
Articles
- Page Path
- HOME > Restor Dent Endod > Volume 46(4); 2021 > Article
- Research Article Errors in light-emitting diodes positioning when curing bulk fill and incremental composites: impact on properties after aging
-
Abdulrahman A. Balhaddad1
 , Isadora M. Garcia1, Haifa Maktabi2, Maria Salem Ibrahim1, Qoot Alkhubaizi3, Howard Strassler2, Fabrício M. Collares4, Mary Anne S. Melo1,2
, Isadora M. Garcia1, Haifa Maktabi2, Maria Salem Ibrahim1, Qoot Alkhubaizi3, Howard Strassler2, Fabrício M. Collares4, Mary Anne S. Melo1,2 -
Restor Dent Endod 2021;46(4):e51.
DOI: https://doi.org/10.5395/rde.2021.46.e51
Published online: September 24, 2021
1Ph.D Program Dental Biomedical Sciences, University of Maryland School of Dentistry, Baltimore, MD, USA.
2Division of Operative Dentistry, Department of General Dentistry, University of Maryland School of Dentistry, Baltimore, MD, USA.
3Advanced Education in General Dentistry Division, Department of General Dentistry, University of Maryland School of Dentistry, Baltimore, MD, USA.
4Department of Dental Materials, School of Dentistry, Federal University of Rio Grande do Sul, Porto Alegre, RS, Brazil.
- Correspondence to Mary Anne S. Melo, DDS, MSc, PhD. Associate Professor, Operative Dentistry Division, Department of General Dentistry, University of Maryland School of Dentistry, 650 W Baltimore St, Baltimore, MD 21201, USA. Mmelo@umaryland.edu
• Received: January 11, 2021 • Revised: June 10, 2021 • Accepted: June 15, 2021
Copyright © 2021. The Korean Academy of Conservative Dentistry
This is an Open Access article distributed under the terms of the Creative Commons Attribution Non-Commercial License (https://creativecommons.org/licenses/by-nc/4.0/) which permits unrestricted non-commercial use, distribution, and reproduction in any medium, provided the original work is properly cited.
Abstract
-
Objectives This study aimed to evaluate the effect of improper positioning single-peak and multi-peak lights on color change, microhardness of bottom and top, and surface topography of bulk fill and incremental composites after artificial aging for 1 year.
-
Materials and Methods Bulk fill and incremental composites were cured using multi-peak and single-peak light-emitting diode (LED) following 4 clinical conditions: (1) optimal condition (no angulation or tip displacement), (2) tip-displacement (2 mm), (3) slight tip angulation (α = 20°) and (4) moderate tip angulation (α = 35°). After 1-year of water aging, the specimens were analyzed for color changes (ΔE), Vickers hardness, surface topography (Ra, Rt, and Rv), and scanning electron microscopy.
-
Results For samples cured by single-peak LED, the improper positioning significantly increases the color change compared to the optimal position regardless of the type of composite (p < 0.001). For multi-peak LED, the type of resin composite and the curing condition displayed a significant effect on ΔE (p < 0.001). For both LEDs, the Vickers hardness and bottom/top ratio of Vickers hardness were affected by the type of composite and the curing condition (p < 0.01).
-
Conclusions The bulk fill composite presented greater resistance to wear, higher color stability, and better microhardness than the incremental composite when subjected to improper curing. The multi-peak LED improves curing under improper conditions compared to single-peak LED. Prevention of errors when curing composites requires the attention of all personnel involved in the patient's care once the clinical relevance of the appropriate polymerization reflects on reliable long-term outcomes.
INTRODUCTION
Resin composites are photocured to achieve the required mechanical and physical properties after placement inside the mouth [1]. The photoactivation begins with the energy delivery by light at a specific wavelength to excite the composites' photoinitiators [2]. However, the light diffusion through resin composites has been limited due to fillers' content and the different refractive indexes between the organic blend and the inorganic particles, leading to light-scattering and reduced light penetration [3]. In addition to the control of shrinkage stress, this limitation led to the incremental placement technique for composites restorations [4].
By using novel photoinitiators and unique fillers, bulk fill composites have reached clinical performance similar to 2 the mm-incrementally placed resin composites [5], with additional advantages of fewer voids in material mass as faster and easier placement [6]. Moreover, the addition of selective modulators of photopolymerization and other slight alterations in the monomers polymerization kinetics contribute to the polymerization of bulk fill resin composites' deep cavities [7,8,9].
To efficiently photoactivate both incremental or bulk fill resin composites, the light-emitting diode (LED) should deliver the required amount of radiant exposure energy to the restoration to activate the photoinitiators within the resin matrix and initiate the polymerization reaction [10]. Single-peak LEDs are designed to overlap only the camphorquinone photoinitiator systems (single-peak system) [11]. The narrow spectrum of light-curing units (LCUs) with single-peak LED may restrict the curing efficiency of composite restorations that contain more than 1 photoinitiator system with different peak absorptions [12]. More recently, multi-peak LED LCUs with higher irradiance have been introduced to excite multiple photoinitiator systems besides the standard camphorquinone initiator system present in the composite composition [11].
The effective positioning of the light-curing unit directly over the composites can also affect the restoration's irradiance [13]. The improper curing techniques, such as the tip's angulation or malposition, can reduce the delivered radiant exposure [14,15]. Reduced energy delivery directly compromises curing quality (degree of conversion), indirectly compromises mechanical properties, negatively affects the color stability and facilitates the penetration of cariogenic species and the release of uncured monomers [16,17,18]. In this context, the shade stability and the physical property tested via microhardness are essential factors to be assessed to predict resin composite restorations' clinical behavior.
Research on the long-term impact of improper positioning single-peak and multi-peak light-emitting diodes on curing bulk fill and incremental composites is still limited. Therefore, this study aimed to evaluate the effect of improper positioning single-peak and multi-peak lights on color change, the microhardness of bottom and top, and surface topography of bulk fill and incremental composites after artificial aging for 1 year.
MATERIALS AND METHODS
In this study, 2 LCUs were included; single-peak (Radii-cal; SDI Limited, Victoria, Australia; standard curing mode, radiant emittance output provided of 689 mW/cm2) and multi-peak (Valo grand; Ultradent Products Inc., South Jordan, UT, USA; standard curing mode; radiant emittance output provided of 1,029 mW/cm2). Both LCUs were used to cure incremental (Amelogen Plus) and bulk fill (Filtek Bulk Fill Posterior Restorative) resin composites (Table 1).
Table 1
Description of the commercial products evaluated in this study at different conditions of light-curing
Four curing conditions were performed, as shown in Figure 1. The first scenario represents the optimal curing technique, while the other 3 represent the most commonly underperformed curing conditions in clinical practice. The tip displacement is represented by distancing the tip 2 mm from the surface of the resin composites. Another illustrated condition is a slight angulation represented by 20° angulation between the tip of LCU and resin composite surface. The other scenario is when the tip was positioned with a moderate angulation of 35° from the resin composite's surface. All the conditions were standardized using 3-dimensional printed molds.
Figure 1
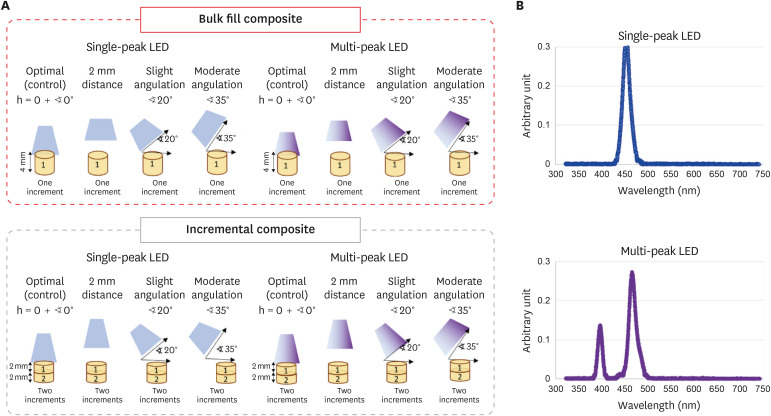
Schematic drawing showing the design of the study. Bulk fill and incremental composites were cured with single-peak and multi-peak LCUs following different conditions (optimal, 2 mm distance, slight angulation, and moderate angulation). The samples were prepared using customized 3D molds to standardization of the distance and angulations. The design of each mold was elaborated to allow the LCU tip to maintain the distance or the specific angulation (20° or 35°) in relation to the composite surface. The composites were aged for 1 year, and then the color stability, Vickers hardness, bottom/top ratio of Vickers hardness, and surface topography parameters were investigated.
LED, light-emitting diode; LCU, light-curing unit.
The resin composite samples were made using a 3D mold (polylactic acid filament, melted Extrusion Modeling, 3D H800 Afinia printer) having 7 mm diameter and 2 mm thickness for the incremental resin composites and 4 mm thickness for the bulk fill cured with either single-peak or multi-peak LCUs for 20 and 40 seconds, respectively, following the manufacturers' recommendation. The samples were prepared using customized 3D molds to standardization of the distance and angulations. Each mold's design was elaborated to allow the LCU tip to maintain the distance or the specific angulation (20° or 35°) in relation to the composite surface. For that, we had 4 different molds for each simulated curing scenario. The radiance emittance of the LCUs was validated via a calibrated radiometer system (MARC; Blue- Light Analytics Inc., Halifax, NS, Canada) before the curing procedure. Resin composite specimens were stored in distilled water for 1 year in a dark environment at 37°C in an incubator.
A dental spectrophotometer (VITA Easyshade; VITA Zahnfabrik, Bad Säckingen, Germany) was used to obtain CIELAB color coordinates (ΔE) before water aging (baseline) and after 1 year of water aging. Before each specimen measurement (n = 3), the probe tip of the VITA Easyshade was placed over the calibration port aperture to calibrate the device. The probe tip was held at 90° on the top of each specimen, and the shade was recorded. The average of 3 different readings was used to determine the most accurate measurement of each specimen. The CIELab system is provided by the Easyshade spectrophotometric device to identify the difference in color between baseline and after 1 year of aging following the equation [19]:
Where L* is the measurement of the object's lightness, a* referred to the measure of red (positive a*) or green (negative a*), and b* referred to the measure of yellow (positive b*) or blue (negative b*). The difference of color between the baseline and the resulting material after 1 year of aging was calculated using ΔE values.
After curing the specimens for 20 seconds and the 1-year aging, the Vickers hardness values were obtained from the top and bottom of the composite specimens (n = 3) using a force of 1.961 for 20 seconds (HMV-G; Shimadzu Corp., Tokyo, Japan) [20]. The indentations were kept randomly on the composites' surface with 100 μm of the distance between each indentation. The average of 5 different readings was calculated. Data were obtained and plotted as hardness values. The bottom/top ratio was then determined using the following formula: hardness ratio = Vickers hardness of bottom surface/Vickers hardness of top surface [21].
The bottom of each sample's surface topography changes was recorded following each curing condition and after the 1 year of water aging via a surface roughness measurement instrument (Surftest SJ-310; Mitutoyo America, Aurora, IL, USA). A stylus tip of 5 μm was used to transverse each sample at a constant speed of 0.5 mm/s, a force of 4 mN, a 0.25-mm cutoff value, and a 1.5-mm tracing length [22]. Then, the following parameters were measured: i) average surface roughness (Ra) to measure the values of the profile deviations from the mean line of the roughness profile, ii) maximum peak height (Rp) to measure the highest peak, iii) maximum valley depth (Rv) to measure the deepest valley, and iv) maximum high of the profile (Rt) to measure the difference between the maximum peak height and the maximum valley depth and detect significant discrepancy.
After the 1-year water aging, representatives of the bottom surface of the optimal curing and moderate angulation conditions were prepared for a qualitative analysis of their surface using scanning electron microscopy (SEM) (Quanta 200; FEI, Hillsboro, OR, USA). The specimens were coated with gold/palladium via sputtering and examined using a magnification of 10,000× at an accelerating voltage of 25 kV.
Shapiro-Wilk test was used to assess the data normality and distribution. Two-way analysis of variance (ANOVA) and Tukey's post hoc test were used to analyze the effect of type of resin composite and the curing condition on color change (determined by ΔE values), Vickers hardness, top/bottom ratio of Vickers hardness, and surface topography parameters. All tests were conducted using the statistical software package Sigma Plot 12.0 (SYSTAT, Chicago, IL, USA), and the statistical significance was set at p < 0.05.
RESULTS
The 2-way ANOVA revealed that when the single-peak LCU was used, the curing condition had a significant effect on the color change after 1 year of aging (p < 0.001), while the type of resin composite, bulk fill or incremental, did not show any significant effect (p = 0.584). No interaction was found between the 2 factors (p = 0.9). With the single-peak LCU, the increased distance or angulation of the LCU tip significantly increased the ΔE value compared to the optimal curing condition (p < 0.05) (Figure 2A). The higher ΔE values were observed with the moderate angulation condition. No significant difference was found between bulk fill and incremental resin composite when the curing condition was similar (p > 0.05).
Figure 2
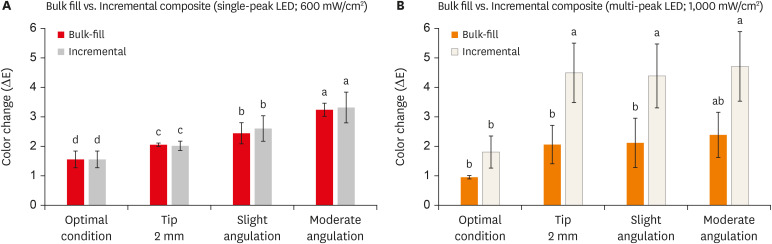
The color change is expressed by ΔE of the bulk fill and incremental composites cured using single-peak (A) and multi-peak (B) following different curing conditions. Values indicated by different letters are statistically different from each other (p < 0.05).
LED, light-emitting diode.
When the samples cured with the multi-peak LCU were investigated, both types of resin composite and curing condition displayed significant effect concerning the color change after 1 year of aging (p < 0.001), and a significant interaction was observed too (p = 0.002). In the incremental resin composite, underperformed curing conditions were associated with higher ΔE values compared to the optimal condition (p < 0.05) (Figure 2B). However, underperformed curing conditions were less pronounced when bulk fill samples were observed as no statistically significant difference was observed between all the curing conditions. Considering the type of resin composite, bulk fill significantly demonstrated lower ΔE compared to incremental resin composite in all curing conditions (p < 0.05) except when investigating the optimal curing condition (Figure 2A).
Both resin composites and the curing condition significantly affected the microhardness values of resin composite samples' top and bottom surface cured with the single-peak LCU (p < 0.001). However, a significant interaction was observed only with the bottom surface (p = 0.002). Incremental resin composite Vickers hardness values were significantly lower compared to bulk fill specimens (p < 0.05) concerning both the top and bottom surface (Figure 3). In addition, moderated angulation curing conditions revealed the lowest value in both types of resin composite. The same observation was reported considering the multi-peak LCU. The incremental resin composites significantly demonstrated lower values than bulk fill in both top and bottom surfaces, with the lower values associated with moderate angulation conditions (Figure 4).
Figure 3
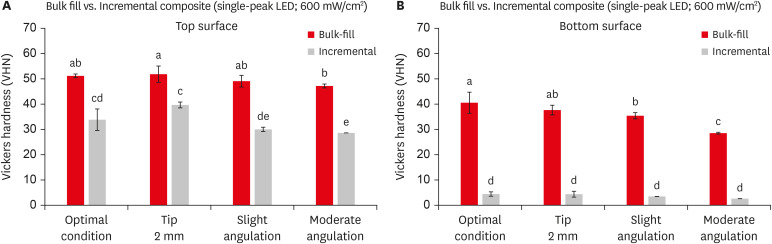
The vickers hardness values of the top (A) and bottom (B) surfaces of bulk fill and incremental composites cured using single-peak light-curing unit following different curing conditions. Values indicated by different letters are statistically different from each other (p < 0.05).
LED, light-emitting diode.
Figure 4
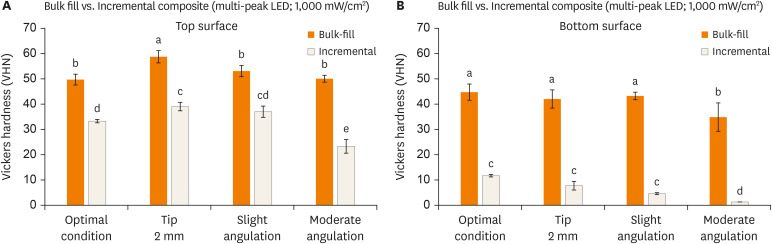
The Vickers hardness values of the top (A) and bottom (B) surfaces of bulk fill and incremental composites cured using multi-peak light-curing unit following different curing conditions. Values indicated by different letters are statistically different from each other (p < 0.05).
LED, light-emitting diode.
For both LCUs used, the 2-way ANOVA showed that the underperformed conditions (angulation or displacement) negatively affected the bottom/top ratio of Vickers hardness (p < 0.05), without interaction between the type of composite and underperformed condition (p > 0.05). Using single-peak, bulk fill samples cured with moderate angulation condition (60.01 ± 0.64) significantly reported a lower bottom/top ratio compared to the other condition (p < 0.05) (Figure 5A). Incremental resin composites did not show a significant difference between the curing conditions (p >0.05). However, all the incremental resin composite samples revealed a lower bottom/top ratio than bulk fill despite the curing condition (p < 0.001).
Figure 5
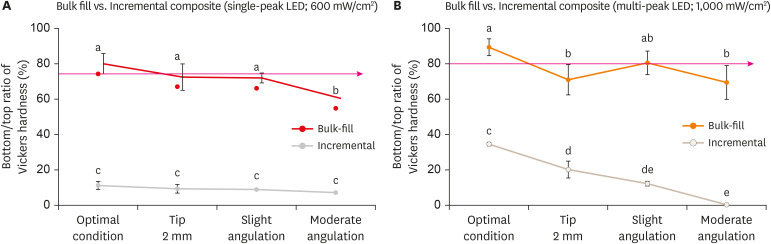
The bottom/top ratio of Vickers hardness of bulk fill and incremental composite cured using single-peak (A) and multi-peak (B) following different curing conditions. Values indicated by different letters are statistically different from each other (p < 0.05).
LED, light-emitting diode.
For the bulk fill resin composites cured with multi-peak, 2 mm distance (71.32 ± 8.36), and moderate angulation (69.26 ± 9.33) conditions revealed a lower bottom/top ratio of Vickers hardness compared to the other conditions (p < 0.001) (Figure 5B). While in incremental resin composites, underperformed curing conditions were significantly lower in their bottom/top ratio of Vickers hardness compared to the optimal curing condition (34.37 ± 0.85), with the lowest value observed on the moderate angulation condition (p < 0.001). All the incremental samples showed a decreased bottom/top ratio of Vickers hardness than bulk fill despite the curing condition (p < 0.001).
Table 2 shows the Ra, Rq, Rv, and Rt of bottom surfaces of both bulk fill and incremental resin composites cured with single-peak LCU. For the bulk fill resin composite, moderate angulation condition significantly reported higher Ra, Rq, and Rt values than the optimal condition. While in the slight angulation curing condition, only the Ra value was significantly higher than the optimal curing condition. No significant difference was observed between the 2 mm distance and optimal curing conditions.
Table 2
Results of surface roughness after photoactivation with LCU600 (Radii-Cal)
Ra, Rq, Rv, and Rt of the bottom surface of bulk fill and incremental resin composites following different curing conditions and 1-year of aging (mean ± SD).
Ra, average surface roughness; Rp, maximum peak height; Rv, maximum valley depth; Rt, average distance between the highest peak and lowest valley; SD, standard deviation.
a,bValues indicated by different letters are statistically different from each other (p < 0.05) concerning the different curing conditions in either bulk fill or incremental resin composites. *Asterisks indicate a significant difference (p < 0.05) comparing bulk fill and incremental resin composite in the same curing condition.
Bulk fill was significantly associated with lower values in all parameters than incremental resin composites when the optimal curing condition was considered. No significant difference was observed between the 2 resin composite types when the 2 mm distance and slight angulation conditions were considered. Rq, Rv, and Rt values were significantly lower in incremental resin composite than bulk fill in the moderate angulation condition.
Table 3 shows the parameters' values related to bulk fill and incremental resin composite curing with multi-peak. In the bulk fill samples, the Ra values were significantly higher in the 2 mm distance and slight angulation condition than the optimal and moderate angulation conditions. Considering Rq, Rv, and Rt values, the optimal curing condition was significantly lower than the other curing conditions. In incremental resin composites, the optimal curing condition was comparable to the underperformed curing conditions concerning all the parameters (p > 0.05).
Table 3
Results of surface roughness after photoactivation with LCU1000 (Valo grand)
Ra, Rq, Rv, and Rt of the bottom surface of bulk fill and incremental resin composites following different curing conditions and 1-year of aging (mean ± SD). All resin composite specimens were cured with LCU1000 (Valo grand), which provides 1,029 mW/cm2 power output.
Ra, average surface roughness; Rp, maximum peak height; Rv, maximum valley depth; Rt, average distance between the highest peak and lowest valley; SD, standard deviation.
a,bValues indicated by different letters are statistically different from each other (p < 0.05) concerning the different curing conditions in either bulk fill or incremental resin composites. *Asterisks indicate a significant difference (p < 0.05) comparing bulk fill and incremental resin composite in the same curing condition.
In the moderate curing condition, incremental resin composite significantly demonstrated a lower Rt value than bulk fill, with no significant difference observed in the other parameters.
The bottom surfaces' SEM images following the optimal and moderate curing conditions with the 2 materials cured with single-peak and multi-peak are shown in Figure 6. Overall, bulk fill bottom surfaces were associated with fewer topography changes compared to incremental resin composites. Figure 6 showed that bulk fill cured with single-peak has fewer surface changes than incremental composite despite the curing condition. The curing conditions did not seem to affect the surface of the sample in both composites. The images of bulk fill had fewer surface alterations than incremental composites. Both bulk fill specimens cured in optimal or moderate angulation conditions, using multi-peak LCU, were comparable. However, the surface alterations are more pronounced in incremental composite cured using moderate angulation than the same type of composite light-cured optimally.
Figure 6
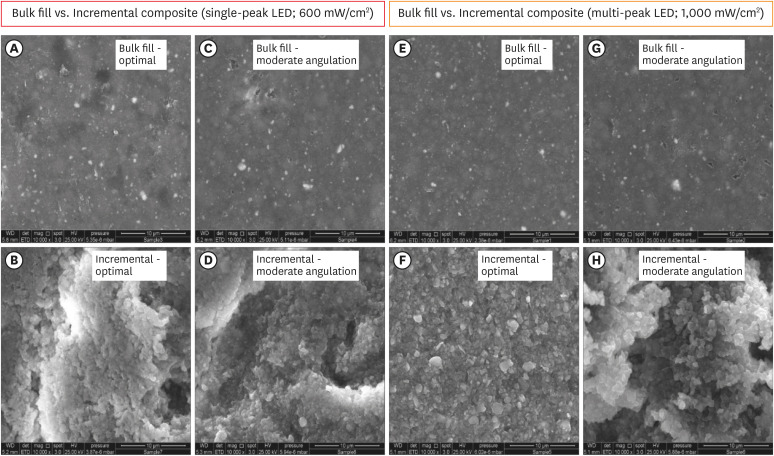
Scanning electron microscopy images for bulk fill and incremental composites cured with single-peak (A-D) and multi-peak (E-H) light-curing unit following the optimal and moderate angulation conditions. The incremental composite was associated with excessive topography changes and alterations compared to bulk fill composites.
LED, light-emitting diode.
DISCUSSION
This study's resulting outcomes illustrated the impact of improper positioning after 1 year of water aging. Bulk fill composites had better color stability, higher microhardness, bottom/top ratio of Vickers hardness, and fewer surface alterations than incremental composites. The study also demonstrated that poor outcomes were associated with single-peak LCU at 600 mW/cm2 and improper positioning during curing. Composites restorations should receive adequate radiant exposure to appropriately polymerize and obtain the optimum mechanical and physical properties [13]. Underperformed curing techniques may negatively affect the quality of the placed restorations. The extent of damages caused by the improper curing positioning was less pronounced when multi-peak LCU was used.
Materials with low shade stability are susceptible to color change with time, which may compromise the esthetic appearance of restorations [23]. Usually, composite restorations are placed with a similar shade to the adjacent teeth. The specification of critical ΔE depends on several factors related to the object, observer, and the surrounding light. The ΔE value of 2.6 was pointed in several studies as a perceptible value distinguished by the human eyes [24,25]. In this study, moderate angulation curing conditions reported values higher than 2.6 in bulk fill and incremental composites cured by single-peak LCU (Figure 2A). As well, slight angulation curing conditions in incremental composite produced a ΔE value of 2.61 ± 0.44. While in multi-peak LCU, this critical threshold was exceeded only when the incremental composites were cured following underperformed curing conditions (Figure 2B). Concerning the composite type, bulk fill's color stability was comparable to incremental composites when single-peak was used. However, when the samples were cured using multi-peak, bulk fill demonstrated better color stability than incremental composites, suggesting that depth of cure and the quality of curing were more effective for this class of material. We are aware that bulk fill composites use different mechanisms to increase the depth of cure. While some composites have increased translucency to create deeper light penetration, others incorporate additional photoinitiators. The related outcome can be associated with the irradiance output of the multi-peak LCU, once the main photoinitiator of the used composites is camphorquinone, which has a peak activity around 470 nm.
The light source's effect and the working distance on the composite polymerization were demonstrated in previous studies using different working distances, and different LCUs resulted in different polymerization patterns [15,26]. Therefore, besides improving the composite composition quality, LCUs and operator techniques need to be deeply investigated as critical variables to assure adequate polymerization. Measuring the material's hardness is 1 of the most commonly used approaches to estimate polymerization quality. Mainly high microhardness values are correlated with adequate polymerization [27]. Low ratios between Vickers hardness's top and bottom surface mean that the restoration's bottom surface located far from the LCU tip during photoactivation did not receive adequate energy to achieve optimum polymerization [28]. Increasing the thickness of resin composite during placement more than manufacturer recommendation may compromise the bottom/top ratio of Vickers hardness of such restoration.
In the present study, we analyzed Vickers hardness's bottom/top ratio, similar to the literature's depth of cure procedures. However, we evaluated the effect of the long-term storage of the specimens concerning this outcome. In the traditional depth of cure analysis, the samples would be tested 24–48 hours after light-curing and storage in water. In this study, the specimens were stored for 1 year and then analyzed via Vickers hardness. Despite these differences, it is interesting to highlight that depths of cure values lower than 80 could be associated with insufficient polymerization concerning the bottom surface of the restorations. This result may facilitate the degradation of the placed resin composite, compromise the mechanical properties, and enhance the invasion's cariogenic species [6,29].
The bulk fill composites are cured optimally with single-peak or multi-peak LCUs. On the other hand, we found that even if the incremental composite was adequately cured, Vickers hardness's bottom/top ratio was very low using single-peak or multi-peak LCUs. All the underperformed curing conditions compromised Vickers hardness's bottom/top ratio except for the bulk fill composites cured with 2 mm distance using multi-peak LCU. The lowest value was observed when the light tip was angulated moderately. This outcome is a highly concerned clinical issue that can be seen more specifically in deep proximal cavities, where placing the light-tip close to the restoration is complex, and the bottom surface can be exposed directly to the oral environment. As a result, dental providers may need to consider doubling the curing time and curing the restoration from the buccal and lingual sides to assure adequate and uniform polymerization through the entire restoration.
Composite restorations with significant surface roughness and topography changes are at high risk for plaque accumulation and biofilm formation [30]. Bacterial species can adhere easily to the irregularities found over the placed restoration or at the tooth-restoration interface, facilitating restoration degradation and the onset of secondary caries [31]. The average surface roughness of 0.2 μm has been defined as a critical threshold as surface roughness values higher than this threshold are positively associated with restoration failure due to bacterial-induced degradation and secondary caries [22]. In the present study, bulk fill composites cured following underperformed curing conditions were associated with higher average surface roughness values at the bottom surface compared to the optimal condition. However, incremental composites reported greater detrimental outcomes when poorly cured, which could be observed by the pronounced topography changes, as shown in Figure 6. In both bulk fill and incremental composites, all the underperformed curing conditions increased the extent of surface changes expressed by Rq, Rv, and Rt value, emphasizing the negative consequences of improper curing techniques.
As shown in Tables 2, 3, and Figure 6, the bulk fill composite's bottom surface was associated with fewer surface alterations than incremental composite despite the curing condition. These observations could be more significant when the composite in deep proximal restoration. When the radiant exposure delivery to the bottom area of the restorations is compromised, the increased topography changes over time may allow the microorganism to attach and colonize, causing another lesion around the gingival margin of the restoration.
It is a limitation of this study to have analyzed only 2 commercial materials. The readers must be aware that over-generalizations may be inappropriate since both material groups (bulk fill and incremental resin composites) are highly heterogeneous. Maybe generalizations do not do justice to the wide variety of materials and their different properties. For instance, low-viscosity and high-viscosity materials may behave differently in both groups (bulk fill and incremental). Future studies may investigate more commercially available bulk fill and incremental composites. However, this study observed that improper curing techniques were related to low color stability, microhardness, bottom/top ratio of Vickers hardness, and increased topography changes.
CONCLUSIONS
After 1 year of aging, this study found that bulk fill composite showed better color stability, higher microhardness, bottom/top ratio of Vickers hardness, and fewer surface alterations than incremental composites. In addition, the multi-peak LED improves curing under the unfavorable conditions of distancing and inclination compared to single-peak LED. However, preventing errors when curing composites requires the attention of all personnel involved in the patient's care once the clinical relevance of the appropriate polymerization reflects on reliable long-term outcomes.
ACKNOWLEDGEMENTS
AAB and MSI acknowledge the scholarship during their Ph.D. studies from the Imam AbdulRahman bin Faisal University, Dammam, Saudi Arabia, and the Saudi Arabia Cultural Mission. IMG acknowledge the scholarship during their Ph.D. studies from the Coordenação de Aperfeiçoamento de Pessoal de Nível Superior - Brasil (CAPES) - Finance Code 001 – scholarship.
-
Funding: This study was supported by a departmental seed grant from the University of Maryland School of Dentistry (MM).
-
Conflict of Interest: No potential conflict of interest relevant to this article was reported.
-
Author Contributions:
Conceptualization: Melo MAS, Strassler H.
Funding acquisition: Melo MAS.
Investigation: Balhaddad AA, Garcia IM, Maktabi H, Ibrahim MS, Alkhubaizi Q.
Project administration: Melo MAS, Strassler H.
Resources: Melo MAS.
Supervision: Melo MAS, Strassler H, Collares FM.
Validation: Melo MAS.
Visualization: Balhaddad AA, Garcia IM.
Writing - original draft: Balhaddad AA, Garcia IM.
Writing - review & editing: Melo MAS, Strassler H, Collares FM.
- 1. AlShaafi MM. Factors affecting polymerization of resin-based composites: a literature review. Saudi Dent J 2017;29:48-58.ArticlePubMedPMC
- 2. Price RB, Ferracane JL, Shortall AC. Light-curing units: a review of what we need to know. J Dent Res 2015;94:1179-1186.ArticlePubMedPDF
- 3. de Oliveira DC, de Menezes LR, Gatti A, Correr Sobrinho L, Ferracane JL, Sinhoreti MA. Effect of nanofiller loading on cure efficiency and potential color change of model composites. J Esthet Restor Dent 2016;28:171-177.ArticlePubMedPDF
- 4. Alrahlah A, Silikas N, Watts DC. Post-cure depth of cure of bulk fill dental resin-composites. Dent Mater 2014;30:149-154.ArticlePubMed
- 5. Gan JK, Yap AU, Cheong JW, Arista N, Tan C. Bulk-fill composites: effectiveness of cure with poly- and monowave curing lights and modes. Oper Dent 2018;43:136-143.ArticlePubMedPDF
- 6. Aggarwal N, Jain A, Gupta H, Abrol A, Singh C, Rapgay T. The comparative evaluation of depth of cure of bulk-fill composites - an in vitro study. J Conserv Dent 2019;22:371-375.ArticlePubMedPMC
- 7. Van Ende A, De Munck J, Van Landuyt KL, Poitevin A, Peumans M, Van Meerbeek B. Bulk-filling of high C-factor posterior cavities: effect on adhesion to cavity-bottom dentin. Dent Mater 2013;29:269-277.ArticlePubMed
- 8. Flury S, Hayoz S, Peutzfeldt A, Hüsler J, Lussi A. Depth of cure of resin composites: is the ISO 4049 method suitable for bulk fill materials? Dent Mater 2012;28:521-528.ArticlePubMed
- 9. Azzopardi N, Moharamzadeh K, Wood DJ, Martin N, van Noort R. Effect of resin matrix composition on the translucency of experimental dental composite resins. Dent Mater 2009;25:1564-1568.ArticlePubMed
- 10. Price RB, Ferracane JL, Hickel R, Sullivan B. The light-curing unit: an essential piece of dental equipment. Int Dent J 2020;70:407-417.ArticlePubMedPMCPDF
- 11. Derchi G, Vano M, Ceseracciu L, Diaspro A, Salerno M. Stiffness effect of using polywave or monowave LED units for photo-curing different bulk fill composites. Dent Mater J 2018;37:709-716.ArticlePubMed
- 12. Menees TS, Lin CP, Kojic DD, Burgess JO, Lawson NC. Depth of cure of bulk fill composites with monowave and polywave curing lights. Am J Dent 2015;28:357-361.PubMedPMC
- 13. Maktabi H, Balhaddad AA, Alkhubaizi Q, Strassler H, Melo MAS. Factors influencing success of radiant exposure in light-curing posterior dental composite in the clinical setting. Am J Dent 2018;31:320-328.PubMed
- 14. Konerding KL, Heyder M, Kranz S, Guellmar A, Voelpel A, Watts DC, Jandt KD, Sigusch BW. Study of energy transfer by different light curing units into a class III restoration as a function of tilt angle and distance, using a MARC Patient Simulator (PS). Dent Mater 2016;32:676-686.ArticlePubMed
- 15. Al-Zain AO, Eckert GJ, Lukic H, Megremis S, Platt JA. Polymerization pattern characterization within a resin-based composite cured using different curing units at two distances. Clin Oral Investig 2019;23:3995-4010.ArticlePubMedPDF
- 16. Eshmawi YT, Al-Zain AO, Eckert GJ, Platt JA. Variation in composite degree of conversion and microflexural strength for different curing lights and surface locations. J Am Dent Assoc 2018;149:893-902.ArticlePubMed
- 17. Janda R, Roulet JF, Latta M, Steffin G, Rüttermann S. Color stability of resin-based filling materials after aging when cured with plasma or halogen light. Eur J Oral Sci 2005;113:251-257.ArticlePubMed
- 18. Maktabi H, Ibrahim M, Alkhubaizi Q, Weir M, Xu H, Strassler H, Fugolin APP, Pfeifer CS, Melo MAS. Underperforming light curing procedures trigger detrimental irradiance-dependent biofilm response on incrementally placed dental composites. J Dent 2019;88:103110.ArticlePubMed
- 19. Meireles SS, Demarco FF, dos Santos IS, Dumith SC, Bona AD. Validation and reliability of visual assessment with a shade guide for tooth-color classification. Oper Dent 2008;33:121-126.ArticlePubMedPDF
- 20. Atai M, Yassini E, Amini M, Watts DC. The effect of a leucite-containing ceramic filler on the abrasive wear of dental composites. Dent Mater 2007;23:1181-1187.ArticlePubMed
- 21. Poggio C, Lombardini M, Gaviati S, Chiesa M. Evaluation of Vickers hardness and depth of cure of six composite resins photo-activated with different polymerization modes. J Conserv Dent 2012;15:237-241.ArticlePubMedPMC
- 22. Balhaddad AA, Ibrahim MS, Weir MD, Xu HHK, Melo MAS. Concentration dependence of quaternary ammonium monomer on the design of high-performance bioactive composite for root caries restorations. Dent Mater 2020;36:e266-e278.ArticlePubMed
- 23. Sabatini C. Color stability behavior of methacrylate-based resin composites polymerized with light-emitting diodes and quartz-tungsten-halogen. Oper Dent 2015;40:271-281.ArticlePubMedPDF
- 24. Diamantopoulou S, Papazoglou E, Margaritis V, Lynch CD, Kakaboura A. Change of optical properties of contemporary resin composites after one week and one month water ageing. J Dent 2013;41(Supplement 5):e62-e69.Article
- 25. Bendary IM, Garcia IM, Collares FM, Takimi A, Samuel SMW, Leitune VCB. Wollastonite as filler of an experimental dental adhesive. J Dent 2020;102:103472.PubMed
- 26. Al-Zain AO, Eckert GJ, Platt JA. The influence of distance on radiant exposure and degree of conversion using different light-emitting-diode curing units. Oper Dent 2019;44:E133-E144.ArticlePubMedPDF
- 27. Ciccone-Nogueira JC, Borsatto MC, de Souza-Zaron WC, Ramos RP, Palma-Dibb RG. Microhardness of composite resins at different depths varying the post-irradiation time. J Appl Oral Sci 2007;15:305-309.ArticlePubMedPMC
- 28. de Camargo EJ, Moreschi E, Baseggio W, Cury JA, Pascotto RC. Composite depth of cure using four polymerization techniques. J Appl Oral Sci 2009;17:446-450.ArticlePubMedPMC
- 29. Moore BK, Platt JA, Borges G, Chu TM, Katsilieri I. Depth of cure of dental resin composites: ISO 4049 depth and microhardness of types of materials and shades. Oper Dent 2008;33:408-412.ArticlePubMedPDF
- 30. Mitwalli H, Alsahafi R, Balhaddad AA, Weir MD, Xu HHK, Melo MAS. Emerging contact-killing antibacterial strategies for developing anti-biofilm dental polymeric restorative materials. Bioengineering (Basel) 2020;7:83.ArticlePubMedPMC
- 31. Tantanuch S, Kukiattrakoon B, Peerasukprasert T, Chanmanee N, Chaisomboonphun P, Rodklai A. Surface roughness and erosion of nanohybrid and nanofilled resin composites after immersion in red and white wine. J Conserv Dent 2016;19:51-55.ArticlePubMedPMC
REFERENCES
Tables & Figures
REFERENCES
Citations
Citations to this article as recorded by 
- A clinical survey of the output intensity of 50 light-curing units in dental clinics across Davangere and Mangalore region using a spectrometer system
Elizbeth Christy Jose, Sakshi Jha, Prema Shantagouda Biradar, J Arun, TN Nandini, Thushara Mohanan
International Journal of Oral Health Sciences.2025; 15(1): 41. CrossRef - The demineralization resistance and mechanical assessments of different bioactive restorative materials for primary and permanent teeth: an in vitro study
Maria Salem Ibrahim, Fahad Rakad Aldhafeeri, Abdullah Sami Banaemah, Mana S. Alhaider, Yousif A. Al-Dulaijan, Abdulrahman A. Balhaddad
BDJ Open.2024;[Epub] CrossRef - Inorganic Compounds as Remineralizing Fillers in Dental Restorative Materials: Narrative Review
Leena Ibraheem Bin-Jardan, Dalal Ibrahim Almadani, Leen Saleh Almutairi, Hadi A. Almoabid, Mohammed A. Alessa, Khalid S. Almulhim, Rasha N. AlSheikh, Yousif A. Al-Dulaijan, Maria S. Ibrahim, Afnan O. Al-Zain, Abdulrahman A. Balhaddad
International Journal of Molecular Sciences.2023; 24(9): 8295. CrossRef
 ePub Link
ePub Link Cite
CiteErrors in light-emitting diodes positioning when curing bulk fill and incremental composites: impact on properties after aging

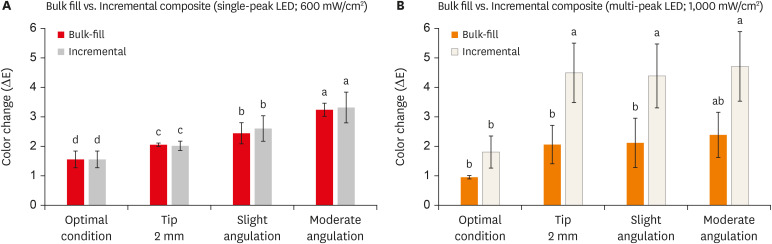
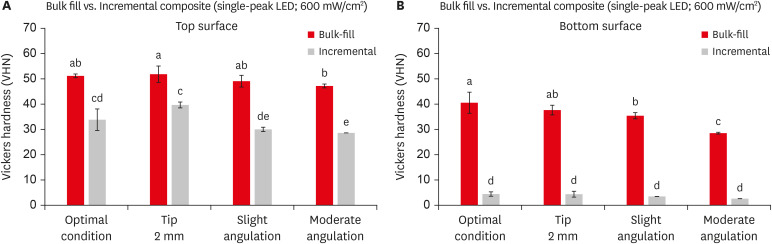
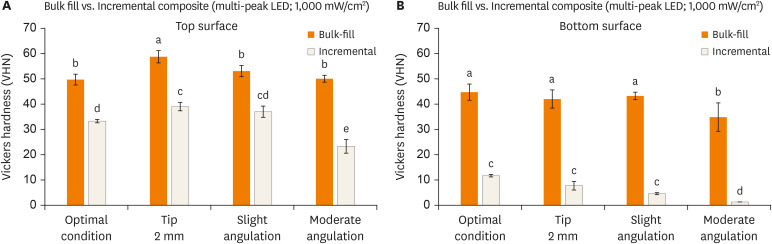
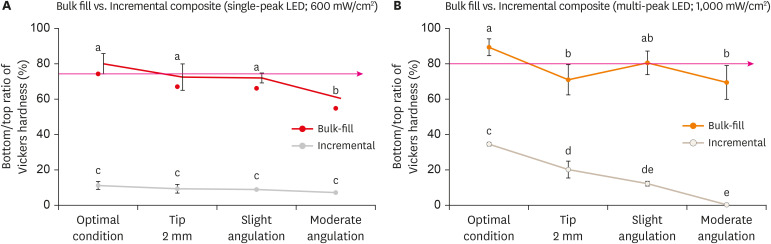
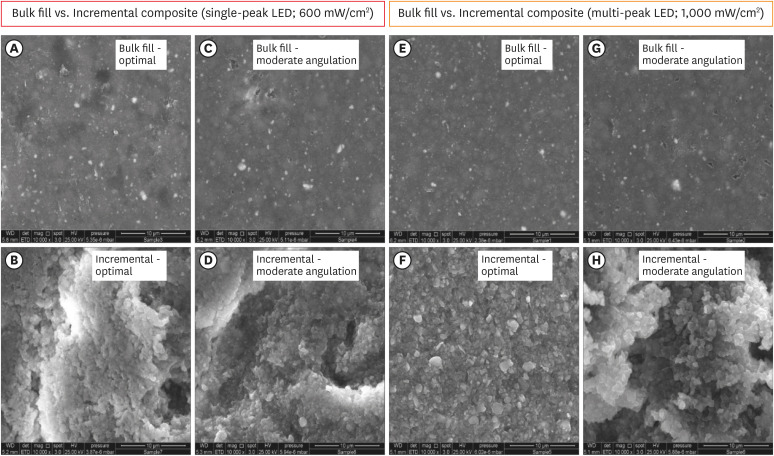
Figure 1 Schematic drawing showing the design of the study. Bulk fill and incremental composites were cured with single-peak and multi-peak LCUs following different conditions (optimal, 2 mm distance, slight angulation, and moderate angulation). The samples were prepared using customized 3D molds to standardization of the distance and angulations. The design of each mold was elaborated to allow the LCU tip to maintain the distance or the specific angulation (20° or 35°) in relation to the composite surface. The composites were aged for 1 year, and then the color stability, Vickers hardness, bottom/top ratio of Vickers hardness, and surface topography parameters were investigated.LED, light-emitting diode; LCU, light-curing unit.
Figure 2 The color change is expressed by ΔE of the bulk fill and incremental composites cured using single-peak (A) and multi-peak (B) following different curing conditions. Values indicated by different letters are statistically different from each other (p < 0.05).LED, light-emitting diode.
Figure 3 The vickers hardness values of the top (A) and bottom (B) surfaces of bulk fill and incremental composites cured using single-peak light-curing unit following different curing conditions. Values indicated by different letters are statistically different from each other (p < 0.05).LED, light-emitting diode.
Figure 4 The Vickers hardness values of the top (A) and bottom (B) surfaces of bulk fill and incremental composites cured using multi-peak light-curing unit following different curing conditions. Values indicated by different letters are statistically different from each other (p < 0.05).LED, light-emitting diode.
Figure 5 The bottom/top ratio of Vickers hardness of bulk fill and incremental composite cured using single-peak (A) and multi-peak (B) following different curing conditions. Values indicated by different letters are statistically different from each other (p < 0.05).LED, light-emitting diode.
Figure 6 Scanning electron microscopy images for bulk fill and incremental composites cured with single-peak (A-D) and multi-peak (E-H) light-curing unit following the optimal and moderate angulation conditions. The incremental composite was associated with excessive topography changes and alterations compared to bulk fill composites.LED, light-emitting diode.
Figure 1
Figure 2
Figure 3
Figure 4
Figure 5
Figure 6
Errors in light-emitting diodes positioning when curing bulk fill and incremental composites: impact on properties after aging
Description of the commercial products evaluated in this study at different conditions of light-curing
| Type of resin composite | Product | Manufacture | Composition | Shade |
|---|---|---|---|---|
| Incremental | Amelogen Plus | Ultradent Products Inc., South Jordan, UT, USA | Bisphenol A-Glycidyl Methacrylate (Bis-GMA, 60 wt.%), triethylene glycol dimethacrylate (TEGMA, 40 wt.%), butylated hydroxytoluene (BHT, 1 wt.%), and barium aluminosilicate glass powder (35 wt.%). | A2 |
| Bulk fill | Filtek Bulk Fill Posterior Restorative | 3M ESPE, St. Paul, MN, USA | Aromatic dimethacrylate, urethane dimethacrylate, 1,12-dodecanediol dimethacrylate, silica, zirconia, zirconia/silica cluster, and ytterbium trifluoride filler particles (76.5 wt.% or 58.4 vol.%). | A2 |
Results of surface roughness after photoactivation with LCU600 (Radii-Cal)
| Curing Condition | Ra (µm) | Rq (µm) | Rv (µm) | Rt (µm) | ||||
|---|---|---|---|---|---|---|---|---|
| Bulk-Fill | Incremental | Bulk-Fill | Incremental | Bulk-Fill | Incremental | Bulk-Fill | Incremental | |
| Optimal Condition | 0.17 ± 0.04a | 0.19 ± 0.20a* | 0.22 ± 0.06a | 0.89 ± 0.12a* | 0.73 ± 0.25a | 0.66 ± 0.21a* | 1.77 ± 0.45a | 1.47 ± 0.55a* |
| 2 mm | 0.32 ± 0.07ab | 0.35 ± 0.11b | 0.45 ± 0.08ab | 0.40 ± 0.17b | 1.03 ± 0.18a | 0.59 ± 0.19b | 2.98 ± 0.33ab | 2.48 ± 0.97b |
| 20° (Slight Angulation) | 0.41 ± 0.14b | 0.51 ± 0.10b | 0.52 ± 0.16ab | 0.63 ± 0.12b | 1.28 ± 0.34a | 1.08 ± 0.23ab | 3.29 ± 0.10ab | 3.57 ± 0.93b |
| 35° (Moderate Angulation) | 0.53 ± 0.20b | 0.33 ± 0.08b | 0.65 ± 0.24b | 0.37 ± 0.12b* | 1.24 ± 0.35a | 0.73 ± 0.30b* | 4.22 ± 1.22b | 2.39 ± 0.66b* |
Ra, Rq, Rv, and Rt of the bottom surface of bulk fill and incremental resin composites following different curing conditions and 1-year of aging (mean ± SD).
Ra, average surface roughness; Rp, maximum peak height; Rv, maximum valley depth; Rt, average distance between the highest peak and lowest valley; SD, standard deviation.
a,bValues indicated by different letters are statistically different from each other (
Results of surface roughness after photoactivation with LCU1000 (Valo grand)
| Curing condition | Ra (µm) | Rq (µm) | Rv (µm) | Rt (µm) | ||||
|---|---|---|---|---|---|---|---|---|
| Bulk fill | Incremental | Bulk fill | Incremental | Bulk fill | Incremental | Bulk fill | Incremental | |
| Optimal condition | 0.28 ± 0.01a | 0.47 ± 0.03ab | 0.35 ± 0.01a | 0.59 ± 0.05a | 0.78 ± 0.18a | 1.14 ± 0.11ab | 1.96 ± 0.22a | 3.50 ± 0.61ab* |
| 2 mm thickness | 0.85 ± 0.27b | 0.42 ± 0.14a* | 1.04 ± 0.27b | 0.55 ± 0.13a* | 2.17 ± 0.67b | 0.87 ± 0.06a* | 6.54 ± 0.26b | 2.94 ± 0.88a* |
| 20° (slight angulation) | 0.65 ± 0.17b | 0.39 ± 0.01a | 0.80 ± 0.26b | 0.49 ± 0.02a* | 1.62 ± 0.30b | 1.01 ± 0.17ab* | 3.93 ± 0.04c | 2.97 ± 0.31a* |
| 35° (moderate angulation) | 0.60 ± 0.15ab | 0.77 ± 0.12b | 0.75 ± 0.16b | 0.86 ± 0.12a | 1.52 ± 0.25b | 1.58 ± 0.06b | 5.32 ± 0.48d | 4.38 ± 0.57b* |
Ra, Rq, Rv, and Rt of the bottom surface of bulk fill and incremental resin composites following different curing conditions and 1-year of aging (mean ± SD). All resin composite specimens were cured with LCU1000 (Valo grand), which provides 1,029 mW/cm2 power output.
Ra, average surface roughness; Rp, maximum peak height; Rv, maximum valley depth; Rt, average distance between the highest peak and lowest valley; SD, standard deviation.
a,bValues indicated by different letters are statistically different from each other (
Table 1 Description of the commercial products evaluated in this study at different conditions of light-curing
Table 2 Results of surface roughness after photoactivation with LCU600 (Radii-Cal)
Ra, Rq, Rv, and Rt of the bottom surface of bulk fill and incremental resin composites following different curing conditions and 1-year of aging (mean ± SD).
Ra, average surface roughness; Rp, maximum peak height; Rv, maximum valley depth; Rt, average distance between the highest peak and lowest valley; SD, standard deviation.
a,bValues indicated by different letters are statistically different from each other (
Table 3 Results of surface roughness after photoactivation with LCU1000 (Valo grand)
Ra, Rq, Rv, and Rt of the bottom surface of bulk fill and incremental resin composites following different curing conditions and 1-year of aging (mean ± SD). All resin composite specimens were cured with LCU1000 (Valo grand), which provides 1,029 mW/cm2 power output.
Ra, average surface roughness; Rp, maximum peak height; Rv, maximum valley depth; Rt, average distance between the highest peak and lowest valley; SD, standard deviation.
a,bValues indicated by different letters are statistically different from each other (

