
Articles
- Page Path
- HOME > Restor Dent Endod > Volume 45(2); 2020 > Article
-
Research Article
Antimicrobial efficacy of QMix on
Enterococcus faecalis infected root canals: a systematic review ofin vitro studies -
Benjamin Syek Hur Lim1
 , Abhishek Parolia2, Margaret Soo Yee Chia1, Jayakumar Jayaraman3, Venkateshbabu Nagendrababu2
, Abhishek Parolia2, Margaret Soo Yee Chia1, Jayakumar Jayaraman3, Venkateshbabu Nagendrababu2 -
Restor Dent Endod 2020;45(2):e23.
DOI: https://doi.org/10.5395/rde.2020.45.e23
Published online: March 11, 2020
1School of Dentistry, International Medical University, Kuala Lumpur, Malaysia.
2Division of Clinical Dentistry, School of Dentistry, International Medical University, Kuala Lumpur, Malaysia.
3Department of Developmental Dentistry, University of Texas Health School of Dentistry, San Antonio, TX, USA.
- Correspondence to Abhishek Parolia, BDS, MDS, MFDS RCPS (Glasgow), MFDS RCS (Edinburgh) Head, Division of Clinical Dentistry, School of Dentistry, International Medical University, 126, Jalan Jalil Perkasa 19, Bukit Jalil, Kuala Lumpur 57000, Malaysia. abhishek_parolia@imu.edu.my
• Received: November 1, 2019 • Revised: December 3, 2019 • Accepted: December 6, 2019
Copyright © 2020. The Korean Academy of Conservative Dentistry
This is an Open Access article distributed under the terms of the Creative Commons Attribution Non-Commercial License (https://creativecommons.org/licenses/by-nc/4.0/) which permits unrestricted non-commercial use, distribution, and reproduction in any medium, provided the original work is properly cited.
- 3,231 Views
- 26 Download
- 10 Crossref
Abstract
-
Objectives This study aimed to summarize the outcome of in vitro studies comparing the antibacterial effectiveness of QMix with other irrigants against Enterococcus faecalis.
-
Materials and Methods The research question was developed by using population, intervention, comparison, outcome, and study design framework. The literature search was performed using 3 electronic databases: PubMed, Scopus, and EBSCOhost until October 2019. The additional hand search was performed from the reference list of the eligible studies. The risk of bias of the studies was independently appraised using the revised Cochrane Risk of Bias tool (RoB 2.0).
-
Results Fourteen studies were included in this systematic review. The overall risk of bias for the selected studies was moderate. QMix was found to have a higher antimicrobial activity compared to 2% sodium hypochlorite (NaOCl), 17% ethylenediaminetetraacetic acid (EDTA), 2% chlorhexidine (CHX), mixture of tetracycline isonomer, an acid and a detergent (MTAD), 0.2% Cetrimide, SilverSol/H2O2, HYBENX, and grape seed extract (GSE). QMix had higher antibacterial efficacy compared to NaOCl, only when used for a longer time (10 minutes) and with higher volume (above 3 mL).
-
Conclusions QMix has higher antibacterial activity than 17% EDTA, 2% CHX, MTAD, 0.2% Cetrimide, SilverSol/H2O2, HYBENX, GSE and NaOCl with lower concentration. To improve the effectiveness, QMix is to use for a longer time and at a higher volume.
-
Trial Registration PROSPERO International prospective register of systematic reviews Identifier: CRD42018096763
INTRODUCTION
Microbiota in the root canal system are found in highly organized and complex entities known as biofilms. The persistence of microorganisms inside the root canal system is the most common reason for the failure of root canal treatment [1,2]. The complexity and variability of the root canal system, along with the nature of biofilm, make the root canal disinfection extremely challenging [3,4]. Enterococcus faecalis (E. faecalis) has been one of the most persistent intra-radicular infections compared with untreated chronic periapical periodontitis [5,6,7]. It can survive in harsh conditions due to its ability to create biofilms, compete with other microorganisms, invade dentinal tubules, and resist nutritional deprivation [7,8,9,10]. Root canal disinfection can be achieved by mechanical and chemical means. However, irrigation plays a crucial role. It can reach areas with anatomical complexities including isthmus, fins of the root canal system as well as facilitate the reduction of microbial biofilms. For this purpose, a wide range of irrigating solutions had been used in endodontics and these include sodium hypochlorite (NaOCl) which is known for its dissolution of organic substances property [11], ethylenediaminetetraacetic acid (EDTA), removal of inorganic debris like smear layer [12], chlorhexidine (CHX), its antibacterial effect [13] and MTAD as a root canal disinfectant [14]. However, no single irrigant has been shown to be effective in meeting the objectives of root canal irrigation such as the dissolution of vital or necrotic pulp tissues, disruption of biofilms, neutralization of endotoxins, and removal of smear layer [15,16,17].
QMix (Dentsply Tulsa, Tulsa, OK, USA) was introduced as a single irrigant that can remove the smear layer considering its high antimicrobial property. It contains a mixture of a bisbiguanide antimicrobial agent (2% CHX), a polyaminocarboxylic acid calcium-chelating agent (17% EDTA), saline, and a surfactant [16]. QMix has shown to have superior antimicrobial property compared to CHX in reducing E. faecalis and the ability to remove the smear layer that is similar to EDTA [18,19]. With this inherent ability to remove the smear layer and antimicrobial action, it may require less time for the dentists to disinfect the root canal system effectively. Many studies have compared the antimicrobial property of QMix with other irrigants against E. faecalis showing varying results; some showed stronger antibacterial action at lower volume/timing while some showed contrary results [20,21,22,23,24,25,26,27,28,29,30,31,32,33]. However, to the authors' knowledge, no systematic review has been published to assess the antibacterial efficacy of QMix against E. faecalis. Therefore, the aim of this systematic review was to compare the antibacterial effectiveness of QMix with other commonly employed irrigants against E. faecalis.
MATERIALS AND METHODS
The protocol for this systematic review has been registered with the PROSPERO International prospective register of systematic reviews, registry No. CRD42018096763 and this review followed PRISMA guidelines [34].
The research question was developed by using the population, intervention, comparison, outcome and study design framework: In the extracted permanent human teeth with E. faecalis (P), does QMix irrigant (I) show better antibacterial property (O) compared to the other irrigants (C) from in vitro studies (S).
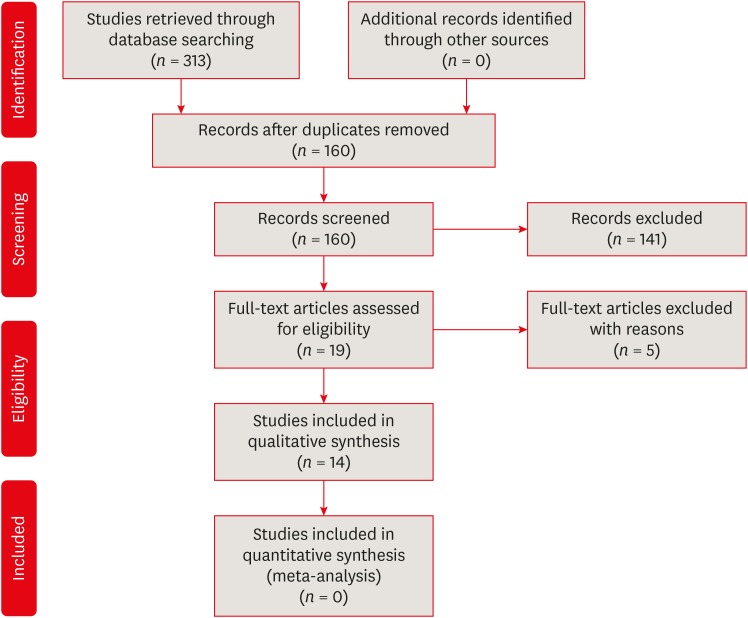
The literature search was performed comprehensively using 3 electronic databases: PubMed, Scopus, and EBSCOhost (Dentistry; Oral Sciences Source) using search strategy (QMix) AND ((root canal) OR endod), from inception to October 2019. The additional literature search was performed from the reference list of the eligible studies. Based on the journals publishing the content relevant to the topic, Journal of Endodontics, International Endodontic Journal, Journal of Dentistry, Australian Endodontic Journal, and Journal of Conservative Dentistry were hand-searched to identify any relevant studies. The search strategy and the articles retrieved through a combination of key words was shown in Figure 1.
Inclusion criteria for this review were: i) Studies performed in the extracted permanent human teeth, ii) studies that compared the antibacterial effect of QMix with at least one irrigant against E. faecalis, iii) antibacterial efficacy assessed by either colony forming units (CFUs) or confocal laser scanning microscopy (CLSM), and iv) studies published in English.
Studies were excluded if they were performed in vivo, on animals or in bovine teeth.
Two reviewers (BL, AP) independently screened the title and abstract of the selected articles based on the specified inclusion and exclusion criteria. The reviewers independently read the articles and extracted the data using the data extraction form exclusively developed for this study. This form consisted of the following details: author, year, country, the total number of samples, type of the teeth, interventions, evaluation method, results based on the antimicrobial property, irrigation time, and irrigation volume. Any disagreement between the 2 reviewers was resolved by discussion with a third reviewer (JJ).
The quality of each article was assessed using the revised Cochrane Risk of Bias tool (RoB 2.0, Cochrane Methods, London, UK) [35]. This tool was modified to include the contents based on the methodology employed in the included in vitro studies. The quality of included studies was assessed based on the following domains: randomization process, deviations from intended intervention, verification of the presence of E. faecalis, the protocol for biofilm formation (21 days), smear layer removal prior to E. faecalis inoculation and irrigating regimen (volume, duration). Two authors (BL, AP) independently evaluated and scored the articles based on the above domains. In case of disagreement, a consensus was reached in discussion with another reviewer (JJ).
RESULTS
A total of 313 studies were identified from the electronic databases. After excluding studies based on title and abstract screening, 19 articles were available for full-text assessment. On careful reading, further 5 studies were excluded for the following reasons: studies were done on agar plate [16], on mixed plaque suspension [18], on bovine teeth [36], QMix as a control variable [37], and QMix used in combination with other irrigants and was not tested individually [38]. Finally, 14 studies were included in the systematic review. The search process employed to identify included studies was shown in Figure 1. We did not perform a meta-analysis due to the presence of heterogeneity in the methodology and reporting antibacterial outcomes of the included studies. Most of the studies reported the remaining E. faecalis log CFUs with mean and standard deviation [20,23,27,30,31]. However, a limited number of studies reported the data in median and percentiles [21,22,32,33]. Within the mean scores, variations were observed in reporting the log CFU mean scores that were represented in different units [24,26,27,28,29]. It was not possible to collate the information from the included studies that rendered difficulty in quantitatively evaluating the extracted data.
Out of 14 studies, 12 studies included single-rooted teeth [21,22,23,24,25,26,27,28,29,30,31,33]. One study contained both maxillary and mandibular molars [20], and 1 study included mandibular incisors and maxillary second premolars [32]. Five studies were done in dentin blocks or discs with specified dimensions [20,22,27,28,29], whereas another 9 studies were done in the root canal [21,23,24,25,26,30,31,32,33]. Six out of these 9 studies mentioned the root length of the tooth sample, at 12 mm [21], 14 mm [23], 15 mm [25,26,31], and 16 mm [33], respectively. Inconsistency was observed in the irrigation protocol in the included studies. One out of 5 studies was done in wells containing dentin blocks and irrigants [20], 3 studies introduced irrigants to the root canal side of the dentin disc [27,28,29], and 1 study did not mention clearly the placement of irrigants to the dentin disc [22]. Four out of 9 studies performed in root canal employed side vented needle for irrigation [21,23,30,32], whereas 5 studies did not mention the details of irrigation [24,25,26,31,33]. The samples were obtained using sterile paper points in 6 studies [21,24,25,26,31,33]. QMix has been compared with various irrigants like EDTA, MTAD, CHX, NaOCl, cetrimide, SilverSol/H2O2, HYBENX, and Gold grape seed extract (GSE) and the antibacterial efficacy was measured by using CFU [20,21,22,23,24,25,26,30,31,32,33] and CLSM [27,28,29]. The characteristics of the included in vitro studies were shown in Table 1.
Table 1
Characteristics of included studies in the systematic review
| No. | Author | Year | Country | Total number of samples | Type of teeth | Interventions (groups) | Evaluation method | Results (gain results (group showing significantly higher bacterial reduction)) | Irrigation time | Irrigation volume |
|---|---|---|---|---|---|---|---|---|---|---|
| 1 | Ma et al. [28] | 2011 | Canada | 12 | Single-rooted teeth | 1. Sterile water | CLSM | QMix and 6% NaOCl killed more bacteria in 1 min than the other solutions in 3 min | 1 and 3 min | 50 μL each irrigant |
| 2. 1% NaOCl | ||||||||||
| 3. 2% NaOCl | ||||||||||
| 4. 6% NaOCl | ||||||||||
| 5. 2% CHX | ||||||||||
| 6. QMix | ||||||||||
| 2 | Wang et al. [27] | 2012 | Canada | 40 | Single-rooted teeth | 1. Sterile water (control) | CLSM | 6% NaOCl and QMix were better and no significant difference was found between the 2 agents | 1 and 3 min | 50 μL each irrigant |
| 2. 2% NaOCl | ||||||||||
| 3. 6% NaOCl | ||||||||||
| 4. 2% CHX | ||||||||||
| 5. QMix | ||||||||||
| 3 | Wang et al. [29] | 2013 | Canada | 40 | Single-rooted teeth | 1. Sterile Water | CLSM | 6% NaOCl + QMix showed the highest level of bacterial killing in 3 min. At 10 min, combinations of 6% NaOCl + QMix and 6% NaOCl + 17% EDTA + 2% CHX were the most effective antibacterial solutions followed by 2% NaOCl + QMix | 3 and 10 min | 50 μL each medicament |
| 2. 2% NaOCl | ||||||||||
| 3. 6% NaOCl | ||||||||||
| 4. 2% CHX | ||||||||||
| 5. 17% EDTA | ||||||||||
| 6. QMix | ||||||||||
| 7. 2% NaOCl + 2% CHX | ||||||||||
| 8. 2% NaOCl + QMiX | ||||||||||
| 9. 6% NaOCl + QMiX | ||||||||||
| 10. 6% NaOCl + 17% EDTA + 2% CHX | ||||||||||
| 4 | Zhang et al. [20] | 2015 | China | 200 | Maxillary and Mandibular molars | 1. 17% EDTA | CFU | QMix group had the lowest logCFU value | 2 min | 100 μL each irrigant |
| 2. 2% CHX | Inoculation time: cultivated under anaerobic conditions at 37°C for 24 hr | |||||||||
| 3. 0.2% Cetrimide | ||||||||||
| 4. MTAD | ||||||||||
| 5. QMix | ||||||||||
| 6. Untreated | ||||||||||
| 5 | Liu et al. [21] | 2015 | China | 62 | Single-rooted maxillary anterior teeth | 1. 17% EDTA/5.25% NaOCl | CFU | EDTA/CHX, EDTA/CTR, or QMix exhibited the greatest antimicrobial activity. No significant differences between these 3 groups | NA | 5 mL each irrigant |
| 2. 17% EDTA/2% CHX | Inoculation time: incubated at 37°C for 48 hr | |||||||||
| 3. 17% EDTA/2% CTR | ||||||||||
| 4. MTAD | ||||||||||
| 5. QMix | ||||||||||
| 6. 0.9% Saline | ||||||||||
| 6 | Elakanti et al. [23] | 2015 | India | 40 | Mandibular premolar teeth | 1. 5.25% NaOCl | CFU | QMix better than 5.25% NaOCl and 2% CHX | 1 min | 3 mL each irrigant |
| 2. 2% CHX | Inoculation time: incubated at 37°C for 24 hr | |||||||||
| 3. QMix | ||||||||||
| 4. 0.9% Saline | ||||||||||
| 7 | Cecchin et al. [25] | 2015 | Brazil | 50 | Single-rooted teeth | 1. 2.5% NaOCl | CFU | CHX and GSE better than NaOCl and QMix | 30 sec | 5 mL each irrigant |
| 2. 2% CHX | Inoculation time: incubated at 37°C for 18 to 24 hr | |||||||||
| 3. 6.5% GSE | ||||||||||
| 4. QMix | ||||||||||
| 5. DW | ||||||||||
| 8 | Bago Jurič et al. [22] | 2016 | Croatia | 65 | Single-rooted teeth | 1. PDT | CFU | NaOCl better followed by PDT, QMix and Nd:YAG | 1 min | 1 mL each irrigant |
| 2. Nd:YAG | Inoculation time: incubated at 37°C for 48 hr | |||||||||
| 3. QMix | ||||||||||
| 4. 5.25% NaOCl | ||||||||||
| 9 | Balić et al. [32] | 2016 | Croatia | 90 | Mandibular incisors and maxillary second premolars | 1. PIPS with 2.5% NaOCl | CFU | The QMix solution showed significantly greater antimicrobial efficacy than 2.5% NaOCl (p = 0.04) when the conventional needle irrigation was used. | 30 sec | 2 mL each irrigant |
| 2. PIPS with QMix | Inoculation time: incubated at 37°C for 48 hr | |||||||||
| 3. Sonic-activated irrigation with 2.5% NaOCl | ||||||||||
| 4. Sonic-activated irrigation with QMix | ||||||||||
| 5. 2.5% NaOCl needle irrigation | ||||||||||
| 6. QMix solution needle irrigation | ||||||||||
| 10 | Vaid et al. [24] | 2017 | India | 190 | Single-rooted anterior teeth | 1. Normal saline | CFU | Maximum percentage of disinfection (99%) was seen in 15 mL of 2.5% NaOCl solution for 3 min and irradiated with PAD which was similar to 15 mL of 2.5% NaOCl for 3 min and 5 mL of 2.5% NaOCl solution, followed by 5 mL of normal saline, and then, 5 mL QMix for 3 min | 3 min | 15 mL of Saline/NaOCl 5 mL of QMix |
| 2. 2.5% NaOCl | Inoculation time: incubated at 37°C for 48 hr | |||||||||
| 3. Qmix | ||||||||||
| 4. Normal saline and PAD | ||||||||||
| 5. 2.5% NaOCl and PAD | ||||||||||
| 6. QMix and PAD | ||||||||||
| 7. No irrigation | ||||||||||
| 11 | Souza et al. [26] | 2017 | Brazil | 60 | Single-rooted teeth | 1. DW | CFU | The greatest bacterial reduction was observed for 2% CHX, QMix and 6.5% GSE, with no statistically significant difference between them. | 5 min | NA |
| 2. 2% CHX | Inoculation time: incubated at 37°C for 18–24 hr | |||||||||
| 3. QMix | ||||||||||
| 4. 6.5% GSE | ||||||||||
| 5. PDT + fiber | ||||||||||
| 6. PDT + no fiber | ||||||||||
| 12 | Ye et al. [30] | 2018 | China | 51 | Single-rooted premolars | 1. 0.9% NaCl | CFU | 6% NaOCl > QMix > HYBENX > SilverSol/H2O2 > 0.9% NaCl SilverSol/H2O2 and HYBENX were less adept than QMix at killing biofilm bacteria in root canals. | 1 min | 6 mL each irrigant |
| 2. 10 ppm SilverSol with 0.1% H2O2 (SilverSol/H2O2) | Inoculation time: incubated at 37°C for 48 hr | |||||||||
| 3. HYBENX | ||||||||||
| 4. QMix | ||||||||||
| 5. 6% NaOCl | ||||||||||
| 13 | Souza et al. [31] | 2018 | Brazil | 60 | Single-rooted | 1. DW | CFU | The greatest ability to promote bacterial reduction was observed in QMix and QMix + US, with no statistically significant difference between them (p < 0.05) | 1 min | NA |
| 2. DW + Ultrasonic | Inoculation time: incubated at 37°C for 18–24 hr | |||||||||
| 3. 17% EDTA | ||||||||||
| 4. QMix | ||||||||||
| 5. 17% EDTA + Ultrasonic | ||||||||||
| 6. QMix + Ultrasonic | ||||||||||
| 14 | Matos et al. [33] | 2019 | Brazil | 40 | Single-rooted | 1. EDTA + MA | CFU | QMix + MA and QMix + PUI had superior antibacterial efficacy to EDTA and eliminated 100% of E. faecalis | 2 min | 3 mL each irrigant |
| 2. QMix + MA | Inoculation time: incubated at 37°C for 24 hr | |||||||||
| 3. EDTA + PUI | ||||||||||
| 4. QMix + PUI |
NA, not available; NaOCl, sodium hypochlorite; CHX, chlorhexidine; CLSM, confocal laser scanning microscopy; EDTA, ethylenediaminetetraacetic acid; CFU, colony forming units; MTAD, mixture of Tetracycline isonomer, an acid and a detergent; log CFU, log colony forming units; GSE, grape seed extract; DW, distilled water; PDT, photodynamic therapy; PIPS, photon-initiated photoacoustic streaming; PAD, photo-activated disinfection; US, ultrasonic activation; MA, manual agitation; PUI, passive ultrasonic irrigation.
The studies were analyzed using the modified Risk of Bias tool and the overall quality of the included studies were found to be “moderate” (Figure 2). Most of the studies followed randomisation process [20,21,22,24,25,26,27,28,29,30,31,32,33] with deviation from intended interventions. The verification of the presence of E. faecalis was not stated in 2 studies [20,25]. Five studies did not follow the protocol for biofilm formation for 21 days [23,26,28,31,32]. Two studies did not follow the protocol for smear layer removal prior to E. faecalis inoculation [21,31]. In the protocol for irrigating regimen, all studies reported information on the volume of irrigants and duration of their use except 3 studies [20,21,26].
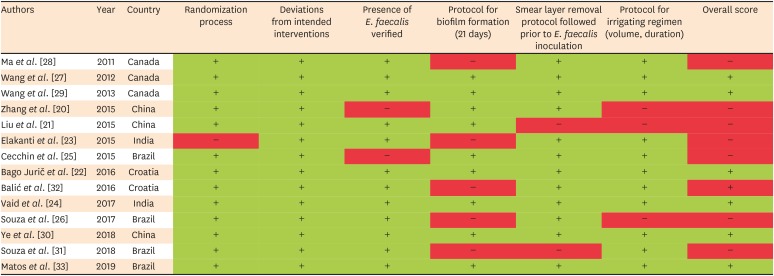
Among the results gathered from the included studies, QMix showed higher antibacterial efficacy if not equal to NaOCl as compared to the other endodontic irrigants tested in the studies. Given the overall moderate risk of bias, standardization is needed to improve the quality and clinical implication of the studies further.
DISCUSSION
The purpose of performing root canal treatment is to remove intracanal microorganisms and to prevent reinfection. Irrigation plays a crucial role in endodontic treatment and facilitates disinfection during and after instrumentation [39]. Thus far, the combination of endodontic irrigation has been commonly employed in root canal treatment to achieve both organic dissolution and removal of inorganic substance. QMix was known for its single irrigant that has both antibacterial and smear layer removal properties [18,19]. Various studies have been published on QMix compared to other commonly used irrigants [20,21,22,23,24,25,26,27,28,29,30,31,32,33]. Although it would be appropriate to test the effectiveness of QMix in vivo setting, no study was done in that manner. For the above reason, only in vitro studies were included in this systematic review.
Four studies showed that 5% to 6% NaOCl was more effective than QMix against E. faecalis biofilm when 1 mL was used for 1 and 3 minutes [22,27,29,30]. However, another study showed no difference between 6% NaOCl and QMix at 1 and 3 minutes of exposure [28]. QMix was more effective than lower concentration of NaOCl (1%, 2%, and 2.5%) at 30 seconds, 1 and 3 minutes' exposure [22,27,28,29,32]. Similarly, QMix was more effective than 5% to 6% NaOCl when used for one [23] and 10 minutes with a volume of 3 mL [29]. QMix showed better antibacterial property compared to NaOCl, when QMix was employed for longer exposure time [29] and at higher volume [23]. In one study, QMix showed no significant difference compared to 2.5% NaOCl when used with different activation systems [32]. Five studies showed that QMix was more effective than 2% CHX against E. faecalis biofilm [20,23,27,28,29], whereas one study showed no difference between QMix and 2% CHX [26]. The superior antibacterial effect of QMix was probably due to its ability to remove the smear layer, and a gradual antibacterial effect on the dentin bacteria through a synergistic effect [28,29]. QMix showed higher antimicrobial activity compared to 17% EDTA [20,29,31,33], MTAD [20], 0.2% Cetrimide [20], Nd:YAG laser [22], SilverSol/H2O2 [30], and HYBENX [30] against E. faecalis biofilm. It is interesting to note that QMix had similar antibacterial effectiveness against E. faecalis biofilm when compared to GSE [26] and photodynamic therapy (PDT) [22]. Considering all the materials, QMix showed higher antimicrobial activity compared to 17% EDTA, 2% CHX, MTAD, 0.2% Cetrimide, SilverSol/H2O2, and HYBENX. Three studies included in the review were conducted by a research team with a potential financial interest in QMix product [27,28,29]. The above studies have been published after robust peer review, and hence we consider that the results from these studies would not have affected the outcome of this review.
CFU methodology has been widely used for microbiological analysis of bacteria inside the dentinal tubules. Although it was able to provide a reading of the bacterial colony that had invaded the dentinal tubules, it was unable to analyze the spatial distribution and viability of the bacteria. In contrast, CLSM was capable of showing intact undisturbed biological samples with optical sections as thin as 0.3 μm. When used with vital staining techniques, it showed the viability profile and spatial distribution of the examined bacteria [40,41]. In addition, it showed consistent results of ranking when used in various studies on the antibacterial activity of disinfecting agents [29]. The CLSM has the ability to eliminate scattered light and focus on individual bacterial cells inside the dentinal tubules. It has been shown that CLSM is a better method to study the bacterial viability in endodontics [41]. Therefore, in order to critically evaluate both the amount and viability of E. faecalis in the root canal system after irrigation, both CFU and CLSM microbiological analysis have been evaluated in this review. By doing so, this had portrayed a clearer picture of the antimicrobial efficacy of QMix irrigant.
In our review, we have modified the revised Cochrane ROB based on the characteristics of the included in vitro studies. Six parameters (randomization process, deviations from intended interventions, verification of E. faecalis, protocol for biofilm formation [21 days], smear layer removal protocol followed prior to E. faecalis inoculation, and protocol for irrigating regimen based on volume and duration) have been used to appraise the quality of included studies as showed in Figure 2. All studies satisfied deviations from the intended interventions parameter. The evaluation of E. faecalis with CFU counts varies with inoculation time. Out of 10 studies, the inoculation time of E. faecalis was 24 hours for 6 studies [20,23,25,26,31,33], whilst in 5 studies, it was done at 48 hours [21,22,24,30,32]. Verification of E. faecalis was an essential step in the study design, which helps to confirm the presence and spread of E. faecalis biofilm [28]. The average time taken for the formation of mature biofilm is around 21 days, and this duration was crucial to assess the effectiveness of any disinfectant against the mature biofilm [27]. Wang et al. [27] showed that mature E. faecalis biofilms in dentin canals at 21 days are more resistant to disinfecting solutions than young biofilms. Hence, we included the protocol for biofilm formation at 21 days as one of the domains for assessing the quality of studies. Smear layer removal protocol prior to E. faecalis inoculation was essential because the smear layer prevents the penetration of microorganisms into the root canal and reduces the effectiveness of disinfecting agents against E. faecalis [29]. Additionally, bacteria remaining in dentinal tubules after root canal preparation may be sealed by the smear layer [42]. In such cases, antibacterial solutions used for root canal disinfection have to penetrate or remove the smear layer to attack the bacteria in the infected dentin. Hence, if the smear layer was not completely removed, in microbial studies, this might show false-positive or false-negative results. Studies have shown that the antimicrobial effect was affected by the volume and concentration of the irrigant. This is apparent in this review as QMix showed better effect when used in higher volume (above 3 mL) and for a longer time (above 10 minutes) [23,29].
The studies included in this review showed substantial differences in their study design. The experimental subject models were not consistent. For example, some studies were done using dentin disc and some in the closed root canal system. Moreover, placement methods of irrigants varied between each study. Studies that were performed in dentin discs, irrigants were added in the wells, whereas experiments done in the root canal employed needle syringe irrigation. The efficacy of irrigants is affected by the vapor lock formation in a closed root canal system surrounded by periodontium [43,44]. Hence, the root canal system should be preferred over the dentin disc to simulate the actual endodontic procedure in clinical scenarios. Despite studies mentioned E. faecalis as the most persistent microorganism in intra-radicular infections hence the inclusion criteria, however, biofilm comprising of multiple microorganisms will give a higher impact factor in clinical relevance. It is strongly recommended to use CLSM to study the antibacterial viability properly. Further, in vitro and in vivo studies are required to check the antibacterial efficacy of QMix against other endodontic pathogens. The clinical relevance of the effect of a root canal disinfection solution considering a single bacterium remains unclear in general.
CONCLUSIONS
This systematic review on the antibacterial efficacy of QMix against E. faecalis reveals superior to the usage of single irrigation solution (2% CHX, MTAD, 17% EDTA, 0.2% Cetrimide, SilverSol/H2O2, HYBENX, and low concentration NaOCl) and it is a promising alternative to the commonly employed irrigation protocols. To improve the effectiveness, it is recommended to use QMix for a longer time and at a higher volume.
-
Conflict of Interest: No potential conflict of interest relevant to this article was reported.
-
Author Contributions:
Conceptualization: Parolia A.
Data curation: Lim BSH, Chia MSY.
Formal analysis: Jayaraman J.
Investigation: Lim BSH, Chia MSY.
Methodology: Parolia A, Lim BSH.
Project administration: Parolia A.
Resources: Parolia A.
Supervision: Parolia A.
Validation: Jayaraman J, Nagendrababu V.
Visualization: Parolia A.
Writing - original draft: Lim BSH, Parolia A.
Writing - review & editing: Lim BSH, Parolia A, Jayaraman J, Nagendrababu V.
- 1. Vieira AR, Siqueira JF Jr, Ricucci D, Lopes WS. Dentinal tubule infection as the cause of recurrent disease and late endodontic treatment failure: a case report. J Endod 2012;38:250-254.ArticlePubMed
- 2. Nair PN, Sjögren U, Krey G, Kahnberg KE, Sundqvist G. Intraradicular bacteria and fungi in root-filled, asymptomatic human teeth with therapy-resistant periapical lesions: a long-term light and electron microscopic follow-up study. J Endod 1990;16:580-588.ArticlePubMed
- 3. Neelakantan P, Romero M, Vera J, Daood U, Khan AU, Yan A, Cheung GSP. Biofilms in endodontics-current status and future directions. Int J Mol Sci 2017;18:E1748.ArticlePubMedPMC
- 4. Song M, Kim HC, Lee W, Kim E. Analysis of the cause of failure in nonsurgical endodontic treatment by microscopic inspection during endodontic microsurgery. J Endod 2011;37:1516-1519.ArticlePubMed
- 5. Love RM. Enterococcus faecalis--a mechanism for its role in endodontic failure. Int Endod J 2001;34:399-405.ArticlePubMedPDF
- 6. Wang QQ, Zhang CF, Chu CH, Zhu XF. Prevalence of Enterococcus faecalis in saliva and filled root canals of teeth associated with apical periodontitis. Int J Oral Sci 2012;4:19-23.ArticlePubMedPMCPDF
- 7. Zhang C, Du J, Peng Z. Correlation between Enterococcus faecalis and persistent intraradicular infection compared with primary intraradicular infection: a systematic review. J Endod 2015;41:1207-1213.ArticlePubMed
- 8. Pinheiro ET, Gomes BP, Ferraz CC, Teixeira FB, Zaia AA, Souza Filho FJ. Evaluation of root canal microorganisms isolated from teeth with endodontic failure and their antimicrobial susceptibility. Oral Microbiol Immunol 2003;18:100-103.ArticlePubMedPDF
- 9. Rossi-Fedele G, Roberts AP. A preliminary study investigating the survival of tetracycline resistant Enterococcus faecalis after root canal irrigation with high concentrations of tetracycline. Int Endod J 2007;40:772-777.ArticlePubMed
- 10. Sedgley CM, Lennan SL, Appelbe OK. Survival of Enterococcus faecalis in root canals ex vivo . Int Endod J 2005;38:735-742.ArticlePubMed
- 11. Zehnder M. Root canal irrigants. J Endod 2006;32:389-398.ArticlePubMed
- 12. Hülsmann M, Heckendorff M, Lennon A. Chelating agents in root canal treatment: mode of action and indications for their use. Int Endod J 2003;36:810-830.ArticlePubMedPDF
- 13. Weber CD, McClanahan SB, Miller GA, Diener-West M, Johnson JD. The effect of passive ultrasonic activation of 2% chlorhexidine or 5.25% sodium hypochlorite irrigant on residual antimicrobial activity in root canals. J Endod 2003;29:562-564.ArticlePubMed
- 14. Johal S, Baumgartner JC, Marshall JG. Comparison of the antimicrobial efficacy of 1.3% NaOCl/BioPure MTAD to 5.25% NaOCl/15% EDTA for root canal irrigation. J Endod 2007;33:48-51.ArticlePubMed
- 15. Siqueira JF Jr, Rôças IN. Optimising single-visit disinfection with supplementary approaches: a quest for predictability. Aust Endod J 2011;37:92-98.ArticlePubMed
- 16. Jose J, Krishnamma S, Peedikayil F, Aman S, Tomy N, Mariodan JP. Comparative evaluation of antimicrobial activity of QMix, 2.5% sodium hypochlorite, 2% chlorhexidine, guava leaf extract and aloevera extract against Enterococcus faecalis and candida albicans: an in-vitro study. J Clin Diagn Res 2016;10:ZC20-ZC23.ArticlePubMedPMC
- 17. Goldman LB, Goldman M, Kronman JH, Lin PS. The efficacy of several irrigating solutions for endodontics: a scanning electron microscopic study. Oral Surg Oral Med Oral Pathol 1981;52:197-204.ArticlePubMed
- 18. Stojicic S, Shen Y, Qian W, Johnson B, Haapasalo M. Antibacterial and smear layer removal ability of a novel irrigant, QMiX. Int Endod J 2012;45:363-371.ArticlePubMed
- 19. Dai L, Khechen K, Khan S, Gillen B, Loushine BA, Wimmer CE, Gutmann JL, Pashley D, Tay FR. The effect of QMix, an experimental antibacterial root canal irrigant, on removal of canal wall smear layer and debris. J Endod 2011;37:80-84.ArticlePubMed
- 20. Zhang R, Chen M, Lu Y, Guo X, Qiao F, Wu L. Antibacterial and residual antimicrobial activities against Enterococcus faecalis biofilm: a comparison between EDTA, chlorhexidine, cetrimide, MTAD and QMix. Sci Rep 2015;5:12944.ArticlePubMedPMCPDF
- 21. Liu Y, Guo L, Li Y, Guo X, Wang B, Wu L. In vitro comparison of antimicrobial effectiveness of QMix and other final irrigants in human root canals. Sci Rep 2015;5:17823.ArticlePubMedPMCPDF
- 22. Bago Jurič I, Plečko V, Anić I, Pleško S, Jakovljević S, Rocca JP, Medioni E. Antimicrobial efficacy of photodynamic therapy, Nd:YAG laser and QMiX solution against Enterococcus faecalis biofilm. Photodiagnosis Photodyn Ther 2016;13:238-243.ArticlePubMed
- 23. Elakanti S, Cherukuri G, Rao VG, Chandrasekhar V, Rao AS, Tummala M. Comparative evaluation of antimicrobial efficacy of QMix™ 2 in 1, sodium hypochlorite, and chlorhexidine against Enterococcus faecalis and Candida albicans. J Conserv Dent 2015;18:128-131.ArticlePubMedPMC
- 24. Vaid D, Shah N, Kothari D, Bilgi P. Additive effect of photoactivated disinfection on the antibacterial activity of QMix 2in1 against 6-week Enterococcus faecalis biofilms: an in vitro study. J Conserv Dent 2017;20:41-45.ArticlePubMedPMC
- 25. Cecchin D, Farina AP, Souza MA, Albarello LL, Schneider AP, Vidal CM, Bedran-Russo AK. Evaluation of antimicrobial effectiveness and dentine mechanical properties after use of chemical and natural auxiliary irrigants. J Dent 2015;43:695-702.ArticlePubMed
- 26. Souza MA, Dalla Lana D, Gabrielli E, Barbosa Ribeiro M, Miyagaki DC, Cecchin D. Effectiveness of final decontamination protocols against Enterococcus faecalis and its influence on bond strength of filling material to root canal dentin. Photodiagnosis Photodyn Ther 2017;17:92-97.ArticlePubMed
- 27. Wang Z, Shen Y, Haapasalo M. Effectiveness of endodontic disinfecting solutions against young and old Enterococcus faecalis biofilms in dentin canals. J Endod 2012;38:1376-1379.ArticlePubMed
- 28. Ma J, Wang Z, Shen Y, Haapasalo M. A new noninvasive model to study the effectiveness of dentin disinfection by using confocal laser scanning microscopy. J Endod 2011;37:1380-1385.ArticlePubMed
- 29. Wang Z, Shen Y, Haapasalo M. Effect of smear layer against disinfection protocols on Enterococcus faecalis-infected dentin. J Endod 2013;39:1395-1400.ArticlePubMed
- 30. Ye WH, Fan B, Purcell W, Meghil MM, Cutler CW, Bergeron BE, Ma JZ, Tay FR, Niu LN. Anti-biofilm efficacy of root canal irrigants against in-situ Enterococcus faecalis biofilms in root canals, isthmuses and dentinal tubules. J Dent 2018;79:68-76.ArticlePubMed
- 31. Souza MA, Hoffmann IP, Menchik VH, Zandoná J, Dias CT, Palhano HS, Bertol CD, Rossato-Grando LG. Influence of ultrasonic activation using different final irrigants on antimicrobial activity, smear layer removal and bond strength of filling material. Aust Endod J 2019;45:209-215.ArticlePubMedPDF
- 32. Balić M, Lucić R, Mehadžić K, Bago I, Anić I, Jakovljević S, Plečko V. The efficacy of photon-initiated photoacoustic streaming and sonic-activated irrigation combined with QMiX solution or sodium hypochlorite against intracanal E. faecalis biofilm. Lasers Med Sci 2016;31:335-342.ArticlePubMedPDF
- 33. Matos FS, Khoury RD, Carvalho CA, Martinho FC, Bresciani E, Valera MC. Effect of EDTA and QMIX ultrasonic activation on the reduction of microorganisms and endotoxins in ex vivo human root canals. Braz Dent J 2019;30:220-226.ArticlePubMed
- 34. Moher D, Liberati A, Tetzlaff J, Altman DG; PRISMA Group. Preferred reporting items for systematic reviews and meta-analyses: the PRISMA statement. PLoS Med 2009;6:e1000097.ArticlePubMedPMC
- 35. Higgins JP, Sterne JA, Savović J, Page MJ, Hróbjartsson A, Boutron I, Reeves B, Eldridge S. A revised tool for assessing risk of bias in randomized trials. Cochrane Database Syst Rev 2016;10:S29-S31.
- 36. Giardino L, Andrade FB, Beltrami R. Antimicrobial effect and surface tension of some chelating solutions with added surfactants. Braz Dent J 2016;27:584-588.ArticlePubMed
- 37. Bortoluzzi EA, Carlon D Jr, Meghil MM, El-Awady AR, Niu L, Bergeron BE, Susin L, Cutler CW, Pashley DH, Tay FR. Efficacy of 3D conforming nickel titanium rotary instruments in eliminating canal wall bacteria from oval-shaped root canals. J Dent 2015;43:597-604.ArticlePubMed
- 38. Batinić M, Ročan M, Budimir A, Anić I, Bago I. Comparison of final disinfection protocols using antimicrobial photodynamic therapy and different irrigants after single-file reciprocating instrumentation against intracanal bacterial biofilm: an in vitro study. Photodiagnosis Photodyn Ther 2018;24:153-157.ArticlePubMed
- 39. Haapasalo M, Shen Y, Qian W, Gao Y. Irrigation in endodontics. Dent Clin North Am 2010;54:291-312.ArticlePubMed
- 40. Parmar D, Hauman CH, Leichter JW, McNaughton A, Tompkins GR. Bacterial localization and viability assessment in human ex vivo dentinal tubules by fluorescence confocal laser scanning microscopy. Int Endod J 2011;44:644-651.ArticlePubMed
- 41. Zapata RO, Bramante CM, de Moraes IG, Bernardineli N, Gasparoto TH, Graeff MS, Campanelli AP, Garcia RB. Confocal laser scanning microscopy is appropriate to detect viability of Enterococcus faecalis in infected dentin. J Endod 2008;34:1198-1201.ArticlePubMed
- 42. Drake DR, Wiemann AH, Rivera EM, Walton RE. Bacterial retention in canal walls in vitro: effect of smear layer. J Endod 1994;20:78-82.ArticlePubMed
- 43. de Gregorio C, Estevez R, Cisneros R, Heilborn C, Cohenca N. Effect of EDTA, sonic, and ultrasonic activation on the penetration of sodium hypochlorite into simulated lateral canals: an in vitro study. J Endod 2009;35:891-895.ArticlePubMed
- 44. de Gregorio C, Estevez R, Cisneros R, Paranjpe A, Cohenca N. Efficacy of different irrigation and activation systems on the penetration of sodium hypochlorite into simulated lateral canals and up to working length: an in vitro study. J Endod 2010;36:1216-1221.ArticlePubMed
REFERENCES
Tables & Figures
REFERENCES
Citations
Citations to this article as recorded by 
- Smear layer removal and antimicrobial efficacy of chitosan as a root canal irrigant: a systematic review of in-vitro studies
Karthikeyan Anbalagan, Amit Jena, Saumyakanta Mohanty, Rashmirekha Mallick, Govind Shashirekha, Priyanka Sarangi
Odontology.2025; 113(1): 61. CrossRef - Mapping risk of bias criteria in systematic reviews of in vitro endodontic studies: an umbrella review
Rafaella Rodrigues da Gama, Lucas Peixoto de Araújo, Evandro Piva, Leandro Perello Duro, Adriana Fernandes da Silva, Wellington Luiz de Oliveira da Rosa
Evidence-Based Dentistry.2025; 26(4): 179. CrossRef - Limosilactobacillus Fermentun ZS09 Can Improve Antibiotic-Induced Motor Dysfunction in Mice by Regulating the Brain–Gut Functions
Yang Yang, Yuanji Zhao, Huan Lei, Xiaohong Tan
Journal of Inflammation Research.2024; Volume 17: 10093. CrossRef - Regulation of colon injury and improvement of exercise performance in exhausted running mice by Lactobacillus pentosus CQZC02
Limin Cai, Beibei Wang
Frontiers in Physiology.2024;[Epub] CrossRef - A Local Desiccant Antimicrobial Agent as an Alternative to Adjunctive Antibiotics in the Treatment of Periodontitis: A Narrative Review
Iulia C. Micu, Alexandrina Muntean, Alexandra Roman, Ștefan I. Stratul, Emöke Pall, Andreea Ciurea, Andrada Soancă, Marius Negucioiu, Lucian Barbu Tudoran, Ada G. Delean
Antibiotics.2023; 12(3): 456. CrossRef -
An
in-vitro
analysis to evaluate the disinfection effectiveness of Cold Atmospheric Pressure (CAP) plasma jet in
Enterococcus faecalis
infected root canals
Pravin Kumar, P. Soundharrajan, Ram Prakash, Sarika Prabhakar Kombade, Pankaj Yadav, Ankita Chugh, Arun Kumar Patnana
Biomaterial Investigations in Dentistry.2023;[Epub] CrossRef - Effect of two graphene derivatives on Enterococcus faecalis biofilms and cytotoxicity
Mi-Ah KIM, Vinicius ROSA, Kyung-San MIN
Dental Materials Journal.2023; 42(2): 211. CrossRef - Antibacterial Activity of Endodontic Gutta-Percha—A Systematic Review
Jakub Kowalski, Joanna Rygas, Karolina Homa, Wojciech Dobrzyński, Rafal J. Wiglusz, Jacek Matys, Maciej Dobrzyński
Applied Sciences.2023; 14(1): 388. CrossRef - Evaluation of the Antibacterial Efficacy of QMix and AgNP Solutions in Root Canals of Primary Molars: An In-Vitro Study
Dania Alkhourbotly, Mohamed K Altinawi, Rouaida Abou-Samra, Hasan M Alzoubi, Abedulrahman K Ebrahim
Cureus.2022;[Epub] CrossRef - Microbiological Aspects of Root Canal Infections and Disinfection Strategies: An Update Review on the Current Knowledge and Challenges
Jasmine Wong, Daniel Manoil, Peggy Näsman, Georgios N. Belibasakis, Prasanna Neelakantan
Frontiers in Oral Health.2021;[Epub] CrossRef
 ePub Link
ePub Link Cite
CiteAntimicrobial efficacy of QMix on Enterococcus faecalis infected root canals: a systematic review of in vitro studies
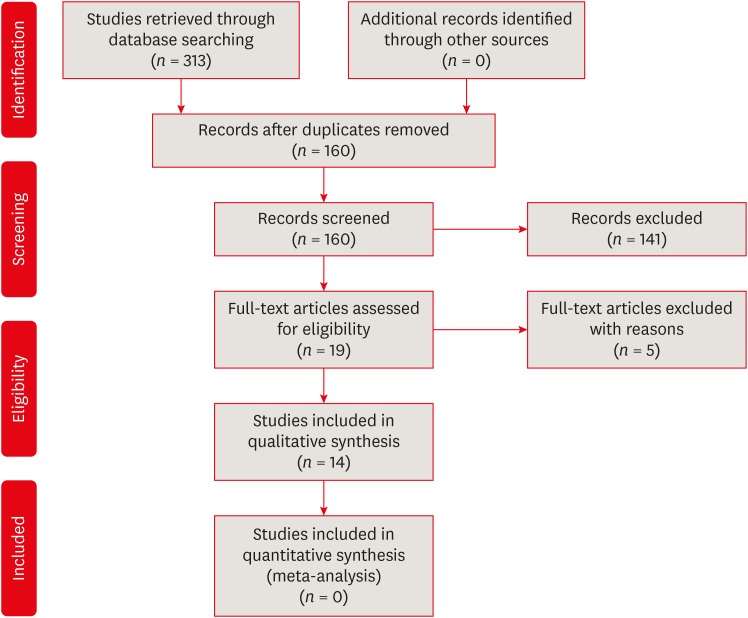
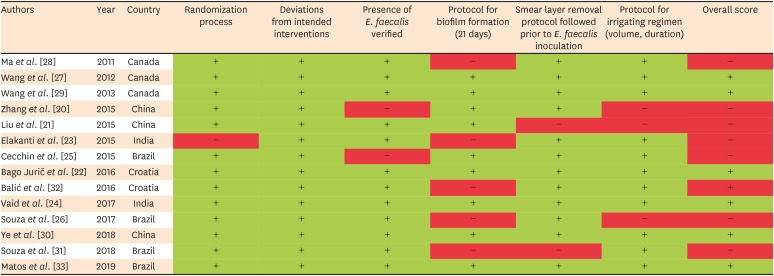
Figure 1 A flowchart of the literature search process.
Figure 2 Risk of bias assessment of included studies.+, low risk of bias; −, high risk of bias.
Figure 1
Figure 2
Antimicrobial efficacy of QMix on Enterococcus faecalis infected root canals: a systematic review of in vitro studies
Characteristics of included studies in the systematic review
| No. | Author | Year | Country | Total number of samples | Type of teeth | Interventions (groups) | Evaluation method | Results (gain results (group showing significantly higher bacterial reduction)) | Irrigation time | Irrigation volume |
|---|---|---|---|---|---|---|---|---|---|---|
| 1 | Ma et al. [ | 2011 | Canada | 12 | Single-rooted teeth | 1. Sterile water | CLSM | QMix and 6% NaOCl killed more bacteria in 1 min than the other solutions in 3 min | 1 and 3 min | 50 μL each irrigant |
| 2. 1% NaOCl | ||||||||||
| 3. 2% NaOCl | ||||||||||
| 4. 6% NaOCl | ||||||||||
| 5. 2% CHX | ||||||||||
| 6. QMix | ||||||||||
| 2 | Wang et al. [ | 2012 | Canada | 40 | Single-rooted teeth | 1. Sterile water (control) | CLSM | 6% NaOCl and QMix were better and no significant difference was found between the 2 agents | 1 and 3 min | 50 μL each irrigant |
| 2. 2% NaOCl | ||||||||||
| 3. 6% NaOCl | ||||||||||
| 4. 2% CHX | ||||||||||
| 5. QMix | ||||||||||
| 3 | Wang et al. [ | 2013 | Canada | 40 | Single-rooted teeth | 1. Sterile Water | CLSM | 6% NaOCl + QMix showed the highest level of bacterial killing in 3 min. At 10 min, combinations of 6% NaOCl + QMix and 6% NaOCl + 17% EDTA + 2% CHX were the most effective antibacterial solutions followed by 2% NaOCl + QMix | 3 and 10 min | 50 μL each medicament |
| 2. 2% NaOCl | ||||||||||
| 3. 6% NaOCl | ||||||||||
| 4. 2% CHX | ||||||||||
| 5. 17% EDTA | ||||||||||
| 6. QMix | ||||||||||
| 7. 2% NaOCl + 2% CHX | ||||||||||
| 8. 2% NaOCl + QMiX | ||||||||||
| 9. 6% NaOCl + QMiX | ||||||||||
| 10. 6% NaOCl + 17% EDTA + 2% CHX | ||||||||||
| 4 | Zhang et al. [ | 2015 | China | 200 | Maxillary and Mandibular molars | 1. 17% EDTA | CFU | QMix group had the lowest logCFU value | 2 min | 100 μL each irrigant |
| 2. 2% CHX | Inoculation time: cultivated under anaerobic conditions at 37°C for 24 hr | |||||||||
| 3. 0.2% Cetrimide | ||||||||||
| 4. MTAD | ||||||||||
| 5. QMix | ||||||||||
| 6. Untreated | ||||||||||
| 5 | Liu et al. [ | 2015 | China | 62 | Single-rooted maxillary anterior teeth | 1. 17% EDTA/5.25% NaOCl | CFU | EDTA/CHX, EDTA/CTR, or QMix exhibited the greatest antimicrobial activity. No significant differences between these 3 groups | NA | 5 mL each irrigant |
| 2. 17% EDTA/2% CHX | Inoculation time: incubated at 37°C for 48 hr | |||||||||
| 3. 17% EDTA/2% CTR | ||||||||||
| 4. MTAD | ||||||||||
| 5. QMix | ||||||||||
| 6. 0.9% Saline | ||||||||||
| 6 | Elakanti et al. [ | 2015 | India | 40 | Mandibular premolar teeth | 1. 5.25% NaOCl | CFU | QMix better than 5.25% NaOCl and 2% CHX | 1 min | 3 mL each irrigant |
| 2. 2% CHX | Inoculation time: incubated at 37°C for 24 hr | |||||||||
| 3. QMix | ||||||||||
| 4. 0.9% Saline | ||||||||||
| 7 | Cecchin et al. [ | 2015 | Brazil | 50 | Single-rooted teeth | 1. 2.5% NaOCl | CFU | CHX and GSE better than NaOCl and QMix | 30 sec | 5 mL each irrigant |
| 2. 2% CHX | Inoculation time: incubated at 37°C for 18 to 24 hr | |||||||||
| 3. 6.5% GSE | ||||||||||
| 4. QMix | ||||||||||
| 5. DW | ||||||||||
| 8 | Bago Jurič et al. [ | 2016 | Croatia | 65 | Single-rooted teeth | 1. PDT | CFU | NaOCl better followed by PDT, QMix and Nd:YAG | 1 min | 1 mL each irrigant |
| 2. Nd:YAG | Inoculation time: incubated at 37°C for 48 hr | |||||||||
| 3. QMix | ||||||||||
| 4. 5.25% NaOCl | ||||||||||
| 9 | Balić et al. [ | 2016 | Croatia | 90 | Mandibular incisors and maxillary second premolars | 1. PIPS with 2.5% NaOCl | CFU | The QMix solution showed significantly greater antimicrobial efficacy than 2.5% NaOCl (p = 0.04) when the conventional needle irrigation was used. | 30 sec | 2 mL each irrigant |
| 2. PIPS with QMix | Inoculation time: incubated at 37°C for 48 hr | |||||||||
| 3. Sonic-activated irrigation with 2.5% NaOCl | ||||||||||
| 4. Sonic-activated irrigation with QMix | ||||||||||
| 5. 2.5% NaOCl needle irrigation | ||||||||||
| 6. QMix solution needle irrigation | ||||||||||
| 10 | Vaid et al. [ | 2017 | India | 190 | Single-rooted anterior teeth | 1. Normal saline | CFU | Maximum percentage of disinfection (99%) was seen in 15 mL of 2.5% NaOCl solution for 3 min and irradiated with PAD which was similar to 15 mL of 2.5% NaOCl for 3 min and 5 mL of 2.5% NaOCl solution, followed by 5 mL of normal saline, and then, 5 mL QMix for 3 min | 3 min | 15 mL of Saline/NaOCl 5 mL of QMix |
| 2. 2.5% NaOCl | Inoculation time: incubated at 37°C for 48 hr | |||||||||
| 3. Qmix | ||||||||||
| 4. Normal saline and PAD | ||||||||||
| 5. 2.5% NaOCl and PAD | ||||||||||
| 6. QMix and PAD | ||||||||||
| 7. No irrigation | ||||||||||
| 11 | Souza et al. [ | 2017 | Brazil | 60 | Single-rooted teeth | 1. DW | CFU | The greatest bacterial reduction was observed for 2% CHX, QMix and 6.5% GSE, with no statistically significant difference between them. | 5 min | NA |
| 2. 2% CHX | Inoculation time: incubated at 37°C for 18–24 hr | |||||||||
| 3. QMix | ||||||||||
| 4. 6.5% GSE | ||||||||||
| 5. PDT + fiber | ||||||||||
| 6. PDT + no fiber | ||||||||||
| 12 | Ye et al. [ | 2018 | China | 51 | Single-rooted premolars | 1. 0.9% NaCl | CFU | 6% NaOCl > QMix > HYBENX > SilverSol/H2O2 > 0.9% NaCl SilverSol/H2O2 and HYBENX were less adept than QMix at killing biofilm bacteria in root canals. | 1 min | 6 mL each irrigant |
| 2. 10 ppm SilverSol with 0.1% H2O2 (SilverSol/H2O2) | Inoculation time: incubated at 37°C for 48 hr | |||||||||
| 3. HYBENX | ||||||||||
| 4. QMix | ||||||||||
| 5. 6% NaOCl | ||||||||||
| 13 | Souza et al. [ | 2018 | Brazil | 60 | Single-rooted | 1. DW | CFU | The greatest ability to promote bacterial reduction was observed in QMix and QMix + US, with no statistically significant difference between them (p < 0.05) | 1 min | NA |
| 2. DW + Ultrasonic | Inoculation time: incubated at 37°C for 18–24 hr | |||||||||
| 3. 17% EDTA | ||||||||||
| 4. QMix | ||||||||||
| 5. 17% EDTA + Ultrasonic | ||||||||||
| 6. QMix + Ultrasonic | ||||||||||
| 14 | Matos et al. [ | 2019 | Brazil | 40 | Single-rooted | 1. EDTA + MA | CFU | QMix + MA and QMix + PUI had superior antibacterial efficacy to EDTA and eliminated 100% of E. faecalis | 2 min | 3 mL each irrigant |
| 2. QMix + MA | Inoculation time: incubated at 37°C for 24 hr | |||||||||
| 3. EDTA + PUI | ||||||||||
| 4. QMix + PUI |
NA, not available; NaOCl, sodium hypochlorite; CHX, chlorhexidine; CLSM, confocal laser scanning microscopy; EDTA, ethylenediaminetetraacetic acid; CFU, colony forming units; MTAD, mixture of Tetracycline isonomer, an acid and a detergent; log CFU, log colony forming units; GSE, grape seed extract; DW, distilled water; PDT, photodynamic therapy; PIPS, photon-initiated photoacoustic streaming; PAD, photo-activated disinfection; US, ultrasonic activation; MA, manual agitation; PUI, passive ultrasonic irrigation.
Table 1 Characteristics of included studies in the systematic review
NA, not available; NaOCl, sodium hypochlorite; CHX, chlorhexidine; CLSM, confocal laser scanning microscopy; EDTA, ethylenediaminetetraacetic acid; CFU, colony forming units; MTAD, mixture of Tetracycline isonomer, an acid and a detergent; log CFU, log colony forming units; GSE, grape seed extract; DW, distilled water; PDT, photodynamic therapy; PIPS, photon-initiated photoacoustic streaming; PAD, photo-activated disinfection; US, ultrasonic activation; MA, manual agitation; PUI, passive ultrasonic irrigation.

