
Search
- Page Path
- HOME > Search
Research Article
- Impact of bacteriological testing using an anaerobic culture system on the success of non-surgical endodontic treatment: a retrospective study
- Jun Nakanishi, Noriko Saito-Nakayama, Shizu Hirata-Tsuchiya, Daisuke Furutama, Ayaka Miyata-Arita, Tomoki Kawayanagi, Takuya Arita, Saki Nishihama, Tomoya Naruse, Wang Chutian, Song Bingxin, Naoki Sadaoka, Tomoki Kumagai, Kazuma Yoshida, Katsuhiro Takeda, Hideki Shiba
- J Korean Acad Conserv Dent ;Published online July 16, 2026
- DOI: https://doi.org/10.5395/rde.2026.51.e33 [Epub ahead of print]
-
 Abstract
Abstract
 PDF
PDF PubReader
PubReader ePub
ePub - Objectives
Residual bacteria at the time of root canal obturation significantly influence endodontic treatment outcomes in teeth with apical periodontitis, and confirmation of bacterial elimination from the root canal prior to obturation may improve long-term prognosis. However, the contribution of root canal bacterial culture to treatment outcomes in teeth with infected root canals is debated. This study aimed to retrospectively evaluate treatment outcomes in cases in which root canal obturation was performed after confirming negative bacteriological test results.
Methods
The medical records of patients with apical periodontitis or pulp necrosis in whom root canal obturation was performed after confirming a negative bacteriological test result using an anaerobic culture system at the Department of Endodontics and Operative Dentistry at Hiroshima University Hospital between April 1, 2015, and September 30, 2023, were retrospectively reviewed. Treatment outcomes were assessed by comparing dental radiographs obtained before treatment with those obtained during the follow-up, ranging from 3 to 24 months after root canal obturation.
Results
This retrospective study included 284 teeth from 218 patients, and the success rate was 89.1%. Tooth type, number of root canals, type of treatment, preoperative radiolucency around the root apex, preoperative root canal obturation material, dentist experience, and postoperative extent of root canal obturation material did not significantly affect treatment outcomes.
Conclusions
The findings of this retrospective study suggest that infection control incorporating bacteriological examination of root canals using an anaerobic culture system may contribute to a high success rate of nonsurgical endodontic treatment, regardless of other prognostic factors.
- 345 View
- 20 Download

Case Report
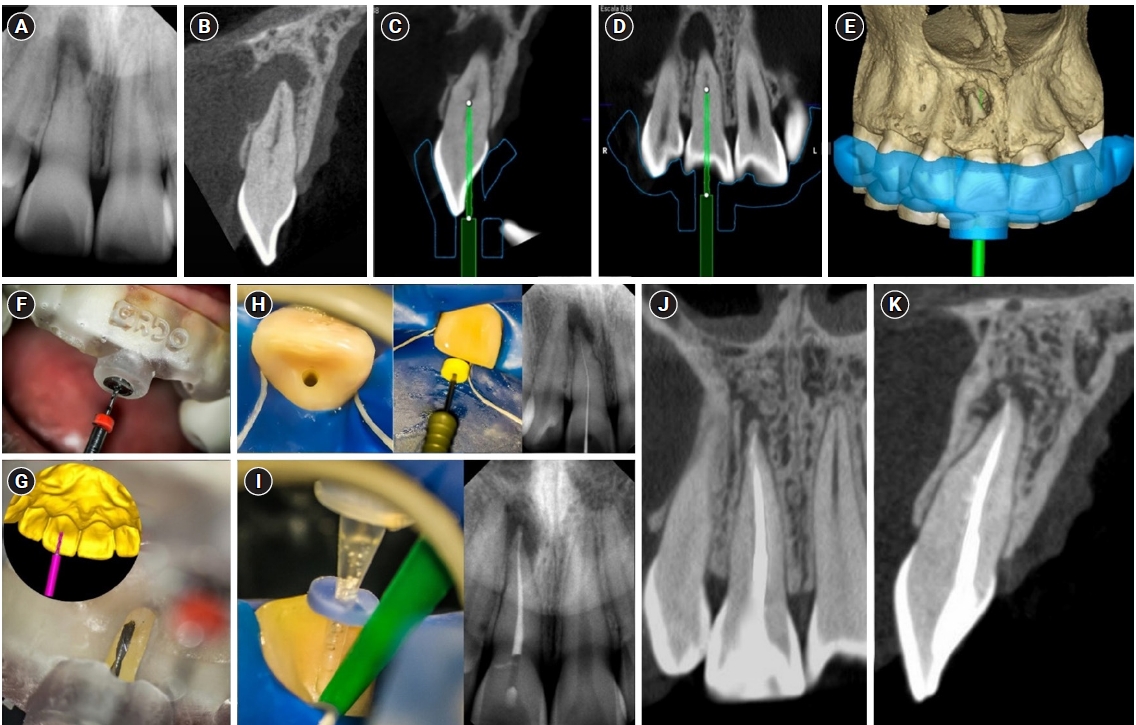
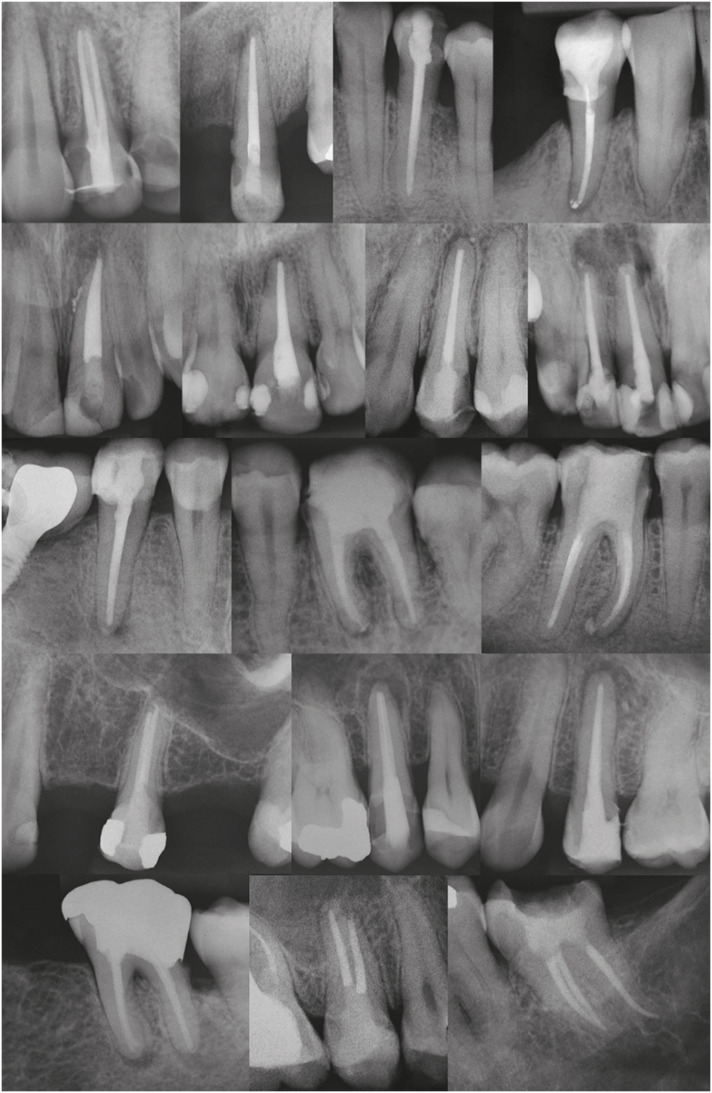
- Guided endodontics, precision and predictability: a case series of mineralized anterior teeth with follow-up cone-beam computed tomography
- Rafael Fernández-Grisales, Wilder Javier Rojas-Gutierrez, Pamela Mejía, Carolina Berruecos-Orozco, Néstor Ríos-Osorio
- Restor Dent Endod 2025;50(1):e4. Published online January 6, 2025
- DOI: https://doi.org/10.5395/rde.2025.50.e4
-
Abstract
PDFPubReaderePub
- Pulp chamber and root canal obliteration (PCO/RCO) presents a challenge for clinicians when nonsurgical endodontic treatment is indicated. Guided endodontics (GE) aims to precisely locate the root canal (RC) system while preserving as much pericervical dentin as possible. GE involves integrating cone-beam computed tomography (CBCT) of the affected tooth with a digital impression of the maxillary/mandibular arch, allowing for careful planning of the drilling path to the RC system through a three-dimensional (3D) static guide. This article reports four cases of teeth with PCO/RCO, accompanied by additional diagnoses of internal and external root resorption and horizontal tooth fracture, all successfully treated with GE. These cases highlight the clinical and radiographic success of GE treatments using CBCT, establishing this technique as a predictable approach for managing mineralized teeth.
-
Citations
Citations to this article as recorded by
- Static Guided Endodontics in Primary Endodontic Treatment of Anterior Teeth: A Narrative Review
Monika Kuczmaja, Wiesława Puchalska, Agata Żółtowska
Dentistry Journal.2026; 14(4): 195. CrossRef - Effect of different rotary instrument designs (protaper ultimate and protaper gold) on postoperative pain and bacterial reduction: a randomized clinical trial
Khaled Hassan Abed, Ahmed Abdel Rahman Hashem, Reem Ahmed Lutfy, Somaia Abdellatif Eissa, Dina Ahmed Morsy
BMC Oral Health.2026;[Epub] CrossRef
- Static Guided Endodontics in Primary Endodontic Treatment of Anterior Teeth: A Narrative Review
- 5,491 View
- 384 Download
- 2 Web of Science
- 2 Crossref
Research Article
- Postoperative pain after endodontic treatment of necrotic teeth with large intentional foraminal enlargement
- Ricardo Machado, Daniel Comparin, Sérgio Aparecido Ignácio, Ulisses Xavier da Silva Neto
- Restor Dent Endod 2021;46(3):e31. Published online May 31, 2021
- DOI: https://doi.org/10.5395/rde.2021.46.e31
-
Abstract
PDFPubReaderePub
Objectives To evaluate postoperative pain after endodontic treatment of necrotic teeth using large intentional foraminal enlargement (LIFE).
Materials and Methods The sample included 60 asymptomatic necrotic teeth (with or without chronic apical periodontitis), and a periodontal probing depth of 3 mm, previously accessed and referred to perform endodontic treatment. After previous procedures, the position and approximate size of the apical foramen (AF) were determined by using an apex locator and K flexo-files, respectively. The chemomechanical preparation was performed with Profile 04 files 2 mm beyond the AF to achieve the LIFE, using 2.5 mL of 2.5% NaOCl at each file change. The filling was performed by Tagger's hybrid technique and EndoFill sealer. Phone calls were made to all the patients at 24, 48 and 72 hours after treatment, to classify postoperative pain. Statistical analysis was performed by different tests with a significance level of 5%.
Results Age, gender, periradicular status and tooth type did not influence postoperative pain (
p > 0.05). Only 1 patient (1.66%) reported severe pain after 72 hours. Moderate pain was reported by 7, 4 and 3 patients after 24, 48 and 72 hours, respectively (p = 0.0001). However, paired analyses showed a statistically significant difference only between 24 and 72 hours (p = 0.04). Sealer extrusion did not influence the postoperative pain (p > 0.05).Conclusions Acute or moderate postoperative pain was uncommon after endodontic treatment of necrotic teeth with LIFE.
Trial Registration The Brazilian Clinical Trials Registry Identifier:
RBR-3r967t -
Citations
Citations to this article as recorded by- Postoperative Pain After Endodontic Treatment in HIV‐Positive Patients Under HAART: A Prospective Observational Cohort Study
Marcos Felipe Iparraguirre Nuñovero, Marco Antonio Hungaro Duarte, Luciana Reis Azevedo Alanis, Bruno Cavalini Cavenago, Ulisses Xavier da Silva Neto, Everdan Carneiro
International Endodontic Journal.2026; 59(5): 788. CrossRef - Does maintaining apical patency reduce early postoperative pain after root canal treatment? A randomized controlled trial in asymptomatic vital single-rooted teeth
Ozan Arda Deger, Sehnaz Yilmaz, Kübra Gürler
Clinical Oral Investigations.2026;[Epub] CrossRef - Evaluation of Postoperative Pain Frequency in Single‐Session Endodontic Treatments With Patency and Foraminal Enlargement
Viviane Barbosa Godoy, Ana Grasiela Limoeiro, Vanessa Sandini, Vini Mehta, Wayne Martins Nascimento, Marilia Fagury Videira Marceliano‐Alves, Marcos Frozoni
Clinical and Experimental Dental Research.2026;[Epub] CrossRef - Assessment of apical extrusion in regenerative endodontics: a comparative study of different irrigation methods using three-dimensional immature tooth models
Vahide Hazal Abat, Gökçen Deniz Bayrak, Mustafa Gündoğar
Odontology.2025; 113(1): 213. CrossRef - Clinical Advances in Calcium Phosphate for Maxillomandibular Bone Regeneration: From Bench to Bedside
Seyed Ali Mostafavi Moghaddam, Hamid Mojtahedi, Amirhossein Bahador, Lotfollah Kamali Hakim, Hamid Tebyaniyan
Ceramics.2025; 8(4): 129. CrossRef - Postoperative pain after single-visit root canal treatments in necrotic teeth comparing instruments’ kinematics and apical instrumentation limits – a prospective randomized multicenter clinical trial
Ricardo Machado, Guilherme Moreira, Daniel Comparin, Arthur Pimentel Barroso, Jaqueline Nascimento, Caio Cézar Randi Ferraz, Sérgio Aparecido Ignácio, Lucas da Fonseca Roberti Garcia, Rodrigo Rodrigues Amaral, David Shadid, Ulisses Xavier da Silva Neto
BMC Oral Health.2024;[Epub] CrossRef - Assessment of mechanical allodynia in healthy teeth adjacent and contralateral to endodontically diseased teeth: a clinical study
Vaishnavi Ratnakar Patankar, Ashish K Jain, Rahul D Rao, Prajakta R Rao
Restorative Dentistry & Endodontics.2024;[Epub] CrossRef - A systematic review and meta-analysis on the effects of phototherapy on postoperative pain in conventional endodontic reintervention
Larissa Pereira Nunes, Gabriel Pereira Nunes, Túlio Morandin Ferrisse, Henrico Badaoui Strazzi-Sahyon, Eloi Dezan-Júnior, Luciano Tavares Angelo Cintra, Gustavo Sivieri-Araujo
Clinical Oral Investigations.2024;[Epub] CrossRef - The effect of intracanal cryotherapy with and without foraminal enlargement on pain prevention after endodontic treatment: a randomized clinical trial
Marcos Felipe Iparraguirre Nuñovero, Marco Antonio Hungaro Duarte, André Vinícius Kaled Segato, Ulisses Xavier da Silva Neto, Vania Portela Ditzel Westphalen, Everdan Carneiro
Scientific Reports.2024;[Epub] CrossRef - Clinical determination of anatomical diameter in different dental groups correlating them with gender, age, tooth/canal and pulpoperiradicular diagnosis: an observational clinical study
Ricardo Machado, Gabriel Filipe Pamplona, Claudemir de Souza Júnior, Jaqueline Nascimento, Eduardo Donato Eing Elgelke Back, Daniel Comparin, Sérgio Aparecido Ignácio, Stella Maria Glaci Reinke, Ana Cristina Kovalik, Ulisses Xavier da Silva Neto
Scientific Reports.2023;[Epub] CrossRef - How much to enlarge? A letter to the editor
Krishnamachari Janani, Kavalipurapu Venkata Teja, Kumar Chandan Srivatsava
Saudi Endodontic Journal.2023; 13(3): 288. CrossRef - Efficiency of diode laser in control of post-endodontic pain: a randomized controlled trial
Hend H. Ismail, Maram Obeid, Ehab Hassanien
Clinical Oral Investigations.2023; 27(6): 2797. CrossRef - Periapical Healing following Root Canal Treatment Using Different Endodontic Sealers: A Systematic Review
Akshay Khandelwal, Krishnamachari Janani, KavalipurapuVenkata Teja, Jerry Jose, Gopi Battineni, Francesco Riccitiello, Alessandra Valletta, Ajitha Palanivelu, Gianrico Spagnuolo, Vincenzo Grassia
BioMed Research International.2022;[Epub] CrossRef
- Postoperative Pain After Endodontic Treatment in HIV‐Positive Patients Under HAART: A Prospective Observational Cohort Study
- 6,628 View
- 72 Download
- 11 Web of Science
- 13 Crossref
Review Article
- Triple antibiotic paste: momentous roles and applications in endodontics: a review
- Ardavan Parhizkar, Hanieh Nojehdehian, Saeed Asgary
- Restor Dent Endod 2018;43(3):e28. Published online June 20, 2018
- DOI: https://doi.org/10.5395/rde.2018.43.e28
-
Abstract
PDFPubReaderePub
This study investigated the latest findings and notions regarding ‘triple antibiotic paste’ (TAP) and its applications in dentistry, particularly endodontics. TAP is a combination of 3 antibiotics, ciprofloxacin, metronidazole, and minocycline. Despite the problems and pitfalls research pertaining to this paste has unveiled, it has been vastly used in endodontic treatments. The paste's applications vary, from vital pulp therapy to the recently introduced regeneration and revascularisation protocol. Studies have shown that the paste can eliminate the root canal microorganisms and prepare an appropriate matrix for further treatments. This combination is able to remove diverse groups of obligate and facultative gram-positive and gram-negative bacteria, providing an environment for healing. In regeneration protocol cases, this allows the development, disinfection, and possible sterilization of the root canal system, so that new tissue can infiltrate and grow into the radicular area. Moreover, TAP is capable of creating a discipline in which other wanted and needed treatments can be successfully performed. In conclusion, TAP, as an antibacterial intracanal medication, has diverse uses. Nevertheless, despite its positive effects, the paste has shown drawbacks. Further research concerning the combined paste and other intracanal medications to control microbiota is a must.
-
Citations
Citations to this article as recorded by- Endodontic Intracanal Medicaments and Agents
Anu Priya Guruswamy Pandian, Depti Bellani, Ritya Mary Jibu, Varsha Agnihotri
Dental Clinics of North America.2026; 70(1): 45. CrossRef - Regenerative Endodontic Treatment in Permanent Incisors: Two Case Reports with 6 Years of Follow-Up
María Biedma-Perea, Marcela Arenas-González, María José Barra-Soto, Carolina Caleza-Jiménez, David Ribas-Pérez
Children.2026; 13(2): 246. CrossRef - Evaluation of antimicrobial efficacy of an herbal preparation vs triple antibiotic paste against E. faecalis: an in vitro study
Chandni Dhyani, Kalpna Chaudhry, Nitin Khanduri, Leina R. Pradhan, Yoshita Gupta
International Journal of Contemporary Pediatrics.2026; 13(3): 449. CrossRef - Comparative antimicrobial efficacy of three intracanal medicaments in an in vitro Enterococcus faecalis root canal infection model
Ali Hasan, Hanan Mohammad, Maher Darwish, Mayssam Khaddam, Asmahan Zainab
BMC Oral Health.2026;[Epub] CrossRef - Comparison of the Antimicrobial Properties of Nanoemulsions Made from Phytosphingosine and Chitosan with a Triple Antibiotic Paste Against Enterococcus faecalis in Endodontics: An in-vitro Study
Ganesh Jadhav, Priya Mittal, Mohammed Abdul Kader M, Suheel Baba, Siddharth Shinde, Dhanashree Dalal, Ahmed Al Malwi, Shahabe Abullais, Siddharthan Selvaraj
International Journal of Nanomedicine.2026; Volume 21: 1. CrossRef - Chihuahuan Propolis as a Non-Antibiotic Intracanal Agent Against Enterococcus faecalis: An In Vitro Intratubular Study
Hilda Natalia Quintana-Pérez, Grissel Guadalupe Orozco-Molina, Carlos Esteban Villegas-Mercado, Sandra Aidé Santana-Delgado, Adolfo Gonzalez-Acosta, Javier Iván Martínez-Hernández, Raquel Duarte-Rico, Lydia Paulina Loya-Hernández, América Susana Mares-Gar
Microorganisms.2026; 14(4): 774. CrossRef - Intentional replantation for the management of external root resorption: A case report with clinical insights
Dipti Jitendra Khairajani, Anamika Chetan Borkar, Sanket D. Aras, Apeksha Sanjeev Gambhir, Saroj Pawar
Saudi Endodontic Journal.2026; 16(2): 287. CrossRef - Antimicrobial Efficacy of Triple Antibiotic Paste and Amoxicillin–Clavulanate against Enterococcus faecalis: A Comparative In Vitro Study
Sufia Parveen, Navin Mishra, FNU Kriti, Md Jawed Iqbal, Sheeri Sabir, Randhir Kumar
Journal of Dentistry and Bio-Allied Health Sciences.2026; 3(1): 1. CrossRef - Evaluation of Effect of Laser in Root Canal Disinfection in Pulp Regenerative Therapy: A Systematic Review
Kiran Kumar N, Abhishek M, Savitha B. Naik, Biji Brigit, Swetha Geervani V, M Manimozhi
Photobiomodulation, Photomedicine, and Laser Surgery.2025; 43(2): 53. CrossRef - Assessing Cell Viability: Comparative Analysis of Calcium Hydroxide, Triple Antibiotic Paste, and Their Synergistic Impact on human Dental Pulp Stem Cells
Dini Asrianti Bagio, Ibramanto Warganegara, Ike Dwi Maharti, Anggraini Margono, Citra Kusumasari, Sylva Dinie Alinda, Valeria Widita Wairooy
European Journal of General Dentistry.2025; 14(01): 073. CrossRef - Cytotoxic and Antibiofilm Properties of Antibiotic-Loaded Thermoresponsive Hydrogels for Root Canal Therapy
Cristiane Duque, Gabriela Pacheco de Almeida Braga, Juliana Machado de Carvalho, Karina Sampaio Caiaffa, Gabriel Pereira Nunes, Rafaela Laruzo Rabelo, Vanessa Rodrigues dos Santos, Geórgia Rondó Peres, Lucas da Silva Ribeiro, Emerson Rodrigues de Camargo
Processes.2025; 13(3): 661. CrossRef - Antibiofilm properties, cytotoxicity, and effect on protease activity of antibiotics and EGCG-based medications for endodontic purposes
Daniela Alvim Chrisostomo, Jesse Augusto Pereira, Polliana Mendes Candia Scaffa, Zach Gouveia, Gabriel Flores Abuna, Sergey V. Plotnikov, Anuradha Prakki, Cristiane Duque
Journal of Dentistry.2025; 156: 105660. CrossRef - The use of three-dimensional-printed guides, static navigation, and bioactive materials to treat bilateral and double dens invaginatus
Parth Patel, Nidhi Bharti, Ankit Arora, C. Nimisha Shah
Saudi Endodontic Journal.2025; 15(2): 207. CrossRef - To Assess the Cell Viability of Triple Antibiotic Paste under Confocal Microscope: An In Vitro Study
Elanthendral Saravanan, Mahesh Ramakrishnan
Journal of South Asian Association of Pediatric Dentistry.2025; 8(2): 81. CrossRef - Eficacia de la pasta triantibiótica en endodoncia: actividad antibacteriana frente a cepas resistentes de Enterococcus faecalis. Una revisión exhaustiva
Elena Patricia Cevallos Fernández, Katherine de los Ángeles Cuenca León
Anatomía Digital.2025; 8(3.1): 88. CrossRef - Efectividad de diferentes antimicóticos, junto con la pasta triantibiotica, para el tratamiento de Candida albicans en conductos radiculares
Carlos Andrés Rodríguez Tapia, Jessica María Sarmiento Ordoñez
Anatomía Digital.2025; 8(3.2): 45. CrossRef - Comparative Evaluation of Calcium Hydroxide, Triple Antibiotic Paste, and Calcium Hydroxide with 2% Chlorhexidine as Intracanal Medicaments in Reducing Interappointment Pain during Endodontic Treatment: An In Vivo Study
Itika Jain, Shyam Agrawal, Rachit Mathur, Shaista Gazal, Akshada Mungee, Babra Khan
International Journal of Clinical Pediatric Dentistry.2025; 18(6): 628. CrossRef - In Vitro Effectiveness of Endodontic Triple Antibiotic Paste Associated With Daptomycin
Sabrina S Azevedo, Gabriela C Chianca, Bruna A Thurler, Raiane C Chamon, Helvécio C Corrêa Póvoa, Leonardo S Antunes, Natalia L Pontes Póvoa Iorio
Cureus.2025;[Epub] CrossRef - Effect of Chitosan and bioactive glass nanomaterials as intracanal medicaments on TGF-β1 release from intraradicular dentin
Sarah Salah Hashem, Mohammed M. Khalefa, Mahmoud Hassan Mohamed, Hemat M. ELSheikh, Fatma Abd El-Rahman Taher
BMC Oral Health.2025;[Epub] CrossRef - Clinical and radiographic success of lesion sterilization and tissue repair in primary teeth: a systematic review and meta-analysis
Khlood Baghlaf, Rana A. Alamoudi
The Saudi Dental Journal.2025;[Epub] CrossRef - Antibacterial Effect of Cannabinoids on Bacteria Associated with Persistent Endodontic Infections
Cassandra Wieczerza, Haoyan Zhai, Mazin Askar, Zheng Zhou, Susan Paurazas
International Journal of Molecular Sciences.2025; 26(24): 11936. CrossRef - A Comparative Evaluation of Herbal Extracts and Triple Antibiotic Paste as Intracanal Medicament against Enterococcus faecalis: A Microbiological Study
Divya Singh, Rashi Singh, Nidhi Gupta, Natasha Gambhir, Saritha Golla
International Journal of Clinical Pediatric Dentistry.2024; 17(3): 285. CrossRef - Comparative Evaluation of Push-Out Bond Strength of Conventional Mineral Trioxide Aggregate, Biodentine, a Modified Mineral Trioxide Aggregate, and Two Novel Antibacterial-Enhanced Mineral Trioxide Aggregates
Arokia Rajkumar Shancy Merlin, Vignesh Ravindran, Ganesh Jeevanandan, Rajalakshmanan Eswaramoorthy, Abirami Arthanari
Cureus.2024;[Epub] CrossRef - In Vitro Evaluation of the Effect of Oleanolic Acid as a Potential Root Canal Medicament on Viability and Proliferation of Dental Pulp Stem Cells
Khalifah A. Alhaila, Manal Farouk Badawi, Mohamed G. Elbeltagy, Amany E. Badr
European Journal of General Dentistry.2024; 13(01): 051. CrossRef - Regenerative Endodontic Treatment in Dentinogenesis Imperfecta‐Induced Apical Periodontitis
Ying Liao, Ting Pan, Xianghui Xing, Sivakumar Nuvvula
Case Reports in Dentistry.2024;[Epub] CrossRef - Efecto antimicrobiano como medicación intraconducto de la pasta triantibiótica.
Paúl Sebastián Ulloa Amores, Diana Álvarez Álvarez, María Elizabeth Moscoso Abad, Magda Zulay Bastidas Calva
Revista de la Asociación Dental Mexicana.2024; 81(4): 211. CrossRef - Synthesis and Characterization of Nanosilica-Coated Antibiotics, TAP: A Comprehensive Study Utilizing XRD, EDS, FTIR, SEM, and TEM – Invitro Study
Mahaboob S. Hameed, S. Delphine P. Antony, Rajeshkumar Shanmugam, Sandhya Raghu
Journal of International Oral Health.2024; 16(5): 386. CrossRef - Association between host defence peptide IDR‐1002 and ciprofloxacin: Effects on human dental pulp cells
Danilo César Mota Martins, Maurício Gonçalves da Costa Sousa, Poliana Amanda Oliveira Silva, Lana Ribeiro Aguiar, Rosângela Vieira de Andrade, Amandda Évellin Silva‐Carvalho, Felipe Saldanha‐Araújo, Octávio Luiz Franco, Taia Maria Berto Rezende
Australian Endodontic Journal.2024; 50(3): 547. CrossRef - Comparative evaluation of antimicrobial efficacy of triple antibiotic paste and amoxicillin clavulanate paste as an intracanal medicament against Enterococcus faecalis: An in vitro study
Dhandayuthapani Sasikala, Parisa Norouzi Baghkomeh, Jamaluddin Mohammed Farzan
Dental Research Journal.2024;[Epub] CrossRef - Triple Antibiotic Paste: A Game Changer in Endodontics
Kalagi G. Panchal, Karima Virani, Vraj Patel, Aquib Ali Khan, Anam Pettiwala, Srikala S. Puranik, Srushti Joshi
Journal of Pharmacy and Bioallied Sciences.2024; 16(Suppl 3): S1913. CrossRef - Non-surgical Management of a Large Periapical Lesion: A Case Study of the Successful Application of a Modified Triple Antibacterial Paste
Srushti Awghad, Joyeeta Mahapatra, Amit Reche, Ankita Burse, Aradhana Kibe
Cureus.2024;[Epub] CrossRef - Enhancing Antimicrobial Efficacy and Synergistic Effects of Nano-Silica-Based Combinations With Doxycycline, Metronidazole, and Ciprofloxacin Against Enterococcus faecalis Biofilms
Shahul Hameed, Delphine P Antony, Rajeshkumar Shanmugam, Sandhya Raghu, Hima Sandeep Adimulapu
Cureus.2024;[Epub] CrossRef - Healing of periapical lesion by non-surgical endodontic therapy: A case series
Athira Ramesh, Rajesh Pillai, Afzal A, Anakha Santhosh, Arunima G.S, Sandeep K. V
IP Indian Journal of Conservative and Endodontics.2024; 9(2): 99. CrossRef - Effect of Calcium Hydroxide Versus Double Antibiotic Paste on Endodontic Treatment Outcomes in Teeth With Large Periapical Lesions: A Triple‐Blind Randomized Clinical Trial
Afsaneh Rahmati, Farshad Seyedein, Omid Dianat, Sara Saedi, Golriz Rostami, Alireza Akbarzadeh Baghban, Shima Sabertahan, Majid Kazem, Kee Y. Kum
International Journal of Dentistry.2024;[Epub] CrossRef - Can antimicrobial photodynamic therapy serve as an effective adjunct protocol for disinfecting the necrotic root canal system? A randomized controlled study
Remy Barazy, Hisham Alafif, Hassan Achour, Ahmad Al-Aloul, Yasser Alsayed Tolibah
BDJ Open.2024;[Epub] CrossRef - Drain and Treat: A Rubber Dam Technique for Acute Periapical Abscess
S. Grover, K. Mala, J. D’Souza
Acta Medica Bulgarica.2024; 51(s2): 143. CrossRef - Microbial Dynamics in Endodontic Pathology—From Bacterial Infection to Therapeutic Interventions—A Narrative Review
Klara Wieczorkiewicz, Anna Jarząbek, Estera Bakinowska, Kajetan Kiełbowski, Andrzej Pawlik
Pathogens.2024; 14(1): 12. CrossRef - An in vitro comparative evaluation of the effect of three intracanal medicaments – chlorhexidine gel, triple antibiotic paste, and calcium hydroxide paste on the push-out bond strength of MTA Plus, Biodentine, and calcium-enriched mixture
Gouthami Datta, Ramya Raghu, Ashish Shetty, Gautham P Manjunath, Dishant Patel, Subhashini Rajasekhara
Endodontology.2023; 35(1): 60. CrossRef - The cytotoxic effect of cysteamine and its combinations with various endodontic intracanal medications on fibroblast cells: in vitro study
Esraa Adel Mohamed Abd Elhameed ElGammal, Abeer Hashem Mahran, Salma Hassan El Ashry, Sara Hossam Fahmy
Bulletin of the National Research Centre.2023;[Epub] CrossRef - Healing of large endodontic lesions using a new combination of triple antibiotics: A case report
Saeed Asgary, Ardavan Parhizkar
Clinical Case Reports.2023;[Epub] CrossRef - Effects of Intracanal Medicaments on the Measurement Accuracy of Four Apex Locators: An In Vitro Study
Hamza Cudal, Tuğrul Aslan, Bertan Kesim
Meandros Medical and Dental Journal.2023; 24(3): 215. CrossRef - Comparative evaluation of the antibacterial efficacy of herbal agents as intracanal medicaments individually or in combination with chitosan: An in vitro RTPCR study
Gaurav Patri, Kotni Sheetal, PrasantiKumar Pradhan, Pratik Agrawal, S Lata
Journal of International Oral Health.2023; 15(1): 89. CrossRef - Recent progress in carbon dots for anti-pathogen applications in oral cavity
Yuying Jiang, Chuqiang Yin, Jianning Mo, Xiaoyu Wang, Ting Wang, Guotai Li, Qihui Zhou
Frontiers in Cellular and Infection Microbiology.2023;[Epub] CrossRef - A Comprehensive Review of Lesion Sterilization and Tissue Repair: An Alternative for Pulpectomy in Deciduous Teeth
Aparna Achanta, Amit Reche, Rishika Dakhale, Rudra R Bharate
Cureus.2023;[Epub] CrossRef - Healing of Large Endodontic Lesions Using Long‐Term Application of a New Combination of Triple Antibiotics: A Series of Cases
Saeed Asgary, Ardavan Parhizkar, Maria Beatriz Duarte Gavião
Case Reports in Dentistry.2023;[Epub] CrossRef - Non-cytotoxic Root Canal Dressing with Improved Antimicrobial Efficacy
Farzad Koosha, Jerome Cymerman, Thomas Manders, Marcia Simon, Stephen Walker, Miriam Rafailovich
Journal of Endodontics.2023; 49(2): 205. CrossRef - Triple antibiotics: A synergistic approach to combating infection
Hemant Sawhney, Anukriti Kumari, Ritik Kashwani, Geetanjali Gupta, SJ Das
IP Indian Journal of Conservative and Endodontics.2023; 8(4): 189. CrossRef - A 1-year Clinical and Radiographic Assessment of Regenerative Endodontic Therapy for Necrotic Primary Molars: A Randomized controlled Trial
Dina D Abdelmoneim, Amr M Abdelaziz, Gehan G Allam, Amira S Badran
International Journal of Clinical Pediatric Dentistry.2023; 16(2): 295. CrossRef - “BIODENTINE” THE DENTINE IN A CAPSULE AS AN APICAL BARRIER IN TRAUMATIZED MAXILLARY CENTRAL INCISOR WITH TWO YEARS FOLLOW UP.
Savita Thakur, Udai Bhanu, Gurkirat Singh Grewal
INTERNATIONAL JOURNAL OF SCIENTIFIC RESEARCH.2022; : 64. CrossRef - Long-term treatment of dentine with triple antibiotic paste promotes stem cell viability and attachment
Samiya Riaz, Ahmad Azlina, Zuliani Mahmood, Aung T. Htun
Journal of Taibah University Medical Sciences.2022; 17(4): 630. CrossRef - Non surgical management of trauma induced root resorption and large periapical
lesion using bioactive material- A case report
Tejasvini Prajapati, Sonali Kapoor, Purnil Shah, Ankit Arora, Hardik Rana
Clinical Dentistry.2022;[Epub] CrossRef - Antibacterial efficacy of antibiotic pastes versus calcium hydroxide intracanal dressing: A systematic review and meta-analysis of ex vivo studies
Mohammadreza Vatankhah, Kamyar Khosravi, Nazanin Zargar, Armin Shirvani, MohammadHossein Nekoofar, Omid Dianat
Journal of Conservative Dentistry.2022; 25(5): 463. CrossRef - Triple Antibiotic Paste: A Suitable Medicament for Intracanal Disinfection
Krutika Malu, Monika Khubchandani
Cureus.2022;[Epub] CrossRef - Present status and future directions of intracanal medicaments
Ronald Ordinola‐Zapata, W. Craig Noblett, Alejandro Perez‐Ron, Zhou Ye, Jorge Vera
International Endodontic Journal.2022; 55(S3): 613. CrossRef - The effect of four different intracanal medicaments on the push-out bond strength of root canal sealers
Shalu Maan, Vijaya Dhar Bhatt, Rohit Singh, Sayak Gupta, Syed Alay Noorain, Aashna Gill, Pradeep Kumar, Sushil Yadav, Preeti Sharma
Journal of Medicine and Life.2022; 15(4): 448. CrossRef - A Comparative Evaluation of Microhardness and Chemical Structure of Radicular Dentin with Two Combinations of TAP and MTAP: An In Vitro Study
Muthumula Daneswari, Nagireddy Venugopal Reddy, Annie P Chris, Nikhila V Reddy, Saigeeta Kondamadugu, P Niharika
International Journal of Clinical Pediatric Dentistry.2022; 15(S2): S151. CrossRef - Comparative Evaluation of Two Antibiotic Pastes for Root Canal Disinfection
Mridula Goswami, CP Baveja, Urvashi Bhushan, Sadhna Sharma
International Journal of Clinical Pediatric Dentistry.2022; 15(S1): S12. CrossRef - Management of External Inflammatory Root Resorption following Tooth Autotransplantation Using a Modified Combination of Triple Antibiotics
Saeed Asgary, Ardavan Parhizkar, Paulo J. Palma
Case Reports in Dentistry.2022;[Epub] CrossRef - Effect of triple antibiotic paste on the bond strength of epoxy and methacrylate resin-based sealers to root canal dentin
Fereshte Sobhnamayan, Alireza Adl, Mahdi Sedigh-Shams, Hossein Mirkhaghani
Journal of Conservative Dentistry.2022; 25(4): 426. CrossRef - Progress of Research on the Application of Triple Antibiotic Paste and Hydrogel Scaffold Materials in Endodontic Revascularization: A Systematic Review
Jia Zhao, Tian Jiao Wang
Evidence-Based Complementary and Alternative Medicine.2022; 2022: 1. CrossRef - The effect of different intracanal medicaments on the dislodgement resistance of mineral trioxide aggregate
Farzaneh Afkhami, Shahrzad Razavi, Sholeh Ghabraei
BMC Oral Health.2022;[Epub] CrossRef - Efficacy of Ciprofloxacin, Metronidazole and Minocycline in Ordered Mesoporous Silica against Enterococcus faecalis for Dental Pulp Revascularization: An In-Vitro Study
Cintia Micaela Chamorro-Petronacci, Beatriz Santos Torres, Rocío Guerrero-Nieves, Mario Pérez-Sayáns, Marcia Carvalho-de Abreu Fantini, Luis Carlos Cides-da-Silva, Beatriz Magariños, Berta Rivas-Mundiña
Materials.2022; 15(6): 2266. CrossRef - Antibiotic Mixtures in Noninstrumental Endodontic Treatment of Primary Teeth with Necrotic Pulps: A Systematic Review
Farah Chouchene, Fatma Masmoudi, Ahlem Baaziz, Fethi Maatouk, Hichem Ghedira, Sivakumar Nuvvula
International Journal of Dentistry.2021; 2021: 1. CrossRef - Potential apply of hydrogel-carried chlorhexidine and metronidazole in root canal disinfection
Yanhong YAN, Peng ZHOU, Haibing LU, Yun GUAN, Ming MA, Juan WANG, Guangwei SHANG, Beizhan JIANG
Dental Materials Journal.2021; 40(4): 986. CrossRef - Evaluation of the Effect of Nitrofurantoin Paste as an Intracanal Medicament on the Chemical Structure of Radicular Dentine
Mewan Abdulrahman, Bestoon Faraj, Kawa Dizaye
Sulaimani Dental Journal.2021; 8(2): 8. CrossRef - Local Drug Delivery Systems for Vital Pulp Therapy: A New Hope
Ardavan Parhizkar, Saeed Asgary, Carlo Galli
International Journal of Biomaterials.2021; 2021: 1. CrossRef - Antibiofilm and cytotoxic effect of 3,3′-dihydroxycurcumin (DHC) as photosensitizer agent in antimicrobial photodynamic therapy for endodontic purposes
Jesse Augusto Pereira, Carlos Roberto Polaquini, VanessaRodrigues dos Santos, Karina Sampaio Caiaffa, Rafaela Laruzo Rabelo, Reinaldo dos Santos Theodoro, Letícia Helena Theodoro, Luis Octavio Regasini, Cristiane Duque
Photodiagnosis and Photodynamic Therapy.2021; 36: 102534. CrossRef - An in-vitro Comparative Evaluation of Quantitative Release of Transforming Growth Factor β-1 from Dentin upon the Action of Endodontic Irrigants, Medicaments, Ultrasonic Activation, and Low-Level Laser Irradiation
Anilkumar Akhila, V. P. Prabath Singh, Kerala R. Varma, Senthil V. Vasudevan, V. Sukhithasri, Salu Sasikumar
Amrita Journal of Medicine.2021; 17(2): 34. CrossRef - Effect of triple antibiotic paste and calcium hydroxide on the rate of healing of periapical lesions: A systematic review
NKiran Kumar, Biji Brigit, BS Annapoorna, SavithaB Naik, Seema Merwade, K Rashmi
Journal of Conservative Dentistry.2021; 24(4): 307. CrossRef - Comparison of the efficacy of CanalBrush, EndoActivator, and Passive Ultrasonic Irrigation on the removal of triple antibiotic paste from root canal walls: An in vitro study
Santosh Kumar, Kavisha Desai, Aparna Palekar, Baswaraj Biradar, Ananjan Chatterjee, Khushboo Kumari
Journal of International Society of Preventive and Community Dentistry.2020; 10(4): 424. CrossRef - Apexification with Calcium Hydroxide vs. Revascularization
H. Boufdil, M. Mtalsi, S. El Arabi, B. Bousfiha, Jose López-López
Case Reports in Dentistry.2020;[Epub] CrossRef - Effect of Intracanal Medicaments and Irrigants on the Release of Transforming Growth Factor Beta 1 and Vascular Endothelial Growth Factor from Cervical Root Dentin
Lívia Nazareth Ferreira, Regina Maria Puppin-Rontani, Fernanda Miori Pascon
Journal of Endodontics.2020; 46(11): 1616. CrossRef - Incorporation of amoxicillin-loaded microspheres in mineral trioxide aggregate cement: an in vitro study
Fábio Rocha Bohns, Vicente Castelo Branco Leitune, Isadora Martini Garcia, Bruna Genari, Nélio Bairros Dornelles, Silvia Stanisçuaski Guterres, Fabrício Aulo Ogliari, Mary Anne Sampaio de Melo, Fabrício Mezzomo Collares
Restorative Dentistry & Endodontics.2020;[Epub] CrossRef - Assessment of Nitrofurantoin as an Experimental Intracanal Medicament in Endodontics
Mewan Salahalddin A. Alrahman, Bestoon Muhammed Faraj, Kawa F. Dizaye, Abdelwahab Omri
BioMed Research International.2020;[Epub] CrossRef - An in vitro assessment of effect on microhardness of dentin using vicker's hardness method
Manoj Chandak, Richa Modi, Rakesh Gogiya, Rakhi Chandak, Anuja Ikhar, Nikhil Mankar
Journal of Datta Meghe Institute of Medical Sciences University.2020; 15(2): 251. CrossRef - Inspection of the Microbiota in Endodontic Lesions
Mario Dioguardi, Giovanni Di Gioia, Gaetano Illuzzi, Claudia Arena, Vito Carlo Alberto Caponio, Giorgia Apollonia Caloro, Khrystyna Zhurakivska, Iolanda Adipietro, Giuseppe Troiano, Lorenzo Lo Muzio
Dentistry Journal.2019; 7(2): 47. CrossRef - Materials for pulpotomy in immature permanent teeth: a systematic review and meta-analysis
Yuan Chen, Xinlei Chen, Yali Zhang, Fangjie Zhou, Jiaxin Deng, Jing Zou, Yan Wang
BMC Oral Health.2019;[Epub] CrossRef - Adjunctive antimicrobial photodynamic therapy to conventional chemo-mechanical debridement of infected root canal systems: A systematic review and meta-analysis
Maryam Pourhajibagher, Abbas bahador
Photodiagnosis and Photodynamic Therapy.2019; 26: 19. CrossRef - Comparison of Antibacterial Effects of Photodynamic Therapy, Modified Triple Antibiotic Paste and Calcium Hydroxide on Root Canals Infected With Enterococcus faecalis: An In Vitro Study
Mohammad Asnaashari, Mohammad Jafar Eghbal, Amirali Sahba Yaghmayi, Mehdi Shokri, Saranaz Azari-Marhabi
Journal of Lasers in Medical Sciences.2019; 10(5): S23. CrossRef
- Endodontic Intracanal Medicaments and Agents
- 21,711 View
- 247 Download
- 79 Crossref
Research Article
- Healing outcomes of root canal treatment for C-shaped mandibular second molars: a retrospective analysis
- Hye-Ra Ahn, Young-Mi Moon, Sung-Ok Hong, Min-Seock Seo
- Restor Dent Endod 2016;41(4):262-270. Published online August 29, 2016
- DOI: https://doi.org/10.5395/rde.2016.41.4.262
-
Abstract
PDFPubReaderePub
Objectives This study aimed to evaluate the healing rate of non-surgical endodontic treatment between C-shaped and non-C-shaped mandibular second molars.
Materials and Methods Clinical records and radiological images of patients who had undergone endodontic treatment on mandibular second molars between 2007 and 2014 were screened. The periapical index scoring system was applied to compare healing outcomes. Information about preoperative and postoperative factors as well as the demographic data of the patients was acquired and evaluated using chi-square and multinomial logistic regression tests.
Results The total healing rate was 68.4%. Healing rates for the mandibular second molar were 70.9% in C-shaped canals (
n = 79) and 66.6% in non-C-shaped ones (n = 117). The difference was not statistically significant.Conclusions The presence of a C-shaped canal in the mandibular second molar did not have a significantly negative effect on healing after treatment. Instead, proper pulpal diagnosis and final restoration were indicated as having significantly greater influence on the healing outcomes of C-shaped and non-C-shaped canals, respectively.
-
Citations
Citations to this article as recorded by- Predicting early endodontic treatment failure following primary root canal treatment
Young-Eun Jang, Yemi Kim, Sin-Young Kim, Bom Sahn Kim
BMC Oral Health.2024;[Epub] CrossRef - Factors Influencing Non-Surgical Root Canal Treatment Outcomes in Mandibular Second Molars: A Retrospective Cone-Beam Computed Tomography Analysis
Da-Min Park, Woo-Hyun Seok, Ji-Young Yoon
Journal of Clinical Medicine.2024; 13(10): 2931. CrossRef - Retrospective Assessment of Healing Outcome of Endodontic Treatment for Mandibular Molars with C-shaped Root Canal
Kishore Kumar Majety, Basanta Kumar Choudhury, Anika Bansal, Achla Sethi, Jaina Panjabi
The Journal of Contemporary Dental Practice.2017; 18(7): 591. CrossRef
- Predicting early endodontic treatment failure following primary root canal treatment
- 2,984 View
- 26 Download
- 3 Crossref
Case Reports
- Nonsurgical endodontic retreatment of fused teeth with transposition: a case report
- Miguel Agostinho Beco Pinto Cardoso, Rita Brandão Noites, Miguel André Duarte Martins, Manuel Pedro da Fonseca Paulo
- Restor Dent Endod 2016;41(2):148-153. Published online February 22, 2016
- DOI: https://doi.org/10.5395/rde.2016.41.2.148
-
Abstract
PDFPubReaderePub
Tooth transposition is a disorder in which a permanent tooth develops and erupts in the normal position of another permanent tooth. Fusion and gemination are developmental disturbances presenting as the union of teeth. This article reports the nonsurgical retreatment of a very rare case of fused teeth with transposition. A patient was referred for endodontic treatment of her maxillary left first molar in the position of the first premolar, which was adjacent to it on the distobuccal side. Orthopantomography and periapical radiography showed two crowns sharing the same root, with a root canal treatment and an associated periapical lesion. Tooth fusion with transposition of a maxillary molar and a premolar was diagnosed. Nonsurgical endodontic retreatment was performed. At four yr follow-up, the tooth was asymptomatic and the radiolucency around the apical region had decreased, showing the success of our intervention. The diagnosis and treatment of fused teeth require special attention. The canal system should be carefully explored to obtain a full understanding of the anatomy, allowing it to be fully cleaned and obturated. Thermoplastic techniques were useful in obtaining hermetic obturation. A correct anatomical evaluation improves the set of treatment options under consideration, leading to a higher likelihood of esthetically and functionally successful treatment.
- 2,133 View
- 18 Download
- Progression of periapical cystic lesion after incomplete endodontic treatment
- Jong-Ki Huh, Dong-Kyu Yang, Kug-Jin Jeon, Su-Jung Shin
- Restor Dent Endod 2016;41(2):137-142. Published online February 22, 2016
- DOI: https://doi.org/10.5395/rde.2016.41.2.137
-
Abstract
PDFPubReaderePub
We report a case of large radicular cyst progression related to endodontic origin to emphasize proper intervention and follow-up for endodontic pathosis. A 25 yr old man presented with an endodontically treated molar with radiolucency. He denied any intervention because of a lack of discomfort. Five years later, the patient returned. The previous periapical lesion had drastically enlarged and involved two adjacent teeth. Cystic lesion removal and apicoectomy were performed on the tooth. Histopathological analysis revealed that the lesion was an inflammatory radicular cyst. The patient did not report any discomfort except for moderate swelling 3 days after the surgical procedure. Although the patient had been asymptomatic, close follow-ups are critical to determine if any periapical lesions persist after root canal treatment.
-
Citations
Citations to this article as recorded by- Prognosis of Vital Teeth Involved in Large Cystic Lesions After a Surgical Intervention: A Longitudinal Ambidirectional Cohort Study
Khalid A. Merdad, Maha Shawky, Khalid A. Aljohani, Rawia Alghamdi, Saja Alzahrani, Omar R. Alkhattab, Abdulaziz Bakhsh
Dentistry Journal.2025; 13(2): 83. CrossRef - Assessing the efficacy of apicoectomy without retrograde filling in treating periapical inflammatory cysts
Jeong-Kui Ku, Woo-Young Jeon, Seung-O Ko, Ji-Young Yoon
Journal of the Korean Association of Oral and Maxillofacial Surgeons.2024; 50(3): 140. CrossRef - Cystic lesion between a deciduous tooth and the succeeding permanent tooth: a retrospective analysis of 87 cases
Changmo Sohn, Jihye Ryu, Inhye Nam, Sang-Hun Shin, Jae-Yeol Lee
Journal of the Korean Association of Oral and Maxillofacial Surgeons.2022; 48(6): 342. CrossRef - The effectiveness of antibacterial treatment of the root canal in chronic apical periodontitis using an erbium-chromium laser
M. A. Postnikov, A. Yu. Rozenbaum, S. E. Chigarina, D. N. Kudryashov, M. B. Khaikin, I. V. Khramova, G. N. Belanov
Endodontics Today.2022; 20(2): 115. CrossRef - Factors Associated with Incomplete Endodontic Care
Carla Y. Falcon, Anthony R. Arena, Rebecca Hublall, Craig S. Hirschberg, Paul A. Falcon
Journal of Endodontics.2021; 47(9): 1398. CrossRef - Tratamento cirúrgico e conservador de cisto periapical de grande proporção: relato de caso
Maraísa Aparecida Pinto Resende, Neuza Maria Souza Picorelli Assis, Augusto César Sette-Dias, Evandro Guimarães de Aguiar, Bruno Salles Sotto-Maior
HU Revista.2018; 43(2): 191. CrossRef
- Prognosis of Vital Teeth Involved in Large Cystic Lesions After a Surgical Intervention: A Longitudinal Ambidirectional Cohort Study
- 4,327 View
- 25 Download
- 6 Crossref
Review Article
- A review of the regenerative endodontic treatment procedure
- Bin-Na Lee, Jong-Wook Moon, Hoon-Sang Chang, In-Nam Hwang, Won-Mann Oh, Yun-Chan Hwang
- Restor Dent Endod 2015;40(3):179-187. Published online March 16, 2015
- DOI: https://doi.org/10.5395/rde.2015.40.3.179
-
Abstract
PDFPubReaderePub
Traditionally, apexification has been used to treat immature permanent teeth that have lost pulp vitality. This technique promotes the formation of an apical barrier to close the open apex so that the filling materials can be confined to the root canal. Because tissue regeneration cannot be achieved with apexification, a new technique called regenerative endodontic treatment was presented recently to treat immature permanent teeth. Regenerative endodontic treatment is a treatment procedure designed to replace damaged pulp tissue with viable tissue which restores the normal function of the pulp-dentin structure. After regenerative endodontic treatment, continued root development and hard tissue deposition on the dentinal wall can occur under ideal circumstances. However, it is difficult to predict the result of regenerative endodontic treatment. Therefore, the purpose of this study was to summarize multiple factors effects on the result of regenerative endodontic treatment in order to achieve more predictable results. In this study, we investigated the features of regenerative endodontic treatment in comparison with those of other pulp treatment procedures and analyzed the factors that have an effect on regenerative endodontic treatment.
-
Citations
Citations to this article as recorded by- Efficacy of combined scaffolds and sodium hypochlorite in regenerative endodontics of immature teeth (in-vivo study)
Hanan Arb, Abeer Darrag, Neveen Shaheen, Dina Attia
Tanta Dental Journal.2026; 23(2): 240. CrossRef - Outcome evaluation of regenerative endodontic procedures using platelet derivatives: a systematic review and meta-analysis of animal models
Nafsika Alevizou, Konstantinos Kodonas, Anastasia Fardi, Christos Gogos
Odontology.2026;[Epub] CrossRef - Evaluation of the Clinical Outcomes of Regenerative Endodontic Procedures Using Autologous Platelet Concentrate: A Systematic Review and Meta-Analysis
Elnaz Mousavi, Navid Nasrabadi, Samira Jamali, Arian Haddadi
Pesquisa Brasileira em Odontopediatria e Clínica Integrada.2025;[Epub] CrossRef - Antimicrobial 3D printed gelatin scaffolds for root canal disinfection in regenerative endodontics procedures
Mateo Dallos Ortega, Jenny Aveyard, Raghda Magdy Abdelgawad, Reem El-Gendy, Alexander Ciupa, David Whetnall, Julia Behnsen, Robert J. Poole, Raechelle A. D'Sa
Biomaterials Science.2025; 13(14): 3795. CrossRef - Regenerative Endodontic Therapies: Harnessing Stem Cells, Scaffolds, and Growth Factors
Rosana Farjaminejad, Samira Farjaminejad, Franklin Garcia-Godoy
Polymers.2025; 17(11): 1475. CrossRef - Effects of combining hyaluronic acid hydrogel with injectable platelet rich fibrin on apical papilla stem cells proliferation and differentiation
Azal H. Al-Masoody, Nasrin Asadi, Hadiseh Mohammadpour, Mahshid Hodjat, Tahereh Sadat Jafarzadeh Kashi
BMC Oral Health.2025;[Epub] CrossRef - Experts consensus on management of tooth luxation and avulsion
Ruijie Huang, Chenchen Zhou, Ling Zhan, Yuan Liu, Xian Liu, Qin Du, Jun Wang, Wei Zhao, Guangtai Song, Li-an Wu, Beizhan Jiang, Yanhong Li, Hongmei Zhang, Jing Zou
International Journal of Oral Science.2024;[Epub] CrossRef - A review of tissue engineering in regenerative endodontic treatment
Eric Priyo Prasetyo, Dian Agustin Wahjuningrum, Galih Sampoerno, Wilson Sukandar, Shafy Shariz Bin Sharizal, Nurfahira Paidal, Menza Fadiyan Amriel, Nathania Elita Gunawan, Ketut Suardita, Evelyn Tjendronegoro
Conservative Dentistry Journal.2024; 14(1): 1. CrossRef - Innovative Paradigms and Established Strategies in Tooth Revitalization: A Review
Ahmad Shah Khan, Zahid Mehmood Khan, Palwasha Ishaque, Muhammad Zubair, Syeda Fatima Tu Zahra, Sana Ashfaq
Dental Update.2024; 51(8): 570. CrossRef - Explore the most recent developments and upcoming outlooks in the field of dental nanomaterials
Ali Alsuraifi, Zainab M. Sulaiman, Noor Alhuda R. Mohammed, Jassim Mohammed, Sarah Kareem Ali, Yousef Husam Abdualihamaid, Fatimah Husam, Abdullah Ayad
Beni-Suef University Journal of Basic and Applied Sciences.2024;[Epub] CrossRef - Recent Advances in Regenerative Endodontics: A Review of Current Techniques and Future Directions
Firas A Alothman, Lamia S Hakami, Ali Alnasser, Faris M AlGhamdi, Abdullah A Alamri, Basel M Almutairii
Cureus.2024;[Epub] CrossRef - Regenerative Potential of Dental Pulp Stem Cells in Response to a Bioceramic Dental Sealer and Photobiomodulation: An In Vitro Study
Hamed A Alshawkani, Mohamed Mansy, Mahmoud Al Ankily, Mohamed Shamel
The Journal of Contemporary Dental Practice.2024; 25(4): 313. CrossRef - Marginal adaptation of customized gutta percha cone with calcium silicate based sealer versus MTA and biodentine apical plugs in simulated immature permanent teeth (an in vitro study)
Mary M. Mina, Sybel M. Moussa, Mahmoud R. Aboelseoud
BMC Oral Health.2024;[Epub] CrossRef - GelMA‐based hydrogel biomaterial scaffold: A versatile platform for regenerative endodontics
Lei Huang, Xuan Chen, XiaoXia Yang, Yinchun Zhang, Xiaoling Qiu
Journal of Biomedical Materials Research Part B: Applied Biomaterials.2024;[Epub] CrossRef - Regenerative Endodontic Treatment in Dentinogenesis Imperfecta‐Induced Apical Periodontitis
Ying Liao, Ting Pan, Xianghui Xing, Sivakumar Nuvvula
Case Reports in Dentistry.2024;[Epub] CrossRef - In vitro and in vivo evaluation of iRoot BP Plus as a coronal sealing material for regenerative endodontic procedures
Ning Yang, Wenxiao Yang, Rou Shen, Shengcai Zhang, Tianchi Ma, Yao Liu
Clinical Oral Investigations.2024;[Epub] CrossRef - Comparative evaluation of pH and Ca+ ion release from MTA on interaction with platelet-rich fibrin and blood clot: an in vitro study
Sonia Khatri, Sylvia Mathew, Shruthi Nagaraja, Swaroop Hegde, Soumyadeep Ghosh, Kavimalar Ravichandran
F1000Research.2023; 12: 364. CrossRef - Photobiomodulation Therapy and Pulp-Regenerative Endodontics: A Narrative Review
Jiawen Yong, Sabine Gröger, Zuping Wu, Sabine Ruf, Yuer Ye, Xiaoyan Chen
Bioengineering.2023; 10(3): 371. CrossRef - Efficacy of disinfection procedures performed prior to regenerative endodontic therapy: An integrative review
Ketillyn da Silva Magalhães, Ana Clara Kuerten Gil, Taynara Santos Goulart, Daniela Peressoni Vieira Schuldt, Beatriz Serrato Coelho, Daniela de Rossi Figueiredo, Lucas da Fonseca Roberti Garcia, Josiane de Almeida
Australian Endodontic Journal.2023; 49(2): 418. CrossRef - Newer Prospects of Regenerative Endodontics: A Comprehensive and Updated Review of Literature
Mohammad Kamran Khan, Mahendra Kumar Jindal
Journal of the Scientific Society.2023; 50(3): 299. CrossRef - Comparative evaluation of pH and Ca+ ion release from MTA on interaction with platelet-rich fibrin and blood clot: an in vitro study
Sonia Khatri, Sylvia Mathew, Shruthi Nagaraja, Swaroop Hegde, Soumyadeep Ghosh, Kavimalar Ravichandran
F1000Research.2023; 12: 364. CrossRef - Effects of CEM cement and emdogain on proliferation and differentiation of human stem cells from the apical papilla: a comparative in vitro study
Elham Khoshbin, Leila Ghasemi, Rezvan Najafi, Hamed Karkehabadi
Biotechnology Letters.2023; 45(1): 69. CrossRef - Comparative Evaluation of the Regenerative Potential of Blood Clot and Platelet-rich Fibrin in Young Permanent Teeth Based on the Revised American Academy of Endodontics Clinical Considerations for Regenerative Procedure: 2016
Aarathi J Prakash, Saraswathi V Naik, Prabhakar Attiguppe
International Journal of Clinical Pediatric Dentistry.2023; 16(S2): S149. CrossRef - Biomechanical characterization of a fibrinogen–blood hydrogel for human dental pulp regeneration
Sofia Silvia Piglionico, Bela Varga, Orsolya Pall, Olivier Romieu, Csilla Gergely, Frédéric Cuisinier, Bernard Levallois, Ivan Vladislavov Panayotov
Biomaterials Science.2023; 11(20): 6919. CrossRef - Intracellular bacterial eradication using a novel peptide in vitro
Wing Nok Isaac Ng, Shanthini Kalimuthu, Carmen Oi Kwan Law, Angeline Hui Cheng Lee, Terrence Chi Kong Lau, Yiu Yan Leung, Gary Shun Pan Cheung, Prasanna Neelakantan
International Endodontic Journal.2023; 56(11): 1360. CrossRef - Regenerative Endodontic Treatment of Previously Treated Mature Permanent Tooth: A Case Report with 3-year Follow Up
Myung-Jin Lee
The Korean Journal of Oral and Maxillofacial Pathology.2023; 47(6): 133. CrossRef - Clinical Outcome and Comparison of Regenerative and Apexification Intervention in Young Immature Necrotic Teeth—A Systematic Review and Meta-Analysis
Pratima Panda, Lora Mishra, Shashirekha Govind, Saurav Panda, Barbara Lapinska
Journal of Clinical Medicine.2022; 11(13): 3909. CrossRef - Evaluation of Attitude and Knowledge of Endodontic, Pedodontic and SBARD Residents in Saudi Arabia toward Regenerative Endodontics—A National Survey
Ali A. Assiry, Mohmed Isaqali Karobari, Niher Tabassum Snigdha, Roshan Noor Mohamed, Syed Nahid Basheer, Mohammed Zameer
Medicina.2022; 58(4): 545. CrossRef - Effects of Intracanal Antimicrobials on Viability and Differentiation of Stem Cells From the Apical Papilla: An In Vitro Study
Gavin Raddall, Isabel Mello, Brendan M. Leung
Journal of Endodontics.2022; 48(7): 880. CrossRef - Awareness and Acceptance of Vital Pulp Therapy and Regenerative Endodontic Procedures among Dental Professionals in India: A Web-based Survey
Saloni Rathi, Priya Chauhan, Suparna Ganguly Saha, Rolly Agarwal, Simar Kaur Manocha, Mrinali Chaddha
Journal of Research and Advancement in Dentistry.2022; 14(1): 10. CrossRef - Exosomes as Biochemistry Tools for Stem Cell Differentiation: A Novel Cell-Based Treatment for Diseases
Saeed Azandeh, Darioush Bijan Nejad, Samaneh Karimi, Fereshtesadat Fakhredini
Jentashapir Journal of Cellular and Molecular Biology.2022;[Epub] CrossRef - Effect of biodentine coated with emdogain on proliferation and differentiation of human stem cells from the apical papilla
Hamed Karkehabadi, Erfan Ahmadyani, Rezvan Najafi, Elham Khoshbin
Molecular Biology Reports.2022; 49(5): 3685. CrossRef - Evaluation of the Effectiveness of Laser‐Assisted Bleaching of the Teeth Discolored due to Regenerative Endodontic Treatment
Noushin Shokouhinejad, Mehrfam Khoshkhounejad, Fatemeh Hamidzadeh, Murilo Baena Lopes
International Journal of Dentistry.2022;[Epub] CrossRef - Triple Antibiotic Paste: A Suitable Medicament for Intracanal Disinfection
Krutika Malu, Monika Khubchandani
Cureus.2022;[Epub] CrossRef - A Comparative Evaluation of Microhardness and Chemical Structure of Radicular Dentin with Two Combinations of TAP and MTAP: An In Vitro Study
Muthumula Daneswari, Nagireddy Venugopal Reddy, Annie P Chris, Nikhila V Reddy, Saigeeta Kondamadugu, P Niharika
International Journal of Clinical Pediatric Dentistry.2022; 15(S2): S151. CrossRef - Comparing Antibiotic Pastes with Electrospun Nanofibers as Modern Drug Delivery Systems for Regenerative Endodontics
Nura Brimo, Dilek Çökeliler Serdaroğlu, Busra Uysal
Current Drug Delivery.2022; 19(9): 904. CrossRef - The Advances of Blood Clots Used as Biomaterials in Regenerative Medicine
Eliza VanZweden, Rachael Tolsma, Victor Hung, Peter Awad, Robert Sawyer, Yong Li
Regenerative Medicine.2022; 17(12): 957. CrossRef - Microstructure and color stability of calcium silicate-based dental materials exposed to blood or platelet-rich fibrin
Noushin Shokouhinejad, Ibrahim Abu Tahun, Shima Saber Tahan, Fatemeh Mohandes, Mohammad H. Nekoofar, Paul M. H. Dummer
Clinical Oral Investigations.2022; 27(3): 1193. CrossRef - Results of “proroot mta” application in treatment of chronic periodontitis in teeth with incomplete root formation
N.M. Korneeva, E.A. Novikova, D.S. Popova, K.S. Rabadanova, L.Ya Rzaeva
Stomatology for All / International Dental review.2022; (2(99)): 10. CrossRef - Antimicrobial Effect of Calcium Hydroxide Combined with Electrolyzed Superoxidized Solution at Neutral pH on Enterococcus faecalis Growth
Héctor Armando Jimenez-Gonzalez, María Argelia Akemi Nakagoshi-Cepeda, Sergio Eduardo Nakagoshi-Cepeda, Víctor Hugo Urrutia-Baca, Myriam Angélica De La Garza-Ramos, Juan Manuel Solis-Soto, Ricardo Gomez-Flores, Patricia Tamez-Guerra, Yeliz Guven
BioMed Research International.2021;[Epub] CrossRef - Unpredictable Outcomes of a Regenerative Endodontic Treatment
Zahra Mohammadi, Hadi Assadian, Behnam Bolhari, Mohammadreza Sharifian, Mehrfam Khoshkhounejad, Nazanin Chitsaz, Andrea Scribante
Case Reports in Dentistry.2021;[Epub] CrossRef - Revascularization of nonvital immature incisor with asymptomatic apical periodontitis
Ema Mulyawati, Pribadi Santosa, Tunjung Nugraheni
Scientific Dental Journal.2020; 4(3): 134. CrossRef - Comparative analysis of calcium hydroxide apexification and regenerative endodontic procedure for root dentine growth stimulation in immature incisors with pulp necrosis
M.S. Rakhmanova, M.V. Korolenkova
Stomatologiya.2020; 99(6): 55. CrossRef - Antimicrobial Efficacy of a Novel Antibiotic‐Eluting Injectable Platelet‐Rich Fibrin Scaffold against a Dual‐Species Biofilm in an Infected Immature Root Canal Model
Azade Rafiee, Mahtab Memarpour, Yasaman Najibi, Bahman Khalvati, Sedigheh Kianpour, Mohammad Hossein Morowvat, Sung-Hwan Choi
BioMed Research International.2020;[Epub] CrossRef - Exosomes Derived from Stem Cells from the Apical Papilla Promote Dentine-Pulp Complex Regeneration by Inducing Specific Dentinogenesis
Xueying Zhuang, Lingli Ji, Huan Jiang, Yao Liu, Xuemei Liu, Jing Bi, Weidong Zhao, Zhenjiang Ding, Xu Chen
Stem Cells International.2020; 2020: 1. CrossRef - Injectable Biomaterials for Dental Tissue Regeneration
Håvard Jostein Haugen, Poulami Basu, Mousumi Sukul, João F Mano, Janne Elin Reseland
International Journal of Molecular Sciences.2020; 21(10): 3442. CrossRef - Viability and Stimulation of Human Stem Cells from the Apical Papilla (hSCAPs) Induced by Silicate-Based Materials for Their Potential Use in Regenerative Endodontics: A Systematic Review
José Luis Sanz, Leopoldo Forner, Alicia Almudéver, Julia Guerrero-Gironés, Carmen Llena
Materials.2020; 13(4): 974. CrossRef - An Innovative Drug Delivery System Loaded with a Modified Combination of Triple Antibiotics for Use in Endodontic Applications
Ardavan Parhizkar, Hanieh Nojehdehian, Fahimeh Tabatabaei, Saeed Asgary
International Journal of Dentistry.2020; 2020: 1. CrossRef - Defining Endodontic Residents' Clinical Experiences: A National Survey
Jonathan D. Blacher, Kamran E. Safavi, Robert H. Aseltine, Blythe M. Kaufman
Journal of Dental Education.2019; 83(5): 504. CrossRef - Coronal tooth discoloration induced by regenerative endodontic treatment using different scaffolds and intracanal coronal barriers: a 6-month ex vivo study
Noushin Shokouhinejad, Hassan Razmi, Maryam Farbod, Marzieh Alikhasi, Josette Camilleri
Restorative Dentistry & Endodontics.2019;[Epub] CrossRef - Comparative Study between Revitalization of Necrotic Immature Permanent Anterior Teeth with and without Platelet Rich Fibrin: A Randomized Controlled Trial
Rasha Adel Ragab, Amr Ezzat Abd El Lattif, Norhan Abd El Wahab El Dokky
Journal of Clinical Pediatric Dentistry.2019; 43(2): 78. CrossRef - Biomaterials and Scaffold Design Strategies for Regenerative Endodontic Therapy
Gavin Raddall, Isabel Mello, Brendan M. Leung
Frontiers in Bioengineering and Biotechnology.2019;[Epub] CrossRef - Iloprost Induces Dental Pulp Angiogenesis in a Growth Factor–free 3-Dimensional Organ Culture System
Sonntana Seang, Prasit Pavasant, Chalida N. Limjeerajarus
Journal of Endodontics.2018; 44(5): 759. CrossRef - Ratio and Rate of Induced Root Growth in Necrotic Immature Teeth
Eun Jung Sang, Ji-Soo Song, Teo Jeon Shin, Young-Jae Kim, Jung-Wook Kim, Ki-Taeg Jang, Sang-Hoon Lee, Hong-Keun Hyun
THE JOURNAL OF THE KOREAN ACADEMY OF PEDTATRIC DENTISTRY.2018; 45(2): 225. CrossRef - Triple antibiotic paste: momentous roles and applications in endodontics: a review
Ardavan Parhizkar, Hanieh Nojehdehian, Saeed Asgary
Restorative Dentistry & Endodontics.2018;[Epub] CrossRef - Traumatic avulsion and delayed replantation of maxillary incisors in an eleven-year-old child
Gokcen Deniz Bayrak
Edorium Journal of Dentistry.2018; 5(1): 1. CrossRef - Influence of Apical Diameter on the Outcome of Regenerative Endodontic Treatment in Teeth with Pulp Necrosis: A Review
Yanjun Fang, Xinhuan Wang, Jingjing Zhu, Chaonan Su, Ying Yang, Liuyan Meng
Journal of Endodontics.2018; 44(3): 414. CrossRef - Assessment of Regaining Pulp Sensibility in Mature Necrotic Teeth Using a Modified Revascularization Technique with Platelet-rich Fibrin: A Clinical Study
Mohamed Nageh, Geraldine M. Ahmed, Alaa A. El-Baz
Journal of Endodontics.2018; 44(10): 1526. CrossRef - Local drug delivery in endodontics: A literature review
Shin Hye Chung, Young-Seok Park
Journal of Drug Delivery Science and Technology.2017; 39: 334. CrossRef - Regenerative Endodontics
Kristina Feigin, Bonnie Shope
Journal of Veterinary Dentistry.2017; 34(3): 161. CrossRef - Intentional Replantation of an Avulsed Immature Permanent Incisor: A Case Report
Claudio Maniglia-Ferreira, Fabio de Almeida Gomes, Marcelo de Morais Vitoriano
Journal of Endodontics.2017; 43(8): 1383. CrossRef - Effect of acidic solutions on the microhardness of dentin and set OrthoMTA and their cytotoxicity on murine macrophage
Soram Oh, Hiran Perinpanayagam, Yoon Lee, Jae-Won Kum, Yeon-Jee Yoo, Sang-Min Lim, Seok Woo Chang, Won-Jun Shon, Woocheol Lee, Seung-Ho Baek, Kee-Yeon Kum
Restorative Dentistry & Endodontics.2016; 41(1): 12. CrossRef - Questioning the spot light on Hi-tech endodontics
Jojo Kottoor, Denzil Albuquerque
Restorative Dentistry & Endodontics.2016; 41(1): 80. CrossRef - Effects of a Bioactive Scaffold Containing a Sustained Transforming Growth Factor-β1–releasing Nanoparticle System on the Migration and Differentiation of Stem Cells from the Apical Papilla
Craig Bellamy, Suja Shrestha, Calvin Torneck, Anil Kishen
Journal of Endodontics.2016; 42(9): 1385. CrossRef - Effects of Novel 3-dimensional Antibiotic-containing Electrospun Scaffolds on Dentin Discoloration
Margaret Louise A. Porter, Eliseu A. Münchow, Maria T.P. Albuquerque, Kenneth J. Spolnik, Anderson T. Hara, Marco C. Bottino
Journal of Endodontics.2016; 42(1): 106. CrossRef
- Efficacy of combined scaffolds and sodium hypochlorite in regenerative endodontics of immature teeth (in-vivo study)
- 8,512 View
- 136 Download
- 65 Crossref
Case Report
- Surgical endodontic management of infected lateral canals of maxillary incisors
- Ji-Hyun Jang, Jung-Min Lee, Jin-Kyu Yi, Sung-Baik Choi, Sang-Hyuk Park
- Restor Dent Endod 2015;40(1):79-84. Published online October 10, 2014
- DOI: https://doi.org/10.5395/rde.2015.40.1.79
-
Abstract
PDFPubReaderePub
This case report presents surgical endodontic management outcomes of maxillary incisors that were infected via the lateral canals. Two cases are presented in which endodontically-treated maxillary central incisors had sustained lateral canal infections. A surgical endodontic treatment was performed on both teeth. Flap elevation revealed vertical bone destruction along the root surface and infected lateral canals, and microscopy revealed that the lateral canals were the origin of the lesions. After the infected lateral canals were surgically managed, both teeth were asymptomatic and labial fistulas were resolved. There were no clinical or radiographic signs of surgical endodontic management failure at follow-up visits. This case report highlights the clinical significance and surgical endodontic management of infected lateral canal of maxillary incisor. It is important to be aware of root canal anatomy variability in maxillary incisors. Maxillary central incisors infected via the lateral canal can be successfully managed by surgical endodontic treatment.
-
Citations
Citations to this article as recorded by- Surgical Management of Radicular Cyst with Platelet-rich Fibrin Placement followed by Nonvital Bleaching of a Discolored Maxillary Left Central Incisor (21)
Sagarika Sortey, Gautam Badole, Pratima Shenoi, Rajesh Kubde, Shriya Shahu, Ankita Ramteke, Varsha Uttarwar
Bharati Vidyapeeth Journal of Dentistry and Allied Sciences.2025; 2(1): 31. CrossRef - Apical Surgery of a Maxillary Left Central Tooth Using NeoPutty After Retreatment Failure: A Case Report
Sajedeh Namaei Ghasemi, Zakieh Kheradmand, Siavash Moushekhian, Zeinab Ghasemi
Clinical Case Reports.2025;[Epub] CrossRef - Cone Beam Computed Tomography as a Diagnostic Tool in the Diagnosis of an Iatrogenic Root Defect of a Root Canal Treated Maxillary Central Incisor with Periapical Lesion and Its Management by Re-apicectomy
Swathi Aravelli, Uday Kumar, Gunnam Sai Nishitha, K. Mallika Yadav, P. Sivaram, Nimeshika Ramachandruni
Bharati Vidyapeeth Journal of Dentistry and Allied Sciences.2025; 2(4): 155. CrossRef - On the Causes of Persistent Apical Periodontitis. Findings From Endodontic Microsurgery: A Case Report
Mateo José Pesántez-Ibarra, Carolina Berruecos-Orozco, Jeimmy Katherine Molina-Barrera, Néstor Ríos-Osorio, Rafael Fernández-Grisales
Journal of Endodontic Microsurgery.2025;[Epub] CrossRef - Expert consensus on difficulty assessment of endodontic therapy
Dingming Huang, Xiaoyan Wang, Jingping Liang, Junqi Ling, Zhuan Bian, Qing Yu, Benxiang Hou, Xinmei Chen, Jiyao Li, Ling Ye, Lei Cheng, Xin Xu, Tao Hu, Hongkun Wu, Bin Guo, Qin Su, Zhi Chen, Lihong Qiu, Wenxia Chen, Xi Wei, Zhengwei Huang, Jinhua Yu, Zhen
International Journal of Oral Science.2024;[Epub] CrossRef - Surgical endodontic treatment of maxillary incisors: Case report
Moazzy I. Almansour
Clinical Case Reports.2023;[Epub] CrossRef - Resective and Regenerative Approach for an Unresolved Periapical Lesion: A Surgical Case Report With 24-Month Follow-Up
Anchu R Thomas, Melwin Mathew, Sunil K Nettemu, Anoop Mayya
Cureus.2023;[Epub] CrossRef - An in vitro endodontic model to quantify the accessory canal filling potential of the vertical and lateral condensation techniques
Thomas Gerhard Wolf, Louisa Willems, Benjamín Briseño‐Marroquín
Australian Endodontic Journal.2021; 47(2): 245. CrossRef - Application of a new system for classifying root and canal anatomy in studies involving micro‐computed tomography and cone beam computed tomography: Explanation and elaboration
H. M. A. Ahmed, N. Ibrahim, N. S. Mohamad, P. Nambiar, R. F. Muhammad, M. Yusoff, P. M. H. Dummer
International Endodontic Journal.2021; 54(7): 1056. CrossRef - German Dentists’ Preferences for the Treatment of Apical Periodontitis: A Cross-Sectional Survey
Jonas Conrad, Jan Retelsdorf, Sameh Attia, Christof Dörfer, Mohamed Mekhemar
International Journal of Environmental Research and Public Health.2020; 17(20): 7447. CrossRef - Surgical management of an accessory canal in a maxillary premolar: a case report
Hee-Jin Kim, Mi-Kyung Yu, Kwang-Won Lee, Kyung-San Min
Restorative Dentistry & Endodontics.2019;[Epub] CrossRef - A new system for classifying accessory canal morphology
H. M. A. Ahmed, P. Neelakantan, P. M. H. Dummer
International Endodontic Journal.2018; 51(2): 164. CrossRef - Effects of antimicrobial photodynamic therapy and surgical endodontic treatment on the bacterial load reduction and periapical lesion healing. Three years follow up
Aguinaldo S. Garcez, Julio G. Arantes-Neto, Debora P. Sellera, Eduardo Rodrigues Fregnani
Photodiagnosis and Photodynamic Therapy.2015; 12(4): 575. CrossRef
- Surgical Management of Radicular Cyst with Platelet-rich Fibrin Placement followed by Nonvital Bleaching of a Discolored Maxillary Left Central Incisor (21)
- 2,905 View
- 19 Download
- 13 Crossref
Research Article
- Prevalence of referral reasons and clinical symptoms for endodontic referrals
- Seonah Kim
- Restor Dent Endod 2014;39(3):210-214. Published online June 23, 2014
- DOI: https://doi.org/10.5395/rde.2014.39.3.210
-
Abstract
PDFPubReaderePub
Objectives To investigate the prevalence of different primary reasons for endodontic referrals and the clinical symptoms of the referred cases.
Materials and Methods Clinical data of total endodontic treatment cases (1,014 teeth) including endodontic referral cases (224 teeth) between January 1, 2010 and December 31, 2012, at Kangdong Sacred Heart Hospital, were investigated retrospectively. The one major reason for referral, the clinical symptoms, and the resulting treatment procedures of referral cases were recorded. The percentages of clinical symptoms of the endodontic referral cases and the total endodontic treatment cases were compared by χ2 test for each symptom.
Results Persistent pain was the most frequent reason for endodontic referral (29.5%), followed by presence of gingival swelling and sinus tract (24.1%), and apical radiolucency (12.9%). Referrals in cases involving endodontic difficulties such as canal calcification, broken instruments, post, perforation, and resorption were less than 5.0%, respectively. The percentages of four major clinical symptoms of pain, apical radiolucency, previous endodontic treatment, and gingival swelling and sinus tract were significantly higher in the endodontic referral cases than those in the total endodontic cases (
p = 0.001). Among the included referral cases, 72.8% were treated with nonsurgical endodontic treatment only. Teeth other than the referred teeth were diagnosed as the origin of the problem in 5.8% of the referrals.Conclusions The high prevalence of pain, apical radiolucency, previous treatment, and gingival swelling and sinus tract in endodontic referral cases suggest that these symptoms may be what general practitioners consider to be difficult and refer to endodontists.
-
Citations
Citations to this article as recorded by- Monitoring Asymptomatic Apical Periodontitis in Root‐Filled Teeth—Results From a One‐Year Follow‐Up Prospective Study
M. Sayady‐Ölander, J. Östlin, V. S. H. Yu, C. Ulin, T. Kvist
International Endodontic Journal.2026; 59(2): 203. CrossRef - Referral Patterns and Professional Perceptions of Referring Dentists and Endodontists
Parth Karia, Hae Young Hong, Jong Ryul Kim
Journal of Endodontics.2026;[Epub] CrossRef - When Pain Shapes Dental Anxiety: A Cross-Sectional Mediation Study in Patients Requiring Endodontic Treatment
Edanur Maraş, Özge Başar, İlyas Çolakoğlu
Journal of Clinical Medicine.2026; 15(12): 4660. CrossRef - The role of endodontists in managing patients with molar incisor hypomineralisation
Lavínia L. Costa, Jaderson F. S. Dantas, Patrícia B. Santos
Primary Dental Journal.2025; 14(1): 74. CrossRef - VARIABLES AFFECTING PATIENT REFERRALS FROM GENERAL DENTAL PRACTITIONERS TO ENDODONTISTS
R. Peršić Bukmir, E Paljević, J. Vidas Hrstić, E Božac, I. Vidović Zdrilić, I. Brekalo Pršo
Česká stomatologie a praktické zubní lékařství.2024; 124(4): 89. CrossRef - The necessity and reasons for referrals to endodontists among general dentists in Mashhad: A cross-sectional study
Maryam Gharechahi, Armita Rouhani, Amin Khazai Ahmadi, Mina Davaji
Saudi Endodontic Journal.2024; 14(1): 75. CrossRef - A comparison of endodontic referrals and treatment in the public and private sectors in Western Australia
Charn Thanissorn, Johnson Ye, Daniel Girgis, Nathan van Dort, Paul V. Abbott
Australian Endodontic Journal.2023; 49(S1): 390. CrossRef - Case complexity of root canal treatments accepted for training in a secondary care setting assessed by three complexity grading systems: A service evaluation
Ruby Long, Arindam Dutta, Matthew B. M. Thomas, Morgana Eli Vianna
International Endodontic Journal.2022; 55(11): 1190. CrossRef - Comparing the pulp/tooth area ratio and dentin thickness of mandibular first molars in different age groups: A cone-beam computed tomography study
Mathukan Chaleefong, Sangsom Prapayasatok, Sakarat Nalampang, Phumisak Louwakul
Journal of Conservative Dentistry.2021; 24(2): 166. CrossRef - Survival of molar teeth in need of complex endodontic treatment: Influence of the endodontic treatment and quality of the restoration
Maurits C.F.M. de Kuijper, Eric W. Meisberger, Amarins G. Rijpkema, Cathleen T. Fong, Jantien H.W. De Beus, Mutlu Özcan, Marco S. Cune, Marco M.M. Gresnigt
Journal of Dentistry.2021; 108: 103611. CrossRef - Novel tier 2 service model for complex NHS endodontics
Gareth M. Thomas, Richard Newton, Warren J. Tolley, Karl Bishop
British Dental Journal.2021;[Epub] CrossRef - Assessment of Dentists’ Referral Patterns to Endodontist in Turkey
Öznur SARIYILMAZ, Elif KALYONCUOĞLU
Middle Black Sea Journal of Health Science.2020; 6(2): 220. CrossRef - Characteristics of teeth referred to a dental university hospital for endodontic reason
Su-Jin Jeon, Soo-Jeong Hwang, Min-Seock Seo
Journal of Dental Rehabilitation and Applied Science.2019; 35(3): 143. CrossRef - Characteristics of teeth referred to a public dental specialist clinic in endodontics
D. Sebring, H. Dimenäs, S. Engstrand, T. Kvist
International Endodontic Journal.2017; 50(7): 629. CrossRef
- Monitoring Asymptomatic Apical Periodontitis in Root‐Filled Teeth—Results From a One‐Year Follow‐Up Prospective Study
- 2,141 View
- 7 Download
- 14 Crossref
Case Report
- Mental nerve paresthesia secondary to initiation of endodontic therapy: a case report
- Syed Mukhtar-Un-Nisar Andrabi, Sharique Alam, Afaf Zia, Masood Hasan Khan, Ashok Kumar
- Restor Dent Endod 2014;39(3):215-219. Published online May 8, 2014
- DOI: https://doi.org/10.5395/rde.2014.39.3.215
-
Abstract
PDFPubReaderePub
Whenever endodontic therapy is performed on mandibular posterior teeth, damage to the inferior alveolar nerve or any of its branches is possible. Acute periapical infection in mandibular posterior teeth may also sometimes disturb the normal functioning of the inferior alveolar nerve. The most common clinical manifestation of these insults is the paresthesia of the inferior alveolar nerve or mental nerve paresthesia. Paresthesia usually manifests as burning, prickling, tingling, numbness, itching or any deviation from normal sensation. Altered sensation and pain in the involved areas may interfere with speaking, eating, drinking, shaving, tooth brushing and other events of social interaction which will have a disturbing impact on the patient. Paresthesia can be short term, long term or even permanent. The duration of the paresthesia depends upon the extent of the nerve damage or persistence of the etiology. Permanent paresthesia is the result of nerve trunk laceration or actual total nerve damage. Paresthesia must be treated as soon as diagnosed to have better treatment outcomes. The present paper describes a case of mental nerve paresthesia arising after the start of the endodontic therapy in left mandibular first molar which was managed successfully by conservative treatment.
-
Citations
Citations to this article as recorded by- A series of complications following extrusion of root canal sealer
Bilgesu Kurt, İnci Rana Karaca
Brazilian Journal of Oral Sciences.2026; 25: e266295. CrossRef - Evolving Paradigms in the Management of Trigeminal Nerve Injuries Post Oral Surgery: A Comprehensive Narrative Review
Saanvi Tank, Amit Patil, Tejal Patil, Minal M Kshirsagar, Aarti S Bedia, Sanpreet S Sachdev, Vyshnavi Mundada
Cureus.2025;[Epub] CrossRef - Separated Surgical Instrument During the Extraction of a Third Molar: A Case Report
Abdulaziz A Mahdi, Abdullah I Alkharji, Safa A Alburayh, Bader A Fatani, Osama A Alharbi
Cureus.2025;[Epub] CrossRef - Treatment of paresthesia induced by periapical lesions: a case report
Hyo Jin Jo, Jung-Hong Ha
Journal of Dental Rehabilitation and Applied Science.2024; 40(4): 305. CrossRef - İMPLANT CERRAHİSİ SONRASI HİPOESTEZİ-6 AYLIK TAKİP: VAKA SERİSİ
Sefa AYDINDOĞAN, Emine Elif MUTAFCİLAR VELİOĞLU, Yunus Emre BALABAN
Selcuk Dental Journal.2023; 10(4): 350. CrossRef - Mental Nerve Paraesthesia: A Report of Two Cases Associated with Endodontic Etiology
Neeta Patel, Akshayraj Langaliya, Shikha Kanodia, Aravind Kumbhar, Aastha Buch, Aarshvi Shah, Himani Bhatt, Drashti Panchal, Sharan Shah, Jinali Shah, Darko Macan
Case Reports in Dentistry.2021;[Epub] CrossRef - Anatomic Danger Zones of the Head and Neck
Guy Talmor, Andy Trang, Omeed Ahadiat, Boris Paskhover, Ashley Wysong
Dermatologic Surgery.2020; 46(12): 1549. CrossRef - The anatomical relationship between the roots of erupted permanent teeth and the mandibular canal: a systematic review
Michał Puciło, Mariusz Lipski, Magdalena Sroczyk-Jaszczyńska, Aleksandra Puciło, Alicja Nowicka
Surgical and Radiologic Anatomy.2020; 42(5): 529. CrossRef - Endodontic-related inferior alveolar nerve injuries: A review and a therapeutic flow chart
R. Castro, M. Guivarc'h, J.M. Foletti, J.H. Catherine, C. Chossegros, L. Guyot
Journal of Stomatology, Oral and Maxillofacial Surgery.2018; 119(5): 412. CrossRef - Neuropathy of Trigeminal Nerve Branches After Oral and Maxillofacial Treatment
Jimoh Olubanwo Agbaje, Elke Van de Casteele, Marjolein Hiel, Ciska Verbaanderd, Ivo Lambrichts, Constantinus Politis
Journal of Maxillofacial and Oral Surgery.2016; 15(3): 321. CrossRef - Facial nerve paralysis following endodontic treatment of lower first molar
Umut Demetoglu, Gokhan Ozkan, Hasan Onur Simsek
Journal of Oral and Maxillofacial Surgery, Medicine, and Pathology.2016; 28(3): 267. CrossRef - Broken Endodontic Instrument Caused Inferior Alveolar Nerve Paraesthesia: A Case Report.
M. Ozbek Selcuk, Kaman Süleyman, Ozgur Demiralp Kemal
Journal of Dentistry And Oral Implants.2016; 1(1): 21. CrossRef
- A series of complications following extrusion of root canal sealer
- 4,690 View
- 24 Download
- 12 Crossref
Clinical Research
- Prognostic factors influencing clinical outcome of nonsurgical endodontic treatment
- Seonah Kim
- J Korean Acad Conserv Dent 2010;35(6):436-444. Published online November 30, 2010
- DOI: https://doi.org/10.5395/JKACD.2010.35.6.436
-
Abstract
PDFPubReaderePub
Objectives This study aimed to assess prospectively the clinical outcome of nonsurgical endodontic treatment and identify patient- and tooth-related factors, rather than treatment-related factors, that were the best predictors of this outcome.
Materials and Methods The inception cohort comprised 441 teeth (320 patients) and 175 teeth (123 patients) were followed up for 1-2 years. Age, gender, presence of medical disease, number of canals, previous endodontic treatment, presence of sensitivity and pain, pulp vitality, swelling or sinus tract of pulpal origin on the gingiva, periapical radiolucency and tendency of unilateral bite on the affected tooth were recorded at treatment start.
Results The outcome was classified on the basis of periapical radiolucency as healed or non healed. The overall healed rate in these cases, including nonsurgical retreatment, was 81.1%. Four tooth-related factors had a negative impact in the bivariate analysis: previous endodontic treatment, necrotic pulp, preoperative gingival swelling or sinus tract of pulpal origin, and preoperative periapical radiolucency. Stepwise logistic regression analysis including patient-, tooth-related factors and level of the root canal filling as a treatment-related factor showed that preoperative gingival lesion (odds ratio [OR]: 4.4;
p = 0.005), preoperative periapical radiolucency (OR: 3.6;p = 0.011), and ≤ 1-2 mm under root filling length (OR: 9.6;p = 0.012) were significant predictors of failure.Conclusions A preoperative gingival lesion of pulpal origin can influence the outcome of nonsurgical endodontic treatment in addition to preoperative periapical radiolucency.
-
Citations
Citations to this article as recorded by- Predicting outcomes of nonsurgical retreatment with artificial intelligence: A multicenter retrospective study using logistic regression, random forest, and extreme gradient boosting
Shreshtha Muskan, T. Vigneshwar Sambandam, Pradeep Solete, Giampiero Rossi-Fedele, Gianrico Spagnuolo, Kavalipurapu Venkata Teja, Salvatore Scolavino, Niccolò Giuseppe Armogida
Journal of Conservative Dentistry and Endodontics.2026; 29(4): 373. CrossRef - NON-SURGICAL ENDODONTIC TREATMENT OF CHRONIC APICAL PERIODONTITIS WITH EXTENSIVE PERIAPICAL AND FURCATION BONE DESTRUCTION: A CASE REPORT WITH 18-MONTH FOLLOW-UP
Magomedov Ibragim, Supiev Lugman, Omarov Muslim
BULLETIN OF STOMATOLOGY AND MAXILLOFACIAL SURGERY.2026; : 34. CrossRef - A retrospective study on the prognostic factors and success, survival, and failure outcomes of treated endodontic‐periodontal lesions
Ingar Wong, An Ton, Amiel J. Cassidy, Nicolette Fozzard, Lavanya Ajay Sharma, Robert M. Love, Ajay Sharma
Clinical and Experimental Dental Research.2024;[Epub] CrossRef - Evaluation of gutta-percha removal from the dentinal tubules using different instrumentation techniques with or without solvent: An In vitro study
MukeshKumar Hasija, Babita Meena, Deepti Wadhwa, KulvinderKaur Wadhwani, Virender Yadav
Journal of the International Clinical Dental Research Organization.2020; 12(1): 27. CrossRef - Surgical endodontic management of infected lateral canals of maxillary incisors
Ji-Hyun Jang, Jung-Min Lee, Jin-Kyu Yi, Sung-Baik Choi, Sang-Hyuk Park
Restorative Dentistry & Endodontics.2015; 40(1): 79. CrossRef - Single visit nonsurgical endodontic therapy for periapical cysts: A clinical study
Ipsita Maity, N. Meena, R. Anitha Kumari
Contemporary Clinical Dentistry.2014; 5(2): 195. CrossRef
- Predicting outcomes of nonsurgical retreatment with artificial intelligence: A multicenter retrospective study using logistic regression, random forest, and extreme gradient boosting
- 6,069 View
- 46 Download
- 6 Crossref
Original Articles
- Endodontic flare-ups incidence and related factors
- Hye-Young Jung, Sang-Hyuk Park, Gi-Woon Choi
- J Korean Acad Conserv Dent 2005;30(2):102-111. Published online March 31, 2005
- DOI: https://doi.org/10.5395/JKACD.2005.30.2.102
-
Abstract
PDFPubReaderePub
The purpose of this study was to assess the incidence of flare-ups among patients who received endodontic treatment and to examine the correlation with pre-operative and operative variables.
Analysis was in two aspects (a) overall incidence of flare-ups as expressed by a percentage of all patients visits and (b) percentage of flare-ups that occurred as related to various factors such as patient demographics, diagnosis, and treatment procedures.
1. From the 840 teeth which were examined in this study, the total number of flare-ups was 13.
2. As to gender of patients, there was no significant difference in flare-ups.
3. As to tooth groups, there was no significant difference in flare-ups.
4. In the teeth with pre-operative symptom, there was a statistically significant higher incidence of flare-ups than the teeth without it.
5. In the teeth with apical periodontitis, there was a statistically significant higher incidence of flare-ups.
6. As to pulp and periapical status, non-vital teeth had a higher incidence as compared with vital teeth, irreversible pulpitis.
7. Multi-visit treatment resulted in the higher incidence of flare-ups than one visit treatment.
8. Re-treatment procedures had a statistically significant higher incidence of flare-ups than root canal treatment.
In this study, overall percentages of flare-ups was 1.55%. It showed a statistically significant higher incidence related to pre-operative symptom, apical periodontitis, and re-treatment. There was no significant difference in flare-ups related to gender, tooth groups, and fistula.
- 2,380 View
- 29 Download
- Three dimensional reconstruction of teeth using x-ray microtomography
- Dong-Hoon Shin
- J Korean Acad Conserv Dent 2003;28(6):485-490. Published online November 30, 2003
- DOI: https://doi.org/10.5395/JKACD.2003.28.6.485
-
Abstract
PDFPubReaderePub
Complete understanding of the exterior and interior structure of the tooth would be prerequisite to the successful clinical results, especially in the restorative and endodontic treatment.
Although three-dimensional reconstruction method using x-ray microtomography could not be used in clinical cases, it may be the best way to reconstruct the morphologic characteristics of the tooth structure in detail without destructing the tooth itself. This study was done to three dimensionally reconstruct every teeth in the arch in order to increase the understanding about the endodontic treatment and to promote the effective restorative treatment by upgrading the knowledge of the tooth morphology.
After placing tooth between the microfocus x-ray tube and the image intensifier to obtain two-dimensional images of each level, scanning was done under the condition of 80 keV, 100 µA, 16.8 magnification with the spot size of 8 µm. Cross-section pixel size of 16.28 µm and 48.83 cross-section to cross-section distance were also used.
From the results of this study, precise three dimensional reconstructed images of every teeth could be obtained. Furthermore, it was possible to see image that showed interested area only, for example, enamel portion only, pulp and dentin area without enamel structure, pulp only, combination image of enamel and pulp, etc.
It was also possible to see transparent image without some part of tooth structure. This image might be used as a guide when restoring and preparing the full and partial crown by showing the positional and morphological relationship between the pulp and the outer tooth structure.
Another profit may be related with the fact that it would promote the understanding of the interior structure by making observation of the auto-rotating image of .AVI file from the various direction possible.
-
Citations
Citations to this article as recorded by- Fracture Flow of Radionuclides in Unsaturated Conditions at LILW Disposal Facility
Won-Seok Kim, Jungjin Kim, Jinmo Ahn, Seongsik Nam, Wooyong Um
Journal of Korean Society of Environmental Engineers.2015; 37(8): 465. CrossRef
- Fracture Flow of Radionuclides in Unsaturated Conditions at LILW Disposal Facility
- 1,728 View
- 1 Download
- 1 Crossref
 First
First Prev
Prev

