
Articles
- Page Path
- HOME > Restor Dent Endod > Volume 46(3); 2021 > Article
- Research Article YouTube as a source of information about pulpotomy and pulp capping: a cross sectional reliability analysis
-
Konstantinos Kodonas1
 , Anastasia Fardi2
, Anastasia Fardi2 -
Restor Dent Endod 2021;46(3):e40.
DOI: https://doi.org/10.5395/rde.2021.46.e40
Published online: July 6, 2021
1Department of Endodontology, School of Dentistry, Aristotle University of Thessaloniki, Thessaloniki, Greece.
2Department of Dentoalveolar Surgery, Surgical Implantology & Radiology, School of Dentistry, Aristotle University of Thessaloniki, Thessaloniki, Greece.
- Correspondence to Kodonas Konstantinos, DDS, MSc, PhD. Contract academic stuff, Department of Endodontology, School of Dentistry, Aristotle University of Thessaloniki, Thessaloniki 54124, Greece. kkodonas@gmail.com
• Received: March 10, 2021 • Revised: May 3, 2021 • Accepted: May 6, 2021
Copyright © 2021. The Korean Academy of Conservative Dentistry
This is an Open Access article distributed under the terms of the Creative Commons Attribution Non-Commercial License (https://creativecommons.org/licenses/by-nc/4.0/) which permits unrestricted non-commercial use, distribution, and reproduction in any medium, provided the original work is properly cited.
Abstract
-
Objectives The purpose of this study was to critically evaluate the quality, reliability and educational content of the information of vital pulp treatment videos available on YouTube.
-
Materials and Methods The keywords “pulpotomy” and “pulp capping” were searched on YouTube on 5th July 2020, until 60 English language videos of each search term with a duration shorter than 15 minutes were acquired. Video characteristics were recorded and Video Power Index (VPI) was calculated. Reliability and educational quality of videos were evaluated using the Modified DISCERN score, the Journal of American Medical Association (JAMA) benchmark criteria and Global Quality Scores (GQS). Videos were categorized by uploading source.
-
Results Regarding pulpotomy, 31.7% of the videos were uploaded by specialists and 68.3% were directed by non-specialists. In the case of pulp capping, the corresponding percentages were 45% and 55%, respectively. Videos uploaded by specialists had significantly higher modified DISCERN, JAMA and GQS scores compared to those uploaded by non-specialists. Endodontists tended to have the highest reliability and VPI scores.
-
Conclusions YouTube videos on vital pulp treatment contain low educational quality or incomplete information. Low popularity of dental pulp capping and pulpotomy videos may be attributed to the specialized nature of these procedures. As YouTube represents an important source for patient information about different health topics, reliable informative videos should be uploaded by specialized dental professionals.
INTRODUCTION
Scientific innovations have increased rapidly over the past years in dentistry. New technologies diffuse into the scientific community in order to improve the quality and experience of dentistry for both patients and clinicians. So far it has been documented that the adoption, non-adoption, or rejection of innovation is affected by specific diffusion factors, including communication channels, time, and the social system [1,2]. Vital pulp therapy includes treatment procedures like pulpotomy or pulp capping, aiming to preserve and maintain normal function of the dentin pulp complex. From the late 50s till today there are more than one thousand studies published regarding this subject. New clinical applications rapidly evolving from being procedure-oriented to biologically evidence-based procedures have been most recently utilized. However, the diffusion pathways of this knowledge to the scientific community still remain unclear.
YouTube has been rated as the number one site for academic and educational purposes [3,4,5]. Innovation spreading through this social media application may be attributed to the easily cost-free educational material, including lessons and PowerPoint presentations from authoritative organizations, universities, dental specialists and opinion leaders or even the preference for video, as an instructive tool, by dental students or even professionals [6]. However, YouTube is not only used by dentists. The ease of access that the internet provides enables everyone in the world’s population to reach health information literacy. Surveys demonstrated that more than 70% of internet users accessed health information online and the number of patients seeking answers about the management of their chronic illnesses in internet-based resources increases on a daily basis [7,8,9].
As the content of YouTube videos is not subjected to any formal peer review process, the evaluation of the scientific validity of the provided information seems imperative. Their educational quality has been widely investigated in a number of different dental and medical disciplines and has been ranging from beneficial to deceptive. The provided information proved to be miscellaneous and concerns about their reliability, accuracy and educational quality have been outlined [10,11,12,13]. As far as the authors are aware, there has been no study assessing the role of YouTube as a source of information on vital pulp therapy. Thus, the aim of this study was to critically evaluate the quality, reliability and educational content of the information of videos regarding pulpotomy and pulp capping, available on YouTube. The research hypothesis was that related videos contain low educational quality or incomplete information.
MATERIALS AND METHODS
The most widely used search terms for pulpotomy and pulp capping were identified using Google Trends, setting the search parameters to the past decade and as “Worldwide,” “YouTube” search. Using Google Chrome as a web browser with cleared cache and deleted cookies, a search was performed on YouTube database on 5 July 2020 with the keywords “pulpotomy” and “pulp capping.” Results were sorted “by relevance” as the default filter for searches.
Inclusion criteria consisted of English language, acceptable audio and visual quality videos. Non-English language videos, irrelevant to pulpotomy or pulp capping information, lasting longer than 15 minutes as long as duplicates were excluded (Table 1). Both researchers scrutinized video contents in the ascending page order until 60 relevant to each search term videos were collected. Finally, they were saved in a YouTube playlist for the subsequent evaluation.
Table 1
Inclusion and exclusion criteria
| Inclusion | Exclusion |
|---|---|
| English language | Non-English language |
| Acceptable audio & visual quality | Irrelevant to pulpotomy or pulp capping |
| Duration longer than 15 min | |
| Duplicates |
Each video was assessed for the following characteristics: video duration, number of views, viewer ratings (likes and dislikes) and days since upload date. Source of videos was categorized into one of 8 groups, according to YouTube channel: 1) dentist, 2) endodontist, 3) pediatric dentist, 4) dental material specialist, 5) institution (university or private), 6) dental manufacturing company, 7) blogger, and 8) independent user. According to the provided affiliation on YouTube videos, sources were also divided into 2 groups; (a) specialists and (b) non-specialists.
The evaluation of the video contents and features was performed by one endodontist (K.K.). Twenty percent of videos were re-evaluated one month later by the same reviewer. Video reliability was assessed using both the modified DISCERN index and the Journal of American Medical Association (JAMA) benchmark criteria [13,14,15,16]. According to the modified DISCERN index, each point is allocated for clarity, reliable source of information, lack of bias, reference supplementation and mention of uncertainty for a maximum possible score of 5 points, indicating the highest reliability of a particular video (Table 2). In the same way, the JAMA criteria (authorship, attribution, disclosure, and currency) collectively evaluate the reliability of online health information (Table 3). More specifically, an observer assigns 1 point for each criterion present in a video for a total score ranging from 0 to 4, with 4 indicating the highest source accuracy and reliability.
Table 2
Information reliability of videos according to modified DISCERN index
Table 3
Journal of American Medical Association benchmark criteria
The overall quality of the video educational content was also assessed using the 5-point Global Quality Score (GQS), with a maximum score of 5, indicating great reliability and high educational quality. This evaluation tool, although non-validated, has been commonly used for the assessment of the content quality of online resources as it rates the quality and usefulness of online resources (Table 4) [14,15]. Finally, video popularity was calculated using the Video Power Index (VPI), as follows: [(view ratio × like ratio/100], where view ratio = views/days and like ratio = [(likes × 100)/(likes + dislikes)] [13,15].
Table 4
The GQS criteria
SPSS Statistics software (version 20.0; SPSS Inc., Chicago, IL, USA) was used for the analysis of data. Descriptive statistics (mean, standard deviation, frequency, percentage) were used to evaluate continuous variables (duration, days since video upload, number of views, likes, dislikes and VPI). Categorical variables were expressed as frequency (n) and percentage (%). The Kolmogorov-Smirnov test was used to analyze the normality of quantitative data. Mann-Whitney U test for 2-group comparisons was used for non-normally distributed continuous variables.
The degree of intra-observer agreement was calculated using Cohen's kappa coefficient. According to previously published data values in excess of 0.8 represent ‘excellent’ agreement; between 0.6 and 0.8 are ‘substantial’; between 0.4 and 0.6 are ‘moderate’ and less than 0.4 are ‘poor.’ Statistical significance was set at p < 0.05.
RESULTS
A total number of 167 videos were screened in order to obtain 120 acceptable videos (60 for each term), after applying the exclusion criteria. In detail, 27 videos were excluded because of irrelevant content, 17 were omitted based on video length duration, while there were 10 videos in non-English language and 3 duplicates. The descriptive data of the pulpotomy and pulp capping-related video characteristics, including mean numbers and standard deviations of duration in seconds, numbers of views, likes, dislikes, days since upload, VPI and mean values of reliability scores are presented in Table 5. According to Cohens’ Kappa statistics, the interrater reliability between the 2 evaluation times was 0.653 for pulpotomy and 0.703 for pulp capping videos.
Table 5
Video characteristics and reliability scores of the included pulpotomy and pulp capping YouTube videos
Regarding pulpotomy videos, upload dates extended from November 10, 2008, to June 26, 2020. The total duration of all pulpotomy videos was 15.517 seconds with a mean individual duration of 259 seconds (Table 5). Eighty-eight percent of the videos had modified DISCERN score less than 3. There were only 2 videos with a perfect modified DISCERN score of 5. Most of the videos did not mention additional sources of patient information (91.6%) or areas of uncertainty (83%). Considering JAMA benchmark, only 11.67% scored 3, confirming the reporting low quality of the videos. JAMA benchmarks 2 and 3 criteria, were only answered in 10% (n = 6) and 3.3% (n = 2) of videos, respectively. Regarding GQS results, most of the videos (85%) were classified as poor or generally poor in educational quality, 10% were rated as having moderate quality and only 5% were scored as presenting good information content.
The majority of all included pulpotomy videos were delivered by dentists (n = 19), followed by endodontists (n = 10) and independent users (n = 9). Other sources, pediatric dentists and institutions, accounted for 8 videos each, whereas health companies for commercial purposes and blogs were responsible for uploading 3 videos, each. Figure 1 presents average reliability scores for each uploading video source. Endodontists received the highest scores in all 4 indexes, followed by pediatric dentists. When video uploaders were divided into 2 main groups; 31.7% of the videos were uploaded by specialists and 68.3% were directed by non-specialists. Comparison of the video parameters among the videos uploaded from specialized and non-specialized individuals in pulpotomy is shown in Table 6. The videos uploaded by specialists were significantly longer (322 seconds) in duration than the non-specialists' videos (210 sec) (p < 0.05) and similarly they received significantly higher mean values of likes (156.7 vs. 101.4) (p < 0.05). There were no significant differences in terms of views, dislikes and days since upload between the 2 different sources. Accordingly, the mean modified DISCERN, JAMA and GQS scores were statistically significantly higher in the specialized compared to the non-specialized group (p = 0.001). Regarding the mean VPI values, there was no statistically significant difference between the 2 groups.
Figure 1
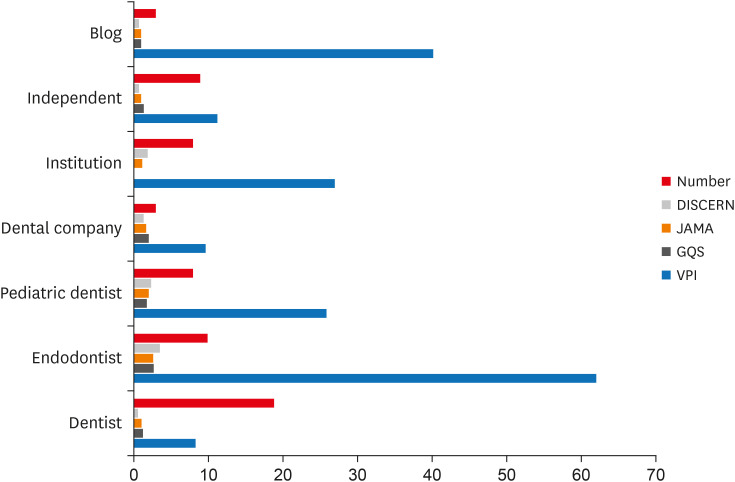
Average reliability scores for pulpotomy videos per video source variables.
JAMA, Journal of American Medical Association; GQS, Global Quality Score; VPI, Video Power Index.
Table 6
Video characteristics and reliability scores of the included pulpotomy and pulp capping YouTube videos among specialists and non-specialists
Concerning the pulp capping-related YouTube videos, upload dates extended from June 16, 2009, to May 5, 2020. YouTube characteristics including duration, numbers of views, likes, dislikes, VPI and other scoring indexes are shown in Table 5. Only 16.7% of the videos had a modified DISCERN score of 4, while none of them achieved a perfect modified DISCERN score. More specifically, 83.3% of the videos had modified DISCERN score of less than 3. Most of the videos did not mention additional sources for patient information (96.7%) and areas of uncertainty (78.3%). Considering JAMA benchmark, only 11.67% scored 3, ascertaining the reporting low quality of the videos. Regarding issues of attribution and disclosure principles, JAMA benchmarks criteria 2 and 3 received full scores only in 3 and 5 out of 60 videos, respectively. According to GQS results, 88% of the videos had poor or generally poor educational quality, while the rest 11.7% was scored as containing moderate or good information content.
The most common pulp capping video sources were classified as dentists (n = 21), followed by endodontists (n = 11) and health companies (n = 9) (Figure 2). Dental material specialists accounted for 7 pulp capping videos and achieved the highest mean DISCERN values. Endodontists scored the highest JAMA, GQS and VPI scores. When video uploading sources were divided into 2 main groups; 45% of the videos were uploaded by specialized individuals and 55% by non-specialists. Specialists uploaded significantly higher video duration (444 sec) than non-specialists (252.3 sec) (p < 0.05). Likewise, there was a significant difference in the number of views (p < 0.05) and number of likes (p < 0.001) between the 2 groups. The rest of the parameters did not show a significant difference (p > 0.05). Furthermore, modified DISCERN, JAMA, GQS score and VPI values were statistically significantly higher in videos delivered by specialists than those of the non-specialist sources (for all, p < 0.05) (Table 6).
Figure 2
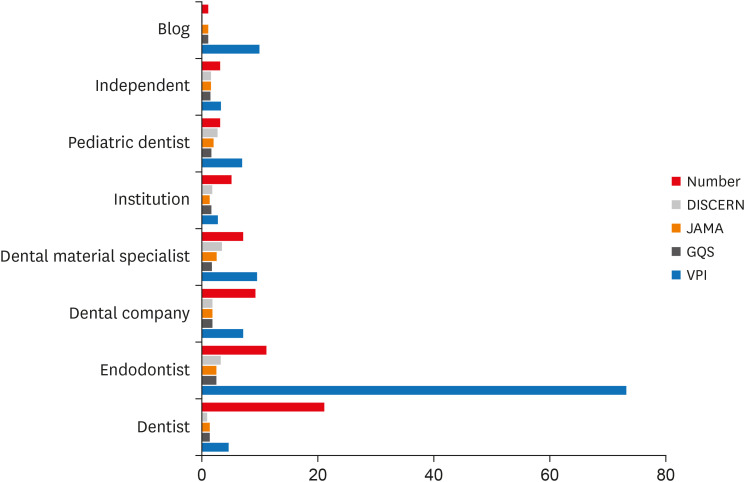
Average reliability scores for pulp capping videos per video source variables.
JAMA, Journal of American Medical Association; GQS, Global Quality Score; VPI, Video Power Index.
In the current study, when video characteristics, DISCERN, JAMA and GQS scores of pulpotomy and pulp capping YouTube videos were compared, only the number of views was found to be significantly higher in pulpotomy contents (Table 5). A comparison of the video parameters, among the pulpotomy and pulp-related videos, is displayed in Table 5. No other statistically significant difference was recorded, when the characteristics, subscales and scores of pulpotomy and pulp capping-related YouTube videos were compared (p > 0.05).
As a feature of YouTube, the upload dates and uploaders are indicated for all videos (Table 7). Consequently, JAMA benchmarks 4 received full points. However, JAMA benchmarks 2 and 3, regarding included information for references and sources of content or website ownership and disclosure principles received very low scores (in total 7.5% and 5.83%, respectively). Equally, according to the modified DISCERN index, question 4, which addresses reference supplementation, scored lower (5.8%) than all other questions, followed by question 5 regarding the mention of uncertainty areas (19.2%). In total, none of the videos found meeting all JAMA benchmark criteria or scored as achieving excellent educational quality in GQS tool.
Table 7
JAMA benchmarks and modified DISCERN questions, number and percentage of vital pulp treatment YouTube videos
DISCUSSION
One of the most widely used internet sources is YouTube, originally created in 2005 and now operates as one of Google's subsidiaries. It is the second most-visited website that allows users to watch, rate, like or report, share, comment on videos, upload their own videos and subscribe to other users. Given its easy accessibility and user-friendly interface, its popularity has been exponential daily. It has been documented that it exceeds 1.5 billion views per day with 1 new video being uploaded every minute and an average user spending at least 40 minutes daily on the site [17].
The number of patients seeking information about treatment choices, dental procedures and outcomes on internet websites and YouTube increases daily. Taking into account the high demands of patients for the maintenance of their teeth, a vast majority of them performs an online search in order to be better informed about their disease and treatment [9]. However, the validity and veracity of the provided information in the YouTube videos have been questioned because of the inability to validate the accuracy of the uploaded videos [10]. Additionally, the lack of minimal guidelines regulating the content of the uploaded material along with the increased use of posting anecdotal information on YouTube disputes the trustworthiness of this information source and increases the risk of disseminating inaccurate or even incomplete information [11]. As a result, the content of YouTube videos for the acquisition of health information has been investigated in different disciplines in the dental literature, including implants, dental avulsion injuries, burning mouth syndrome, oral cancer and root canal treatment [12,18,19,20,21].
The purpose of this study was to evaluate the quality of the information provided on pulpotomy and pulp capping videos on a massive online, media-sharing platform. The use of multiple assessment tools is recommended to achieve more objective results, as JAMA criteria essentially evaluate the reliability of the videos, the modified DISCERN instrument evaluates simultaneously the quality, accuracy and reliability of the videos’ content, while GQS instrument assesses the educational quality of the video. The research hypothesis was that YouTube videos on pulpotomy and pulp capping contain low educational quality or incomplete information.
In our study, average scores in pulpotomy-related videos using mean modified DISCERN, JAMAS and GQS values were 1.53/5.00, 1.47/4.00 and 1.63/5.00, reflecting a lack of accurate and reliable information provided. Considering the same instruments for pulp capping YouTube videos, the mean values were also low and calculated as 1.77/5.00, 1.65/4.00 and 1.70/5.00, respectively, a fact indicating poor quality and reliability of video information. The results verify our research hypothesis for both pulpotomy and pulp capping videos.
Interestingly, modified DISCERN, JAMA and GQS scores were significantly higher in both, pulpotomy and pulp capping videos uploaded by specialists compared to those uploaded by non-specialists. This is in accordance with previously published data indicating that videos posted on YouTube regarding root canal treatment by dental professionals were significantly more complete than videos posted by laypeople [12]. Contradictory results were reported in a study by Gas et al. [22] evaluating the quality of YouTube videos related to botulinum toxin injections for bruxism treatment; they stated that the uploading source did not affect the quality of information.
In this study, the highest value of VPI was recorded in the case of pulpotomy and pulp capping videos uploaded from endodontists (62.7 & 73). This might result from the reference of patients to endodontists for vital pulp treatment procedures. Excluding the videos uploaded from endodontists, the total average VPI of the remaining videos was very low, indicative of the specialized nature of these dental procedures and much lower than that of other kinds of surgical videos on YouTube. These results emphasize the fact that the information provided by different endodontist pioneers around the world is an invaluable supplement to understand the aims, procedure and treatment outcome of specialized dental procedures and might reveal the tendency of patients to look for a second opinion for their treatment decision in YouTube videos, using relative keywords.
An interesting statistically significant difference was recorded in total VPI score, between the specialists, including all categories of specialization, and non-specialist groups in the case of pulp capping videos. This finding might, also, suggest that video popularity, expressed by views and ratings on the internet, is influenced by the uploading source. However, contradictory results have recently been reported by Radonjic et al. [13] who evaluated the quality of abdominal aortic aneurysms videos on YouTube. They attributed the conflictingly high popularity of educational videos delivered by non-experts to the attraction of views by the user-friendly and visually appealing media, regardless of their actual accuracy and completeness of content therein.
In the current study, apart from the number of video views, there were no statistically significant differences between pulpotomy and pulp capping-related YouTube videos for any of the recorded video data characteristics, subscales and scores. The number of views was found to be significantly higher in pulpotomy contents, probably because of the applicability of this procedure to deciduous teeth in pediatric dentistry and the specialized nature of the pulp capping treatment for young permanent teeth with open apices that are usually referred to experts. In general, it has been documented that vital pulp treatment procedures for the fully developed permanent teeth are less popular and root canal treatment is preferable among dentists, a fact that may be reflected by the lower number of views regarding direct pulp cap videos [23,24]. Regarding patients, low popularity of dental pulp capping videos may be attributed to the specialized nature of these procedures.
Most videos featured health professional sources of information. The majority of videos originated from sources of information like dentists, endodontists, pediatric dentists or dental material specialists, health companies and institutions, while patient sources through individuals that had experienced treatment themselves were under-represented amongst the top 120 videos. Since there is no review system for the contents uploaded to social media platforms, people seeking health information should be advised to be consulted by YouTube contents uploaded by dental specialists. Moreover, healthcare information available on YouTube should be supported by interventions that enable consumers to critically assimilate the information posted with more authoritative information sources [10].
This is significantly important if such material is used for educational purposes. Dental students might search YouTube for a clinical demonstration of a certain procedure and consider it as educational material. If this material is not uploaded by professionals it might include much incomplete or even misleading information which will affect the learning outcome for those students. Therefore, it is also the responsibility of undergraduate and postgraduate dental educators to shift the attention of their students to the possible incorrect and misleading content of some YouTube videos and instruct them to the correct sources.
As YouTube video contents increase on a daily basis, measurement and evaluation of the provided information quality have never been more important. Besides the great variability in source and content, the information offered on YouTube regarding vital pulp treatment procedures was proved to be incomplete, verifying the research hypothesis of this study. The low reliability & low educational quality, reflected by modified DISCERN, JAMAS and GQS scores, indicated the viability of YouTube videos as an incomplete source of information for patients, which is in accordance with previous findings of poor quality and insufficient or missing information associated with YouTube content as an information source for healthcare patients [10]. So, regarding the potential of YouTube for the patients’ information, it is generally considered of low quality. Nonetheless, by isolating the videos uploaded by specialists all the reviewed scores significantly increase, a fact highlighting the importance of scrutinizing the uploading sources' reliability. As long as YouTube is an online platform where anyone may upload videos, it is strongly recommended for the patients or people using YouTube as an informational tool to identify and critically evaluate the uploading source.
YouTube videos have been evaluated for smile, wisdom tooth surgical removal, dental implants, dental avulsion injuries, root canal treatment, orthognathic surgery, orthodontics, burning mouth syndrome and mouth (oral) cancer [12,16,18,19,20,21,25,26,27,28]. The majority of these research papers recommended avoidance of this source for educating patients about dental diseases and treatment options. Regarding endodontics, Nason et al. [12] highlighted the need for endodontic professionals to play an active role in directing patients towards alternative high-quality information sources. On the contrary, conflicting results have arisen in the case of systemic lupus erythematosus and accelerated orthodontic treatment. In spite of the considerable heterogeneity in the quality of available information, the majority of the studies concluded that the quality of the information provided in YouTube videos is ‘poor.’
As long as YouTube offers healthcare professionals the opportunity to disseminate correct and complete health information, policymakers should consider screening and removing videos with inaccurate information to prevent public misleading and develop regulations on health-related internet content. Supervision mechanisms should be deployed to confine the uploading source of these contents only to healthcare professionals. Future orientations may focus on standardized, peer-reviewed videos with updated information on the diagnosis and treatment of pulpal disease to open-access platforms such as YouTube by national endodontic guideline associations.
The search methodology adopted in the present study possesses several limitations. Firstly, the results of the present cross sectional study are time dependent because of the dynamic and changing nature of YouTube. As videos are constantly uploaded and frequently deleted on YouTube platform, the reproducibility of the study cannot be confirmed and the content will inevitably change over time, through the addition of new videos and removal of others. Secondly, the selection procedure included only the first 60 relevant videos. This was based on the fact that the first 3 pages incorporated basic search results. Indeed, Desai et al. [29] concluded that 95% of people conducting an online search will look no further than the first 3 pages of output. This methodology replicates the average individual's search attempt as most internet users conducting an online search do not look further than the first 50 search results [13,26,27]. Only English language videos were included, as the majority of videos stored on YouTube are English language videos and originated from the USA. Furthermore, the consistently low quality and reliability of the total 120 videos are likely to be good representatives of the total number of pulpotomy and pulp capping videos, comparable to the results of other literature. In addition, the exclusion of videos lasting longer than 15 minutes has been used in line with previous studies suggesting that longer videos would be unlikely to keep the attention of the online viewer and do not receive much viewership [12,27]. Additionally, as an average time spent per day on YouTube has been estimated at 40 minutes with an average audience retention rate ranging between 50–60% [17], short-lasting videos would be expected to perform best. Finally, the lack of validated instruments for reviewing online information remains another important limitation for this kind of study. However, these tools continue to be the most commonly used in the literature evaluating online resources and YouTube quality and reliability in particular.
CONCLUSIONS
Although specialists have contributed better quality videos than non-specialists, the overall educational quality and reliability of the videos concerning pulpotomy and pulp capping were low. As YouTube represents an important source for patient information about different health topics, reliable informative videos should be uploaded by specialized dental professionals. Future directions may include encouragement of international associations, universities and specialized healthcare professionals to create and publish beneficial material and peer-reviewed videos with updated information on the diagnosis and treatment of pulpal disease to open-access platforms such as YouTube in order to give comprehensive and reliable information to people who seek on the internet.
-
Conflict of Interest: No potential conflict of interest relevant to this article was reported.
-
Author Contributions:
Conceptualization: Kodonas K.
Data curation: Kodonas K.
Formal analysis: Kodonas K, Fardi A.
Investigation: Kodonas K, Fardi A.
Methodology: Kodonas K, Fardi A.
Project administration: Kodonas K, Fardi A.
Resources: Kodonas K, Fardi A.
Software: Kodonas K, Fardi A.
Supervision: Kodonas K.
Validation: Kodonas K.
Visualization: Kodonas K.
Writing - original draft: Fardi A.
Writing - review & editing: Kodonas K.
- 1. Parashos P, Messer HH. The diffusion of innovation in dentistry: a review using rotary nickel-titanium technology as an example. Oral Surg Oral Med Oral Pathol Oral Radiol Endod 2006;101:395-401.ArticlePubMed
- 2. Rogers EM. Diffusion of innovations. 5th ed. New York, NY: Free Press; 2003.
- 3. AlFaris E, Irfan F, Ponnamperuma G, Jamal A, Van der Vleuten C, Al Maflehi N, Al-Qeas S, Alenezi A, Alrowaished M, Alsalman R, Ahmed AM. The pattern of social media use and its association with academic performance among medical students. Med Teach 2018;40(Supplement 1):S77-S82.ArticlePubMed
- 4. Rapp AK, Healy MG, Charlton ME, Keith JN, Rosenbaum ME, Kapadia MR. YouTube is the most frequently used educational video source for surgical preparation. J Surg Educ 2016;73:1072-1076.ArticlePubMedPMC
- 5. Tackett S, Slinn K, Marshall T, Gaglani S, Waldman V, Desai R. medical education videos for the world: an analysis of viewing patterns for a YouTube channel. Acad Med 2018;93:1150-1156.ArticlePubMed
- 6. Wiid J, Cant MC, Nell C. Open distance learning students' perception of the use of social media networking systems as an educational tool. IBER 2013;12:867-882.ArticlePDF
- 7. Fox S, Purcell K. Chronic disease and the internet [Internet]. Washington, D.C.: Pew Research Center; 2010. Updated 2020 Jul 12]. Available from: www.pewinternet.org/2010/03/24/chronic-disease-and-the-internet/.
- 8. Bujnowska-Fedak MM, Waligóra J, Mastalerz-Migas A. The internet as a source of health information and services. Adv Exp Med Biol 2019;1211:1-16.ArticlePubMed
- 9. Bujnowska-Fedak MM, Węgierek P. The impact of online health information on patient health behaviours and making decisions concerning health. Int J Environ Res Public Health 2020;17:880.ArticlePubMedPMC
- 10. Madathil KC, Rivera-Rodriguez AJ, Greenstein JS, Gramopadhye AK. Healthcare information on YouTube: a systematic review. Health Informatics J 2015;21:173-194.ArticlePubMedPDF
- 11. Nason GJ, Kelly P, Kelly ME, Burke MJ, Aslam A, Giri SK, Flood HD. YouTube as an educational tool regarding male urethral catheterization. Scand J Urol 2015;49:189-192.ArticlePubMed
- 12. Nason K, Donnelly A, Duncan HF. YouTube as a patient-information source for root canal treatment. Int Endod J 2016;49:1194-1200.ArticlePubMed
- 13. Radonjic A, Fat Hing NN, Harlock J, Naji F. YouTube as a source of patient information for abdominal aortic aneurysms. J Vasc Surg 2020;71:637-644.ArticlePubMed
- 14. Ng CH, Lim GR, Fong W. Quality of English-language videos on YouTube as a source of information on systemic lupus erythematosus. Int J Rheum Dis 2020;23:1636-1644.ArticlePubMedPDF
- 15. Erdem MN, Karaca S. Evaluating the accuracy and quality of the information in kyphosis videos shared on YouTube. Spine 2018;43:E1334-EE1339.ArticlePubMed
- 16. Eksi Ozsoy H. Evaluation of YouTube videos about smile design using the DISCERN tool and Journal of the American Medical Association benchmarks. J Prosthet Dent 2021;125:151-154.ArticlePubMed
- 17. BroadbandSearch.net. Average daily time on YouTube [Internet]. Updated 2021]. Available from: https://www.broadbandsearch.net/blog/average-daily-time-on-social-media#post-navigation-4.
- 18. Abukaraky A, Hamdan AA, Ameera MN, Nasief M, Hassona Y. Quality of YouTube TM videos on dental implants. Med Oral Patol Oral Cir Bucal 2018;23:e463-ee468.ArticlePubMedPMC
- 19. Fortuna G, Schiavo JH, Aria M, Mignogna MD, Klasser GD. The usefulness of YouTube™ videos as a source of information on burning mouth syndrome. J Oral Rehabil 2019;46:657-665.ArticlePubMedPDF
- 20. Hassona Y, Taimeh D, Marahleh A, Scully C. YouTube as a source of information on mouth (oral) cancer. Oral Dis 2016;22:202-208.ArticlePubMed
- 21. Hutchison CM, Cave V, Walshaw EG, Burns B, Park C. YouTube™ as a source for patient education about the management of dental avulsion injuries. Dent Traumatol 2020;36:207-211.ArticlePubMedPDF
- 22. Gaş S, Zincir ÖÖ, Bozkurt AP. Are YouTube videos useful for patients \xc4\xb1nterested in botulinum toxin for bruxism? J Oral Maxillofac Surg 2019;77:1776-1783.PubMed
- 23. Crespo-Gallardo I, Hay-Levytska O, Martín-González J, Jiménez-Sánchez MC, Sánchez-Domínguez B, Segura-Egea JJ. Criteria and treatment decisions in the management of deep caries lesions: Is there endodontic overtreatment? J Clin Exp Dent 2018;10:e751-ee760.ArticlePubMedPMC
- 24. Croft K, Kervanto-Seppälä S, Stangvaltaite L, Kerosuo E. Management of deep carious lesions and pulps exposed during carious tissue removal in adults: a questionnaire study among dentists in Finland. Clin Oral Investig 2019;23:1271-1280.ArticlePubMedPDF
- 25. Özdal Zincir Ö, Bozkurt AP, Gaş S. Potential patient education of YouTube videos related to wisdom tooth surgical removal. J Craniofac Surg 2019;30:e481-ee484.ArticlePubMed
- 26. Hegarty E, Campbell C, Grammatopoulos E, DiBiase AT, Sherriff M, Cobourne MT. YouTube™ as an information resource for orthognathic surgery. J Orthod 2017;44:90-96.ArticlePubMed
- 27. Lena Y, Dindaroğlu F. Lingual orthodontic treatment: a YouTube™ video analysis. Angle Orthod 2018;88:208-214.ArticlePubMedPDF
- 28. Guo J, Yan X, Li S, Van der Walt J, Guan G, Mei L. Quantitative and qualitative analyses of orthodontic-related videos on YouTube. Angle Orthod 2020;90:411-418.ArticlePubMedPMCPDF
- 29. Desai T, Shariff A, Dhingra V, Minhas D, Eure M, Kats M. Is content really king? An objective analysis of the public's response to medical videos on YouTube. PLoS One 2013;8:e82469.ArticlePubMedPMC
REFERENCES
Tables & Figures
REFERENCES
Citations
Citations to this article as recorded by 
- Evaluation of YouTubeTM Videos Regarding ICON as an Information Resource: A Cross-Sectional Study
Sevim Atılan Yavuz, Zeyneb Merve Ozdemır, Derya Gursel Surmelioglu
Mersin Üniversitesi Tıp Fakültesi Lokman Hekim Tıp Tarihi ve Folklorik Tıp Dergisi.2026; 16(1): 282. CrossRef - Quality and Accuracy Assessment of YouTube Videos on Vital Pulp Therapy
Divya Nangia, Vasudev Ballal, Prashant Bhasin, Esha Sukhala, Ashima Garg, Meenu G. Singla, Hemanshi Kumar
Australian Endodontic Journal.2026;[Epub] CrossRef - Assessing the Quality of YouTube® Videos on Nitrous Oxide/Oxygen Inhalation: A Multi-Dimensional Approach for Pediatric Dentists
Sanaa N. Al-Haj Ali, Nehal AlHarbi, Hessah H. Almutairi
Pesquisa Brasileira em Odontopediatria e Clínica Integrada.2025;[Epub] CrossRef - Is YouTube™ a useful resource of information about bichectomy? A cross-sectional study
H.ɪ. Durmuş, B. Ege, S. Bayazıt, M. Koparal
Annales de Chirurgie Plastique Esthétique.2025;[Epub] CrossRef - Assessing the reliability and educational value of YouTube videos on computer-controlled local anesthesia in dentistry
Hulya Cerci Akcay, Erdal Cem Kargu, Nefise Seker, Tanay Chaubal
PLOS One.2025; 20(8): e0329291. CrossRef - A content analysis of YouTube videos on interproximal enamel reduction
Weng Yan Tam, Jack Shen Tham, Smita Nimbalkar, Shilpa Gunjal, Kirti Saxena
APOS Trends in Orthodontics.2025; 0: 1. CrossRef - Comparison of YouTube, TikTok, and Instagram as digital sources for obtaining information about pulp therapy in primary and permanent teeth
Hüseyin Gürkan Güneç, Emine Kaya, Dila Nur Okumuş, Merve Gül Erence
Restorative Dentistry & Endodontics.2025; 50(3): e26. CrossRef - Evaluation of Endodontic Retreatment Videos on The Youtube Platform: Quality and Content Analysis
Birgül Özaşır, Tufan Özaşır, Derin Buğu Yüzer, Deniz İmamoğlu, Kamran Gülşahı
European Annals of Dental Sciences.2025; 52(2): 103. CrossRef - Is YouTube a reliable source for learning pre-endodontic build-up? A cross-sectional study
Merve Gökyar, İdil Özden, Hesna Sazak Öveçoğlu
Restorative Dentistry & Endodontics.2025; 50(3): e27. CrossRef - Quality of Patient-Centered eHealth Information on Erosive Tooth Wear: Systematic Search and Evaluation of Websites and YouTube Videos
Lena Holland, Amelie Friederike Kanzow, Annette Wiegand, Philipp Kanzow
Journal of Medical Internet Research.2024; 26: e49514. CrossRef - Is it safe to learn about vital pulp capping from YouTube™ videos? A content and quality analysis
Celalettin Topbaş, Tuğçe Paksoy, Ayşe Gülnihal İslamoğlu, Kemal Çağlar, Abdurrahman Kerim Kul
International Journal of Medical Informatics.2024; 185: 105409. CrossRef - Assessment of the quality of oral biopsy procedure videos shared on YouTube
A. Díaz‐Rodríguez, J. Limeres‐Posse, R. Albuquerque, V. Brailo, R. Cook, J. C. Fricain, G. Lodi, L. Monteiro, L. Silva, B. Carey, M. Diniz‐Freitas
Oral Diseases.2024; 30(5): 3081. CrossRef - İmplant üstü protezler hakkında bilgi veren internet sitelerinin okunabilirliklerinin değerlendirilmesi
Tugba TEMİZCİ
Selcuk Dental Journal.2023; 10(4): 156. CrossRef - Online Audio-Visual Information on the Treatment of OSA with Mandibular Advancement Devices: Analysis of Quality, Reliability and Contents
Serena Incerti-Parenti, Maria Lavinia Bartolucci, Elena Biondi, Andrea Fiordelli, Corrado Paganelli, Giulio Alessandri-Bonetti
Applied Sciences.2023; 13(9): 5727. CrossRef - Evaluating YouTube as a Patient Information Source for the Risks of Root Canal Treatment
Stewart McLean, Neil Cook, Alexander Rovira-Wilde, Shanon Patel, Shalini Kanagasingam
Journal of Endodontics.2023; 49(2): 155. CrossRef - Assessment of reliability and information quality of YouTube videos about root canal treatment after 2016
Myoung-jun Jung, Min-Seock Seo
BMC Oral Health.2022;[Epub] CrossRef - Is the YouTube™ a useful resource of information about orthognathic surgery?: A cross-sectional study
Seyma Bayazıt, Bilal Ege, Mahmut Koparal
Journal of Stomatology, Oral and Maxillofacial Surgery.2022; 123(6): e981. CrossRef - YoutubeTM Content Analysis as a Means of Information in Oral Medicine: A Systematic Review of the Literature
Antonio Romano, Fausto Fiori, Massimo Petruzzi, Fedora Della Vella, Rosario Serpico
International Journal of Environmental Research and Public Health.2022; 19(9): 5451. CrossRef
 ePub Link
ePub Link Cite
CiteYouTube as a source of information about pulpotomy and pulp capping: a cross sectional reliability analysis
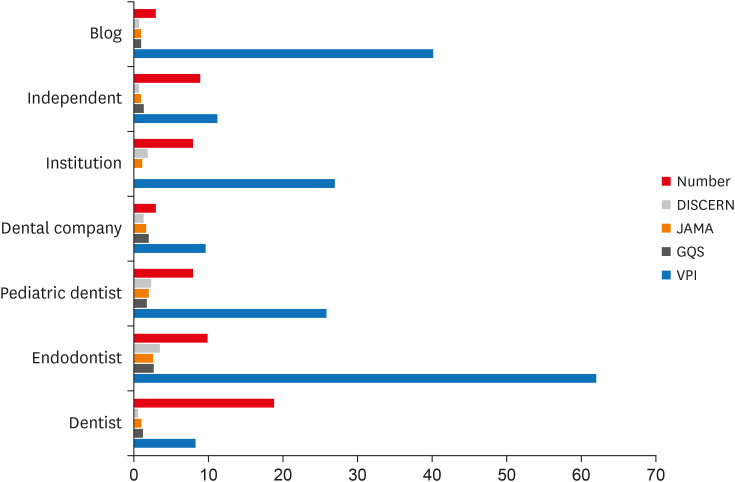
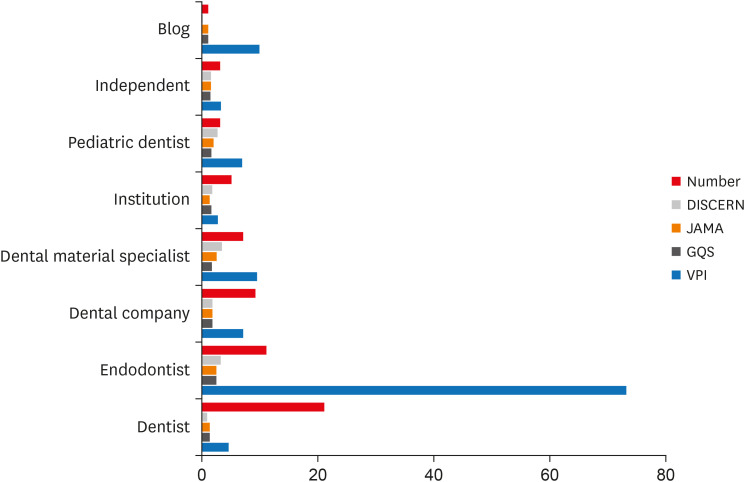
Figure 1 Average reliability scores for pulpotomy videos per video source variables.JAMA, Journal of American Medical Association; GQS, Global Quality Score; VPI, Video Power Index.
Figure 2 Average reliability scores for pulp capping videos per video source variables.JAMA, Journal of American Medical Association; GQS, Global Quality Score; VPI, Video Power Index.
Figure 1
Figure 2
YouTube as a source of information about pulpotomy and pulp capping: a cross sectional reliability analysis
Inclusion and exclusion criteria
| Inclusion | Exclusion |
|---|---|
| English language | Non-English language |
| Acceptable audio & visual quality | Irrelevant to pulpotomy or pulp capping |
| Duration longer than 15 min | |
| Duplicates |
Information reliability of videos according to modified DISCERN index
| 1. Are the aims clear, concise and achieved? |
| 2. Are reliable sources of information used? (i.e., board-certified speakers, publication cited, video content were from valid studies) |
| 3. Is the information presented balanced and unbiased? Is there any reference to other treatment choices? |
| 4. Are additional sources of information listed for patient reference? |
| 5. Does the video address areas of uncertainty? |
Journal of American Medical Association benchmark criteria
| Criteria | Description |
|---|---|
| Authorship | Authors, partnerships and contributors, their affiliations and relevant credentials should be provided |
| Attribution | References and resources used for the content and a copyright statement should be listed clearly |
| Disclosure | Sponsorship, advertising, commercial financing, potential conflicts of interest should be prominently and fully disclosed |
| Currency | Dates when content was posted and updated should be indicated |
The GQS criteria
| GQS | Description of quality |
|---|---|
| 1 | Poor quality, poor flow, most information missing, not useful for patient education. |
| 2 | Generally poor quality and flow, of limited use to patients because only some information is present but many important topics missing. |
| 3 | Moderate quality, suboptimal flow, somewhat useful for patients as some important information is adequately discussed but others poorly discussed. |
| 4 | Good quality, generally good flow, useful to patients because most relevant information is covered but some topics not covered. |
| 5 | Excellent quality and flow, highly useful to patients. |
GQS, Global Quality Score.
Video characteristics and reliability scores of the included pulpotomy and pulp capping YouTube videos
| Characteristics and reliability scores | Pulpotomy | Pulp capping | p value* |
|---|---|---|---|
| Video length (sec) | 259 ± 201.3 | 338.6 ± 267.9 | 0.133 |
| Number of views | 22,046 ± 39,916 | 17,631 ± 74,087 | 0.040* |
| Number of likes | 118.9 ± 210.6 | 133.3 ± 311.3 | 0.347 |
| Number of dislikes | 6.9 ± 12.2 | 5.2 ± 20.1 | 0.115 |
| Days since upload | 1,370 ± 1,157 | 1,055 ± 1,016 | 0.157 |
| VPI | 24.4 ± 72.2 | 17.96 ± 81.2 | 0.158 |
| Modified DISCERN | 1.53 ± 1.47 | 1.77 ± 1.5 | 0.381 |
| JAMA | 1.47 ± 0.72 | 1.65 ± 0.69 | 0.074 |
| GQS | 1.63 ± 0.86 | 1.70 ± 0.77 | 0.382 |
Values are presented as mean ± standard deviation.
GQS, Global Quality Score; JAMA, Journal of American Medical Association; VPI, Video Power Index.
*Results of Mann-Whitney U test.
Video characteristics and reliability scores of the included pulpotomy and pulp capping YouTube videos among specialists and non-specialists
| Characteristics | Pulpotomy | Pulp capping | ||||
|---|---|---|---|---|---|---|
| Specialist (n = 19) | Non-specialist (n = 41) | p value* | Specialist (n = 27) | Non-specialist (n = 33) | p value* | |
| Video length (sec) | 322 ± 214 | 229 ± 190.6 | 0.047* | 444 ± 271.88 | 252.3 ± 234.9 | 0.002* |
| Number of views | 18,359 ± 20,880 | 237,534 ± 46,308 | 0.395 | 30,865 ± 108,931 | 6,803 ± 14,509 | 0.015 |
| Number of likes | 156.7 ± 230.3 | 101.4 ± 201.4 | 0.039 | 248.2 ± 419.4 | 39.2 ± 124.4 | 0.000* |
| Number of dislikes | 7.26 ± 10.34 | 6.68 ± 13.06 | 0.674 | 8.4 ± 29.3 | 2.52 ± 5.57 | 0.058 |
| Days since upload | 1,102 ± 984.4 | 1,494.7 ± 1,220 | 0.348 | 928.7 ± 950.2 | 1,157.6 ± 1,070 | 0.629 |
| VPI | 44.4 ± 121.1 | 15.1 ± 28.4 | 0.086 | 35.1 ± 119.8 | 3.97 ± 6.08 | 0.000* |
| Modified DISCERN | 3.00 ± 1.25 | 0.85 ± 0.99 | 0.000* | 2.96 ± 0.98 | 0.79 ± 1.08 | 0.000* |
| JAMA | 2.37 ± 0.6 | 1.05 ± 0.22 | 0.000* | 2.26 ± 0.45 | 1.15 ± 0.36 | 0.000* |
| GQS | 2.32 ± 1.06 | 1.32 ± 0.52 | 0.000* | 2.00 ± 0.83 | 1.45 ± 0.62 | 0.006* |
Values are presented as mean ± standard deviation.
GQS, Global Quality Score; JAMA, Journal of American Medical Association; VPI, Video Power Index.
*Results of Mann-Whitney U test.
JAMA benchmarks and modified DISCERN questions, number and percentage of vital pulp treatment YouTube videos
| Variables | Pulpotomy | Pulp capping | Total | |
|---|---|---|---|---|
| JAMA | ||||
| Authorship | 20 (33.3%) | 31 (51.7%) | 51 (42.5%) | |
| Attributions | 6 (10%) | 3 (5%) | 9 (7.5%) | |
| Explanations | 2 (3.3%) | 5 (8.3%) | 7 (5.8%) | |
| Currency | 60 (100%) | 60 (100%) | 120 (100%) | |
| Modified DISCERN | ||||
| Aims | 39 (65%) | 37 (61.7%) | 76 (63.3%) | |
| Reliability of sources | 19 (31.7%) | 31 (51.7%) | 50 (41.7%) | |
| Bias | 19 (31.7%) | 23 (38.3%) | 42 (35%) | |
| Additional sources | 5 (8.3%) | 2 (3.3%) | 7 (5.8%) | |
| Areas of uncertainty | 10 (16.7%) | 13 (21.7%) | 23 (19.2%) | |
JAMA, Journal of American Medical Association.
Table 1 Inclusion and exclusion criteria
Table 2 Information reliability of videos according to modified DISCERN index
Table 3 Journal of American Medical Association benchmark criteria
Table 4 The GQS criteria
GQS, Global Quality Score.
Table 5 Video characteristics and reliability scores of the included pulpotomy and pulp capping YouTube videos
Values are presented as mean ± standard deviation.
GQS, Global Quality Score; JAMA,
*Results of Mann-Whitney
Table 6 Video characteristics and reliability scores of the included pulpotomy and pulp capping YouTube videos among specialists and non-specialists
Values are presented as mean ± standard deviation.
GQS, Global Quality Score; JAMA,
*Results of Mann-Whitney
Table 7 JAMA benchmarks and modified DISCERN questions, number and percentage of vital pulp treatment YouTube videos
JAMA,

