
Articles
- Page Path
- HOME > Restor Dent Endod > Volume 47(3); 2022 > Article
- Research Article Effect of intracanal cryotherapy on postoperative pain after endodontic treatment: systematic review with meta-analysis
-
Fernanda Garcias Hespanhol1
 , Ludmila Silva Guimarães1, Lívia Azeredo Alves Antunes1,2, Leonardo Santos Antunes1,2
, Ludmila Silva Guimarães1, Lívia Azeredo Alves Antunes1,2, Leonardo Santos Antunes1,2 -
Restor Dent Endod 2022;47(3):e30.
DOI: https://doi.org/10.5395/rde.2022.47.e30
Published online: July 4, 2022
1Postgraduate Program, School of Dentistry, Fluminense Federal University, Niterói, RJ, Brazil.
2Specific Formation Department, School of Dentistry of Nova Friburgo, Fluminense Federal University, Niterói, RJ, Brazil.
- Correspondence to Leonardo Santos Antunes, DDS, MSc, PhD. Professor, Department of Specific Formation, School of Dentistry, Fluminense Federal University, Rua Doutor Silvio Henrique Braune, 22 Centro, Nova Friburgo, Rio de Janeiro 28625-650, Brazil. leonardoantunes@id.uff.br
• Received: December 16, 2021 • Revised: January 31, 2022 • Accepted: February 15, 2022
Copyright © 2022. The Korean Academy of Conservative Dentistry
This is an Open Access article distributed under the terms of the Creative Commons Attribution Non-Commercial License (https://creativecommons.org/licenses/by-nc/4.0/) which permits unrestricted non-commercial use, distribution, and reproduction in any medium, provided the original work is properly cited.
Abstract
-
Objectives This study aimed to evaluate the effectiveness of final irrigation with cold saline solution after endodontic treatment compared with saline solution at room temperature against postoperative pain following endodontic treatment.
-
Materials and Methods A broad search was performed in the PubMed, Web of Science, Scopus, Cochrane Library, Virtual Health Library (LILACS), and Grey Literature databases. Two independent reviewers performed data extraction, risk of bias using the Cochrane methodology, and certainty of evidence using the Grading of Recommendations, Assessment, Development and Evaluations (GRADE) approach.
-
Results Eight studies were included in qualitative synthesis. Intracanal cryotherapy favored the reduction of postoperative pain in the systematic review. Four studies were included in meta-analyses. The meta-analysis showed that intracanal cryotherapy reduced postoperative pain in teeth with symptomatic apical periodontitis (SAP) at 24 hours. There was no association between intracanal cryotherapy and control (room temperature) groups in teeth with normal periapical tissue with respect to postoperative pain at 24 hours and 48 hours.
-
Conclusions Intracanal cryotherapy was effective in reducing postoperative pain after endodontic treatment in teeth with SAP.
INTRODUCTION
One of the most important aspects of endodontic practice is the management of the postoperative pain and discomfort frequently reported by patients after endodontic treatment [1]; it has a high rate of occurrence and presents in 3 to 58% of all cases [2]. Vital and necrotic remains of root canals, microorganisms and their toxins, and irrigators that extrude beyond the apical foramen during endodontic treatment may trigger inflammation and postoperative symptoms such as mild to severe pain or so-called flare-ups [3,4,5]. Pharmacological and non-pharmacological methods are used to reverse the inflammatory process and control pain. The use of drugs such as analgesics, non-steroidal anti-inflammatory agents, and corticosteroids, despite being relatively safe medications, they may cause gastrointestinal [6,7,8,9], as well as renal, hepatic, and respiratory problems [10,11]. In order to avoid these side effects, alternative treatments have been proposed, such as laser treatments and cryotherapy [12,13,14].
Cryotherapy, also known as cold therapy, has been physiological and clinically proven to reduce musculoskeletal pain, muscle spasms, connective tissue distension, hemorrhage, inflammation, and nerve conductivity [10]. This therapy has been frequently applied for pain management and postoperative care for sports injuries and surgical procedures and has been effective in reducing edema and recovery time, with short-term applications in abdominal, orthopedic, and gynecological operations [15,16,17,18,19]. Basically, low temperatures cause vasoconstriction, and pain reduction is achieved because the temperature blocks nerve endings [11]. This analgesic effect is the combination of slower propagation of neural pain signals and decreased release of chemical pain mediators, which also triggers a decrease in metabolism by more than 50%, allowing better oxygen flow to the injured tissues [20].
In dentistry, cryotherapy has already been adopted by professionals, especially for postoperative pain control after surgical procedures [21,22]. Although the effectiveness of cryotherapy has been well established in the literature, there is no standardization of the type or volume of the cryoagent used, mode of application, or duration to identify an ideal protocol for this treatment [16,23].
As it is a low cost, simple, and atoxic technique, several randomized controlled clinical studies have evaluated cryotherapy treatment for relieving pain after endodontic treatment [24,25,26,27,28,29,30,31]. Therefore, the objective of this systematic review with meta-analysis was to investigate whether the evidence currently available in major databases confirms the effectiveness of cryotherapy against postoperative pain following endodontic treatment. Based on the Population, Intervention, Comparison and Outcome (PICO) design, the following question was asked: “Does final irrigation with cold saline solution after cleaning and shaping procedures reduce postoperative pain in adult patients?”
MATERIALS AND METHODS
This systematic review with meta-analysis followed the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) statement checklist and has been registered with the International Prospective Register of Systematic Reviews (PROSPERO) (protocol number CRD42020154796) [32].
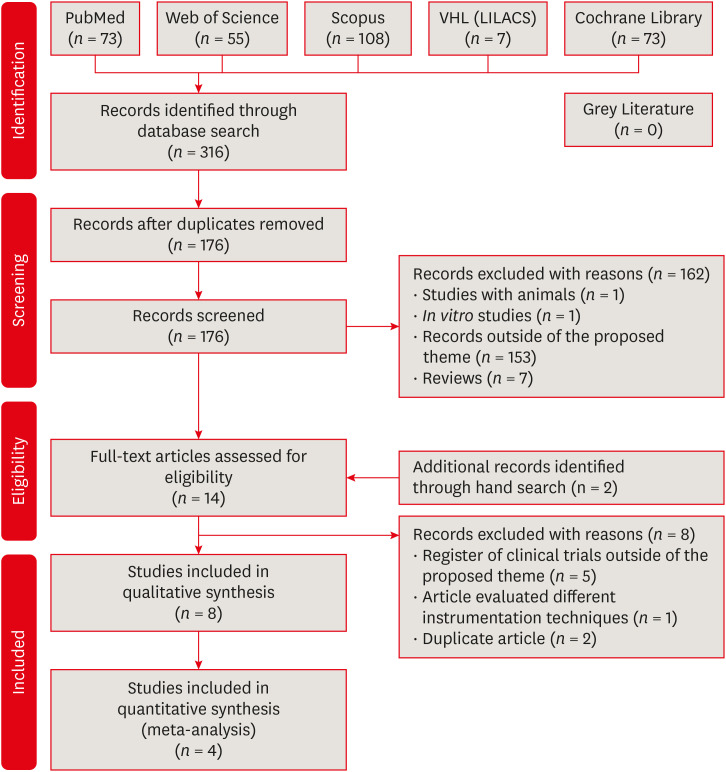
PubMed, Scopus, Web of Science, Cochrane Library, Virtual Health Library (LILACS) databases were consulted, and articles published before July 30th, 2019 were considered for review. The search of the literature was applied in Grey literature through the OpenGrey site (http://www.opengrey.eu), and references of included studies were also searched to identify other studies that might have been missed in the initial electronic search. No language or date restrictions were applied; all references were managed using Mendeley software. The selection process is described in Figure 1.
The keywords used were selected from Medical Subject Headings (MeSH) specified by the U.S. National Library of Medicine and from Health Sciences Descriptors (DeCS). Besides these, MeSH synonyms and free terms were also included. The terms were combined through boolean operators to improve the search; all combinations of terms have been collated in Table 1.
Table 1
Electronic database used and search strategy
The studies were screened and included according to the PICO study design:
Population: patients who presented permanent maxillary or mandibular teeth requiring endodontic treatment.
Intervention: final irrigation with cold saline solution (intracanal cryotherapy group).
Comparison: final irrigation with saline solution at room temperature (control group).
Outcome: measurement of postoperative pain after endodontic treatment with different types of visual analogue scales (VAS).
Study design: clinical trials, controlled clinical trials, and randomized controlled trials.
Letters to the editor, reviews, systematic reviews, guidelines, expert opinions, animal studies, in vitro studies, case reports, and articles outside the proposed theme were excluded.
Initially, two independent reviewers (FGH and LSG) screened and applied the inclusion and exclusion criteria to 10 titles and abstracts. A Kappa match of 0.90 was calculated to guarantee the reliability between them.
These independent reviewers (FGH and LSG) evaluated and applied the eligibility criteria in the titles and abstracts identified from electronic databases and manual search. An expert reviewer (LSA) was consulted to discuss the possible differences if a consensus could not be reached between the two independent reviewers. Studies that appeared in more than one database were considered only once, and full texts of those that did not have adequate information in the abstract were examined to avoid the exclusion of important studies.
The following data were extracted from the included studies independently by two researchers (FGH and LSG): 1) Author/year; 2) Study design; 3) Case/control; 4) Sex; 5) Types of teeth; 6) Diagnostic pulp; 7) Endodontic treatment (Instrumentation; Irrigation; Foraminal enlargement; Number of sessions; Cryotherapy).
Another data extraction was conducted to evaluate the tools of post-operative pain: 1) Author/year; 2) Assessment (Method; Period; Classification); 3) Postoperative medications; 4) Results.
The same authors (FGH and LSG) independently assessed the risk of bias in the included studies following the criteria of the Cochrane Handbook for Systematic Reviews of Interventions [33]. The studies were categorized as having low (+), high (-), or uncertain (?) risk of bias in the following seven domains: random sequence generation, allocation concealment, blinding of participants and personnel, blinding of outcome assessment, incomplete outcome data, selective reporting, other biases (inclusion and exclusion criteria, sample calculation). Authors of the included studies were contacted for additional missing data when required.
The meta-analysis calculations were performed using Review Manager 5.4.
Mean and standard deviation data for the included studies were extracted in relation to postoperative pain in the control group (room temperature) and in the intracanal cryotherapy group, according to periapical tissue condition. Four studies were not included in this meta-analysis due to lack of metadata for comparison—standard deviation, percentage data, and division into subgroups without reporting of the sample number of each subgroup [24,25,27,29]. The corresponding authors were contacted by email, but we received no response.
The random-effect model was adopted for this meta-analysis. Statistical heterogeneity between the studies was assessed based on the I2, where I2 values of 0% to 40%, 30% to 60%, 50% to 90%, and 75% to 100% indicated insignificant, moderate, substantial, and considerable heterogeneity, respectively [34], and a forest plot was created for this comparison. The sensitivity and subgroups analyses were also planned. If the sum of included studies of an outcome exceeded 10, funnel plots can also be generated to analyze the publication bias test.
The certainty of evidence was determined through the GRADE approach. The GRADE assessment was carried out independently by two reviewers (FGH and LSG), and disagreements were resolved by consensus or by a third author (LAA). We used the GRADEpro software GDT to create the ‘Summary of findings’ tables for the main intervention comparison. Randomized trials start with high evidence, and the quality of, or certainty in, the body of evidence decreases to very low quality if serious or very serious issues, related to risk of bias, inconsistency, indirectness, imprecision, or publication bias are present.
RESULTS
Initially, 316 records were identified through the database search, 73 from PubMed, 55 from Web of Science, 108 from Scopus, 7 from Lilacs, and 73 from the Cochrane Library. After duplicates were removed, 176 titles and abstracts were screened for applying the eligibility criteria. One hundred sixty-two articles were excluded, and 14 studies were assessed in their entirety. Two studies were included after the manual search; thus, a total of 16 studies were assessed. Then, 8 articles were excluded, 8 studies were included in qualitative synthesis, and 4 in the quantitative analysis (Figure 1).
Data extraction from the selected articles is described in Table 2 and 3. All studies were considered randomized clinical trials. The size of the samples ranged from 20 to 105 patients. The participants were divided based on sex; however, 4 studies did not specify the sex in relation to the case/control groups. Three studies evaluated the effect of intracanal cryotherapy on postoperative pain in single-rooted teeth [24,27,28,29,31]; 2 studies assessed only molar teeth, and 2 evaluated both maxillary and mandibular molar, premolar, and anterior teeth [25,26,27,30]. The study performed by Bazaid and Kenawi [29] lacked any information in this regard.
Table 2
Characteristics of the included studies: endodontic treatment
| Author/year | Study design | Case/Control | Gender (Case/Control) | Types of teeth | Diagnostic pulp | Instrumentation | Irrigation | Foraminal enlargement | No. of sessions | Cryotherapy |
|---|---|---|---|---|---|---|---|---|---|---|
| Al-Nahlawi et al. 2016 [24] | Randomized clinical trial with blind assessment technique | Group I (control): 25 | MD | Single-rooted teeth | Vital teeth with irreversible pulpitis | Rotatory (ProTaper Universal) | NaOCl 5.25% | No | 1 | 20 mL of 2°C to 4°C cold saline for 5 min using Endovac at WL |
| Group II (room temperature saline): 25 | ||||||||||
| Group III (cold saline): 25 | ||||||||||
| Keskin et al. 2017 [25] | MD | Control group (room temperature): 85 | Female: (45/57) | Incisor, Premolar, Molar | Asymptomatic irreversible pulpitis or symptomatic irreversible pulpitis with either normal apical tissues or symptomatic apical periodontitis | Rotatory (Protaper Next) | NaOCl 5.25% | No | 1 | 2.5°C cold saline for 5 min using a 31 G Navi-Tip needle 2 mm short of the WL |
| Cryotherapy group: 85 | Male: (40/28) | |||||||||
| Vera et al. 2018 [28] | Randomized multicenter clinical trial | Control group (room temperature): 105 | Female: (60/57) | Uniradicular teeth | Necrotic pulp and symptomatic apical periodontitis | Rotatory (Kerr Endo) | NaOCl 5.25% | No | 2 | 20 mL of 2.5°C cold saline for 5 min using Endovac to the WL |
| Cryotherapy group: 105 | Male: (33/36) | |||||||||
| Bazaid and Kenawi 2018 [29] | Randomized control trial | Control group (room temperature): 16 | MD | MD | Irreversible pulpitis with either normal apical tissues or apical periodontitis. | Manual (Hand files to size 25) | NaOCl | No | 1 | 2.5°C cold saline for 2 min using side vented needle |
| Cryotherapy group: 20 | ||||||||||
| Gundogdu and Arslan 2018 [26] | Randomized prospective clinical trial | Control group (room temperature): 21 | Female: 9 | Maxillary or mandibular molar teeth | Vital teeth with symptomatic apical periodontitis. | Reciprocating (Reciproc) | NaOCl 2.5% | No | 1 | Intracanal Cryotherapy Group: 20 mL of 2.5°C cold saline for 5 min |
| Male: 12 | Intraoral Cryotherapy Group: small ice packs on the vestibular surface of the tooth for 30 min | |||||||||
| Intracanal cryotherapy group: 22 | Female: 10 | Extraoral Cryotherapy Group: ice packs on the cheek surface for 30 min | ||||||||
| Male: 12 | ||||||||||
| Intraoral cryotherapy group: 21 | Female: 9 | |||||||||
| Male: 12 | ||||||||||
| Extraoral cryotherapy group: 20 | Female: 10 | |||||||||
| Male: 10 | ||||||||||
| Jain et al. 2018 [27] | In vivo study | Control group (room temperature): 30 | MD | Mandibular first molar | Symptomatic irreversible pulpitis with normal periodicals tissue, asymptomatic or symptomatic apical periodontitis. | Manual (Step back technique) | NaOCl 2.5% | No | 2 | 5 mL of 2.5°C cold saline with side vented |
| Cryotherapy group: 30 | ||||||||||
| Vieyra and Guardado, 2018 [30] | Randomized clinical trial | Control group (room temperature): 80 | Female: 43 | Maxillary and mandibular molar, premolar, anterior teeth | Vital teeth with irreversible pulpitis | Reciprocating (Reciproc) | NaOCl 5.25% | No | 1 | Group A: 5 mL of 6°C EDTA 17% + 10 mL of 6°C cold saline dispensed to the WL using Endovac for 1 min |
| Male: 37 | Group B: 5 mL of 2.5°C EDTA 17% + 10 mL of 2.5°C cold saline dispensed to the WL using Endovac for 1 min | |||||||||
| Group A (6°C): 80 | Female: 43 | |||||||||
| Male: 37 | ||||||||||
| Group B (2.5°C): 80 | Female: 43 | |||||||||
| Male: 37 | ||||||||||
| Alharthi et al. 2019 [31] | Randomized controlled trial | Group I (Cryotherapy): 35 | MD | Single-rooted teeth | Vital and non-vital teeth | Rotatory (ProTaper Universal) | NaOCl 5.25% | No | 1 | 10 mL of 1.5–2.5°C cold saline delivered to the WL by using a two |
| Group II (Room temperature): 35 | 96 side–vented needle over a period of 5 min | |||||||||
| Group III (Control): 35 |
Table 3
Analysis tools of post-operative pain
| Author/year | Assessment | ||||
|---|---|---|---|---|---|
| Method | Period | Measurement | Postoperative medications | Results | |
| Al- Nahlawi et al., 2016 [24] | VAS | 6 hr, 12 hr, 24 hr, 48 hr, 7 days | 0–100 | Ibuprofen 400 mg | VAS pain values after 6, 12, 24, and 48 hr in cold saline irrigation group were lower than those of both saline irrigation at room temperature and control groups. |
| Keskin et al., 2017 [25] | VAS | 24 hr, 48 hr | 0: no pain | MD | Patients in the cryotherapy group reported significantly lower VAS scores compared with patients in the control group (p < 0.05) at 24 hr follow-ups. |
| 1–3: mild pain | |||||
| 4–6: moderate pain | |||||
| 7–9: severe pain | |||||
| 10: the worst pain experienced | |||||
| Vera et al., 2018 [28] | VAS | 6 hr, 24 hr, 72 hr | Mild pain | Ibuprofen 600 mg | Patients in the cryotherapy group suffered significantly less pain after 6, 24, and 72 hr and needed fewer analgesics postoperatively (p < 0.05). |
| Moderate pain | |||||
| Intense pain | |||||
| Bazaid and Kenawi, 2018 [29] | VAS | 24 hr, 48 hr | MD | MD | Intracanal cryotherapy is effective in reducing postoperative pain in patients with irreversible pulpitis with apical periodontitis. But it does not affect patients with irreversible pulpitis without apical periodontitis. |
| Gundogdu and Arslan, 2018 [26] | VAS | 24 hr, 72 hr, 5 days, 7 days | MD | Ibuprofen 400 mg | When compared with control group, all the cryotherapy groups exhibited lower postoperative pain levels on the first, third, fifth, and seventh days and lower levels of pain on percussion on the seventh day (p < 0.05). |
| Jain et al., 2018 [27] | VAS | 6 hr, 24 hr, 48 hr | 0–10 | MD | There was no significant difference between cryotherapy and normal saline groups in irreversible pulpitis with normal periapical tissue. |
| In irreversible pulpitis with asymptomatic apical periodontitis, at 6 hr, normal saline group were significantly higher pain than cryotherapy group. | |||||
| In irreversible pulpitis with symptomatic apical periodontitis, at 6, 24, and 48 hr, normal saline group were significantly higher pain than cryotherapy group. | |||||
| Therefore, intracanal cryotherapy is effective in reducing post-operative pain in patient with irreversible pulpitis with apical periodontitis. | |||||
| Vieyra and Guardado, 2018 [30] | VAS | 24 hr, 48 hr, 72 hr | 0–0.5 cm: no pain | MD | No statistically relevant modification (p > 0.05) between control group and group A were encountered concerning level or period of pain. There was no statistically relevant difference (p > 0.05) among Group A and control group compared with Group B. Group B showed less pain than the rest of the groups in relation to the existence of pain at any of the three time points measured. |
| 0.6–4.0 cm: mild pain | |||||
| 0.45–7.4 cm: moderate pain | |||||
| 7.5–10 cm: severe pain | |||||
| Alharthi et al., 2019 [31] | VAS | 6 hr, 24 hr, 48 hr | 0: no pain | MD | Group I had the lowest post-endodontic pain (6 , 24 and 48 hr). Nevertheless, there was no significant difference between Group I and Group II. The highest post-endodontic pain (6, 24 and 48 hr) was in Group III. |
| 1–3: mild pain | |||||
| 4–6: moderate pain | |||||
| 7–9: severe pain | |||||
| 10: the worst pain | |||||
Regarding the type of instrumentation, manual chemomechanical preparation using conventional files was performed in 2 studies [27,29]; rotatory instrumentation was used in 4 studies, and single-file reciprocation was used in 2 [24,25,26,28,30,31].
Sodium hypochlorite (NaOCl) was used as an irrigating solution in all studies [24,25,26,27,28,29,30,31], varying only in the concentration used. Five studies used a concentration of 5.25%, whereas 2 used 2.5% [24,25,26,27,28,30,31]; 1 article did not specify the concentration [29]. Foraminal enlargement was not performed during root canal instrumentation in any included study. The treatment was performed in a single visit in most of the studies [24,25,26,29,30,31].
In relation to the cryotherapy solutions used, cold sterile saline using EndoVac or side vented needles to dispense the solution in the working length was used in 7 studies, varying only in terms of the temperatures (between 1.5°C and 4°C) and time (2 or 5 minutes) [24,25,26,27,28,29,31]. Cold EDTA 17% with cold saline for 1 minute after chemomechanical preparation was used in the working length, with EndoVac to transport the solution, in 1 study with temperatures varying between 2.5°C and 6°C [30].
All studies assessed postoperative pain through a VAS [24,25,26,27,28,29,30,31]. The period evaluated ranged from 6 hours to 7 days. Only 3 studies specified the postoperative medications used (ibuprofen) [24,26,28].
In most of the studies, vital teeth with irreversible pulpitis were included. Some studies also evaluated necrotic pulp and symptomatic apical periodontitis (SAP) [24,25,26,27,28,29,30].
Several of these articles concluded that intracanal cryotherapy is effective in reducing postoperative pain when compared with that in the control group, and lower pain levels were observed over the course of the analyzed time [24,25,26,27,28,29].
It is possible to observe different results in the reduction of postoperative pain with the use of intracanal cryotherapy according to the pulp and periapical tissue condition. In a study with vital teeth designated for conventional root canal treatment for prosthetic reasons, there was no significant difference between groups [30]. In teeth with irreversible pulpitis and normal periapical tissues, 3 articles did not observe a significant difference, while 1 article did [24,27,29,31]. All articles that evaluated teeth with SAP found a significant reduction in postoperative pain after endodontic treatment in the group that used intracanal cryotherapy [26,27,28,29]. In the study by Keskin et al. [25], patient selection encompassed teeth with asymptomatic irreversible pulpitis or symptomatic irreversible pulpitis with either normal apical tissues or SAP.
Random sequence generation; description of the completeness of outcome data for each main outcome, including attrition and exclusions from the analysis; selective reporting; and inclusion and exclusion criteria were performed in all included studies [24,25,26,27,28,29,30,31]. Regarding allocation concealment, due to insufficient information about the random sequence generation process, the corresponding articles in this domain were labeled as having unclear risk of bias [24,26,27,28,30]. Blinding of participants and personnel were not performed in 2 studies, and blinding of outcome assessment was not also performed in 3 studies [27,30,31]. Four studies performed sample calculation [25,26,28,30].
Therefore, the most common risk of bias in the selected articles was allocation concealment followed blinding of participants and personnel, blinding of outcome assessment, and sample calculation (Figure 2).
Figure 2
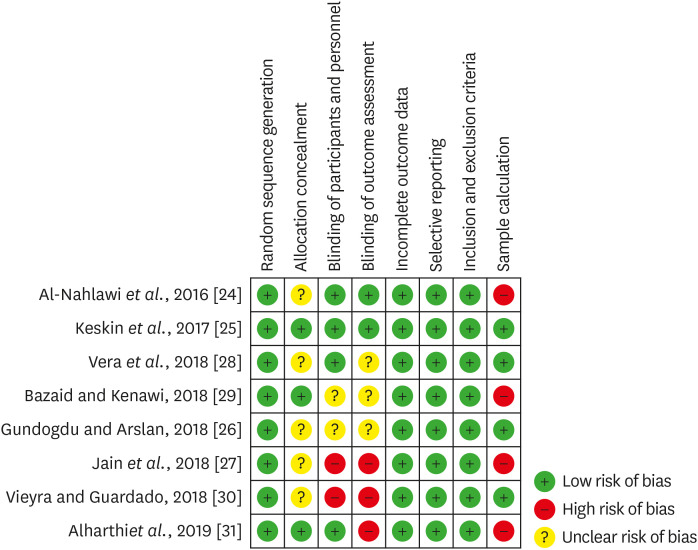
Quality assessment of the selected studies (The Cochrane Collaboration tool for assessing risk of bias).
Postoperative pain data from the control (room temperature) and intracanal cryotherapy groups, according to the condition of the periapical tissue, of the included studies were pooled and compared by meta-analysis. In initial hours (24 hours) [26,28,30,31], intracanal cryotherapy was more effective in the reduction of postoperative pain in teeth with SAP (mean difference [MD], 2.69; confidence interval, 0.35–5.03; p = 0.02; I2 = 93%). At 72 hours, the two groups showed no association regarding postoperative pain reduction (MD, 1.97; confidence interval, −1.55 to 5.50; p = 0.27; I2 = 96%); however, we can observe a greater tendency to improve this symptom when using intracanal cryotherapy. When periapical tissue was normal, no association was observed between intracanal cryotherapy and control (room temperature) groups at 24 hours (MD, 0.09; confidence interval, −0.33 to 0.51; p = 0.68; I2 = 59%) and 48 hours (MD, 0.01; confidence interval, −0.10 to 0.11; p = 0.89; I2 = 0%) [26,28,30,31]. The heterogeneity among studies (I2) ranged from 0% to 96% as shown by the forest plot (Figure 3).
Figure 3
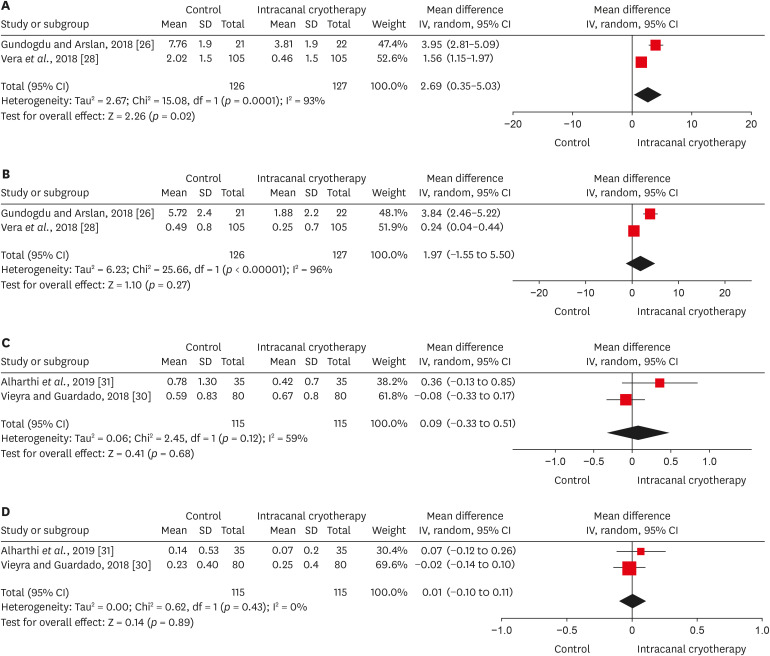
Forest plots of postoperative pain between intracanal cryotherapy group and control group (saline solution at room temperature). (A) Symptomatic apical periodontitis at 24 hours. (B) Symptomatic apical periodontitis at 72 hours. (C) Normal periapical tissue at 24 hours. (D) Normal periapical tissue at 48 hours.
SD, standard deviation; CI, confidence interval.
This study did not have enough co-variables to perform the meta-regression or sensitivity analysis. Publication bias cannot be assessed once there were not at least 10 studies included in the meta-analysis.
The quality of evidence is presented according to periapical condition. The certainty of evidence of the selected articles in all evaluated outcomes was considered very low. Serious or very serious issues with respect to risk of bias, inconsistency, imprecision, and publication bias were detected in the studies included in this meta-analysis. Explanations of these categorizations are present in the tables (Tables 4 and 5).
Table 4
Evidence profile in relation to symptomatic periapical tissue
CI, confidence interval; MD, mean difference.
*Unclear of important domains by Cochrane Collaboration tool for assessing risk of bias: Allocation concealment, Blinding of participants, personnel, and outcome assessment; †Considerable heterogeneity across studies and there is no overlap of confidence intervals; ‡Small sample.
Table 5
Evidence profile in relation to normal periapical tissue
CI, confidence interval; MD, mean difference.
*Lack of important domains by Cochrane Collaboration tool for assessing risk of bias: Allocation concealment, Blinding of participants, personnel, and outcome assessment, and Sample calculation; †Moderate heterogeneity across studies and there is little overlap of confidence intervals; ‡Small sample.
DISCUSSION
Control of postoperative pain after endodontic treatment is still a challenge for dentists. In order to minimize the effects of this discomfort, cryotherapy is often used, because it is able to promote local vasoconstriction with anti-edema effects, thus reducing inflammation in periradicular tissues [11].
A total of eight studies were included in this systematic review, and for a careful analysis of the selected studies to be performed, the Cochrane Handbook for Systematic Reviews of Interventions was used, allowing the assessment of the methodological quality to measure the risk of bias [33]. Therefore, the risk of bias was more frequent in concealment of allocation, blinding of participants and personnel, blinding of outcome assessment, and sample calculation.
Blinding was one of the aspects evaluated regarding the methodological quality of the articles. Preferably, participants and personnel, as well as outcome examiner, should be blinded in relation to the treatment to avoid the risk of performance bias [35]. However, it should be noted that operator blinding was not possible in the studies included in this systematic review due to the temperature of the solution used during the cryotherapy protocol. Being aware that this was not possible, participant and outcome examiner masking was considered a minimum requirement. Two studies did not perform the blinding of participants and personnel, and 3 studies did not perform the blinding of outcome assessment [27,30,31].
Randomization was also one of the criteria for evaluating the quality of the selected studies, and all studies performed well in this domain [24,25,26,27,28,29,30,31]. This is an extremely important requirement, as it allows patients to have the same chance of being allocated to the control and case groups without interfering with the outcome [36]. Another relevant factor is the concealment of allocation, which ensures that the operator is impartial, because he does not know to which group the participant belongs; however, in this regard only three studies reported how allocation concealment was performed, indicating a considerable risk of bias [25,29,31].
In this systematic review and meta-analysis, four studies performed sample size calculations [25,26,28,30]. In randomized clinical trials, sample size calculation is necessary to ensure that the sample is representative of the population and has the same characteristics as the population with respect to the variables under study. Thus, this calculation allows the determination of the number of elements needed to compose the sample such that valid sample results that can be generalized to the population are obtained [37].
Due to the technical limitations of endodontic treatment instrumentation and the complexity of the root canal system anatomy, irrigating solutions play a very important role in the removal of organic and inorganic debris from areas where instruments cannot reach [38]. NaOCl is the most used irrigant in endodontics due to its broad antimicrobial activity and the ability to dissolve organic matter, even though it is irritating to periapical tissues, especially at high concentrations [39,40,41,42]. NaOCl concentration was a variable factor in several studies, ranging from 2.5 to 5.25%; only one study did not report the concentration used [29]. Negative pressure irrigation was used in several of the studies and is a safe method that aims to minimize the risks of irrigating agent leakage and thus, not interfere with postoperative pain assessment [24,28,30]. Knowing that foraminal enlargement was not performed in all studies and that irrigation was performed at working lengths using safe methods, despite the different irrigation protocols, we can state that postoperative pain scores and pain severity were not related to these factors. Another factor that reduces the risk of bias is that, regardless of the concentrations of the solution and the different irrigation protocols, the same methods were applied for all groups in each study.
Pain threshold and its assessment are subjective and vary considerably among individuals [43]. All studies included in this systematic review used the VAS as a method for postoperative pain assessment. This instrument is commonly used, because it is a simple and relevant method for pain intensity assessment [44]; nevertheless, it does not identify the source of the pain, which is a disadvantage. In addition, studies can use it with different measurements and time intervals, but not prevent the analysis and compilation of data since this instrument is effective in the analysis of endodontic postoperative pain [24,25,26,27,28,29,30,31].
The conditions of the pulp and periradicular tissue can directly interfere with the postoperative pain scores and, consequently, with the assessment of the VAS scores of patients due to infection by microorganisms present in the root canal system and in the surrounding inflammatory infiltrate present in the related apical region [45]. In studies in which the included teeth had necrotic pulp or SAP, there was a clinical reduction in postoperative pain in the cryotherapy group when compared to the control group, corroborating the observation that cold solutions cause local vasoconstriction, allowing a reduction of pain by blocking the nerve endings surrounding the injured tissue [11,25,26,27,28,29,31]. However, the status of the condition of the pulp and periradicular tissue in the included primary studies is a limiting factor in this systematic review and meta-analysis, mainly due to the lack of standardization and a more specific approach regarding the inclusion criteria of the selected samples.
The absence of an ideal cryotherapy protocol leads to a lack of standardization of the type, volume, and temperature of the irrigating agent used [16,23]. In the included studies, the irrigating agent used most for cryotherapy was saline, followed by EDTA + saline [24,25,26,27,28,29,30,31]. The volume used was also a variable factor and ranged between 5 and 20 ml; in addition, the temperature ranged from 2 to 6ºC. Although the protocols between studies are very different, in most of them, when compared to the control groups, the cryotherapy groups, regardless of the agent, volume, or temperature used, had a lower postoperative pain index [24,25,26,28,30,31]. That said, the type of irrigating agent is considered less important than the maintenance of low temperatures, which promote local analgesia and reduce the chances of postoperative pain [11].
Meta-analysis, a useful statistical tool to pool data from individual studies with increased statistical accuracy, showed that intracanal cryotherapy was effective against postoperative pain after endodontic therapy in teeth with SAP. Intracanal cryotherapy groups showed better results in postoperative pain in the initial hours (24 hours). When the periapical tissue was normal, both treatments were similar in reducing postoperative pain; that is, cryotherapy did not show favorable results. The certainty of the evidence was considered very low, mainly due to the lack of important domains recommended by the Cochrane Manual of Systematic Reviews of Interventions, inconsistency, imprecision, and publication bias [33]. Future randomized clinical trials should be designed following the guidelines of the Cochrane Collaboration Tool and should mainly reduce methodological heterogeneity and increase the sample size to allow the extrapolation of outcomes.
CONCLUSIONS
Based on this systematic review and meta-analysis, there is evidence to support that intracanal cryotherapy as an adjunct to root canal treatment was effective in reducing postoperative pain in teeth with symptomatic periapical; however, the certainty of the scientific evidence was considered very low.
ACKNOWLEDGEMENTS
We are indebted to the study participants.
-
Funding: The work was supported by individual scholarships FAPERJ – Fundação de Amparo à Pesquisa do Estado do Rio de Janeiro (#E-26/010.100995/2018; #E-26/202.805/2019; #E-26/010.002195/2019), and CNPQ – Conselho Nacional de Desenvolvimento Científico e Tecnológico.
-
Conflict of Interest: No potential conflict of interest relevant to this article was reported.
-
Author Contributions:
Conceptualization: Hespanhol FG, Guimarães LS, Antunes LAA, Antunes LS.
Data curation: Hespanhol FG, Guimarães LS, Antunes LAA, Antunes LS.
Formal analysis: Hespanhol FG, Guimarães LS, Antunes LAA.
Funding acquisition: Antunes LAA, Antunes LS.
Investigation: Hespanhol FG, Guimarães LS, Antunes LAA, Antunes LS.
Methodology: Hespanhol FG, Guimarães LS, Antunes LAA, Antunes LS.
Project administration: Antunes LAA, Antunes LS.
Resources: Hespanhol FG, Guimarães LS, Antunes LAA, Antunes LS.
Software: Hespanhol FG, Guimarães LS,.
Supervision: Antunes LAA, Antunes LS.
Validation: Hespanhol FG, Guimarães LS, Antunes LAA, Antunes LS.
Visualization: Hespanhol FG, Guimarães LS, Antunes LAA, Antunes LS.
Writing - original draft: Hespanhol FG, Guimarães LS, Antunes LAA, Antunes LS.
Writing - review & editing: Hespanhol FG, Guimarães LS, Antunes LAA, Antunes LS.
- 1. Rosenberg PA. Clinical strategies for managing endodontic pain. Endod Topics 2002;3:78-92.Article
- 2. Sathorn C, Parashos P, Messer H. The prevalence of postoperative pain and flare-up in single- and multiple-visit endodontic treatment: a systematic review. Int Endod J 2008;41:91-99.ArticlePubMed
- 3. Ferraz CC, Gomes NV, Gomes BP, Zaia AA, Teixeira FB, Souza-Filho FJ. Apical extrusion of debris and irrigants using two hand and three engine-driven instrumentation techniques. Int Endod J 2001;34:354-358.ArticlePubMedPDF
- 4. Bürklein S, Schäfer E. Apically extruded debris with reciprocating single-file and full-sequence rotary instrumentation systems. J Endod 2012;38:850-852.ArticlePubMed
- 5. Tanalp J, Güngör T. Apical extrusion of debris: a literature review of an inherent occurrence during root canal treatment. Int Endod J 2014;47:211-221.ArticlePubMed
- 6. Peuhkuri K, Nevala R, Vapaatalo H, Moilanen E, Korpela R. Ibuprofen augments gastrointestinal symptoms in lactose maldigesters during a lactose tolerance test. Aliment Pharmacol Ther 1999;13:1227-1233.ArticlePubMedPDF
- 7. Püspök A, Kiener HP, Oberhuber G. Clinical, endoscopic, and histologic spectrum of nonsteroidal anti-inflammatory drug-induced lesions in the colon. Dis Colon Rectum 2000;43:685-691.ArticlePubMed
- 8. Etienney I, Beaugerie L, Viboud C, Flahault A. Non-steroidal anti-inflammatory drugs as a risk factor for acute diarrhoea: a case crossover study. Gut 2003;52:260-263.ArticlePubMedPMC
- 9. Khan AZ, George K, DeFriend DJ. Nonsteroidal anti-inflammatory drug-induced colonic stenosis: an unusual cause of a right-sided colonic mass: report of a case. Dis Colon Rectum 2003;46:403-405.PubMed
- 10. Belitsky RB, Odam SJ, Hubley-Kozey C. Evaluation of the effectiveness of wet ice, dry ice, and cryogenic packs in reducing skin temperature. Phys Ther 1987;67:1080-1084.PubMed
- 11. Modabber A, Rana M, Ghassemi A, Gerressen M, Gellrich NC, Hölzle F, Rana M. Three-dimensional evaluation of postoperative swelling in treatment of zygomatic bone fractures using two different cooling therapy methods: a randomized, observer-blind, prospective study. Trials 2013;14:238.ArticlePubMedPMC
- 12. Doğanay Yıldız E, Arslan H. Effect of low-level laser therapy on postoperative pain in molars with symptomatic apical periodontitis: a randomized placebo-controlled clinical trial. J Endod 2018;44:1610-1615.ArticlePubMed
- 13. Coelho MS, Vilas-Boas L, Tawil PZ. The effects of photodynamic therapy on postoperative pain in teeth with necrotic pulps. Photodiagnosis Photodyn Ther 2019;27:396-401.ArticlePubMed
- 14. Fayyad DM, Abdelsalam N, Hashem N. Cryotherapy: a new paradigm of treatment in endodontics. J Endod 2020;46:936-942.ArticlePubMed
- 15. Swenson C, Swärd L, Karlsson J. Cryotherapy in sports medicine. Scand J Med Sci Sports 1996;6:193-200.ArticlePubMed
- 16. Watkins AA, Johnson TV, Shrewsberry AB, Nourparvar P, Madni T, Watkins CJ, Feingold PL, Kooby DA, Maithel SK, Staley CA, Master VA. Ice packs reduce postoperative midline incision pain and narcotic use: a randomized controlled trial. J Am Coll Surg 2014;219:511-517.ArticlePubMed
- 17. McDowell JH, McFarland EG, Nalli BJ. Use of cryotherapy for orthopaedic patients. Orthop Nurs 1994;13:21-30.Article
- 18. Kwekkeboom KL. Pain management strategies used by patients with breast and gynecologic cancer with postoperative pain. Cancer Nurs 2001;24:378-386.ArticlePubMed
- 19. Koç M, Tez M, Yoldaş O, Dizen H, Göçmen E. Cooling for the reduction of postoperative pain: prospective randomized study. Hernia 2006;10:184-186.ArticlePubMedPDF
- 20. Bleakley C, McDonough S, MacAuley D. The use of ice in the treatment of acute soft-tissue injury: a systematic review of randomized controlled trials. Am J Sports Med 2004;32:251-261.PubMed
- 21. Forsgren H, Heimdahl A, Johansson B, Krekmanov L. Effect of application of cold dressings on the postoperative course in oral surgery. Int J Oral Surg 1985;14:223-228.ArticlePubMed
- 22. Laureano Filho JR, de Oliveira e Silva ED, Batista CI, Gouveia FM. The influence of cryotherapy on reduction of swelling, pain and trismus after third-molar extraction: a preliminary study. J Am Dent Assoc 2005;136:774-778.PubMed
- 23. Hubbard TJ, Denegar CR. Does cryotherapy improve outcomes with soft tissue injury? J Athl Train 2004;39:278-279.PubMedPMC
- 24. Al-Nahlawi T, Hatab TA, Alrazak MA, Al-Abdullah A. Effect of intracanal cryotherapy and negative irrigation technique on postendodontic pain. J Contemp Dent Pract 2016;17:990-996.ArticlePubMed
- 25. Keskin C, Özdemir Ö, Uzun İ, Güler B. Effect of intracanal cryotherapy on pain after single-visit root canal treatment. Aust Endod J 2017;43:83-88.ArticlePubMedPDF
- 26. Gundogdu EC, Arslan H. Effects of various cryotherapy applications on postoperative pain in molar teeth with symptomatic apical periodontitis: a preliminary randomized prospective clinical trial. J Endod 2018;44:349-354.ArticlePubMed
- 27. Jain A, Davis D, Bahuguna R, Agrawal A, Singh S, Ramachandran R, Varguese A. Role of cryotherapy in reducing postoperative pain in patients with irreversible pulpitis: an in-vivo study. Int J Dent Med Sci Res 2018;2:43-49.
- 28. Vera J, Ochoa J, Romero M, Vazquez-Carcaño M, Ramos-Gregorio CO, Aguilar RR, Cruz A, Sleiman P, Arias A. Intracanal cryotherapy reduces postoperative pain in teeth with symptomatic apical periodontitis: a randomized multicenter clinical trial. J Endod 2018;44:4-8.ArticlePubMed
- 29. Bazaid DS, Kenawi LM. The effect of intracanal cryotherapy in reducing postoperative pain in patients with irreversible pulpitis: a randomized control trial. Int J Health Sci Res 2018;8:83-88.
- 30. Vieyra JP, Guardado JA. Reduction of post-endodontic pain after one-visit root canal treatment using three cryotherapy protocols with different temperature. Ann Materials Sci Eng 2018;3:1033.
- 31. Alharthi AA, Aljoudi MH, Almaliki MN, Almalki MA, Sunbul MA. Effect of intra-canal cryotherapy on post-endodontic pain in single-visit RCT: a randomized controlled trial. Saudi Dent J 2019;31:330-335.ArticlePubMedPMC
- 32. Moher D, Liberati A, Tetzlaff J, Altman DG. PRISMA Group. Preferred reporting items for systematic reviews and meta-analyses: the PRISMA statement. Ann Intern Med 2009;151:264-269.ArticlePubMed
- 33. Higgins JP, Altman DG, Gøtzsche PC, Jüni P, Moher D, Oxman AD, Savovic J, Schulz KF, Weeks L, Sterne JA; Cochrane Statistical Methods Group. Cochrane Bias Methods Group. The Cochrane Collaboration’s tool for assessing risk of bias in randomised trials. BMJ 2011;343:d5928.ArticlePubMedPMC
- 34. Deeks JJ, Higgins JP. Chapter 10: Analysing data and undertaking meta-analyses. Cochrane handbook for systematic reviews of interventions. Chichester: John Wiley & Sons; 2019. p. 243-296.
- 35. Ammari MM, Soviero VM, da Silva Fidalgo TK, Lenzi M, Ferreira DM, Mattos CT, de Souza IP, Maia LC. Is non-cavitated proximal lesion sealing an effective method for caries control in primary and permanent teeth? A systematic review and meta-analysis. J Dent 2014;42:1217-1227.ArticlePubMed
- 36. Borges Silva EA, Guimarães LS, Küchler EC, Antunes LA, Antunes LS. Evaluation of effect of foraminal enlargement of necrotic teeth on postoperative symptoms: a systematic review and meta-analysis. J Endod 2017;43:1969-1977.ArticlePubMed
- 37. Moher D, Hopewell S, Schulz KF, Montori V, Gøtzsche PC, Devereaux PJ, Elbourne D, Egger M, Altman DG. CONSORT 2010 explanation and elaboration: updated guidelines for reporting parallel group randomised trials. BMJ 2010;340:c869.ArticlePubMedPMC
- 38. Varela P, Souza E, de Deus G, Duran-Sindreu F, Mercadé M. Effectiveness of complementary irrigation routines in debriding pulp tissue from root canals instrumented with a single reciprocating file. Int Endod J 2019;52:475-483.ArticlePubMedPDF
- 39. Zehnder M. Root canal irrigants. J Endod 2006;32:389-398.ArticlePubMed
- 40. Zehnder M, Kosicki D, Luder H, Sener B, Waltimo T. Tissue-dissolving capacity and antibacterial effect of buffered and unbuffered hypochlorite solutions. Oral Surg Oral Med Oral Pathol Oral Radiol Endod 2002;94:756-762.ArticlePubMed
- 41. Gernhardt CR, Eppendorf K, Kozlowski A, Brandt M. Toxicity of concentrated sodium hypochlorite used as an endodontic irrigant. Int Endod J 2004;37:272-280.ArticlePubMed
- 42. de Sermeño RF, da Silva LA, Herrera H, Herrera H, Silva RA, Leonardo MR. Tissue damage after sodium hypochlorite extrusion during root canal treatment. Oral Surg Oral Med Oral Pathol Oral Radiol Endod 2009;108:e46-e49.Article
- 43. Silva EJ, Menaged K, Ajuz N, Monteiro MR, Coutinho-Filho TS. Postoperative pain after foraminal enlargement in anterior teeth with necrosis and apical periodontitis: a prospective and randomized clinical trial. J Endod 2013;39:173-176.ArticlePubMed
- 44. Haefeli M, Elfering A. Pain assessment. Eur Spine J 2006;15(Suppl 1):S17-S24.ArticlePubMedPDF
- 45. Nair PN. Apical periodontitis: a dynamic encounter between root canal infection and host response. Periodontol 2000 1997;13:121-148.ArticlePubMed
REFERENCES
Tables & Figures
REFERENCES
Citations
Citations to this article as recorded by 
- Postoperative Pain After Endodontic Treatment in HIV‐Positive Patients Under HAART: A Prospective Observational Cohort Study
Marcos Felipe Iparraguirre Nuñovero, Marco Antonio Hungaro Duarte, Luciana Reis Azevedo Alanis, Bruno Cavalini Cavenago, Ulisses Xavier da Silva Neto, Everdan Carneiro
International Endodontic Journal.2026; 59(5): 788. CrossRef - Effect of low-temperature intracanal sodium hypochlorite on root surface temperature reduction and organic tissue dissolution: an in vitro study
Marcos Felipe Iparraguirre Nuñovero, Marco Antonio Hungaro Duarte, Ulisses Xavier da Silva Neto, Vânia Portela Ditzel Westphalen, Pedro Cesar Gomes Titato, Bruno Cavalini Cavenago, Everdan Carneiro
Scientific Reports.2026;[Epub] CrossRef - Effectiveness of intracanal cryotherapy in reducing post-endodontic pain in irreversible pulpitis: a systematic review and meta-analysis
Maged Mohamed, Asmaa Abdelmajeed, Muhammad Salah-Uddin Anwar Laithy, Dina Abozaid
Scientific Reports.2026;[Epub] CrossRef - Post-Operative Pain After Endodontic Instrumentation, Irrigation and Obturation: An Umbrella Review of Systematic Reviews Published from 2016 to 2025
Fausto Zamparini, Andrea Spinelli, Gioia Quadrini, Maria Giovanna Gandolfi, Carlo Prati
Journal of Clinical Medicine.2026; 15(12): 4775. CrossRef - Impact of intracanal cryotherapy on postoperative pain in symptomatic apical periodontitis: A systematic review and meta-analysis of randomized clinical trials
Nishtha K. Patel, Prerak Doshi, Shaily R. Dalal, Pooja R. Kesharani, Shilpa S. Shah, Mohil H. Kale
Endodontology.2025; 37(2): 101. CrossRef - Evaluation of Post‐Endodontic Pain Reduction Using Intracanal Cryotherapy in Symptomatic Apical Periodontitis
Anam Fayyaz Bashir, Ussamah Waheed Jatala, Muhammad Amber Fareed, Sheryar Sheryar, Saadia Ahmad Chattha, Saima Razaq Khan, Shahzad Ahmad, Shazia Iqbal, Muhammad Sohail Zafar, Shahzad Ali
Australian Endodontic Journal.2025; 51(3): 677. CrossRef - Comparing cryotherapy and ketorolac tromethamine against room-temperature saline irrigation using interleukin-8 levels and post-operative pain within single-visit endodontic treatment of symptomatic irreversible pulpitis superimposed by apical periodontit
Yousra Khaled Ezzat, Alaa Diab, Olfat Shaker, Sarah Abouelenien
BMC Oral Health.2025;[Epub] CrossRef - Determining Efficacy of Intracanal Cryotherapy on Post Endodontic Pain in Irreversible Pulpitis
Anam Fayyaz Bashir, Ussamah Waheed Jatala, Moeen ud din Ahmad, Muhammad Talha Khan, Saima Razzaq Khan, Aisha Arshad Butt
Pakistan Journal of Health Sciences.2024; : 68. CrossRef - The effect of intracanal cryotherapy with and without foraminal enlargement on pain prevention after endodontic treatment: a randomized clinical trial
Marcos Felipe Iparraguirre Nuñovero, Marco Antonio Hungaro Duarte, André Vinícius Kaled Segato, Ulisses Xavier da Silva Neto, Vania Portela Ditzel Westphalen, Everdan Carneiro
Scientific Reports.2024;[Epub] CrossRef - Effect of cryotherapy duration on experimentally induced connective tissue inflammationin vivo
Jorge Vera, Mayra Alejandra Castro-Nuñez, María Fernanda Troncoso-Cibrian, Ana Gabriela Carrillo-Varguez, Edgar Ramiro Méndez Sánchez, Viviana Sarmiento, Lourdes Lanzagorta-Rebollo, Prasanna Neelakantan, Monica Romero, Ana Arias
Restorative Dentistry & Endodontics.2023;[Epub] CrossRef - Evaluation of knowledge and awareness of pediatric oral health among school teachers of Hazaribag before and after oral health education.
Vipin Ahuja, Annapurna Ahuja, Nilima Thosar
F1000Research.2023; 12: 1292. CrossRef
 ePub Link
ePub Link Cite
CiteEffect of intracanal cryotherapy on postoperative pain after endodontic treatment: systematic review with meta-analysis
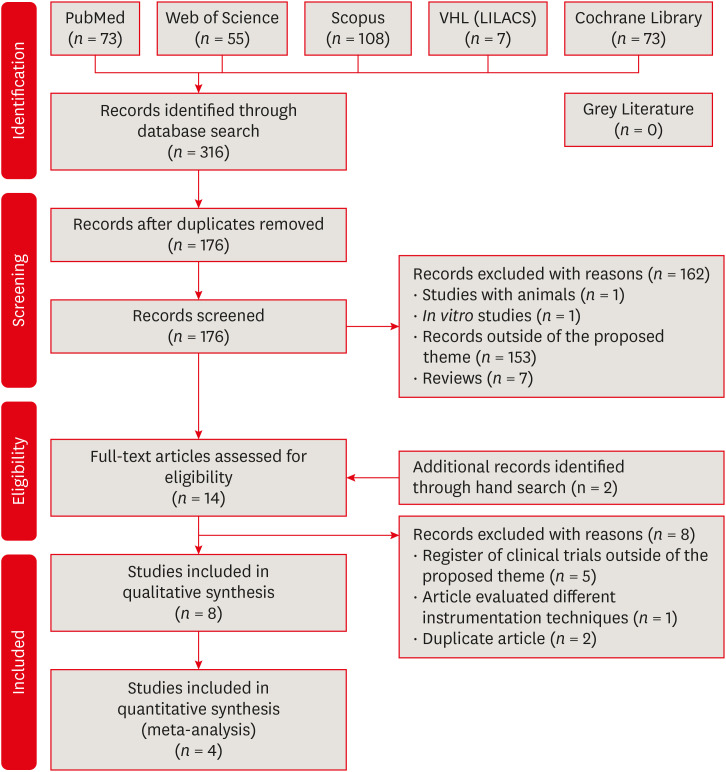
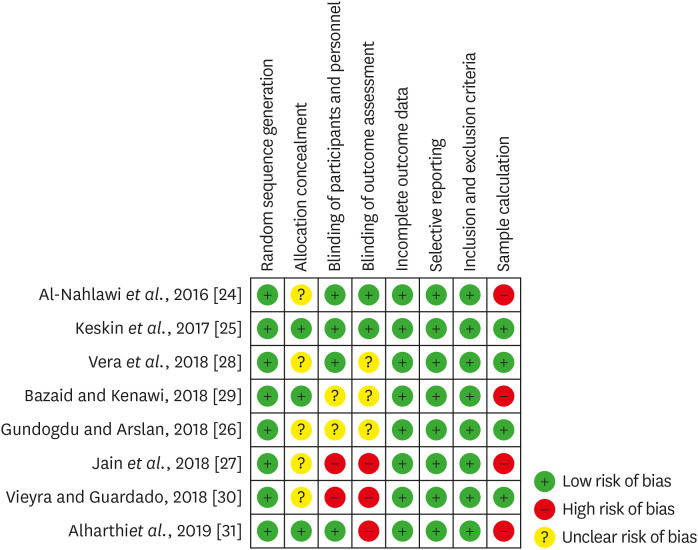
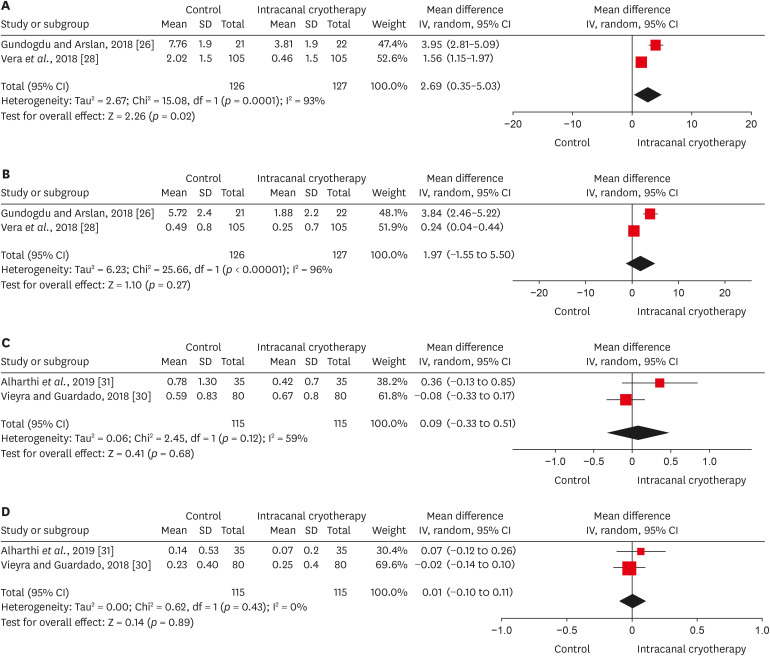
Figure 1 Modified PRISMA 2009 flow diagram.
Figure 2 Quality assessment of the selected studies (The Cochrane Collaboration tool for assessing risk of bias).
Figure 3 Forest plots of postoperative pain between intracanal cryotherapy group and control group (saline solution at room temperature). (A) Symptomatic apical periodontitis at 24 hours. (B) Symptomatic apical periodontitis at 72 hours. (C) Normal periapical tissue at 24 hours. (D) Normal periapical tissue at 48 hours.SD, standard deviation; CI, confidence interval.
Figure 1
Figure 2
Figure 3
Effect of intracanal cryotherapy on postoperative pain after endodontic treatment: systematic review with meta-analysis
Electronic database used and search strategy
| Database | Search strategy |
|---|---|
| PubMed | #1(root canal preparation[MeSH Terms]) OR root canal therapy[MeSH Terms]) OR root canal obturation[MeSH Terms]) OR periapical periodontitis[MeSH Terms]) OR dental pulp necrosis[MeSH Terms]) OR root canal preparation[Title/Abstract]) OR root canal therapy[Title/Abstract]) OR root canal obturation[Title/Abstract]) OR periapical periodontitis[Title/Abstract]) OR dental pulp necrosis[Title/Abstract]) OR root canal treatment[Title/Abstract]) OR endodontic treatment[Title/Abstract]) OR endodontic obturation[Title/Abstract]) OR root canal instrumentation[Title/Abstract]) OR apical periodontitis[Title/Abstract] |
| #2(pain[MeSH Terms]) OR postoperative pain[MeSH Terms]) OR hyperemia[MeSH Terms]) OR edema[MeSH Terms]) OR hyperesthesia[MeSH Terms]) OR pain[Title/Abstract]) OR postoperative pain[Title/Abstract]) OR hyperemia[Title/Abstract]) OR edema[Title/Abstract]) OR hyperesthesia[Title/Abstract]) OR postendodontic pain[Title/Abstract]) OR touch pain[Title/Abstract] | |
| #3(cryotherapy[MeSH Terms]) OR cryotherapy[Title/Abstract]) OR cold therapy[Title/Abstract]) OR cold[Title/Abstract] | |
| #1 and #2 and #3 | |
| Scopus | #1(TITLE-ABS-KEY (root AND canal AND preparation) OR TITLE-ABS KEY (root AND canal AND therapy) OR TITLE-ABS-KEY (root AND canal AND obturation) OR TITLE-ABS-KEY (periapical AND periodontitis) OR TITLE-ABS-KEY (dental AND pulp AND necrosis) OR TITLE-ABS-KEY (root AND canal AND treatment) OR TITLE-ABS-KEY (endodontic AND treatment) OR TITLE-ABS-KEY (endodontic AND obturation) OR TITLE-ABS-KEY (root AND canal AND instrumentation) OR TITLE-ABS-KEY (apical AND periodontitis)) |
| #2(TITLE-ABS-KEY (postendodontic AND pain) OR TITLE-ABS-KEY (pain) OR TITLE-ABS-KEY (postoperative AND pain) OR TITLE-ABS-KEY (touch AND pain) OR TITLE-ABS-KEY (hyperemia) OR TITLE-ABS-KEY (edema) OR TITLE-ABS-KEY (hyperesthesia)) | |
| #3TITLE-ABS-KEY (cryotherapy) OR TITLE-ABS-KEY (cold AND therapy) OR TITLE-ABS-KEY (cold)) | |
| #1 and #2 and #3 | |
| Web of Science |
#1TOPIC: (root canal preparation) |
|
#2TOPIC: (postendodontic pain) | |
|
#3TOPIC: (cryotherapy) | |
| #1 and #2 and #3 | |
| Cochrane Library | ‘root canal therapy OR root canal preparation OR root canal obturation OR periapical periodontitis OR dental pulp necrosis OR endodontic obturation OR apical periodontitis)) AND (tw:(pain OR postoperative pain OR hyperemia OR edema OR hyperesthesia)) AND (tw:(cryotherapy OR cold therapy OR cold in Title, Abstract, Keywords in Trials’ |
| VHL (LILACS) | (tw:(root canal therapy OR root canal preparation OR root canal obturation OR periapical periodontitis OR dental pulp necrosis OR endodontic obturation OR apical periodontitis)) AND (tw:(pain OR postoperative pain OR hyperemia OR edema OR hyperesthesia)) AND (tw:(cryotherapy OR cold therapy OR cold)) |
| Grey Literature | (root canal preparation OR endodontic treatment) AND (postoperative pain) AND (cryotherapy) |
Characteristics of the included studies: endodontic treatment
| Author/year | Study design | Case/Control | Gender (Case/Control) | Types of teeth | Diagnostic pulp | Instrumentation | Irrigation | Foraminal enlargement | No. of sessions | Cryotherapy |
|---|---|---|---|---|---|---|---|---|---|---|
| Al-Nahlawi | Randomized clinical trial with blind assessment technique | Group I (control): 25 | MD | Single-rooted teeth | Vital teeth with irreversible pulpitis | Rotatory (ProTaper Universal) | NaOCl 5.25% | No | 1 | 20 mL of 2°C to 4°C cold saline for 5 min using Endovac at WL |
| Group II (room temperature saline): 25 | ||||||||||
| Group III (cold saline): 25 | ||||||||||
| Keskin | MD | Control group (room temperature): 85 | Female: (45/57) | Incisor, Premolar, Molar | Asymptomatic irreversible pulpitis or symptomatic irreversible pulpitis with either normal apical tissues or symptomatic apical periodontitis | Rotatory (Protaper Next) | NaOCl 5.25% | No | 1 | 2.5°C cold saline for 5 min using a 31 G Navi-Tip needle 2 mm short of the WL |
| Cryotherapy group: 85 | Male: (40/28) | |||||||||
| Vera | Randomized multicenter clinical trial | Control group (room temperature): 105 | Female: (60/57) | Uniradicular teeth | Necrotic pulp and symptomatic apical periodontitis | Rotatory (Kerr Endo) | NaOCl 5.25% | No | 2 | 20 mL of 2.5°C cold saline for 5 min using Endovac to the WL |
| Cryotherapy group: 105 | Male: (33/36) | |||||||||
| Bazaid and Kenawi 2018 [ | Randomized control trial | Control group (room temperature): 16 | MD | MD | Irreversible pulpitis with either normal apical tissues or apical periodontitis. | Manual (Hand files to size 25) | NaOCl | No | 1 | 2.5°C cold saline for 2 min using side vented needle |
| Cryotherapy group: 20 | ||||||||||
| Gundogdu and Arslan 2018 [ | Randomized prospective clinical trial | Control group (room temperature): 21 | Female: 9 | Maxillary or mandibular molar teeth | Vital teeth with symptomatic apical periodontitis. | Reciprocating (Reciproc) | NaOCl 2.5% | No | 1 | Intracanal Cryotherapy Group: 20 mL of 2.5°C cold saline for 5 min |
| Male: 12 | Intraoral Cryotherapy Group: small ice packs on the vestibular surface of the tooth for 30 min | |||||||||
| Intracanal cryotherapy group: 22 | Female: 10 | Extraoral Cryotherapy Group: ice packs on the cheek surface for 30 min | ||||||||
| Male: 12 | ||||||||||
| Intraoral cryotherapy group: 21 | Female: 9 | |||||||||
| Male: 12 | ||||||||||
| Extraoral cryotherapy group: 20 | Female: 10 | |||||||||
| Male: 10 | ||||||||||
| Jain | In vivo study | Control group (room temperature): 30 | MD | Mandibular first molar | Symptomatic irreversible pulpitis with normal periodicals tissue, asymptomatic or symptomatic apical periodontitis. | Manual (Step back technique) | NaOCl 2.5% | No | 2 | 5 mL of 2.5°C cold saline with side vented |
| Cryotherapy group: 30 | ||||||||||
| Vieyra and Guardado, 2018 [ | Randomized clinical trial | Control group (room temperature): 80 | Female: 43 | Maxillary and mandibular molar, premolar, anterior teeth | Vital teeth with irreversible pulpitis | Reciprocating (Reciproc) | NaOCl 5.25% | No | 1 | Group A: 5 mL of 6°C EDTA 17% + 10 mL of 6°C cold saline dispensed to the WL using Endovac for 1 min |
| Male: 37 | Group B: 5 mL of 2.5°C EDTA 17% + 10 mL of 2.5°C cold saline dispensed to the WL using Endovac for 1 min | |||||||||
| Group A (6°C): 80 | Female: 43 | |||||||||
| Male: 37 | ||||||||||
| Group B (2.5°C): 80 | Female: 43 | |||||||||
| Male: 37 | ||||||||||
| Alharthi | Randomized controlled trial | Group I (Cryotherapy): 35 | MD | Single-rooted teeth | Vital and non-vital teeth | Rotatory (ProTaper Universal) | NaOCl 5.25% | No | 1 | 10 mL of 1.5–2.5°C cold saline delivered to the WL by using a two |
| Group II (Room temperature): 35 | 96 side–vented needle over a period of 5 min | |||||||||
| Group III (Control): 35 |
MD, missing data; NaOCl, sodium hypochlorite; WL, working length.
Analysis tools of post-operative pain
| Author/year | Assessment | ||||
|---|---|---|---|---|---|
| Method | Period | Measurement | Postoperative medications | Results | |
| Al- Nahlawi | VAS | 6 hr, 12 hr, 24 hr, 48 hr, 7 days | 0–100 | Ibuprofen 400 mg | VAS pain values after 6, 12, 24, and 48 hr in cold saline irrigation group were lower than those of both saline irrigation at room temperature and control groups. |
| Keskin | VAS | 24 hr, 48 hr | 0: no pain | MD | Patients in the cryotherapy group reported significantly lower VAS scores compared with patients in the control group ( |
| 1–3: mild pain | |||||
| 4–6: moderate pain | |||||
| 7–9: severe pain | |||||
| 10: the worst pain experienced | |||||
| Vera | VAS | 6 hr, 24 hr, 72 hr | Mild pain | Ibuprofen 600 mg | Patients in the cryotherapy group suffered significantly less pain after 6, 24, and 72 hr and needed fewer analgesics postoperatively ( |
| Moderate pain | |||||
| Intense pain | |||||
| Bazaid and Kenawi, 2018 [ | VAS | 24 hr, 48 hr | MD | MD | Intracanal cryotherapy is effective in reducing postoperative pain in patients with irreversible pulpitis with apical periodontitis. But it does not affect patients with irreversible pulpitis without apical periodontitis. |
| Gundogdu and Arslan, 2018 [ | VAS | 24 hr, 72 hr, 5 days, 7 days | MD | Ibuprofen 400 mg | When compared with control group, all the cryotherapy groups exhibited lower postoperative pain levels on the first, third, fifth, and seventh days and lower levels of pain on percussion on the seventh day ( |
| Jain | VAS | 6 hr, 24 hr, 48 hr | 0–10 | MD | There was no significant difference between cryotherapy and normal saline groups in irreversible pulpitis with normal periapical tissue. |
| In irreversible pulpitis with asymptomatic apical periodontitis, at 6 hr, normal saline group were significantly higher pain than cryotherapy group. | |||||
| In irreversible pulpitis with symptomatic apical periodontitis, at 6, 24, and 48 hr, normal saline group were significantly higher pain than cryotherapy group. | |||||
| Therefore, intracanal cryotherapy is effective in reducing post-operative pain in patient with irreversible pulpitis with apical periodontitis. | |||||
| Vieyra and Guardado, 2018 [ | VAS | 24 hr, 48 hr, 72 hr | 0–0.5 cm: no pain | MD | No statistically relevant modification ( |
| 0.6–4.0 cm: mild pain | |||||
| 0.45–7.4 cm: moderate pain | |||||
| 7.5–10 cm: severe pain | |||||
| Alharthi | VAS | 6 hr, 24 hr, 48 hr | 0: no pain | MD | Group I had the lowest post-endodontic pain (6 , 24 and 48 hr). Nevertheless, there was no significant difference between Group I and Group II. The highest post-endodontic pain (6, 24 and 48 hr) was in Group III. |
| 1–3: mild pain | |||||
| 4–6: moderate pain | |||||
| 7–9: severe pain | |||||
| 10: the worst pain | |||||
MD, missing data; VAS, visual analogue scale.
Evidence profile in relation to symptomatic periapical tissue
| Certainty assessment | No. of patients | Effect | Certainty | Importance | |||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| No. of studies | Study design | Risk of bias | Inconsistency | Indirectness | Imprecision | Other considerations | Intracanal cryotherapy | Control | Relative (95% CI) | Absolute (95% CI) | |||
| Symptomatic periapical tissue (24 hr) | |||||||||||||
| 2 | Randomized trials | Serious* | Very serious† | Not serious | Serious‡ | Publication bias strongly suspected‡ | 127 | 126 | - | MD 2.69 higher (0.35 higher to 5.03 higher) | ⊕○○○ | IMPORTANT | |
| VERY LOW | |||||||||||||
| Symptomatic periapical tissue (72 hr) | |||||||||||||
| 2 | Randomized trials | Serious* | Very serious† | Not serious | Serious‡ | Publication bias strongly suspected‡ | 127 | 126 | - | MD 1.97 higher (1.55 lower to 5.5 higher) | ⊕○○○ | IMPORTANT | |
| VERY LOW | |||||||||||||
CI, confidence interval; MD, mean difference.
*Unclear of important domains by Cochrane Collaboration tool for assessing risk of bias: Allocation concealment, Blinding of participants, personnel, and outcome assessment; †Considerable heterogeneity across studies and there is no overlap of confidence intervals; ‡Small sample.
Evidence profile in relation to normal periapical tissue
| Certainty assessment | No. of patients | Effect | Certainty | Importance | |||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| No. of studies | Study design | Risk of bias | Inconsistency | Indirectness | Imprecision | Other considerations | Intracanal cryotherapy | Control | Relative (95% CI) | Absolute (95% CI) | |||
| Normal periapical tissue (24 hr) | |||||||||||||
| 2 | Randomized trials | Serious* | Serious† | Not serious | Serious‡ | Publication bias strongly suspected‡ | 115 | 115 | - | MD 0.09 higher (0.33 lower to 0.51 higher) | ⊕○○○ | IMPORTANT | |
| VERY LOW | |||||||||||||
| Normal periapical tissue (48 hr) | |||||||||||||
| 2 | Randomized trials | Serious* | Not serious | Not serious | Serious‡ | Publication bias strongly suspected‡ | 115 | 115 | - | MD 0.01 higher (0.1 lower to 0.11 higher) | ⊕○○○ | IMPORTANT | |
| VERY LOW | |||||||||||||
CI, confidence interval; MD, mean difference.
*Lack of important domains by Cochrane Collaboration tool for assessing risk of bias: Allocation concealment, Blinding of participants, personnel, and outcome assessment, and Sample calculation; †Moderate heterogeneity across studies and there is little overlap of confidence intervals; ‡Small sample.
Table 1 Electronic database used and search strategy
Table 2 Characteristics of the included studies: endodontic treatment
MD, missing data; NaOCl, sodium hypochlorite; WL, working length.
Table 3 Analysis tools of post-operative pain
MD, missing data; VAS, visual analogue scale.
Table 4 Evidence profile in relation to symptomatic periapical tissue
CI, confidence interval; MD, mean difference.
*Unclear of important domains by Cochrane Collaboration tool for assessing risk of bias: Allocation concealment, Blinding of participants, personnel, and outcome assessment; †Considerable heterogeneity across studies and there is no overlap of confidence intervals; ‡Small sample.
Table 5 Evidence profile in relation to normal periapical tissue
CI, confidence interval; MD, mean difference.
*Lack of important domains by Cochrane Collaboration tool for assessing risk of bias: Allocation concealment, Blinding of participants, personnel, and outcome assessment, and Sample calculation; †Moderate heterogeneity across studies and there is little overlap of confidence intervals; ‡Small sample.

