
Articles
- Page Path
- HOME > Restor Dent Endod > Volume 46(2); 2021 > Article
- Research Article Effects of radiation therapy on the dislocation resistance of root canal sealers applied to dentin and the sealer-dentin interface: a pilot study
-
Pallavi Yaduka1
 , Rubi Kataki1, Debosmita Roy1, Lima Das1, Shachindra Goswami2
, Rubi Kataki1, Debosmita Roy1, Lima Das1, Shachindra Goswami2 -
Restor Dent Endod 2021;46(2):e22.
DOI: https://doi.org/10.5395/rde.2021.46.e22
Published online: March 29, 2021
1Department of Conservative Dentistry and Endodontics, Regional Dental College, Guwahati, AS, India.
2Medical Physics Division, Department of Radiation Oncology, Dr. B Borooah Cancer Institute, Guwahati, AS, India.
- Correspondence to Pallavi Yaduka, MDS. Postgraduate Student, Department of Conservative Dentistry and Endodontics, Regional Dental College, Behind GMC, Bhangagarh, Guwahati, P.O. Indrapur, Dist. Kamrup (M), Guwahati, AS 781032, India. pallavi.yaduka@gmail.com
• Received: April 22, 2020 • Revised: June 19, 2020 • Accepted: June 24, 2020
Copyright © 2021. The Korean Academy of Conservative Dentistry
This is an Open Access article distributed under the terms of the Creative Commons Attribution Non-Commercial License (https://creativecommons.org/licenses/by-nc/4.0/) which permits unrestricted non-commercial use, distribution, and reproduction in any medium, provided the original work is properly cited.
Abstract
-
Objectives This study evaluated and compared the effects of radiation therapy on the dislocation resistance of AH Plus and BioRoot RCS applied to dentin and the sealer-dentin interface.
-
Materials and Methods Thirty single-rooted teeth were randomly assigned to 2 groups (n = 15 each): AH Plus (Dentsply DeTrey) and BioRoot RCS (Septodont). Each group was subdivided into control and experimental groups. The experimental group was subjected to a total radiation dose of 60 Gy. The root canals of all samples were cleaned, shaped, and obturated using the single-cone technique. Dentin slices (1 mm) were sectioned from each root third for the push-out test and scanning electron microscopy (SEM) was done to examine the sealer-dentin interface. The failure mode was determined using stereomicroscopy. Bond strength data were analyzed by the independent t-test, 1-way analysis of variance, and the Tukey post hoc test (α = 0.05).
-
Results Significantly lower bond strength was observed in irradiated teeth than non-irradiated teeth in the AH Plus group (p < 0.05). The BioRoot RCS group showed no significant reduction in bond strength after irradiation (p > 0.05) and showed a higher post-irradiation bond strength (209.92 ± 172.26 MPa) than the AH Plus group. SEM revealed slightly larger gap-containing regions in irradiated specimens from both groups.
-
Conclusions The dislocation resistance of BioRoot RCS was not significantly changed by irradiation and was higher than that of AH Plus. BioRoot RCS may be the sealer of choice for root canal treatment in patients undergoing radiation therapy.
INTRODUCTION
Radiation therapy is commonly used to treat patients diagnosed with head and neck cancer [1]. In radiation therapy, ionizing radiation is used as a therapeutic agent and causes various post-treatment complications, such as mucositis, loss of taste, trismus, microvascular alterations, soft tissue necrosis, osteoradionecrosis, and radiation caries. Radiation can also reduce salivary flow (xerostomia) and secretion, as well as causing changes in its composition [2,3]. Recent studies have demonstrated chemical and morphological changes in enamel and dentin crystalline structure, decreased dentinal microhardness, reduced bond strength to enamel and dentin, and increased acid solubility of enamel following irradiation [4]. These changes in enamel and dentin place patients at a higher risk of pulpal diseases, and these patients might require endodontic treatment [5]. The success of root canal treatment lies in the triad of debridement, elimination of microbes, and 3-dimensional obturation. Adequate sealing of the root canal system is necessary to prevent reinfection due to microleakage, apically or coronally [6].
Gutta-percha is the most commonly used material for root canal obturation, but it cannot bond to the dentin of the root canal wall. Most obturation techniques utilize gutta-percha with a cementing medium (root canal sealer) [6,7]. The sealer should have good adhesion to the root dentin, forming an impermeable fluid-tight seal for the root canal system and efficiently avoiding the ingress of bacteria post-obturation [8]. Newer root canal sealers are being developed with improved properties, as no commercially available sealers currently possess the properties required to be an ideal root canal sealer.
AH Plus (Dentsply DeTrey GmbH, Konstanz, Germany) is a thermoplastic epoxy resin-based sealer that has gained popularity because of its good adhesion to dentin, penetration into tubules, and adaptation to the peritubular dentin. It is characterized by very good mechanical properties, high radiopacity, relatively little polymerization shrinkage, low solubility, a high degree of stability in storage, ease of use, and biocompatibility [9]. Due to its properties, it is now considered as a gold standard for root canal sealers [10].
Bioceramic sealers are becoming increasingly popular due to their ability to bond to dentin and form hydroxyapatite. BioRoot RCS (Septodont, St. Maur-des-Fosses, France) is a new bioceramic, calcium silicate-based root canal sealer, which comes in a formulation of powder and liquid. The powder mainly consists of tricalcium silicate, povidone, and zirconium dioxide. The liquid is an aqueous solution of calcium chloride with polycarboxylate. This sealer is biocompatible and stable in biological environments [11].
The adhesion of the root canal sealers to radicular dentin is of major clinical significance. The bond strength to dentin (or dislodgement resistance) of an endodontic sealer is a measure of its adhesive capacity [12]. A strong adhesive interface between the sealer and radicular dentin and the sealer and the root canal-obturating material will prevent microleakage, thereby improving the longevity of the endodontically treated tooth [8,13]. The number of patients diagnosed with cancer is increasing every year, and these patients might require endodontic therapy. The current in vitro study was designed to address the limited information available in the literature regarding the effect of therapeutic radiation on the bonding ability of different root canal sealers and the materials that can be used to enhance bond strength in patients who have undergone radiation therapy. Hence, the present study aimed to determine the effect of therapeutic radiation on the bond strength of AH Plus and BioRoot RCS to dentin and the sealer-dentin interface.
The null hypothesis stated for the present study is that there would be no significant difference in the bond strength and sealer-dentin interface of teeth filled with AH Plus and BioRoot RCS when exposed to radiation therapy.
MATERIALS AND METHODS
Prior to conducting the study, ethical approval was obtained from the Institutional Ethical Committee board. Non-carious, single-rooted teeth with closed apices, preferably canines, with an approximate root length of at least 16 mm and no anatomical deformities or cracks were chosen. Teeth with previous endodontic treatment or metallic restorations, which could produce secondary radiation, were excluded. A total sample of 30 teeth, corresponding to the sample size determined by a statistician at 95% confidence level, was divided into 2 groups as follows: AH Plus sealer (Dentsply DeTrey GmbH) (n = 15) and BioRoot RCS (Septodont) (n = 15). Each group was subdivided into a control group (n = 5), which contained non-irradiated teeth, and an experimental group (n = 10), which contained irradiated teeth.
The samples in the experimental group were arranged in columns on a strip of wax sheet and suspended in a water phantom containing distilled water using an orthodontic wire (Figure 1). The set-up was scanned in a computed tomography machine (16-slice; Brilliance, Philips Medical Systems, Gurgaon, HR, India) and 3-dimensional radiographic images were obtained. The obtained data were transferred to a treatment planning system (photon beam calculation algorithm: Analytical Anisotropic Algorithm, Eclipse version 15.6; Varian Medical Systems, Las Vegas, NV, USA). Planning was done using 2 parallel opposed lateral beams, and the number of monitor units required to deliver a 2 Gy dose to the plane containing the samples was calculated. The set-up containing each sample was transferred to a medical linear accelerator machine (Trilogy Linear Accelerator; Varian Medical Systems), which was used to deliver radiation with 6 MV X-rays (Figure 2). A total radiation dose of 60 Gy divided into 30 fractions (2 Gy per fraction, 1 Gy on each side) was delivered for 5 consecutive days per week, over 6 weeks. The samples were transferred to a tray containing artificial saliva after the irradiation cycle every day.
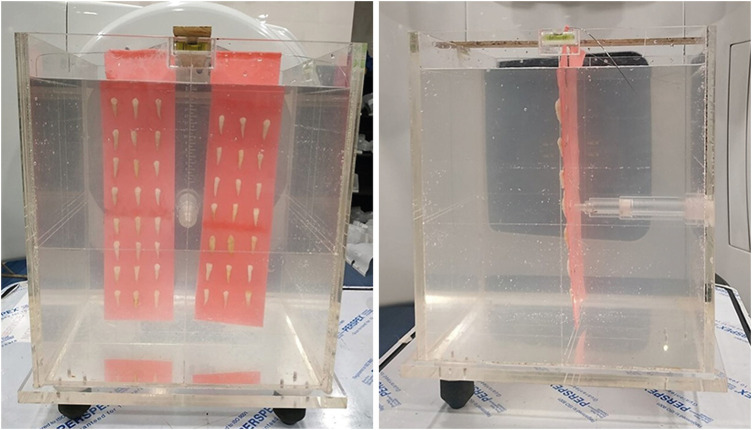
Figure 2

Arrangement of the water phantom with samples on the right and left side of the linear accelerator machine in order to receive bilateral radiation.
After radiation therapy, access cavities were prepared in all the samples. A size 10 and 15 K-files were used to negotiate the canal and measure the working length, 0.5 mm short of the apex. The root canals were sequentially cleaned and shaped by a single operator to size 35 with a taper of 0.06 using the Neo Endo Flex Rotary File System (Orikam, Gurugram, India) followed by irrigation with 5 mL of 3% sodium hypochlorite (NaOCl), 17% ethylenediaminetetraacetic acid (EDTA), and saline for 5 minutes between each preparation step. The canals were dried using paper points and obturated with gutta-percha using the single-cone obturation technique. The sealer used was either AH Plus or BioRoot RCS according to the group to which the sample belonged. The sealers were manipulated following the manufacturer's instructions. The gutta-percha was seared at the cervical level, sealed with a temporary restorative material, and stored in phosphate-buffered solution at 37°C for a period 3 times longer than the setting time of the sealer [14].
The root of each sample was sectioned perpendicular to its long axis into 10 sections, each measuring 1 mm thick, using a water-cooled linear precision saw (Isomet 4000; Buehler, Lake Bluff, IL, USA). The tests were performed by a different operator who was blinded to the groups. The first slice obtained from each root third was used for the push-out test in a universal testing machine (Instron 8801; Instron, Norwood, MA, USA), operating at a cross-head speed of 0.5 mm/min. Stainless steel plungers with tip diameters of 0.3, 0.5, and 1 mm were used for testing the apical, middle, and coronal thirds, respectively, which were calculated based on the diameters at each third as the root canal was prepared up to the size of 35 with a taper of 0.06 [15]. The apical surface was placed facing the plunger tip. The plunger tip was placed such that it contacted the filling material only and a constant load was applied until dislodgement of the filling material. The dislodgement was noted by the sudden loss of resistance and extrusion of filling material. Bond strength data in megapascals (MPa) were collected from the computer.
Five samples that were tested for dislocation resistance from each group were viewed under a stereomicroscope (Nikon SMZ25; Nikon Instruments Inc., Melville, NY, USA) at ×40 magnification to visualize the mode of failure.
The second slices of the apical third of 5 samples from each group were used for a qualitative analysis of the sealer-dentin interface by field-emission scanning electron microscopy (FE-SEM) (GeminiSEM300; Zeiss, Moringen, Germany) at ×1,500, ×3,000, and ×5,000 magnifications.
The results of the present study were statistically analyzed using the independent-samples t-test for intra-group comparisons, 1-way analysis of variance for inter-group comparisons, and the Tukey post hoc test for pair-wise comparisons. These tests were conducted at a 5% level of significance.
RESULTS
Samples from the control (non-irradiated) and experimental (irradiated) groups were assessed. The AH Plus control group showed the highest bond strength (490.74 ± 429 MPa). In the comparison of the control and experimental values of bond strength in each sealer group, the bond strength to radicular dentin was highly significantly reduced in teeth subjected to irradiation compared to non-irradiated teeth in the AH Plus group (p < 0.001). Although there was a decrease in strength in the BioRoot RCS group (p = 0.146), it was not statistically significant (Table 1).
Table 1
Comparison between the control and experimental values of bond strength (MPa) in each group irrespective of the root third
The bond strength of the 2 sealers in the experimental groups were assessed. The highest bond strength was noted in the BioRoot RCS group (209.92 ± 172.26 MPa). The difference in bond strength between AH Plus and BioRoot RCS was found to be significant (p = 0.005) (Table 2).
Table 2
Bond strength (MPa) of the 2 sealers in the experimental groups irrespective of the root third
| Group | Mean ± standard deviation | t-test (p value) |
|---|---|---|
| AH Plus | 127.01 ± 90.06 | 0.005 (significant) |
| BioRoot RCS | 209.92 ± 172.26 |
The bond strength values of the sealers at coronal, middle, and apical thirds in both the control and experimental groups are given in Figure 3. The bond strength was found to be significantly higher in the coronal third, followed by middle and apical thirds in both groups irrespective of irradiation. However, the difference between the middle and apical thirds was found to be insignificant (Table 3).
Figure 3
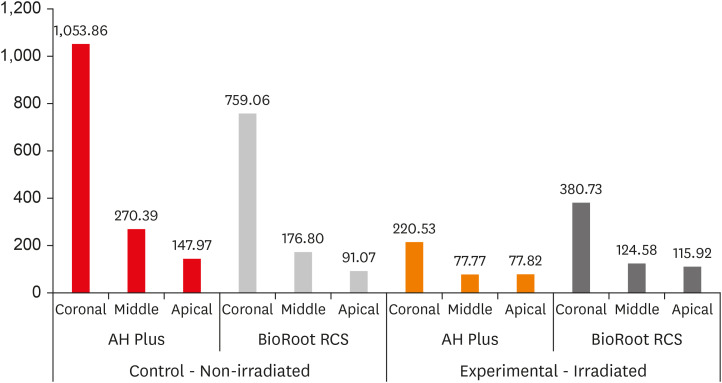
Bar chart showing the mean bond strength (MPa) of the 2 sealer groups at the coronal, middle, and apical levels in the non-irradiated and irradiated samples.
Table 3
Bond strength values (MPa) at different root thirds in the control and experimental groups irrespective of sealers
The failure modes as viewed under the stereomicroscope were classified as adhesive (between the sealer and dentin of the root canal wall), cohesive (within the sealer itself), and mixed (areas of both adhesive and cohesive failure). AH Plus predominantly showed cohesive failure and BioRoot RCS showed mixed failure, irrespective of exposure to radiation (Figure 4).
Figure 4
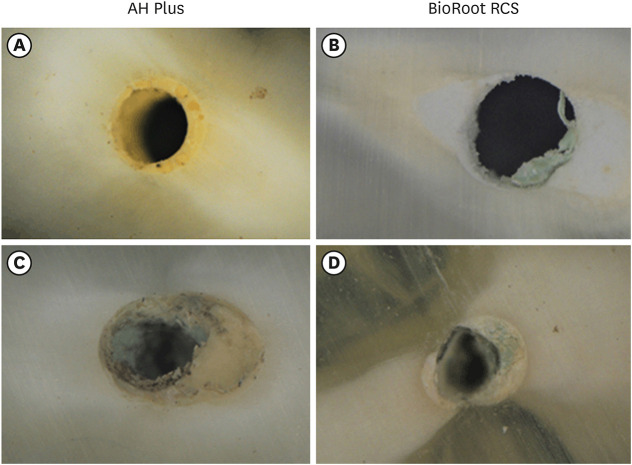
Failure mode analysis using a stereomicroscope at ×40 magnification. (A and B) represent images of control group. (C and D) represent images of experimental group.
Qualitative analysis of the sealer dentin interface by FE-SEM in both the AH Plus and BioRoot RCS experimental groups showed slightly larger gap-containing areas at sealer-dentin interface than the corresponding controls, although there was little difference between the 2 sealers after irradiation (Figure 5).
Figure 5
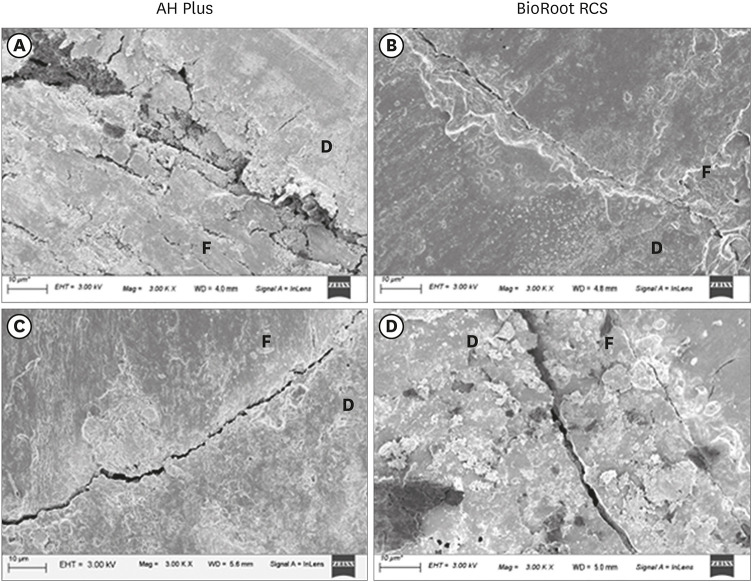
Qualitative analysis of the sealer-dentin interface by field-emission scanning electron microscopy (Gemini 300) at ×3,000 magnification. (A and B) represent images of the control group. (C and D) show larger gaps at the interface after irradiation (experimental group).
D, dentin; F, filling.
DISCUSSION
Ionizing radiation used for radiation therapy has direct and indirect detrimental effects on dental tissues. Radiation caries is regarded as an indirect effect, which results in a higher frequency of root canal treatment in patients undergoing radiation therapy [14]. Extractions are not recommended in such patients, due to the risk of osteoradionecrosis [16]. Hence, endodontic treatment plays an important role in patients who receive radiation therapy.
An in vitro model was chosen to simulate oral cancer radiotherapy since teeth cannot be tested before and after in vivo radiotherapy [2,3,4]. In this study, fractionated radiation was used because it allows repopulation of tissue cells between fractions, thereby reducing the early effects of radiation [17]. The methodology followed in this study was adopted from other similar studies [14,18,19,20].
The samples were stored in artificial saliva between the irradiation cycles, as in the clinical setting, the teeth are always surrounded by saliva in the oral cavity. They were transferred to distilled water for irradiation every day, as the viscosity and high ion concentration of artificial saliva can affect the homogeneous distribution of radiation [2,14]. Furthermore, the use of distilled water can physically and chemically mimic the surrounding soft tissues by the formation of free radicals, as water is also abundantly present in human tissues [20]. It is necessary that all areas to be irradiated receive a uniform amount of radiation or a similar dose, for which a treatment planning system was used. This term refers to a computer-based algorithmic system that uses radiographic images and dosimetric data to determine the optimum treatment parameters (beam angles and collimation) [21].
The push-out bond strength test was used to evaluate the dislocation resistance between the sealer and root canal dentin in this study. The push-out model has been widely used to study interactions between sealers and dentin, but its relevance has also been called into question [22,23]. The experimental model used in this study was adopted from guidelines given in previous studies [24,25].
In the present study, significantly lower dislocation resistance was observed in the teeth subjected to radiation than in non-irradiated teeth in the AH Plus group. Studies done by Martins et al. [14], Yamin et al. [18], and Bodrumlu et al. [19] have also reported reductions in bond strength after irradiation. The BioRoot RCS group did not show a significant reduction in bond strength after irradiation. Therefore, the null hypothesis was partially rejected. However, the AH Plus control group showed higher bond strength than the BioRoot RCS control group. This finding is supported by many studies [8]. Among the experimental groups, higher bond strength was shown by the BioRoot RCS sealer than by the AH Plus sealer. A similar study by Martins et al. [14] in 2016 compared the bond strength of AH Plus and MTA Fillapex and reported a higher bond strength of AH Plus after irradiation.
The decrease in the bond strength of AH Plus might be related to changes in structure of dentin. AH Plus bonds chemically with the collagen network of dentin by the formation of covalent bonds between the open epoxy rings of the sealer and the exposed amine groups in collagen, which increases the strength of bonds between the sealer and root dentin [26,27]. The effects of radiation on dentin occur due to its water content (approximately 12% by volume), which leads to the formation of free radicals and hydrogen peroxide [28]. This in turn causes disturbances in the protein structures of collagen fibers, causing harmful effects [14] such as disintegration of the collagen fiber network [2,3,4] and activation of matrix metalloproteinases [29]. This may be an explanation for the decrease in the dislocation resistance of AH Plus after irradiation.
BioRoot RCS contains calcium phosphate, which enhances its setting properties [30]. Sarkar et al. [31] and Reyes-Carmona et al. [32,33] suggested that the uptake of calcium and silicon in the dentin in contact with calcium silicate cements occurs following contact with phosphate ions present in the canal, which increases the acid resistance and bond strength of calcium silicate-based materials, enhancing biomineralization [34].
Previous studies have reported that therapeutic radiation did not cause any change in the calcium/phosphorus ratios of enamel [35]. A study by Reed et al. [1] reported that the protein/mineral ratio of enamel and dentin decreased following radiotherapy. Therefore, it can be assumed that changes in organic components do occur following therapeutic irradiation, which exert an indirect effect on the inorganic components of the tooth [2]. Soares et al. [4] also reported that radiation was more harmful to organic components than to inorganic components of the tooth.
No previous studies provide support for the superior bond strength of BioRoot RCS after irradiation. BioRoot RCS adheres to both the organic and inorganic content of dentin [36]. Since the organic content of dentin is more strongly affected by radiation than the inorganic content [1,4], this might have been one of the reasons for the greater dislocation resistance of BioRoot RCS than AH Plus after irradiation.
The dislocation resistance of the tested sealers was found to be higher in the coronal third than in the middle and apical thirds, as supported by other studies [14,27,37]. This could be due to the lower number and smaller diameter of dentinal tubules in the apical region [27]. Inadequate removal of the smear layer from the apical area of the canal compared to the coronal area could also be a reason for this finding, as the presence of a residual smear layer reduces sealer penetration into the dentinal tubules, which is responsible for adhesion of the filling materials [14,37].
Failure mode analysis showed cohesive failure in AH Plus, while areas of mixed failure were noted for BioRoot RCS. There was no significant effect of radiation on the failure mode of AH Plus and BioRoot RCS. Sealers with cohesive failure have been associated with higher bond strength values. The observation of cohesive failure in AH Plus most likely indicates that its bond to dentin is stronger than that to gutta-percha, while the mixed failure in BioRoot RCS may indicate that its adhesion to both dentin and gutta-percha may be comparable [8]. Slightly larger gaps at the sealer-dentin interface were seen in the irradiated samples in the qualitative FE-SEM analysis. Studies by Donnermeyer et al. [8] and Martins et al. [14] also reported similar results in their study.
The limitations of this in vitro study are its small sample size and the fact that it did not analyze clinical variables such as surrounding structures (qualitative and quantitative changes in saliva, attached gingiva, alveolar bone and periodontal ligament), oral temperature, oral hygiene conditions, the extent of caries, the time elapsed after radiation, the longevity of sealers, and changes in the properties of sealers after irradiation. The observations of this study broaden the perspectives for further research into the influence of therapeutic radiation on the properties of dental materials and their interactions with dentin.
CONCLUSIONS
Within the limitations of the study, it is concluded that radiation therapy was associated with lower dislocation resistance of obturated teeth and the formation of more gaps at the sealer-dentin interface. BioRoot RCS was not significantly affected by irradiation and showed higher dislocation resistance than AH Plus after radiation therapy. Therefore, BioRoot RCS may be the sealer of choice for root canal treatment in patients undergoing radiation therapy.
ACKNOWLEDGEMENT
The authors would like to thank the team of medical physicists and radiation oncologists at Dr. B Borooah Cancer Institute, Guwahati, Assam and the Department of Material Sciences at the Indian Institute of Technology, Guwahati, Assam for their assistance, co-operation and for letting us carry out the study at their esteemed institution. They would also like to thank Mr. Pranjoy Das for his contribution and revision of statistical analysis.
-
Conflict of Interest: No potential conflict of interest relevant to this article was reported.
-
Author Contributions:
Conceptualization: Yaduka P.
Data curation: Yaduka P, Roy D.
Formal analysis: Yaduka P, Kataki R, Das L, Goswami S.
Funding acquisition: Yaduka P.
Investigation: Yaduka P.
Methodology: Yaduka P, Roy D, Goswami S, Kataki R, Das L.
Project administration: Yaduka P, Kataki R, Das L, Goswami S.
Resources: Yaduka P, Roy D.
Supervision: Kataki R, Das L, Goswami S.
Validation: Kataki R, Das L, Goswami S.
Visualization: Yaduka P, Kataki R, Roy D.
Writing - original draft: Yaduka P.
Writing - review & editing: Yaduka P, Roy D, Goswami S.
- 1. Reed R, Xu C, Liu Y, Gorski JP, Wang Y, Walker MP. Radiotherapy effect on nano-mechanical properties and chemical composition of enamel and dentine. Arch Oral Biol 2015;60:690-697.ArticlePubMedPMC
- 2. Gonçalves LM, Palma-Dibb RG, Paula-Silva FW, Oliveira HF, Nelson-Filho P, Silva LA, Queiroz AM. Radiation therapy alters microhardness and microstructure of enamel and dentin of permanent human teeth. J Dent 2014;42:986-992.ArticlePubMed
- 3. de Siqueira Mellara T, Palma-Dibb RG, de Oliveira HF, Garcia Paula-Silva FW, Nelson-Filho P, da Silva RA, da Silva LA, de Queiroz AM. The effect of radiation therapy on the mechanical and morphological properties of the enamel and dentin of deciduous teeth--an in vitro study. Radiat Oncol 2014;9:30.PubMedPMC
- 4. Soares CJ, Castro CG, Neiva NA, Soares PV, Santos-Filho PC, Naves LZ, Pereira PN. Effect of gamma irradiation on ultimate tensile strength of enamel and dentin. J Dent Res 2010;89:159-164.ArticlePubMedPDF
- 5. Springer IN, Niehoff P, Warnke PH, Böcek G, Kovács G, Suhr M, Wiltfang J, Açil Y. Radiation caries--radiogenic destruction of dental collagen. Oral Oncol 2005;41:723-728.ArticlePubMed
- 6. Muliyar S, Shameem KA, Thankachan RP, Francis PG, Jayapalan CS, Hafiz KA. Microleakage in endodontics. J Int Oral Health 2014;6:99-104.
- 7. Dow PR, Ingle JI. Isotope determination of root canal failure. Oral Surg Oral Med Oral Pathol 1955;8:1100-1104.ArticlePubMed
- 8. Donnermeyer D, Dornseifer P, Schäfer E, Dammaschke T. The push-out bond strength of calcium silicate-based endodontic sealers. Head Face Med 2018;14:13.ArticlePubMedPMCPDF
- 9. Balguerie E, van der Sluis L, Vallaeys K, Gurgel-Georgelin M, Diemer F. Sealer penetration and adaptation in the dentinal tubules: a scanning electron microscopic study. J Endod 2011;37:1576-1579.PubMed
- 10. Tyagi S, Mishra P, Tyagi P. Evolution of root canal sealers: an insight story. Eur J Gen Dent 2013;2:199.Article
- 11. Siboni F, Taddei P, Zamparini F, Prati C, Gandolfi MG. Properties of BioRoot RCS, a tricalcium silicate endodontic sealer modified with povidone and polycarboxylate. Int Endod J 2017;50(Supplement 2):e120-e136.ArticlePubMedPDF
- 12. Gurgel-Filho ED, Leite FM, de Lima JB, Montenegro JPC, Saavedra F, Silva EJNL. Comparative evaluation of push-out bond strength of a MTA-based root canal sealer. Braz J Oral Sci 2014;13:114-117.Article
- 13. Ørstavik D, Eriksen HM, Beyer-Olsen EM. Adhesive properties and leakage of root canal sealers in vitro . Int Endod J 1983;16:59-63.ArticlePubMed
- 14. Martins CV, Leoni GB, Oliveira HF, Arid J, Queiroz AM, Silva LA, Sousa-Neto MD. Influence of therapeutic cancer radiation on the bond strength of an epoxy- or an MTA-based sealer to root dentine. Int Endod J 2016;49:1065-1072.PubMed
- 15. Pane ES, Palamara JE, Messer HH. Critical evaluation of the push-out test for root canal filling materials. J Endod 2013;39:669-673.ArticlePubMed
- 16. Jawad H, Hodson NA, Nixon PJ. A review of dental treatment of head and neck cancer patients, before, during and after radiotherapy: part 1. Br Dent J 2015;218:65-68.ArticlePubMedPDF
- 17. Vissink A, Jansma J, Spijkervet FK, Burlage FR, Coppes RP. Oral sequelae of head and neck radiotherapy. Crit Rev Oral Biol Med 2003;14:199-212.PubMed
- 18. Yamin PA, Pereira RD, Lopes FC, Queiroz AM, Oliveira HF, Saquy PC, Sousa-Neto MD. Longevity of bond strength of resin cements to root dentine after radiation therapy. Int Endod J 2018;51:1301-1312.ArticlePubMedPDF
- 19. Bodrumlu E, Avsar A, Meydan AD, Tuloglu N. Can radiotherapy affect the apical sealing ability of resin-based root canal sealers? J Am Dent Assoc 2009;140:326-330.ArticlePubMed
- 20. Paiola FG, Lopes FC, Mazzi-Chaves JF, Pereira RD, Oliveira HF, Queiroz AM, Sousa-Neto MD. How to improve root canal filling in teeth subjected to radiation therapy for cancer. Braz Oral Res 2018;32:e121.ArticlePubMed
- 21. World Health Organization. Medical devices: managing the mismatch: an outcome of the priority medical devices project. Geneva: World Health Organization; 2010.
- 22. Sudsangiam S, van Noort R. Do dentin bond strength tests serve a useful purpose? J Adhes Dent 1999;1:57-67.PubMed
- 23. Moinzadeh AT, Jongsma LA, Wesselink PR. Considerations about the use of the “push-out” test in Endodontic research. Int Endod J 2015;48:498-500.PubMed
- 24. Neelakantan P, Ahmed HMA, Wong MCM, Matinlinna JP, Cheung GSP. Effect of root canal irrigation protocols on the dislocation resistance of mineral trioxide aggregate-based materials: a systematic review of laboratory studies. Int Endod J 2018;51:847-861.ArticlePubMedPDF
- 25. Nagas E, Uyanik O, Durmaz V, Cehreli ZC. Effect of plunger diameter on the push-out bond values of different root filling materials. Int Endod J 2011;44:950-955.ArticlePubMed
- 26. Lee KW, Williams MC, Camps JJ, Pashley DH. Adhesion of endodontic sealers to dentin and gutta-percha. J Endod 2002;28:684-688.ArticlePubMed
- 27. Neelakantan P, Subbarao C, Subbarao CV, De-Deus G, Zehnder M. The impact of root dentine conditioning on sealing ability and push-out bond strength of an epoxy resin root canal sealer. Int Endod J 2011;44:491-498.ArticlePubMed
- 28. Mjör IA. Human coronal dentine: structure and reactions. Oral Surg Oral Med Oral Pathol 1972;33:810-823.ArticlePubMed
- 29. McGuire JD, Mousa AA, Zhang BJ, Todoki LS, Huffman NT, Chandrababu KB, Moradian-Oldak J, Keightley A, Wang Y, Walker MP, Gorski JP. Extracts of irradiated mature human tooth crowns contain MMP-20 protein and activity. J Dent 2014;42:626-635.ArticlePubMedPMC
- 30. Ginebra MP, Fernández E, De Maeyer EA, Verbeeck RM, Boltong MG, Ginebra J, Driessens FC, Planell JA. Setting reaction and hardening of an apatitic calcium phosphate cement. J Dent Res 1997;76:905-912.ArticlePubMedPDF
- 31. Sarkar NK, Caicedo R, Ritwik P, Moiseyeva R, Kawashima I. Physicochemical basis of the biologic properties of mineral trioxide aggregate. J Endod 2005;31:97-100.ArticlePubMed
- 32. Reyes-Carmona JF, Felippe MS, Felippe WT. Biomineralization ability and interaction of mineral trioxide aggregate and white portland cement with dentin in a phosphate-containing fluid. J Endod 2009;35:731-736.ArticlePubMed
- 33. Reyes-Carmona JF, Felippe MS, Felippe WT. The biomineralization ability of mineral trioxide aggregate and Portland cement on dentin enhances the push-out strength. J Endod 2010;36:286-291.ArticlePubMed
- 34. Han L, Okiji T. Uptake of calcium and silicon released from calcium silicate-based endodontic materials into root canal dentine. Int Endod J 2011;44:1081-1087.ArticlePubMed
- 35. Zach GA. X-ray diffraction and calcium-phosphorous analysis of irradiated human teeth. J Dent Res 1976;55:907-909.ArticlePubMedPDF
- 36. Al-Haddad A, Che Ab Aziz ZA. Bioceramic-based root canal sealers: a review. Int J Biomater 2016;2016:9753210.ArticlePubMedPMCPDF
- 37. Topçuoğlu HS, Tuncay Ö, Demirbuga S, Dinçer AN, Arslan H. The effect of different final irrigant activation techniques on the bond strength of an epoxy resin-based endodontic sealer: a preliminary study. J Endod 2014;40:862-866.ArticlePubMed
REFERENCES
Tables & Figures
REFERENCES
Citations
Citations to this article as recorded by 
- The impact of radiotherapy on endodontic treatment: a scoping review
Guilherme Pauletto, Giovanna Isabel Mittmann Voigt, Sidnei Flores de Pellegrin, Yasmin Padoin, Carlos Alexandre Souza Bier
Odontology.2026; 114(1): 24. CrossRef - Effects of radiotherapy dose and endodontic irrigants on universal resin cement bonding to root dentin: mechanical and interfacial analyses
Lívia Ribeiro, Luíz Carlos de Lima Dias-Júnior, Paulo Henrique dos Santos, Mariana Comparotto Minamisako, Paulo Marcelo Rodrigues, Vicente Ribeiro Netto, Bruno Alexandre Pacheco de Castro Henriques, Renata Gondo Machado, Cleonice da Silveira Teixeira, Luc
International Journal of Adhesion and Adhesives.2026; 146: 104252. CrossRef - Push-out bond strength of bioceramic-based sealers following different irrigation activation techniques
Fatma Begüm Peker, Hümeyra Çapkın, Ahsen Narbay
Journal of Applied Biomaterials & Functional Materials.2026;[Epub] CrossRef - Endodontic Management Before, During and After Head and Neck Radiotherapy: Biological, Diagnostic and Clinical Considerations in Head and Neck Cancer Patients
Jing‐zhi Ma, Franklin Tay
International Endodontic Journal.2026;[Epub] CrossRef - Effect of radiation therapy on the micro push-out bond strength of tricalcium silicate-based repair cements used for furcation perforation sealing
Emanuelle Luize Meurer, Bruna Venzke Fischer, Luíz Carlos de Lima Dias-Júnior, Augusto Vanni Bodanezi, Mariana Comparotto Minamisako, Paulo Marcelo Rodrigues, Vicente Ribeiro Netto, Cleonice da Silveira Teixeira, Lucas da Fonseca Roberti Garcia
International Journal of Adhesion and Adhesives.2026; 150: 104390. CrossRef - Impact of radiation therapy regimen on the dislodgement resistance of endodontic sealers: A micro push-out test
Marcos Testa Magoga, Rafaela Lourdes de Sousa, Luiz Carlos Lima Dias-Junior, Rayssa Sabino-Silva, Mariana Comparotto Minamisako, Paulo Marcelo Rodrigues, Vicente Ribeiro Netto, Ricardo Machado, Cleonice da Silveira Teixeira, Lucas da Fonseca Roberti Garci
International Journal of Adhesion and Adhesives.2025; 136: 103894. CrossRef - Evaluation of the root dentin bond strength and intratubular biomineralization of a premixed calcium aluminate-based hydraulic bioceramic endodontic sealer
Yu-Na Lee, Min-Kyeong Kim, Hee-Jin Kim, Mi-Kyung Yu, Kwang-Won Lee, Kyung-San Min
Journal of Oral Science.2024; 66(2): 96. CrossRef - Effects of radiotherapy dose and application time on the load-to-failure values of teeth filled with different sealers
Ozgun Gulderen, Esma Saricam, Sedef Gökhan Açikgöz, Yılmaz Tezcan
BMC Oral Health.2024;[Epub] CrossRef - Ultrasonic activation of the endodontic sealer enhances its intratubular penetration and bond strength to irradiated root dentin
Luana Duart Jordani, Amanda Freitas da Rosa, Luiz Carlos de Lima Dias-Junior, Julia Menezes Savaris, Mariana Comparotto Minamisako, Luciano Roberto da Silva, Marcio Toshio Umeda Takashima, Eduardo Antunes Bortoluzzi, Cleonice da Silveira Teixeira, Lucas d
Odontology.2024; 112(3): 917. CrossRef - Effect of the timing of primary endodontic treatment and dosage of radiation therapy on the filling material removal
Bruna Venzke Fischer, Luiz Carlos de Lima Dias‐Junior, Mariana Comparotto Minamisako, Cristiane Maria Almeida, Luciano Roberto da Silva, Eduardo Antunes Bortoluzzi, Cleonice da Silveira Teixeira, Lucas da Fonseca Roberti Garcia
Australian Endodontic Journal.2024; 50(2): 321. CrossRef - Does radiation therapy affect adhesion of tricalcium silicate cements to root dentin?
Lochan KHULLAR, Nidambur Vasudev BALLAL, Tan Fırat EYÜBOĞLU, Mutlu ÖZCAN
Journal of Applied Oral Science.2023;[Epub] CrossRef - Effect of the timing of radiation therapy on the push‐out strength of resin cement to root dentine
Patrícia da Agostim Cancelier, Renata Gondo Machado, Júlia Menezes Savaris, Eduardo Antunes Bortoluzzi, Cleonice da Silveira Teixeira, Mariana Comparotto Minamisako, Paulo Marcelo Rodrigues, Vicente Ribeiro Netto, Kamile Leonardi Dutra‐Horstmann, Lucas da
Australian Endodontic Journal.2023; 49(S1): 122. CrossRef - Influence of irrigation and laser assisted root canal disinfection protocols on dislocation resistance of a bioceramic sealer
Ivona Bago, Ana Sandrić, Katarina Beljic-Ivanovic, Boris Pažin
Photodiagnosis and Photodynamic Therapy.2022; 40: 103067. CrossRef - Influence of 2% chlorhexidine on the dislodgement resistance of AH plus, bioroot RCS, and GuttaFlow 2 sealer to dentin and sealer-dentin interface
Debosmita Roy, Rubi Kataki, Lima Das, Khushboo Jain
Journal of Conservative Dentistry.2022; 25(6): 642. CrossRef
 ePub Link
ePub Link Cite
CiteEffects of radiation therapy on the dislocation resistance of root canal sealers applied to dentin and the sealer-dentin interface: a pilot study
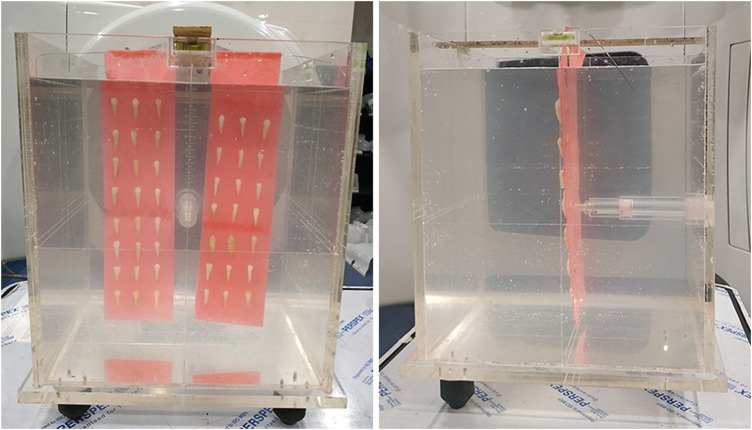

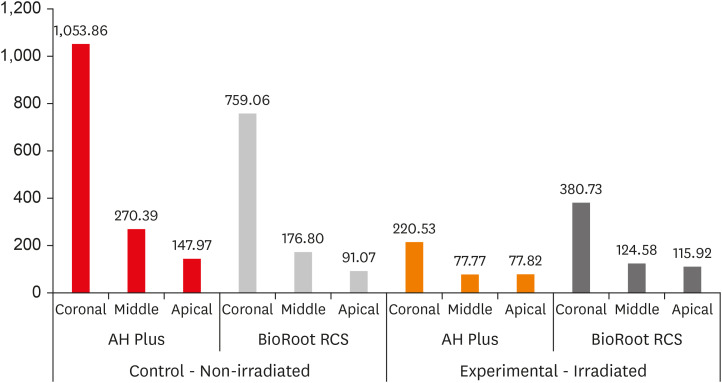
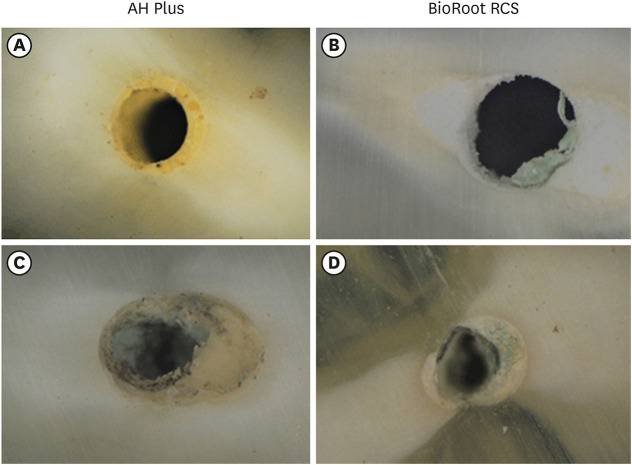
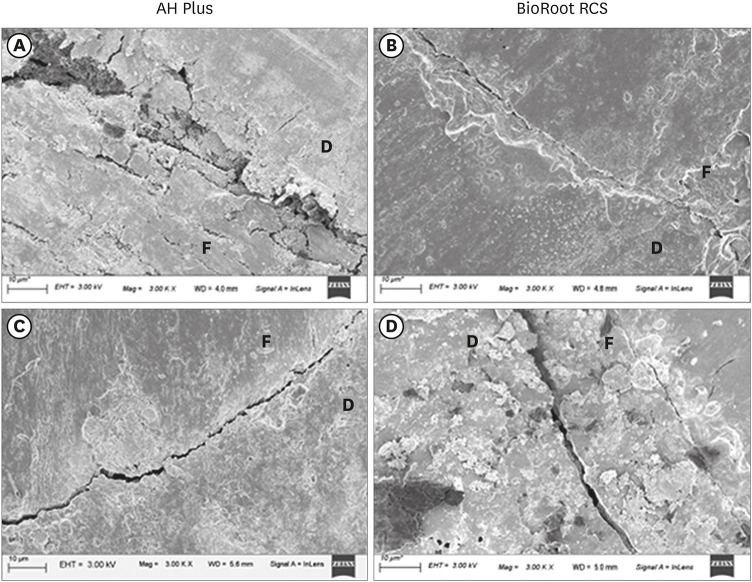
Figure 1 Arrangement of samples in the water phantom with distilled water (front and side view).
Figure 2 Arrangement of the water phantom with samples on the right and left side of the linear accelerator machine in order to receive bilateral radiation.
Figure 3 Bar chart showing the mean bond strength (MPa) of the 2 sealer groups at the coronal, middle, and apical levels in the non-irradiated and irradiated samples.
Figure 4 Failure mode analysis using a stereomicroscope at ×40 magnification. (A and B) represent images of control group. (C and D) represent images of experimental group.
Figure 5 Qualitative analysis of the sealer-dentin interface by field-emission scanning electron microscopy (Gemini 300) at ×3,000 magnification. (A and B) represent images of the control group. (C and D) show larger gaps at the interface after irradiation (experimental group).D, dentin; F, filling.
Figure 1
Figure 2
Figure 3
Figure 4
Figure 5
Effects of radiation therapy on the dislocation resistance of root canal sealers applied to dentin and the sealer-dentin interface: a pilot study
Comparison between the control and experimental values of bond strength (MPa) in each group irrespective of the root third
| Group | Mean ± standard deviation | Decrease in mean value | p value | |
|---|---|---|---|---|
| AH Plus | 363.73 (74.1%) | p < 0.001, highly significant | ||
| Control: non-irradiated | 490.74 ± 429.00 | |||
| Experimental: irradiated | 127.01 ± 90.07 | |||
| BioRoot RCS | 132.39 (42%) | p = 0.070, non-significant | ||
| Control: non-irradiated | 342.31 ± 314.71 | |||
| Experimental: irradiated | 209.92 ± 172.27 | |||
Bond strength (MPa) of the 2 sealers in the experimental groups irrespective of the root third
| Group | Mean ± standard deviation | t-test (p value) |
|---|---|---|
| AH Plus | 127.01 ± 90.06 | 0.005 (significant) |
| BioRoot RCS | 209.92 ± 172.26 |
Bond strength values (MPa) at different root thirds in the control and experimental groups irrespective of sealers
| Groups | Mean ± standard deviation | ANOVA (p value) | Pairs | p value | ||
|---|---|---|---|---|---|---|
| Control:Coronal | 906.46 ± 214.56 | p < 0.001, HS | Coronal | Middle | p < 0.001, HS | |
| Middle | 223.59 ± 72.32 | Coronal | Apical | p < 0.001, HS | ||
| Apical | 119.51 ± 36.95 | Middle | Apical | 0.203, NS | ||
| Experimental:Coronal | 300.63 ± 172.90 | p < 0.001, HS | Coronal | Middle | p < 0.001, HS | |
| Middle | 101.18 ± 32.27 | Coronal | Apical | p < 0.001, HS | ||
| Apical | 96.86 ± 43.77 | Middle | Apical | 0.991, NS | ||
ANOVA, analysis of variance; HS, highly significant; NS, not significant.
Table 1 Comparison between the control and experimental values of bond strength (MPa) in each group irrespective of the root third
Table 2 Bond strength (MPa) of the 2 sealers in the experimental groups irrespective of the root third
Table 3 Bond strength values (MPa) at different root thirds in the control and experimental groups irrespective of sealers
ANOVA, analysis of variance; HS, highly significant; NS, not significant.

