
Search
- Page Path
- HOME > Search
Case Report
- Straightforward replication of digital wax-up design into direct composite resin restorations in adolescents using a custom 3-dimensionally printed index
- Ra’fat Ibrahim Farah, Sanaa Najeh Al-Haj Ali, Abdullah Alharbi, Bandar Alresheedi
- Restor Dent Endod 2024;49(4):e36. Published online October 10, 2024
- DOI: https://doi.org/10.5395/rde.2024.49.e36

-
 Abstract
Abstract
 PDF
PDF PubReader
PubReader ePub
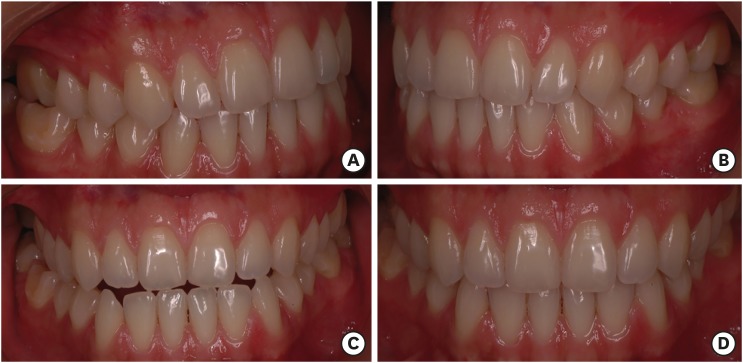
ePub This case report introduces a straightforward, noninvasive approach for the esthetic rehabilitation of malformed anterior teeth in adolescents using direct composite restorations. The universal composite resin restorations are applied within a transparent 3-dimensionally printed rigid-resin index, which is individually customized from a digital wax-up. Compared to other methods, this technique streamlines the restoration process, significantly reducing chairside time while enhancing the predictability, accuracy, and patient acceptance of the aesthetic outcome.
-
Citations
Citations to this article as recorded by
- Diastema closure and esthetic rehabilitation with peg-shaped laterals: A case series
Afsana Ansari, Dipika Yadav
The Saint's International Dental Journal.2024; 8(2): 48. CrossRef
- Diastema closure and esthetic rehabilitation with peg-shaped laterals: A case series
- 5,561 View
- 269 Download
- 1 Crossref

Research Articles
- Alkasite restorative material for endodontically treated teeth: a randomized controlled pilot study
- Davi Ariel Nobuo Bepu, Renata Siqueira Scatolin, Natalia Saud Junqueira Franco, Luiza Pejon Sanchez, Aline Evangelista Souza-Gabriel, Silmara Aparecida Milori Corona
- Restor Dent Endod 2024;49(3):e24. Published online June 11, 2024
- DOI: https://doi.org/10.5395/rde.2024.49.e24
-
Abstract
PDFPubReaderePub
Objectives This study aimed to evaluate the clinical performance of an alkasite restorative material in molars that had undergone root canal treatment.
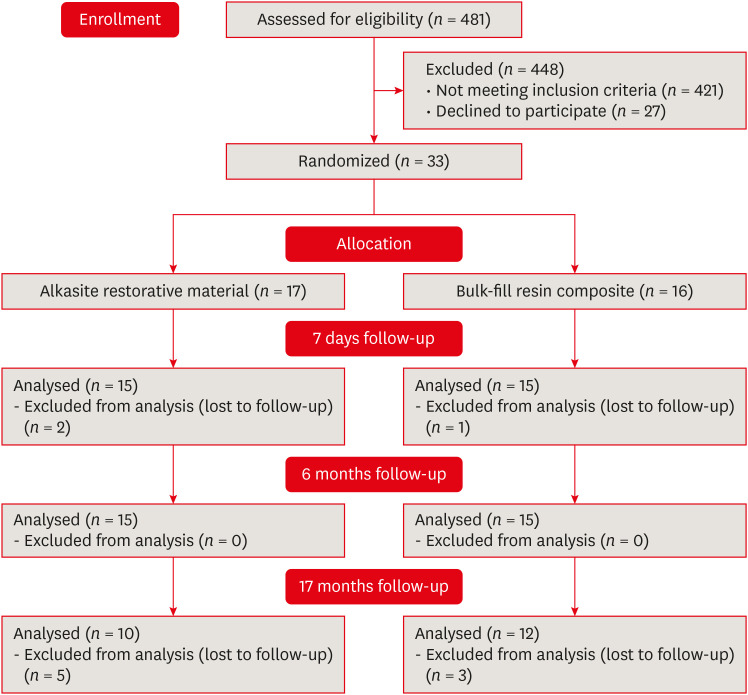
Materials and Methods The research was registered in Brazilian Registry of Clinical Trials. The randomized clinical trial involved 33 patients, each with at least 1 mandibular molar requiring restoration after receiving endodontic treatment. Patients were randomly assigned to receive either bulk-fill resin composite (Tetric N Ceram Bulk Fill, Ivoclar Vivadent) or the alkasite restorative material (Cention N, Ivoclar Vivadent). Upon completion of the restorations, 3 calibrated professionals utilized the United States Public Health Service criteria to assess various factors, including retention, secondary caries, marginal adaptation, restoration color, marginal pigmentation, and anatomical form. Evaluations were conducted at intervals of 7 days, 6 months, and 17 months. Additionally, the assessment encompassed the presence of radiolucent lines adjacent to the restoration, material deficiencies or excess, contact points, and caries recurrence. The data underwent analysis using the Friedman and Mann-Whitney tests (α = 0.05).
Results After 17 months, the results revealed that the alkasite restorative material exhibited greater wear of anatomical shape compared to the bulk-fill resin composite (
p = 0.0189). Furthermore, the alkasite restorative material significantly differed from the natural tooth color in most cases (p = 0.0000). However, no other criteria displayed significant differences between the materials or over time (p > 0.05).Conclusions The alkasite restorative material (Cention N) emerges as a viable option for restoring endodontically treated teeth, displaying clinically acceptable alterations after a 17-month evaluation period.
Trial Registration Brazilian Registry of Clinical Trials (ReBEC) Identifier:
RBR-97kx5jv -
Citations
Citations to this article as recorded by- The Effect of Intraorifice Barrier Materials on the Fracture Resistance of Endodontically Treated Teeth: A Systematic Review and Network Meta-Analysis
Sevilay Karahan, Zeynep Buket Dağ, Emel Uzunoğlu Özyürek
Journal of Endodontics.2026; 52(5): 696. CrossRef - A Systematic Review and Meta-Analysis on the Clinical Performance and Longevity of Bioactive Composite Resin Restorations
Ahmed A. Holiel, Mounir M. Al Nakouzi, Rim Bourgi, Carlos Enrique Cuevas-Suárez, Iván Olivares Acosta, Louis Hardan, Naji Kharouf, Youssef Haikel
Journal of Composites Science.2026; 10(1): 39. CrossRef - Evaluation of Clinical Performance of Alkasite Restorative Materials: A Systematic Review and Meta-Analysis
Chloé Laporte, Rim Bourgi, Carlos Enrique Cuevas-Suárez, Naji Kharouf, Louis Hardan, Miguel Ángel Fernández-Barrera, Anh Tuan Dang, Youssef Haikel, Abigailt Flores-Ledesma
Journal of Functional Biomaterials.2026; 17(2): 93. CrossRef - 48-month clinical performance of an Alkasite restorative material versus resin composite in class II restorations: a randomized controlled trial
Ece Meral, Betül Kesim, Fatma Dilşad Öz, Sevil Gürgan
Journal of Dentistry.2026; 173: 106792. CrossRef - Alkasites in restorative dentistry: a review of their performance and properties
Alexander Bonchev, Ralitsa Bogovska-Gigova
Journal of Dentistry.2025; 160: 105916. CrossRef - Comparative Analysis of Flexural and Compressive Strengths of Bioactive Alkasite Compared to Other Ion-Releasing Restorative Materials
Hanin E. Yeslam, Fatin A. Hasanain
Biomimetics.2025; 10(11): 751. CrossRef
- The Effect of Intraorifice Barrier Materials on the Fracture Resistance of Endodontically Treated Teeth: A Systematic Review and Network Meta-Analysis
- 5,035 View
- 152 Download
- 5 Web of Science
- 6 Crossref
- Effects of surrounding and underlying shades on the color adjustment potential of a single-shade composite used in a thin layer
- Mariana Silva Barros, Paula Fernanda Damasceno Silva, Márcia Luciana Carregosa Santana, Rafaella Mariana Fontes Bragança, André Luis Faria-e-Silva
- Restor Dent Endod 2023;48(1):e7. Published online December 29, 2022
- DOI: https://doi.org/10.5395/rde.2023.48.e7
-
Abstract
PDFPubReaderePub
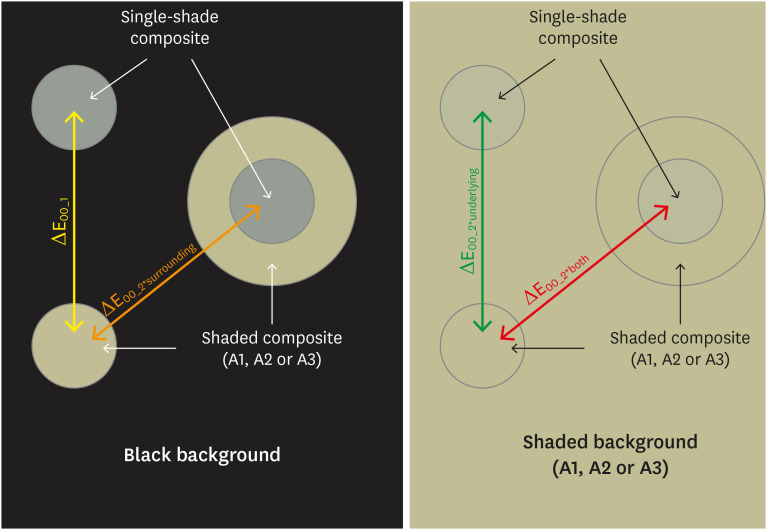
Objectives This study aimed to evaluate the surrounding and underlying shades’ effect on the color adjustment potential (CAP) of a single-shade composite used in a thin layer.
Materials and Methods Cylinder specimens (1.0 mm thick) were built with the Vittra APS Unique composite, surrounded (dual specimens) or not (simple specimens) by a control composite (shade A1, A2, or A3). Simple specimens were also built only with the control composites. Each specimen’s color was measured against white and black backgrounds or the simple control specimens with a spectrophotometer (CIELAB system). The whiteness index for dentistry (WID) and translucency parameters (TP00) were calculated for simple specimens. Differences (ΔE00) in color between the simple/dual specimens and the controls were calculated. The CAP was calculated based on the ratios between data from simple and dual specimens.
Results The Vittra APS Unique composite showed higher WID and TP00 values than the controls. The highest values of ΔE00 were observed among simple specimens. The color measurements of Vittra APS Unique (simple or dual) against the control specimens presented the lowest color differences. Only surrounding the single-shade composite with a shaded composite barely impacted the ΔE00. The highest CAP values were obtained using a shaded composite under simple or dual specimens.
Conclusions The CAP of Vittra APS Unique was strongly affected by the underlying shade, while surrounding this composite with a shaded one barely affected its color adjustment.
-
Citations
Citations to this article as recorded by- Impact of water absorption on the translucency of single-shade and conventional resin composites: an in vitro comparative study
Ceyda Sari, Elifnur Aydemir Aydın
Odontology.2026;[Epub] CrossRef - Baseline color-matching in anterior non-carious cervical lesions of patients of two single-shade resin composites: a randomized clinical trial
Ayşe Nur Doğan, Soley Arslan
Odontology.2026;[Epub] CrossRef - Evaluation of color blending effect of a single-shade resin composite with hybrid ceramics: an in vitro study
Jongchan Lee, Jinsoo Ahn, Sun-Young Kim
BMC Oral Health.2026;[Epub] CrossRef - At‐Home and In‐Office Bleaching Protocols on the Color Match of Restorations Made With Single‐Shade Composites
Luciana Vasconcelos Ramos, Dayana Fernandes Rocha Aparicio, André Luis Faria‐e‐Silva, Maíra do Prado, Andréa Vaz Braga Pintor, Marcela Baraúna Magno
Journal of Esthetic and Restorative Dentistry.2025; 37(6): 1567. CrossRef - Evaluation of color matching of three single-shade composites employing simulated 3D printed cavities with different thicknesses using CIELAB and CIEDE2000 color difference formulae
Engin Kariper, Aylin Cilingir
REVIEWS ON ADVANCED MATERIALS SCIENCE.2025;[Epub] CrossRef - Impact of kombucha, coffee, and turmeric beverages on the color stability of a single-shade versus a multi-shade resin-based composite
Hanin E. Yeslam, Abdulaziz F. Bakhsh
PeerJ.2025; 13: e19759. CrossRef - Comparative Study of Esthetic Outcome of Pedo Shades of Composite Resin—A Randomized Controlled Trial: In Vivo and In Vitro Study
Priyanka Raj, Shikha Choubey, Divya Doneria, Diksha Bhat, Shivani Mathur, Shailja Sinha
International Journal of Clinical Pediatric Dentistry.2025; 18(S1): S22. CrossRef - Influence of cavity wall thickness on the color adjustment potential of single-shade resin composites
Fabrício Luscino Alves de Castro, Letícia Brandão Durand
The Journal of the American Dental Association.2024; 155(7): 605. CrossRef - Assessing color mismatch in single-shade composite resins for enamel replacement
Rafaella Mariana Fontes de Bragança, Diana Leyva Del Rio, Luiz Alves Oliveira-Neto, William Michael Johnston
The Journal of Prosthetic Dentistry.2024; 132(3): 613.e1. CrossRef - Color discrepancy of single-shade composites at different distances from the interface measured using cell phone images
Márcia Luciana Carregosa Santana, Gabriella de Jesus Santos Livi, André Luis Faria-e-Silva
Restorative Dentistry & Endodontics.2024;[Epub] CrossRef - Is It Possible for Single-shade Composites to Mimic the Color, Lightness, Chroma, and Hue of Other Single-shade Composites? An In Vitro Study
M Buldur, G Ayan
Operative Dentistry.2024; 49(6): 691. CrossRef - Color evaluation of a one-shade used for restoration of non-carious cervical lesions: an equivalence randomized clinical trial
Michael Willian Favoreto, Amanda de Oliveira de Miranda, Thalita P. Matos, Andrea dos Santos de Castro, Mylena de Abreu Cardoso, Julia Beatriz, Jenny Collantes-Acuña, Alessandra Reis, Alessandro Dourado Loguercio
BMC Oral Health.2024;[Epub] CrossRef - Influence of Thickness on the Translucency Parameter and Whiteness Index of Single-Shade Resin Composites
Ö Yağcı, M Fidan
Operative Dentistry.2024; 49(2): 189. CrossRef - A Comparative Study of the Sensitivity and Specificity of the Ishihara Test With Various Displays
Thomas Klinke, Wolfgang Hannak, Klaus Böning, Holger Jakstat
International Dental Journal.2024; 74(4): 892. CrossRef - Color match evaluation using instrumental method for three single-shade resin composites before and after in-office bleaching
Aylin Cilingir, Engin Kariper
REVIEWS ON ADVANCED MATERIALS SCIENCE.2023;[Epub] CrossRef - The role of interface distance and underlying substrate on the color adjustment potential of single‐shade composites
Gabriella Jesus Santos de Livi, Tauan Rosa Santana, Rafaella Mariana Fontes Bragança, Rosa Maria Viana de Bragança Garcez, André Luis Faria‐e‐Silva
Journal of Esthetic and Restorative Dentistry.2023; 35(8): 1279. CrossRef
- Impact of water absorption on the translucency of single-shade and conventional resin composites: an in vitro comparative study
- 5,525 View
- 122 Download
- 16 Web of Science
- 16 Crossref
- Errors in light-emitting diodes positioning when curing bulk fill and incremental composites: impact on properties after aging
- Abdulrahman A. Balhaddad, Isadora M. Garcia, Haifa Maktabi, Maria Salem Ibrahim, Qoot Alkhubaizi, Howard Strassler, Fabrício M. Collares, Mary Anne S. Melo
- Restor Dent Endod 2021;46(4):e51. Published online September 24, 2021
- DOI: https://doi.org/10.5395/rde.2021.46.e51

-
Abstract
PDFPubReaderePub
Objectives This study aimed to evaluate the effect of improper positioning single-peak and multi-peak lights on color change, microhardness of bottom and top, and surface topography of bulk fill and incremental composites after artificial aging for 1 year.
Materials and Methods Bulk fill and incremental composites were cured using multi-peak and single-peak light-emitting diode (LED) following 4 clinical conditions: (1) optimal condition (no angulation or tip displacement), (2) tip-displacement (2 mm), (3) slight tip angulation (α = 20°) and (4) moderate tip angulation (α = 35°). After 1-year of water aging, the specimens were analyzed for color changes (ΔE), Vickers hardness, surface topography (Ra, Rt, and Rv), and scanning electron microscopy.
Results For samples cured by single-peak LED, the improper positioning significantly increases the color change compared to the optimal position regardless of the type of composite (
p < 0.001). For multi-peak LED, the type of resin composite and the curing condition displayed a significant effect on ΔE (p < 0.001). For both LEDs, the Vickers hardness and bottom/top ratio of Vickers hardness were affected by the type of composite and the curing condition (p < 0.01).Conclusions The bulk fill composite presented greater resistance to wear, higher color stability, and better microhardness than the incremental composite when subjected to improper curing. The multi-peak LED improves curing under improper conditions compared to single-peak LED. Prevention of errors when curing composites requires the attention of all personnel involved in the patient's care once the clinical relevance of the appropriate polymerization reflects on reliable long-term outcomes.
-
Citations
Citations to this article as recorded by- A clinical survey of the output intensity of 50 light-curing units in dental clinics across Davangere and Mangalore region using a spectrometer system
Elizbeth Christy Jose, Sakshi Jha, Prema Shantagouda Biradar, J Arun, TN Nandini, Thushara Mohanan
International Journal of Oral Health Sciences.2025; 15(1): 41. CrossRef - The demineralization resistance and mechanical assessments of different bioactive restorative materials for primary and permanent teeth: an in vitro study
Maria Salem Ibrahim, Fahad Rakad Aldhafeeri, Abdullah Sami Banaemah, Mana S. Alhaider, Yousif A. Al-Dulaijan, Abdulrahman A. Balhaddad
BDJ Open.2024;[Epub] CrossRef - Inorganic Compounds as Remineralizing Fillers in Dental Restorative Materials: Narrative Review
Leena Ibraheem Bin-Jardan, Dalal Ibrahim Almadani, Leen Saleh Almutairi, Hadi A. Almoabid, Mohammed A. Alessa, Khalid S. Almulhim, Rasha N. AlSheikh, Yousif A. Al-Dulaijan, Maria S. Ibrahim, Afnan O. Al-Zain, Abdulrahman A. Balhaddad
International Journal of Molecular Sciences.2023; 24(9): 8295. CrossRef
- A clinical survey of the output intensity of 50 light-curing units in dental clinics across Davangere and Mangalore region using a spectrometer system
- 2,287 View
- 20 Download
- 2 Web of Science
- 3 Crossref
- Evaluation of the relation between the pulp stones and direct restorations using cone beam computed tomography in a Turkish subpopulation
- Güzide Pelin Sezgin, Sema Sönmez Kaplan, Tuna Kaplan
- Restor Dent Endod 2021;46(3):e34. Published online June 8, 2021
- DOI: https://doi.org/10.5395/rde.2021.46.e34
-
Abstract
PDFPubReaderePub
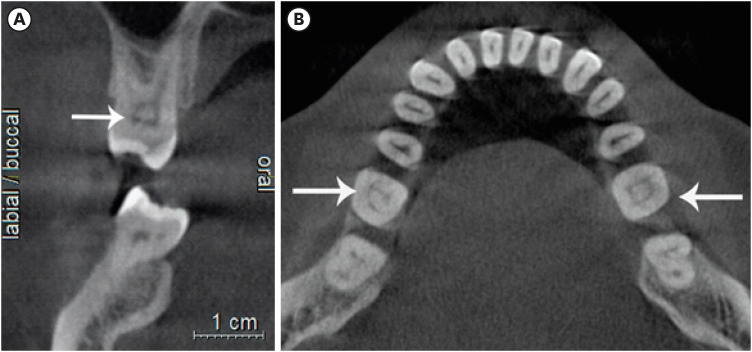
Objectives This study aimed to assess the presence of pulp stones through an examination of cone beam computed tomography images and correlate their prevalence with age, sex, dental arch and side, tooth type, and restoration type and depth.
Materials and Methods Cone beam computed tomography images obtained from 673 patients and archival data on 11,494 teeth were evaluated. The associations of pulp stones with age, sex, dental arch and side, tooth type, and restoration type and depth were noted. All the measurements were subjected to a χ2 test and one sample χ2 test (
p < 0.05).Results In the study group, 163 (24.2%) patients and 379 (3.3%) teeth had at least one pulp stone. The pulp stone frequency in those aged 30–39 years was significantly greater than in those aged 18–29 and ≥ 60 years, and the frequency was higher in females than in males (
p < 0.05). The highest prevalence of pulp stones was found in maxillary dental arches and molar teeth (p < 0.05). Pulp stones were significantly more common in medium-depth restorations (p < 0.05).Conclusions Maxillary molar teeth, medium-depth restorations, individuals aged 30–39 years and females had a greater percentage of pulp stones.
-
Citations
Citations to this article as recorded by- Comparative Detection and Inter-Modality Agreement of Pulp Stones Using Digital Periapical Radiography and CBCT at Two Voxel Sizes: An Ex Vivo Study
Hassan Hamed Kaabi, Sarah Saeed Binhassan, Sultan Hamad Alrumaih, Mohammed Jamal Alotaibi, Abdullah Khalid Bakarman, Nawaf Abdulaziz Alghamdi, Hamad Abdullah Almuhaythif, Qamar Mohammadziad Hashem, Abdulfatah Samih Alazmah
Diagnostics.2026; 16(7): 961. CrossRef - Cone-Beam Computed Tomography Assessment of the Prevalence and Association of Pulp Calcification with Dental and Periodontal Pathology: A Descriptive Study
José Luis Sanz, Lucía Callado, Stefana Mantale, Jenifer Nicolás, James Ghilotti, Carmen Llena
Journal of Clinical Medicine.2025; 14(4): 1373. CrossRef - Prevalence of mineralization in the pulp chamber in patients according to CBCT data
V. A. Molokova, I. N. Antonova, V. A. Osipova
Endodontics Today.2025; 23(2): 188. CrossRef - Could carotid artery calcifications and pulp stones be an alarm sign for diabetes mellitus? A retrospective observational study
Motahare Baghestani, Mohadese Faregh, Seyed Hossein Razavi, Fatemeh Owlia
BMC Endocrine Disorders.2025;[Epub] CrossRef - Distribution and influencing factors of pulp stones based on CBCT: a retrospective observational study from southwest China
Wantong Zhang, Yao Wang, Lin Ye, Yan Zhou
BMC Oral Health.2024;[Epub] CrossRef - Prevalence and Association of Calcified Pulp Stones with Periodontitis: A Cone-Beam Computed Tomography Study in Saudi Arabian Population
Abdullah Saad Alqahtani
Journal of Pharmacy and Bioallied Sciences.2024; 16(Suppl 1): S644. CrossRef - The Prevalence And Distribution Of Pulp Stones: A Cone-Beam Computed Tomography Study İn A Group Of Turkish Patients
Mujgan Firincioglulari, Seçil Aksoy, Melis Gülbeş, Umut Aksoy, Kaan Orhan
ADO Klinik Bilimler Dergisi.2024; 13(3): 496. CrossRef - Radiographical examination of pulp stone distribution by cone beam computed tomography
Fatma Tunç, Emre Çulha, Muazzez Naz Baştürk
Journal of Health Sciences and Medicine.2024; 7(4): 472. CrossRef - Cone-Beam Computed Tomography-Based Investigation of the Prevalence and Distribution of Pulp Stones and Their Relation to Local and Systemic Factors in the Makkah Population: A Cross-Sectional Study
Laila M Kenawi, Haytham S Jaha, Mashael M Alzahrani, Jihan I Alharbi, Shahad F Alharbi, Taif A Almuqati, Rehab A Alsubhi, Wahdan M Elkwatehy
Cureus.2024;[Epub] CrossRef - Cone beam computed tomography assessment of the prevalence and association of pulp calcification with periodontitis
Lingling Xiang, Botao Wang, Yuan Zhang, Jintao Wang, Peipei Wu, Jian Zhang, Liangjun Zhong, Rui He
Odontology.2023; 111(1): 248. CrossRef - Three-dimensional analysis for detection of pulp stones in a Saudi population using cone beam computed tomography
Hassan H. Kaabi, Abdullah M. Riyahi, Nassr S. Al-Maflehi, Saleh F. Alrumayyan, Abdullah K. Bakrman, Yazeed A. Almutaw
Journal of Oral Science.2023; 65(4): 257. CrossRef
- Comparative Detection and Inter-Modality Agreement of Pulp Stones Using Digital Periapical Radiography and CBCT at Two Voxel Sizes: An Ex Vivo Study
- 2,856 View
- 33 Download
- 12 Web of Science
- 11 Crossref
- The polymerization efficiency of a bulk-fill composite based on matrix-modification technology
- Tarek M. Elshazly, Christoph Bourauel, Moustafa N. Aboushelib, Dalia I. Sherief, Dalia I. El-Korashy
- Restor Dent Endod 2020;45(3):e32. Published online May 29, 2020
- DOI: https://doi.org/10.5395/rde.2020.45.e32

-
Abstract
PDFPubReaderePub
Objectives To evaluate the polymerization efficiency of a matrix-modified bulk-fill composite, and compare it to a conventional composite which has a similar filler system. The degree of conversion (DC%) and monomer elution were measured over different storage periods. Additionally, fillers' content was examined.
Materials and Methods Cylindrical specimens were prepared, in bulk and incrementally, from Filtek Bulk Fill (B) and Filtek Supreme XTE (S) composites using a Teflon mold, for each test (
n = 6). Using attenuated total reflection method of Fourier transformation infrared spectroscopy, DC% was measured after 24 hours, 7 days, and 30 days. Using high-performance liquid chromatography, elution of hydroxyethyl methacrylate, triethylene glycol dimethacrylate, urethane dimethacrylate, and bisphenol-A glycidyl dimethacrylate was measured after 24 hours, 7 days and 30 days. Filler content was examined by scanning electron microscopy (SEM). Data were analyzed using 2-way mixed-model analysis of variance (α = 0.05).Results There was no significant difference in DC% over different storage periods between B-bulk and S-incremental. Higher monomer elution was detected significantly from S than B. The elution quantity and rate varied significantly over storage periods and between different monomers. SEM images showed differences in fillers' sizes and agglomeration between both materials.
Conclusions Matrix-modified bulk-fill composites could be packed and cured in bulk with polymerization efficiency similar to conventional composites.
-
Citations
Citations to this article as recorded by- Mechanical Properties of Composite Core Build-Up Materials: A Comparative Study
Emily Mundy, Sanaya V. Engineer, Sheila Butler, Amin Rizkalla, Gildo Coelho Santos Junior, Maria Jacinta Moraes Coelho Santos
Materials.2026; 19(8): 1487. CrossRef - Comparative Evaluation of Volumetric Polymerization Shrinkage and Diametral Tensile Strength of Self-cure and Light-cure Composite Resins: An In Vitro Study
Eko Fibryanto, Imanuel B Wijaya, Fourier D Eljabbar, Elline Elline
International Journal of Prosthodontics and Restorative Dentistry.2026; 16(1): 17. CrossRef - Bioactive Fillers in Bulk-Fill Composite Resins: A Comprehensive Review of the Effects on Polymerization Shrinkage Behavior and Mechanical Performance
Vlad Constantin, Ionut Luchian, Ionut Taraboanta, Teona Anamaria Tudorici, Nicoleta Tofan, Florinel Cosmin Bida, Florin Razvan Curca, Dana Gabriela Budala, Dragos Ioan Virvescu, Andrei Georgescu
Materials.2026; 19(11): 2181. CrossRef - Evaluation of the degree of conversion of flowable bulk fill and dual-cure composite resins for intracanal root reinforcement in teeth with structurally weakened roots: An in vitro Fourier transformer infrared study
Saloni Sanjay Bhandari, Sumanthini V. Margasahayam, Vanitha Umesh Shenoy, Anuradha Bhausaheb Patil, Manasi Arun Surwade
Journal of Conservative Dentistry and Endodontics.2025; 28(12): 1279. CrossRef - Effect of Polywave and Monowave Light Curing Units on the Microtensile Bond Strength and Failure Types of Different Bulk-Fill Resin Composites: An in vitro Study
Leonor Castro-Ramirez, María Espinoza-Salcedo, José Huamani-Echaccaya, Marysela Ladera-Castañeda, Luis Cervantes-Ganoza, Emily Hernández-Huamaní, Rosa Aroste-Andía, Percy Gavilán-Chávez, César Cayo-Rojas
Clinical, Cosmetic and Investigational Dentistry.2024; Volume 16: 153. CrossRef - Effect of Aging of Orthodontic Aligners in Different Storage Media on Force and Torque Generation: An In Vitro Study
Tarek M. Elshazly, Diva Nang, Bijan Golkhani, Hanaa Elattar, Christoph Bourauel
Oral.2023; 3(1): 67. CrossRef - Delayed light‐curing of dual‐cure bulk‐fill composites on internal adaptation and depth of cure
Lucas Dutra Rissato, May Anny Alves Fraga, Michelly Pires Gonçalves, Mario Alexandre Coelho Sinhoreti, Lourenço Correr‐Sobrinho, Américo Bortolazzo Correr
Journal of Esthetic and Restorative Dentistry.2023; 35(4): 698. CrossRef - Interfacial integrity of bulk-fill resin composite restorations in deep Class-II cavities
Rana Abdelrehim SEDKY, Hooi Pin CHEW, Khaled Aly NOUR, Shaimaa Mohamed ABUELSADAT, Dina ELSHERBINI, Alex Siu Lun FOK
Dental Materials Journal.2023; 42(5): 692. CrossRef - Effect of thermomechanical aging of orthodontic aligners on force and torque generation: An in vitro study
Tarek M. Elshazly, Diva Nang, Bijan Golkhani, Hanaa Elattar, Ludger Keilig, Christoph Bourauel
Journal of the Mechanical Behavior of Biomedical Materials.2023; 143: 105911. CrossRef - The influence of different placement techniques on the clinical success of bulk-fill resin composites placed in Class II cavities: a 4-year randomized controlled clinical study
Nazire Nurdan Çakır Kılınç, Sezer Demirbuğa
Clinical Oral Investigations.2022; 27(2): 541. CrossRef - Comparative Evaluation of Bulk-Fill Composite Resins: Knoop Microhardness, Diametral Tensile Strength and Degree of Conversion
Bruna Scarcello Strini, Joyce Figueiredo de Lima Marques, Renata Pereira, Danielle Ferreira Sobral-Souza, Vanessa Gallego Arias Pecorari, Priscila Christiane Suzy Liporoni, Flávio Henrique Baggio Aguiar
Clinical, Cosmetic and Investigational Dentistry.2022; Volume 14: 225. CrossRef
- Mechanical Properties of Composite Core Build-Up Materials: A Comparative Study
- 3,305 View
- 20 Download
- 11 Crossref
Case Report
- A CAD/CAM-based strategy for concurrent endodontic and restorative treatment
- Patricia Maria Escobar, Anil Kishen, Fabiane Carneiro Lopes, Caroline Cristina Borges, Eugenio Gabriel Kegler, Manoel Damião Sousa-Neto
- Restor Dent Endod 2019;44(3):e27. Published online July 24, 2019
- DOI: https://doi.org/10.5395/rde.2019.44.e27
-
Abstract
PDFPubReaderePub
This case report describes a technique in which endodontic treatment and permanent indirect restoration were completed in the same clinical appointment with the aid of a computer-aided design/computer-aided manufacturing (CAD/CAM) system. Two patients were diagnosed with irreversible pulpitis of the mandibular first molar. After access preparation, root canals were located, irrigation was performed until bleeding ceased, and the coronal tooth structure was prepared for indirect restoration. Then, utilizing an interim 3-mm build-up of the endodontic access cavity, a hemi-arch digital scan was performed with an intraoral scanner. Subsequent to digital scanning, restoration design was performed simultaneously with the endodontic procedure. The root canals were shaped using the Race system under irrigation with 2.5% sodium hypochlorite followed by root canal filling. The pulp chamber was subsequently filled with a 3-mm-thick composite resin restoration mimicking the interim build-up previously utilized to facilitate block milling in the CAD/CAM system. Clinical try-in of the permanent onlay restoration was followed by acid etching, application of a 5th generation adhesive, and cementation of the indirect restoration. Once the restoration was cemented, rubber dam isolation was removed, followed by occlusal adjustment and polishing. After 2 years of follow-up, the restorations were esthetically and functionally satisfactory, without complications.
-
Citations
Citations to this article as recorded by- Effect of root canal molding method on bond strength and cement thickness of milled fiber posts
Geovane Evangelista Moreira, João Pedro Rangel-Coelho, Lísia Aparecida Costa Gonçalves, Denismar Alves Nogueira, Roberta Tarkany Basting, Cecilia Pedroso Turssi, Flávia Lucisano Botelho Amaral
Odontology.2026;[Epub] CrossRef - Pretreatment Effects on the Microtensile Bond Strength Between a Bulk-Fill Resin-Based Composite Cavity Base Material and Methyl Methacrylate (MMA)-Based Luting Cement
Reiko Kohsaka, Saho Komatsu, Akiko Haruyama, Toshiaki Ara, Akihiro Kuroiwa, Nobuo Yoshinari, Atsushi Kameyama
Micro.2026; 6(2): 32. CrossRef - Endodontic Management with Posterior Indirect Adhesive Restoration by CAD-CAM Procedure - Case Report
Intan Syuhada, Wandania Farahanny, Widi Prasetia
Journal of Evolution of Medical and Dental Sciences.2025; : 88. CrossRef - Evaluation of Marginal Adaptation of Three Different Materials Restored in Class II Inlay Cavity Preparations: An In Vitro Study
Rajasekhar Vemareddy, Someshwar Battu, Jyotsnanjali Thati, Sudhakar Naidu, Balaraju Korrai, Akhila Nalli
World Journal of Dentistry.2024; 15(5): 411. CrossRef
- Effect of root canal molding method on bond strength and cement thickness of milled fiber posts
- 4,605 View
- 43 Download
- 4 Crossref
Research Article
- Influence of different universal adhesives on the repair performance of hybrid CAD-CAM materials
- Gülbike Demirel, İsmail Hakkı Baltacıoğlu
- Restor Dent Endod 2019;44(3):e23. Published online May 20, 2019
- DOI: https://doi.org/10.5395/rde.2019.44.e23
-
Abstract
PDFPubReaderePub
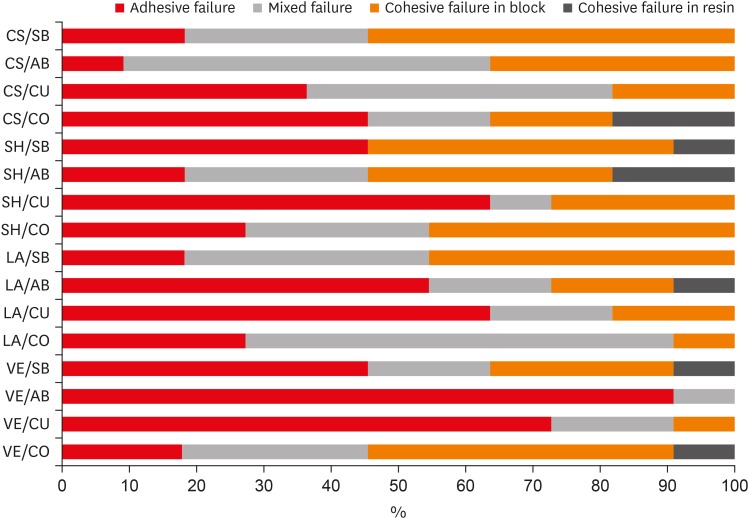
Objectives The aim of this study was to investigate the microshear bond strength (μSBS) of different universal adhesive systems applied to hybrid computer-aided design/computer-aided manufacturing (CAD-CAM) restorative materials repaired with a composite resin.
Materials and Methods Four types of CAD-CAM hybrid block materials—Lava Ultimate (LA), Vita Enamic (VE), CeraSmart (CS), and Shofu Block HC (SH)—were used in this study, in combination with the following four adhesive protocols: 1) control: porcelain primer + total etch adhesive (CO), 2) Single Bond Universal (SB), 3) All Bond Universal (AB), and 4) Clearfil Universal Bond (CU). The μSBS of the composite resin (Clearfil Majesty Esthetic) was measured and the data were analyzed using two-way analysis of variance and the Tukey test, with the level of significance set at
p < 0.05.Results The CAD-CAM block type and block-adhesive combination had significant effects on the bond strength values (
p < 0.05). Significant differences were found between the following pairs of groups: VE/CO and VE/AB, CS/CO and CS/AB, VE/CU and CS/CU, and VE/AB and CS/AB (p < 0.05).Conclusions The μSBS values were affected by hybrid block type. All tested universal adhesive treatments can be used as an alternative to the control treatment for repair, except the AB system on VE blocks (the VE/AB group). The μSBS values showed variation across different adhesive treatments on different hybrid CAD-CAM block types.
-
Citations
Citations to this article as recorded by- Micro-shear bond strength of repaired additively manufactured resin composites after artificial aging: effect of surface treatment and universal adhesives
Neşe Ciziroğlu, Didar Dilan Hartavi, Rafat Sasany, Mutlu Özcan
Journal of Adhesion Science and Technology.2026; : 1. CrossRef - Effect of surface treatments on the bond strength of resin-repaired resin matrix CAD-CAM ceramic: A scoping review
Ana Beatriz de Souza Albergardi, João Pedro Justino de Oliveira Limírio, Jéssica Marcela de Luna Gomes, Aldiéris Alves Pesqueira, Eduardo Piza Pellizzer
Journal of Dentistry.2025; 154: 105594. CrossRef - Bond strength to aged CAD/CAM composites and polymer-infiltrated ceramic network using a universal adhesive with or without previous application of a universal primer
Clemens Lechte, Lisa Sophia Faesser, Jana Biermann, Alexandra Schmidt, Philipp Kanzow, Annette Wiegand
International Journal of Adhesion and Adhesives.2025; 140: 104017. CrossRef - The Influence of Thermocycling and Ultraviolet Aging on Surface Characteristics and the Repair Bond Strength of CAD/CAM Resin Nanoceramics
Beyza Unalan Degirmenci, Alperen Degirmenci, Zelal Seyfioglu Polat
Journal of Functional Biomaterials.2025; 16(5): 156. CrossRef - Impact of in vitro findings on clinical protocols for the adhesion of CAD-CAM blocks: A systematic integrative review and meta-analysis
Maria João Calheiros-Lobo, Ricardo Carbas, Lucas F.M. da Silva, Teresa Pinho
The Journal of Prosthetic Dentistry.2024; 131(6): 1051. CrossRef - Repair protocols for indirect monolithic restorations: a literature review
Lucas Saldanha da Rosa, Rafaela Oliveira Pilecco, Pablo Machado Soares, Marília Pivetta Rippe, Gabriel Kalil Rocha Pereira, Luiz Felipe Valandro, Cornelis Johannes Kleverlaan, Albert J. Feilzer, João Paulo Mendes Tribst
PeerJ.2024; 12: e16942. CrossRef - Bonding performance of universal adhesives with concomitant use of silanes to CAD/CAM blocks
Marina AMARAL, Jaqueline Maria Brandão RIZZATO, Victoria Caroline Souza de ALMEIDA, Priscila Christiane Suzy LIPORONI, Rayssa Ferreira ZANATTA
RGO - Revista Gaúcha de Odontologia.2023;[Epub] CrossRef - Resistencia a la fractura de una nanocerámica CAD/CAM reparada con dos tratamientos de superficie: estudio in vitro
Marcelo Geovanny Cascante-Calderón, Kevin Alejandro Reascos Flores, Inés María Villacís-Altamirano, Anggely Maite Bayas Salinas, Jessica Elizabeth Taraguay Galindo
Universitas Odontologica.2023;[Epub] CrossRef - Influence of surface treatments and adhesive protocols on repair bond strength of glass‐matrix and resin‐matrix CAD/CAM ceramics
Rana Turunç‐Oğuzman, Soner Şişmanoğlu
Journal of Esthetic and Restorative Dentistry.2023; 35(8): 1322. CrossRef - Effect of Anti-COVID-19 Mouthwashes on Shear Bond Strength of Resin-Matrix Ceramics Repaired with Resin Composite Using Universal Adhesive: An In Vitro Study
Wichuda Limsiriwong, Awiruth Klaisiri, Nantawan Krajangta
Journal of Functional Biomaterials.2023; 14(3): 158. CrossRef - Effect of ceramic primers with different chemical contents on the shear bond strength of CAD/CAM ceramics with resin cement after thermal ageing
Mehmet Uğur, İdris Kavut, Özgür Ozan Tanrıkut, Önder Cengiz
BMC Oral Health.2023;[Epub] CrossRef - Effect of microstructure of reinforced CAD/CAM hybrid composite resin block on shear bond strength of composite resin
Sung-Ho Um, Minjeong Shin, Shin-hye Chung, Young-Seok Park, Bum-Soon Lim
Korean Journal of Dental Materials.2023; 50(1): 29. CrossRef - Dentin contamination during repair procedures: A threat to universal adhesives?
Anne‐Katrin Lührs, Cosima Brachmann, Silke Jacker‐Guhr
Clinical and Experimental Dental Research.2022; 8(3): 771. CrossRef - Influence of mechanical and chemical pre-treatments on the repair of a hybrid ceramic
Sascha Niklas Jung, Stefan Rüttermann
Dental Materials.2022; 38(7): 1140. CrossRef - Influence of different repair protocols and artificial aging on bond strength of composite to a CAD/CAM polymer-infiltrated ceramic
Ece İrem OĞUZ, Gökhan ÇİÇEKCİ
Cumhuriyet Dental Journal.2021; 24(1): 37. CrossRef - REZİN MATRİKS SERAMİKLER-DERLEME
Elif Melike AKARCA, Dilara ŞAHİN, Ragibe Şenay CANAY
Atatürk Üniversitesi Diş Hekimliği Fakültesi Dergisi.2021; : 1. CrossRef - REZİN MATRİKS SERAMİKLER-DERLEME
Elif Melike AKARCA, Dilara ŞAHİN, Ragibe Şenay CANAY
Atatürk Üniversitesi Diş Hekimliği Fakültesi Dergisi.2021; : 1. CrossRef - Microshear bond strength of contemporary self-adhesive resin cements to CAD/CAM restorative materials: effect of surface treatment and aging
Soner Şişmanoğlu, Rana Turunç-Oğuzman
Journal of Adhesion Science and Technology.2020; 34(22): 2484. CrossRef - Influence of different surface treatments and universal adhesives on the repair of CAD-CAM composite resins: An in vitro study
Soner Sismanoglu, Zuhal Yildirim-Bilmez, Aysegul Erten-Taysi, Pınar Ercal
The Journal of Prosthetic Dentistry.2020; 124(2): 238.e1. CrossRef
- Micro-shear bond strength of repaired additively manufactured resin composites after artificial aging: effect of surface treatment and universal adhesives
- 4,317 View
- 19 Download
- 19 Crossref
Case Report
- Management of large class II lesions in molars: how to restore and when to perform surgical crown lengthening?
- Ana Belén Dablanca-Blanco, Juan Blanco-Carrión, Benjamín Martín-Biedma, Purificación Varela-Patiño, Alba Bello-Castro, Pablo Castelo-Baz
- Restor Dent Endod 2017;42(3):240-252. Published online August 3, 2017
- DOI: https://doi.org/10.5395/rde.2017.42.3.240
-
Abstract
PDFPubReaderePub
The restoration of endodontic tooth is always a challenge for the clinician, not only due to excessive loss of tooth structure but also invasion of the biological width due to large decayed lesions. In this paper, the 7 most common clinical scenarios in molars with class II lesions ever deeper were examined. This includes both the type of restoration (direct or indirect) and the management of the cavity margin, such as the need for deep margin elevation (DME) or crown lengthening. It is necessary to have the DME when the healthy tooth remnant is in the sulcus or at the epithelium level. For caries that reaches the connective tissue or the bone crest, crown lengthening is required. Endocrowns are a good treatment option in the endodontically treated tooth when the loss of structure is advanced.
-
Citations
Citations to this article as recorded by- Adhesive Restoration Performance in Deep Subgingival Margins: Deep Margin Elevation Versus Surgical Crown Lengthening—A Systematic Review
Margherita Ceravolo, Filipe Castro, Antonio González-Mosquera, Alicia López-Solache, Patrícia Manarte-Monteiro, Lígia Pereira da Silva
Adhesives.2026; 2(2): 9. CrossRef - Awareness and Practice of Deep Margin Elevation among Dental Practitioners in India: A Cross-Sectional Survey
Mythri Padaru, Preethesh Shetty, Namith Rai, Raksha Bhat
Pesquisa Brasileira em Odontopediatria e Clínica Integrada.2025;[Epub] CrossRef - Rubber dam isolation to optimise intraoral scanning and the restoration of teeth with subgingival margins
Renato Lardin Sartori Sanchez, Gisele Lie Fukuoka, Nathália Pereira Censi Stapani, Isabella Neme Ribeiro dos Reis
BMJ Case Reports.2025; 18(4): e264082. CrossRef - Impact of spacers and thermocycling on porosity and gaps in class II endodontic temporary restorations evaluated by microcomputed tomography
Fahda N. Algahtani, Manal Alkadi, Hiba R. Talic, Sarah S. AlShalawi, Lujain M. Alqarni, Reem M. Barakat, Rasha Haridy, Sara M. ElKhateeb, Rahaf A. Almohareb
Scientific Reports.2025;[Epub] CrossRef - Deep Margin Elevation: Current Evidence and a Critical Approach to Clinical Protocols—A Narrative Review
Athanasios Karageorgiou, Maria Fostiropoulou, Maria Antoniadou, Eftychia Pappa
Adhesives.2025; 1(3): 10. CrossRef - Deep margin elevation in restorative dentistry: A scoping review
Anna Taylor, Lorna Burns
Journal of Dentistry.2024; 146: 105066. CrossRef - Effect of cervical margin relocation on marginal adaptation and microleakage of indirect ceramic restorations
Marwa Adel, Amina Hamdy, Ahmed Sabet, Kamal Ebeid
Journal of Prosthodontics.2024; 33(4): 374. CrossRef - Application of one-piece endodontic crowns fabricated with CAD-CAM system to molars
Haruto Hiraba, Kensuke Nishio, Yoshimasa Takeuchi, Takashi Ito, Tetsuo Yamamori, Atsushi Kamimoto
Japanese Dental Science Review.2024; 60: 81. CrossRef - Structurally compromised teeth. Part II: A novel approach to peripheral build up procedures
Guido Fichera, Claudia Mazzitelli, Vincenzo Picciariello, Tatjana Maravic, Uros Josic, Annalisa Mazzoni, Lorenzo Breschi
Journal of Esthetic and Restorative Dentistry.2024; 36(1): 20. CrossRef - Biomimetic Restorative Dentistry: an evidence-based discussion of common myths
Alessandra REIS, Victor Pinheiro FEITOSA, Ana Cláudia CHIBINSKI, Michael Willian FAVORETO, Mario Felipe GUTIERREZ, Alessandro Dourado LOGUERCIO
Journal of Applied Oral Science.2024;[Epub] CrossRef - Comparative clinical evaluation of correct anatomic contour and tight contact in Class II direct composite restoration using two newer contact forming instruments
Jaimini Patel, Nimisha C. Shah, Meetkumar Dedania, Deebah Choudhary, Nidhi Bharti, Aishwarya Jain
Journal of Conservative Dentistry and Endodontics.2024; 27(11): 1135. CrossRef - Effect of Deep Margin Elevation on the Pulpal and Periodontal Health of Teeth: A Systematic Review
S Srirama, S Jain, B Arul, K Prabakar, V Natanasabapathy
Operative Dentistry.2024; 49(4): 388. CrossRef - New Technique for Wedge Selection in Direct Class II Restorations: A Pilot Study
Tania Gancedo-Gancedo, Benjamín Martín-Biedma, Javier Domínguez-Cachón, Sara Garrido-Parada, Victoria Ababii, Patricia Pereira-Lores, Sandra García-Varela, Pablo Castelo-Baz
Journal of Clinical Medicine.2024; 13(5): 1324. CrossRef - Different Designs of Deep Marginal Elevation and Its Influence on Fracture Resistance of Teeth with Monolith Zirconia Full-Contour Crowns
Ali Robaian, Abdullah Alqahtani, Khalid Alanazi, Abdulrhman Alanazi, Meshal Almalki, Anas Aljarad, Refal Albaijan, Ahmed Maawadh, Aref Sufyan, Mubashir Baig Mirza
Medicina.2023; 59(4): 661. CrossRef - M-i-M for DME: matrix-in-a-matrix technique for deep margin elevation
Pascal Magne
The Journal of Prosthetic Dentistry.2023; 130(4): 434. CrossRef - A New Concept of Posterior Mini-invasive Restorations: Clinical Procedures and Requirements—Case Report
Zeineb Riahi, Belhassen Harzallah, Mounir Cherif, Dalenda Hadyaoui, Imen Kalghoum, Oumayma Mejri
CODS - Journal of Dentistry.2023; 14(2): 61. CrossRef - Evaluation of biologic width re-establishment using CHU aesthetic gauges in crown lengthening cases- a clinical study
Avantika Rani, Shiva Shankar Gummaluri, Hirak S. Bhattacharya, Preeti Bhattacharya, Sumbul Saifi, saummya singh
Journal of Oral Biology and Craniofacial Research.2023; 13(2): 138. CrossRef - Interfacial integrity of bulk-fill resin composite restorations in deep Class-II cavities
Rana Abdelrehim SEDKY, Hooi Pin CHEW, Khaled Aly NOUR, Shaimaa Mohamed ABUELSADAT, Dina ELSHERBINI, Alex Siu Lun FOK
Dental Materials Journal.2023; 42(5): 692. CrossRef - Biological evaluation of indirect restorations in endodontically treated posterior teeth with deeply located proximal margins following deep margin elevation versus surgical crown lengthening: a randomized controlled trial
Ahmed Tarek Farouk, Olfat El Sayed Hassanein, Ola Ibrahim Fahmy, Ahmed M. Elkady, Hani ElNahass
Clinical Oral Investigations.2023;[Epub] CrossRef - Deep Margin Elevation: Current Concepts and Clinical Considerations: A Review
Majed Aldakheel, Khalid Aldosary, Shatha Alnafissah, Rahaf Alaamer, Anwar Alqahtani, Nora Almuhtab
Medicina.2022; 58(10): 1482. CrossRef - Deep Margin Elevation: A Literature Review
Theodora Kalliopi Samartzi, Dimokritos Papalexopoulos, Panagiotis Ntovas, Christos Rahiotis, Markus B. Blatz
Dentistry Journal.2022; 10(3): 48. CrossRef - Examination of caries‐affected dentin and composite‐resin interface after different caries removal methods: A scanning electron microscope study
Nazmiye Donmez, Magrur Kazak, Zeynep Buket Kaynar, Yesim Sesen Uslu
Microscopy Research and Technique.2022; 85(6): 2212. CrossRef - Clinical performance of indirect restorations with cervical margin relocation in posterior teeth: A systematic review
Ghaida Alhumaidan, Raghad Alammar, Dhafer Al Asmari, Ali Alenezi
Dentistry Review.2022; 2(1): 100034. CrossRef - Current Strategies to Control Recurrent and Residual Caries with Resin Composite Restorations: Operator- and Material-Related Factors
Moataz Elgezawi, Rasha Haridy, Moamen A. Abdalla, Katrin Heck, Miriam Draenert, Dalia Kaisarly
Journal of Clinical Medicine.2022; 11(21): 6591. CrossRef - Survival and success of endocrowns: A systematic review and meta-analysis
Raghad A. Al-Dabbagh
The Journal of Prosthetic Dentistry.2021; 125(3): 415.e1. CrossRef - The Relationships Between Tooth‐Supported Fixed Dental Prostheses and Restorations and the Periodontium
Carlo Ercoli, Dennis Tarnow, Carlo E. Poggio, Alexandra Tsigarida, Marco Ferrari, Jack G. Caton, Konstantinos Chochlidakis
Journal of Prosthodontics.2021; 30(4): 305. CrossRef - Placement of Posterior Composite Restorations: A Cross-Sectional Study of Dental Practitioners in Al-Kharj, Saudi Arabia
Mohamed M. Awad, Mansour Alradan, Nawaf Alshalan, Ali Alqahtani, Feras Alhalabi, Mohammed Ali Salem, Ahmed Rabah, Ali Alrahlah
International Journal of Environmental Research and Public Health.2021; 18(23): 12408. CrossRef - Microleakage of Direct Restorations-Comparisonbetween Bulk-Fill and Traditional Composite Resins:Systematic Review and Meta-Analysis
Francesca Zotti, Edoardo Falavigna, Giorgia Capocasale, Daniele De Santis, Massimo Albanese
European Journal of Dentistry.2021; 15(04): 755. CrossRef - Assessment of knowledge, attitude, and practice regarding Deep Margin Elevation (DME) among dental practitioners in Riyadh, Saudi Arabia
Sultan R. Binalrimal, Weam M. Banjar, Sara H. Alyousef, Mada I. Alawad, Ghalia I. Alawad
Journal of Family Medicine and Primary Care.2021; 10(5): 1931. CrossRef - Treatment Prognosis of Restored Teeth with Crown Lengthening vs. Deep Margin Elevation: A Systematic Review
Maryam H. Mugri, Mohammed E. Sayed, Binoy Mathews Nedumgottil, Shilpa Bhandi, A. Thirumal Raj, Luca Testarelli, Zohaib Khurshid, Saurabh Jain, Shankargouda Patil
Materials.2021; 14(21): 6733. CrossRef - Direct resin composite restoration of endodontically-treated permanent molars in adolescents: bite force and patient-specific finite element analysis
Monise de Paula RODRIGUES, Priscilla Barbosa Ferreira SOARES, Márcio Alex Barros GOMES, Renata Afonso PEREIRA, Daranee TANTBIROJN, Antheunis VERSLUIS, Carlos Jose SOARES
Journal of Applied Oral Science.2020;[Epub] CrossRef - Up to 12 years clinical evaluation of 197 partial indirect restorations with deep margin elevation in the posterior region
R.A. Bresser, D. Gerdolle, I.A. van den Heijkant, L.M.A. Sluiter-Pouwels, M.S. Cune, M.M.M. Gresnigt
Journal of Dentistry.2019; 91: 103227. CrossRef - How biomechanics can affect the endodontic treated teeth and their restorative procedures?
Carlos José Soares, Monise de Paula Rodrigues, André Luis Faria-e-Silva, Paulo Cesar Freitas Santos-Filho, Crisnicaw Veríssimo, Hyeon-Cheol Kim, Antheunis Versluis
Brazilian Oral Research.2018;[Epub] CrossRef
- Adhesive Restoration Performance in Deep Subgingival Margins: Deep Margin Elevation Versus Surgical Crown Lengthening—A Systematic Review
- 4,230 View
- 131 Download
- 33 Crossref
Research Article
-
Retentive strength of different intracanal posts in restorations of anterior primary teeth: an
in vitro study - Mahtab Memarpour, Fereshteh Shafiei, Maryam Abbaszadeh
- Restor Dent Endod 2013;38(4):215-221. Published online November 12, 2013
- DOI: https://doi.org/10.5395/rde.2013.38.4.215
-
Abstract
PDFPubReaderePub
Objectives To determine the retentive strength and failure mode of undercut composite post, glass fiber post and polyethylene fiber post luted with flowable composite resin and resin-cement.
Materials and Methods Coronal parts of 120 primary canine teeth were sectioned and specimens were treated endodontically. The teeth were randomly divided into 6 groups (
n = 20). Prepared root canals received intracanal retainers with a short composite post, undercut composite post, glass fiber post luted with flowable resin or resin-cement, and polyethylene fiber post luted with flowable resin or resin-cement. After crown reconstruction, samples were tested for retentive strength and failure mode. Statistical analysis was done with one-way ANOVA and Tukey tests (p < 0.05).Results There were statistically significant differences between groups (
p = 0.001). Mean bond strength in the undercut group was significantly greater than in the short composite post (p = 0.030), and the glass fiber post (p = 0.001) and the polyethylene fiber post group luted with resin-cement (p = 0.008). However, the differences between the undercut group and the groups with flowable composite as the luting agent were not significant (p = 0.068,p = 0.557). Adhesive failure was more frequent in the fiber post groups.Conclusions Although the composite post with undercutting showed the greatest resistance to dislodgement, fiber posts cemented with flowable composite resin provided acceptable results in terms of retentive strength and fracture mode.
-
Citations
Citations to this article as recorded by- Evaluation of fracture resistance of three types of post utilized in restoration of root canal treated primary anterior teeth (an in-vitro study)
Doaa K. Hassan, Nagwa A. Ghoname, Arafa M. Khatab, Samy M. El Safty, Nahed S. Shoker
Tanta Dental Journal.2025; 22(1): 172. CrossRef - Comparative Evaluation of Compressive Strength and Modes of Failure of Unpolymerized Glass Fiber Post, Polyethylene Fiber Post, and Short Composite Post Used in Endodontically Treated Primary Anterior Teeth: An In Vitro Experimental Study
Gouri R Reddy, Bharath KP, Tejashree Rajanna, Praveen KS Bali, Nagaveni NB, Nivedita Bhovi
Dental Journal of Advance Studies.2025; 13(3): 120. CrossRef - Mechanical Properties and Clinical Success of Intracanal Posts in Primary Maxillary Anterior Teeth: A Systematic Review and Meta-analysis
Yamuna Shanmugam, Aksshaya Raghu, MS Muthu, Selvakumar Haridoss, Kavitha Swaminathan, Krishnapillai Chandrababu Vignesh, Sunil Babu Kotha
International Journal of Clinical Pediatric Dentistry.2024; 16(S3): S293. CrossRef - Comparison of shear bond strength of different types of intracanal posts in restoring extensively damaged primary anterior teeth
Shabnam Asghari Mollabashi, Shima Nourmohamadi, Afrooz Nakhostin
Journal of Dental Research, Dental Clinics, Dental Prospects.2024; 18(2): 95. CrossRef - Effects of glass fibers reinforced and non-reinforced composite resin on fracture behavior of severely destructed primary incisors and restored with post and core system
Rizk El Agamy
The Saudi Dental Journal.2024; 36(3): 451. CrossRef - Evaluation of the Effects of Different Types of Resin Cement Systems on the Push-Out Bond Strength of the Fiber Post to Intracanal Dentin in Anterior Primary Teeth
Ali Nozari, Boshra Rasoolzade, Zahra Jowkar, Seyed Ahmadreza Hamidi, Mohammad Jowkar, Murilo Baena Lopes
International Journal of Dentistry.2023; 2023: 1. CrossRef - Comparison of the Pull-Out Resistance of Grossly Decayed Primary Anterior Teeth Restored With Two Different Intracanal Posts: An In Vitro Study
Ayham Hijaz, Mohamed K Altinawi, Imad Katbeh, Eyad Gergos, Gharawi Alhamzah
Cureus.2023;[Epub] CrossRef - Comparison of fracture resistance of primary incisor teeth restored with glass fiber post and reversed-oriented metal post – an in vitro study
Hamideh Barghi, Samira Sharifi
Dental Research Journal.2023;[Epub] CrossRef - Clinical and radiographic comparative study to evaluate the efficacy of restoring destroyed primary incisors using two different techniques—A pilot study
Seba Ibrahim, Abdul Wahab Nourallah
Clinical and Experimental Dental Research.2020; 6(5): 537. CrossRef - Coronal Microleakage of Teeth Restored with Cast Posts and Cores Cemented with Four Different Luting Agents after Thermocycling
Maryam Mohajerfar, Kaveh Nadizadeh, Tabasom Hooshmand, Elaheh Beyabanaki, Hamid Neshandar Asli, Siamak Sabour
Journal of Prosthodontics.2019;[Epub] CrossRef - Evaluation of the effect of different post materials and adhesive systems on the bonding strength of short‐post technique for primary teeth
Nihal Beldüz Kara, Tunahan Kanyilmaz, Soner Çankaya, Cankat Kara
International Journal of Paediatric Dentistry.2018; 28(2): 239. CrossRef - Effect of ultrasonic tip designs on intraradicular post removal
Anny Carine Barros Aguiar, Daniely Amorim de Meireles, André Augusto Franco Marques, Emílio Carlos Sponchiado Júnior, Angela Delfina Bitencourt Garrido, Lucas da Fonseca Roberti Garcia
Restorative Dentistry & Endodontics.2014; 39(4): 265. CrossRef
- Evaluation of fracture resistance of three types of post utilized in restoration of root canal treated primary anterior teeth (an in-vitro study)
- 2,641 View
- 15 Download
- 12 Crossref
 First
First Prev
Prev

