
Search
- Page Path
- HOME > Search
Research Articles
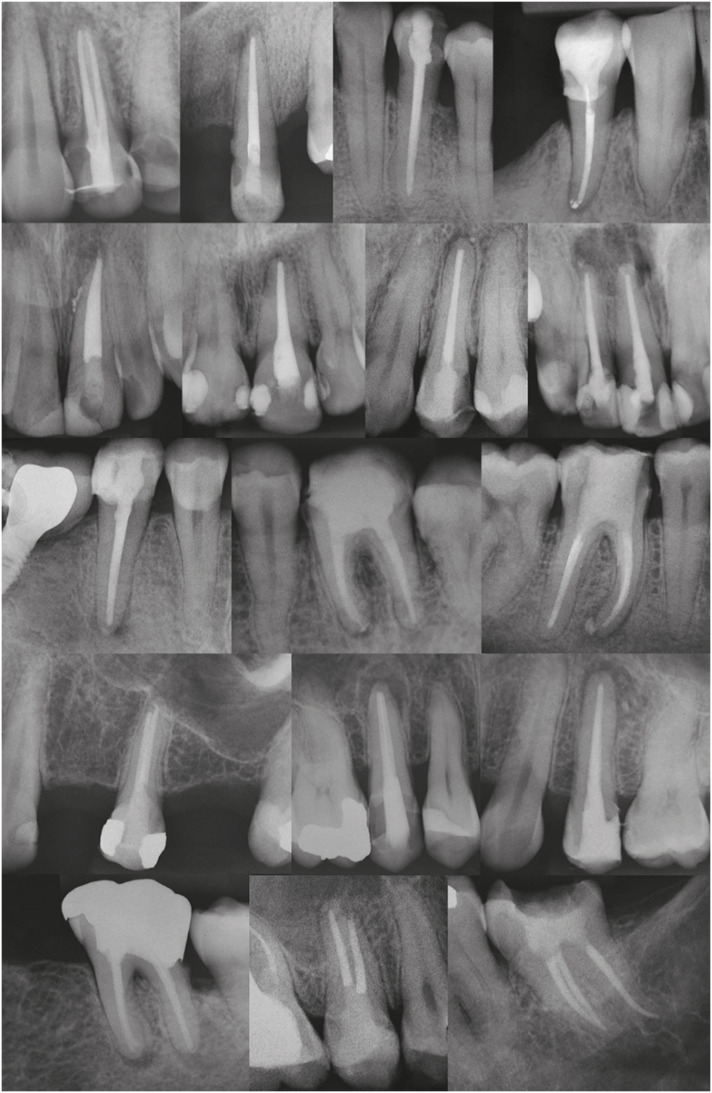
- Postoperative pain after endodontic treatment of necrotic teeth with large intentional foraminal enlargement
- Ricardo Machado, Daniel Comparin, Sérgio Aparecido Ignácio, Ulisses Xavier da Silva Neto
- Restor Dent Endod 2021;46(3):e31. Published online May 31, 2021
- DOI: https://doi.org/10.5395/rde.2021.46.e31
-
 Abstract
Abstract
 PDF
PDF PubReader
PubReader ePub
ePub Objectives To evaluate postoperative pain after endodontic treatment of necrotic teeth using large intentional foraminal enlargement (LIFE).
Materials and Methods The sample included 60 asymptomatic necrotic teeth (with or without chronic apical periodontitis), and a periodontal probing depth of 3 mm, previously accessed and referred to perform endodontic treatment. After previous procedures, the position and approximate size of the apical foramen (AF) were determined by using an apex locator and K flexo-files, respectively. The chemomechanical preparation was performed with Profile 04 files 2 mm beyond the AF to achieve the LIFE, using 2.5 mL of 2.5% NaOCl at each file change. The filling was performed by Tagger's hybrid technique and EndoFill sealer. Phone calls were made to all the patients at 24, 48 and 72 hours after treatment, to classify postoperative pain. Statistical analysis was performed by different tests with a significance level of 5%.
Results Age, gender, periradicular status and tooth type did not influence postoperative pain (
p > 0.05). Only 1 patient (1.66%) reported severe pain after 72 hours. Moderate pain was reported by 7, 4 and 3 patients after 24, 48 and 72 hours, respectively (p = 0.0001). However, paired analyses showed a statistically significant difference only between 24 and 72 hours (p = 0.04). Sealer extrusion did not influence the postoperative pain (p > 0.05).Conclusions Acute or moderate postoperative pain was uncommon after endodontic treatment of necrotic teeth with LIFE.
Trial Registration The Brazilian Clinical Trials Registry Identifier:
RBR-3r967t -
Citations
Citations to this article as recorded by
- Postoperative Pain After Endodontic Treatment in HIV‐Positive Patients Under HAART: A Prospective Observational Cohort Study
Marcos Felipe Iparraguirre Nuñovero, Marco Antonio Hungaro Duarte, Luciana Reis Azevedo Alanis, Bruno Cavalini Cavenago, Ulisses Xavier da Silva Neto, Everdan Carneiro
International Endodontic Journal.2026; 59(5): 788. CrossRef - Does maintaining apical patency reduce early postoperative pain after root canal treatment? A randomized controlled trial in asymptomatic vital single-rooted teeth
Ozan Arda Deger, Sehnaz Yilmaz, Kübra Gürler
Clinical Oral Investigations.2026;[Epub] CrossRef - Evaluation of Postoperative Pain Frequency in Single‐Session Endodontic Treatments With Patency and Foraminal Enlargement
Viviane Barbosa Godoy, Ana Grasiela Limoeiro, Vanessa Sandini, Vini Mehta, Wayne Martins Nascimento, Marilia Fagury Videira Marceliano‐Alves, Marcos Frozoni
Clinical and Experimental Dental Research.2026;[Epub] CrossRef - Assessment of apical extrusion in regenerative endodontics: a comparative study of different irrigation methods using three-dimensional immature tooth models
Vahide Hazal Abat, Gökçen Deniz Bayrak, Mustafa Gündoğar
Odontology.2025; 113(1): 213. CrossRef - Clinical Advances in Calcium Phosphate for Maxillomandibular Bone Regeneration: From Bench to Bedside
Seyed Ali Mostafavi Moghaddam, Hamid Mojtahedi, Amirhossein Bahador, Lotfollah Kamali Hakim, Hamid Tebyaniyan
Ceramics.2025; 8(4): 129. CrossRef - Postoperative pain after single-visit root canal treatments in necrotic teeth comparing instruments’ kinematics and apical instrumentation limits – a prospective randomized multicenter clinical trial
Ricardo Machado, Guilherme Moreira, Daniel Comparin, Arthur Pimentel Barroso, Jaqueline Nascimento, Caio Cézar Randi Ferraz, Sérgio Aparecido Ignácio, Lucas da Fonseca Roberti Garcia, Rodrigo Rodrigues Amaral, David Shadid, Ulisses Xavier da Silva Neto
BMC Oral Health.2024;[Epub] CrossRef - Assessment of mechanical allodynia in healthy teeth adjacent and contralateral to endodontically diseased teeth: a clinical study
Vaishnavi Ratnakar Patankar, Ashish K Jain, Rahul D Rao, Prajakta R Rao
Restorative Dentistry & Endodontics.2024;[Epub] CrossRef - A systematic review and meta-analysis on the effects of phototherapy on postoperative pain in conventional endodontic reintervention
Larissa Pereira Nunes, Gabriel Pereira Nunes, Túlio Morandin Ferrisse, Henrico Badaoui Strazzi-Sahyon, Eloi Dezan-Júnior, Luciano Tavares Angelo Cintra, Gustavo Sivieri-Araujo
Clinical Oral Investigations.2024;[Epub] CrossRef - The effect of intracanal cryotherapy with and without foraminal enlargement on pain prevention after endodontic treatment: a randomized clinical trial
Marcos Felipe Iparraguirre Nuñovero, Marco Antonio Hungaro Duarte, André Vinícius Kaled Segato, Ulisses Xavier da Silva Neto, Vania Portela Ditzel Westphalen, Everdan Carneiro
Scientific Reports.2024;[Epub] CrossRef - Clinical determination of anatomical diameter in different dental groups correlating them with gender, age, tooth/canal and pulpoperiradicular diagnosis: an observational clinical study
Ricardo Machado, Gabriel Filipe Pamplona, Claudemir de Souza Júnior, Jaqueline Nascimento, Eduardo Donato Eing Elgelke Back, Daniel Comparin, Sérgio Aparecido Ignácio, Stella Maria Glaci Reinke, Ana Cristina Kovalik, Ulisses Xavier da Silva Neto
Scientific Reports.2023;[Epub] CrossRef - How much to enlarge? A letter to the editor
Krishnamachari Janani, Kavalipurapu Venkata Teja, Kumar Chandan Srivatsava
Saudi Endodontic Journal.2023; 13(3): 288. CrossRef - Efficiency of diode laser in control of post-endodontic pain: a randomized controlled trial
Hend H. Ismail, Maram Obeid, Ehab Hassanien
Clinical Oral Investigations.2023; 27(6): 2797. CrossRef - Periapical Healing following Root Canal Treatment Using Different Endodontic Sealers: A Systematic Review
Akshay Khandelwal, Krishnamachari Janani, KavalipurapuVenkata Teja, Jerry Jose, Gopi Battineni, Francesco Riccitiello, Alessandra Valletta, Ajitha Palanivelu, Gianrico Spagnuolo, Vincenzo Grassia
BioMed Research International.2022;[Epub] CrossRef
- Postoperative Pain After Endodontic Treatment in HIV‐Positive Patients Under HAART: A Prospective Observational Cohort Study
- 6,089 View
- 65 Download
- 11 Web of Science
- 13 Crossref

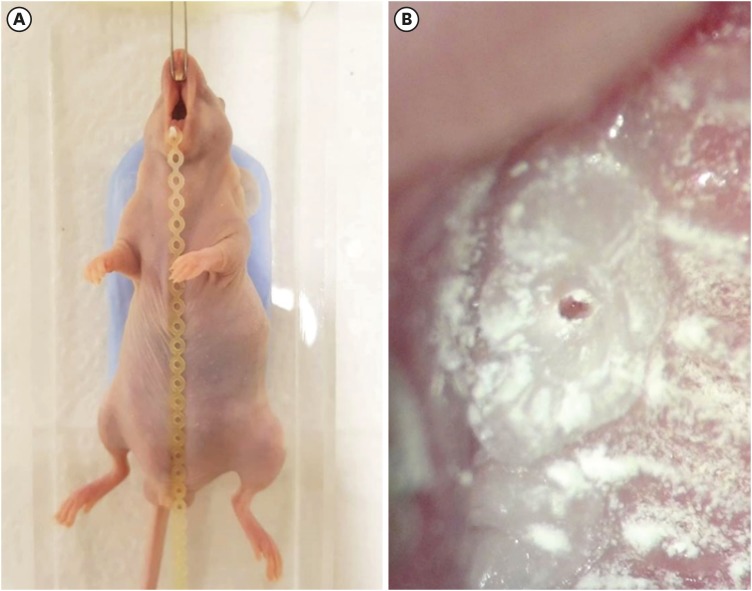
- Development of a mouse model for pulp-dentin complex regeneration research: a preliminary study
- Sunil Kim, Sukjoon Lee, Han-Sung Jung, Sun-Young Kim, Euiseong Kim
- Restor Dent Endod 2019;44(2):e20. Published online May 7, 2019
- DOI: https://doi.org/10.5395/rde.2019.44.e20
-
Abstract
PDFPubReaderePub
Objectives To achieve pulp-dentin complex regeneration with tissue engineering, treatment efficacies and safeties should be evaluated using
in vivo orthotopic transplantation in a sufficient number of animals. Mice have been a species of choice in which to study stem cell biology in mammals. However, most pulp-dentin complex regeneration studies have used large animals because the mouse tooth is too small. The purpose of this study was to demonstrate the utility of the mouse tooth as a transplantation model for pulp-dentin complex regeneration research.Materials and Methods Experiments were performed using 7-week-old male Institute of Cancer Research (ICR) mice; a total of 35 mice had their pulp exposed, and 5 mice each were sacrificed at 1, 2, 4, 7, 9, 12 and 14 days after pulp exposure. After decalcification in 5% ethylenediaminetetraacetic acid, the samples were embedded and cut with a microtome and then stained with hematoxylin and eosin. Slides were observed under a high-magnification light microscope.
Results Until 1 week postoperatively, the tissue below the pulp chamber orifice appeared normal. The remaining coronal portion of the pulp tissue was inflammatory and necrotic. After 1 week postoperatively, inflammation and necrosis were apparent in the root canals inferior to the orifices. The specimens obtained after experimental day 14 showed necrosis of all tissue in the root canals.
Conclusions This study could provide opportunities for researchers performing
in vivo orthotopic transplantation experiments with mice.-
Citations
Citations to this article as recorded by- Is dental pulp inflammation capable of causing central inflammation, behavioral, and sensory alterations? A pre-clinical study
Iago Ramirez, Igor Bassi Ferreira Petean, Francisco Wanderley Garcia de Paula-Silva, Aline Aparecida Ferraresi Tiballi, Manoel Damião Sousa-Neto, Fabiane Carneiro Lopes-Olhê, Christie Ramos Andrade Leite-Panissi, Jardel Francisco Mazzi-Chaves
Archives of Oral Biology.2025; 177: 106320. CrossRef - PRIASE 2021 guidelines for reporting animal studies in Endodontology: explanation and elaboration
V. Nagendrababu, A. Kishen, P. E. Murray, M. H. Nekoofar, J. A. P. de Figueiredo, E. Priya, J. Jayaraman, S. J. Pulikkotil, A. Jakovljevic, P. M. H. Dummer
International Endodontic Journal.2021; 54(6): 858. CrossRef
- Is dental pulp inflammation capable of causing central inflammation, behavioral, and sensory alterations? A pre-clinical study
- 2,277 View
- 13 Download
- 2 Crossref
Case Reports
- Necrosis of intact premolar caused by an adjacent apical infection: a case report
- Saeed Asgary, Laleh Alim Marvasti
- Restor Dent Endod 2013;38(2):90-92. Published online May 28, 2013
- DOI: https://doi.org/10.5395/rde.2013.38.2.90
-
Abstract
PDFPubReaderePub
Although periapical inflammatory lesions are usually resulted by infection in the root canal system, this rare case showed that a periapical lesion related to an infected tooth may cause pulpal necrosis in adjacent intact tooth, with no history or clinical signs of caries, disease, trauma or developmental anomaly. This case also suggests that the periapical lesion can be treated conservatively, without surgical intervention. Furthermore, this case highlights the importance of prompt treatment of apical periodontitis before the lesion becomes extensive as well as follows up of large lesions.
-
Citations
Citations to this article as recorded by- Accidentally Extruded Calcium Hydroxide Into a Cystic Lesion Associated With an Adjacent Tooth—A Case Report
Emmanuel Mazinis, Nikolaos Tsanidis, Vasilios Thomaidis
Clinical Case Reports.2025;[Epub] CrossRef - Atypically grown large periradicular cyst affecting adjacent teeth and leading to confounding diagnosis of non‐endodontic pathology
Domenico Ricucci, Massimiliano Amantea, Christian Girone, José F. Siqueira
Australian Endodontic Journal.2020; 46(2): 272. CrossRef
- Accidentally Extruded Calcium Hydroxide Into a Cystic Lesion Associated With an Adjacent Tooth—A Case Report
- 3,238 View
- 29 Download
- 2 Crossref
- Pulp necrosis following luxated injury to teeth in a patient with uncontrolled type II diabetes mellitus: a case report
- Haneol Shin, Seung-Jong Lee, Il-Young Jung, Chan-Young Lee
- Restor Dent Endod 2012;37(1):61-65. Published online March 2, 2012
- DOI: https://doi.org/10.5395/rde.2012.37.1.61
-
Abstract
PDFPubReaderePub
Patients with diabetes mellitus show delayed wound healing and increased susceptibility to infection. Therefore, the effects of diabetes on pulpal and periodontal healing should be taken into consideration when treating diabetic dental traumatized patients. This case presents the treatment for dental traumatized 20 yr old female with uncontrolled type II diabetes. The traumatized upper central incisors had showed pulpal healing in early days. However, 7 mon after the trauma, the teeth had been diagnosed with pulp necrosis with apical abscess. Eventually, non surgical root canal treatment on the teeth had been performed.
-
Citations
Citations to this article as recorded by- Effects of diabetes mellitus on dental pulp: A systematic review of in vivo and in vitro studies
Rafaella Milla Nunes Pimenta, Alexandre Henrique dos Reis‐Prado, Sabrina de Castro Oliveira, Juliana Goto, Leopoldo Cosme‐Silva, Luciano Tavares Angelo Cintra, Francine Benetti
Oral Diseases.2024; 30(2): 100. CrossRef
- Effects of diabetes mellitus on dental pulp: A systematic review of in vivo and in vitro studies
- 3,253 View
- 13 Download
- 1 Crossref
- Partial pulp necrosis caused by excessive orthodontic force
- Min-Young Kim, Seung-Jong Lee, Il-Young Jung, Euiseong Kim
- J Korean Acad Conserv Dent 2011;36(2):149-153. Published online March 31, 2011
- DOI: https://doi.org/10.5395/JKACD.2011.36.2.149
-
Abstract
PDFPubReaderePub
As the dental pulp is encased with a rigid, noncompliant shell, changes in pulpal blood flow or vascular tissue pressure can have serious implication for the health of pulp. Numerous studies have demonstrated that orthodontic force application may influence both blood flow and cellular metabolism, leading degenerative and/or inflammatory responses in the dental pulp. The aim of this case report is to present a case about tooth with chronic periapical abscess which showed normal vital responses. Excessive orthodontic force is thought to be the prime cause of partial pulp necrosis. Owing to remaining vital tissue, wrong dianosis can be made, and tooth falsely diagnosed as vital may be left untreated, causing the necrotic tissue to destroy the supporting tissuses. Clinician should be able to utilize various diagnostic tools for the precise diagnosis, and be aware of the endodontic-orthodontic inter-relationship.
- 2,490 View
- 41 Download
- The palato-gingival groove - anatomical anomaly occurred in maxillary lateral incisors: case reports
- Hyun-Il Kim, Young-Shin Noh, Hoon-Sang Chang, Hyun-Wook Ryu, Kyung-San Min
- J Korean Acad Conserv Dent 2007;32(6):483-490. Published online November 30, 2007
- DOI: https://doi.org/10.5395/JKACD.2007.32.6.483
-
Abstract
PDFPubReaderePub
This report describes clinical cases of a palato-gingival groove on a maxillary lateral incisor with associated localized periodontal disease and pulp necrosis. The tooth of the first case was extracted because of severe bone destruction. The palato-gingival groove of the second case was eliminated using a round bur, and the resulting defect was filled with synthetic graft and covered by an absorbable membrane. Both diagnosis and treatment of palato-gingival groove were very difficult and usually extraction of the involved tooth is the treatment of choice, but combined endodontic-periodontic treatment allowed the tooth to be saved.
-
Citations
Citations to this article as recorded by- Exploring anatomical uniqueness: A rare case report of the buccomesial groove variation in maxillary lateral incisor and its management
Shubhangi Kadoo, Pallav Mahesh Patni, Sanket Hans Pandey, Rahul Vaswani
Journal of Conservative Dentistry and Endodontics.2025; 28(4): 394. CrossRef - Radicular lingual groove: A contributory factor in periodontal pathology
Gaurav Didhra, Jagjit Singh, Rajan Gupta, Parveen Dahiya
Archives of Medicine and Health Sciences.2019; 7(2): 240. CrossRef - Management of a Palatal Gingival Groove in a Maxillary Lateral Incisor: A Case Report
Ashkan Salari, Maosumeh Faramarzi, Seyedeh Fereshteh Naser alavi
Journal of Periodontology & Implant Dentistry.2016; 7(2): 66. CrossRef - Endodontic treatment of maxillary lateral incisors with anatomical variations
Moon-Hwan Lee, Jung-Hong Ha, Myoung-Uk Jin, Young-Kyung Kim, Sung-Kyo Kim
Restorative Dentistry & Endodontics.2013; 38(4): 253. CrossRef
- Exploring anatomical uniqueness: A rare case report of the buccomesial groove variation in maxillary lateral incisor and its management
- 2,267 View
- 5 Download
- 4 Crossref
 First
First Prev
Prev

