
Articles
- Page Path
- HOME > Restor Dent Endod > Volume 46(4); 2021 > Article
- Research Article Fracture incidence of Reciproc instruments during root canal retreatment performed by postgraduate students: a cross-sectional retrospective clinical study
-
Liliana Machado Ruivo1
 , Marcos de Azevedo Rios2, Alexandre Mascarenhas Villela3, Alexandre Sigrist de Martin1, Augusto Shoji Kato4, Rina Andrea Pelegrine1, Ana Flávia Almeida Barbosa5, Emmanuel João Nogueira Leal Silva5,6, Carlos Eduardo da Silveira Bueno1
, Marcos de Azevedo Rios2, Alexandre Mascarenhas Villela3, Alexandre Sigrist de Martin1, Augusto Shoji Kato4, Rina Andrea Pelegrine1, Ana Flávia Almeida Barbosa5, Emmanuel João Nogueira Leal Silva5,6, Carlos Eduardo da Silveira Bueno1 -
Restor Dent Endod 2021;46(4):e49.
DOI: https://doi.org/10.5395/rde.2021.46.e49
Published online: September 9, 2021
1Department of Endodontics, São Leopoldo Mandic Dental Research Center, Campinas, SP, Brazil.
2Department of Endodontics, Universidade Estadual de Feira de Santana, Feira de Santana, BA, Brazil.
3Department of Endodontics, Centro Baiano de Estudos Odontológicos, Salvador, BA, Brazil.
4Department of Restorative Dentistry, Endodontics and Dental Materials, Bauru Dental School, University of São Paulo, Bauru, SP, Brazil.
5Department of Endodontics, Rio de Janeiro State University (UERJ), Rio de Janeiro, RJ, Brazil.
6Department of Endodontic, Grande Rio University (UNIGRANRIO), Rio de Janeiro, RJ, Brazil.
- Correspondence to Emmanuel João Nogueira Leal Silva, DDS, MSc, PhD. Associate Professor, Department of Endodontics, Grande Rio University (UNIGRANRIO) School of Dentistry, Rua Herotides de Oliveira, 61/902 Icaraí, Niterói, RJ 24230-230, Brazil. nogueiraemmanuel@hotmail.com
• Received: January 8, 2021 • Revised: February 18, 2021 • Accepted: February 21, 2021
Copyright © 2021. The Korean Academy of Conservative Dentistry
This is an Open Access article distributed under the terms of the Creative Commons Attribution Non-Commercial License (https://creativecommons.org/licenses/by-nc/4.0/) which permits unrestricted non-commercial use, distribution, and reproduction in any medium, provided the original work is properly cited.
Abstract
-
Objectives To evaluate the fracture incidence of Reciproc R25 instruments (VDW) used during non-surgical root canal retreatments performed by students in a postgraduate endodontic program.
-
Materials and Methods From the analysis of clinical record cards and periapical radiographs of root canal retreatments performed by postgraduate students using the Reciproc R25, a total of 1,016 teeth (2,544 root canals) were selected. The instruments were discarded after a single use. The general incidence of instrument fractures and its frequency was analyzed considering the group of teeth and the root thirds where the fractures occurred. Statistical analysis was performed using the χ2 test (p < 0.01).
-
Results Seven instruments were separated during the procedures. The percentage of fracture in relation to the number of instrumented canals was 0.27% and 0.68% in relation to the number of instrumented teeth. Four fractures occurred in maxillary molars, 1 in a mandibular molar, 1 in a mandibular premolar and 1 in a maxillary incisor. A greater number of fractures was observed in molars when compared with the number of fractures observed in the other dental groups (p < 0.01). Considering all of the instrument fractures, 71.43% were located in the apical third and 28.57% in the middle third (p < 0.01). One instrument fragment was removed, one bypassed, while in 5 cases, the instrument fragment remained inside the root canal.
-
Conclusions The use of Reciproc R25 instruments in root canal retreatments carried out by postgraduate students was associated with a low incidence of fractures.
INTRODUCTION
Despite the improvement of the technology used in root canal treatment, failures can occur. Most failures are usually related to the survival of microorganisms within the root canal systems, and in such cases, root canal reintervention is indicated as an attempt to correct flaws of the initial treatment [1,2]. During retreatment procedures, it is important to properly remove the filling materials and gain access to the apical foramen to make cleaning, shaping and disinfection procedures of the root canal system easier [3,4].
Several instruments were developed in order to perform the retreatment procedures [5,6,7]; however, despite not being originally designed for retreatment, the reciprocating movement could potentially be beneficial for the effective and safe removal of root filling material as confirmed by previous studies [8,9,10]. In addition, the idea of a reduced number of nickel-titanium (NiTi) instruments to remove filling materials is indeed appealing due to its safety and technique simplification. From an educational point of view, these aspects may result in a shorter and straighter learning curve, favoring professionals with little experience and allowing good results to be achieved [11].
Reciprocating kinematics per se has been linked to an extended lifespan of instruments when compared to continuous rotary motion [12]. Reciprocating kinematics relives the stress of the instrument by alternating counterclockwise and clockwise movements, explaining the greater fatigue resistance of instruments activated under this motion. Furthermore, the reciprocating motion reduces taper lock and thus, the overall risk of torsion fracture, as the instrument does not perform continuous full-360º turns [13]. As a direct result, clinical studies show reduced rates of kinematic fracture when these instruments were used during root canal treatment and retreatment [14,15,16,17]. Reciprocating systems have been considered to be safe and present a low incidence of instrument fractures, even when the root canal treatment was performed by undergraduate students [18]. However, an assessment of fracture incidence during root canal retreatment cases conducted by less experienced professionals, such as postgraduate students is currently not available in literature. Therefore, the aim of the present study was to evaluate the fracture incidence of Reciproc R25 instruments (VDW, Munich, Germany) in root canal retreatments performed by students from a post graduate program in endodontics.
MATERIALS AND METHODS
This study was approved by the local ethics committee (approval No. 1.563.723). A sample size calculation was performed using the χ2 test. Based on degrees of freedom 1, α = 0.01 and 95% power, a total of 726 samples were indicated as the ideal size required for observing significant differences. Therefore, a total of 1,016 teeth matching the inclusion criteria were obtained from medical records. The number of teeth and the number of root canals used in this study are shown in Table 1.
Table 1
Number of total teeth and root canals used in this study
The root canal retreatment was performed in incisors, canines, premolars and molars. The reintervention with the instrument Reciproc R25 (VDW) was performed with “RECIPROC ALL” movement on a VDW Silver motor (VDW) according to the instructions provided by the manufacturer. Each instrument was used for a single tooth.
All root canal retreatments were performed by 24 postgraduate students from July 2014 until March 2017. The teeth were selected from patients with ages between 18 to 60 years old, with completely formed apices and curvatures under 45° [19].
The same protocol was adopted for every procedure, and it is as follows [17]: First off infiltrative anesthesia would be administered, followed by removal of the previous restoration with the aid of a high-speed spherical diamond bur, with sizes compatible with the volume of each pulp chamber; once the form of convenience was established, the isolation was performed and the access was finished. Afterwards, the top coronal part of the root filling material was removed by Gates Glidden or ultrasonic tips, followed by the Reciproc R25 instrument, used with three “in-and-out” movements with slight apical pressure. The instrument was, then, removed and cleaned with a sterile gauze; the root canal was irrigated with 2.5% sodium hypochlorite (NaOCl). These steps were repeated until apical patency was achieved with a size 10 K-file (Dentsply-Sirona, Baillagues, Switzerland). The working length (WL) was established at 1 mm short of the apical foramen using a Romiapex A15 electronic foraminal locator (Romidan, Kiryat Ono, Israel). The apical third of the root canal was prepared, repeating the same movement until the R25 instrument reached the WL. After 3 movements, the instrument was removed from the canal, cleaned with a sterile gauze and reintroduced. A total of 20 ml of 2.5% NaOCl were used for each tooth. A size 10 K-file was used to verify and maintain patency every time an instrument was removed from the root canal. In the retreatment cases in which the WL could not be reached, Reciproc R25 instruments were used up until where the hand file would reach. Instruments were used until no gutta-percha residues were observed neither on the instrument nor within the root canal by means of an operating microscope with a 16× magnification (Alliance Microscopia, São Paulo, Brazil). In all cases, a lateral brushing cutting action was performed to relocate the orifices and to prepare around the entire canal circumference. When necessary, R40 and/or R50 instruments were used to complement the removal of gutta-percha.
After root canal preparation, irrigation using ultrasonic activation with 2.5% NaOCl and 17% ethylenediaminetetraacetic acid was performed and the root canals were dried and filled, either in the same or in a subsequent visit. A database of all cases was maintained including data on instrument fracture, such as tooth, canal involved and resolution of the case, that is, instrument removed, bypassed or remained inside the root canal.
The risk of fracture was calculated according to tooth types and root canal thirds and compared using χ2 test at a 5% significance level.
RESULTS
A total of 1,016 retreatments involving 2,544 root canals were performed. The details of the samples used are shown in Table 1.
A total of 7 Reciproc R25 instruments were fractured during root canal retreatments, which represents 0.68% of the number of teeth and 0.27% of the number of root canals treated. Four fractures occurred in maxillary molars, 1 in a mandibular molar, 1 in a mandibular premolar and 1 in a maxillary incisor (Figure 1). A greater number of fractures was observed in molars when compared with the number of fractures observed in the other dental groups (p < 0.01). Considering all of the instrument fractures, 71.43% were located in the apical third and 28.57% in the middle third (p < 0.01). One instrument fragment was removed and one bypassed, while in 5 cases the instrument fragment remained inside the root canal. These results are available in Table 2. Thirteen R40 instruments and 7 R50 instruments were used to complement the removal of gutta-percha. No fracture was registered for the Reciproc R40 and R50 instruments.
Figure 1
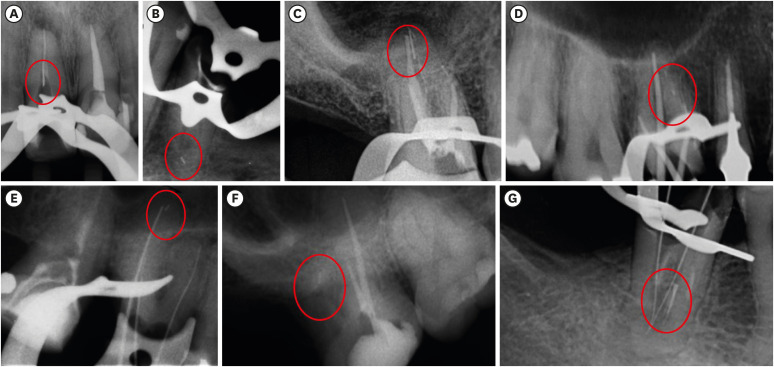
Radiograph images of the 7 Reciproc R25 instruments fractured during root canal retreatments in each tooth and respective root canal. A maxillary central incisor with a fragment of fractured instrument in its middle third (A); a mandibular second premolar with a fragment of fractured instrument in the apical third of its vestibular root canal (B); a maxillary second molar with a fragment of fractured instrument in the apical third of its palatal root canal (C); a maxillary first molar with a fragment of fractured instrument in the apical third of its mesiobuccal root canal (D); a maxillary first molar with a fragment of fractured instrument in the apical third of its palatal root canal (E); a maxillary second molar with a fragment of fractured instrument in the apical third of its distobuccal root canal (F); a mandibular first molar with a fragment of fractured instrument in the middle third of its mesiobuccal root canal (G).
Table 2
Number of fractures in each group of teeth according to the respective tooth and root canal, fracture position, fragment size, and fragment management
DISCUSSION
The success of root canal retreatment is directly related to the maximum removal of root filling materials, since these remnants may contain necrotic tissues and microorganisms responsible for the failure of the original endodontic treatment [1,2]. The use of instruments with reciprocating movement during the retreatment procedures is well established in literature, as these instruments require less time to complete the removal of filling material while being just as efficient as the other systems but with smaller fracture rates [8,9,20,21]. The majority of the studies performed were in vitro and, to this day, only one clinical study was performed to assess the fracture incidence of Reciproc instruments during root canal retreatment [17]. However, the mentioned study evaluated 757 retreatment cases, while in this study 1,016 cases were evaluated.
All the dental groups retreated with the Reciproc R25 instrument were included in this study, in order to have a wider and more varied pool of samples. In addition, while some studies regarding endodontic treatment, assessed the total number of teeth in which the instrument fractured occurred, this study, as others, also evaluated the total number of instrumented root canals [14,16,17,22,23].
The fracture incidence of reciprocating instruments in relation to the number of root canals, and the number of teeth was 0.27% and 0.68%, respectively. These results might be related to the physical and mechanical properties of the instruments manufactured with the M-Wire alloy. The considerable resistance to cyclic fatigue of these instruments has been reported by several studies [15,22,24,25,26]. Similar results were found by Cunha et al. [14] and Shen et al. [16] during root canal treatment, and Plotino et al. [17] during root canal treatment and retreatment. However, the studies of Cunha et al. [14] and Plotino et al. [17] were performed by specialists in endodontics, whereas in Shen et al. [16], the teeth were treated by graduate and postgraduate students. In this study, the teeth were retreated only by postgraduate students previously trained in preclinical laboratories.
Previous clinical studies have assessed the influence of operator training on the incidence of instrument fractures in cases of endodontic treatment when using manual and motor-driven instruments [14,15,16,17,22,23,25,27,28,29]. The present retrospective clinical study showed a reduced percentage of fractures in relation to the number of root canals (0.27%) using Reciproc R25 instruments in retreatment cases, regardless of the fact that it was performed by postgraduate students. This might indicate that reciprocating kinematics also amounts to a shorter learning curve in endodontics retreatment, as reported by Muñoz et al. [30]. That may be proven to be even more so if one considers previous studies in which continuous rotation instruments were used and the experience of the operator was a determining factor in the quality of the instrumentation of the teeth and in the fracture or deformation of NITI instruments [24,25].
A greater number of instrument fractures was observed in molars when compared with the number of fractures observed in the other groups of teeth, a fact corroborated by previous studies [27,29,31]. This finding is related to the anatomic characteristics of these teeth, which imposed greater difficulties during instrumentation, predisposing a higher incidence of instrument fractures. Besides that, it must be considered that anterior and posterior teeth have a different number of root canals, with the former usually presenting a single root canal, whereas the latter presents multiple. That means that a single instrument is used in multiple root canals for each posterior tooth, while each instrument is used in a single root canal for anterior teeth. The fractures occurred during the preparation of middle and apical root thirds. These results are corroborated by the study of Cheung [32], according to which the curvature between the middle and the apical thirds of the root canals of molars are the sections most prone to fractures. In this study, the fractures occurred mostly in the apical third, as a result of their anatomy, smaller dimensions and the eventual presence of curvatures [14,33,34].
The results obtained in the present study, the studies of Muñoz et al. [30] and Shen et al. [16] showed a reduced rate of reciprocating instruments fracture when used by postgraduate students. The fact that students with limited experience are being able to safely use reciprocating instruments suggests that the resort to these kinds of instruments can shorten the learning process and improve the results of inexperienced professionals.
CONCLUSIONS
Based on the results of this retrospective clinical study, Reciproc R25 showed a low fracture incidence during root canal retreatment, despite it being performed by students in a postgraduate program of endodontics.
-
Conflict of Interest: No potential conflict of interest relevant to this article was reported.
-
Author Contributions:
Conceptualization: Ruivo LM, Rios MA, Vilela AM, Bueno CES.
Formal analysis: Martin AS.
Investigation: Ruivo LM, Pelegrine RA, Kato AS.
Methodology: Ruivo LM, Pelegrine RA, Rios MA, Vilela AM, Bueno CES.
Project administration: Bueno CES.
Supervision: Bueno CES.
Writing - original draft: Barbosa AFA.
Writing - review & editing: Silva EJNL.
- 1. Siqueira JF Jr, Rôças IN. Clinical implications and microbiology of bacterial persistence after treatment procedures. J Endod 2008;34:1291-1301.e3.ArticlePubMed
- 2. Mollo A, Botti G, Prinicipi Goldoni N, Randellini E, Paragliola R, Chazine M, Ounsi HF, Grandini S. Efficacy of two Ni-Ti systems and hand files for removing gutta-percha from root canals. Int Endod J 2012;45:1-6.ArticlePubMed
- 3. Saad AY, Al-Hadlaq SM, Al-Katheeri NH. Efficacy of two rotary NiTi instruments in the removal of gutta-percha during root canal retreatment. J Endod 2007;33:38-41.ArticlePubMed
- 4. Marques da Silva B, Baratto-Filho F, Leonardi DP, Henrique Borges A, Volpato L, Branco Barletta F. Effectiveness of ProTaper, D-RaCe, and Mtwo retreatment files with and without supplementary instruments in the removal of root canal filling material. Int Endod J 2012;45:927-932.ArticlePubMed
- 5. Akbulut MB, Akman M, Terlemez A, Magat G, Sener S, Shetty H. Efficacy of Twisted File Adaptive, Reciproc and ProTaper Universal Retreatment instruments for root-canal-filling removal: a cone-beam computed tomography study. Dent Mater J 2016;35:126-131.ArticlePubMed
- 6. Alves FR, Marceliano-Alves MF, Sousa JC, Silveira SB, Provenzano JC, Siqueira JF Jr. Removal of root canal fillings in curved canals using either reciprocating single- or rotary multi-instrument systems and a supplementary step with the XP-Endo Finisher. J Endod 2016;42:1114-1119.ArticlePubMed
- 7. Crozeta BM, Silva-Sousa YT, Leoni GB, Mazzi-Chaves JF, Fantinato T, Baratto-Filho F, Sousa-Neto MD. Micro-computed tomography study of filling material removal from oval-shaped canals by using rotary, reciprocating, and adaptive motion systems. J Endod 2016;42:793-797.ArticlePubMed
- 8. Zuolo AS, Mello JE Jr, Cunha RS, Zuolo ML, Bueno CES. Efficacy of reciprocating and rotary techniques for removing filling material during root canal retreatment. Int Endod J 2013;46:947-953.ArticlePubMed
- 9. Rios Mde A, Villela AM, Cunha RS, Velasco RC, De Martin AS, Kato AS, Bueno CES. Efficacy of 2 reciprocating systems compared with a rotary retreatment system for gutta-percha removal. J Endod 2014;40:543-546.ArticlePubMed
- 10. Kırıcı D, Demirbuga S, Karataş E. Micro-computed tomographic assessment of the residual filling volume, apical transportation, and crack formation after retreatment with Reciproc and Reciproc Blue systems in curved root canals. J Endod 2020;46:238-243.ArticlePubMed
- 11. Silva EJNL, Vieira VTL, Hecksher F, Dos Santos Oliveira MRS, Dos Santos Antunes H, Moreira EJL. Cyclic fatigue using severely curved canals and torsional resistance of thermally treated reciprocating instruments. Clin Oral Investig 2018;22:2633-2638.ArticlePubMedPDF
- 12. Ferreira F, Adeodato C, Barbosa I, Aboud L, Scelza P, Zaccaro Scelza M. Movement kinematics and cyclic fatigue of NiTi rotary instruments: a systematic review. Int Endod J 2017;50:143-152.ArticlePubMedPDF
- 13. Varela-Patiño P, Ibañez-Párraga A, Rivas-Mundiña B, Cantatore G, Otero XL, Martin-Biedma B. Alternating versus continuous rotation: a comparative study of the effect on instrument life. J Endod 2010;36:157-159.ArticlePubMed
- 14. Cunha RS, Junaid A, Ensinas P, Nudera W, Bueno CES. Assessment of the separation incidence of reciprocating WaveOne files: a prospective clinical study. J Endod 2014;40:922-924.ArticlePubMed
- 15. Bueno CSP, Oliveira DP, Pelegrine RA, Fontana CE, Rocha DGP, Bueno CES. Fracture incidence of WaveOne and Reciproc files during root canal preparation of up to 3 posterior teeth: a prospective clinical study. J Endod 2017;43:705-708.ArticlePubMed
- 16. Shen Y, Coil JM, Mo AJ, Wang Z, Hieawy A, Yang Y, Haapasalo M. WaveOne rotary instruments after clinical use. J Endod 2016;42:186-189.ArticlePubMed
- 17. Plotino G, Grande NM, Porciani PF. Deformation and fracture incidence of Reciproc instruments: a clinical evaluation. Int Endod J 2015;48:199-205.PubMed
- 18. Caballero-Flores H, Nabeshima CK, Binotto E, Machado ME. Fracture incidence of instruments from a single-file reciprocating system by students in an endodontic graduate programme: a cross-sectional retrospective study. Int Endod J 2019;52:13-18.ArticlePubMedPDF
- 19. Schneider SW. A comparison of canal preparations in straight and curved root canals. Oral Surg Oral Med Oral Pathol 1971;32:271-275.ArticlePubMed
- 20. Özyürek T, Demiryürek EÖ. Efficacy of different nickel-titanium instruments in removing gutta-percha during root canal retreatment. J Endod 2016;42:646-649.ArticlePubMed
- 21. De-Deus G, Belladonna FG, Zuolo AS, Simões-Carvalho M, Santos CB, Oliveira DS, Cavalcante DM, Silva EJNL. Effectiveness of Reciproc Blue in removing canal filling material and regaining apical patency. Int Endod J 2019;52:250-257.ArticlePubMedPDF
- 22. Iqbal MK, Kohli MR, Kim JS. A retrospective clinical study of incidence of root canal instrument separation in an endodontics graduate program: a PennEndo database study. J Endod 2006;32:1048-1052.ArticlePubMed
- 23. Ehrhardt IC, Zuolo ML, Cunha RS, De Martin AS, Kherlakian D, Carvalho MC, Bueno CES. Assessment of the separation incidence of mtwo files used with preflaring: prospective clinical study. J Endod 2012;38:1078-1081.ArticlePubMed
- 24. Yared GM, Dagher FE, Machtou P, Kulkarni GK. Influence of rotational speed, torque and operator proficiency on failure of Greater Taper files. Int Endod J 2002;35:7-12.ArticlePubMed
- 25. Al-Omari MA, Aurich T, Wirtti S. Shaping canals with ProFiles and K3 instruments: does operator experience matter? Oral Surg Oral Med Oral Pathol Oral Radiol Endod 2010;110:e50-e55.ArticlePubMed
- 26. Plotino G, Grande NM, Testarelli L, Gambarini G. Cyclic fatigue of Reciproc and WaveOne reciprocating instruments. Int Endod J 2012;45:614-618.ArticlePubMed
- 27. Di Fiore PM, Genov KA, Komaroff E, Li Y, Lin L. Nickel-titanium rotary instrument fracture: a clinical practice assessment. Int Endod J 2006;39:700-708.ArticlePubMed
- 28. Knowles KI, Hammond NB, Biggs SG, Ibarrola JL. Incidence of instrument separation using LightSpeed rotary instruments. J Endod 2006;32:14-16.ArticlePubMed
- 29. Wolcott S, Wolcott J, Ishley D, Kennedy W, Johnson S, Minnich S, Meyers J. Separation incidence of ProTaper rotary instruments: a large cohort clinical evaluation. J Endod 2006;32:1139-1141.ArticlePubMed
- 30. Muñoz E, Forner L, Llena C. Influence of operator's experience on root canal shaping ability with a rotary nickel-titanium single-file reciprocating motion system. J Endod 2014;40:547-550.ArticlePubMed
- 31. Machado R, Júnior CS, Colombelli MF, Picolli AP, Junior JS, Cosme-Silva L, Garcia LDFR, Alberton LR. Incidence of ProTaper universal system instrument fractures - a retrospective clinical study. Eur Endod J 2018;3:77-81.ArticlePubMedPMC
- 32. Cheung GS. Instrument fracture: mechanisms, removal of fragments, and clinical outcomes. Endod Topics 2009;16:1-26.Article
- 33. Parashos P, Messer HH. Rotary NiTi instrument fracture and its consequences. J Endod 2006;32:1031-1043.ArticlePubMed
- 34. Ungerechts C, Bårdsen A, Fristad I. Instrument fracture in root canals - where, why, when and what? A study from a student clinic. Int Endod J 2014;47:183-190.ArticlePubMed
REFERENCES
Tables & Figures
REFERENCES
Citations
Citations to this article as recorded by 
- Reciprocating Kinematics in Endodontics: 18 Years of Scientific Evolution and Global Research Trends
Luiz Fernando Monteiro Czornobay, Aurélio de Oliveira Rocha, Lucas Menezes dos Anjos, Christiane Cabral Leite, Bruno Alexandre Pacheco de Castro Henriques, Cleonice da Silveira Teixeira, Emmanuel João Nogueira Leal da Silva, Lucas da Fonseca Roberti Garci
International Endodontic Journal.2026;[Epub] CrossRef - Reciprocating Torsional Fatigue and Mechanical Tests of Thermal-Treated Nickel Titanium Instruments
Victor Talarico Leal Vieira, Alejandro Jaime, Carlos Garcia Puente, Giuliana Soimu, Emmanuel João Nogueira Leal Silva, Carlos Nelson Elias, Gustavo de Deus
Journal of Endodontics.2025; 51(3): 359. CrossRef - Neodymium-Doped Yttrium Aluminum Perovskite (Nd:YAP) Laser in the Elimination of Endodontic Nickel-Titanium Files Fractured in Rooted Canals (Part 2: Teeth With Significant Root Curvature)
Amaury Namour, Marwan El Mobadder, Clément Cerfontaine, Patrick Matamba, Lucia Misoaga, Delphine Magnin , Praveen Arany, Samir Nammour
Cureus.2025;[Epub] CrossRef - Temperature-Dependent Effects on Cyclic Fatigue Resistance in Three Reciprocating Endodontic Systems: An In Vitro Study
Marcela Salamanca Ramos, José Aranguren, Giulia Malvicini, Cesar De Gregorio, Carmen Bonilla, Alejandro R. Perez
Materials.2025; 18(5): 952. CrossRef - The Cost of Instrument Retrieval on the Root Integrity
Marco A. Versiani, Hugo Sousa Dias, Emmanuel J. N. L. Silva, Felipe G. Belladonna, Jorge N. R. Martins, Gustavo De‐Deus
International Endodontic Journal.2025; 58(12): 1948. CrossRef - Multimethod analysis of large‐ and low‐tapered single file reciprocating instruments: Design, metallurgy, mechanical performance, and irrigation flow
Emmanuel João Nogueira Leal Silva, Fernando Peña‐Bengoa, Natasha C. Ajuz, Victor T. L. Vieira, Jorge N. R. Martins, Duarte Marques, Ricardo Pinto, Mario Rito Pereira, Francisco Manuel Braz‐Fernandes, Marco A. Versiani
International Endodontic Journal.2024; 57(5): 601. CrossRef - Nd: YAP Laser in the Elimination of Endodontic Nickel-Titanium Files Fractured in Rooted Canals (Part 1: Teeth With Minimal Root Curvature)
Amaury Namour, Marwan El Mobadder, Patrick Matamba, Lucia Misoaga, Delphine Magnin , Praveen Arany, Samir Nammour
Cureus.2024;[Epub] CrossRef - Cyclic Fatigue of Different Reciprocating Endodontic Instruments Using Matching Artificial Root Canals at Body Temperature In Vitro
Sebastian Bürklein, Paul Maßmann, Edgar Schäfer, David Donnermeyer
Materials.2024; 17(4): 827. CrossRef - Endodontic Orthograde Retreatments: Challenges and Solutions
Alessio Zanza, Rodolfo Reda, Luca Testarelli
Clinical, Cosmetic and Investigational Dentistry.2023; Volume 15: 245. CrossRef - Design, metallurgy, mechanical properties, and shaping ability of 3 heat-treated reciprocating systems: a multimethod investigation
Emmanuel J. N. L. Silva, Jorge N. R. Martins, Natasha C. Ajuz, Henrique dos Santos Antunes, Victor Talarico Leal Vieira, Francisco Manuel Braz-Fernandes, Felipe Gonçalves Belladonna, Marco Aurélio Versiani
Clinical Oral Investigations.2023; 27(5): 2427. CrossRef - Noncontact 3D evaluation of surface topography of reciprocating instruments after retreatment procedures
Miriam Fatima Zaccaro-Scelza, Renato Lenoir Cardoso Henrique Martinez, Sandro Oliveira Tavares, Fabiano Palmeira Gonçalves, Marcelo Montagnana, Emmanuel João Nogueira Leal da Silva, Pantaleo Scelza
Brazilian Dental Journal.2022; 33(3): 38. CrossRef
 ePub Link
ePub Link Cite
CiteFracture incidence of Reciproc instruments during root canal retreatment performed by postgraduate students: a cross-sectional retrospective clinical study
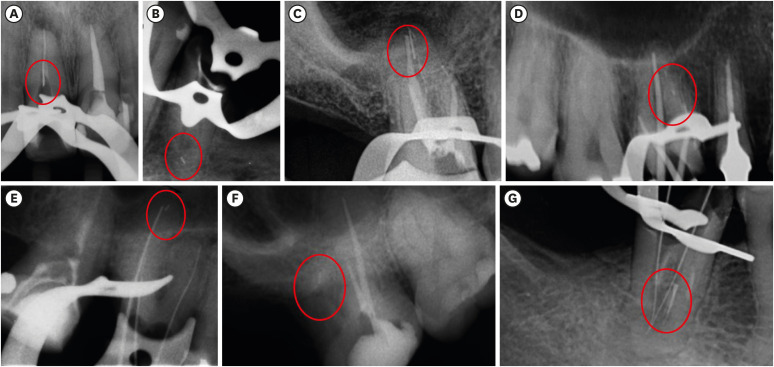
Figure 1 Radiograph images of the 7 Reciproc R25 instruments fractured during root canal retreatments in each tooth and respective root canal. A maxillary central incisor with a fragment of fractured instrument in its middle third (A); a mandibular second premolar with a fragment of fractured instrument in the apical third of its vestibular root canal (B); a maxillary second molar with a fragment of fractured instrument in the apical third of its palatal root canal (C); a maxillary first molar with a fragment of fractured instrument in the apical third of its mesiobuccal root canal (D); a maxillary first molar with a fragment of fractured instrument in the apical third of its palatal root canal (E); a maxillary second molar with a fragment of fractured instrument in the apical third of its distobuccal root canal (F); a mandibular first molar with a fragment of fractured instrument in the middle third of its mesiobuccal root canal (G).
Figure 1
Fracture incidence of Reciproc instruments during root canal retreatment performed by postgraduate students: a cross-sectional retrospective clinical study
Number of total teeth and root canals used in this study
| Variables | Incisors | Canines | Premolars | Molars | ||||
|---|---|---|---|---|---|---|---|---|
| No. of teeth | No. of root canals | No. of teeth | No. of root canals | No. of teeth | No. of root canals | No. of teeth | No. of root canals | |
| Maxillary | 140 | 140 | 26 | 26 | 171 | 342 | 194 | 747 |
| Mandibular | 76 | 76 | 15 | 15 | 115 | 138 | 279 | 1,060 |
Number of fractures in each group of teeth according to the respective tooth and root canal, fracture position, fragment size, and fragment management
| Group of teeth | No. of fractures | Tooth | Root canal | Fracture position | Fragment size | Fragment management |
|---|---|---|---|---|---|---|
| Incisor | 1 | 11 | - | Middle third | 6 mm | Removed |
| Premolar | 1 | 35 | Vestibular | Apical third | 2 mm | NRNB |
| Maxillary molar | 4 | 16 | Palatal | Apical third | 5 mm | NRNB |
| 16 | Mesiobuccal | Apical third | 1 mm | NRNB | ||
| 16 | Palatal | Apical third | 2 mm | NRNB | ||
| 17 | Distobuccal | Apical third | 2 mm | NRNB | ||
| Mandibular molar | 1 | 46 | Mesiobuccal | Middle third | 4 mm | Bypassed |
DB, distobuccal; MB, mesiobuccal; P, palatal. NRNB, neither removed nor bypassed.
Table 1 Number of total teeth and root canals used in this study
Table 2 Number of fractures in each group of teeth according to the respective tooth and root canal, fracture position, fragment size, and fragment management
DB, distobuccal; MB, mesiobuccal; P, palatal. NRNB, neither removed nor bypassed.

