
Search
- Page Path
- HOME > Search
Research Articles
-
Procedural errors detected by cone beam tomography in cases with indication for retreatment:
in vivo cross-sectional study - Henry Paul Valverde Haro, Carmen Rosa Garcia Rupaya, Flávio R. F. Alves
- Restor Dent Endod 2024;49(3):e26. Published online June 24, 2024
- DOI: https://doi.org/10.5395/rde.2024.49.e26
-
 Abstract
Abstract
 PDF
PDF PubReader
PubReader ePub
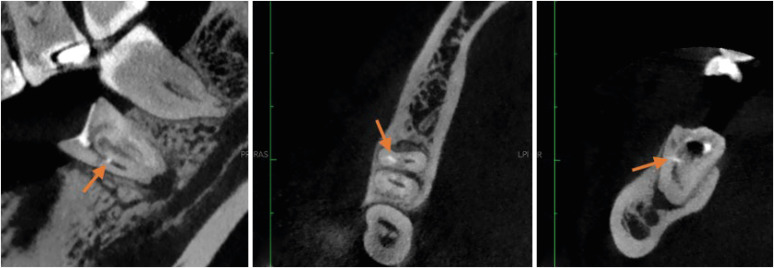
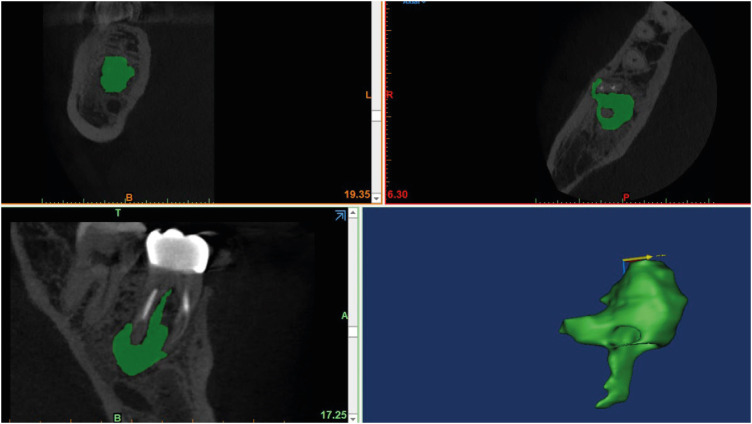
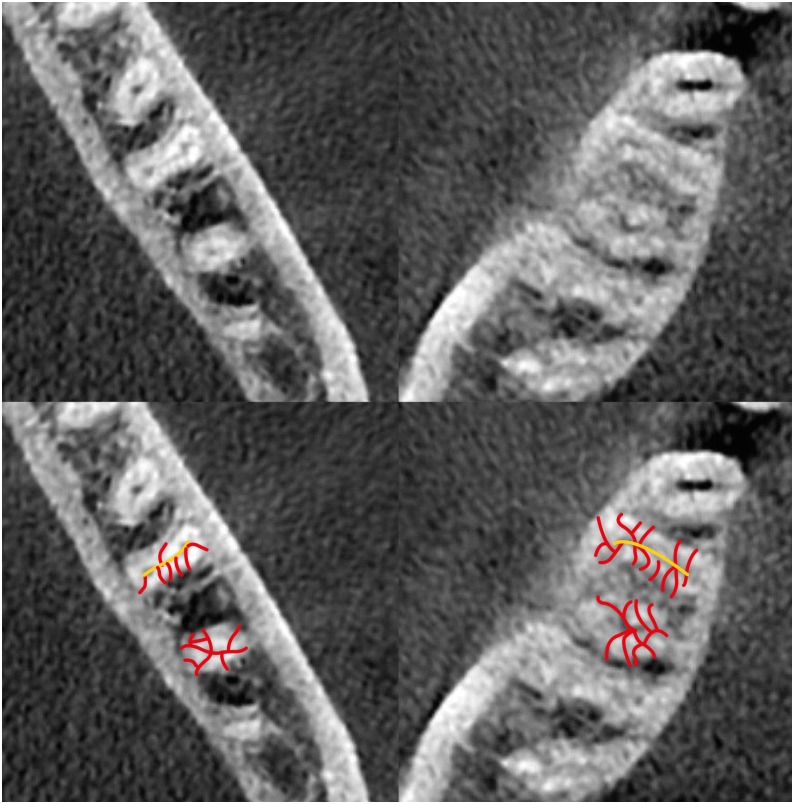
ePub Objectives This study aimed to investigate the frequency and type of endodontic procedural errors in cases indicated for retreatment through cone-beam computed tomography (CBCT) analysis.
Materials and Methods The sample consisted of 96 CBCT scans, encompassing 122 permanent teeth with fully formed roots. Errors included perforation, instrument fracture, canal transportation, missed canals, and inadequate apical limit of filling. Additionally, potential risk factors were analyzed and subjected to statistical modeling.
Results The most frequent procedural error observed was the inadequate apical limit of filling, followed by canal transportation, perforation, missed canal, and instrument fracture. Statistically significant associations were identified between various procedural errors and specific factors. These include canal transportation and root canal wall, with the buccal wall being the most commonly affected; missed canal and tooth type, particularly the palatine and second mesiobuccal canal canals; inadequate apical limit of filling and root curvature, showing a higher deviation to the mesial direction in severely curved canals; inadequate apical limit of filling and the presence of calcifications, with underfilling being the most frequent; canal transportation and periapical lesion, notably with deviation to the buccal direction; and the direction of perforation and periapical lesion, most frequently occurring to buccal direction.
Conclusions CBCT emerges as a valuable tool in identifying procedural errors and associated factors, crucial for their prevention and management.
-
Citations
Citations to this article as recorded by
- Regenerative endodontic treatment of a necrotic immature taurodont mandibular second molar with endodontic infection
Ali Mohammed Addokhi, Ahmed Abuhaimed
Saudi Endodontic Journal.2026; 16(2): 271. CrossRef - Repair of furcal perforations using different calcium silicate cements: An in vitro study
Ariana Esperanza Apolo Aguilar, Maria Soledad Peñaherrera Manosalvas, Henry Paul Valverde Haro
Journal of Conservative Dentistry and Endodontics.2025; 28(10): 1007. CrossRef - Impact of Downward Load and Rotational Kinematics on Root Canal Instrumentation with a Heat-Treated Nickel–Titanium Rotary Instrument
Risako Yamamoto, Keiichiro Maki, Shunsuke Kimura, Satoshi Omori, Keiko Hirano, Arata Ebihara, Yoshio Yahata, Takashi Okiji
Materials.2025; 19(1): 108. CrossRef - ANALYSIS OF THE QUALITY OF ROOT CANAL OBTURATION AND PREVALENCE OF APICAL PERIODONTITIS IN ENDODONTICALLY TREATED TEETH
Cristina Coralia Nistor, Ioana Suciu , Elena Zabrac , Ruxandra Ioana Bartok , Bogdan Dimitriu , Andreea Baluta
Romanian Journal of Oral Rehabilitation.2024; 16(4): 311. CrossRef
- Regenerative endodontic treatment of a necrotic immature taurodont mandibular second molar with endodontic infection
- 4,150 View
- 141 Download
- 2 Web of Science
- 4 Crossref

- Radiographic patterns of periosteal bone reactions associated with endodontic lesions
- Poorya Jalali, Jessica Riccobono, Robert A. Augsburger, Mehrnaz Tahmasbi-Arashlow
- Restor Dent Endod 2023;48(3):e23. Published online June 8, 2023
- DOI: https://doi.org/10.5395/rde.2023.48.e23
-
Abstract
PDFPubReaderePub
Objectives The formation of new bone by periosteum due to an insult is called periosteal bone reaction (PBR). This study assessed the cone beam computed tomography (CBCT) patterns of periosteal bone reactions associated with periapical inflammatory lesion (apical periodontitis/periapical rarefying osteitis).
Materials and Methods Twenty-two small field of view CBCT images of patients with PBR were selected from a database of a private practice limited to endodontics. The volume of the periapical inflammatory lesion, the presence of cortical fenestration, the distance of the root apices to the affected cortex, and the location, pattern, and longest diameter of the periosteal reaction were recorded. Statistical analysis was performed using Wilcoxon Ranksum, Fischer’s exact, Spearman Correlation Coefficient, and paired
t -test.Results In all cases, periosteal bone reaction manifested as either parallel (90.9%) or irregular (9.1%). No correlation was found between periapical inflammatory lesion volume and the periosteal reaction's longest diameter (
p > 0.05). Cortical fenestration was noted in 72.7% of the cases. In addition, the findings showed that periosteal reactions were located mostly on the buccal and were present 53.8% and 100% of the time in the mandible and maxilla, respectively.Conclusions The periosteal reactions of endodontic origin had a nonaggressive form (
i.e ., parallel or irregular), and none of the lesions resulted in a periosteal reaction with an ominous Codman’s triangle or spicule pattern.-
Citations
Citations to this article as recorded by- ENDODONTIA E INTERCORRÊNCIAS: COMPREENDENDO OS ACIDENTES E OTIMIZANDO O PROGNÓSTICO
Ana Paula Oliveira Rocha, Flávia Cordeiro Antunes , Millena Alberto Luna , Raissa Danielle Muniz Da Silva , Gustavo Henrique Palma Durães , Juliano Magno de Valadares Bicalho , Lorena Miranda Lima , Barbara Quadros Tonelli
REMUNOM.2026; 2(03): 1. CrossRef - Endodontic Intervention in Chronic Osteomyelitis With Proliferative Periostitis: A Rare Case Report and Scoping Review
Gabriel Lima Braz, Ana Paula Neutzling Gomes, Lisandrea Rocha Schardosim, Nadia de Souza Ferreira, Jose Francisco Gomez-Sosa
Case Reports in Dentistry.2026;[Epub] CrossRef - The influence of endodontic treatment quality on periapical lesions' architecture in cone‐beam computed tomography
Ewa Mackiewicz, Tobias Bonsmann, Krzysztof Safranow, Patrycja Nowicka, Janusz Kołecki, Alicja Nowicka
Australian Endodontic Journal.2025; 51(1): 36. CrossRef - Novel radiographic pattern of maxillary periostitis induced by endodontic inflammation: A case report
Pai-Chun Huang, I-Hao Su, Meng-Ling Chiang, Jyh-Kwei Chen
Journal of Dental Sciences.2025; 20(3): 1982. CrossRef - Garre’s osteomyelitis of the mandible managed by nonsurgical re-endodontic treatment
Heegyun Kim, Jiyoung Kwon, Hyun-Jung Kim, Soram Oh, Duck-Su Kim, Ji-Hyun Jang
Restorative Dentistry & Endodontics.2024;[Epub] CrossRef
- ENDODONTIA E INTERCORRÊNCIAS: COMPREENDENDO OS ACIDENTES E OTIMIZANDO O PROGNÓSTICO
- 6,797 View
- 105 Download
- 4 Web of Science
- 5 Crossref
-
Isthmuses, accessory canals, and the direction of root curvature in permanent mandibular first molars: an
in vivo computed tomography study - Aria Chuppani Dastgerdi, Manizheh Navabi, Vahid Rakhshan
- Restor Dent Endod 2020;45(1):e7. Published online December 12, 2019
- DOI: https://doi.org/10.5395/rde.2020.45.e7
-
Abstract
PDFPubReaderePub
Objectives This study was performed to assess the anatomy of mandibular first molars.
Materials and Methods In this
in vivo study, cone-beam computed tomography (CBCT) volumes of 312 bilateral intact first mandibular molars from 156 patients (79 men and 77 women; average age, 35.6 ± 11.2 years) were investigated in terms of the direction of each canal's curvature in the buccolingual and mesiodistal dimensions (direction of the position of the apex in relation to the longitudinal axis of the root), the presence of an isthmus (a narrow, ribbon-shaped communication between 2 root canals) in 3 segments (0–2, 2–4, and 4–6 mm) from the apex), and the presence and number of accessory canals (smaller canals besides the main root canals, connecting the pulp to the periodontium). Data were analyzed statistically (α = 0.05).Results Mesiolingual canals were mostly buccally and distally inclined, while mesiobuccal and distolingual canals were mostly distally curved. Isthmuses were more common in younger patients (χ2 test,
p < 0.05). The average numbers of accessory canals in the apical, middle, and coronal segments were 9.9 ± 4.2, 6.9 ± 2.9, and 9.3 ± 3.0 canals per segment, respectively (analysis of variance,p < 0.001). Age and sex were not associated with the number of accessory canals (p > 0.05).Conclusions The complex anatomy of these teeth deserves attention during non-surgical or surgical endodontic treatment. Around the apex, isthmuses might be more prevalent in younger and female individuals.
-
Citations
Citations to this article as recorded by- Micro-CT and histological examination of accessory canals in 34 equine cheek teeth
Szabolcs A. Korsós, Carsten Staszyk, Matthieu Boone, Iván Josipovic, Jörg Vogelsberg, Lieven Vlaminck
Frontiers in Veterinary Science.2024;[Epub] CrossRef - Diagnostic value of cone beam computed tomography for root canal morphology assessment – a micro-CT based comparison
Mariana Pires, Jorge N.R. Martins, Mário Rito Pereira, Isabel Vasconcelos, Rui Pereira da Costa, Isabel Duarte, António Ginjeira
Clinical Oral Investigations.2024;[Epub] CrossRef - Exploring age and gender variations in root canal morphology of maxillary premolars in Saudi sub population: a cross-sectional CBCT study
Mohmed Isaqali Karobari, Azhar Iqbal, Rumesa Batul, Abdul Habeeb Adil, Jamaluddin Syed, Hmoud Ali Algarni, Meshal Aber Alonazi, Tahir Yusuf Noorani
BMC Oral Health.2024;[Epub] CrossRef - Comprehensive analysis of root canal morphology in maxillary premolars among the Pakistani subpopulation: a CBCT-based study
Hmoud Ali Algarni, Meshal Aber Alonazi, Hamza Arshad, Fatima Zahra, Fahad Umer, Irfan Maqbool, Azhar Iqbal, Mohmed Isaqali Karobari
European Journal of Medical Research.2024;[Epub] CrossRef - The efficacy of a novel SWEEPS laser-activated irrigation compared to ultrasonic activation in the removal of pulp tissue from an isthmus area in the apical third of the root canal
Ivona Bago, Adriana Đurin, Debora Kanižaj, Lovorka Batelja Vuletić, Ivana Vidović Zdrilić, Ivica Anić
Lasers in Medical Science.2023;[Epub] CrossRef - Effect of passive ultrasonic irrigation on hard tissue debris removal: a systematic review and meta-analysis
Ana Flávia Almeida Barbosa, Carolina Oliveira de Lima, Luciana Moura Sassone, Raissa Dias Fares, Tatiana Kelly da Silva Fidalgo, Emmanuel João Nogueira Leal Silva
Brazilian Oral Research.2021;[Epub] CrossRef
- Micro-CT and histological examination of accessory canals in 34 equine cheek teeth
- 3,672 View
- 30 Download
- 6 Crossref
- Detection of root perforations using conventional and digital intraoral radiography, multidetector computed tomography and cone beam computed tomography
- Abbas Shokri, Amir Eskandarloo, Maruf Noruzi-Gangachin, Samira Khajeh
- Restor Dent Endod 2015;40(1):58-67. Published online November 13, 2014
- DOI: https://doi.org/10.5395/rde.2015.40.1.58
-
Abstract
PDFPubReaderePub
Objectives This study aimed to compare the accuracy of conventional intraoral (CI) radiography, photostimulable phosphor (PSP) radiography, cone beam computed tomography (CBCT) and multidetector computed tomography (MDCT) for detection of strip and root perforations in endodontically treated teeth.
Materials and Methods Mesial and distal roots of 72 recently extracted molar were endodontically prepared. Perforations were created in 0.2, 0.3, or 0.4 mm diameter around the furcation of 48 roots (strip perforation) and at the external surface of 48 roots (root perforation); 48 roots were not perforated (control group). After root obturation, intraoral radiography, CBCT and MDCT were taken. Discontinuity in the root structure was interpreted as perforation. Two observers examined the images. Data were analyzed using Stata software and Chi-square test.
Results The sensitivity and specificity of CI, PSP, CBCT and MDCT in detection of strip perforations were 81.25% and 93.75%, 85.42% and 91.67%, 97.92% and 85.42%, and 72.92% and 87.50%, respectively. For diagnosis of root perforation, the sensitivity and specificity were 87.50% and 93.75%, 89.58% and 91.67%, 97.92% and 85.42%, and 81.25% and 87.50%, respectively. For detection of strip perforation, the difference between CBCT and all other methods including CI, PSP and MDCT was significant (
p < 0.05). For detection of root perforation, only the difference between CBCT and MDCT was significant, and for all the other methods no statistically significant difference was observed.Conclusions If it is not possible to diagnose the root perforations by periapical radiographs, CBCT is the best radiographic technique while MDCT is not recommended.
-
Citations
Citations to this article as recorded by- Factors Influencing the Outcome of Iatrogenic Perforation Repair in Permanent Teeth—A Narrative Review
Saravanan Poorni, Srividhya Srinivasan, Thomas Clauder, Manali Ramakrishnan Srinivasan, Paul M. H. Dummer, Venkateshbabu Nagendrababu
Australian Endodontic Journal.2026;[Epub] CrossRef - The relationship between radiographic measurements of alveolar bone in posterior single-tooth edentulous regions and non-alveolar jawbones using multidetector computed tomography
Imad Barngkgei, Leen Khattash, Samar Kakhia
Oral Radiology.2025; 41(1): 10. CrossRef - Prevention, Diagnostic Challenges, and Management of Endodontic Perforations: A Narrative Review
Taylor M. DeVine, Nora L. Paisner, Adeyinka F. Dayo
Complications.2025; 2(3): 17. CrossRef - Extrusion of debris during retreatment using various nickel-titanium files in teeth with simulated lateral root perforation
Hatice Harorlı, Simay Koç, Alper Kuştarcı
Journal of Oral Science.2024; 66(3): 189. CrossRef - The importance of cone-beam computed tomography in endodontic therapy: A review
Shaul Hameed Kolarkodi
The Saudi Dental Journal.2023; 35(7): 780. CrossRef - Assessment of the diagnostic accuracy of strip and furcal perforations in different sizes by cone beam computed tomography
Zahra Ghoncheh, Hanieh Kaviani, Sara Soleimani, Shifteh Nasri, Fatemeh Malekpour, Farzaneh Afkhami
Oral Radiology.2023; 39(4): 654. CrossRef - Konik Işınlı Bilgisayarlı Tomografinin Endodontik Uygulamalarda Kullanımı
Gülsün AKAY, Kahraman GÜNGÖR
ADO Klinik Bilimler Dergisi.2022; 11(1): 8. CrossRef - CBCT Visualization of Furcation Perforation Repair Materials Using Different Voxel Sizes
Ayse Isıl ORHAN, Pelin TUFENKCİ, Aysenur ONCU, Sevinc SEVGI, Berkan CELİKTEN, Kaan ORHAN
Clinical and Experimental Health Sciences.2021; 11(4): 654. CrossRef - Accuracy of Conventional Periapical Radiography in Diagnosing Furcation Repair after Perforation Treatment
Stephanie Díaz Huamán, Maria Gerusa Brito Aragão, Ana Paula Dias Moreno, Alexandra Mussolino de Queiroz, Raquel Assed Bezerra da Silva, Francisco Wanderley Garcia de Paula-Silva, Léa Assed Bezerra da Silva
Journal of Endodontics.2020; 46(6): 827. CrossRef - Association between marginal bone loss and bone quality at dental implant sites based on evidence from cone beam computed tomography and periapical radiographs
Amir Eskandarloo, Reza Arabi, Mohsen Bidgoli, Faezeh Yousefi, Jalal Poorolajal
Contemporary Clinical Dentistry.2019; 10(1): 36. CrossRef - Effect of exposure parameters of cone beam computed tomography on metal artifact reduction around the dental implants in various bone densities
Abbas Shokri, Mohammad Reza Jamalpour, Atefeh Khavid, Zeinab Mohseni, Masoud Sadeghi
BMC Medical Imaging.2019;[Epub] CrossRef - Enhancing the three-dimensional visualization of a foreign object using Mimics software
Muhammad Khan Asif, Phrabhakaran Nambiar, Iqra Muhammad Khan, Zeti Adura Binti Che Ab Aziz, Nora Sakina Binti Mohd Noor, Palasuntharam Shanmuhasuntharam, Norliza Ibrahim
Radiology Case Reports.2019; 14(12): 1545. CrossRef - Diagnostic Accuracy of Three Cone Beam Computed Tomography Systems and Periapical Radiography for Detection of Fenestration Around Dental Implants
Amir Eskandarloo, Samira Saati, Mahbubeh Purabdolahi Ardakani, Mohamadreza Jamalpour, Naser Mohammad Gholi Mezerji, Vahid Akheshteh
Contemporary Clinical Dentistry.2018; 9(3): 376. CrossRef - Evidence-based decision-making in endodontics
Eyal Rosen, Igor Tsesis
Clinical Dentistry Reviewed.2017;[Epub] CrossRef - Incidence of pulp sensibility loss of anterior teeth after paramedian insertion of orthodontic mini-implants in the anterior maxilla
Jan Hourfar, Dirk Bister, Jörg A. Lisson, Björn Ludwig
Head & Face Medicine.2017;[Epub] CrossRef - Image analysis for dental bone quality assessment using CBCT imaging
Suprijanto, L Epsilawati, M S Hajarini, E Juliastuti, H Susanti
Journal of Physics: Conference Series.2016; 694: 012065. CrossRef - Identification of the Procedural Accidents During Root Canal Preparation Using Digital Intraoral Radiography and Cone Beam Computed Tomography
K.-Ivácson A.- Csinszka, Monea Adriana Maria, Monea Monica, Pop Mihai, Borda Angela
Acta Medica Marisiensis.2016; 62(3): 326. CrossRef
- Factors Influencing the Outcome of Iatrogenic Perforation Repair in Permanent Teeth—A Narrative Review
- 3,339 View
- 17 Download
- 17 Crossref
 First
First Prev
Prev

