
Articles
- Page Path
- HOME > Restor Dent Endod > Volume 40(3); 2015 > Article
- Review Article A review of the regenerative endodontic treatment procedure
- Bin-Na Lee1, Jong-Wook Moon2, Hoon-Sang Chang1, In-Nam Hwang1, Won-Mann Oh1, Yun-Chan Hwang1
-
2015;40(3):-187.
DOI: https://doi.org/10.5395/rde.2015.40.3.179
Published online: March 16, 2015
1Department of Conservative Dentistry, School of Dentistry, Dental Science Research Institute, Chonnam National University, Gwangju, Korea.
2School of Dentistry, Chonnam National University, Gwangju, Korea.
- Correspondence to Yun-Chan Hwang, DDS, MSD, PhD. Professor, Department of Conservative Dentistry, School of Dentistry, Chonnam National University, 77 Young-bong ro, Bukgu, Gwangju, Korea 500-757. TEL, +82-62-530-5831; FAX, +82-62-530-5629; ychwang@chonnam.ac.kr
• Received: January 7, 2014 • Accepted: January 29, 2015
©Copyrights 2015. The Korean Academy of Conservative Dentistry.
This is an Open Access article distributed under the terms of the Creative Commons Attribution Non-Commercial License (http://creativecommons.org/licenses/by-nc/3.0/) which permits unrestricted non-commercial use, distribution, and reproduction in any medium, provided the original work is properly cited.
- 8,358 Views
- 134 Download
- 65 Crossref
Abstract
- Traditionally, apexification has been used to treat immature permanent teeth that have lost pulp vitality. This technique promotes the formation of an apical barrier to close the open apex so that the filling materials can be confined to the root canal. Because tissue regeneration cannot be achieved with apexification, a new technique called regenerative endodontic treatment was presented recently to treat immature permanent teeth. Regenerative endodontic treatment is a treatment procedure designed to replace damaged pulp tissue with viable tissue which restores the normal function of the pulp-dentin structure. After regenerative endodontic treatment, continued root development and hard tissue deposition on the dentinal wall can occur under ideal circumstances. However, it is difficult to predict the result of regenerative endodontic treatment. Therefore, the purpose of this study was to summarize multiple factors effects on the result of regenerative endodontic treatment in order to achieve more predictable results. In this study, we investigated the features of regenerative endodontic treatment in comparison with those of other pulp treatment procedures and analyzed the factors that have an effect on regenerative endodontic treatment.
Introduction
The purpose of pulp treatment is to maintain the tooth structure intact in order to preserve optimal function. Maintaining the vitality of teeth damaged due to dental caries or trauma is also one of the purposes of pulp treatment. Especially, in case of immature permanent teeth, maintaining the pulp vitality is essential for continuous root development and apical closure. If the pulp of immature permanent teeth is infected, apexification that includes removal of the infected pulp and application of calcium hydroxide has been performed traditionally.1 Calcium hydroxide is the material of choice for closing the apical foramen. However, while apexification can induce apical closure, it cannot maintain pulp vitality.2 Recently, regenerative endodontic treatment procedure has been suggested in order to replace the damaged pulp tissue with the viable tissue. Especially when the tooth is damaged by trauma, pulp regenerative endodontic treatment is performed because the pulp tissue is uninfected. On the other hand, when apical periodontitis is associated with tooth infection, regenerative endodontic treatment procedure is not considered. But recently, a case report demonstrated continuous root develoment and apical closure with the application of antibiotics.3 Procedures used in this case reports are based on the concept that stem cells have self-regenerating capacity and are multipotent. Stem cells are used to induce pulp regeneration so as to treat immature permanent teeth in a conservative way.4
In apexification, calcium hydroxide is used as an intracanal medication, which should be replaced every 3 months, and a long-term follow-up is necessary. Long-term application of the intra-canal medication increases the possibility of root fracture and developing defects in the root walls due to its porous characteristics.1,2 On the other hand, regenerative endodontic treatment can result in complete root development after a short-term treatment procedure. Thus, regenerative endodontic treatment causes an increase in root length and thickness.3,5,6,7,8,9
Regenerative endodontic treatment is a procedure that involves disinfection of the root canal with the use of antibiotics. Multiple aerobic and anaerobic bacteria cause infection of the root canals, and hence it is difficult to disinfect the canals effectively with just one type of antibiotic. Therefore, Hoshino and Sato recommended a combination of three antibiotics including ciprofloxacin, metronidazole, minocycline.10,11 In this study, various aspects of regenerative endodontic treatment such as clinical features, biological features, and their effects on regenerative endodontic treatment are discussed.
Review
Since many types of regenerative endodontic treatment procedures have been suggested, it is important to have knowledge of the procedure that is generally used. The American Association of Endodontics (AAE) suggests that regenerative endodontic treatment can be used for teeth of a compliant patient with necrotic pulp, an immature apex, and pulp space not needed for post and core. At the first appointment for regenerative endodontic treatment, risks and potential benefits should be explained to the patient after collecting the clinical information and establishing a pulpal and periradicular diagnosis. The tooth is anesthetized and isolated with rubber dam for creating an access opening. Copious, gentle irrigation with 20 mL sodium hypochlorite (NaOCl) using an irrigation system that minimizes the possibility of extrusion of irrigants into the periapical space and lower concentrations of NaOCl are advised to minimize cytotoxicity to stem cells in the apical tissues. The root canal is then dried with sterile paper points, and the antimicrobial medicament is applied into the canal space. A triple antibiotic paste is applied to disinfect the canal space.12 The triple antibiotic paste has the advantage of being a very effective antibiotic combination against intracanal microorganisms.10,11 On the other hand, calcium hydroxide has the advantage of being widely available, but it may be cytotoxic to stem cells.13 After the antimicrobial medicament is applied, the tooth is sealed with a temporary filling, and the patient should be asked to visit for a check-up after 3 to 4 weeks.
At the second appointment, the patient is evaluated for resolution of signs or symptoms of an acute infection. If there are no symptoms or signs of infection, it is appropriate to proceed with the next step of the regenerative endodontic treatment. Local anesthetic without vasocontrictors is recommended at this appointment to avoid the disturbance of intracanal bleeding. After rubber dam isolation and making a coronal access opening, the tooth is irrigated with 20 mL of ethylenediamine tetraacetic acid, followed by normal saline, and the antimicrobial medicament is carefully removed. After drying the canal with a paper point, a file is placed a few milimeters beyond the apical foramen and bleeding is induced up to 3 mm from the cemento-enamel junction (CEJ). To position the mineral trioxide aggregate (MTA), Colla-Plug, which serves as a resorbable matrix, is placed into the canal. Then about 3 mm of MTA is placed, followed by placement of the final restoration.12 A 12 to 18 month recall is probably the minimal time to judge radiographic evidence of root development and to conduct the clinical examination.13
There are several treatment options for a necrotic or infected immature permanent tooth. Traditionally, the apexification procedure has been recommended for treating an immature tooth with an open apex. Apexification is a procedure that promotes the formation of an apical barrier to prevent the extrusion of filling materials.14 Materials such as calcium hydroxide which are capable of forming a calcified apical barrier are used for apexification. Although calcium hydroxide can be used to form a calcified apical barrier, it has some drawbacks.2 The most critical drawback is the reduction in root strength due to the use of calcium hydroxide, and this increases the possibility of root fracture. Another drawback is the long time span of the entire treatment. At least 6 months are required to create an apical barrier, and mulitple visits are needed to replenish calcium hydroxide.15 Due to these drawbacks, alternative apexification methods have been proposed recently. MTA has been proposed as a material to create an apical barrier that prevents the extrusion of obturation materials. In comparison with calcium hydroxide, MTA is used in the one or two step apexification procedure, and therefore a fewer number of appointments are needed.13 In spite of this advantage, apexification with MTA neither strengthens the root nor induces further root development. As a result, the roots remain thin and fragile, and hence another treatment approach is needed.14 It has been recently suggested that regenerative endodontic treatment can be alternative approach of apexification. Regenerative endodontic treatment has the advantages of further root development and reinforcement of dentinal walls by deposition of hard tissue, thus strengthening the root against fracture.16 The characteristics of three treatment procedures are summarized in Table 1.
Considering these characteristics, regenerative endodontic treatment seems to be the most effective procedure. However, without clinical data of comparison of the outcomes of these three treatment procedures, it is difficult to determine which procedure is the most effective to treat an immature tooth with a necrotic pulp. Jeeruphan conducted a retrospective study about the comparison of radiographic and survival outcomes of immature teeth treated with either regenerative endodontic treatment or apexification. A total of 61 cases were included in this study. The cases included regenerative endodontic treatment (20 cases), apexification with MTA (19 cases), and apexification with calcium hydroxide (22 cases). In this retrospective study, the percentage increase in root width and root length after the treatment procedure was analyzed using radiographic data (Table 2).14
Immature teeth treated with regenerative endodontic treatment showed a significantly higher percentage increase in root width (28.2%) and root length (14.9%) as compared with teeth treated by either apexification with MTA (percentage increase in root width, 0.00% and percentage increase in root length, 6.1%) or apexification with calcium hydroxide (percentage increase in root width, 1.52% and percentage increase in root length, 0.4%).14 The results of this study indicated that regenerative endodontic treatment has the advantage of promoting further root development and thickening of dentinal walls by hard tissue deposition.
Regenerative endodontic treatment can occur in infected immature permanent teeth because of mesenchymal stem cells which exist in the apical papilla of immature teeth. These stem cells from the apical papilla (SCAP) are capable of differentiating into odontoblast-like cells forming root dentin.4,17 Another type of mesenchymal cells, which are called dental pulp stem cells (DPSCs) were discovered and isolated earlier, and DPSCs have the ability to differentiate into odontoblast-like cells and form dentin/pulp-like complex when implanted into subcutaneous spaces of immunocompromised mice.18 Both SCAP and DPSCs are as potent in osteo/dentinogenic differentiation as mesenchymal cells from bone marrows, whereas they are weaker in adipogenic potential.17 SCAP and DPSCs show similar features, but they have some differences. In order to examine the differences between SCAP and DPSCs, both cells were isolated from the same tooth and cultured under the same conditions.4 It was found that SCAP showed a significantly greater bromodeoxyuridine uptake rate (an indication of cell proliferation), number of population doublings, and tissue regeneration capacity than DPSCs (Table 3). These evidences suggest that SCAP derived from a developing tissue may be a superior cell source for tissue regeneration.19
There are some factors that affect the results of regenerative endodontic treatment. To achieve successful results of the treatment procedure, a thorough understanding of these factors is very important. The first factor is the disinfection of the canal. During the early stage of research, the regenerative endodontic treatment of pulp tissue in an infected tooth was thought to be impossible. The first attempt at regenerative endodontic treatment of an avulsed immature tooth with necrotic non-infected pulp was successful.3 Therefore, researchers suggested that regenerative endodontic treatment will occur if it was possible to create an environment similar to the avulsed tooth. In other words, if the canals were effectively disinfected and the coronal access was effectively sealed, regenerative endodontic treatment should occur as in an avulsed tooth. To disinfect the canal, many types of medications are used nowadays.3
The second factor is the apex diameter. A tooth with an open apex allows the migration of mesenchymal stem cells into the root canal space, and this could allow host cell homing to form new tissue in the root canal space.20,21 An apical opening of 1.1 mm in diameter or larger is beneficial, with natural regenerative endodontic treatment occurring in approximately 18% to 34% of teeth with immature roots.22
The third factor is the patient age. Several case reports of regenerative endodontic treatment procedures have generally been limited to patients who are reaching adolescence, mostly aged from 8 - 16 years.3,6,22,23 Based on these case reports, it would not be advisable to perform regenerative endodontic treatment procedures in children younger than 8 years or older than 16 years. Also, regenerative endodontic treatment procedure should not be performed on deciduous teeth, because of the possible risk of impairing the eruption pattern of permanent teeth.22 The three factors that affect the results of regenerative endodontic treatment are summarized in Table 4.
Banchs and Trope reported successful multiple visit regenerative endodontic treatment of the lower right second premolar in an 11 year-old boy.3 During the first visit, access opening, canal irrigation and application of tri-antibiotic paste were performed. The patient returned 26 days later for the second visit, and after this a two year follow-up was performed. During this period, the radiograph showed closure of the apex and thickening of the dentinal walls.3 Chueh and Huang also suggested multiple visit regenerative endodontic treatment to achieve successful results.23 Regenerative endodontic treatment of an immature tooth was performed in a 10 year-old girl. During the first visit, an access cavity was made, followed by canal irrigation and application of tri-antibiotic paste. Thirty-five months after the initial treatment, the radiographs showed a reduction of the root canal space and maturation of the root apex.23 In contrast, Shin et al. performed single visit regenerative endodontic treatment of the lower right second premolar in a 12 year-old girl.6 An access cavity was made, and the coronal portion of the canal was irrigated with 10 mL of 6% NaOCl. After rinsing the canal with sterile saline solution, the canal was irrigated with 10 mL of 2% chlorhexidine gluconate and it was allowed to remain in the canal for 5 minutes. The canal was dried with paper points and MTA was placed into the canal. Finally, the access cavity was filled with resin-bonded composite restoration. At the 13 and 19 month follow-up, the radiographs showed evidence of complete periradicular bone healing and root maturation. In this case, a single visit regenerative endodontic treatment protocol was successful, because the tooth exhibited partial pulpal necrosis. If the tooth had complete pulpal necrosis, this protocol would not have been successful. Therefore, it seems that a multiple visit protocol using a tri-antibiotic paste may be better treatment option for teeth with complete pulpal necrosis. Hence, case selection is critical when deciding which regenerative endodontic treatment protocol is ideal for a particular pulpal condition.6 The above three cases of regenerative endodontic treatment are summarized in Table 5.
In 1996, Hoshino et al. recommended a tri-antibiotic paste, which was composed of ciprofloxacin, metronidazole, and minocycline, to disinfect the canal, and this medicament can be used effectively in regenerative endodontic treatment.10 On the other hand, Chueh et al. reported that complete disinfection of the canal and regeneration can be achieved by using calcium hydroxide alone.24 In 2009, Bose et al. analyzed cases of regenerative endodontic treatment performed all over the world.13 Regenerative endodontic treatment with the triple antibiotic paste, calcium hydroxide, and formocresol produced significantly greater increases in root length and width compared with that in the control group. There were no significant differences in root length among the three groups of medicaments. In terms of changes in root width, the triple antibiotic paste produced significantly greater increases in dentin wall thickness compared with the other two medicament groups.12,13 Although application of the triple antibiotic paste can be effective, drawbacks of the triple antibiotic paste have been reported recently. Ding et al. reported that two patients suffered from pain after the application of the triple antibiotic paste, and they were excluded from the research.25 Jung et al. reported the development of a persistent sinus tract after using triple antibiotic paste.26 They replaced this intracanal medicament with calcium hydroxide, after which the symptoms of the patient settled down.26
Especially, when the triple antibiotic paste is placed in contact with the anterior teeth, discoloration can occur. According to Kim et al., minocycline, which is one of the components of the triple antibiotic paste is the main cause of tooth discoloration. Minocycline can penetrate the tooth through dentinal tubules, and it can integrate with the crystal structure of the tooth.27 Administration of minocycline is contraindicated in pregnant women who are in the 3rd trimester or in children who are under 8 years of age, due to the induction of tooth discoloration, reduction of bone growth, and amelogenesis imperfecta.28 Reynolds reported the methods to prevent tooth discoloration. One method is sealing the coronal dentin wall with flowable resin before application of the triple antibiotic paste, and the other method is retrograde filling of antibiotics with 20 gauge needle to minimize the contact with the coronal part of teeth.27 There are case reports suggesting that cefaclor, amoxicillin should be used instead of minocycline. But amoxicillin has side effects such as an allergic reaction.29
Another material that is used in the regenerative endodontic treatment procedure is MTA. The coronal space is usually filled with MTA after inducing bleeding with a file. The reason why MTA is used in regenerative endodontic treatment is that MTA has a remarkable biocompatibility and sealing ability. MTA is also able to set in a moist environment such as the bleeding area of the tooth.30
In conclusion, there are no guidelines regarding which medicament should be used for regenerative endodontic treatment for specific situations, and the results of regenerative endodontic treatment are at odds with the medicaments that are used for treatment. Therefore, disinfection of canals and preservation of the tissue vitality are more important than selection of the medicament. If these factors can be controlled, successful results of the regenerative endodontic treatment procedure can be obtained.
Regenerative endodontic treatment is based on the concept that multipotent stem cells from the apical area are able to induce pulp regeneration in immature permanent teeth. As a result of this concept, the treatment becomes more conservative.2,4 SCAP are known to have a greater differentiation capacity than other stem cells and they are loosely attached to the root apical area. The root apical area contains an abundant number of stem cells which are responsible for root development. Even when the pulp becomes necrotic, SCAP are able to maintain their vitality through collateral circulation.31 The size of the apical foramen is an important factor that needs to be considered for successful regenerative endodontic treatment. Regenerative endodontic treatment of avulsed teeth was more successful when the diameter of the apical foramen was greater than 1.1 mm. This is because a bigger size of apical foramen allows more blood to be supplied.22 In terms of the frequency of application of antibiotics for treatment of infected root canal, it was found that repeated application of antibiotics increases their antibacterial efficacy.10 A combination of three antibiotics is very effective in disinfecting dentin in the root. This triple antibiotic paste is composed of ciprofloxacin, metronidazole, and minocycline in a 1 : 1 : 1 ratio.10,11 The drawbacks of the triple antibiotic paste such as discoloration of the crown, increase in bacterial resistance and allergic reactions have been reported.32 MTA is being used as the final canal filling material when the tooth is treated by the regenerative endodontic treatment procedure.3,25 MTA allows cell proliferation and cell attachment because it has less cytotoxicity and good biocompatibility.31 These characteristics enhance the tissue healing process and prevent the weakening of the dentin structure which was caused by long-term administration of calcium hydroxide.33 The regenerative endodontic treatment procedure is based on the conservative concept that recommends treatment by induction of pulp regeneration; however, if the procedure fails, conventional root canal therapy should be performed. Therefore, dentists should explain to the patients that there is a possibility that conventional root canal therapy may be performed before the initiation of regenerative endodontic treatment procedure. Especially for the treatment of molars, the regenerative endodontic treatment procedure has many disadvantages such as discoloration of root canal and access cavity, limited access due to canal calcification, and difficulty in MTA removal. Therefore, prudent case selection is important and when applying MTA, local application of MTA over the canal orifice is recommended. After filling the canals with MTA, a periodic check-up is necessary.
Conclusions
Recently many cases of regenerative endodontic treatment of teeth with infected canals have been reported. But these cases do not provide clinical results such as the long-term success rate of regenerative endodontic treatment. Therefore, to achieve successful results of the regenerative endodontic treatment procedure, prudent case selection and a long-term follow-up are considered to be very important.
Acknowledgement
This study was supported by the National Research Foundation of Korea grant funded by the Korea government (MSIP) (no. 2011-0030121) and Chonnam National University, 2013.
- 1. Rafter M. Apexification: a review. Dent Traumatol 2005;21:1-8.ArticlePubMed
- 2. Huang GJ. Apexification: the beginning of its end. Int Endod J 2009;42:855-866.ArticlePubMed
- 3. Banchs F, Trope M. Revascularization of immature permanent teeth with apical periodontitis: new treatment protocol? J Endod 2004;30:196-200.ArticlePubMed
- 4. Huang GT, Sonoyama W, Liu Y, Liu H, Wang S, Shi S. The hidden treasure in apical papilla: the potential role in pulp/dentin regeneration and bioroot engineering. J Endod 2008;34:645-651.ArticlePubMedPMC
- 5. Shah N, Logani A, Bhaskar U, Aggarwal V. Efficacy of revascularization to induce apexification/apexogensis in infected, nonvital, immature teeth: a pilot clinical study. J Endod 2008;34:919-925.ArticlePubMed
- 6. Shin SY, Albert JS, Mortman RE. One step pulp revascularization treatment of an immature permanent tooth with chronic apical abscess: a case report. Int Endod J 2009;42:1118-1126.ArticlePubMed
- 7. Forghani M, Parisay I, Maghsoudlou A. Apexogenesis and revascularization treatment procedures for two traumatized immature permanent maxillary incisors: a case report. Restor Dent Endod 2013;38:178-181.ArticlePubMedPMC
- 8. Hotwani K, Sharma K. Platelet rich fibrin - a novel acumen into regenerative endodontic therapy. Restor Dent Endod 2014;39:1-6.ArticlePubMedPMC
- 9. Goyal L. Clinical effectiveness of combining platelet rich fibrin with alloplastic bone substitute for the management of combined endodontic periodontal lesion. Restor Dent Endod 2014;39:51-55.ArticlePubMedPMC
- 10. Hoshino E, Kurihara-Ando N, Sato I, Uematsu H, Sato M, Kota K, Iwaku M. In-vitro antibacterial susceptibility of bacteria taken from infected root dentine to a mixture of ciprofloxacin, metronidazole and minocycline. Int Endod J 1996;29:125-130.ArticlePubMed
- 11. Sato I, Ando-Kurihara N, Kota K, Iwaku M, Hoshino E. Sterilization of infected root-canal dentine by topical application of a mixture of ciprofloxacin, metronidazole and minocycline in situ. Int Endod J 1996;29:118-124.ArticlePubMed
- 12. Hargreaves KM, Law AS. Regenerative Endodontics. In: Hargreaves KM, Cohen S, editors. Pathways of the Pulp. 10th ed. St Louis, MO: Mosby Elsevier; 2011. p. 602-619.
- 13. Bose R, Nummikoski P, Hargreaves K. A retrospective evaluation of radiographic outcomes in immature teeth with necrotic root canal systems treated with regenerative endodontic procedures. J Endod 2009;35:1343-1349.ArticlePubMed
- 14. Jeeruphan T, Jantarat J, Yanpiset K, Suwannapan L, Khewsawai P, Hargreaves KM. Mahidol study 1: comparison of radiographic and survival outcomes of immature teeth treated with either regenerative endodontic or apexification methods: a retrospective study. J Endod 2012;38:1330-1336.ArticlePubMed
- 15. Andreasen JO, Farik B, Munksgaard EC. Long-term calcium hydroxide as a root canal dressing may increase risk of root fracture. Dent Traumatol 2002;18:134-137.ArticlePubMedPDF
- 16. Witherspoon DE, Small JC, Regan JD, Nunn M. Retrospective analysis of open apex teeth obturated with mineral trioxide aggregate. J Endod 2008;34:1171-1176.ArticlePubMed
- 17. Sonoyama W, Liu Y, Yamaza T, Tuan RS, Wang S, Shi S, Huang GT. Characterization of the apical papilla and its residing stem cells from human immature permanent teeth: a pilot study. J Endod 2008;34:166-171.ArticlePubMedPMC
- 18. Gronthos S, Mankani M, Brahim J, Robey PG, Shi S. Postnatal human dental pulp stem cells (DPSCs) in vitro and in vivo. Proc Natl Acad Sci U S A 2000;97:13625-13630.ArticlePubMedPMC
- 19. Sonoyama W, Liu Y, Fang D, Yamaza T, Seo BM, Zhang C, Liu H, Gronthos S, Wang CY, Wang S, Shi S. Mesenchymal stem cell-mediated functional tooth regeneration in swine. PLoS One 2006;1:e79.ArticlePubMedPMC
- 20. Lovelace TW, Henry MA, Hargreaves KM, Diogenes A. Evaluation of the delivery of mesenchymal stem cells into the root canal space of necrotic immature teeth after clinical regenerative endodontic procedure. J Endod 2011;37:133-138.ArticlePubMed
- 21. Kim JY, Xin X, Moioli EK, Chung J, Lee CH, Chen M, Fu SY, Koch PD, Mao JJ. Regeneration of dental-pulp-like tissue by chemotaxis-induced cell homing. Tissue Eng Part A 2010;16:3023-3031.ArticlePubMedPMC
- 22. Garcia-Godoy F, Murray PE. Recommendations for using regenerative endodontic procedures in permanent immature traumatized teeth. Dent Traumatol 2012;28:33-41.ArticlePubMed
- 23. Chueh LH, Huang GT. Immature teeth with periradicular periodontitis or abscess undergoing apexogenesis: a paradigm shift. J Endod 2006;32:1205-1213.ArticlePubMed
- 24. Chueh LH, Ho YC, Kuo TC, Lai WH, Chen YH, Chiang CP. Regenerative endodontic treatment for necrotic immature permanent teeth. J Endod 2009;35:160-164.ArticlePubMed
- 25. Ding RY, Cheung GS, Chen J, Yin XZ, Wang QQ, Zhang CF. Pulp revascularization of immature teeth with apical periodontitis: a clinical study. J Endod 2009;35:745-749.ArticlePubMed
- 26. Jung IY, Lee SJ, Hargreaves KM. Biologically based treatment of immature permanent teeth with pulpal necrosis: a case series. J Endod 2008;34:876-887.ArticlePubMed
- 27. Kim JH, Kim Y, Shin SJ, Park JW, Jung IY. Tooth discoloration of immature permanent incisor associated with triple antibiotic therapy: a case report. J Endod 2010;36:1086-1091.ArticlePubMed
- 28. Dummett CO, Thikkurissy S. Anomalies of the developing dentition. In: Casamassimo PS, Fields HW, McTigue DJ, Nowak A, editors. Pediatric dentistry. Infancy through adolescence. 5th ed. Philadelphia: WB Saunders Co.; 2013. p. 54-80.
- 29. Thomson A, Kahler B. Regenerative endodontics-biologically-based treatment for immature permanent teeth: a case report and review of the literature. Aust Dent J 2010;55:446-452.ArticlePubMed
- 30. D'Arcangelo C, D'Amario M. Use of MTA for orthograde obturation of nonvital teeth with open apices: report of two cases. Oral Surg Oral Med Oral Pathol Oral Radiol Endod 2007;104:e98-e101.ArticlePubMed
- 31. Huang GT. A paradigm shift in endodontic management of immature teeth: conservation of stem cells for regeneration. J Dent 2008;36:379-386.ArticlePubMed
- 32. Reynolds K, Johnson JD, Cohenca N. Pulp revascularization of necrotic bilateral bicuspids using a modified novel technique to eliminate potential coronal discolouration: a case report. Int Endod J 2009;42:84-92.ArticlePubMed
- 33. Osorio RM, Hefti A, Vertucci FJ, Shawley AL. Cytotoxicity of endodontic materials. J Endod 1998;24:91-96.ArticlePubMed
REFERENCES
Figure 1
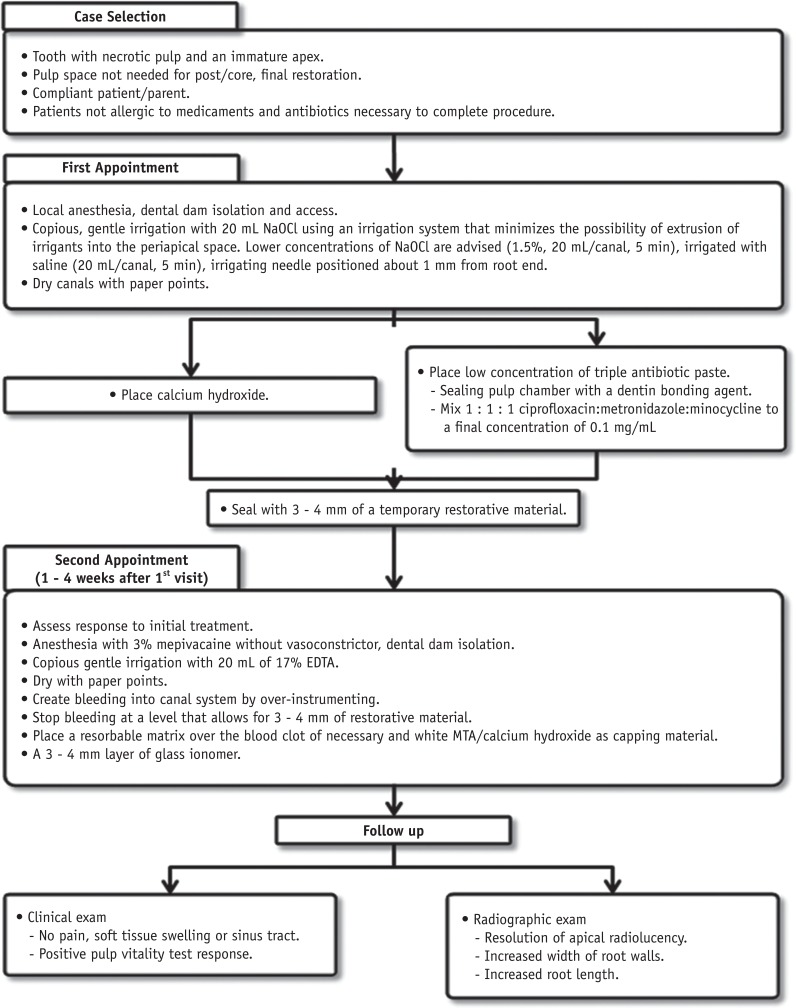
The current considerations for regenerative endodontic treatment procedures (Courtesy of the American Association of Endodontics). NaOCl, sodium hypochlorite; EDTA, ethylenediaminetetraacetic acid; MTA, mineral trioxide aggregate.
Table 1
The characteristics of three treatment procedures for immature root formation
Table 2
The percentage increase in root width and root length after the treatment procedure
| Revascularization | Apexification with MTA | Apexification with calcium hydroxide | |
|---|---|---|---|
| Root width | 28.2% | 0.00% | 1.52% |
| Root length | 14.9% | 6.1% | 0.4% |
Table 3
Comparison between stem cells from the apical papilla (SCAP) and dental pulp stem cells (DPSCs)
Table 4
Factors that affect the results of revascularization
Table 5
Case reports of multiple visit & single visit revascularization
Tables & Figures
REFERENCES
Citations
Citations to this article as recorded by 
- Efficacy of combined scaffolds and sodium hypochlorite in regenerative endodontics of immature teeth (in-vivo study)
Hanan Arb, Abeer Darrag, Neveen Shaheen, Dina Attia
Tanta Dental Journal.2026; 23(2): 240. CrossRef - Outcome evaluation of regenerative endodontic procedures using platelet derivatives: a systematic review and meta-analysis of animal models
Nafsika Alevizou, Konstantinos Kodonas, Anastasia Fardi, Christos Gogos
Odontology.2026;[Epub] CrossRef - Evaluation of the Clinical Outcomes of Regenerative Endodontic Procedures Using Autologous Platelet Concentrate: A Systematic Review and Meta-Analysis
Elnaz Mousavi, Navid Nasrabadi, Samira Jamali, Arian Haddadi
Pesquisa Brasileira em Odontopediatria e Clínica Integrada.2025;[Epub] CrossRef - Antimicrobial 3D printed gelatin scaffolds for root canal disinfection in regenerative endodontics procedures
Mateo Dallos Ortega, Jenny Aveyard, Raghda Magdy Abdelgawad, Reem El-Gendy, Alexander Ciupa, David Whetnall, Julia Behnsen, Robert J. Poole, Raechelle A. D'Sa
Biomaterials Science.2025; 13(14): 3795. CrossRef - Regenerative Endodontic Therapies: Harnessing Stem Cells, Scaffolds, and Growth Factors
Rosana Farjaminejad, Samira Farjaminejad, Franklin Garcia-Godoy
Polymers.2025; 17(11): 1475. CrossRef - Effects of combining hyaluronic acid hydrogel with injectable platelet rich fibrin on apical papilla stem cells proliferation and differentiation
Azal H. Al-Masoody, Nasrin Asadi, Hadiseh Mohammadpour, Mahshid Hodjat, Tahereh Sadat Jafarzadeh Kashi
BMC Oral Health.2025;[Epub] CrossRef - Experts consensus on management of tooth luxation and avulsion
Ruijie Huang, Chenchen Zhou, Ling Zhan, Yuan Liu, Xian Liu, Qin Du, Jun Wang, Wei Zhao, Guangtai Song, Li-an Wu, Beizhan Jiang, Yanhong Li, Hongmei Zhang, Jing Zou
International Journal of Oral Science.2024;[Epub] CrossRef - A review of tissue engineering in regenerative endodontic treatment
Eric Priyo Prasetyo, Dian Agustin Wahjuningrum, Galih Sampoerno, Wilson Sukandar, Shafy Shariz Bin Sharizal, Nurfahira Paidal, Menza Fadiyan Amriel, Nathania Elita Gunawan, Ketut Suardita, Evelyn Tjendronegoro
Conservative Dentistry Journal.2024; 14(1): 1. CrossRef - Innovative Paradigms and Established Strategies in Tooth Revitalization: A Review
Ahmad Shah Khan, Zahid Mehmood Khan, Palwasha Ishaque, Muhammad Zubair, Syeda Fatima Tu Zahra, Sana Ashfaq
Dental Update.2024; 51(8): 570. CrossRef - Explore the most recent developments and upcoming outlooks in the field of dental nanomaterials
Ali Alsuraifi, Zainab M. Sulaiman, Noor Alhuda R. Mohammed, Jassim Mohammed, Sarah Kareem Ali, Yousef Husam Abdualihamaid, Fatimah Husam, Abdullah Ayad
Beni-Suef University Journal of Basic and Applied Sciences.2024;[Epub] CrossRef - Recent Advances in Regenerative Endodontics: A Review of Current Techniques and Future Directions
Firas A Alothman, Lamia S Hakami, Ali Alnasser, Faris M AlGhamdi, Abdullah A Alamri, Basel M Almutairii
Cureus.2024;[Epub] CrossRef - Regenerative Potential of Dental Pulp Stem Cells in Response to a Bioceramic Dental Sealer and Photobiomodulation: An In Vitro Study
Hamed A Alshawkani, Mohamed Mansy, Mahmoud Al Ankily, Mohamed Shamel
The Journal of Contemporary Dental Practice.2024; 25(4): 313. CrossRef - Marginal adaptation of customized gutta percha cone with calcium silicate based sealer versus MTA and biodentine apical plugs in simulated immature permanent teeth (an in vitro study)
Mary M. Mina, Sybel M. Moussa, Mahmoud R. Aboelseoud
BMC Oral Health.2024;[Epub] CrossRef - GelMA‐based hydrogel biomaterial scaffold: A versatile platform for regenerative endodontics
Lei Huang, Xuan Chen, XiaoXia Yang, Yinchun Zhang, Xiaoling Qiu
Journal of Biomedical Materials Research Part B: Applied Biomaterials.2024;[Epub] CrossRef - Regenerative Endodontic Treatment in Dentinogenesis Imperfecta‐Induced Apical Periodontitis
Ying Liao, Ting Pan, Xianghui Xing, Sivakumar Nuvvula
Case Reports in Dentistry.2024;[Epub] CrossRef - In vitro and in vivo evaluation of iRoot BP Plus as a coronal sealing material for regenerative endodontic procedures
Ning Yang, Wenxiao Yang, Rou Shen, Shengcai Zhang, Tianchi Ma, Yao Liu
Clinical Oral Investigations.2024;[Epub] CrossRef - Comparative evaluation of pH and Ca+ ion release from MTA on interaction with platelet-rich fibrin and blood clot: an in vitro study
Sonia Khatri, Sylvia Mathew, Shruthi Nagaraja, Swaroop Hegde, Soumyadeep Ghosh, Kavimalar Ravichandran
F1000Research.2023; 12: 364. CrossRef - Photobiomodulation Therapy and Pulp-Regenerative Endodontics: A Narrative Review
Jiawen Yong, Sabine Gröger, Zuping Wu, Sabine Ruf, Yuer Ye, Xiaoyan Chen
Bioengineering.2023; 10(3): 371. CrossRef - Efficacy of disinfection procedures performed prior to regenerative endodontic therapy: An integrative review
Ketillyn da Silva Magalhães, Ana Clara Kuerten Gil, Taynara Santos Goulart, Daniela Peressoni Vieira Schuldt, Beatriz Serrato Coelho, Daniela de Rossi Figueiredo, Lucas da Fonseca Roberti Garcia, Josiane de Almeida
Australian Endodontic Journal.2023; 49(2): 418. CrossRef - Newer Prospects of Regenerative Endodontics: A Comprehensive and Updated Review of Literature
Mohammad Kamran Khan, Mahendra Kumar Jindal
Journal of the Scientific Society.2023; 50(3): 299. CrossRef - Comparative evaluation of pH and Ca+ ion release from MTA on interaction with platelet-rich fibrin and blood clot: an in vitro study
Sonia Khatri, Sylvia Mathew, Shruthi Nagaraja, Swaroop Hegde, Soumyadeep Ghosh, Kavimalar Ravichandran
F1000Research.2023; 12: 364. CrossRef - Effects of CEM cement and emdogain on proliferation and differentiation of human stem cells from the apical papilla: a comparative in vitro study
Elham Khoshbin, Leila Ghasemi, Rezvan Najafi, Hamed Karkehabadi
Biotechnology Letters.2023; 45(1): 69. CrossRef - Comparative Evaluation of the Regenerative Potential of Blood Clot and Platelet-rich Fibrin in Young Permanent Teeth Based on the Revised American Academy of Endodontics Clinical Considerations for Regenerative Procedure: 2016
Aarathi J Prakash, Saraswathi V Naik, Prabhakar Attiguppe
International Journal of Clinical Pediatric Dentistry.2023; 16(S2): S149. CrossRef - Biomechanical characterization of a fibrinogen–blood hydrogel for human dental pulp regeneration
Sofia Silvia Piglionico, Bela Varga, Orsolya Pall, Olivier Romieu, Csilla Gergely, Frédéric Cuisinier, Bernard Levallois, Ivan Vladislavov Panayotov
Biomaterials Science.2023; 11(20): 6919. CrossRef - Intracellular bacterial eradication using a novel peptide in vitro
Wing Nok Isaac Ng, Shanthini Kalimuthu, Carmen Oi Kwan Law, Angeline Hui Cheng Lee, Terrence Chi Kong Lau, Yiu Yan Leung, Gary Shun Pan Cheung, Prasanna Neelakantan
International Endodontic Journal.2023; 56(11): 1360. CrossRef - Regenerative Endodontic Treatment of Previously Treated Mature Permanent Tooth: A Case Report with 3-year Follow Up
Myung-Jin Lee
The Korean Journal of Oral and Maxillofacial Pathology.2023; 47(6): 133. CrossRef - Clinical Outcome and Comparison of Regenerative and Apexification Intervention in Young Immature Necrotic Teeth—A Systematic Review and Meta-Analysis
Pratima Panda, Lora Mishra, Shashirekha Govind, Saurav Panda, Barbara Lapinska
Journal of Clinical Medicine.2022; 11(13): 3909. CrossRef - Evaluation of Attitude and Knowledge of Endodontic, Pedodontic and SBARD Residents in Saudi Arabia toward Regenerative Endodontics—A National Survey
Ali A. Assiry, Mohmed Isaqali Karobari, Niher Tabassum Snigdha, Roshan Noor Mohamed, Syed Nahid Basheer, Mohammed Zameer
Medicina.2022; 58(4): 545. CrossRef - Effects of Intracanal Antimicrobials on Viability and Differentiation of Stem Cells From the Apical Papilla: An In Vitro Study
Gavin Raddall, Isabel Mello, Brendan M. Leung
Journal of Endodontics.2022; 48(7): 880. CrossRef - Awareness and Acceptance of Vital Pulp Therapy and Regenerative Endodontic Procedures among Dental Professionals in India: A Web-based Survey
Saloni Rathi, Priya Chauhan, Suparna Ganguly Saha, Rolly Agarwal, Simar Kaur Manocha, Mrinali Chaddha
Journal of Research and Advancement in Dentistry.2022; 14(1): 10. CrossRef - Exosomes as Biochemistry Tools for Stem Cell Differentiation: A Novel Cell-Based Treatment for Diseases
Saeed Azandeh, Darioush Bijan Nejad, Samaneh Karimi, Fereshtesadat Fakhredini
Jentashapir Journal of Cellular and Molecular Biology.2022;[Epub] CrossRef - Effect of biodentine coated with emdogain on proliferation and differentiation of human stem cells from the apical papilla
Hamed Karkehabadi, Erfan Ahmadyani, Rezvan Najafi, Elham Khoshbin
Molecular Biology Reports.2022; 49(5): 3685. CrossRef - Evaluation of the Effectiveness of Laser‐Assisted Bleaching of the Teeth Discolored due to Regenerative Endodontic Treatment
Noushin Shokouhinejad, Mehrfam Khoshkhounejad, Fatemeh Hamidzadeh, Murilo Baena Lopes
International Journal of Dentistry.2022;[Epub] CrossRef - Triple Antibiotic Paste: A Suitable Medicament for Intracanal Disinfection
Krutika Malu, Monika Khubchandani
Cureus.2022;[Epub] CrossRef - A Comparative Evaluation of Microhardness and Chemical Structure of Radicular Dentin with Two Combinations of TAP and MTAP: An In Vitro Study
Muthumula Daneswari, Nagireddy Venugopal Reddy, Annie P Chris, Nikhila V Reddy, Saigeeta Kondamadugu, P Niharika
International Journal of Clinical Pediatric Dentistry.2022; 15(S2): S151. CrossRef - Comparing Antibiotic Pastes with Electrospun Nanofibers as Modern Drug Delivery Systems for Regenerative Endodontics
Nura Brimo, Dilek Çökeliler Serdaroğlu, Busra Uysal
Current Drug Delivery.2022; 19(9): 904. CrossRef - The Advances of Blood Clots Used as Biomaterials in Regenerative Medicine
Eliza VanZweden, Rachael Tolsma, Victor Hung, Peter Awad, Robert Sawyer, Yong Li
Regenerative Medicine.2022; 17(12): 957. CrossRef - Microstructure and color stability of calcium silicate-based dental materials exposed to blood or platelet-rich fibrin
Noushin Shokouhinejad, Ibrahim Abu Tahun, Shima Saber Tahan, Fatemeh Mohandes, Mohammad H. Nekoofar, Paul M. H. Dummer
Clinical Oral Investigations.2022; 27(3): 1193. CrossRef - Results of “proroot mta” application in treatment of chronic periodontitis in teeth with incomplete root formation
N.M. Korneeva, E.A. Novikova, D.S. Popova, K.S. Rabadanova, L.Ya Rzaeva
Stomatology for All / International Dental review.2022; (2(99)): 10. CrossRef - Antimicrobial Effect of Calcium Hydroxide Combined with Electrolyzed Superoxidized Solution at Neutral pH on Enterococcus faecalis Growth
Héctor Armando Jimenez-Gonzalez, María Argelia Akemi Nakagoshi-Cepeda, Sergio Eduardo Nakagoshi-Cepeda, Víctor Hugo Urrutia-Baca, Myriam Angélica De La Garza-Ramos, Juan Manuel Solis-Soto, Ricardo Gomez-Flores, Patricia Tamez-Guerra, Yeliz Guven
BioMed Research International.2021;[Epub] CrossRef - Unpredictable Outcomes of a Regenerative Endodontic Treatment
Zahra Mohammadi, Hadi Assadian, Behnam Bolhari, Mohammadreza Sharifian, Mehrfam Khoshkhounejad, Nazanin Chitsaz, Andrea Scribante
Case Reports in Dentistry.2021;[Epub] CrossRef - Revascularization of nonvital immature incisor with asymptomatic apical periodontitis
Ema Mulyawati, Pribadi Santosa, Tunjung Nugraheni
Scientific Dental Journal.2020; 4(3): 134. CrossRef - Comparative analysis of calcium hydroxide apexification and regenerative endodontic procedure for root dentine growth stimulation in immature incisors with pulp necrosis
M.S. Rakhmanova, M.V. Korolenkova
Stomatologiya.2020; 99(6): 55. CrossRef - Antimicrobial Efficacy of a Novel Antibiotic‐Eluting Injectable Platelet‐Rich Fibrin Scaffold against a Dual‐Species Biofilm in an Infected Immature Root Canal Model
Azade Rafiee, Mahtab Memarpour, Yasaman Najibi, Bahman Khalvati, Sedigheh Kianpour, Mohammad Hossein Morowvat, Sung-Hwan Choi
BioMed Research International.2020;[Epub] CrossRef - Exosomes Derived from Stem Cells from the Apical Papilla Promote Dentine-Pulp Complex Regeneration by Inducing Specific Dentinogenesis
Xueying Zhuang, Lingli Ji, Huan Jiang, Yao Liu, Xuemei Liu, Jing Bi, Weidong Zhao, Zhenjiang Ding, Xu Chen
Stem Cells International.2020; 2020: 1. CrossRef - Injectable Biomaterials for Dental Tissue Regeneration
Håvard Jostein Haugen, Poulami Basu, Mousumi Sukul, João F Mano, Janne Elin Reseland
International Journal of Molecular Sciences.2020; 21(10): 3442. CrossRef - Viability and Stimulation of Human Stem Cells from the Apical Papilla (hSCAPs) Induced by Silicate-Based Materials for Their Potential Use in Regenerative Endodontics: A Systematic Review
José Luis Sanz, Leopoldo Forner, Alicia Almudéver, Julia Guerrero-Gironés, Carmen Llena
Materials.2020; 13(4): 974. CrossRef - An Innovative Drug Delivery System Loaded with a Modified Combination of Triple Antibiotics for Use in Endodontic Applications
Ardavan Parhizkar, Hanieh Nojehdehian, Fahimeh Tabatabaei, Saeed Asgary
International Journal of Dentistry.2020; 2020: 1. CrossRef - Defining Endodontic Residents' Clinical Experiences: A National Survey
Jonathan D. Blacher, Kamran E. Safavi, Robert H. Aseltine, Blythe M. Kaufman
Journal of Dental Education.2019; 83(5): 504. CrossRef - Coronal tooth discoloration induced by regenerative endodontic treatment using different scaffolds and intracanal coronal barriers: a 6-month ex vivo study
Noushin Shokouhinejad, Hassan Razmi, Maryam Farbod, Marzieh Alikhasi, Josette Camilleri
Restorative Dentistry & Endodontics.2019;[Epub] CrossRef - Comparative Study between Revitalization of Necrotic Immature Permanent Anterior Teeth with and without Platelet Rich Fibrin: A Randomized Controlled Trial
Rasha Adel Ragab, Amr Ezzat Abd El Lattif, Norhan Abd El Wahab El Dokky
Journal of Clinical Pediatric Dentistry.2019; 43(2): 78. CrossRef - Biomaterials and Scaffold Design Strategies for Regenerative Endodontic Therapy
Gavin Raddall, Isabel Mello, Brendan M. Leung
Frontiers in Bioengineering and Biotechnology.2019;[Epub] CrossRef - Iloprost Induces Dental Pulp Angiogenesis in a Growth Factor–free 3-Dimensional Organ Culture System
Sonntana Seang, Prasit Pavasant, Chalida N. Limjeerajarus
Journal of Endodontics.2018; 44(5): 759. CrossRef - Ratio and Rate of Induced Root Growth in Necrotic Immature Teeth
Eun Jung Sang, Ji-Soo Song, Teo Jeon Shin, Young-Jae Kim, Jung-Wook Kim, Ki-Taeg Jang, Sang-Hoon Lee, Hong-Keun Hyun
THE JOURNAL OF THE KOREAN ACADEMY OF PEDTATRIC DENTISTRY.2018; 45(2): 225. CrossRef - Triple antibiotic paste: momentous roles and applications in endodontics: a review
Ardavan Parhizkar, Hanieh Nojehdehian, Saeed Asgary
Restorative Dentistry & Endodontics.2018;[Epub] CrossRef - Traumatic avulsion and delayed replantation of maxillary incisors in an eleven-year-old child
Gokcen Deniz Bayrak
Edorium Journal of Dentistry.2018; 5(1): 1. CrossRef - Influence of Apical Diameter on the Outcome of Regenerative Endodontic Treatment in Teeth with Pulp Necrosis: A Review
Yanjun Fang, Xinhuan Wang, Jingjing Zhu, Chaonan Su, Ying Yang, Liuyan Meng
Journal of Endodontics.2018; 44(3): 414. CrossRef - Assessment of Regaining Pulp Sensibility in Mature Necrotic Teeth Using a Modified Revascularization Technique with Platelet-rich Fibrin: A Clinical Study
Mohamed Nageh, Geraldine M. Ahmed, Alaa A. El-Baz
Journal of Endodontics.2018; 44(10): 1526. CrossRef - Local drug delivery in endodontics: A literature review
Shin Hye Chung, Young-Seok Park
Journal of Drug Delivery Science and Technology.2017; 39: 334. CrossRef - Regenerative Endodontics
Kristina Feigin, Bonnie Shope
Journal of Veterinary Dentistry.2017; 34(3): 161. CrossRef - Intentional Replantation of an Avulsed Immature Permanent Incisor: A Case Report
Claudio Maniglia-Ferreira, Fabio de Almeida Gomes, Marcelo de Morais Vitoriano
Journal of Endodontics.2017; 43(8): 1383. CrossRef - Effect of acidic solutions on the microhardness of dentin and set OrthoMTA and their cytotoxicity on murine macrophage
Soram Oh, Hiran Perinpanayagam, Yoon Lee, Jae-Won Kum, Yeon-Jee Yoo, Sang-Min Lim, Seok Woo Chang, Won-Jun Shon, Woocheol Lee, Seung-Ho Baek, Kee-Yeon Kum
Restorative Dentistry & Endodontics.2016; 41(1): 12. CrossRef - Questioning the spot light on Hi-tech endodontics
Jojo Kottoor, Denzil Albuquerque
Restorative Dentistry & Endodontics.2016; 41(1): 80. CrossRef - Effects of a Bioactive Scaffold Containing a Sustained Transforming Growth Factor-β1–releasing Nanoparticle System on the Migration and Differentiation of Stem Cells from the Apical Papilla
Craig Bellamy, Suja Shrestha, Calvin Torneck, Anil Kishen
Journal of Endodontics.2016; 42(9): 1385. CrossRef - Effects of Novel 3-dimensional Antibiotic-containing Electrospun Scaffolds on Dentin Discoloration
Margaret Louise A. Porter, Eliseu A. Münchow, Maria T.P. Albuquerque, Kenneth J. Spolnik, Anderson T. Hara, Marco C. Bottino
Journal of Endodontics.2016; 42(1): 106. CrossRef
 ePub Link
ePub Link Cite
CiteA review of the regenerative endodontic treatment procedure
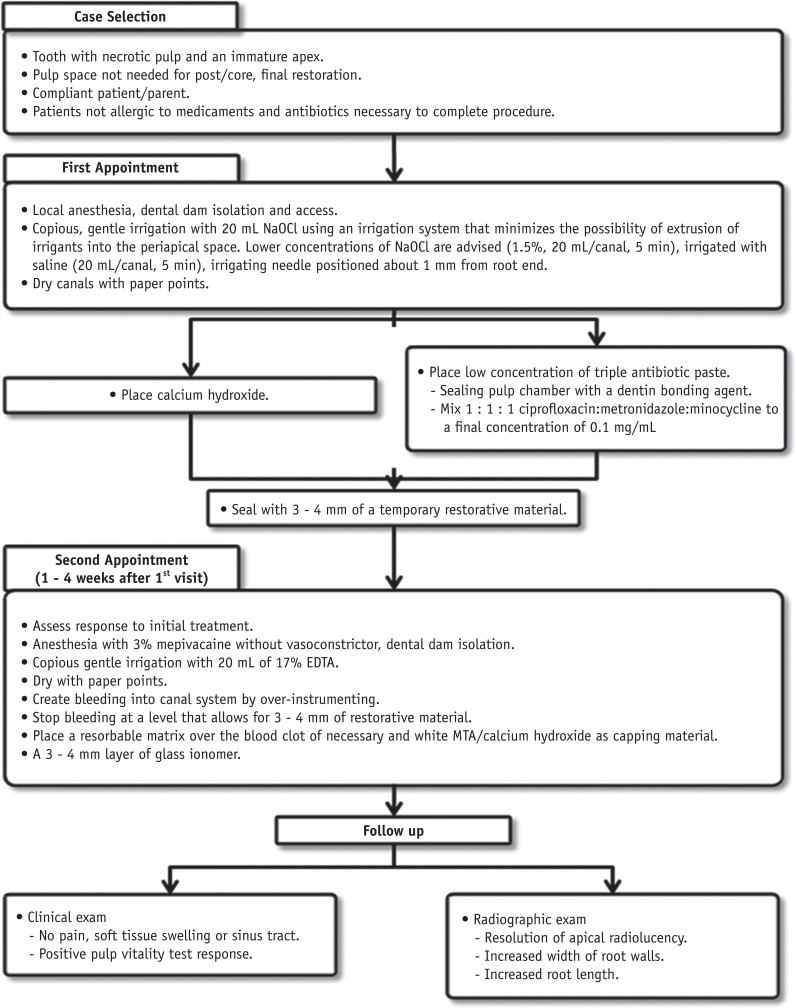
Figure 1 The current considerations for regenerative endodontic treatment procedures (Courtesy of the American Association of Endodontics). NaOCl, sodium hypochlorite; EDTA, ethylenediaminetetraacetic acid; MTA, mineral trioxide aggregate.
Figure 1
A review of the regenerative endodontic treatment procedure
The characteristics of three treatment procedures for immature root formation
| Procedure | Characteristic |
|---|---|
| Apexification with calcium hydroxide | Long time span of the entire treatment |
| Multiple visits | |
| Increased risk of tooth fracture due to long-term application of Ca(OH)2 | |
| Apexification with MTA | One- or two-step apexification |
| Neither strengthens the root nor promotes further root development | |
| Roots remain thin and fragile | |
| Revascularization | Promotes further root development |
| Causes reinforcement of dentinal walls by deposition of hard tissue (strengthening the root against fracture) |
MTA, mineral trioxide aggregate.
The percentage increase in root width and root length after the treatment procedure
| Revascularization | Apexification with MTA | Apexification with calcium hydroxide | |
|---|---|---|---|
| Root width | 28.2% | 0.00% | 1.52% |
| Root length | 14.9% | 6.1% | 0.4% |
MTA, mineral trioxide aggregate.
Comparison between stem cells from the apical papilla (SCAP) and dental pulp stem cells (DPSCs)
| Feature | |
|---|---|
| Similarity | Osteogenic differentiation |
| Dentinogenic differentiation | |
| Low adipogenic potential | |
| Difference | Cell proliferation: SCAP > DPSCs |
| Number of population doublings: SCAP > DPSCs | |
| Tissue regeneration capacity: SCAP > DPSCs |
Factors that affect the results of revascularization
| Factor | Finding |
|---|---|
| Degree of infection of the canal | It is impossible to treat an infected tooth with the revascularization procedure |
| Tri-antibiotic paste. Calcium hydroxide is used to disinfect the canal | |
| Apex diameter | An open apical foramen > 1.1 mm is beneficial |
| Possibility of revascularization increases in approximately 18 - 34% of teeth with immature roots | |
| Patient age | Recommended age range: 8 - 16 years |
| Revascularization should not be performed on deciduous teeth |
Case reports of multiple visit & single visit revascularization
| Author | Irrigation | Intracanal medication | Pulpal space barrier/Restoration | Recall | Root lengthening & Thickening |
|---|---|---|---|---|---|
| Branchs & Trope | 5.2% NaOCl peridex | Tri-antibiotics | MTA/Resin | 2 yr (multiple visits) | Yes |
| Chueh & Huang | 2.5% NaOCl | Calcium hydroxide | Amalgam | 7 mon to 5 yr (multiple visits) | Yes |
| Shin & Albert | 6% NaOCl | None | MTA/Resin | 19 mon (single visit) | Yes |
| 2% Chlorhexidine |
NaOCl, sodium hypochlorite; MTA, mineral trioxide aggregate.
Table 1 The characteristics of three treatment procedures for immature root formation
MTA, mineral trioxide aggregate.
Table 2 The percentage increase in root width and root length after the treatment procedure
MTA, mineral trioxide aggregate.
Table 3 Comparison between stem cells from the apical papilla (SCAP) and dental pulp stem cells (DPSCs)
Table 4 Factors that affect the results of revascularization
Table 5 Case reports of multiple visit & single visit revascularization
NaOCl, sodium hypochlorite; MTA, mineral trioxide aggregate.

