
Articles
- Page Path
- HOME > Restor Dent Endod > Volume 42(3); 2017 > Article
- Review Article Survival rates against fracture of endodontically treated posterior teeth restored with full-coverage crowns or resin composite restorations: a systematic review
-
Warattama Suksaphar1, Danuchit Banomyong1
 , Titalee Jirathanyanatt1, Yaowaluk Ngoenwiwatkul2
, Titalee Jirathanyanatt1, Yaowaluk Ngoenwiwatkul2 -
2017;42(3):-167.
DOI: https://doi.org/10.5395/rde.2017.42.3.157
Published online: July 31, 2017
1Department of Operative Dentistry and Endodontics, Mahidol University Faculty of Dentistry, Bangkok, Thailand.
2Department of Community Dentistry, Mahidol University Faculty of Dentistry, Bangkok, Thailand.
- Correspondence to Danuchit Banomyong, DDS, PhD. Assistant Professor, Department of Operative Dentistry and Endodontics, Mahidol University Faculty of Dentistry, 6, Yothi Road, Ratchathewi, Bangkok 10400, Thailand. Tel: +66-2-200-7825, Fax: +66-2-200-7824, danuchit.ban@mahidol.ac.th
• Received: April 25, 2017 • Accepted: July 3, 2017
Copyright © 2017. The Korean Academy of Conservative Dentistry
This is an Open Access article distributed under the terms of the Creative Commons Attribution Non-Commercial License (https://creativecommons.org/licenses/by-nc/3.0/) which permits unrestricted non-commercial use, distribution, and reproduction in any medium, provided the original work is properly cited.
- 7,199 Views
- 87 Download
- 29 Crossref
Abstract
- This systematic review aims to summarize the current clinical studies that investigated survival rates against fracture of endodontically treated posterior teeth restored with crowns or resin composite restorations. Literature search were performed using keywords. Publications from 1980 to 2016 were searched in PubMed, ScienceDirect, Web of Science, MEDLINE, and SCOPUS. Included studies were selected based on inclusion and exclusion criteria. Three clinical studies were included: 1 randomized controlled trial and 1 prospective and 1 retrospective cohort studies. Pooled survival rates ranged from 94%–100% and 91.9%–100% for crowns and resin composite, respectively. The majority of teeth had no more than 3 surface loss of tooth structure. The studies included were heterogeneous, and were not appropriate for further meta-analysis. Current evidence suggested that the survival rates against the fracture of endodontically treated posterior teeth restored with crowns or resin composites were not significantly different in the teeth with minimum to moderate loss of tooth structure.
INTRODUCTION
Endodontically treated tooth (ETT) is primarily weakened due to dental caries, trauma, or pre-existing restorations [1,2,3]. Tooth fracture usually occurs when the ETT is not immediately or properly restored, which leads to unrestorable fracture or root canal retreatment due to coronal leakage [4]. Success rate in ETT with immediate permanent restorations is higher than those with long-term provisional restorations, especially in the posterior teeth with excessive loss of tooth structure [5,6].
For posterior ETT, a post-endodontic restoration with cuspal protection is traditionally recommended to reduce the potential of tooth fracture [7,8]. Incidence of tooth fracture after endodontic treatment was lower in posterior teeth with cuspal protection; cuspal-coverage restoration significantly improves clinical success in posterior ETT [9,10,11].
Recently, it has been proposed that posterior ETT with minimum to moderate loss of tooth structure may be successfully restored with adhesive resin composite restoration [12]. Similar clinical success rates between crown and resin composite restorations in premolar ETTs with loss of 1 or 2 marginal ridges were reported [13]. However, the clinical implication of this concept is still controversial.
In the evidence-based medicine, a systematic review collects and critically analyzes all relevant research studies in order to gather a summary of the specific subject. From Cochrane Database of Systematic Review, there is a current systematic review that reported the effects of post-endodontic restorations, crowns, and direct resin composites, on the outcome of ETT [14]. Due to the strict criteria for the study selection, the result was only summarized from one randomized controlled trial that investigated in the premolars with no more than 3 surfaces loss [13]. The study reported similar success rate between the ETT restored with resin composites and crown restorations at 3 years.
Clinical decision making for selection of a final restoration in posterior ETT is mainly based on the limited current clinical evidence [9,11,13]. Systematic reviews generally include only randomized controlled trials in the analysis [14]. However, randomized controlled trial needs time and budget to establish, so the number of study is sometimes rare in a specific topic such as for post-endodontic restoration. In such circumstances, a high-quality retrospective or prospective cohort study could be included to increase the number of selected studies and provide more information in systematic review. Therefore, the purpose of this systematic review was to summarize the current available clinical studies on the survival rates against fracture of posterior ETT using a systematic approach.
MATERIALS AND METHODS
For the systematic review, a research question was firstly set based on the PICO model:
P (population): endodontically treated posterior permanent teeth (with mature root formation).
I (intervention): post-endodontic restoration with non-cuspal coverage, direct resin composite.
C (comparison): post-endodontic restoration with full-coverage crown.
O (outcome): survival rate against fracture.
Therefore, the research question was “Are survival rates against fracture of endodontically treated posterior teeth restored with non-cuspal coverage direct resin composite similar to those restored with full-coverage crown?”.
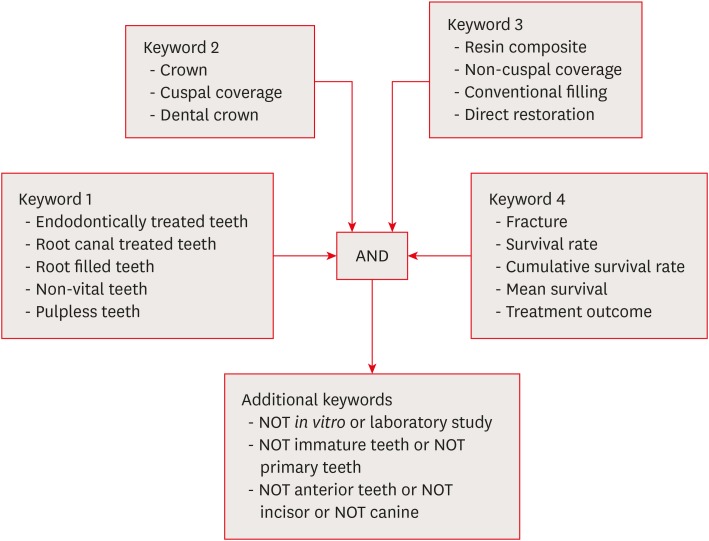
Literature electronic search was performed in PubMed, Web of Science, ScienceDirect, SCOPUS, and MEDLINE from the period of 1980 to 2016. The search was limited to clinical studies in the English language. Based on the question, the 17 keywords and MeSH terms were used as follows: 1) endodontically treated teeth, 2) root canal treated teeth, 3) root filled teeth, 4) non-vital teeth, 5) pulpless teeth, 6) cuspal coverage, 7) crown, 8) dental crown, 9) resin composite, 10) non-cuspal coverage, 11) conventional filling, 12) direct restoration, 13) fracture, 14) survival rate, 15) cumulative survival rate, 16) mean survival, and 17) treatment outcome. Final search was obtained with combination strategies of the 17 key terms: (1 OR 2 OR 3 OR 4 OR 5) AND (6 OR 7 OR 8) AND (9 OR 10 OR 11 OR 12) AND (13 OR 14 OR 15 OR 16 OR 17). The search result was filtered with additional keywords as follows: NOT in vitro or NOT laboratory study, NOT immature teeth or NOT primary teeth, NOT anterior teeth or NOT incisor or NOT canine. All keywords and combination strategies are shown in Figure 1.
Titles and abstracts of the searched studies were screened by a reviewer (W.S.) based on the inclusion criteria:
Clinical study on posterior ETTs with indirect full-coverage crowns or direct non-cuspal coverage resin composite restorations, presenting comparison of survival rates.
The clinical study could be randomized or non-randomized controlled trials, or retrospective or prospective cohort studies.
The studies that did not correspond with inclusion criteria, i.e., case reports, case series, literature reviews, systematic reviews, or meta-analyses were not selected. In addition, manual search was performed on the cited references and citations of the selected studies to find any potentially relevant studies that were not initially found in the electronic search. Full articles of the included studies were screened, and the studies were further excluded if based on exclusion criteria:
No evaluation of survival rate against fracture.
No detail on the types of post-endodontic restoration.
Tooth types were combined between anterior and posterior teeth.
The reasons for study exclusion were recorded. Finally, details of the included studies were collected including publication date, study design, number and type of teeth, type of restorations, type of posts, number of tooth surface loss, evaluation criteria, statistical methods, survival rates from fracture, and follow-up periods.
LOE (Table 1) of the included studies were justified following the criteria of Oxford Centre for Evidence Based Medicine (OCEBM) Levels of Evidence [15].
Table 1
Levels of evidence and definitions based on the Oxford Centre for Evidence Based Medicine (OCEBM) Levels of Evidence [15]
RESULTS
An overview of literature searching and study selection for the systematic review is presented in Figure 2. From the studies published from 1980 to 2016, 404 articles were initially identified through electronic search in the 6 databases. After screening, 38 duplicated articles were removed, and 366 potentially relevant articles remained. The titles and abstracts of these articles were assessed according to the inclusion criteria, and 360 articles were not included. The reasons for removing these studies are presented in Figure 2.
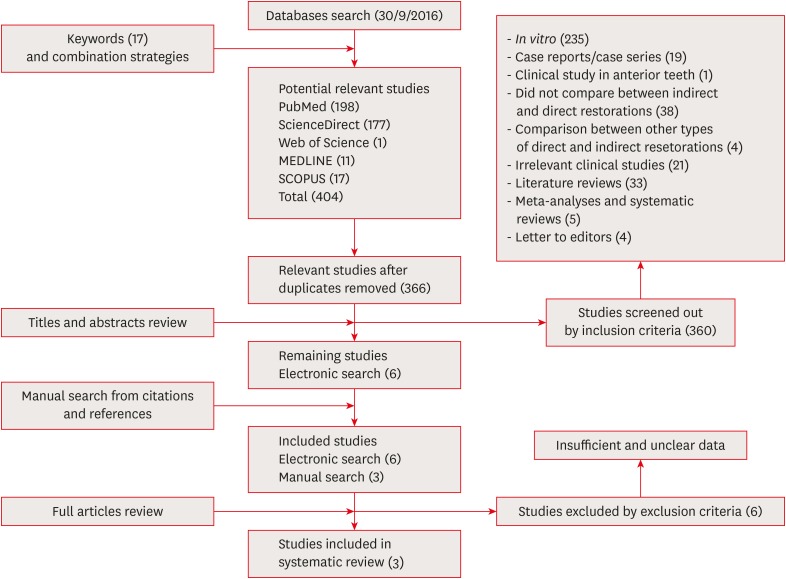
Six articles were included from the electronic search. From the manual search, 3 more relevant articles, according to the inclusion and exclusion criteria, were additionally included. These 9 selected studies [9,11,13,16,17,18,19,20,21] were qualified for full-text review. Six studies [9,11,18,19,20,21] were further excluded following the exclusion criteria because of insufficient data as shown in Table 2. Finally, 3 studies [13,16,17] were included in this systematic review.
Table 2
Six excluded studies after full paper reviewing and reasons for exclusion
| Study | LOE | Study designs | Reasons for exclusion |
|---|---|---|---|
| Pratt et al. [18] | 3 | R | · Could not identify definite number and survival rate of resin composite restorations (combined numbers of amalgam and resin composite in direct restorations). |
| Skupien et al. [19] | 2 | RCT | · Could not identify definite number and survival rate of posterior teeth (combined numbers of anterior and posterior teeth). |
| Fransson et al. [20] | 3 | R | · Could not identify definite number and survival rate of posterior teeth (combined numbers of anterior and posterior teeth). |
| · Could not identify definite number and survival rate of full-crown or resin composite (including full-crown, inlay and onlay in indirect restorations; combining all types of direct restorations). | |||
| · Could not identify reasons for tooth extraction. | |||
| Skupien et al. [21] | 3 | R | · Could not identify definite number and survival rate of posterior teeth (combined numbers of anterior and posterior teeth). |
| Aquilino et al. [9] | 3 | R | · Could not identify definite number and survival rate of posterior teeth (combined numbers of anterior and posterior teeth). |
| · Could not identify definite number of resin composite restorations (combined numbers of amalgam and resin composite in direct restorations). | |||
| Sorensen et al. [11] | 3 | R | · Could not identify definite number and survival rate of posterior teeth restored with full-coverage crown or resin composite restoration (combining numbers of crown and onlay in cuspal-coverage indirect restoration; combining numbers of amalgam and resin composite in non-cuspal coverage direct restorations). |
LOE of 3 included studies are shown in Table 3. These studies were published between 2002 and 2013, and directly compared the survival rates against fracture of posterior ETT between full-coverage crowns and direct resin composite restorations. These studies were 1 randomized controlled trial (Mannocci et al. [13]; LOE level 2), 1 prospective cohort study (Cagidiaco et al. [16]; LOE level 3), and 1 retrospective cohort study (Dammaschke et al. [17]; LOE level 3).
Table 3
Characteristics and survival rates of 3 included studies
| Studies | LOE | Study design | No. of teeth | Type of teeth | Restoration | Type of post | Criterion of survival from fracture | Statistical method | Survival rate against fracture | F/U period (mon) | |
|---|---|---|---|---|---|---|---|---|---|---|---|
| Crown | Composite | ||||||||||
| Dammaschke et al. [17] | 3 | R | 401 | Premolar/molar | Crown/bridge (364) | Without post, prefabricated, or cast metal post | Fracture of tooth and/or restorations | LR | 94% | 91.90% | 60–192 (Mean 116.4) |
| Resin composite (37) | Without post | Mean survival times (mon) | |||||||||
| 152.4–168.0 | 160.8 | ||||||||||
| Cagidiaco et al. [16] | 3 | P | 105 | Premolar/molar | Crown (86) | Prefabricated fiber post | Post fracture, vertical, or horizontal root fracture | χ2 | 100% | 100% | 24 |
| Resin composite (19) | Prefabricated fiber post | ||||||||||
| Mannocci et al. [13] | 2 | RCT | 117 | Premolar | Crown (57) | Prefabricated fiber post | Root fracture, post fracture | 1-way ANOVA | 100% | 100% | 12, 24, 36 |
| Resin composite (60) | Prefabricated fiber post | ||||||||||
Posterior ETTs in the studies of Cagidiaco et al. [16] and Dammaschke et al. [17] were premolars and molars, while the study of Mannocci et al. [13] investigated premolars. From the 3 studies, the number of teeth restored with full-coverage crowns ranged from 57 to 364 teeth, and those restored with resin composite restorations ranged from 19 to 60 teeth. The pooled samples composed of 507 teeth restored with full-coverage crowns and 116 teeth restored with resin composite restorations. Types of post used in the studies of Mannocci et al. [13] and Cagidiaco et al. [16] were prefabricated fiber posts. Prefabricated fiber post, cast metal post or core built-up without post were used in the study of Dammaschke et al. [17]. Criteria of survival against fracture were identified as shown in Table 3.
The posterior ETTs in the 2 studies, Mannocci et al. [13] and Cagidiaco et al. [16], had 1 to 3 surfaces loss, while the posterior ETTs in the study of Dammaschke et al. [17] had 1 to 5 surfaces loss. Most of the teeth restored with resin composite restorations had 1 to 3 surfaces loss of tooth structure. The number of teeth restored with resin composite restorations according to tooth structure loss are shown in Table 4.
Table 4
Number of teeth restored with resin composite restorations according to the number of tooth structure loss (surfaces) from the 3 included studies
| Clinical studies | No. | 1–3 surfaces loss | 4–5 surfaces loss | ||
|---|---|---|---|---|---|
| No. | % | No. | % | ||
| Dammaschke et al. [17] | 37 | 31 | 83.8 | 6 | 16.2 |
| Cagidiaco et al. [16] | 19 | 19 | 100.0 | 0 | 0 |
| Mannocci et al. [13] | 60 | 60 | 100.0 | 0 | 0 |
| Total | 116 | 110 | 94.8 | 6 | 5.2 |
Overall survival rates against fracture of full-coverage crowns ranged from 94% to 100%, while those of resin composite restorations ranged from 91.9% to 100%. For the short-term follow-up, 2 studies (Mannocci et al. [13] and Cagidiaco et al. [16]) reported 100% survival at 12–36 months of both full-coverage crowns and resin composite restorations. For the long-term follow-up, the study of Dammaschke et al. [17] reported survival rate of 94% for full-coverage crowns and 91.9% for resin composite restorations.
Included clinical studies reported high survival rates against fracture in the posterior ETTs restored with full-coverage crowns and resin composite restorations that were not significantly different. In this systematic review, the heterogeneity of the study designs and methodology were observed among the included studies and, therefore, meta-analysis was not performed.
DISCUSSION
For the posterior ETT, a cuspal-coverage restoration is traditionally recommended after endodontic treatment to prevent tooth fracture and improve long-term success [9,10,11,12]. This recommendation has been questioned by the result from a randomized controlled clinical trial [13]. From the trial, the posterior ETTs (premolars) with minimal to moderate loss of tooth structure (2–3 surfaces loss) could be successfully restored with direct resin composite as a final restoration [13]. At 3 year recall, the premolars restored with resin composite had a high success rate above 90% that was similar to those with full-coverage crowns. This study was included in the previous systematic review by the Cochrane Database of Systematic Review [14]. In our systematic review, the study of Mannocci et al. [13] was identified as the highest LOE among the 3 included studies. The indifference in survival against fracture between direct resin composite and crown restoration was supported by the results of the 2 included cohort studies [16,17].
The 2 cohort studies (Cagidiaco et al. [16] and Dammaschke et al. [17]) were also included in the present systematic review, while the previous systematic review [14] included only a randomized controlled trial. In general, a higher variation in the studied population is expected due to the nature of cohort study. However, the authors decided to include these cohort studies in the systematic review due to the lack of randomized controlled trial; otherwise, only one study would have been included for the analysis. In our systematic review, the number of studied teeth was increased, and the recall period was longer to confirm the short-term result of the randomized controlled trial [13].
The high survival rate of resin composite restorations was also observed in the 2 cohort studies [16,17]. In the randomized controlled trial of Mannocci et al. [13], all premolars with resin composite restorations were restored in combination with fiber-post placement. The question is raised whether the fiber post is necessary to achieve the favorable clinical outcome. In the cohort study of Dammaschke et al. [17], high survival rate from fracture was confirmed in the ETTs with resin composite and without post placement [17]. This might indicate that the ETTs with 1- to 2-surface resin composite restorations, with or without fiber post, should have high survival rate comparable to the crown restorations.
However, in this systematic review, the indifference between the survival rates of the 2 restorations may have been affected by the tooth selection and the assignment of restorations in the studies. From the 2 cohort studies [16,17], the assignment of the 2 restorations were not controlled, and this might lead to a bias. In those studies, the ETTs restored with resin composite restorations tended to have mild to moderate tooth structure loss (1–3 surfaces), while the ETTs with severe tooth structure loss tended to receive full-coverage crowns. In fact, the more tooth structure remains, the higher chance of survival from fracture is expected [17,22]. Thus, the resin composite group tended to receive a positive effect from these confounding factors. In the randomized control trial [13], the teeth selection was controlled between 2 restorations and included if tooth structure loss was no more than 3 surfaces. However, the results were limited in the premolars that the occlusal force is different from the molars.
Moreover, the numbers of the indirect restorations in the cohort studies were higher than those of the direct restorations, especially at long-term recall periods [16,17]. On the other hand, the number of samples between the direct and indirect restorations were similar in the randomized controlled trial [13] due to the nature of the study. From the 2 cohort studies, direct resin composite restorations were likely to be placed in the ETT with a limited tooth structure loss at short term. Therefore, survival rate of the resin composite group tended to be affected and improved by these positive factors. These might lead to a limitation for generalization, and any clinical implication must be carefully interpreted.
The remaining tooth structure affects the survival rate against fracture of posterior ETT [1,17,22,23]. The posterior ETTs with 1 to 3 surfaces loss had a significantly higher survival rate than those with more than 3 surfaces loss [17,22,24]. The higher the number of surface loss is, the higher the risk of tooth fracture after post-endodontic restorations is anticipated. For the ETT that has higher amount of residual walls with low or normal occlusal force, higher survival rate against fracture would be expected, regardless of the type of post-endodontic restorations.
Tooth type is also an important factor for the survival rate against the fracture of ETT [7,9]. Several studies reported that the premolar ETT had significantly higher survival rate than the molar ETT [7,9,25]. Occlusal load of posterior tooth is associated with the distance to temporo-mandibular joint. The closer the distance to the fulcrum (temporo-mandibular joint), the higher the mechanical biting force on the tooth is expected [26,27]. It is possible that vertical occlusal forces to the premolars are lower than the molars. However, lateral occlusal forces on premolars are to be higher, and this may have more potential effect on tooth fracture, and should be a concern. Moreover, the smaller size of the occlusal area in premolars withstands less occlusal stress than molars [28]. Therefore, a consideration of survival rate against the fracture in the posterior ETT should be separated between premolars and molars. However, most of the clinical studies presented the survival rate with a combination of premolars and molars [16,17]. Only the study by Mannocci et al. [13] specifically reported the survival rate of premolars, but the study did not collect the survival rate of molars.
The placement of a fiber post may affect the survival against the fracture in ETT. In general, posterior ETT does not need a post if the tooth has enough remaining tooth structure to retain a core built-up restoration [12]. From the 2 included studies by Cagidiaco et al. [16] and Mannocci et al. [13], all the teeth were restored with a placement of fiber post, and 100% survival rate against fracture was observed in both types of restorations. In the study by Dammaschke et al. [17], the teeth restored with resin composite restorations without post placement had slightly higher fracture rate than those in the 2 studies. From these results, we may consider the advantage of post placement to provide retention and support of the coronal restoration in posterior ETT. These are supported by the result of a laboratory study that reported the post placement increased fracture resistance and improved stress distribution in the ETT with 2–4 remaining walls [29].
Resin composite restoration is able to reinforce remaining tooth structure of ETT through the concept of adhesion between the restorative materials and tooth substrate [30,31]. In a laboratory study, the fracture resistance of ETT restored with resin composite restoration was similar to that of sound natural tooth [32]. Several retrospective studies reported higher survival against the fracture in the ETT restored with resin composite restorations than those restored with un-bonded amalgam restorations [22,33,34]. However, long-term degradation of bond between the adhesive material and tooth substrate is a concern [35]. This leads to a reduction in bond strength to dentin at long term and, subsequently, fracture strength of the restored tooth [36].
To confirm the result, a randomized controlled trial with long-term follow-up period should be performed. Survival rate in the posterior ETT should be separately investigated between premolars and molars with a consideration of remaining tooth structure or tooth surface loss. In addition, the benefit of post placement in posterior ETT restored with resin composite restoration should be also verified.
Conclusions
Based on this systematic review, survival rates against fracture of posterior ETT restored with either full-coverage crowns or direct resin composite restorations were not significantly different in the teeth with minimal to moderate loss of tooth structure.
Acknowledgement
The authors would like to thank Mr. Arthur Navarro (Forum for Ethical Review Committees in Asia and the Western Pacific [FERCAP] Research Fellow World Health Organization's Special Program on Tropical Disease Research [WHO-TDR] Clinical Coordination and Training Center) for his editorial assistance.
-
Conflict of Interest: No potential conflict of interest relevant to this article was reported.
-
Author Contributions:
Conceptualization: Banomyong D, Jirathanyanatt T.
Data curation: Suksaphar W, Ngoenwiwatkul Y.
Formal analysis: Suksaphar W, Ngoenwiwatkul Y.
Funding acquisition: Banomyong D, Jirathanyanatt T.
Investigation: Suksaphar W, Banomyong D.
Methodology: Suksaphar W, Banomyong D, Jirathanyanatt T, Ngoenwiwatkul Y.
Project administration: Suksaphar W.
Resources: Banomyong D, Jirathanyanatt T.
Software: Suksaphar W, Ngoenwiwatkul Y.
Supervision: Banomyong D, Jirathanyanatt T, Ngoenwiwatkul Y.
Validation: Banomyong D, Ngoenwiwatkul Y.
Visualization: Banomyong D, Ngoenwiwatkul Y.
Writing - original draft: Suksaphar W, Banomyong D.
Writing - review & editing: Suksaphar W, Banomyong D.
- 1. Panitvisai P, Messer HH. Cuspal deflection in molars in relation to endodontic and restorative procedures. J Endod 1995;21:57-61.ArticlePubMed
- 2. Reeh ES, Douglas WH, Messer HH. Stiffness of endodontically-treated teeth related to restoration technique. J Dent Res 1989;68:1540-1544.ArticlePubMedPDF
- 3. Sedgley CM, Messer HH. Are endodontically treated teeth more brittle? J Endod 1992;18:332-335.ArticlePubMed
- 4. Saunders WP, Saunders EM. Coronal leakage as a cause of failure in root-canal therapy: a review. Endod Dent Traumatol 1994;10:105-108.ArticlePubMed
- 5. Safavi KE, Dowden WE, Langeland K. Influence of delayed coronal permanent restoration on endodontic prognosis. Endod Dent Traumatol 1987;3:187-191.ArticlePubMed
- 6. Uranga A, Blum JY, Esber S, Parahy E, Prado C. A comparative study of four coronal obturation materials in endodontic treatment. J Endod 1999;25:178-180.ArticlePubMed
- 7. Chan CP, Lin CP, Tseng SC, Jeng JH. Vertical root fracture in endodontically versus nonendodontically treated teeth: a survey of 315 cases in Chinese patients. Oral Surg Oral Med Oral Pathol Oral Radiol Endod 1999;87:504-507.ArticlePubMed
- 8. Kumagai H, Suzuki T, Hamada T, Sondang P, Fujitani M, Nikawa H. Occlusal force distribution on the dental arch during various levels of clenching. J Oral Rehabil 1999;26:932-935.ArticlePubMed
- 9. Aquilino SA, Caplan DJ. Relationship between crown placement and the survival of endodontically treated teeth. J Prosthet Dent 2002;87:256-263.ArticlePubMed
- 10. Ng YL, Mann V, Gulabivala K. A prospective study of the factors affecting outcomes of non-surgical root canal treatment: part 2: tooth survival. Int Endod J 2011;44:610-625.ArticlePubMed
- 11. Sorensen JA, Martinoff JT. Intracoronal reinforcement and coronal coverage: a study of endodontically treated teeth. J Prosthet Dent 1984;51:780-784.ArticlePubMed
- 12. Schwartz RS, Jordan R. Restoration of endodontically treated teeth: the endodontist's perspective, part 1. updated 2017 Jun 7]. Available from: http://www.aae.org/publications-and-research/endodontics-colleagues-for-excellence-newsletter/restoration-of-endodontically-treated-teeth,-the-endodontist-s-perspective-part-1.aspx.
- 13. Mannocci F, Bertelli E, Sherriff M, Watson TF, Ford TR. Three-year clinical comparison of survival of endodontically treated teeth restored with either full cast coverage or with direct composite restoration. J Prosthet Dent 2002;88:297-301.ArticlePubMed
- 14. Sequeira-Byron P, Fedorowicz Z, Carter B, Nasser M, Alrowaili EF. Single crowns versus conventional fillings for the restoration of root-filled teeth. Cochrane Database Syst Rev 2015;CD009109.ArticlePubMedPMC
- 15. Centre for Evidence-Based Medicine (GB). Oxford Centre for Evidence-Based Medicine: levels of evidence (March 2009). updated 2009]. Available from: http://www.cebm.net/oxford-centre-evidence-based-medicine-levels-evidence-march-2009.
- 16. Cagidiaco MC, Radovic I, Simonetti M, Tay F, Ferrari M. Clinical performance of fiber post restorations in endodontically treated teeth: 2-year results. Int J Prosthodont 2007;20:293-298.PubMed
- 17. Dammaschke T, Nykiel K, Sagheri D, SchaferSchäfer E. Influence of coronal restorations on the fracture resistance of root canal-treated premolar and molar teeth: a retrospective study. Aust Endod J 2013;39:48-56.ArticlePubMed
- 18. Pratt I, Aminoshariae A, Montagnese TA, Williams KA, Khalighinejad N, Mickel A. Eight-year retrospective study of the critical time lapse between root canal completion and crown placement: its influence on the survival of endodontically treated teeth. J Endod 2016;42:1598-1603.ArticlePubMed
- 19. Skupien JA, Cenci MS, Opdam NJ, Kreulen CM, Huysmans MC, Pereira-Cenci T. Crown vs. composite for post-retained restorations: Aa randomized clinical trial. J Dent 2016;48:34-39.PubMed
- 20. Fransson H, Dawson VS, Frisk F, Bjørndal L, Kvist T, Bjørndal L, Dawson VS, Fransson H, Frisk F, Jonasson P, Kvist T, Markvart M, Petersson K, Pigg M, Reit C, Wolf E. EndoReCo. Survival of root-filled teeth in the Swedish adult population. J Endod 2016;42:216-220.ArticlePubMed
- 21. Skupien JA, Opdam N, Winnen R, Bronkhorst E, Kreulen C, Pereira-Cenci T, Huysmans MC. A Practicepractice-based Studystudy on the Survivalsurvival of Restored Endodontically Treated Teeth.restored endodontically treated teeth. J Endod 2013;39:1335-1340.PubMed
- 22. Nagasiri R, Chitmongkolsuk S. Long-term survival of endodontically treated molars without crown coverage: a retrospective cohort study. J Prosthet Dent 2005;93:164-170.ArticlePubMed
- 23. Ferrari M, Vichi A, Fadda GM, Cagidiaco MC, Tay FR, Breschi L, Polimeni A, Goracci C. A randomized controlled trial of endodontically treated and restored premolars. J Dent Res 2012;91:72S-78S.ArticlePubMedPDF
- 24. Salameh Z, Sorrentino R, Papacchini F, Ounsi HF, Tashkandi E, Goracci C, Ferrari M. Fracture resistance and failure patterns of endodontically treated mandibular molars restored using resin composite with or without translucent glass fiber posts. J Endod 2006;32:752-755.ArticlePubMed
- 25. Tan L, Chen NN, Poon CY, Wong HB. Survival of root filled cracked teeth in a tertiary institution. Int Endod J 2006;39:886-889.ArticlePubMed
- 26. Hiatt WH. Incomplete crown-root fracture in pulpal-periodontal disease. J Periodontol 1973;44:369-379.ArticlePubMed
- 27. Lynch CD, McConnell RJ. The cracked tooth syndrome. J Can Dent Assoc 2002;68:470-475.PubMed
- 28. Cavel WT, Kelsey WP, Blankenau RJ. An in vivo study of cuspal fracture. J Prosthet Dent 1985;53:38-42.ArticlePubMed
- 29. Nam SH, Chang HS, Min KS, Lee Y, Cho HW, Bae JM. Effect of the number of residual walls on fracture resistances, failure patterns, and photoelasticity of simulated premolars restored with or without fiber-reinforced composite posts. J Endod 2010;36:297-301.ArticlePubMed
- 30. Dietschi D, Bouillaguet S, Sadan A. Restoration of the endodontically treated tooth. In: Hargreaves KM, Cohen S, editors. Cohen's pathways of the pulp. 10th ed. St. Louis (MO): Mosby Elsevier; 2011. p. 777-807.
- 31. Mincik J, Urban D, Timkova S, Urban R. Fracture resistance of endodontically treated maxillary premolars restored by various direct filling materials: an in vitro study. Int J Biomater 2016;2016:9138945.ArticlePubMedPMCPDF
- 32. Ausiello P, De Gee AJ, Rengo S, Davidson CL. Fracture resistance of endodontically-treated premolars adhesively restored. Am J Dent 1997;10:237-241.PubMed
- 33. Hansen EK. In vivo cusp fracture of endodontically treated premolars restored with MOD amalgam or MOD resin fillings. Dent Mater 1988;4:169-173.ArticlePubMed
- 34. Mannocci F, Qualtrough AJ, Worthington HV, Watson TF, Pitt Ford TR. Randomized clinical comparison of endodontically treated teeth restored with amalgam or with fiber posts and resin composite: five-year results. Oper Dent 2005;30:9-15.PubMed
- 35. Hashimoto M, Fujita S, Endo K, Ohno H. In vitro degradation of resin-dentin bonds with one-bottle self-etching adhesives. Eur J Oral Sci 2009;117:611-617.ArticlePubMed
- 36. Opdam NJ, van de Sande FH, Bronkhorst E, Cenci MS, Bottenberg P, Pallesen U, Gaengler P, Lindberg A, Huysmans MC, van Dijken JW. Longevity of posterior composite restorations: a systematic review and meta-analysis. J Dent Res 2014;93:943-949.ArticlePubMedPMCPDF
REFERENCES
Tables & Figures
REFERENCES
Citations
Citations to this article as recorded by 
- Clinical Outcomes and Complication Rates of Crown Restorations with Various Endodontic Posts: A Retrospective Analysis
Ali Alenezi, Hanin Alsalhi
Journal of Functional Biomaterials.2026; 17(2): 84. CrossRef - Restoration of the fractured or heavily restored premolar
Chris Redman, Ewen McColl, Graeme Bryce
Dental Update.2026; 53(5): 323. CrossRef - Comparison of fracture resistance among restorative techniques for endodontically treated mandibular premolars: an in vitro study
Dinie Qurratuaini Zulkifly, Mohd Haikal Muhamad Halil, Ubadah Zamry, Siti Nabilah Huda Mohamad Nor
The Saudi Dental Journal.2026;[Epub] CrossRef - Effect of using different materials and restorative techniques on cuspal deflection and microleakage in endodontically treated teeth
Ceyda Sari, Oya Bala, Sinem Akgul, Cemile Kedici Alp
BMC Oral Health.2025;[Epub] CrossRef - Direct restorations versus full crowns in endodontically treated molar teeth: A three-year randomized clinical trial
Motasum Abu-Awwad, Ruba Halasa, Laila Haikal, Ahmad El-Ma'aita, Mohammad Hammad, Haralampos Petridis
Journal of Dentistry.2025; 156: 105699. CrossRef - Is the use of an intraradicular post essential for reducing failures in restoring endodontically treated teeth? A systematic review and meta-analysis
Jacqueline Salomão Jardim, Vinicius de Menezes Félix Ferreira, Hiskell Francine Fernandes e Oliveira, Daniele Sorgatto Faé, Cleidiel Aparecido Araujo Lemos
Journal of Dentistry.2025; 159: 105739. CrossRef - Systematic Reviews Comparing Direct and Indirect Restorations: An Umbrella Review That Examines Restoration Type and Confidence in Results
Mona Kimmel, Clovis Mariano Faggion
Clinical and Experimental Dental Research.2025;[Epub] CrossRef - Knowledge, Awareness, and Perceptions on Root Canal Treatment among Patients Reporting with Dental Pain to Conservative Dentistry and Endodontics Department: An Institution-based Survey
Abdu Semeer Palottil, Moopil Midhun Mohanan, N. T. Nishad, S. Jayasree
Journal of Primary Care Dentistry and Oral Health.2025; 6(2): 99. CrossRef - One-year clinical performance of restorations with and without a bulk-fill flowable base in endodontically treated premolars: a pilot randomized controlled trial
Brenda Leyton, Jullyana Dezanetti, Rodrigo Rached, Sérgio Ignácio, Evelise Souza
BMC Oral Health.2025;[Epub] CrossRef - One-piece endodontic crown fixed partial denture: Is it possible?
João Paulo M. Tribst, Amanda Maria de O. Dal Piva, Joris Muris, Cornelis J. Kleverlaan, Albert J. Feilzer
The Journal of Prosthetic Dentistry.2024; 131(6): 1118. CrossRef - Survival Rate Against Fracture of Endodontically Treated Premolars Restored with Crowns and Resin Composites: A Retrospective Study
Enas Khamakhim, Farida Alsayeh
AlQalam Journal of Medical and Applied Sciences.2024; : 398. CrossRef - Knowledge and Awareness of Root Canal Treatment among Patients in Tripoli: A Survey-Based Study
Sumaya Aghila
AlQalam Journal of Medical and Applied Sciences.2024; : 532. CrossRef - Clinical performance of polyethylenefiber reinforced resin composite restorations in endodontically treated teeth: (a randomized controlled clinical trial)
Ahmed Abdelsattar Metwaly, Amira Farid Elzoghby, Rawda Hesham Abd ElAziz
BMC Oral Health.2024;[Epub] CrossRef - Direct Versus Indirect Treatment Options of Endodontically Treated Posterior Teeth: A Narrative Review
Mai M Alhamdan, Rodina F Aljamaan, Munira M Abuthnain, Shahd A Alsumikhi, Ghada S Alqahtani, Reem A Alkharaiyef
Cureus.2024;[Epub] CrossRef - Single crown vs. composite for glass fiber post-retained restorations: An 8-year randomized clinical trial
Victório Poletto-Neto, Luiz Alexandre Chisini, Wietske Fokkinga, Cees Kreulen, Bas Loomans, Maximiliano Sérgio Cenci, Tatiana Pereira-Cenci
Journal of Dentistry.2024; 142: 104837. CrossRef - Factors influencing the clinical performance of the restoration of endodontically treated teeth: An assessment of systematic reviews of clinical studies
Lara Dotto, Luiza Paloma S. Girotto, Yara Teresinha Correa Silva Sousa, Gabriel Kalil Rocha Pereira, Ataís Bacchi, Rafael Sarkis-Onofre
The Journal of Prosthetic Dentistry.2024; 131(6): 1043. CrossRef - Influence of technical quality and coronal restoration on periapical health of root canal treatment performed by Malaysian undergraduate students
Norazlina Mohammad, Faizah Abdul Fatah, Azlan Jaafar, Siti Hajar Omar, Aimi Amalina Ahmad, Abdul Azim Asy Abdul Aziz, Aws Hashim Ali Al-Kadhim
Saudi Endodontic Journal.2023; 13(1): 63. CrossRef - The success rate of indirect adhesive restorations in the distal dentition fabricated with chairside CAD/CAM system
Marek Šupler, Andrej Jenča, Michal Straka, Juraj Deglovič, Janka Jenčová
Stomatológ.2023; 33(2): 10. CrossRef - A Comparative Study of the Marginal Fit of Endocrowns Fabricated From Three Different Computer-Aided Design/Computer-Aided Manufacturing (CAD/CAM) Ceramic Materials: An In Vitro Study
Esraa Attar, Shatha Alshali, Tariq Abuhaimed
Cureus.2023;[Epub] CrossRef - Evaluation of titanium mesh and fibers in reinforcing endodontically treated molars: An in vitro study
Hemalatha Hiremath, Devansh Verma, Sheetal Khandelwal, AishwaryaSingh Solanki, Sonam Patidar
Journal of Conservative Dentistry.2022; 25(2): 189. CrossRef - Effect of surface treatment, ferrule height, and luting agent type on pull-out bond strength of monolithic zirconia endocrowns
Emine B. Buyukerkmen, Durmuş A. Bozkurt, Arslan Terlemez
Journal of Oral Science.2022; 64(4): 279. CrossRef - An Umbrella Review of Systematic Reviews and Meta‐Analyses Evaluating the Success Rate of Prosthetic Restorations on Endodontically Treated Teeth
Amirhossein Fathi, Behnaz Ebadian, Sara Nasrollahi Dezaki, Nahal Mardasi, Ramin Mosharraf, Sabire Isler, Shiva Sadat Tabatabaei, Stefano Pagano
International Journal of Dentistry.2022;[Epub] CrossRef - Survival and success of endocrowns: A systematic review and meta-analysis
Raghad A. Al-Dabbagh
The Journal of Prosthetic Dentistry.2021; 125(3): 415.e1. CrossRef - Fracture strength of non-invasively reinforced MOD cavities on endodontically treated teeth
René Daher, Stefano Ardu, Enrico Di Bella, Giovanni T. Rocca, Albert J. Feilzer, Ivo Krejci
Odontology.2021; 109(2): 368. CrossRef - Retrospective study of fracture survival in endodontically treated molars: the effect of single-unit crowns versus direct-resin composite restorations
Kanet Chotvorrarak, Warattama Suksaphar, Danuchit Banomyong
Restorative Dentistry & Endodontics.2021;[Epub] CrossRef - An insight into patient's perceptions regarding root canal treatment: A questionnaire-based survey
Ramta Bansal, Aditya Jain
Journal of Family Medicine and Primary Care.2020; 9(2): 1020. CrossRef - Endodontically treated posterior teeth restored with or without crown restorations: A 5‐year retrospective study of survival rates from fracture
Titalee Jirathanyanatt, Warattama Suksaphar, Danuchit Banomyong, Yaowaluk Ngoenwiwatkul
Journal of Investigative and Clinical Dentistry.2019;[Epub] CrossRef - Fracture resistance, gap and void formation in root‐filled mandibular molars restored with bulk‐fill resin composites and glass‐ionomer cement base
Nathamon Thongbai‐on, Kanet Chotvorrarak, Danuchit Banomyong, Michael F. Burrow, Sittichoke Osiri, Nattha Pattaravisitsate
Journal of Investigative and Clinical Dentistry.2019;[Epub] CrossRef - Current options concerning the endodontically-treated teeth restoration with the adhesive approach
Marco Aurélio de Carvalho, Priscilla Cardoso Lazari, Marco Gresnigt, Altair Antoninha Del Bel Cury, Pascal Magne
Brazilian Oral Research.2018;[Epub] CrossRef
 ePub Link
ePub Link Cite
Cite- Figure
-
- Related articles
-
- Fracture resistance and failure modes of endodontically-treated permanent teeth restored with Ribbond posts vs other post systems: a systematic review and meta-analysis of in vitro studies
- The prevalence of apical periodontitis in patients prior to hematopoietic cell transplantation: a systematic review
Survival rates against fracture of endodontically treated posterior teeth restored with full-coverage crowns or resin composite restorations: a systematic review
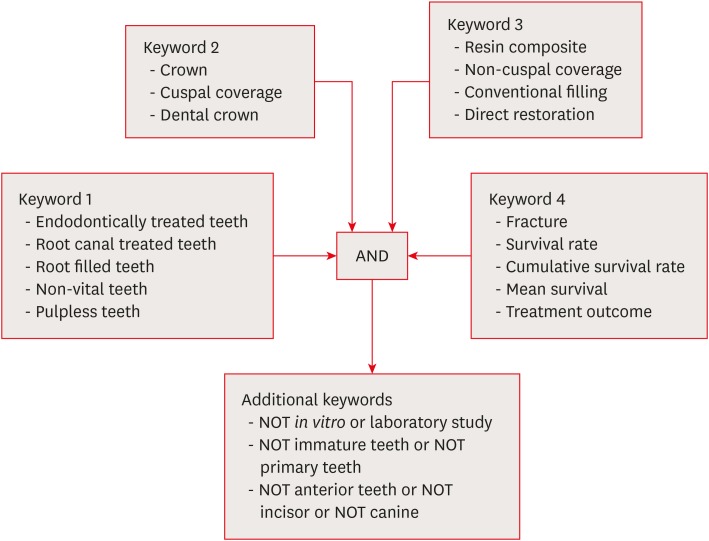
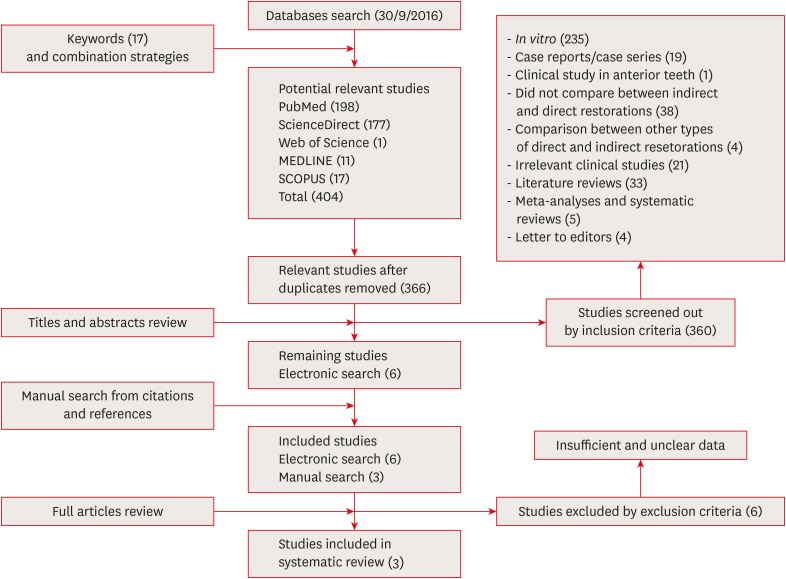
Figure 1 The combination strategies for literature search.
Figure 2 Overview of literature search and study selection for systematic review.
Figure 1
Figure 2
Survival rates against fracture of endodontically treated posterior teeth restored with full-coverage crowns or resin composite restorations: a systematic review
Levels of evidence and definitions based on the Oxford Centre for Evidence Based Medicine (OCEBM) Levels of Evidence [15]
| Levels | Definitions |
|---|---|
| 1 | Systematic review of randomized trials or n-of-1 trials |
| 2 | Randomized trial or observational study with dramatic effect |
| 3 | Non-randomized controlled cohort/follow-up study |
| 4 | Case-series, case-control studies, or historically controlled studies |
| 5 | Mechanism-based reasoning |
Six excluded studies after full paper reviewing and reasons for exclusion
| Study | LOE | Study designs | Reasons for exclusion |
|---|---|---|---|
| Pratt et al. [ | 3 | R | · Could not identify definite number and survival rate of resin composite restorations (combined numbers of amalgam and resin composite in direct restorations). |
| Skupien et al. [ | 2 | RCT | · Could not identify definite number and survival rate of posterior teeth (combined numbers of anterior and posterior teeth). |
| Fransson et al. [ | 3 | R | · Could not identify definite number and survival rate of posterior teeth (combined numbers of anterior and posterior teeth). |
| · Could not identify definite number and survival rate of full-crown or resin composite (including full-crown, inlay and onlay in indirect restorations; combining all types of direct restorations). | |||
| · Could not identify reasons for tooth extraction. | |||
| Skupien et al. [ | 3 | R | · Could not identify definite number and survival rate of posterior teeth (combined numbers of anterior and posterior teeth). |
| Aquilino et al. [ | 3 | R | · Could not identify definite number and survival rate of posterior teeth (combined numbers of anterior and posterior teeth). |
| · Could not identify definite number of resin composite restorations (combined numbers of amalgam and resin composite in direct restorations). | |||
| Sorensen et al. [ | 3 | R | · Could not identify definite number and survival rate of posterior teeth restored with full-coverage crown or resin composite restoration (combining numbers of crown and onlay in cuspal-coverage indirect restoration; combining numbers of amalgam and resin composite in non-cuspal coverage direct restorations). |
LOE, level of evidence; R, retrospective cohort study; RCT, randomized control trial study.
Characteristics and survival rates of 3 included studies
| Studies | LOE | Study design | No. of teeth | Type of teeth | Restoration | Type of post | Criterion of survival from fracture | Statistical method | Survival rate against fracture | F/U period (mon) | |
|---|---|---|---|---|---|---|---|---|---|---|---|
| Crown | Composite | ||||||||||
| Dammaschke et al. [ | 3 | R | 401 | Premolar/molar | Crown/bridge (364) | Without post, prefabricated, or cast metal post | Fracture of tooth and/or restorations | LR | 94% | 91.90% | 60–192 (Mean 116.4) |
| Resin composite (37) | Without post | Mean survival times (mon) | |||||||||
| 152.4–168.0 | 160.8 | ||||||||||
| Cagidiaco et al. [ | 3 | P | 105 | Premolar/molar | Crown (86) | Prefabricated fiber post | Post fracture, vertical, or horizontal root fracture | χ2 | 100% | 100% | 24 |
| Resin composite (19) | Prefabricated fiber post | ||||||||||
| Mannocci et al. [ | 2 | RCT | 117 | Premolar | Crown (57) | Prefabricated fiber post | Root fracture, post fracture | 1-way ANOVA | 100% | 100% | 12, 24, 36 |
| Resin composite (60) | Prefabricated fiber post | ||||||||||
LOE, level of evidence; F/U, follow-up; R, retrospective cohort study; LR, log-rank test; P, prospective cohort study; RCT, randomized control trial study; ANOVA, analysis of variance.
Number of teeth restored with resin composite restorations according to the number of tooth structure loss (surfaces) from the 3 included studies
| Clinical studies | No. | 1–3 surfaces loss | 4–5 surfaces loss | ||
|---|---|---|---|---|---|
| No. | % | No. | % | ||
| Dammaschke et al. [ | 37 | 31 | 83.8 | 6 | 16.2 |
| Cagidiaco et al. [ | 19 | 19 | 100.0 | 0 | 0 |
| Mannocci et al. [ | 60 | 60 | 100.0 | 0 | 0 |
| Total | 116 | 110 | 94.8 | 6 | 5.2 |
Table 1 Levels of evidence and definitions based on the Oxford Centre for Evidence Based Medicine (OCEBM) Levels of Evidence [15]
Table 2 Six excluded studies after full paper reviewing and reasons for exclusion
LOE, level of evidence; R, retrospective cohort study; RCT, randomized control trial study.
Table 3 Characteristics and survival rates of 3 included studies
LOE, level of evidence; F/U, follow-up; R, retrospective cohort study; LR, log-rank test; P, prospective cohort study; RCT, randomized control trial study; ANOVA, analysis of variance.
Table 4 Number of teeth restored with resin composite restorations according to the number of tooth structure loss (surfaces) from the 3 included studies

