
Search
- Page Path
- HOME > Search
Research Articles
- Comparison of remineralization in caries-affected dentin using calcium silicate, glass ionomer cement, and resin-modified glass ionomer cement: an in vitro study
- Kwanchanok Youcharoen, Onwara Akkaratham, Papichaya Intajak, Pipop Saikaew, Sirichan Chiaraputt
- Restor Dent Endod 2025;50(4):e37. Published online November 14, 2025
- DOI: https://doi.org/10.5395/rde.2025.50.e37
-
 Abstract
Abstract
 PDF
PDF PubReader
PubReader ePub
ePub - Objectives
This study evaluated the ability of calcium silicate cement (CSC) as a remineralizing agent compared with conventional glass ionomer cement (GIC) and resin-modified GIC (RMGIC) to remineralize artificial caries-affected dentin.
Methods
Twenty-five class V cavities were prepared on extracted human third molars. Twenty teeth underwent artificial caries induction. The remaining five teeth with sound dentin serve as the positive control. The twenty demineralized teeth were subdivided into four groups (n = 5): carious dentin without restoration (negative control [NC]), carious dentin restored with CSC (Biodentine, Septodont), carious dentin restored with GI (Fuji IX, GC Corporation), and carious dentin restored with RMGIC (Fuji II LC, GC Corporation). Following restoration, the specimens were stored in artificial saliva for 7 days. The elastic modulus was evaluated by a nanoindentation test. The mineral composition was analyzed by scanning electron microscopy-energy-dispersive X-ray spectroscopy (SEM-EDX), and the mineral composition at the dentin-material interface.
Results
CSC had a higher modulus of elasticity compared to GI, RMGI, and NC groups (p < 0.05). Higher calcium and phosphorus content was observed under CSC restorations, as indicated by SEM-EDX examination, which may lead to better remineralization.
Conclusions
Compared to GI and RMGI, CSC showed the best remineralization and mechanical reinforcement in caries-affected dentin, indicating CSC for use in minimally invasive restorative dentistry. -
Citations
Citations to this article as recorded by
- Comparison of mineral precipitation, elemental release, pH change and cytotoxicity of calcium-silicate cements and an experimental resin-modified glass ionomer cement containing bioactive glass
Wisitsin Potiprapanpong , Parichart Naruphontjirakul, Naruporn Monmaturapoj, Siriporn Tanodekaew, Somruethai Channasanon, Arnit Toneluck, Somying Patntirapong, Piyaphong Panpisut
Biomaterial Investigations in Dentistry.2026; 13: 337. CrossRef
- Comparison of mineral precipitation, elemental release, pH change and cytotoxicity of calcium-silicate cements and an experimental resin-modified glass ionomer cement containing bioactive glass
- 3,040 View
- 272 Download
- 1 Crossref

- Stress distribution of restorations in external cervical root resorption under occlusal and traumatic loads: a finite element analysis
- Padmapriya Ramanujam, Paul Kevin Abishek Karthikeyan, Vignesh Srinivasan, Selvakarthikeyan Ulaganathan, Velmurugan Natanasabapathy, Nandini Suresh
- Restor Dent Endod 2025;50(2):e21. Published online May 21, 2025
- DOI: https://doi.org/10.5395/rde.2025.50.e21
-
Abstract
PDFPubReaderePub
- Objectives
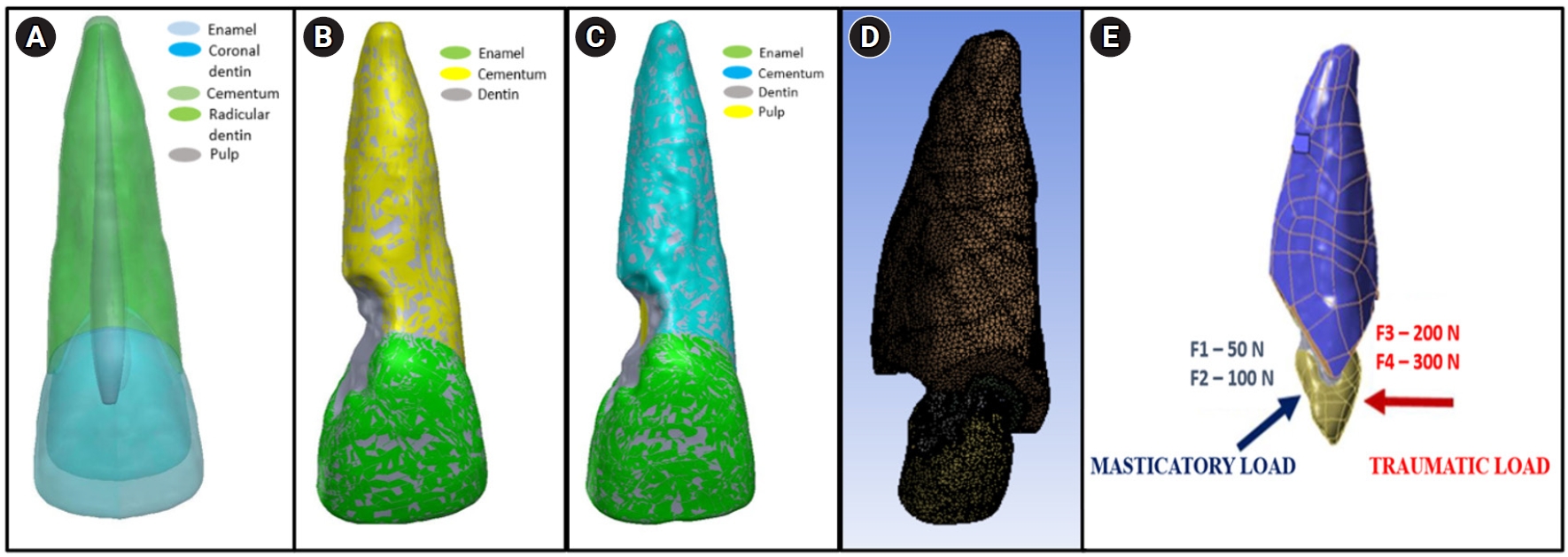
This study analyzed the stress distribution in a maxillary central incisor with external cervical resorptive defect restored with different restorative materials under normal masticatory and traumatic loading conditions using finite element analysis.
Methods
Cone-beam computed tomography of an extracted intact incisor and created resorptive models (Patel’s 3D classification-2Bd and 2Bp) in the maxillary central incisor was performed for finite element models. The 2Bd models were restored either with glass ionomer cement (GIC)/Biodentine (Septodont) or a combination of both with composite resin. 2Bp models were restored externally with a combination technique and internally with root canal treatment. The other model was external restoration with GIC and internal with fiber post. Two masticatory loads were applied at 45˚ to the palatal aspect, and two traumatic loads were applied at 90˚ to the buccal aspect. Maximum von Mises stresses were calculated, and stress distribution patterns were studied.
Results
In 2Bd models, all restorative strategies decreased stress considerably, similar to the control model under all loads. In 2Bp models, the dentin component showed maximum stress at the deepest portion of the resorptive defect, which transfers into the adjacent pulp space. In 2Bp defects, a multilayered restoration externally and root canal treatment internally provides better stress distribution compared to the placement of a fiber post.
Conclusions
Increase in load, proportionally increased von Mises stress, despite the direction or angulation of the load. Multilayered restoration is preferred for 2Bd defects, and using an internal approach of root canal treatment is suggested to restore 2Bp defects.
- 2,953 View
- 168 Download
- Effect of surface treatment on glass ionomers in sandwich restorations: a systematic review and meta-analysis of laboratory studies
- Hoda S. Ismail, Ashraf Ibrahim Ali, Franklin Garcia-Godoy
- Restor Dent Endod 2025;50(2):e13. Published online April 16, 2025
- DOI: https://doi.org/10.5395/rde.2025.50.e13
-
Abstract
PDFPubReaderePub
- Objectives
This study aimed to evaluate the effect of different surface treatments on the bond strength between new or aged glass ionomers (GI) and resin composites in sandwich restorations.
Methods
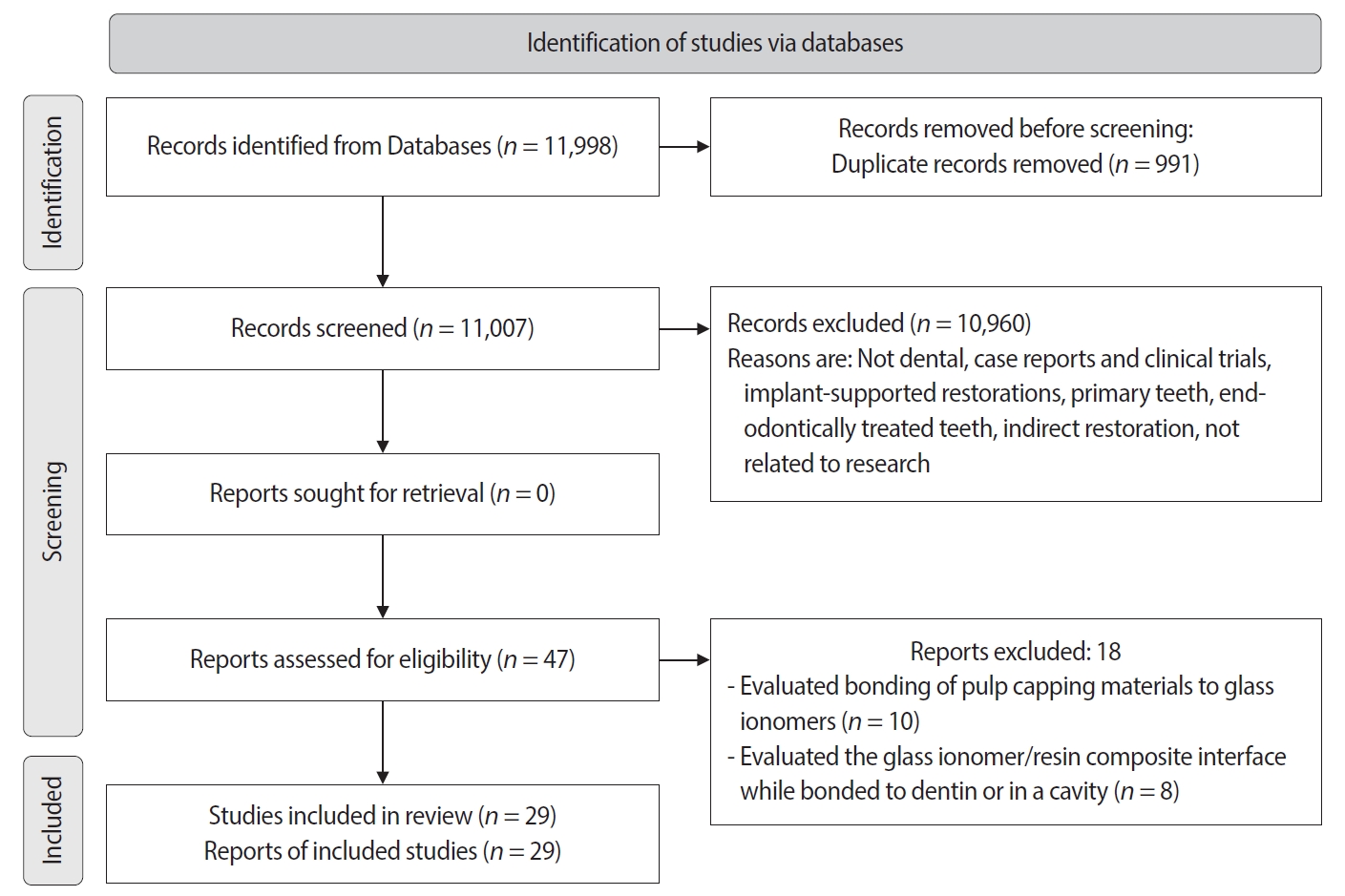
A comprehensive search was conducted in three databases to identify studies focusing on the bond strength of new or aged GIs and resin composites in laboratory settings. The selected studies were assessed for potential biases based on predetermined criteria. Additionally, a meta-analysis was performed using three studies.
Results
A total of 29 studies were included, with 24 investigating the bond strength of new GIs and five focusing on GI repair. Three studies were included in the meta-analysis (with a 95% confidence interval) which revealed no significant difference in the mean MPa values of resin-modified glass ionomer (RMGI) treated with phosphoric acid or Er,Cr:YSGG laser before the application of an etch-and-rinse adhesive. Surface treatment was found to be crucial for achieving optimal bonding between GI and resin composite, regardless of the GI’s condition.
Conclusions
The combination of mechanical and chemical surface treatments does not significantly affect the bond strength between new RMGI and composite. However, for GI repair, it is recommended to use both treatments to enhance the bond strength. -
Citations
Citations to this article as recorded by- The impact of alloy treatment on the dynamic cyclic fatigue resistance of triangular base cross-section NiTi endodontic instruments
Rashid El Abed, Amre R. Atmeh, Mohamed Jamal, Anas Al Jadaa, Hamza El-Faraj, Abdel Rahman Bani Amer, Taher Al Omari
Odontology.2026; 114(3): 1665. CrossRef - Biological Performance of Modified Glass Ionomer Cement: Antibacterial Activity, Cytocompatibility, and Rabbit Pulpal Response
Krittee Dejyong, Saowakon Indoung, Peerapon Sornying, Sareepah Manmoo, Nattapon Rotpenpian
International Dental Journal.2026; 76(3): 109491. CrossRef
- The impact of alloy treatment on the dynamic cyclic fatigue resistance of triangular base cross-section NiTi endodontic instruments
- 10,129 View
- 253 Download
- 1 Web of Science
- 2 Crossref
Review Article
- Comparative evaluation of the biological response of conventional and resin modified glass ionomer cement on human cells: a systematic review
- Shishir Singh, Gaurav Kulkarni, R S Mohan Kumar, Romi Jain, Ameya M Lokhande, Teena K Sitlaney, Musharraf H F Ansari, Navin S Agarwal
- Restor Dent Endod 2024;49(4):e41. Published online November 1, 2024
- DOI: https://doi.org/10.5395/rde.2024.49.e41
-
Abstract
PDFPubReaderePub
This review aimed to evaluate and compare the biological response (biocompatibility and cytotoxicity) of resin modified glass ionomer cement (RMGIC) in contrast to conventional glass ionomer cement (GIC) on human cells. Articles reporting parallel and split-mouth clinical trials, randomized controlled trials, non-randomized controlled trials, prospective studies, and
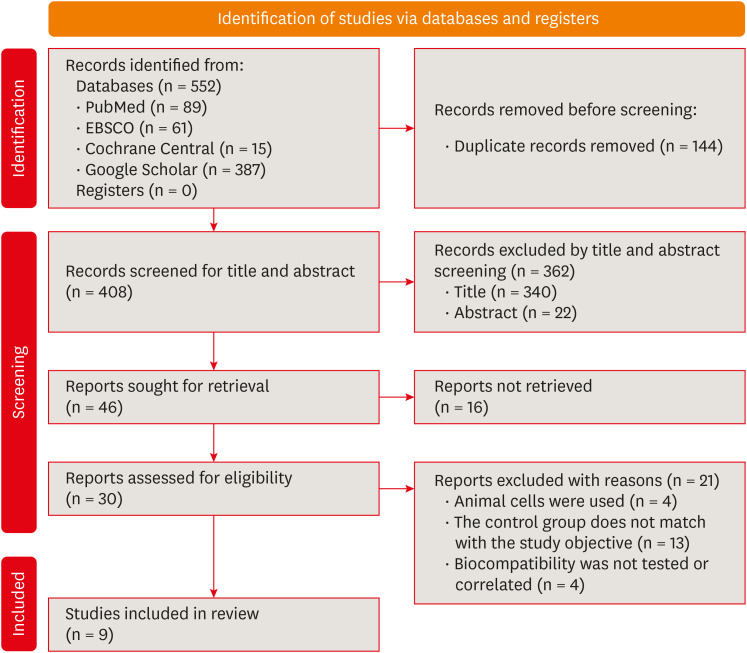
in vitro studies on human permanent teeth that assessed the biological response of GIC and RMGIC were included. The following electronic bibliographic databases were searched using the keywords: MEDLINE/PubMed, EBSCO, Cochrane Central Register of Controlled Trials, and Google Scholar. For the risk of bias MINORS tool and the modified scale of Animal Research: Reporting ofIn Vivo Experiments and Consolidated Standards of Reporting Trials were used. Initial screening identified 552 studies, of which 9 articles met the inclusion criteria and were included in the study. Different parameters such as odontoblastic changes, inflammatory response, tertiary dentin formation, presence of microorganisms, morphological changes, cell viability, number, and metabolism were used to evaluate the biological response of conventional GIC and RMGICs. Conventional GIC shows lower cytotoxicity compared to RMGIC in vital pulp therapy procedures. Further,in vivo studies and long-term clinical trials are needed to compare these observations for pulp therapy using the 2 test materials.Trial Registration PROSPERO Identifier:
CRD42023426021 -
Citations
Citations to this article as recorded by- Thermal Aging-Induced Alterations in Surface and Interface Topography of Bio-Interactive Dental Restorative Materials Assessed by 3D Non-Contact Profilometry
Zehra Güner, Gökçe Keçeci, Sadık Olguner, Hakan Çandar, Ayşenur Güngör Borsöken, Lezize Sebnem Turkun
Coatings.2026; 16(1): 53. CrossRef - Gümüş Nanopartikülle Modifiye Edilmiş Geleneksel Cam İyonomer Simanların Antimikrobiyal Etkinliği: Sistematik Derleme
Feyza Nur Altan, Zeynep Aslı Güçlü
Sağlık Bilimleri Dergisi.2026; 35(1): 190. CrossRef - Surface Roughness and Color Stability of Conventional Glass Ionomer Cement Reinforced With a Nanofiller Synthesized by the Coprecipitation Method
Neven S. Aref, Kaliannan Durairaj
International Journal of Biomaterials.2026;[Epub] CrossRef - Cytotoxicity of hexagonal boron nitride incorporated conventional and resin modified glass ionomer cements: in vitro study
Songul Kilic, Sema Yazici Akbiyik, Demet Kacaroglu
BMC Oral Health.2026;[Epub] CrossRef - Potential of Nano-Gum Arabic on the Physical, Mechanical, Adhesive, Optical, and Biological Performance of Glass Ionomer Cement: A Comprehensive In Vitro Study
Marwa Beleidy, Soha A. Hassan, Rania Rashad Omar Taha, Yousra Nashaat, Yasmine Alaa El-din
BMC Oral Health.2026;[Epub] CrossRef - Advanced Platelet-Rich Fibrin Plus Sealed Exclusively with Glass Ionomer Cement: Setting a New Standard for Healing, Aesthetics and Predictive Modelling in Regenerative Endodontics
Dubravka Turjanski, Dragutin Lisjak, Petra Bučević Sojčić, Jelena Valpotić, Tea Borojević Renić, Kristina Goršeta, Domagoj Glavina
Materials.2025; 18(18): 4421. CrossRef - The conventional glass ionomers – A forgotten paradigm
Shishir Singh
Journal of Conservative Dentistry and Endodontics.2024; 27(12): 1201. CrossRef
- Thermal Aging-Induced Alterations in Surface and Interface Topography of Bio-Interactive Dental Restorative Materials Assessed by 3D Non-Contact Profilometry
- 6,458 View
- 204 Download
- 5 Web of Science
- 7 Crossref
Research Articles
- Physical-mechanical, chemical and biological properties of graphene-reinforced glass ionomer cements
- Tatiane Ramos dos Santos Jordão, Laura Soares Viana Fernandes, Karla Lorene de França Leite, Adílis Alexandria, Emmanuel João Nogueira Leal Silva, Lucianne Cople Maia, Tatiana Kelly da Silva Fidalgo
- Restor Dent Endod 2024;49(4):e37. Published online October 10, 2024
- DOI: https://doi.org/10.5395/rde.2024.49.e37
-
Abstract
PDFPubReaderePub
Objectives This study aimed to evaluate the physical-mechanical, chemical, and biological properties of graphene-reinforced glass ionomer cements (GICs).
Materials and Methods Different proportions of graphene powder were incorporated into 2 high-viscosity self-curing GIC, Ketac Molar (GKetac) and Fuji IX (GFuji), in 4 different concentrations: 0.5%, 1%, 2%, and 5%. The control groups included the GICs without graphene. Experiments were performed to analyze linear (Ra) and volumetric roughness (Sa), antimicrobial activity, radiopacity, fluoride release, microhardness, solubility, and water sorption. Data were analyzed using Kruskal-Wallis, Mann-Whitney, Wilcoxon, analysis of variance, and Tukey’s test (
p ≤ 0.05).Results The GKetac 0% and GFuji0% groups presented higher Ra (4.05 and 2.72) and Sa (4.76 and 5.16), respectively. No inhibition zone was observed, and the incorporation of graphene reduced radiopacity. Moreover, there was no influence on the solubility and water sorption after 21 days. A greater fluoride release was observed in the period of 7 days for most of the groups. After 21 days, GKetac 5%, 2%, and 1% presented higher releasing than 0% and 0.5% (
p ≤ 0.05).Conclusions The graphene incorporation improved the microhardness of GICs in lower concentrations. Graphene incorporation to GICs modified some physical-mechanical, and chemical, but not affected biological properties.
-
Citations
Citations to this article as recorded by- Laboratory-based additive modifications in glass ionomer cements: A scoping review using a systematic data mining and trend analysis framework (2015-2024)
Kenta Tsuchiya, Sharanbir K Sidhu, Salvatore Sauro, Jukka P. Matinlinna, Hidehiko Sano, Monica Yamauti, Shuhei Hoshika, James Kit Hon Tsoi, Atsushi Tomokiyo
Journal of Dentistry.2026; 166: 106349. CrossRef - Physicomechanical and Antibacterial Properties of Resin-Based Dental Sealants Modified with Graphene Oxide Nanoparticles
Ploypim Kraisintu, Suparaksa Yamockul, Tool Sriamporn, Niyom Thamrongananskul, Awiruth Klaisiri, Theerapat Chanamuangkon, Somphob Thompho, Thanchanok Suriyapongprapai, Guang Hong
European Journal of Dentistry.2026;[Epub] CrossRef - Influence of expanded graphene on physical and chemical properties, and in vitro toxicity of glass ionomer cements for luting
Sarah Pereira Martins, Carolina Mara Geraldino Monteiro, Renan Rocha Da Silva, Andrea Vaz Braga Pintor, Marcela Baraúna Magno, Maria Augusta Visconti, Maria Teresa Villela Romanos, Livia Rodrigues De Menezes, Lucianne Cople Maia, Matheus Melo Pithon
Biomaterial Investigations in Dentistry.2026; 13: 440. CrossRef - Graphene Oxide Incorporation Enhances Biocompatibility and Surface Stability of Conventional Glass Ionomer Cements
Mayara Silva de Santana, Lucas dos Santos Silva, Joicy Cortez de Sá Sousa, Thalita Santana Conceição, Barbara Emanoele Costa Oliveira, Ceci Nunes Carvalho, Edilausson Moreno Carvalho, Luís Cláudio Nascimento da Silva
Pesquisa Brasileira em Odontopediatria e Clínica Integrada.2026;[Epub] CrossRef - Impact of graphene incorporation on the mechanical and optical properties of glass ionomer cements
Sarah Pereira Martins, Carolina Mara Geraldino Monteiro, Kenderson Santos Silva, Renan Rocha da Silva, Cássia Almeida Brito, Lívia Rodrigues de Menezes, Lucianne Cople Maia, Matheus Melo Pithon
Brazilian Journal of Oral Sciences.2026; 25: e269444. CrossRef - Potential of Nano-Gum Arabic on the Physical, Mechanical, Adhesive, Optical, and Biological Performance of Glass Ionomer Cement: A Comprehensive In Vitro Study
Marwa Beleidy, Soha A. Hassan, Rania Rashad Omar Taha, Yousra Nashaat, Yasmine Alaa El-din
BMC Oral Health.2026;[Epub] CrossRef
- Laboratory-based additive modifications in glass ionomer cements: A scoping review using a systematic data mining and trend analysis framework (2015-2024)
- 4,027 View
- 198 Download
- 5 Web of Science
- 6 Crossref
- The clinical success of ART restorations and Hall technique in primary molars: a randomized 18-month follow-up study
- Esra Oz, Zuhal Kırzıoglu, Canan Kale
- Restor Dent Endod 2023;48(2):e19. Published online May 1, 2023
- DOI: https://doi.org/10.5395/rde.2023.48.e19
-
Abstract
PDFPubReaderePub
Objectives The aim of the study was to evaluate the clinical and radiographic success of the Hall technique (HT) and atraumatic restorative treatment (ART) restorations using high-viscosity glass-ionomer cement for the management of occlusal carious lesions in primary molars.
Materials and Methods This randomized clinical study observed 40 children (aged 5–6 years). For each child, one tooth was treated with HT and one with ART. The primary outcome measures for HT restorations were successful, minor, and major failure rates. Clinical evaluations of ART restorations were performed according to the modified United States Public Health Service criteria during 18-month follow-up. McNemar test was used for statistical analysis.
Results Thirty of 40 (75%) participants returned for 18 months of follow-up. In the clinical evaluations of teeth that were treated with HT, the patients did not have complaints of pain or other symptoms, all crowns remained in the oral cavity, the gums were healthy, and the teeth were functional in all evaluations. At the end of the 18-month follow-up, the surface texture and marginal integrity criteria of ART restorations were recorded as 26.7% and 33.3%, respectively. In the radiographic evaluation of 30 patients treated with ART and HT, all restorations were considered successful.
Conclusions The 18-month clinical and radiographic results after treatments applied to single-surface cavities in anxious children showed that both treatment methods were successful.
-
Citations
Citations to this article as recorded by- Two-year outcomes of hall technique and modified hall technique in deep carious lesions of primary molars: a randomized clinical trial
Sumeyye Konukman Turker, Ayse Isil Cihan
BMC Oral Health.2026;[Epub] CrossRef - Clinical Performance of High-Viscosity Glass Hybrid Restorative Systems in Posterior Teeth: A Scoping Review
Antonia Theodora Vrabie, Tinela Panaite, Bogdan Radu Dragomir, Simona Stoleriu, Angela Ghiorghe, Irina Nica, Alice Murariu, Sorin Andrian, Gianina Iovan
Prosthesis.2026; 8(7): 71. CrossRef - Success rate of Hall Technique for restoring carious primary molars - systematic review and meta-analysis
Tamara Kerber Tedesco, Nicola Patricia Innes, Claudia Lopez Gallegos, Gabriela Seabra Silva, Thais Gimenez, Mariana Minatel Braga, Mariana Pinheiro Araujo, Jayakumar Jayaraman, Waraf Al-yaseen, Daniela Prócida Raggio
Evidence-Based Dentistry.2025; 26(1): 65. CrossRef - Effectiveness of Dental Restorative Materials in the Atraumatic Treatment of Carious Primary Teeth in Pediatric Dentistry: A Systematic Review
Gianna Dipalma, Angelo Michele Inchingolo, Lucia Casamassima, Paola Nardelli, Danilo Ciccarese, Paolo De Sena, Francesco Inchingolo, Andrea Palermo, Marco Severino, Cinzia Maria Norma Maspero, Alessio Danilo Inchingolo
Children.2025; 12(4): 511. CrossRef - Clinical, radiographic, and microhardness evaluation of caries in primary molars managed with modified Hall technique
Eman El Sayed El Bedewy, Nahed A.A. Abohamila, Shereen A. M. Ali, Shimaa M.M. Hadwa
Tanta Dental Journal.2025; 22(1): 133. CrossRef - Pain Perception During Minimally Invasive Caries Removal in Children: A Randomized Clinical Trial Comparing Chemo-Mechanical Caries Removal
Dhirja Goel, Neha Awasthi, Yanina Singh, Sukhdeep Singh, Nenung Yirang
Journal of International Society of Preventive and Community Dentistry.2025; 15(4): 348. CrossRef - Clinical and histological evaluation of hall technique with and without silver diamine fluoride in the treatment of carious primary molars
Marwa M.A.Z. Abd-Elhaleium, Fatma A.-A. El-Hendawy, Lamis A. El-Ghareb, Sara Y. AboAli
Tanta Dental Journal.2025; 22(2): 351. CrossRef - Comparative success of minimally invasive treatments for cavitated caries in primary teeth: a network meta-analysis
Rasoul Sahebalam, Mahsa Ghorbani, Alireza Sarraf Shirazi, Motahareh Khosrojerdi, Mana Mowji
BMC Oral Health.2025;[Epub] CrossRef
- Two-year outcomes of hall technique and modified hall technique in deep carious lesions of primary molars: a randomized clinical trial
- 8,089 View
- 146 Download
- 6 Web of Science
- 8 Crossref
- Porosity and pore size distribution in high-viscosity and conventional glass ionomer cements: a micro-computed tomography study
- Aline Borburema Neves, Laísa Inara Gracindo Lopes, Tamiris Gomes Bergstrom, Aline Saddock Sá da Silva, Ricardo Tadeu Lopes, Aline de Almeida Neves
- Restor Dent Endod 2021;46(4):e57. Published online October 29, 2021
- DOI: https://doi.org/10.5395/rde.2021.46.e57

-
Abstract
PDFPubReaderePub
Objectives This study aimed to compare and evaluate the porosity and pore size distribution of high-viscosity glass ionomer cements (HVGICs) and conventional glass ionomer cements (GICs) using micro-computed tomography (micro-CT).
Materials and Methods Forty cylindrical specimens (
n = 10) were produced in standardized molds using HVGICs and conventional GICs (Ketac Molar Easymix, Vitro Molar, MaxxionR, and Riva Self-Cure). The specimens were prepared according to ISO 9917-1 standards, scanned in a high-energy micro-CT device, and reconstructed using specific parameters. After reconstruction, segmentation procedures, and image analysis, total porosity and pore size distribution were obtained for specimens in each group. After checking the normality of the data distribution, the Kruskal-Wallis test followed by the Student-Newman-Keuls test was used to detect differences in porosity among the experimental groups with a 5% significance level.Results Ketac Molar Easymix showed statistically significantly lower total porosity (0.15%) than MaxxionR (0.62%), Riva (0.42%), and Vitro Molar (0.57%). The pore size in all experimental cements was within the small-size range (< 0.01 mm3), but Vitro Molar showed statistically significantly more pores/defects with a larger size (> 0.01 mm3).
Conclusions Major differences in porosity and pore size were identified among the evaluated GICs. Among these, the Ketac Molar Easymix HVGIC showed the lowest porosity and void size.
-
Citations
Citations to this article as recorded by- The effect of contouring instruments on immediate quality and porosity of direct restorations
Carlos Soler-Tornero, Pekka Toivonen, Jaakko Suorsa, Sakari S. Karhula, Simo Saarakkala, Vuokko Anttonen, Jukka Leinonen
Clinical Oral Investigations.2025;[Epub] CrossRef - Impact of spacers and thermocycling on porosity and gaps in class II endodontic temporary restorations evaluated by microcomputed tomography
Fahda N. Algahtani, Manal Alkadi, Hiba R. Talic, Sarah S. AlShalawi, Lujain M. Alqarni, Reem M. Barakat, Rasha Haridy, Sara M. ElKhateeb, Rahaf A. Almohareb
Scientific Reports.2025;[Epub] CrossRef - Influence of Human Blood Contamination on Microhardness of Glass-Ionomer Cements and Glass-Hybrid Material
Katarina Franić, Ana Brundić, Jurica Matijević, Ana Ivanišević, Ivana Miletić, Anja Baraba
Materials.2025; 18(17): 4075. CrossRef - Effect of crown seating methods on the remnant cement in the subgingival region of a cement-retained implant crown
Fanghui Ji, Ji Suk Shim, Jeongyol Lee, Hwiseong Oh, Jae Jun Ryu
Scientific Reports.2024;[Epub] CrossRef - Enhancing Wear Resistance in Glass Ionomer Cement through Green-mediated Chitosan-, Titanium-, Zirconium-, and Hydroxyapatite-based Nanocomposites: An Analysis before and after Chewing Simulator Endurance
Srinavasa Surya Sitaram, Jessy Paulraj, Subhabrata Maiti, Rajeshkumar Shanmugam
International Journal of Clinical Pediatric Dentistry.2024; 17(11): 1229. CrossRef - The effect of mesoporous silica doped with silver nanoparticles on glass ionomer cements; physiochemical, mechanical and ion release analysis
Syed Saad Bin Qasim, Ali Bmuajdad
BMC Oral Health.2024;[Epub] CrossRef - Hyperbaric Pressure Effect on Dental Luting Cements
Secil OZKAN ATA, Nazım ATA, Rıfat UGURLUTAN
Journal of Basic and Clinical Health Sciences.2023; 7(1): 464. CrossRef - In Vitro Comparison of Differences in Setting Time of Premixed Calcium Silicate-Based Mineral Trioxide Aggregate According to Moisture Content of Gypsum
Hyun-Jin Kim, Jun-Seok Lee, Dong-Hoon Gwak, Yong-Seok Ko, Chun-Il Lim, Seung-Youl Lee
Materials.2023; 17(1): 35. CrossRef - Adhesion and Surface Roughness of Apatite-Containing Carbomer and Improved Ionically Bioactive Resin Compared to Glass Ionomers
Handan Yıldırım Işık, Aylin Çilingir
Journal of Functional Biomaterials.2023; 14(7): 367. CrossRef - An influence of finishing procedures and protective coating on the ultrastructure of conventional and hybrid glass ionomer cement restorations
Antonije Stankovic, Jelena Popovic, Marija Nikolic, Aleksandar Mitic, Nenad Stosic, Radomir Barac, Aleksandra Milovanovic
Stomatoloski glasnik Srbije.2023; 70(3): 138. CrossRef - Effect of aging on mechanical and antibacterial properties of fluorinated graphene reinforced glass ionomer: In vitro study
Suzan Khaled Arafa, Dalia Ibrahim Sherief, Mohamed Salah Nassif
Journal of the Mechanical Behavior of Biomedical Materials.2023; 142: 105803. CrossRef
- The effect of contouring instruments on immediate quality and porosity of direct restorations
- 3,521 View
- 22 Download
- 8 Web of Science
- 11 Crossref
- Bonding of a resin-modified glass ionomer cement to dentin using universal adhesives
- Muhittin Ugurlu
- Restor Dent Endod 2020;45(3):e36. Published online June 15, 2020
- DOI: https://doi.org/10.5395/rde.2020.45.e36
-
Abstract
PDFPubReaderePub
Objectives This study aims to assess the effect of universal adhesives pretreatment on the bond strength of resin-modified glass ionomer cement to dentin.
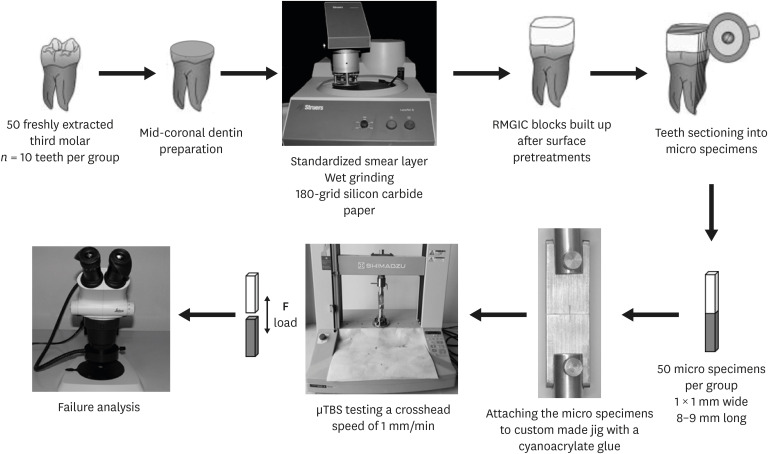
Materials and Methods Fifty caries-free human third molars were employed. The teeth were randomly assigned into five groups (
n = 10) based on dentin surface pretreatments: Single Bond Universal (3M Oral Care), Gluma Bond Universal (Heraeus Kulzer), Prime&Bond Elect (Dentsply), Cavity Conditioner (GC) and control (no surface treatment). After Fuji II LC (GC) was bonded to the dentin surfaces, the specimens were stored for 7 days at 37°C. The specimens were segmented into microspecimens, and the microspecimens were subjugated to microtensile bond strength testing (1.0 mm/min). The modes of failure analyzed using a stereomicroscope and scanning electron microscopy. Data were statistically analyzed with one-way analysis of variance and Duncan tests (p = 0.05).Results The surface pretreatments with the universal adhesives and conditioner increased the bond strength of Fuji II LC to dentin (
p < 0.05). Single Bond Universal and Gluma Bond Universal provided higher bond strength to Fuji II LC than Cavity Conditioner (p < 0.05). The bond strengths obtained from Prime&Bond Elect and Cavity Conditioner were not statistically different (p > 0.05).Conclusions The universal adhesives and polyacrylic acid conditioner could increase the bond strength of resin-modified glass ionomer cement (RMGIC) to dentin. The use of universal adhesives before the application of RMGIC may be more beneficial in improving bond strength.
-
Citations
Citations to this article as recorded by- Bioactive restorative materials in dentistry: a comprehensive review of mechanisms, clinical applications, and future directions
Dina Abozaid, Amr Azab, Mohammad A. Bahnsawy, Mohamed Eldebawy, Abdullah Ayad, Romesa soomro, Enas Elwakeel, Maged Ahmed Mohamed
Odontology.2026; 114(2): 349. CrossRef - Impact of nanochitosan incorporation on the performance of resin-modified glass ionomer luting cement: a comprehensive in vitro study
Mostafa A. Abdelshafi, Nesma Elgohary, Ahmed Shams
BMC Oral Health.2026;[Epub] CrossRef - Coronal cavity pretreatment agents and restoration protocols effect on microleakage of endodontically treated teeth
Lena Bal, Cangül Keskin, Aybüke Karaca Sakallı, Osman Fatih Aydın
Journal of Medicine and Palliative Care.2026; 7(1): 40. CrossRef - Comparative evaluation of effect of natural collagen cross-linker and silver diamine fluoride pre-treatment before resin-modified glass ionomer cement restoration on dentin of primary teeth: An in vitro study
Mrunal Pawar, N. D. Shashikiran, Sachin Chandrashekar Gugwad, Namrata Gaonkar, Savita Hadakar, Pali Nikose, Sonali Kisan Waghmode, Ankita Maurya
Journal of Indian Society of Pedodontics and Preventive Dentistry.2026; 44(1): 132. CrossRef - Contemporary biomimetic and bioactive materials in paediatric dentistry: a narrative review
Melis Ünsal-Çalışkaner, Aydın Emre Lermi
The Saudi Dental Journal.2026;[Epub] CrossRef - An In Vitro Evaluation of the Effect of Nanoparticle Graphene Oxide on Compressive Strength of Conventional and Resin-Modified Glass Ionomer Cements (GICs)
Arushi Dhole, Neha Jaju, Sneha Rathaur, Pankaj Kumar Gupta, Shrenika Lall, Somraj Podder
Cureus.2026;[Epub] CrossRef - Clinical evaluation of giomer-based injectable resin composite versus resin-modified glass ionomer in class V carious lesions over 18 months: A randomized clinical trial
Reham Hendam, Rania Mosallam, Dina Kamal
Journal of Conservative Dentistry and Endodontics.2025; 28(1): 50. CrossRef - Push-Out Bond Strength of Different Luting Cements Following Post Space Irrigation with 2% Chitosan: An In Vitro Study
Shimaa Rifaat, Ahmed Rahoma, Hind Muneer Alharbi, Sawsan Jamal Kazim, Shrouq Ali Aljuaid, Basmah Omar Alakloby, Faraz A. Farooqi, Noha Taymour
Prosthesis.2025; 7(1): 18. CrossRef - A Comparative Evaluation of Marginal Leakage and Shear Bond Strength of Cention N, Resin-Modified Glass Ionomer Cement (RMGIC), and Conventional Glass Ionomer Cement (GIC): An In Vitro Study
Khushboo Singh, Debapriya Pradhan, Saurabh Tiwari, Raksha Thakur, Priyamvada Sharma, Devika Agrawal, Mahima Singh, Devshree Jawalikar, Delphina Michael Kapoor, Jyoti Priiya Kodimela
Cureus.2025;[Epub] CrossRef - Assessment of Nanosilver Fluoride Application on the Microtensile Bond Strength of Glass Ionomer Cement and Resin-modified Glass Ionomer Cement on Primary Carious Dentin: An In Vitro Study
Anushka Das, Neeraja Ramamurthy, Ila Srinivasan, Yuthi Milit
International Journal of Clinical Pediatric Dentistry.2024; 17(5): 565. CrossRef - Effect of Surface Treatments on Shear-bond Strength of Glass Ionomer Cements to Silver Diamine Fluoride-treated Simulated Carious Dentin
WT Koh, OT Yeoh, NA Yahya, AU Yap
Operative Dentistry.2024; 49(6): 714. CrossRef - Desensitizing agents’ post-bleaching effect on orthodontic bracket bond strength
Gufa Bagus Pamungkas, Dyah Karunia, Sri Suparwitri
Dental Journal.2024; 57(1): 45. CrossRef - Successful Rehabilitation of Traumatized Immature Teeth by Different Vital Pulp Therapies in Pediatric Patients
Mohammad Kamran Khan
Journal of the Scientific Society.2023; 50(1): 111. CrossRef - Do bioactive materials show greater retention rates in restoring permanent teeth than non-bioactive materials? A systematic review and network meta-analysis of randomized controlled trials
Juliana Benace Fernandes, Sheila Mondragón Contreras, Manuela da Silva Spinola, Graziela Ribeiro Batista, Eduardo Bresciani, Taciana Marco Ferraz Caneppele
Clinical Oral Investigations.2023;[Epub] CrossRef - Effects of tooth preparation on the microleakage of fissure sealant
Gesti Kartiko Sari, Sri Kuswandari, Putri Kusuma Wardani Mahendra
Dental Journal (Majalah Kedokteran Gigi).2022; 55(2): 67. CrossRef - Rheological Properties, Surface Microhardness, and Dentin Shear Bond Strength of Resin-Modified Glass Ionomer Cements Containing Methacrylate-Functionalized Polyacids and Spherical Pre-Reacted Glass Fillers
Whithipa Thepveera, Wisitsin Potiprapanpong, Arnit Toneluck, Somruethai Channasanon, Chutikarn Khamsuk, Naruporn Monmaturapoj, Siriporn Tanodekaew, Piyaphong Panpisut
Journal of Functional Biomaterials.2021; 12(3): 42. CrossRef
- Bioactive restorative materials in dentistry: a comprehensive review of mechanisms, clinical applications, and future directions
- 5,926 View
- 49 Download
- 16 Crossref
- Comparative assessment of antibacterial activity of different glass ionomer cements on cariogenic bacteria
- Rahul Gaybarao Naik, Arun Suresh Dodamani, Mahesh Ravindra Khairnar, Harish Chaitram Jadhav, Manjiri Abhay Deshmukh
- Restor Dent Endod 2016;41(4):278-282. Published online September 20, 2016
- DOI: https://doi.org/10.5395/rde.2016.41.4.278
-
Abstract
PDFPubReaderePub
Objectives Glass ionomer cements (GICs), which are biocompatible and adhesive to the tooth surface, are widely used nowadays for tooth restoration. They inhibit the demineralization and promote the remineralization of the tooth structure adjacent to the restoration, as well as interfere with bacterial growth. Hence, the present study was conducted to assess and compare the antimicrobial activity of three commercially available GICs against two cariogenic bacteria.
Materials and Methods An agar plate diffusion test was used for evaluating the antimicrobial effect of three different GICs (Fuji IX, Ketac Molar, and d-tech) on
Streptococcus mutans (S. mutans ) andLactobacillus acidophilus (L. acidophilus ). Thirty plates were prepared and divided into two groups. The first group was inoculated withS. mutans , and the second group was inoculated withL. acidophilus . These plates were then incubated at 37℃ for 24 hours. Zones of bacterial growth inhibition that formed around each well were recorded in millimeters (mm).Results The zones of inhibition for Fuji IX, Ketac Molar, and d-tech on
S. mutans were found to be 10.84 ± 0.22 mm, 10.23 ± 0.15 mm, and 15.65 ± 0.31 mm, respectively, whereas those forL. acidophilus were found to be 10.43 ± 0.12 mm, 10.16 ± 0.11 mm, and 15.57 ± 0.13 mm, respectively.Conclusions D-tech cement performed better in terms of the zone of bacterial inhibition against the two test bacteria, than the other two tested glass ionomers.
-
Citations
Citations to this article as recorded by- Effect of conditioning and 3-year aging on the bond strength and interfacial morphology of glass-ionomer cement bonded to dentin
Ahmed Zubaer, Rime Shamme Akter, Al Azad Salahuddin, Rahman Mir Ayubur, Sano Hidehiko, Hoshika Shuhei
Journal of Dental Sciences.2025; 20(2): 1229. CrossRef - Surface energetics of antibiofilm property of dental material added with green synthesized copper nanoparticles
Haris Saddique, Muhammad Aasim, Tariq Khan, Ajab Khan, Haroon Muhammad Ali, Umar Aziz
AMB Express.2025;[Epub] CrossRef - Effect of titanium dioxide nanotubes incorporated into conventional glass ionomer cement on L. acidophilus
Layse de Góis SENA, Maria Davoli MEYER, Mariana Gallante RICARDO, Isaac Jordão de Souza ARAÚJO, Julia Puppin RONTANI, Vanessa Arias PECORARI, Elizabeth Ferreira MARTINEZ, Lucas Novaes TEIXEIRA, Francisco Humberto NOCITI-JUNIOR, Paulo Noronha LISBOA-FILHO,
Brazilian Oral Research.2025;[Epub] CrossRef - Modifications of polyalkenoic acid and its effect on glass ionomer cement
Sreejith Sasidharan Lathikumari, Manju Saraswathy
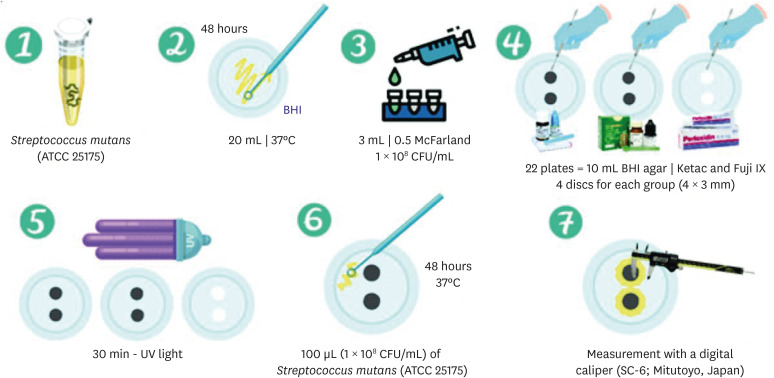
Materials Advances.2024; 5(7): 2719. CrossRef - Evaluation of the Clinical Impact and In Vitro Antibacterial Activities of Two Bioactive Restoratives against S. mutans ATCC 25175 in Class II Carious Restorations
YA Maher, MT Rajeh, FA Hamooda, GO Zerain, RM Habis, RH Sulaimani, ST Albar, FMH Ali, NA Abdelaleem
Nigerian Journal of Clinical Practice.2023; 26(4): 404. CrossRef - Comparison and Advanced Antimicrobial Strategies of Silver and Copper Nanodrug-Loaded Glass Ionomer Cement against Dental Caries Microbes
Amal Adnan Ashour, Mohammed Fareed Felemban, Nayef H. Felemban, Enas T. Enan, Sakeenabi Basha, Mohamed M. Hassan, Sanaa M. F. Gad El-Rab
Antibiotics.2022; 11(6): 756. CrossRef - Antibacterial Activity and Biofilm Inhibition of New-Generation Hybrid/Fluoride-Releasing Restorative Materials
Sevil Gurgan, Uzay Koc Vural, Cansu Atalay, Herve Tassery, Ivana Miletic, Suna Sibel Gurpinar
Applied Sciences.2022; 12(5): 2434. CrossRef - Comparative evaluation of long-term fluoride release and antibacterial activity of an alkasite, nanoionomer, and glass ionomer restorative material – An in vitro study
RV Aparajitha, PSenthamil Selvan, AShafie Ahamed, S Bhavani, V Nagarajan
Journal of Conservative Dentistry.2021; 24(5): 485. CrossRef - Dental Restorative Materials for Elderly Populations
Yuyao Huang, Bingqing Song, Xuedong Zhou, Hui Chen, Haohao Wang, Lei Cheng
Polymers.2021; 13(5): 828. CrossRef - The Comparison of Biofilm Formation, Mechanical and Chemical Properties between Glass Ionomer Cement and Giomer
Sylva Dinie Alinda, Anggraini Margono, Aditya Wisnu Putranto, Ike Dwi Maharti, Retno Amalina, Sherly Firsta Rahmi
The Open Dentistry Journal.2021; 15(1): 274. CrossRef - Effect of conditioning and 1 year aging on the bond strength and interfacial morphology of glass-ionomer cement bonded to dentin
Shuhei Hoshika, Shihchun Ting, Zubaer Ahmed, Fei Chen, Yu Toida, Norihito Sakaguchi, Bart Van Meerbeek, Hidehiko Sano, Sharanbir K. Sidhu
Dental Materials.2021; 37(1): 106. CrossRef - The synergistic effects of SrF2 nanoparticles, YSZ nanoparticles, and poly-ε-l-lysin on physicomechanical, ion release, and antibacterial-cellular behavior of the flowable dental composites
Saeed Hesaraki, Mohammad Karimi, Nader Nezafati
Materials Science and Engineering: C.2020; 109: 110592. CrossRef
- Effect of conditioning and 3-year aging on the bond strength and interfacial morphology of glass-ionomer cement bonded to dentin
- 2,420 View
- 8 Download
- 12 Crossref
- Elemental analysis of caries-affected root dentin and artificially demineralized dentin
- Young-Hye Sung, Ho-Hyun Son, Keewook Yi, Juhea Chang
- Restor Dent Endod 2016;41(4):255-261. Published online August 19, 2016
- DOI: https://doi.org/10.5395/rde.2016.41.4.255
-
Abstract
PDFPubReaderePub
Objectives This study aimed to analyze the mineral composition of naturally- and artificially-produced caries-affected root dentin and to determine the elemental incorporation of resin-modified glass ionomer (RMGI) into the demineralized dentin.
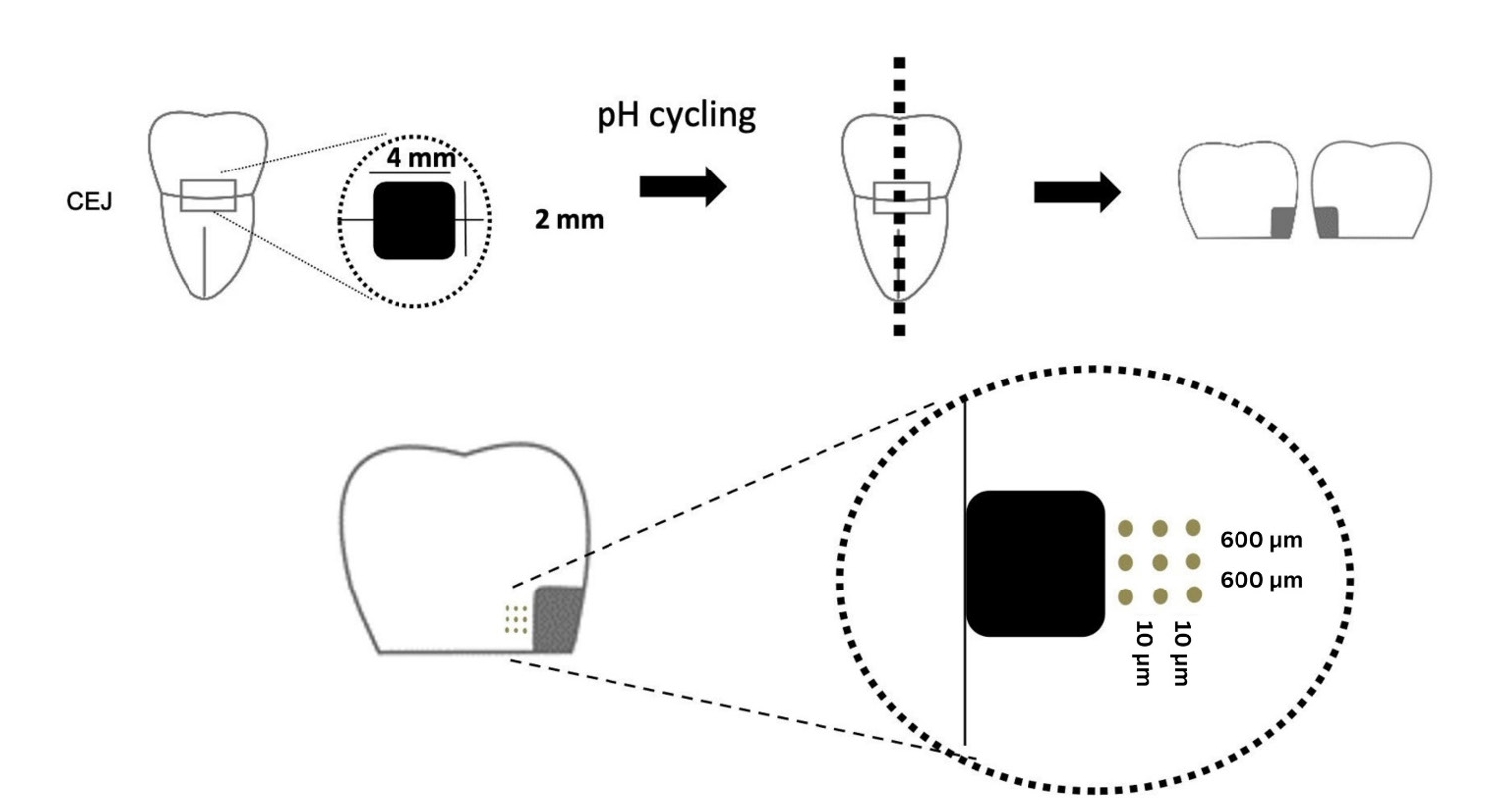
Materials and Methods Box-formed cavities were prepared on buccal and lingual root surfaces of sound human premolars (
n = 15). One cavity was exposed to a microbial caries model using a strain of Streptococcus mutans. The other cavity was subjected to a chemical model under pH cycling. Premolars and molars with root surface caries were used as a natural caries model (n = 15). Outer caries lesion was removed using a carbide bur and a hand excavator under a dyeing technique and restored with RMGI (FujiII LC, GC Corp.). The weight percentages of calcium (Ca), phosphate (P), and strontium (Sr) and the widths of demineralized dentin were determined by electron probe microanalysis and compared among the groups using ANOVA and Tukey test (p < 0.05).Results There was a pattern of demineralization in all models, as visualized with scanning electron microscopy. Artificial models induced greater losses of Ca and P and larger widths of demineralized dentin than did a natural caries model (
p < 0.05). Sr was diffused into the demineralized dentin layer from RMGI.Conclusions Both microbial and chemical caries models produced similar patterns of mineral composition on the caries-affected dentin. However, the artificial lesions had a relatively larger extent of demineralization than did the natural lesions. RMGI was incorporated into the superficial layer of the caries-affected dentin.
-
Citations
Citations to this article as recorded by- Effectiveness of Fluoride Varnish Versus Conventional Glass Ionomer in Preventing Occlusal Caries: A Systematic Review and Meta-Analysis
Abdullah Dh Alharbi, Masoud Almasoud, Fahad Alfadhli, Abdullah N Alharbi, Talal Aldhufairi, Rahaf Kh Alrashidi, Aisha Alameer, Abdulsalam Alenezi, Yousef Alqattan , Ahmed Abdelaziz
Cureus.2026;[Epub] CrossRef - pH-driven progression: Dental caries to pulpal and periapical disorders
Lingxi Hu, Jing Chen, Chun Hung Chu, Quan Tang, Wanjing Li, Tao Qin, Alice Kit Ying Chan, Lei Cheng
Archives of Oral Biology.2026; 186: 106574. CrossRef - Comparative evaluation of the remineralisation potential of biomimetic agents on phosphorylated dentine using SEM–EDX analysis: an in vitro study
Maruthi Gupta, Annapoorna B. M, Pravallika Chaluvadi, Rama Laxmi Koruprolu, Nikita Sebastian, Ram Sateesh Babu Mynam
Biomaterial Investigations in Dentistry.2026; 13: 278. CrossRef - Knowledge, Attitudes, and Practices of Dentists Regarding the Diagnosis and Management of White Spot Lesions
Nina Novozhilova, Anastasia Mun, Maria Polyakova, Irina Makeeva, Anna Mikheikina, Inna Sokhova, Alexandr Zaytsev, Ksenia Babina
Dentistry Journal.2026; 14(6): 365. CrossRef - The Cariostatic Mechanisms of Fluoride—An Updated Review
Ivana Šutej, Krešimir Bašić, Kristina Peroš
Dentistry Journal.2026; 14(7): 390. CrossRef - 3D Multi-modal Imaging of demineralised dentine using combined synchrotron µ-XRD-CT and STXM-CT
Nathanael Leung, Robert A. Harper, Bin Zhu, Stuart A. Bartlett, Konstantin Ignatyev, Richard M. Shelton, Gabriel Landini, Tan Sui
Journal of Structural Biology.2025; 217(2): 108208. CrossRef - A dynamic microcosm biofilm model for root carious-like lesion development: analysis of demineralization and microbiological characterization
Tamires Timm Maske, Glenda Ávila Marques, Bruna Dalongaro Fritsch, Bruna Moraes Kremer, Maximiliano Sérgio Cenci, Pabulo Henrique Rampelotto, Rodrigo Alex Arthur
Biofouling.2025; 41(5): 536. CrossRef - Bond strength durability of three bioactive restorative materials to silver diamine fluoride treated artificially demineralized dentine
Mostafa A. Abdelshafi, Hanan A.N. Soliman, Dina Abdelaziz
BMC Oral Health.2025;[Epub] CrossRef - Frontiers of Global Research Trend on Root Caries: A Bibliometric Analysis
Grace Yuchan Xu, Irene Shuping Zhao, Christie Ying Kei Lung, Iris Xiaoxue Yin, Edward Chin Man Lo, Chun Hung Chu
International Dental Journal.2024; 74(6): 1197. CrossRef - Effects of NaF versus SDF treatment on microhardness of artificial radiation caries at cervical and root areas
Pipop SAIKAEW, Karis KATEKOVIT, Anocha BURANARACHADA, Nattapat SAIMALA, Anussara PRAYONGRAT, Pornpoj FUANGTHARNTHIP
Dental Materials Journal.2024; 43(4): 591. CrossRef - Degradable polycaprolactone/buffer composites as pH regulating carrier materials for drug delivery and 3D printed biomaterials
Therese Schüler, Celine Guder, Franziska Alt, Katrin Lorenz, Torsten Sterzenbach, Christian Hannig, Hans-Peter Wiesmann, Benjamin Kruppke
Materialia.2024; 34: 102087. CrossRef - The Effect of Oral Care Foams and a Spray on Salivary pH Changes after Exposure to Acidic Beverages in Young Adults
Maria Polyakova, Anna Egiazaryan, Vladlena Doroshina, Alexandr Zaytsev, Alexey Malashin, Ksenia Babina, Nina Novozhilova
Dentistry Journal.2024; 12(4): 93. CrossRef - In Vitro Models Used in the Formation of Root Caries Lesions—A Review of the Literature
Zaid Dohan, Lara T. Friedlander, Paul R. Cooper, Kai-Chun Li, Jithendra T. Ratnayake, May L. Mei
Dentistry Journal.2023; 11(12): 269. CrossRef - Yttrium Trifluoride as a Marker of Infiltration Rate of Decalcified Root Cementum: An In Vitro Study
Anna Nowak-Wachol, Anna Korytkowska-Wałach, Bartosz Chmiela, Kacper Wachol, Maciej Łopaciński, Magdalena Wyszyńska, Yousuf Al-Dulaimi, Małgorzata Skucha-Nowak
Polymers.2022; 14(4): 780. CrossRef - Effect of fluoride, chlorhexidine or Nd:YAG on the progression of root dentin demineralization after removal of the demineralized organic matrix
Andrea Maselli, Tânia Mara da Silva, Lucélia Lemes Gonçalves, Aline Silva Braga, Eduardo Bresciani, Ana Carolina Magalhães, Sérgio Eduardo de Paiva Gonçalves
Journal of Applied Oral Science.2022;[Epub] CrossRef - Effect of ionizing radiation and cariogenic biofilm challenge on root-dentin caries
Camila de Carvalho Almança Lopes, Renata Borges Rodrigues, Maximiliano Sérgio Cenci, Juliana Lays Stolfo Uehara, Tamires Timm Maske, Pedro Henrique Justino Oliveira Limirio, Priscilla Barbosa Ferreira Soares, Veridiana Resende Novais
Clinical Oral Investigations.2021; 25(6): 4059. CrossRef - Silver diamine fluoride treatment of active root caries lesions in older adults: A case series
Chelsea Mitchell, Andrew J Gross, Peter Milgrom, Lloyd Mancl, David B Prince
Journal of Dentistry.2021; 105: 103561. CrossRef - A Hydrogel Drink With High Fructose Content Generates Higher Exogenous Carbohydrate Oxidation and a Reduced Drop in Dental Biofilm pH Compared to Two Other, Commercially Available, Carbohydrate Sports Drinks
Stefan Pettersson, Martin Ahnoff, Fredrik Edin, Peter Lingström, Charlotte Simark Mattsson, Ulrika Andersson-Hall
Frontiers in Nutrition.2020;[Epub] CrossRef
- Effectiveness of Fluoride Varnish Versus Conventional Glass Ionomer in Preventing Occlusal Caries: A Systematic Review and Meta-Analysis
- 2,598 View
- 18 Download
- 18 Crossref
- Do conventional glass ionomer cements release more fluoride than resin-modified glass ionomer cements?
- Maria Fernanda Costa Cabral, Roberto Luiz de Menezes Martinho, Manoel Valcácio Guedes-Neto, Maria Augusta Bessa Rebelo, Danielson Guedes Pontes, Flávia Cohen-Carneiro
- Restor Dent Endod 2015;40(3):209-215. Published online May 26, 2015
- DOI: https://doi.org/10.5395/rde.2015.40.3.209
-
Abstract
PDFPubReaderePub
Objectives The aim of this study was to evaluate the fluoride release of conventional glass ionomer cements (GICs) and resin-modified GICs.
Materials and Methods The cements were grouped as follows: G1 (Vidrion R, SS White), G2 (Vitro Fil, DFL), G3 (Vitro Molar, DFL), G4 (Bioglass R, Biodinâmica), and G5 (Ketac Fil, 3M ESPE), as conventional GICs, and G6 (Vitremer, 3M ESPE), G7 (Vitro Fil LC, DFL), and G8 (Resiglass, Biodinâmica) as resin-modified GICs. Six specimens (8.60 mm in diameter; 1.65 mm in thickness) of each material were prepared using a stainless steel mold. The specimens were immersed in a demineralizing solution (pH 4.3) for 6 hr and a remineralizing solution (pH 7.0) for 18 hr a day. The fluoride ions were measured for 15 days. Analysis of variance (ANOVA) and Tukey's test with 5% significance were applied.
Results The highest amounts of fluoride release were found during the first 24 hr for all cements, decreasing abruptly on day 2, and reaching gradually decreasing levels on day 7. Based on these results, the decreasing scale of fluoride release was as follows: G2 > G3 > G8 = G4 = G7 > G6 = G1 > G5 (
p < 0.05).Conclusions There were wide variations among the materials in terms of the cumulative amount of fluoride ion released, and the amount of fluoride release could not be attributed to the category of cement, that is, conventional GICs or resin-modified GICs.
-
Citations
Citations to this article as recorded by-
Impact of biofilm model of
Streptococcus mutans
on the pH, ions release, and sorption/solubility of glass ionomer cements enriched with 45S5 bioglass
Fábia Regina Vieira de Oliveira Roma, Mayron Guedes Silva, Tarcisio Jorge Leitão de Oliveira, José Bauer, Leily Macedo Firoozmand
Biofouling.2026; 42(1): 42. CrossRef - Gümüş Nanopartikülle Modifiye Edilmiş Geleneksel Cam İyonomer Simanların Antimikrobiyal Etkinliği: Sistematik Derleme
Feyza Nur Altan, Zeynep Aslı Güçlü
Sağlık Bilimleri Dergisi.2026; 35(1): 190. CrossRef - Effect of Cervical Restorations on Periodontal Health: An Observational Cross-Sectional Study
Mohd Zeeshan Ahmad, Nitish Mittal, Shreya Bhukal, Khushabu Deshmukh, Sachin Sarjerao Deshmukh, Banashree Sankeshwari, Priyanka Vhanmane
Cureus.2026;[Epub] CrossRef - Quantitative and Structural Characterization of Streptococcus mutans Biofilms on Dental Restorative Materials Using Scanning Electron Microscopy and Machine Learning
Krishna Kumar Kungumaraj, Sivashankari Rajasekaran, Bao Huynh, Jack Ferracane, Jens Kreth, Ana Paula Fugolin
Journal of Biomedical Materials Research Part B: Applied Biomaterials.2026;[Epub] CrossRef - Fluoride Uptake and Surface Characteristics of Ion-Releasing Restoratives After Brushing with Fluoride Toothpastes
Llubitza Slaviza Banic Vidal, Ivan Šalinović, Nikolina Nika Veček, Anja Ivica, Ivana Miletić, Silvana Jukić Krmek
Materials.2025; 18(9): 2152. CrossRef - Strategic approaches for enhancing the bioactivity of glass ionomer cement: A mechanistic and clinical perspective in terms of structural and surface modifications
Ali Saatchifard, Nader Nezafati, Saeed Hesaraki
Journal of Dentistry.2025; 163: 106126. CrossRef - Antibacterial effects of bioactive restorative dental materials on Streptococcus mutans: An in vitro study using the direct contact test
Sirirat Boondireke, Onsasi Kitrueangphatchara, Charnsak Sukajintanakarn, Sirichan Chiaraputt
The Saudi Dental Journal.2025;[Epub] CrossRef - Ion release of the glass ionomer restoration with silver diamine fluoride dentin pretreatment
Kelsey Xingyun Ge, Ryan Quock, Feng Yan, Walter Yu-Hang Lam, Chun-Hung Chu, Ollie Yiru Yu
Journal of Dentistry.2024; 148: 105247. CrossRef - Dual function of anti-biofilm and modulating biofilm equilibrium of orthodontic cement containing quaternary ammonium salt
Wenqi YU, Chaochao REN, Ning ZHANG, Li CAO, Michael D. WEIR, Kai YANG, Hockin H. K. XU, Yuxing BAI
Dental Materials Journal.2023; 42(2): 149. CrossRef - Fluoride exchange by glass-ionomer dental cements and its clinical effects: a review
John W. Nicholson, Sharanbir K. Sidhu, Beata Czarnecka
Biomaterial Investigations in Dentistry.2023;[Epub] CrossRef - Effects of Protective Surface Coating on Fluoride Release and Recharge of Recent Uncoated High-Viscosity Glass Ionomer Cement
Nantawan Krajangta, Chayanee Dulsamphan, Tongjai Chotitanmapong
Dentistry Journal.2022; 10(12): 233. CrossRef - Reinforcing an immature tooth model using three different restorative materials
Pooja Misar, Hemalatha Hiremath, Chhaya Harinkhere, ShailendraS Sonawane, Vinay Sharma, KuldeepSingh Rana
Dental Research Journal.2022; 19(1): 28. CrossRef - Fluoride release from two types of fluoride-containing orthodontic adhesives: Conventional versus resin-modified glass ionomer cements—An in vitro study
Yasemin Dziuk, Sachin Chhatwani, Stephan C. Möhlhenrich, Sabrina Tulka, Ella A. Naumova, Gholamreza Danesh, Richard Johannes Wierichs
PLOS ONE.2021; 16(2): e0247716. CrossRef - Phosphate Ion Release and Alkalizing Potential of Three Bioactive Dental Materials in Comparison with Composite Resin
Shahin Kasraei, Sahebeh Haghi, Sara Valizadeh, Narges Panahandeh, Sogol Nejadkarimi, Shinn Jyh Ding
International Journal of Dentistry.2021; 2021: 1. CrossRef - The effect of the polishing procedure and surface sealant application on the fluoride release of different restorative materials
Muhittin Ugurlu, Hikmet Orhan
Journal of Conservative Dentistry.2021; 24(2): 135. CrossRef - Mechanical and antimicrobial property of different surface treated glass ionomer cements under desiccated condition
Hemalatha Hiremath, Chhaya Harinkhere, Pooja Misar, Kshitij Sabley, Trupti Bajpai
Dental Research Journal.2021; 18(1): 64. CrossRef - Dental Restorative Materials for Elderly Populations
Yuyao Huang, Bingqing Song, Xuedong Zhou, Hui Chen, Haohao Wang, Lei Cheng
Polymers.2021; 13(5): 828. CrossRef - Monomer conversion, dimensional stability, biaxial flexural strength, and fluoride release of resin-based restorative material containing alkaline fillers
Piyaphong PANPISUT, Arnit TONELUCK
Dental Materials Journal.2020; 39(4): 608. CrossRef - Factors influencing fluoride release in atraumatic restorative treatment (ART) materials: A review
P.Divya Kumari, Shahnawaz Khijmatgar, Avidyuti Chowdhury, Edward Lynch, Chitta R. Chowdhury
Journal of Oral Biology and Craniofacial Research.2019; 9(4): 315. CrossRef - Incorporation of chlorhexidine and nano-sized sodium trimetaphosphate into a glass-ionomer cement: Effect on mechanical and microbiological properties and inhibition of enamel demineralization
Márjully Eduardo Rodrigues da Silva, Marcelle Danelon, José Antonio Santos Souza, Dinah Fressato Silva, Jesse Augusto Pereira, Denise Pedrini, Emerson Rodrigues de Camargo, Alberto Carlos Botazzo Delbem, Cristiane Duque
Journal of Dentistry.2019; 84: 81. CrossRef
-
Impact of biofilm model of
Streptococcus mutans
on the pH, ions release, and sorption/solubility of glass ionomer cements enriched with 45S5 bioglass
- 4,244 View
- 14 Download
- 20 Crossref
Case Report
- Treatment of a lateral incisor anatomically complicated with palatogingival groove
- Moon-Sun Choi, Se-Hee Park, Kyung-Mo Cho, Jin-Woo Kim
- J Korean Acad Conserv Dent 2011;36(3):238-242. Published online May 31, 2011
- DOI: https://doi.org/10.5395/JKACD.2011.36.3.238
-
Abstract
PDFPubReaderePub
Objectives Palatogingival groove is a developmental anomaly that starts near the cingulum of the tooth and runs down the cementoenamel junction in apical direction, terminating at various depths along the roots. While frequently associated with periodontal pockets and bone loss, pulpal necrosis of these teeth may precipitate a combined endodontic-periodontal lesion. This case presents a case of a lateral incisor anatomically complicated with palatogingival groove.
Methods Two patients with lesion associated with the palatogingival groove were chosen for this report. Palatogingival grooves were treated with different restoration materials with endodontic treatment.
Conclusions Maxillary lateral incisor with a palatogingival groove may occur the periodontal disease with pulpal involvement. Elimination of groove may facilitate the periodontal re-attachment and prevent the recurrence.
-
Citations
Citations to this article as recorded by- Endodontic treatment of maxillary lateral incisors with anatomical variations
Moon-Hwan Lee, Jung-Hong Ha, Myoung-Uk Jin, Young-Kyung Kim, Sung-Kyo Kim
Restorative Dentistry & Endodontics.2013; 38(4): 253. CrossRef
- Endodontic treatment of maxillary lateral incisors with anatomical variations
- 1,790 View
- 2 Download
- 1 Crossref
Original Article
- Micro-shear bond strength of resin-modified glass ionomer and resin-based adhesives to dentin
- Hyun-Kyung Hong, Kyoung-Kyu Choi, Sang-Hyuk Park, Sang-Jin Park
- J Korean Acad Conserv Dent 2003;28(4):314-325. Published online July 31, 2003
- DOI: https://doi.org/10.5395/JKACD.2003.28.4.314
- 1,661 View
- 1 Download
 First
First Prev
Prev

