
Articles
- Page Path
- HOME > Restor Dent Endod > Volume 46(4); 2021 > Article
- Research Article Bone repair in defects filled with AH Plus sealer and different concentrations of MTA: a study in rat tibiae
-
Jessica Emanuella Rocha Paz1
 , Priscila Oliveira Costa2, Albert Alexandre Costa Souza2, Ingrid Macedo de Oliveira2, Lucas Fernandes Falcão3, Carlos Alberto Monteiro Falcão2,4, Maria Ângela Area Leão Ferraz2,4, Lucielma Salmito Soares Pinto4
, Priscila Oliveira Costa2, Albert Alexandre Costa Souza2, Ingrid Macedo de Oliveira2, Lucas Fernandes Falcão3, Carlos Alberto Monteiro Falcão2,4, Maria Ângela Area Leão Ferraz2,4, Lucielma Salmito Soares Pinto4 -
Restor Dent Endod 2021;46(4):e48.
DOI: https://doi.org/10.5395/rde.2021.46.e48
Published online: September 2, 2021
1Department of Oral & Maxillofacial Surgery and Periodontology, São Paulo University, School of Dentistry, Ribeirão Preto, SP, Brazil.
2Department of Endodontics, Dental School, Uninovafapi University Center, Teresina, PI, Brazil.
3Department of Endodontics, São Leopoldo Mandic Dental School, Campinas, SP, Brazil.
4Department of Morphology, Health Science Center, State University of Piauí, Teresina, PI, Brazil.
- Correspondence to Lucielma Salmito Soares Pinto, DDS, PhD. Professor, Department of Morphology, Health Science Center, State University of Piauí, Rua Olavo Bilac, 2335, CEP 64001-280, Teresina, PI, Brazil. lucielmasalmito@ccs.uespi.br
• Received: November 10, 2020 • Revised: December 15, 2020 • Accepted: December 16, 2020
Copyright © 2021. The Korean Academy of Conservative Dentistry
This is an Open Access article distributed under the terms of the Creative Commons Attribution Non-Commercial License (https://creativecommons.org/licenses/by-nc/4.0/) which permits unrestricted non-commercial use, distribution, and reproduction in any medium, provided the original work is properly cited.
Abstract
-
Objectives This study aimed to evaluate the effects on bone repair of different concentrations of mineral trioxide aggregate (MTA) added to AH Plus.
-
Materials and Methods Bone tissue reactions were evaluated in 30 rats (Rattus norvegicus) after 7 and 30 days. In the AH + MTA10, AH + MTA20, and AH + MTA30 groups, defects in the tibiae were filled with AH Plus with MTA in proportions of 10%, 20% and 30%, respectively; in the MTA-FILL group, MTA Fillapex was used; and in the control group, no sealer was used. The samples were histologically analyzed to assess bone union and maturation. The Kruskal-Wallis and Mann-Whitney tests were performed for multiple pairwise comparisons (p ≤ 0.05).
-
Results At the 7-day time point, AH + MTA10 was superior to MTA-FILL with respect to bone union, and AH + MTA20 was superior to MTA-FILL with respect to bone maturity (p < 0.05). At the 30-day time point, both the AH + MTA10 and AH + MTA20 experimental sealers were superior not only to MTA-FILL, but also to AH + MTA30 with respect to both parameters (p < 0.05). The results of the AH + MTA10 and AH + MTA20 groups were superior to those of the control group for both parameters and experimental time points (p < 0.05).
-
Conclusions The results suggest the potential benefit of using a combination of these materials in situations requiring bone repair.
INTRODUCTION
Root canal sealers are used to provide a seal between the dentinal walls and the filling material along the entire length of the root canal. Ideally, these cements should have sealing ability, dimensional stability, adequate setting time, insolubility, and biocompatibility, given the risk of material extrusion beyond the apical constriction and direct contact with periapical tissues [1,2,3,4]. Sealers are commonly categorized according to their main chemical constituents: zinc oxide eugenol, calcium hydroxide, glass ionomer, silicone, resin, and bioceramic-based sealers [3,5]. Bioceramics were introduced in endodontics as root repair cements and root canal sealers, and this category includes alumina, zirconia, bioactive glass, glass ceramics, hydroxyapatite, and calcium phosphates. They may be categorized into 2 groups: calcium silicate-based sealers (mineral trioxide aggregate [MTA]-based and non-MTA-based) and calcium phosphate-based sealers [5].
MTA was introduced as a root filling material in the 1990s. It is a powder that forms a hardened cement after it is mixed with water. Its main components are tricalcium silicate, tricalcium aluminate, tricalcium oxide, and silicate oxide [6]. Osteoconductivity is one of the favorable properties of MTA. This property enables the material to stimulate the production of tissue similar to bone and cementum in the periapical region in response to endodontic treatment, thereby providing an effective apical seal [6]. However, its long setting time, unfavorable handling characteristics, and poor flow performance still compromise its use. Therefore, a number of bioactive endodontic cements, the composition of which includes calcium and silicate, have been introduced to the market. It has been claimed that these materials have properties similar to those of MTA, but without its drawbacks [7].
MTA Fillapex is a paste-catalyst MTA containing a resin-based bioceramic sealer, which allows it to be appropriately inserted into the root canal as a conventional endodontic sealer [5]. It is composed of salicylate resin, resin diluent, natural resin, radiopacifying agent, silica nanoparticles, MTA, and pigments. MTA Fillapex is one of the most studied sealers [2,8,9,10]. All in vivo studies have shown an inflammatory reaction in response to the various sealers, independently of type, ranging from slight to severe inflammatory reactions [2]. Nevertheless, most studies have shown that calcium silicate sealers, such as MTA Fillapex, are biocompatible [1]. The ability of MTA Fillapex to facilitate re-establishment of the original bone structure has been shown [2,8].
The epoxy resin-based AH Plus sealer is considered the gold standard for endodontic sealers, owing to its excellent physicochemical properties, such as resistance and dimensional stability [1]. It is also one of the materials that have been most widely assessed in the literature [2]. However, its biological properties, such as possible mutagenicity, cytotoxicity, and an inflammatory response, require further improvement [1,2]. Thus, several studies have tried to increase its biocompatibility by adding materials such as calcium hydroxide or MTA [11,12,13].
In the present study, MTA was added to AH Plus with the ultimate aim of combining the ability of MTA to stimulate hard tissue deposition with the physicochemical properties of AH Plus. Therefore, the purpose was to compare the repair of bone defects filled with different concentrations of MTA added to AH Plus and MTA Fillapex in rat tibiae. The null hypothesis was that there would be no differences among the materials tested.
MATERIALS AND METHODS
The procedures used and the animal care protocol were approved by the Institutional Animal Care and Use Committee of Uninovafapi University Center (approval No. 001/18). Thirty male rats (Rattus norvegicus, Wistar; age, 6 months; weight, up to 300 g) were selected. The animals were placed in plastic cages (40 × 32 × 17 cm), kept in an air-conditioned vivarium (21°C to 25°C) with adequate lighting (12:12 hour light-dark cycle), and received a balanced diet (Nuvilab, Colombo, PR, Brazil) and water ad libitum [14].
The animals' weight was measured and drug doses were adjusted. All animals were anesthetized with intramuscular injections of xylazine hydrochloride solution (10 mg/kg, Ceva Saúde Animal, Paulínia, SP, Brazil) and ketamine (25 mg/kg Dopalen, Ceva Saúde Animal). After confirming the anesthetic effect, trichotomy and disinfection of the areas over the tibiae of the right and left paws with 5% iodopovidone solution, a 3.0-cm incision was made in the skin and muscle in the middle third of the bone until the periosteum was reached [14].
After exposure of the bone tissue, a unicortical defect sufficiently deep to attain the medullary canal (3.0 mm) was made on each tibia, in the region of the largest lateral extent of the middle third of the bone. To do this, a trephine bur 3.3 mm in diameter (Dentsply Sirona, Petrópolis, RJ, Brazil), mounted in an implant contra-angle handpiece (FX 200, Dentflex, Ribeirão Preto, SP, Brazil) was used, driven by an electric motor (D Force 1000, Dentflex), under copious cooling with a sterile physiological solution [14].
Thirty rats (Rattus norvegicus) were divided into 5 groups according to the material used to fill the bone defect. For random allocation, we employed IBM SPSS Statistics 20 software (IBM Brasil, São Paulo, SP, Brazil) to generate a table of random numbers. The 5 groups were as follows: the AH + MTA10 group, which received AH Plus sealer (Dentsply DeTrey GmbH, Konstanz, Germany) and MTA (Angelus, Londrina, PR, Brazil) in a proportion of 10% (w/w); the AH + MTA20 group, which received AH Plus sealer with MTA in a proportion of 20% (w/w); the AH + MTA30 group, which received AH Plus sealer with MTA in a proportion of 30% (w/w); the MTA-FILL group, which received MTA Fillapex sealer (Angelus); and the control group, in which the defect was filled only with the animal's own blood clot. All the materials were manipulated according to the recommendations of their respective manufacturers: AH Plus sealer was used at a ratio of 1:1, MTA Fillapex at a ratio of 1:1, and AH Plus was used together with 10%, 20%, and 30% proportions of MTA calculated using a precision scale; after all weighing, the materials were spatulated on a glass plate until homogeneous consistency [15].
After mixing the cements, they were individually inserted into the bone defects until the defects were completely filled, thereby establishing the experimental groups. Each rat had a different cement randomly placed in the right and left tibiae. In each fifth bone defect, no type of material was inserted. The muscle and skin layers were then sutured with 3-0 silk thread (Shalon Fios Cirúrgicos, São Paulo, SP, Brazil), and the area was cleaned again with a 5% povidone-iodine solution [14].
After 7 and 30 days, the animals were euthanized (15 per period) using a 10% ketamine hydrochloride solution at 0.35 mL/kg (Dopalen, Ceva Saúde Animal). Their tibiae were dissected and fixed in a 10% formaldehyde solution, thus producing the 6 specimens planned for each group per period. After 24 hours of fixation, the specimens were washed in running water for 12 hours and demineralized in a solution of ethylenediaminetetraacetic acid (Merck, Darmstadt, Germany). Subsequently, the specimens were dehydrated in alcohol and hemisectioned in the transverse direction in the central region of the bone defect and embedded in paraffin in the direction of the cut surface. Five-micrometer-thick semi-serial sections were obtained and stained with a hematoxylin-eosin solution (Merck) [14].
The tissue reactions observed in the specimens of the different groups were analyzed using an optical microscope (Olympus, Tokyo, Japan) coupled to a digital camera (Olympus), at magnifications of up to × 400. Three histological sections of each tibia were obtained, for a total of 180 sections.
The 5-level scoring system described by Hedner and Linde [16] was used to assess the healing process, based on the parameters of bone union and maturation (Table 1). A qualified pathologist, blinded to the type of material and period of time elapsed after material implantation, conducted the histological assessments.
Table 1
Histological scoring system described by Hedner and Linde [16] based on the parameters of bone union and bone maturation
The data distribution was analyzed using the Kolmogorov-Smirnov test. Since the observed distribution was non-normal, the values obtained in the study groups were compared using the non-parametric Kruskal-Wallis test, followed by the Mann-Whitney test for multiple pairwise comparisons (p ≤ 0.05). IBM SPSS Statistics version 20 software (IBM Brasil) was used to perform the analyses.
RESULTS
1. AH + MTA10
At 7 days, the histological analyses mainly revealed a small or moderate amount of new bone at the defect rims, thick collagen fiber union, and proliferation and differentiation of osteoprogenitor cells to osteogenic cells in specimens of all groups. In particular, the AH + MTA10 group exhibited a moderate amount of immature bone at the defect rims, with only a small bone defect remaining in most samples. There was evidence of a moderate inflammatory infiltrate, composed mainly of polymorphous and mononuclear cells. Adjacent to the bone defect, residues of dispersed material were observed (Figure 1A). At 30 days, all specimens of different groups presented partial or complete formation of the hard tissue barrier. The AH + MTA10 group presented complete closure of the experimental defect with the formation of a thick cortical bone bridge, morphologically similar to the bone adjacent to the defect. There was a reduction in the intensity of inflammatory infiltrate relative to the 7-day period (Figure 1B).
Figure 1
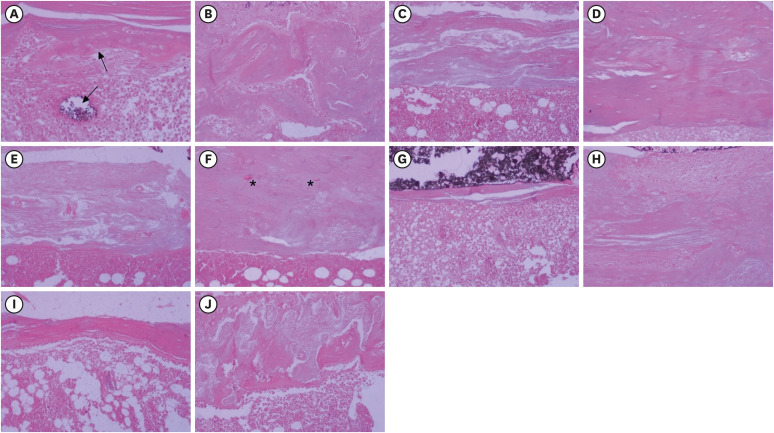
Histological images representative of the bone repair observed after filling experimental defects created in rat tibiae with AH + MTA10 (A, B), AH + MTA20 (C, D), and AH+MTA30 (E, F), MTA Fillapex sealer (G, H), and the control group (I, J). At 7 days, only a small bone defect and immature bone consisting of osteoblasts and bone matrix (upward-pointing arrow) can be seen in the AH + MTA10 group, and residual material is also observed (downward-pointing arrow) (A). Differentiation of immature cells into osteoblasts and the deposition of varying amounts of collagen fibers predominate in the other groups (C, D, G, and I). At 30 days, closure of the experimental defect with the formation of a thick cortical bone bridge, morphologically similar to the bone adjacent to the defect, can be seen in the AH + MTA20 group (D). Mineralized, lamellar and irregular compact bone of variable thickness, and persistent medullary spaces (asterisks) can be seen in the other groups (B, F, H, and J) (hematoxylin and eosin stain; original magnification × 200).
AH + MTA10, AH Plus sealer and mineral trioxide aggregate in proportions of 10%; AH + MTA20, AH Plus sealer and mineral trioxide aggregate in proportions of 20%; AH + MTA30, AH Plus sealer and mineral trioxide aggregate in proportions of 30%.
2. AH + MTA20
The tissue reaction in the AH + MTA20 group was similar to that in the AH + MTA10 group for the different experimental periods, mainly with regard to the presence of inflammatory infiltrate and linear closure of the bone defect. At 7 days, the AH + MTA20 group exhibited a predominantly moderate amount of new bone at the rims, with about two-thirds of the bone defect remaining (Figure 1C). At 30 days, the inflammatory infiltrate was scarce and a large number of osteogenic cells were observed, with the formation of a compact mineralized bridge closing the experimental defect. Complete bone union with compact woven bone was the main finding at this time point (Figure 1D).
3. AH + MTA30
The bone defect repair observed in the AH + MTA30 group at 7 days was morphologically more immature than the previously described groups, consisting mainly of thick collagen fiber union, with proliferation and differentiation of osteoprogenitor cells to osteogenic cells; moreover, there was only a small amount of new bone at the defect rims. Additionally, there was a moderate to intense inflammatory component (Figure 1E). At 30 days, reductions were observed in the inflammatory response and the formation of a compact mineralized bridge, with lamellar bone and a larger amount of osteocytes, but persistent medullary spaces (Figure 1F).
4. MTA-FILL
At 7 days, the results of the MTA-FILL group were very similar to those of the AH + MTA30 group: the defects exhibited thick collagen fiber union, with proliferation and differentiation of osteoprogenitor cells to osteogenic cells, and a small amount of new bone. Numerous congested blood vessels were observed among mononuclear phagocytes engulfing residues of dispersed material (Figure 1G). At 30 days, there was partial formation of a hard tissue barrier, with a larger amount of osteocytes but persistent medullary spaces (Figure 1H).
5. Control
As described previously for the AH + MTA30 and MTA-FILL groups, the control group defects exhibited thick collagen fiber union, with proliferation and differentiation of osteoprogenitor cells to osteogenic cells, and a small amount of new bone at 7 days (Figure 1I). At 30 days, partial formation of a hard tissue barrier was observed, with a larger amount of osteocytes and persistent medullary spaces (Figure 1J).
Data were compared for each time point, as shown in Table 2. At 7 days, the bone union scores of the AH + MTA10 group were higher than those of the other groups (p < 0.05). Additionally, the bone union scores of the AH + MTA20 group were higher than those of the AH + MTA30 and control groups (p < 0.05). The bone maturation scores of the AH + MTA20 group were higher than those of the MTA-FILL group, and those of the AH + MTA10, AH + MTA20, and AH + MTA30 groups were higher than those of the control group (p < 0.05), with a higher concentration of scattered immature bone islands. At 30 days, the bone union and maturation scores of both the AH + MTA10 and AH + MTA20 groups were higher than those of the other groups (p < 0.05), with complete bone union and the formation of compact bone in most specimens.
Table 2
Median bone union and maturation scores of specimens 7 and 30 days after surgery performed to create and fill critical defects in rat tibiae
AH + MTA10, AH + MTA20, and AH + MTA30, AH Plus endodontic sealer (batch No. 294566) and mineral trioxide aggregate (batch No. 37310) in proportions of 10%, 20%, and 30% (w/w), respectively; MTA-FILL, MTA Fillapex endodontic sealer (batch No. 28382); Q1, first quartile (25%); Q3, third quartile (75%).
*Kruskal-Wallis test followed by the Mann-Whitney test (p ≤ 0.05).
DISCUSSION
The AH Plus sealer has been the most studied sealer over the last 2 decades, either as a test sealer or as a reference material. It is considered the gold standard in terms of physicochemical properties; however, its biological properties require further improvement [1,2]. Compared to other resin-containing sealants, AH Plus had the least cytotoxic effects, which makes it a good candidate for combination with materials that add bioactive properties [9,17]. Experiments combining MTA and AH Plus were previously described [13,15,18]. The adhesive strength of AH Plus increased significantly when MTA was added in proportions of 20% and 30%, but was similar to that of the original AH Plus when MTA was added in a proportion of 10% [15]. The addition of MTA to AH Plus in proportions of 20% and 30% did not interfere with the radiopacity of the material, whereas MTA addition in a proportion of 10% significantly reduced radiopacity, even though the levels were still acceptable [18]. Regarding biocompatibility, the combination of 30% AH Plus and 70% MTA after 7 days induced slight to moderate inflammatory response in the subcutaneous tissue of rats, and after 50 days, the materials tested induced an insignificant inflammatory response. The authors concluded that the addition of AH Plus sealer to MTA did not influence its biological behavior [13]. However, the main benefit obtained by combining both materials is the addition of the osteoconductivity of MTA to AH Plus, which has yet to be investigated. Therefore, to the best of our knowledge, the present study was the first to evaluate the reparative capacity of different concentrations of MTA added to AH Plus in bone defects produced in the tibiae of rats.
On the basis of the results obtained, the null hypothesis tested was rejected, as significant differences were observed among the materials that were examined. At the 7-day time point, AH + MTA10 was superior to MTA-FILL with respect to bone union, and AH + MTA20 was superior to MTA-FILL with respect to bone maturity. At the 30-day time point, both the AH + MTA10 and AH + MTA20 experimental sealers were superior not only to MTA-FILL, but also to AH + MTA30, with respect to both parameters. The results of the AH + MTA10 and AH + MTA20 groups were superior to those of the control group regarding both parameters at both experimental time points. Although a higher percentage of MTA added to AH Plus would be expected to produce better results for bone neoformation, it was observed that more advanced stages of osteogenesis were seen in the specimens from the AH + MTA10 and AH + MTA20 groups. It is possible that the physicochemical characteristics of the materials resulting from the combinations of AH Plus with MTA in proportions of 10% and 20% resulted in higher MTA availability and consequently better osteoconductive performance than was found in the control and MTA Fillapex groups. It was observed subjectively that AH + MTA20 had less flow than AH + MTA10 and a longer working time than AH + MTA30. This furnishes evidence that the AH Plus sealer modified by the addition of 20% MTA provided the most favorable conditions for insertion and accommodation of the material into the cavity, but further research is necessary to confirm these findings.
The bioactivity of MTA is related to its ability to promote cell proliferation and migration, as well as tissue mineralization. The main component of MTA is calcium silicate, which is converted into calcium hydroxide following contact with tissue. Calcium hydroxide, in turn, dissociates into calcium and hydroxide ions, and these are continuously released into the surrounding environment [6,7]. When MTA was exposed to synthetic tissue fluid, simulating in vivo conditions, it produced precipitates that were similar to the hydroxyapatite layer. Hydroxyapatite layers, which have low toxicity, are highly biocompatible. This layer might have osteogenic potential because it can release calcium and phosphorus ions, which are involved in bone metabolism [19]. This property of MTA may have been preserved in the tested materials, since bone repair was observed in the present study.
The MTA-FILL and control groups presented similar results. A remaining bone defect was observed in these groups even after 30 days, with a predominance of relatively undifferentiated cells, collagen fibrils, and premature bone. Previous studies have reported the cytotoxicity of MTA Fillapex in contact with mesenchymal stem cells, endothelial cells, fibroblasts, and osteoblasts [9,20,21]. Nonetheless, MTA Fillapex may still be accepted as a cytocompatible sealer due to viability values superior to 70% [21]. It was also reported that after setting, the cytotoxicity of MTA Fillapex decreased and the sealer presented suitable bioactivity to stimulate hydroxyapatite crystal nucleation [22]. Saraiva et al. [23] using a subcutaneous test, observed that MTA Fillapex was associated with fewer inflammatory cells mediated by interleukin-6, suggesting that the immune response is suppressed more rapidly in the MTA-based sealers. In bone studies, MTA Fillapex caused an inflammatory response similar to or more intense than that caused by AH Plus [8,24]. Regardless, both MTA Fillapex and AH Plus facilitated re-establishment of the original bone tissue structure and the inflammatory response decreased over time, meaning that they could be considered biocompatible [8]. Costa et al. [20] observed that MTA Fillapex sealer promoted the formation of a mineralized matrix and partial regeneration of bone defects in an ex vivo model.
An attempt was made to increase the biocompatibility of MTA Fillapex by adding ceramic particles; however, even though a decrease was observed in the acute and chronic inflammatory responses, no formation of mineralized tissue was seen [25]. The toxicity of MTA Fillapex has been attributed to its chemical composition, since the salicylate resin has already been shown to induce apoptosis [9,23]. Additionally, bismuth oxide, used as a radiopacifier in MTA Fillapex, is related to the inhibition of cellular proliferation and induction of the inflammatory response, so it was recently replaced by calcium tungstate in an effort to improve its biological properties [1,17]. With this new composition, cytocompatibility was reported both in a direct contact test and in terms of alkaline phosphatase activity and bioactive potential in subcutaneous tissue, but the authors highlighted the scarcity of studies to compare their data [10,17].
Some limitations of the present study must be considered. First, an animal model was used, so the results cannot be extrapolated directly to humans. Second, the physical and chemical properties of the experimental materials have not been evaluated. However, the bone defect model is considered adequate to identify differences in tissue response to endodontic cements and has been widely adopted [8,11,24,25].
CONCLUSIONS
The present study showed that the osteoconductivity of AH Plus sealer modified by the addition of 10% and 20% MTA was superior to that of all other groups with respect to bone union and maturity at 30 days under the present experimental conditions. The results suggest a probable benefit of using a combination of these materials in situations in which bone repair is required. Nevertheless, additional properties must be further tested in order to validate the potential use of these combinations.
-
Conflict of Interest: No potential conflict of interest relevant to this article was reported.
-
Author Contributions:
Conceptualization: Paz JER, Costa PO, Falcão CAM.
Data curation: Paz JER, Costa PO, Souza AAC, Oliveira IM, Falcão LF.
Formal analysis: Falcão CAM, Ferraz MAAL, Pinto LSS.
Funding acquisition: Paz JER, Costa PO, Falcão CAM.
Investigation: Paz JER, Costa PO, Falcão CAM.
Methodology: Paz JER, Costa PO, Souza AAC, Oliveira IM, Falcão LF, Falcão CAM, Ferraz MAAL, Pinto LSS.
Project administration: Falcão CAM, Ferraz MAAL, Pinto LSS.
Resources: Paz JER, Costa PO, Souza AAC, Oliveira IM, Falcão LF.
Software: Paz JER, Costa PO, Souza AAC, Oliveira IM, Falcão LF.
Supervision: Falcão CAM, Ferraz MAAL, Pinto LSS.
Validation: Paz JER, Costa PO, Falcão CAM.
Visualization: Paz JER, Costa PO, Souza AAC, Oliveira IM, Falcão LF, Falcão CAM, Ferraz MAAL, Pinto LSS.
Writing - original draft: Paz JER, Costa PO, Pinto LSS.
Writing - review & editing: Paz JER, Costa PO, Souza AAC, Oliveira IM, Falcão LF, Falcão CAM, Ferraz MAAL, Pinto LSS.
- 1. Lim M, Jung C, Shin DH, Cho YB, Song M. Calcium silicate-based root canal sealers: a literature review. Restor Dent Endod 2020;45:e35.ArticlePubMedPMCPDF
- 2. Fonseca DA, Paula AB, Marto CM, Coelho A, Paulo S, Martinho JP, Carrilho E, Ferreira MM. Biocompatibility of root canal sealers: a systematic review of in vitro and in vivo studies. Materials (Basel) 2019;12:4113-4117.PubMedPMC
- 3. Al-Haddad A, Che Ab Aziz ZA. Bioceramic-based root canal sealers: a review. Int J Biomater 2016;2016:9753210.ArticlePubMedPMCPDF
- 4. Kaur A, Shah N, Logani A, Mishra N. Biotoxicity of commonly used root canal sealers: a meta-analysis. J Conserv Dent 2015;18:83-88.ArticlePubMedPMC
- 5. Jafari F, Jafari S. Composition and physicochemical properties of calcium silicate based sealers: a review article. J Clin Exp Dent 2017;9:e1249-e1255.ArticlePubMedPMC
- 6. Torabinejad M, Hong CU, McDonald F, Pitt Ford TR. Physical and chemical properties of a new root-end filling material. J Endod 1995;21:349-353.ArticlePubMed
- 7. Torabinejad M, Parirokh M, Dummer PMH. Mineral trioxide aggregate and other bioactive endodontic cements: an updated overview - part II: other clinical applications and complications. Int Endod J 2018;51:284-317.ArticlePubMedPDF
- 8. Assmann E, Böttcher DE, Hoppe CB, Grecca FS, Kopper PM. Evaluation of bone tissue response to a sealer containing mineral trioxide aggregate. J Endod 2015;41:62-66.ArticlePubMed
- 9. Jung S, Sielker S, Hanisch MR, Libricht V, Schäfer E, Dammaschke T. Cytotoxic effects of four different root canal sealers on human osteoblasts. PLoS One 2018;13:e0194467.ArticlePubMedPMC
- 10. Kebudi Benezra M, Schembri Wismayer P, Camilleri J. Interfacial characteristics and cytocompatibility of hydraulic sealer cements. J Endod 2018;44:1007-1017.ArticlePubMed
- 11. Cintra LTA, Benetti F, de Azevedo Queiroz ÍO, Ferreira LL, Massunari L, Bueno CRE, de Oliveira SHP, Gomes-Filho JE. Evaluation of the cytotoxicity and biocompatibility of new resin epoxy-based endodontic sealer containing calcium hydroxide. J Endod 2017;43:2088-2092.ArticlePubMed
- 12. de Oliveira RL, Oliveira Filho RS, Gomes HC, de Franco MF, Enokihara MM, Duarte MA. Influence of calcium hydroxide addition to AH Plus sealer on its biocompatibility. Oral Surg Oral Med Oral Pathol Oral Radiol Endod 2010;109:e50-e54.ArticlePubMed
- 13. Falcão LF, Silva PR, Falcão DF, Pinto LSS, Falcão CAM. Evaluation of the biocompatibility of AH Plus sealer associated to Portland cement or MTA. Subcutaneous study in rats. Rev Interd 2018;11:1-11.
- 14. Garcia LF, Huck C, Scardueli CR, de Souza Costa CA. Repair of bone defects filled with new calcium aluminate cement (EndoBinder). J Endod 2015;41:864-870.ArticlePubMed
- 15. Falcão CA, Lima EM, Júnior JDM, Freitas SA, Veras ESL, Moura LK, Falcão LF. Plus adhesiveness assessment associated with mineral trioxide aggregate in different proportions (push-out test). J Contemp Dent Pract 2018;19:1444-1447.PubMed
- 16. Hedner E, Linde A. Efficacy of bone morphogenetic protein (BMP) with osteopromotive membranes--an experimental study in rat mandibular defects. Eur J Oral Sci 1995;103:236-241.ArticlePubMed
- 17. Delfino MM, Guerreiro-Tanomaru JM, Tanomaru-Filho M, Sasso-Cerri E, Cerri PS. Immunoinflammatory response and bioactive potential of GuttaFlow bioseal and MTA Fillapex in the rat subcutaneous tissue. Sci Rep 2020;10:7173.ArticlePubMedPMCPDF
- 18. Sousa Filho JL, Moreira KMS, Amaral GCLS, Fortunato CFP, Dias IVA, Falcão CAM. Radiopacity of AH Plus endodontic sealer plus MTA and Portland cement. Dental Press Endod 2018;8:18-21.Article
- 19. Sarkar NK, Caicedo R, Ritwik P, Moiseyeva R, Kawashima I. Physicochemical basis of the biologic properties of mineral trioxide aggregate. J Endod 2005;31:97-100.ArticlePubMed
- 20. Costa F, Sousa Gomes P, Fernandes MH. Osteogenic and angiogenic response to calcium silicate–based endodontic sealers. J Endod 2016;42:113-119.ArticlePubMed
- 21. Mestieri LB, Zaccara IM, Pinheiro LS, Barletta FB, Kopper PMP, Grecca FS. Cytocompatibility and cell proliferation evaluation of calcium phosphate-based root canal sealers. Restor Dent Endod 2019;45:e2.ArticlePubMedPMCPDF
- 22. Salles LP, Gomes-Cornélio AL, Guimarães FC, Herrera BS, Bao SN, Rossa-Junior C, Guerreiro-Tanomaru JM, Tanomaru-Filho M. Mineral trioxide aggregate-based endodontic sealer stimulates hydroxyapatite nucleation in human osteoblast-like cell culture. J Endod 2012;38:971-976.ArticlePubMed
- 23. Saraiva JA, da Fonseca TS, da Silva GF, Sasso-Cerri E, Guerreiro-Tanomaru JM, Tanomaru-Filho M, Cerri PS. Reduced interleukin-6 immunoexpression and birefringent collagen formation indicate that MTA Plus and MTA Fillapex are biocompatible. Biomed Mater 2018;13:035002.ArticlePubMedPDF
- 24. Scelza MZ, Campos CA, Scelza P, Adeodato CS, Barbosa IB, de Noronha F, Montalli V, Napimoga M, de Araújo VC, Alves GG. Evaluation of inflammatory response to endodontic sealers in a bone defect animal model. J Contemp Dent Pract 2016;17:536-541.ArticlePubMed
- 25. Almeida LH, Gomes APN, Gastmann AH, Pola NM, Moraes RR, Morgental RD, Cava SS, Felix AOC, Pappen FG. Bone tissue response to an MTA-based endodontic sealer, and the effect of the addition of calcium aluminate and silver particles. Int Endod J 2019;52:1446-1456.PubMed
REFERENCES
Tables & Figures
REFERENCES
Citations
Citations to this article as recorded by 
- Bone Healing Response to Different Concentrations of Nano-Hydroxyapatite Incorporated into Mineral Trioxide Aggregate and Bioceramic Sealers
Arkhawan Ali Abdulhaq, Chenar Anwar Mohammad, Bassam Karem Amin
Polymers.2026; 18(14): 1743. CrossRef - Analysis of the cytotoxicity and bioactivity of CeraSeal, BioRoot™ and AH Plus® sealers in pre-osteoblast lineage cells
Luciano Aparecido de Almeida-Junior, Giuliana de Campos Chaves Lamarque, Henry Herrera, Maya Fernanda Manfrin Arnez, Francine Lorencetti-Silva, Raquel Assed Bezerra Silva, Léa Assed Bezerra Silva, Francisco Wanderley Garcia Paula-Silva
BMC Oral Health.2024;[Epub] CrossRef - A Review of the research methods and progress of biocompatibility evaluation of root canal sealers
Xiliang Yang, Tianxia Zheng, Nuoya Yang, Zihan Yin, Wuliang Wang, Yuhong Bai
Australian Endodontic Journal.2023; 49(S1): 508. CrossRef - Effect of Vitapex Combined with AH-Plus Paste on Inflammation in Middle-Aged and Elderly Patients with Periodontal-Endodontic Disease
Rong Hu, Fulan Zhang, Xiangyu Guo, Youren Jing, Xiaowan Lin, Liping Tian, Min Tang
Computational and Mathematical Methods in Medicine.2022; 2022: 1. CrossRef
 ePub Link
ePub Link Cite
CiteBone repair in defects filled with AH Plus sealer and different concentrations of MTA: a study in rat tibiae
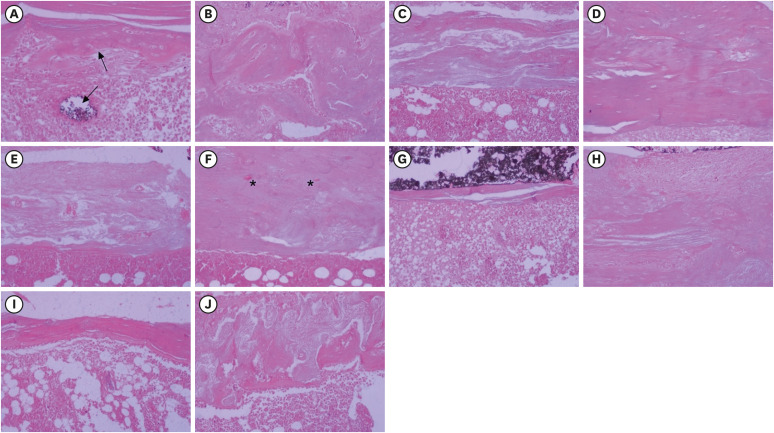
Figure 1 Histological images representative of the bone repair observed after filling experimental defects created in rat tibiae with AH + MTA10 (A, B), AH + MTA20 (C, D), and AH+MTA30 (E, F), MTA Fillapex sealer (G, H), and the control group (I, J). At 7 days, only a small bone defect and immature bone consisting of osteoblasts and bone matrix (upward-pointing arrow) can be seen in the AH + MTA10 group, and residual material is also observed (downward-pointing arrow) (A). Differentiation of immature cells into osteoblasts and the deposition of varying amounts of collagen fibers predominate in the other groups (C, D, G, and I). At 30 days, closure of the experimental defect with the formation of a thick cortical bone bridge, morphologically similar to the bone adjacent to the defect, can be seen in the AH + MTA20 group (D). Mineralized, lamellar and irregular compact bone of variable thickness, and persistent medullary spaces (asterisks) can be seen in the other groups (B, F, H, and J) (hematoxylin and eosin stain; original magnification × 200).AH + MTA10, AH Plus sealer and mineral trioxide aggregate in proportions of 10%; AH + MTA20, AH Plus sealer and mineral trioxide aggregate in proportions of 20%; AH + MTA30, AH Plus sealer and mineral trioxide aggregate in proportions of 30%.
Figure 1
Bone repair in defects filled with AH Plus sealer and different concentrations of MTA: a study in rat tibiae
Histological scoring system described by Hedner and Linde [16] based on the parameters of bone union and bone maturation
| Score | Parameters | |
|---|---|---|
| Bone union | ||
| 0 | No signs of newly formed bone. | |
| 1 | Small amount of new bone at the defect rims. | |
| 2 | Moderate amount of new bone at the rims; two-thirds of the defect remains. | |
| 3 | Profuse new bone formation; one-third of the defect remains. | |
| 4 | A minor rest defect remains. | |
| 5 | Complete bone union. | |
| Bone maturity | ||
| 0 | No signs of bone union. | |
| 1 | Cellular bone, consisting of relatively undifferentiated cells and thin collagen fibrils. | |
| 2 | Thick collagen fiber union. Proliferation and differentiation of osteoprogenitor cells to osteogenic cells. | |
| 3 | Scattered islands of premature bone. | |
| 4 | Branching and anastomosing spicules of premature bone organized in a heterogeneous pattern. | |
| 5 | Compact woven bone. | |
Median bone union and maturation scores of specimens 7 and 30 days after surgery performed to create and fill critical defects in rat tibiae
| Variables | 7 days | 30 days | |||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Bone union | Bone maturity | Bone union | Bone maturity | ||||||||||
| Q1 | Median | Q3 | Q1 | Median | Q3 | Q1 | Median | Q3 | Q1 | Median | Q3 | ||
| Study group | |||||||||||||
| AH + MTA10 | 3.00 | 4.00 | 5.00 | 3.00 | 3.00 | 3.00 | 4.00 | 5.00 | 5.00 | 4.00 | 5.00 | 5.00 | |
| AH + MTA20 | 2.00 | 2.00 | 3.00 | 2.00 | 3.00 | 4.00 | 5.00 | 5.00 | 5.00 | 5.00 | 5.00 | 5.00 | |
| AH + MTA30 | 1.00 | 1.00 | 2.00 | 1.00 | 2.00 | 2.00 | 5.00 | 5.00 | 5.00 | 2.00 | 4.00 | 5.00 | |
| MTA-FILL | 1.00 | 2.00 | 2.00 | 1.00 | 2.00 | 3.00 | 3.00 | 3.00 | 5.00 | 2.00 | 3.00 | 4.00 | |
| Control | 1.00 | 1.00 | 2.00 | 1.00 | 1.00 | 2.00 | 3.00 | 4.00 | 4.00 | 2.00 | 3.00 | 3.00 | |
| Multiple comparisons ( | |||||||||||||
| AH + MTA10 × AH + MTA20 | 0.010* | 0.164 | 0.722 | 0.446 | |||||||||
| AH + MTA10 × AH + MTA30 | < 0.001* | 0.489 | < 0.001* | 0.023* | |||||||||
| AH + MTA10 × MTA-FILL | < 0.001* | 0.070 | 0.011* | 0.002* | |||||||||
| AH + MTA10 × Control | < 0.001* | 0.007* | < 0.001* | < 0.001* | |||||||||
| AH + MTA20 × AH + MTA30 | 0.006* | 0.789 | < 0.001* | 0.007* | |||||||||
| AH + MTA20 × MTA-FILL | 0.084 | 0.003* | 0.040* | 0.001* | |||||||||
| AH + MTA20 × Control | 0.002* | < 0.001* | < 0.001* | < 0.001* | |||||||||
| AH + MTA30 × MTA-FILL | 0.264 | 0.071 | 0.196 | 0.913 | |||||||||
| AH + MTA30 × Control | 0.608 | 0.006* | 0.193 | 0.294 | |||||||||
| MTA-FILL × Control | 0.101 | 0.675 | 0.054 | 0.216 | |||||||||
AH + MTA10, AH + MTA20, and AH + MTA30, AH Plus endodontic sealer (batch No. 294566) and mineral trioxide aggregate (batch No. 37310) in proportions of 10%, 20%, and 30% (w/w), respectively; MTA-FILL, MTA Fillapex endodontic sealer (batch No. 28382); Q1, first quartile (25%); Q3, third quartile (75%).
*Kruskal-Wallis test followed by the Mann-Whitney test (
Table 1 Histological scoring system described by Hedner and Linde [16] based on the parameters of bone union and bone maturation
Table 2 Median bone union and maturation scores of specimens 7 and 30 days after surgery performed to create and fill critical defects in rat tibiae
AH + MTA10, AH + MTA20, and AH + MTA30, AH Plus endodontic sealer (batch No. 294566) and mineral trioxide aggregate (batch No. 37310) in proportions of 10%, 20%, and 30% (w/w), respectively; MTA-FILL, MTA Fillapex endodontic sealer (batch No. 28382); Q1, first quartile (25%); Q3, third quartile (75%).
*Kruskal-Wallis test followed by the Mann-Whitney test (

