
Search
- Page Path
- HOME > Search
Research Articles
- Influence of adjacent restorative material and distance on the accuracy of inlay cavity impressions with intraoral scanner: an in vitro study
- So-Yeon Lee, Sung-Ae Son, Jae-Hoon Kim, Deog-Gyu Seo, Jeong-Kil Park
- Restor Dent Endod 2026;51(1):e6. Published online January 23, 2026
- DOI: https://doi.org/10.5395/rde.2026.51.e6
-
 Abstract
Abstract
 PDF
PDF PubReader
PubReader ePub
ePub - Objectives
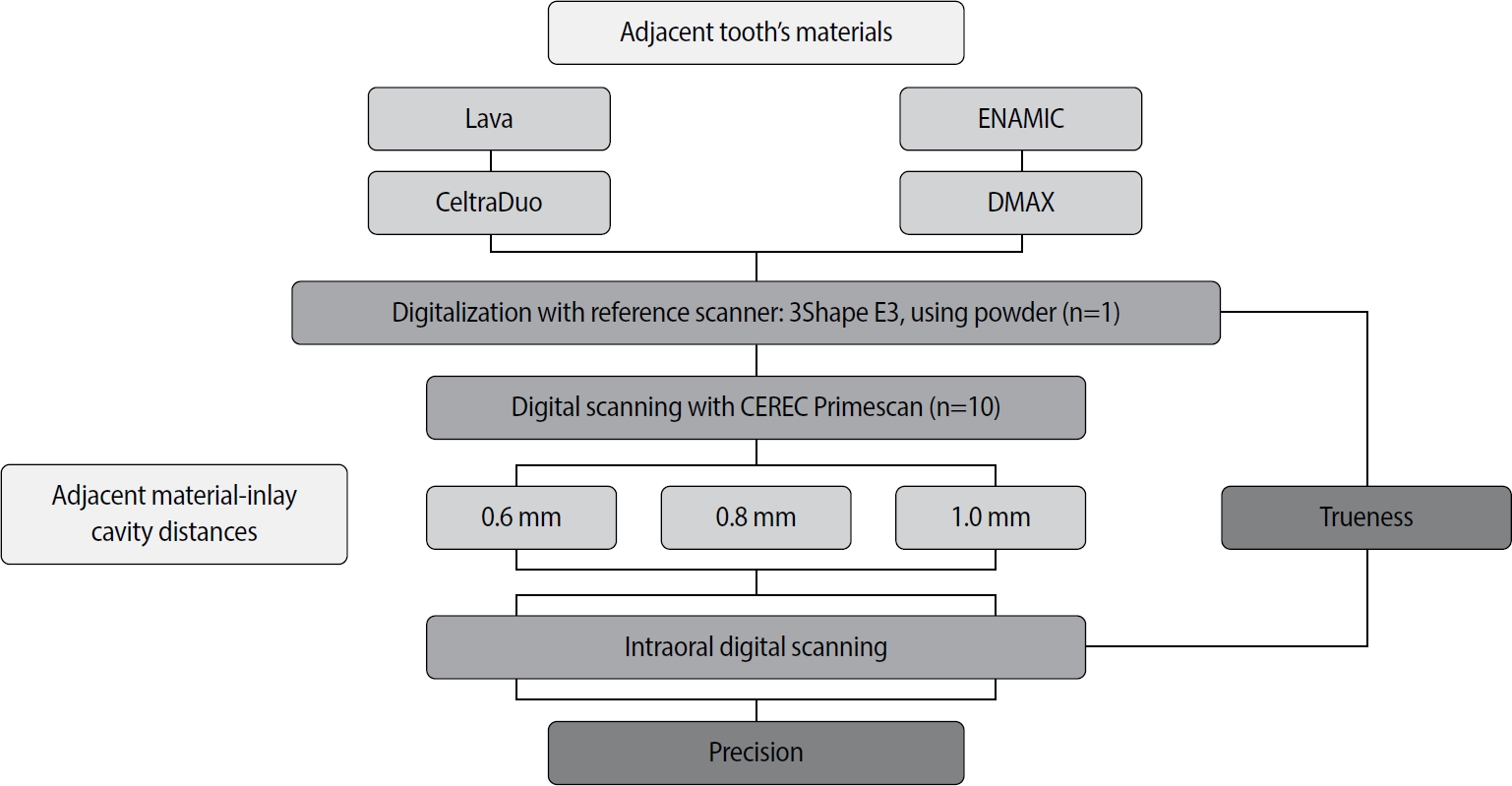
This study aimed to evaluate the influence of adjacent restorative material and interproximal distance on the accuracy of digital impressions of inlay cavities obtained using an intraoral scanner.
Methods
A disto-occlusal inlay cavity was prepared on a mandibular right first molar model, and digital scans were performed using a CEREC Primescan (Dentsply Sirona). The adjacent restorative materials used were Lava (3M ESPE), ENAMIC (VITA Zahnfabrik), Celtra Duo (Dentsply Sirona), and DMAX (DMAX), and the interproximal distances were set to 0.6 mm, 0.8 mm, and 1.0 mm. The obtained scan data were analyzed using GOM Inspect software (GOM GmbH).
Results
Trueness, maximum positive and negative deviations, and precision were significantly influenced by both the adjacent restorative material and the interproximal distance, while their interaction showed a significant effect only on precision. Celtra Duo demonstrated the highest trueness, with mean deviation values decreasing from 7.8 μm at a 0.6 mm interproximal distance to 7.3 μm at 1.0 mm. ENAMIC showed the best precision, presenting mean deviations of 2.6 μm at 0.6 mm, 2.9 μm at 0.8 mm, and 2.4 μm at 1.0 mm. A narrow interproximal distance of 0.6 mm resulted in lower trueness, measured at 8.3 μm, and the highest precision deviation of 3.4 μm. In contrast, an interproximal distance of 1.0 mm yielded improved scan accuracy, with increased trueness and reduced precision variation.
Conclusions
Digital impression accuracy of inlay cavities was influenced by adjacent restorative material and interproximal distance, suggesting clinical consideration is needed in CAD/CAM workflows to optimize restoration fit. -
Citations
Citations to this article as recorded by
- 3D-SCANNING IN PROSTHETIC DENTISTRY: ADVANTAGES, DISADVANTAGES, AND DEVELOPMENT PROSPECTS
V. S. Kuz, O. I. Teslenko, H. M. Kuz, H. M. Balia, Yu. S. Lunkova, O. V. Shemetov, I. M. Martynenko
Bulletin of Problems Biology and Medicine.2026; 1(1): 98. CrossRef
- 3D-SCANNING IN PROSTHETIC DENTISTRY: ADVANTAGES, DISADVANTAGES, AND DEVELOPMENT PROSPECTS
- 2,174 View
- 123 Download
- 1 Crossref

- Enhanced visualization of the root canal morphology using a chitosan-based endo-radiopaque solution
- Shashirekha Govind, Amit Jena, Satabdi Pattanaik, Mahaprasad Anarasi, Satyajit Mohapatra, Vinay Shivagange
- Restor Dent Endod 2021;46(3):e33. Published online June 4, 2021
- DOI: https://doi.org/10.5395/rde.2021.46.e33
-
Abstract
PDFPubReaderePub
Objectives This study aimed to investigate the efficacy of ionic and non-ionic-based contrast media (
in vitro study) and the combinatorial effect of chitosan-based endo-radiopaque solution (CERS) (in vivo study) for visualization of the root canal anatomy.Materials and Methods In vitr o study (120 teeth): The root canal of maxillary premolars and molars (in vitro group 1 and 2 respectively,n = 60 each) were analyzed using 4 different contrast media (subgroups: Omnipaque 350, Iopamidol, Xenetix 350, and Urografin 76;n = 15 each) in combination with 5.25% sodium hypochlorite (NaOCl). Based on the results of thein vitro study,in vivo study (80 teeth) was done to compare Xenetix 350 + 5.25% NaOCl with CERS (in vivo group 1 and 2 respectively,n = 40 each) on maxillary and mandibular premolars and molars. Two endodontists used radiovisiography to assess the depth of ingress and identify the aberrant root anatomy after access cavity preparation, and after initial cleaning and shaping of canals. Kruskal-Wallis test was used forin vitro comparison (p < 0.05), and Wilcoxon signed-rank test and Mann-WhitneyU test forin vivo analysis (p < 0.01).Results In vitro study, Xenetix 350 + 5.25% NaOCl facilitated a significant higher visualization (p < 0.05). Forin vivo study, CERS had a statistically significant depth of ingress (p < 0.01), and was efficient in identifying the aberrant root canal anatomy of premolars and molars.Conclusions CERS facilitates better visualization of the root canal anatomy of human premolars and molars.
-
Citations
Citations to this article as recorded by- Influence of irrigating solutions on the hydration of calcium silicate-based dental biomaterials: An in vitro study
Pradeep M. Divya, Amit Jena, Saumyakanta Mohanty, Govind Shashirekha, Rashmi Rekha Mallick, Priyanka Sarangi
Journal of Conservative Dentistry and Endodontics.2025; 28(8): 758. CrossRef - Improving Endodontic Radiograph Interpretation with TV-CLAHE for Enhanced Root Canal Detection
Barbara Obuchowicz, Joanna Zarzecka, Michał Strzelecki, Marzena Jakubowska, Rafał Obuchowicz, Adam Piórkowski, Elżbieta Zarzecka-Francica, Julia Lasek
Journal of Clinical Medicine.2025; 14(15): 5554. CrossRef - Efficacy of sonic and ultrasonic activation on irrigant penetration in different tapered preparations: An in vitro study
M. Rama Sowmya, Kavalipurapu Venkata Teja, Pradeep Solete, Sahil Choudhari, S Delphine Priscilla Antony, Mohammed Mustafa
Endodontology.2024; 36(4): 370. CrossRef - Analysis of the value of visualized root canal technique in the clinical treatment of endodontics
Nana SUN, Nannan WANG, Xin QIAN
Panminerva Medica.2023;[Epub] CrossRef
- Influence of irrigating solutions on the hydration of calcium silicate-based dental biomaterials: An in vitro study
- 2,569 View
- 26 Download
- 2 Web of Science
- 4 Crossref
- The effects of image acquisition control of digital X-ray system on radiodensity quantification
- Wook-Jin Seong, Hyeon-Cheol Kim, Soocheol Jeong, Youngcheul Heo, Woo-Bin Song, Mansur Ahmad
- Restor Dent Endod 2013;38(3):146-153. Published online August 23, 2013
- DOI: https://doi.org/10.5395/rde.2013.38.3.146
-
Abstract
PDFPubReaderePub
Objectives Aluminum step wedge (ASW) equivalent radiodensity (eRD) has been used to quantify restorative material's radiodensity. The aim of this study was to evaluate the effects of image acquisition control (IAC) of a digital X-ray system on the radiodensity quantification under different exposure time settings.
Materials and Methods Three 1-mm thick restorative material samples with various opacities were prepared. Samples were radiographed alongside an ASW using one of three digital radiographic modes (linear mapping (L), nonlinear mapping (N), and nonlinear mapping and automatic exposure control activated (E)) under 3 exposure time settings (underexposure, normal-exposure, and overexposure). The ASW eRD of restorative materials, attenuation coefficients and contrasts of ASW, and the correlation coefficient of linear relationship between logarithms of gray-scale value and thicknesses of ASW were compared under 9 conditions.
Results The ASW eRD measurements of restorative materials by three digital radiographic modes were statistically different (
p = 0.049) but clinically similar. The relationship between logarithms of background corrected grey scale value and thickness of ASW was highly linear but attenuation coefficients and contrasts varied significantly among 3 radiographic modes. Varying exposure times did not affect ASW eRD significantly.Conclusions Even though different digital radiographic modes induced large variation on attenuation of coefficient and contrast of ASW, E mode improved diagnostic quality of the image significantly under the under-exposure condition by improving contrasts, while maintaining ASW eRDs of restorative materials similar. Under the condition of this study, underexposure time may be acceptable clinically with digital X-ray system using automatic gain control that reduces radiation exposure for patient.
-
Citations
Citations to this article as recorded by- Is the radiopacity of CAD/CAM aesthetic materials sufficient?
Rua S. Babaier, Modi S. Aldeeb, Nick Silikas, David C. Watts
Dental Materials.2022; 38(6): 1072. CrossRef
- Is the radiopacity of CAD/CAM aesthetic materials sufficient?
- 2,320 View
- 5 Download
- 1 Crossref
- The reduction methods of operator's radiation dose for portable dental X-ray machines
- Jeong-Yeon Cho, Won-Jeong Han
- Restor Dent Endod 2012;37(3):160-164. Published online August 29, 2012
- DOI: https://doi.org/10.5395/rde.2012.37.3.160
-
Abstract
PDFPubReaderePub
Objectives This study was aimed to investigate the methods to reduce operator's radiation dose when taking intraoral radiographs with portable dental X-ray machines.
Materials and Methods Two kinds of portable dental X-ray machines (DX3000, Dexcowin and Rextar, Posdion) were used. Operator's radiation dose was measured with an 1,800 cc ionization chamber (RadCal Corp.) at the hand level of X-ray tubehead and at the operator's chest and waist levels with and without the backscatter shield. The operator's radiation dose at the hand level was measured with and without lead gloves and with long and short cones.
Results The backscatter shield reduced operator's radiation dose at the hand level of X-ray tubehead to 23 - 32%, the lead gloves to 26 - 31%, and long cone to 48 - 52%. And the backscatter shield reduced operator's radiation dose at the operator's chest and waist levels to 0.1 - 37%.
Conclusions When portable dental X-ray systems are used, it is recommended to select X-ray machine attached with a backscatter shield and a long cone and to wear the lead gloves.
-
Citations
Citations to this article as recorded by- Handheld dental X-ray devices: a scoping review of radiation safety and image quality
Marco M Herz, Constanze Keutel, Johannes Oesterreicher
Dentomaxillofacial Radiology.2026;[Epub] CrossRef - SpaceXray: Feasibility and Diagnostic Capabilities of On-Orbit Medical Radiography
Sheyna E. Gifford, Michael Pohlen, Adam S. Wang, David J. Lerner, Anna Wadhwa, Michael Cairnie, Jeanne Walter, Karim S. Karim, Steven Tilley, Amol Karnick, Marissa A. Rosenberg, Lonnie G. Petersen
Radiology.2026;[Epub] CrossRef - Assessment of the Occupational Radiation Dose from a Handheld Portable X-ray Unit During Full-mouth Intraoral Dental Radiographs in the Dog and the Cat – A Pilot Study
Lenin A. Villamizar-Martinez, Jeannie Losey
Journal of Veterinary Dentistry.2024; 41(2): 106. CrossRef - Seguridad y protección radiológica con el uso de rayos X portátiles. Revisión de literatura
Francisco Javier Marichi-Rodríguez, Janeth Serrano-Bello, Marine Ortiz-Magdaleno, Febe Carolina Vázquez-Vázquez
Revista Odontológica Mexicana Órgano Oficial de la Facultad de Odontología UNAM.2024;[Epub] CrossRef - Evaluation of Operator and Patient Doses after Irradiation with Handheld X-ray Devices
Ali Altındağ, Hakan Eren, Kaan Orhan, Sebahat Görgün
Applied Sciences.2023; 13(18): 10414. CrossRef - Hand-held dental X-ray device: Attention to correct use
Guilherme Ceschia Martins, Thaíza Gonçalves Rocha, Thaís de Lima Azeredo, Andréa de Castro Domingos, Maria Augusta Visconti, Eduardo Murad Villoria
Imaging Science in Dentistry.2023; 53(3): 265. CrossRef - Effect of cranium structure on dose distribution during intraoral radiography
Takeru Ishii, Atsushi Iwawaki, Yusei Otaka, Atsuharu Nitanda, Akihiro Ochiai, Shinji Kito, Hirofumi Aboshi, Hideki Saka
Journal of Oral Biosciences.2022; 64(1): 131. CrossRef - Application of the Monte Carlo Method for the Evaluation of Scattered Radiation Dose Due to the Use of Handheld X-Ray in Dentistry
A Cc Gonzales, M R Soares, W O G Batista, A R Cardeña, J P Marquez, J R Vega
Radiation Protection Dosimetry.2022;[Epub] CrossRef - ASSESSMENT OF OCCUPATIONAL RADIATION DOSE FROM CAMERA MODEL INTRAORAL HANDHELD X-RAY DEVICE WITHOUT STRAY RADIATION PROTECTION SHIELD
Mahkameh Moshfeghi, Yaser Safi, Alireza Afzalan, Mitra Ghazizadeh Ahsaie
Radiation Protection Dosimetry.2022; 198(1-2): 1. CrossRef - Evaluation of radiation exposure to operators of portable hand-held dental X-ray units
Justin Leadbeatter, Jennifer Diffey
Physical and Engineering Sciences in Medicine.2021; 44(2): 377. CrossRef - Update on Hand-Held X-Ray Devices in Dentistry: a Literature Review
Lucía Barba Ramírez, Deivi Cascante-Sequeira
Odovtos - International Journal of Dental Sciences.2021; 24(2): 26. CrossRef - Comparison of air dose and operator exposure from portable X-ray units
Atsushi Iwawaki, Yusei Otaka, Ruri Asami, Takeru Ishii, Shinji Kito, Yuichi Tamatsu, Hirofumi Aboshi, Hideki Saka
Legal Medicine.2020; 47: 101787. CrossRef - Dental research using intraoral techniques with portable digital radiography adapted for fieldwork in Qubbet el-Hawa (Egypt)
Sandra López-Lázaro, Violeta C. Yendreka, Alejandro Jiménez-Serrano, José Alba-Gómez, Gabriel M. Fonseca
Archaeological and Anthropological Sciences.2020;[Epub] CrossRef - Evaluation of stray radiation to the operator for five hand-held dental X-ray devices
Richard Smith, Richard Tremblay, Graeme M Wardlaw
Dentomaxillofacial Radiology.2019; 48(5): 20180301. CrossRef - Assessment of image quality and exposure parameters of an intraoral portable X-rays device
Elton G Zenóbio, Madelon AF Zenóbio, Carolina DB Azevedo, Maria do Socorro Nogueira, Cláudio D Almeida, Flávio R Manzi
Dentomaxillofacial Radiology.2019; 48(3): 20180329. CrossRef - The study of protection of operators and surrounding workers at the time of using portable intraoral X-ray unit
Atsushi Iwawaki, Yusei Otaka, Ruri Asami, Tomonori Ozawa, Maki Izawa, Hideki Saka
Legal Medicine.2018; 33: 66. CrossRef - The effects of device position on the operator's radiation dose when using a handheld portable X-ray device
Jimmy Makdissi, Ravikiran R Pawar, Ben Johnson, Bun S Chong
Dentomaxillofacial Radiology.2016; 45(3): 20150245. CrossRef - Patient and staff dosimetry during radiographic procedures in an intensive care unit
Rosario Fernández, Miguel Moreno-Torres, Antonia M Contreras, María I Núñez, Damián Guirado, Luis Peñas
Journal of Radiological Protection.2015; 35(3): 727. CrossRef - The effects of image acquisition control of digital X-ray system on radiodensity quantification
Wook-Jin Seong, Hyeon-Cheol Kim, Soocheol Jeong, Youngcheul Heo, Woo-Bin Song, Mansur Ahmad
Restorative Dentistry & Endodontics.2013; 38(3): 146. CrossRef
- Handheld dental X-ray devices: a scoping review of radiation safety and image quality
- 7,096 View
- 38 Download
- 19 Crossref
Basic Research
- Evaluation of radiopacity and discriminability of various fiber reinforced composite posts
- Eun-Hye Lee, Hang-Moon Choi, Se-Hee Park, Jin-Woo Kim, Kyung-Mo Cho
- J Korean Acad Conserv Dent 2010;35(3):188-197. Published online May 31, 2010
- DOI: https://doi.org/10.5395/JKACD.2010.35.3.188
-
Abstract
PDFPubReaderePub
The purpose of this study was to compare radiopacity and radiographic discriminability of various FRC-Posts.
Six FRC-Posts were investigated ; 1) FRC Postec Plus (Ivoclar Vivadent AG, Schaan, Liechtenstein), 2) Snowlight (Carbotech, Lewis center, OH, USA), 3) Dentin Post (Komet Brasseler, Lamgo, Germany), 4) Rely-X Fiber Post (3M ESPE, St.paul, MN, USA), 5) D.T.-Light Post (BISCO, Schaumburg, IL,USA), 6) Luxapost (DMG, Hamburg, Germany)
The radiographs of each post with a reference 1 mm / 2 mm aluminum step-wedge was taken using digital sensor. The optical density were calculated by gray value of 10 × 10 pixel and compared in mm Al equivalent at five points.
Six maxillary incisors of similar radiopacity were used. Radiographs of posts in Mx. incisors of lingual side of dry mandible were taken.
We showed radiographs and asked the questionnaire to 3 radiologists, 3 endodontists, 3 general practitioners. The questionnaire was comprised of choices of the highest, lowest radiopaque individual post and the choices of best discriminable post at apical, coronal area.
The following results were obtained.
Each post system showed various radiopacity.
There was change of discriminability between each post and simulated specimens regardless of examiner.
Although each post showed various radiopacity, the difference of radiopacity did not affect on discriminability.
- 1,446 View
- 5 Download
Original Articles
- Evaluating the reliability and repeatability of the digital color analysis system for dentistry
- Joong-Jae Jeong, Su-Jung Park, Hyun-Gu Cho, Yun-Chan Hwang, Won-Mann Oh, In-Nam Hwang
- J Korean Acad Conserv Dent 2008;33(4):352-368. Published online July 31, 2008
- DOI: https://doi.org/10.5395/JKACD.2008.33.4.352
-
Abstract
PDFPubReaderePub
This study was done to evaluate the reliability of the digital color analysis system (ShadeScan, CYNOVAD, Montreal, Canada) for dentistry.
Sixteen tooth models were made by injecting the A2 shade chemical cured resin for temporary crown into the impression acquired from 16 adults. Surfaces of the model teeth were polished with resin polishing cloth. The window of the ShadeScan handpiece was placed on the labial surface of tooth and tooth images were captured, and each tooth shade was analyzed with the ShadeScan software. Captured images were selected in groups, and compared one another.
Two models were selected to evaluate repeatability of ShadeScan, and shade analysis was performed 10 times for each tooth.
And, to ascertain the color difference of same shade code analyzed by ShadeScan, CIE L*a*b*values of shade guide of Gradia Direct (GC, Tokyo, Japan) were measured on the white and black background using the Spectrolino (GretagMacbeth, USA), and Shade map of each shade guide was captured using the ShadeScan.
There were no teeth that were analyzed as A2 shade and unique shade. And shade mapping analyses of the same tooth revealed similar shade and distribution except incisal third.
Color difference (ΔE*) among the Shade map which analyzed as same shade by ShadeScan were above 3.
Within the limits of this study, digital color analysis instrument for dentistry has relatively high repeatability, but has controversial in accuracy.
-
Citations
Citations to this article as recorded by- Development of polarization dental imaging modality and evaluation of its clinical feasibility
Eunji Kim, Taeyoon Son, Yoon Lee, Byungjo Jung
Journal of Dentistry.2012; 40: e18. CrossRef
- Development of polarization dental imaging modality and evaluation of its clinical feasibility
- 1,927 View
- 2 Download
- 1 Crossref
- Comparative study of digital and conventional radiography for the diagnostic ability of artificial proximal surface caries
- Young-Gon Cho, Si-Seung Park
- J Korean Acad Conserv Dent 2002;27(2):113-121. Published online March 31, 2002
- DOI: https://doi.org/10.5395/JKACD.2002.27.2.113
-
Abstract
PDFPubReaderePub
Conventional intraoral radiography continues to be the most widely used image modality for the diagnosis of dental caries. But, conventional intraoral radiography has several shortcomings, including the difficulty of exposing and processing intraoral film of consistently acceptable quality. In addition, radiographic retaking that was the result of processing errors, may result in increased discomfort and radiation dose to the patient.
Recently, various digital radiographies substitute for conventional intraoral radiography to overcome these disadvantages. The advantages of digital radiography are numerous. One of advantages is the elimination of processing errors. In addition, the radiation dose for digital system is approximately 20% to 25% of that required for conventional intraoral radiography. Another potential advantage of digital imaging is the ability to perform image quality enhancements such as contrast and density modulation, which may increase diagnostic accuracy.
The purpose of this study was to compare the diagnostic ability of artificial proximal defects to conventional intraoral radiography, direct digital image(CDX2000HQ®) and indirect digital image(Digora®).
Artificial defects were made in proximal surfaces of 60 extracted human molars using #1/2, #1, #2 round bur. Five dentists assessed proximal defects on conventional intraoral radiography, direct digital image(CDX2000HQ®) and indirect digital image(Digora®). ROC(Receiver Operating Characteristic) analysis and Two-way ANOVA test were used for the evaluation of detectability, and following results were acquired.
1. The mean ROC area of conventional intraoral radiography, direct digital image(CDX2000HQ®)and indirect digital image(Digora®) were 0.6766, 0.7538, 0.6791(Grade I), 0.7176, 0.7594, 0.7361(Grade II), and 0.7449, 0.7608, 0.7414(Grade III), respectively.
2. Diagnostic ability of direct digital image was higher than other image modalities. But, there was no statistically significant difference among other imaging modalities for Grade I, II, III lesion(p>0.05).
In conclusion, when direct and indirect digital system are comparable with conventional intraoral radiography, these systems may be considered an alternative of conventional intraoral radiography for the diagnosis of proximal surface caries.
- 4,283 View
- 42 Download
 First
First Prev
Prev

