zeola, Guilherme Faria Moura, Daniela Navarro Ribeiro Teixeira, Ramon Corrêa de Queiroz Gonzaga, Gisele Rodrigues da Silva, Paulo Vinícius Soares
Journal of Dentistry.2019; 89: 103180. CrossRef
 ePub Link
ePub Link Cite
CiteComparing the effect of a desensitizing material and a self-etch adhesive on dentin sensitivity after periodontal surgery: a randomized clinical trial
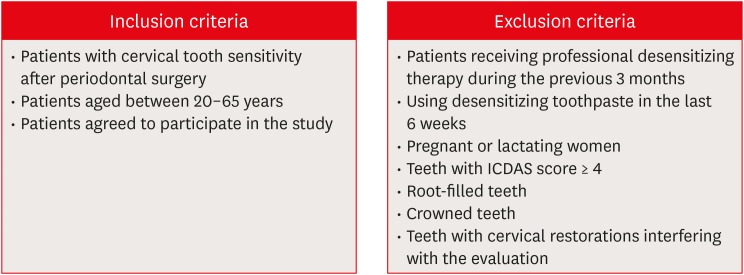
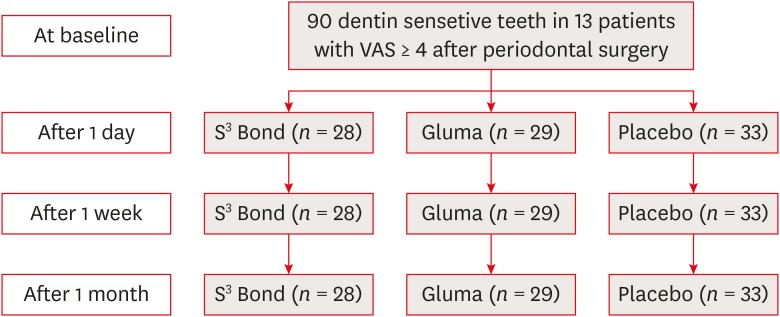
Figure 1 Inclusion and exclusion criteria. ICDAS, International Caries Detection and Assessment System.
Figure 2 Flowchart of allocating the samples in each group.VAS, visual analog scale.
Figure 1
Figure 2
Comparing the effect of a desensitizing material and a self-etch adhesive on dentin sensitivity after periodontal surgery: a randomized clinical trial
Mean visual analog scale (VAS) scores for each treatment group within each assessment time
| Material | Baseline (T0) | One day (T1) | One week (T2) | One month (T3) |
|---|---|---|---|---|
| S3 Bond (G1) | 5.38 ± 1.62Aa | 3.70 ± 1.97Ab | 3.10 ± 1.67Ac | 2.46 ± 1.10ABc |
| Gluma Desensitizer (G2) | 5.15 ± 1.39Aa | 2.92 ± 1.37Ab | 2.42 ± 1.46Ab | 1.57 ± 0.84Ac |
| Placebo (G3) | 5.06 ± 1.19Aa | 4.24 ± 1.63Ab | 3.65 ± 1.74Ab | 2.78 ± 1.40Bc |
The data were presented as mean ± standard deviation.
Same superscript letter indicates no significant differences between groups as per the results of pairwise multiple comparisons (p < 0.05). Lowercase superscripts denote differences in each row (horizontal). Uppercase superscripts denote differences in each column (vertical).
Table 1 Mean visual analog scale (VAS) scores for each treatment group within each assessment time
The data were presented as mean ± standard deviation.
Same superscript letter indicates no significant differences between groups as per the results of pairwise multiple comparisons (

