
Articles
- Page Path
- HOME > Restor Dent Endod > Volume 45(2); 2020 > Article
- Review Article Age-dependent root canal instrumentation techniques: a comprehensive narrative review
-
Michael Solomonov1
 , Hyeon-Cheol Kim2, Avi Hadad1, Dan Henry Levy1, Joe Ben Itzhak1, Oleg Levinson3, Hadas Azizi1
, Hyeon-Cheol Kim2, Avi Hadad1, Dan Henry Levy1, Joe Ben Itzhak1, Oleg Levinson3, Hadas Azizi1 -
Restor Dent Endod 2020;45(2):e21.
DOI: https://doi.org/10.5395/rde.2020.45.e21
Published online: March 4, 2020
1Department of Endodontics, Israel Defense Forces (IDF) Medical Corps, Tel Hashomer, Israel.
2Department of Conservative Dentistry, School of Dentistry, Dental Research Institute, Pusan National University, Yangsan, Korea.
3Private Practice, Tel Aviv, Israel.
- Correspondence to Hyeon-Cheol Kim, DDS, MS, PhD. Professor, Department of Conservative Dentistry, School of Dentistry, Pusan National University, 20 Geumo-ro, Mulgeum-eup, Yangsan 50612, Korea. golddent@pusan.ac.kr
• Received: September 4, 2019 • Revised: November 20, 2019 • Accepted: November 20, 2019
Copyright © 2020. The Korean Academy of Conservative Dentistry
This is an Open Access article distributed under the terms of the Creative Commons Attribution Non-Commercial License (https://creativecommons.org/licenses/by-nc/4.0/) which permits unrestricted non-commercial use, distribution, and reproduction in any medium, provided the original work is properly cited.
- 4,359 Views
- 46 Download
- 10 Crossref
Abstract
- The aim of this article was to review age-dependent clinical recommendations for appropriate root canal instrumentation techniques. A comprehensive narrative review of canal morphology, the structural characteristics of dentin, and endodontic outcomes at different ages was undertaken instead of a systematic review. An electronic literature search was carried out, including the Medline (Ovid), PubMed, and Web of Science databases. The searches used controlled vocabulary and free-text terms, as follows: ‘age-related root canal treatment,’ ‘age-related instrumentation,’ ‘age-related chemo-mechanical preparation,’ ‘age-related endodontic clinical recommendations,’ ‘root canal instrumentation at different ages,’ ‘geriatric root canal treatment,’ and ‘pediatric root canal treatment.’ Due to the lack of literature with practical age-based clinical recommendations for an appropriate root canal instrumentation technique, a narrative review was conducted to suggest a clinical algorithm for choosing the most appropriate instrumentation technique during root canal treatment. Based on the evidence found through the narrative review, an age-related clinical algorithm for choosing appropriate instrumentation during root canal treatment was proposed. Age affects the morphology of the root canal system and the structural characteristics of dentin. The clinician’s awareness of root canal morphology and dentin characteristics can influence the choice of instruments for root canal treatment.
INTRODUCTION
The global population is growing and is experiencing both an increase in life expectancy and a decrease in tooth loss [1]. Since root canal treatment is performed in patients of all ages, clinicians should be aware of differences in root canal system morphology and dentinal structure depending on the patient's age.
It has been previously stated that it is virtually impossible to establish guidelines or instrument calibers that will guarantee adequate canal preparation in any age group [2]. Nonetheless, based on differences in canal morphology and dentinal structure and as a result of the diverse endodontic instruments and techniques that are available today, the clinician may adopt different means for instrumentation of the root canal system.
Meanwhile, various instruments—especially shaping files made of different heat-treated alloys with different geometric characteristics—have been reported to have distinctive mechanical properties and consequent shaping results [3,4,5]. The choice of instrumentation may result in inappropriate clinical results in certain cases, depending on the instrument's properties and the patient's clinical condition, including age. Therefore, the aim of this article was to review age-dependent clinical recommendations for root canal instrumentation techniques via a literature search and review.
METHODS
An electronic literature search was carried out, including the MEDLINE (Ovid), PubMed, and Web of Science databases. The searches used controlled vocabulary and free-text terms, as follows: ‘age-related root canal treatment,’ ‘age-related instrumentation,’ ‘age-related chemo-mechanical preparation,’ ‘age-related endodontic clinical recommendations,’ ‘root canal instrumentation at different ages,’ ‘geriatric root canal treatment,’ and ‘pediatric root canal treatment.’ However, the review of the literature revealed a lack of studies with practical clinical recommendations referring to age in choosing appropriate root canal instrumentation.
Therefore, a comprehensive narrative review of canal morphology, the structural characteristics of dentin, and endodontic outcomes at different ages was undertaken from articles that were published from 1925 to 2018 instead of a systematic review. Narrative reviews are most useful for obtaining a broad perspective on a topic and are often more comparable to a textbook chapter, including sections on the physiology and/or epidemiology of a topic. Based on this narrative review, a clinical algorithm for choosing the most appropriate instrumentation during root canal treatment was proposed.
Previous studies have taken different approaches to categorizing age-related morphological and structural changes, either basing them on statistical preferences (to ensure larger sample sizes) [6,7] or without explaining the categorization [8,9,10]. This review categorizes age-related differences by the following age groups: individuals who are 20 years old or less, between 21 and 40 years old, and 41 years old or more.
1. Canal cross-sectional outline and diameter
Differentiation of the root canal system due to the deposition of secondary dentin is an age-dependent process [8]. The pulp cavity generally decreases in size as an individual ages (Figure 1) [11,12,13].
Figure 1
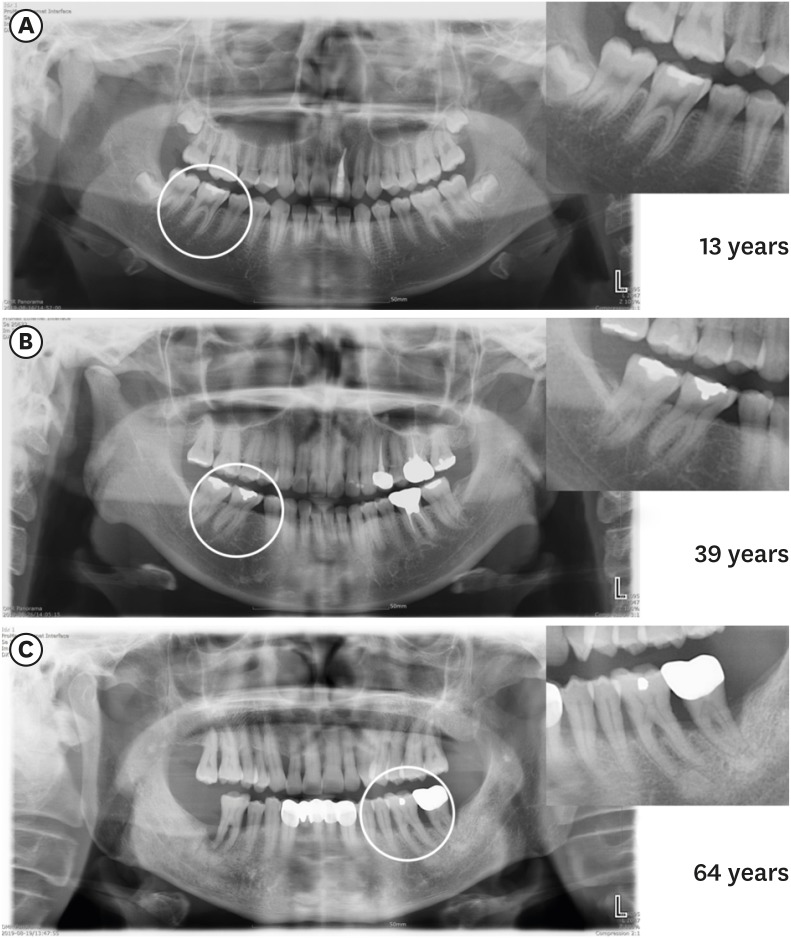
Panoramic radiography images showing the chamber and canal sizes according at different ages. (A) Individuals under 20 years old (13 years), (B) individuals between 20 and 40 years old (39 years), (C) individuals over 40 years old (64 years). The image in (A) shows a large chamber and a straight direction to the canal orifice. The image in (B) shows a dentin shelf area and an angulated direction to canal orifice. The image in (C) shows a thin chamber area and sclerotic canals.
In general, in individuals who are 20 years old or less, the roots have a single large root canal (mostly oval) [7,8,11,14,15]. Middle mesial canals in mandibular molars occur mostly in individuals younger than 21 years old [16]. Individuals who are 20 to 40 years old have multiple separate canals [7,8,11,15]. The number of root canals was mainly found to increase in the maxillary and mandibular second premolars, the distal root of mandibular first molars, and the lower incisors [7,14,17,18]. More round canals were found in the second mandibular molars in patients over 35 years old, while more oval canals were found in the teeth of individuals younger than 35 years of age [14].
A C-shaped configuration (category III) is more common in the mandibular molars of individuals who are 40 years old or less [14,19]. In a cone-beam computed tomography study, patients less than 42 years old were 4 times more likely to have a middle mesial canal than patients older than 42 years [20]. In individuals older than 40 years of age, the deposition of secondary dentin resulted in decreased canal diameter and the disappearance of additional canals [21]. In individuals 51–70 years of age, fewer canals were found [22]. For example, a decrease in the presence of the second mesiobuccal canal in the maxillary molars was observed in this age group [6,15,17,22,23,24,25,26,27].
2. Isthmuses
The incidence of canal isthmuses appears to be age-related [28]. Individuals who are 20 years old or less have wide and oval canals without isthmuses at the early stages of root development [29]. In individuals between 20 and 40 years old, the deposition of secondary dentin in the mesiodistal direction results in the formation of 2 canals with an isthmus [29,30]. Up to 81% of mesial roots of the mandibular first molars of individuals aged 20-39 years old have isthmuses, particularly at apical 4 to 6 mm [29]. In individuals who are 40 years old or more, the prevalence and volume of isthmuses significantly decrease, and the canal becomes completely separated. In individuals who are over 50, the prevalence of isthmuses was found to be 16.7% [31] and only 24% of individuals over 60 years of age had isthmuses in mesial roots of the mandibular molars [29]. The ratio of partial isthmuses to complete isthmuses has been shown to increase with age [29,32]. Figure 2 shows the characteristics of isthmuses at different ages with axial cone-beam computed tomography images.
Figure 2
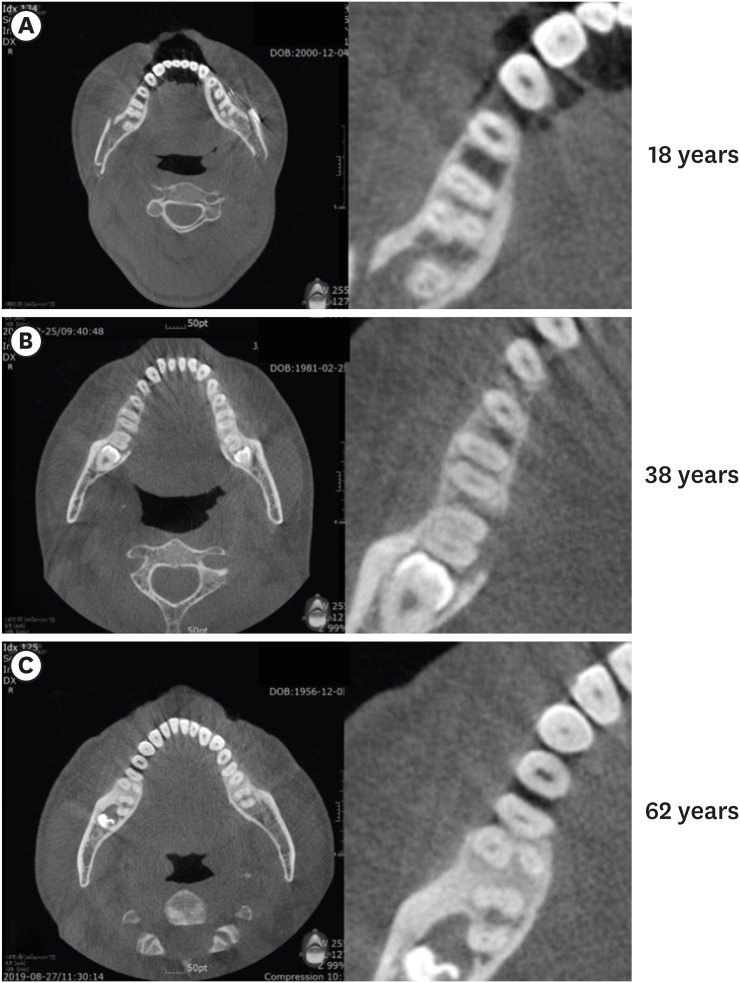
Axial cone-beam computed tomography images of 3 mandibular first molars, showing isthmus characteristics at different ages. (A) Individuals under 20 years old (18 years): a wide canal without an isthmus, (B) individuals between 20 and 40 years old (38 years): an isthmus in the mesial root, (C) individuals who are 40 years old or more (62 years): sclerotic mesial canals without an isthmus, resembling a single canal.
Normal dentin undergoes physiological alteration to transparent (sclerotic) dentin with age [33,34]. As the tooth matures, the peritubular dentin becomes more mineralized [35], and there is a decrease in the mean number of dentinal tubules [36]. The mineralization process and dentin sclerosis result in a narrowing of the tubules. In some instances, the process can lead to complete obliteration of the dentinal tubules [33,35,37]. Mineralization starts in the third decade of life in the apical region and advances coronally with age [5,38,39].
The penetration of bacteria into the dentinal tubules could be a determinant of their virulence in the root canal environment [40]. The microbial load and diversity are higher in young individuals and decrease with age [41]. This decrease may be attributed to tubular mineralization, as well as to a decrease in the pulp cavity space, isthmuses, and additional canals. Tubules are usually larger in diameter than the average Enterococcus faecalis (E. faecalis) cell diameter by approximately 0.8–1 nm [42,43,44,45,46]. However, due to age-dependent tubular mineralization, there is a decreased depth of E. faecalis penetration into the dentin through sclerotic or obliterated tubules in aged dentin [40]. On average, bacteria invade 65 µm less deeply in individuals who are 60–77 years old than in individuals who are 18–24 years old [40].
As an individual ages, the water content of dentin decreases and modifications of collagen, such as cross-linking, increase [47]. Due to these age-related changes, the damage tolerance of teeth decreases in older individuals [48,49,50], as well as a significant reduction in dentin strength and fracture toughness, resulting in an increase in vertical root fracture (VRF) incidence with age [49,51,52]. VRFs mostly occur in the posterior teeth of patients between 40 and 60 years old [53,54]. In addition, the incremental crack growth rate in ‘old’ dehydrated dentin is 100 times faster than in ‘young’ hydrated dentin [55]. Pre-existing dentinal microcracks in non-endodontically treated roots become more common with age (8.3% in individuals over 40 years old vs. 3.7% in individuals who are 20–39 years old) [56]. In contrast, in individuals who are under 20 years old, the dentin walls are thin, which may lead to coronal or radicular tooth fractures during normal functional stress [57,58].
The reports of the effects of the patient's age on the outcomes of endodontic treatment are conflicting. Some studies have reported that age had no statistically significant influence on the results [59,60,61,62], while others claimed that the patient's age significantly influenced the results [63]. Some studies found that older patients had a higher percentage of success than younger patients [12,64,65,66], while other researchers found better outcomes in younger patients [63,67] and demonstrated that age was a risk factor for experiencing an adverse event. For instance, older patients were 1.4 times more likely to undergo an extraction procedure after root canal therapy [68]. The incidence of a subsequent extraction increases by 1% to 2% each decade, until reaching a plateau after the age of 60 [69].
Findings of better outcomes for older individuals might be explained by the progressive reduction of pulp space, disappearance of auxiliary canals and isthmuses, and narrowing of dentinal tubules up to total obliteration [36,40]. These changes limit the volume available for infection and make it easier to provide adequate canal debridement, as well as root canal shaping and cleaning [12]. Reports of better outcomes for younger individuals might be explained by the increased prevalence of pre-existing apical periodontitis with age, which has been associated with a lower likelihood of success of endodontic procedures [70]. Another explanation might be that older individuals have slower and less effective healing processes or a prolonged healing time [12,71]. The immunological changes that occur due to aging [72,73] include changes in the pulpal cells expressing macrophage-associated antigens [74]. Aging is associated with a low level of expression of genes encoding for transcription regulators and a high level of expression of genes involved in apoptotic processes [75].
Furthermore, systemic diseases are more prevalent in older age groups [76], and it has been reported that some systemic diseases might be correlated with endodontic outcomes [77]. Diabetes (non-insulin dependent or insulin dependent) or an impaired, nonspecific immune response results in a reduced likelihood of successful endodontic treatment in patients with preoperative periradicular lesions [78,79].
Table 1 displays the characteristics of canal morphology and dentinal structure in different age groups, including the canal cross-sectional outline and diameter, the presence and characteristics of isthmuses, auxiliary canals, the quantity and diameter of dentinal tubules, and dentinal sclerosis. Collectively, these age-related changes suggest that the clinician may opt for different clinical approaches for different age groups.
Table 1
Characteristics of canal morphology and dentinal structure in different age groups
| Age groups | |||
|---|---|---|---|
| 20 years old or less | 21 to 40 years old | 41 years old or more | |
| Canal morphology [4,5,8,9,10,11,12,13,14,15,16,17,18,19,20,21,22,23,24,25,26,27,28,29,30,31,32] | - Simple anatomy | - Oval and round canals | - Rounder canals with a small diameter |
| - Mostly wide-oval canal | - Prominent isthmuses | - Decreasing volume of isthmuses, more partial isthmuses up to disappearance | |
| - No isthmuses | - Auxiliary canals | - Fewer auxiliary canals | |
| - No auxiliary canals | |||
| Dentin structure [5,33,34,35,36,37,38,39,40,41,42,43,44,45,46,47,48,49,50,51,52,53,54,55,56,57,58] | - Large number of tubules with large diameter | - Dentinal sclerosis starting at the apical region | - Massive obliteration of dentinal tubules |
| - Thin dentinal walls | - Reduction in the dentin water content and more modifications of collagen | ||
Within the limitations of the studies that were analyzed, the following possible clinical suggestions for root canal instrumentation can be made. For individuals who are 20 years old or less, the recommendations are as follows. Large canals do not require additional widening. Instruments with a scraping action may be preferred to clean the root canal wall of biofilm and simultaneously activate the irrigation solution [80,81]. Possible instruments are the Self-Adjusting File (SAF; ReDent, Ra'anana, Israel) [82] and the XP-Endo Finisher (FKG Dentaire, La Chaux-de-Fonds, Switzerland) [83]. These systems are efficient for cleaning the comparably large and oval canal lumen by a scrubbing action with simultaneous continual replacement of the irrigant for the SAF or eccentric movements drawing upon the specific properties of controlled-memory wired instruments such as the XP-Endo Finisher.
For individuals who are 20 to 40 years old, the following recommendations can be made. The canals are mostly patent and difficulties in the glide path are rare. In these root canal systems, regular nickel-titanium (NiTi) rotary systems can be used to shape the canal up to an apical diameter size of #30–#35 [84] with subsequent agitation using sodium hypochlorite. Possible instruments include the ProTaper Next (Dentsply Sirona, Ballaigues, Switzerland), XP-Shaper (FKG Dentaire, La Chaux-de-Fonds, Switzerland), and 2Shape (MicroMega, Besançon, France). Using scraping instruments in this age group can be considered in oval canals.
For individuals who are 40 years old or more, the recommendations are as follows. In these root canal systems, after the use of manual stainless-steel K-files (#06, #08, and #10), a NiTi system for the glide path can be used. Possible instruments include the G-file (MicroMega), PathFile (Dentsply Sirona), OneG (MicroMega), ProGlider (Dentsply Sirona), Scout RaCe, and Race ISO 10 (FKG Dentaire). Afterward, widening of the canal apical diameter up to size #30 or #35 is preferably done with NiTi instruments, which create less loading on dentin [85]. Possible instruments for this purpose are those with a smaller core (MTwo [VDW, Munich, Germany], Race [FKG Dentaire], ProFile [Dentsply Sirona], 2Shape), those with a smaller taper (0.02 and 0.04) (Race, ProFile), and those made of flexible NiTi (controlled memory wire) such as HyFlex (Coltene/Whaledent, Inc, Cuyahoga Falls, OH, USA) and Typhoon (Clinician's Choice Dental Products, New Milford, CT, USA).
Table 2 displays the proposed algorithm for root canal instrumentation in different age groups. The current suggestions are based on the available evidence and reflect the limitations of the studies that were included in the review. However, no one algorithm suits all teeth. The clinician may face incompatibility between chronological age and biological age. Pathological or iatrogenic factors might modify the canal cross-sectional outline and diameter. These factors include carious lesions or deep restorations [27], attrition or abrasion [86], occlusal trauma [87], periodontal disease and treatment [88,89], and orthodontic treatment [90]. The stimuli that each tooth encounters over its lifespan should be taken into consideration due to a possible rapid increase in reactionary dentin deposition [7]. In contrast, pulp necrosis in younger patients due to trauma or caries might lead to the formation of wider canals with thin dentinal walls when those patients become older.
Table 2
The algorithm for root canal instrumentation in different age groups
The content of this review does not necessarily support any specific technique for certain clinical conditions in patients of various age ranges and root canal conditions. However, it may be generally acceptable to reinforce the importance of chemo-mechanical preparation, which always enhances canal cleaning by shaping, and activated irrigation, regardless of patients' age and canal condition. A proper evaluation of root canal morphology, coupled with an adequate understanding of the influence of age on these characteristics, may help the clinician to choose the most appropriate instrumentation and irrigation activation technique.
CONCLUSIONS
The current review considered age-dependent differences in canal morphology, the structural characteristics of dentin, and endodontic outcomes. Age-dependent clinical suggestions for instrumentation would be ideally based on a systematic review of randomized controlled trials considering the quality of the evidence and patients' values, preferences, and financial resources. However, no studies suitable for this purpose have been carried out. Thus, the present article is the first to attempt to interpret age-dependent morphological and structural changes and to make practical clinical suggestions within the limitations of existing studies.
A systematic review is a comprehensive search method for relevant studies on a specific topic, and the identified studies are then appraised and synthesized according to a predetermined and explicit method. In contrast, a narrative review is a traditional expert review method. This method is subjective and there are no formal rules for selecting studies or standard statistical methods for combining studies. Therefore, when reading and evaluating a narrative review, readers need to keep in mind that authorial bias may or may not be present.
An additional limitation of these proposed clinical suggestions is that the abovementioned instruments are not available to all clinicians because of characteristics of the local market and financial resources. Further studies should investigate the influence of the patient's age on other aspects of root canal treatment (e.g., the preparation of access cavities, irrigant agitation methods, and obturation technique). It can be concluded that the clinician's awareness of age-related differences in root canal morphology and dentin characteristics can influence the choice of instruments for root canal treatment.
-
Conflict of Interest: No potential conflict of interest relevant to this article was reported.
-
Author Contributions:
Conceptualization: Solomonov M.
Data curation: Hadad A, Levy DH, Ben Itzhak J, Levinson O, Azizi H.
Formal analysis: Solomonov M, Kim HC, Azizi H.
Investigation: Solomonov M, Hadad A, Levy DH, Ben Itzhak J, Levinson O, Azizi H.
Methodology: Solomonov M, Kim HC, Hadad A, Levy DH, Ben Itzhak J, Levinson O, Azizi H.
Project administration: Solomonov M.
Software: Azizi H.
Supervision: Solomonov M, Kim HC.
Validation: Solomonov M, Kim HC.
Visualization: Hadad A, Levy DH, Ben Itzhak J, Levinson O, Azizi H.
Writing - original draft: Solomonov M, Hadad A, Azizi H.
Writing - review & editing: Kim HC.
- 1. Kassebaum NJ, Bernabé E, Dahiya M, Bhandari B, Murray CJ, Marcenes W. Global burden of untreated caries: a systematic review and metaregression. J Dent Res 2015;94:650-658.ArticlePubMedPDF
- 2. Gani O, Visvisian C. Apical canal diameter in the first upper molar at various ages. J Endod 1999;25:689-691.ArticlePubMed
- 3. Yared G. Canal preparation using only one Ni-Ti rotary instrument: preliminary observations. Int Endod J 2008;41:339-344.ArticlePubMed
- 4. Ahn SY, Kim HC, Kim E. Kinematic effects of nickel-titanium instruments with reciprocating or continuous rotation motion: a systematic review of in vitro studies. J Endod 2016;42:1009-1017.ArticlePubMed
- 5. Pérez-Higueras JJ, Arias A, de la Macorra JC. Cyclic fatigue resistance of K3, K3XF, and twisted file nickel-titanium files under continuous rotation or reciprocating motion. J Endod 2013;39:1585-1588.ArticlePubMed
- 6. Martins JN, Alkhawas MA, Altaki Z, Bellardini G, Berti L, Boveda C, Chaniotis A, Flynn D, Gonzalez JA, Kottoor J, Marques MS, Monroe A, Ounsi HF, Parashos P, Plotino G, Ragnarsson MF, Aguilar RR, Santiago F, Seedat HC, Vargas W, von Zuben M, Zhang Y, Gu Y, Ginjeira A. Worldwide analyses of maxillary first molar second mesiobuccal prevalence: a multicenter cone-beam computed tomographic study. J Endod 2018;44:1641-1649.e1.ArticlePubMed
- 7. Martins JN, Ordinola-Zapata R, Marques D, Francisco H, Caramês J. Differences in root canal system configuration in human permanent teeth within different age groups. Int Endod J 2018;51:931-941.ArticlePubMedPDF
- 8. Peiris HR, Pitakotuwage TN, Takahashi M, Sasaki K, Kanazawa E. Root canal morphology of mandibular permanent molars at different ages. Int Endod J 2008;41:828-835.ArticlePubMed
- 9. Zheng QH, Wang Y, Zhou XD, Wang Q, Zheng GN, Huang DM. A cone-beam computed tomography study of maxillary first permanent molar root and canal morphology in a Chinese population. J Endod 2010;36:1480-1484.ArticlePubMed
- 10. Guo J, Vahidnia A, Sedghizadeh P, Enciso R. Evaluation of root and canal morphology of maxillary permanent first molars in a North American population by cone-beam computed tomography. J Endod 2014;40:635-639.ArticlePubMed
- 11. Hess W, Zurcher E. The anatomy of root canals of the teeth of the permanent and deciduous dentitions. New York, NY: William Wood & Co; 1925.
- 12. Ørstavik D, Qvist V, Stoltze K. A multivariate analysis of the outcome of endodontic treatment. Eur J Oral Sci 2004;112:224-230.ArticlePubMed
- 13. Vertucci FJ. Root canal morphology and its relationship to endodontic procedures. Endod Topics 2005;10:3-29.Article
- 14. Manning SA. Root canal anatomy of mandibular second molars. Part I. Int Endod J 1990;23:34-39.ArticlePubMed
- 15. Thomas RP, Moule AJ, Bryant R. Root canal morphology of maxillary permanent first molar teeth at various ages. Int Endod J 1993;26:257-267.ArticlePubMed
- 16. Nosrat A, Deschenes RJ, Tordik PA, Hicks ML, Fouad AF. Middle mesial canals in mandibular molars: incidence and related factors. J Endod 2015;41:28-32.ArticlePubMed
- 17. Pattanshetti N, Gaidhane M, Al Kandari AM. Root and canal morphology of the mesiobuccal and distal roots of permanent first molars in a Kuwait population--a clinical study. Int Endod J 2008;41:755-762.ArticlePubMed
- 18. Liu J, Luo J, Dou L, Yang D. CBCT study of root and canal morphology of permanent mandibular incisors in a Chinese population. Acta Odontol Scand 2014;72:26-30.ArticlePubMed
- 19. Al-Fouzan KS. C-shaped root canals in mandibular second molars in a Saudi Arabian population. Int Endod J 2002;35:499-504.ArticlePubMed
- 20. Akbarzadeh N, Aminoshariae A, Khalighinejad N, Palomo JM, Syed A, Kulild JC, Sadeghi G, Mickel A. The association between the anatomic landmarks of the pulp chamber floor and the prevalence of middle mesial canals in mandibular first molars: an in vivo analysis. J Endod 2017;43:1797-1801.ArticlePubMed
- 21. Kaya S, Adiguzel O, Yavuz I, Tumen EC, Akkus Z. Cone-beam dental computerized tomography for evaluating changes of aging in the dimensions central superior incisor root canals. Med Oral Patol Oral Cir Bucal 2011;16:e463-e466.PubMed
- 22. Reis AG, Grazziotin-Soares R, Barletta FB, Fontanella VR, Mahl CR. Second canal in mesiobuccal root of maxillary molars is correlated with root third and patient age: a cone-beam computed tomographic study. J Endod 2013;39:588-592.ArticlePubMed
- 23. Neaverth EJ, Kotler LM, Kaltenbach RF. Clinical investigation. Clinical investigation (in vivo) of endodontically treated maxillary first molars. J Endod 1987;13:506-512.ArticlePubMed
- 24. Gilles J, Reader A. An SEM investigation of the mesiolingual canal in human maxillary first and second molars. Oral Surg Oral Med Oral Pathol 1990;70:638-643.ArticlePubMed
- 25. Fogel HM, Peikoff MD, Christie WH. Canal configuration in the mesiobuccal root of the maxillary first molar: a clinical study. J Endod 1994;20:135-137.ArticlePubMed
- 26. Yoshioka T, Kikuchi I, Fukumoto Y, Kobayashi C, Suda H. Detection of the second mesiobuccal canal in mesiobuccal roots of maxillary molar teeth ex vivo . Int Endod J 2005;38:124-128.ArticlePubMed
- 27. Lee JH, Kim KD, Lee JK, Park W, Jeong JS, Lee Y, Gu Y, Chang SW, Son WJ, Lee WC, Baek SH, Bae KS, Kum KY. Mesiobuccal root canal anatomy of Korean maxillary first and second molars by cone-beam computed tomography. Oral Surg Oral Med Oral Pathol Oral Radiol Endod 2011;111:785-791.ArticlePubMed
- 28. al Shalabi RM, Omer OE, Glennon J, Jennings M, Claffey NM. Root canal anatomy of maxillary first and second permanent molars. Int Endod J 2000;33:405-414.ArticlePubMed
- 29. Gu L, Wei X, Ling J, Huang X. A microcomputed tomographic study of canal isthmuses in the mesial root of mandibular first molars in a Chinese population. J Endod 2009;35:353-356.ArticlePubMed
- 30. Villas-Bôas MH, Bernardineli N, Cavenago BC, Marciano M, Del Carpio-Perochena A, de Moraes IG, Duarte MH, Bramante CM, Ordinola-Zapata R. Micro-computed tomography study of the internal anatomy of mesial root canals of mandibular molars. J Endod 2011;37:1682-1686.ArticlePubMed
- 31. Srivastava S, Alrogaibah NA, Aljarbou G. Cone-beam computed tomographic analysis of middle mesial canals and isthmus in mesial roots of mandibular first molars-prevalence and related factors. J Conserv Dent 2018;21:526-530.ArticlePubMedPMC
- 32. Oi T, Saka H, Ide Y. Three-dimensional observation of pulp cavities in the maxillary first premolar tooth using micro-CT. Int Endod J 2004;37:46-51.ArticlePubMed
- 33. Miller WA, Eick JD, Neiders ME. Inorganic components of the peritubular dentin in young human permanent teeth. Caries Res 1971;5:264-278.ArticlePubMed
- 34. Kishen A. Biomechanics of fractures in endodontically treated teeth. Endod Topics 2015;33:3-13.Article
- 35. Tronstad L. Ultrastructural observations on human coronal dentin. Scand J Dent Res 1973;81:101-111.ArticlePubMed
- 36. Carrigan PJ, Morse DR, Furst ML, Sinai IH. A scanning electron microscopic evaluation of human dentinal tubules according to age and location. J Endod 1984;10:359-363.ArticlePubMed
- 37. Ozdemir HO, Buzoglu HD, Calt S, Stabholz A, Steinberg D. Effect of ethylenediaminetetraacetic acid and sodium hypochlorite irrigation on Enterococcus faecalis biofilm colonization in young and old human root canal dentin: in vitro study. J Endod 2010;36:842-846.ArticlePubMed
- 38. Stanley HR, Pereira JC, Spiegel E, Broom C, Schultz M. The detection and prevalence of reactive and physiologic sclerotic dentin, reparative dentin and dead tracts beneath various types of dental lesions according to tooth surface and age. J Oral Pathol 1983;12:257-289.ArticlePubMed
- 39. Paqué F, Luder HU, Sener B, Zehnder M. Tubular sclerosis rather than the smear layer impedes dye penetration into the dentine of endodontically instrumented root canals. Int Endod J 2006;39:18-25.ArticlePubMed
- 40. Kakoli P, Nandakumar R, Romberg E, Arola D, Fouad AF. The effect of age on bacterial penetration of radicular dentin. J Endod 2009;35:78-81.ArticlePubMedPMC
- 41. Sánchez-Sanhueza G, Bello-Toledo H, González-Rocha G, Gonçalves AT, Valenzuela V, Gallardo-Escárate C. Metagenomic study of bacterial microbiota in persistent endodontic infections using next-generation sequencing. Int Endod J 2018;51:1336-1348.ArticlePubMedPDF
- 42. Ketterl W. Age-induced changes in the teeth and their attachment apparatus. Int Dent J 1983;33:262-271.PubMed
- 43. Morse DR. Age-related changes of the dental pulp complex and their relationship to systemic aging. Oral Surg Oral Med Oral Pathol 1991;72:721-745.ArticlePubMed
- 44. Love RM, Jenkinson HF. Invasion of dentinal tubules by oral bacteria. Crit Rev Oral Biol Med 2002;13:171-183.PubMed
- 45. Kinney JH, Nalla RK, Pople JA, Breunig TM, Ritchie RO. Age-related transparent root dentin: mineral concentration, crystallite size, and mechanical properties. Biomaterials 2005;26:3363-3376.ArticlePubMed
- 46. Rigden MD, Baier C, Ramirez-Arcos S, Liao M, Wang M, Dillon JA. Identification of the coiled-coil domains of Enterococcus faecalis DivIVA that mediate oligomerization and their importance for biological function. J Biochem 2008;144:63-76.ArticlePubMed
- 47. Kishen A. Mechanisms and risk factors for fracture predilection in endodontically treated teeth. Endod Topics 2006;13:57-83.Article
- 48. Arola D, Reprogel RK. Effects of aging on the mechanical behavior of human dentin. Biomaterials 2005;26:4051-4061.ArticlePubMed
- 49. Mireku AS, Romberg E, Fouad AF, Arola D. Vertical fracture of root filled teeth restored with posts: the effects of patient age and dentine thickness. Int Endod J 2010;43:218-225.ArticlePubMedPMC
- 50. Yan W, Montoya C, Øilo M, Ossa A, Paranjpe A, Zhang H, Arola D. Reduction in fracture resistance of the root with aging. J Endod 2017;43:1494-1498.ArticlePubMed
- 51. Koester KJ, Ager JW 3rd, Ritchie RO. The effect of aging on crack-growth resistance and toughening mechanisms in human dentin. Biomaterials 2008;29:1318-1328.ArticlePubMed
- 52. Nazari A, Bajaj D, Zhang D, Romberg E, Arola D. Aging and the reduction in fracture toughness of human dentin. J Mech Behav Biomed Mater 2009;2:550-559.ArticlePubMedPMC
- 53. Tamse A. Iatrogenic vertical root fractures in endodontically treated teeth. Endod Dent Traumatol 1988;4:190-196.ArticlePubMed
- 54. Testori T, Badino M, Castagnola M. Vertical root fractures in endodontically treated teeth: a clinical survey of 36 cases. J Endod 1993;19:87-91.ArticlePubMed
- 55. Bajaj D, Sundaram N, Nazari A, Arola D. Age, dehydration and fatigue crack growth in dentin. Biomaterials 2006;27:2507-2517.ArticlePubMed
- 56. PradeepKumar AR, Shemesh H, Chang JW, Bhowmik A, Sibi S, Gopikrishna V, Lakshmi-Narayanan L, Kishen A. Preexisting dentinal microcracks in nonendodontically treated teeth: an ex vivo micro-computed tomographic analysis. J Endod 2017;43:896-900.ArticlePubMed
- 57. Sathorn C, Palamara JE, Palamara D, Messer HH. Effect of root canal size and external root surface morphology on fracture susceptibility and pattern: a finite element analysis. J Endod 2005;31:288-292.ArticlePubMed
- 58. Tang W, Wu Y, Smales RJ. Identifying and reducing risks for potential fractures in endodontically treated teeth. J Endod 2010;36:609-617.ArticlePubMed
- 59. Swartz DB, Skidmore AE, Griffin JA Jr. Twenty years of endodontic success and failure. J Endod 1983;9:198-202.ArticlePubMed
- 60. Sjogren U, Hagglund B, Sundqvist G, Wing K. Factors affecting the long-term results of endodontic treatment. J Endod 1990;16:498-504.ArticlePubMed
- 61. Dammaschke T, Steven D, Kaup M, Ott KH. Long-term survival of root-canal-treated teeth: a retrospective study over 10 years. J Endod 2003;29:638-643.ArticlePubMed
- 62. Kojima K, Inamoto K, Nagamatsu K, Hara A, Nakata K, Morita I, Nakagaki H, Nakamura H. Success rate of endodontic treatment of teeth with vital and nonvital pulps. A meta-analysis. Oral Surg Oral Med Oral Pathol Oral Radiol Endod 2004;97:95-99.ArticlePubMed
- 63. Grossman LI, Shepard LI, Pearson LA. Roentgenologic and clinical evaluation of endodontically treated teeth. Oral Surg Oral Med Oral Pathol 1964;17:368-374.ArticlePubMed
- 64. Harty FJ, Parkins BJ, Wengraf AM. Success rate in root canal therapy. A retrospective study of conventional cases. Br Dent J 1970;128:65-70.ArticlePubMedPDF
- 65. Smith CS, Setchell DJ, Harty FJ. Factors influencing the success of conventional root canal therapy--a five-year retrospective study. Int Endod J 1993;26:321-333.ArticlePubMed
- 66. Imura N, Pinheiro ET, Gomes BP, Zaia AA, Ferraz CC, Souza-Filho FJ. The outcome of endodontic treatment: a retrospective study of 2000 cases performed by a specialist. J Endod 2007;33:1278-1282.ArticlePubMed
- 67. Seltzer S, Bender IB, Turkenkopf S. Factors affecting successful repairs after root canal therapy. J Am Dent Assoc 1963;67:651-662.PubMed
- 68. Caplan DJ, Weintraub JA. Factors related to loss of root canal filled teeth. J Public Health Dent 1997;57:31-39.ArticlePubMed
- 69. Lazarski MP, Walker WA 3rd, Flores CM, Schindler WG, Hargreaves KM. Epidemiological evaluation of the outcomes of nonsurgical root canal treatment in a large cohort of insured dental patients. J Endod 2001;27:791-796.ArticlePubMed
- 70. Eriksen HM. Epidemiology of apical periodontitis. In: Orstavik D, Pitt Ford TR, editors. Essential endodontology. Prevention and treatment of apical periodontitis. London: Blackwell Science Ltd; 1998. p. 179-191.
- 71. Azim AA, Griggs JA, Huang GT. The Tennessee study: factors affecting treatment outcome and healing time following nonsurgical root canal treatment. Int Endod J 2016;49:6-16.ArticlePubMed
- 72. Lloberas J, Celada A. Effect of aging on macrophage function. Exp Gerontol 2002;37:1325-1331.ArticlePubMed
- 73. Renshaw M, Rockwell J, Engleman C, Gewirtz A, Katz J, Sambhara S. Cutting edge: impaired Toll-like receptor expression and function in aging. J Immunol 2002;169:4697-4701.ArticlePubMedPDF
- 74. Okiji T, Kosaka T, Kamal AM, Kawashima N, Suda H. Age-related changes in the immunoreactivity of the monocyte/macrophage system in rat molar pulp. Arch Oral Biol 1996;41:453-460.ArticlePubMed
- 75. Tranasi M, Sberna MT, Zizzari V, D'Apolito G, Mastrangelo F, Salini L, Stuppia L, Tetè S. Microarray evaluation of age-related changes in human dental pulp. J Endod 2009;35:1211-1217.ArticlePubMed
- 76. Prince MJ, Wu F, Guo Y, Gutierrez Robledo LM, O'Donnell M, Sullivan R, Yusuf S. The burden of disease in older people and implications for health policy and practice. Lancet 2015;385:549-562.ArticlePubMed
- 77. Aminoshariae A, Kulild JC, Mickel A, Fouad AF. Association between systemic diseases and endodontic outcome: a systematic review. J Endod 2017;43:514-519.ArticlePubMed
- 78. Fouad AF, Burleson J. The effect of diabetes mellitus on endodontic treatment outcome: data from an electronic patient record. J Am Dent Assoc 2003;134:43-51.PubMed
- 79. Lima SM, Grisi DC, Kogawa EM, Franco OL, Peixoto VC, Gonçalves-Júnior JF, Arruda MP, Rezende TM. Diabetes mellitus and inflammatory pulpal and periapical disease: a review. Int Endod J 2013;46:700-709.ArticlePubMed
- 80. Siqueira JF Jr, Alves FR, Almeida BM, de Oliveira JC, Rôças IN. Ability of chemomechanical preparation with either rotary instruments or self-adjusting file to disinfect oval-shaped root canals. J Endod 2010;36:1860-1865.ArticlePubMed
- 81. Lin J, Shen Y, Haapasalo M. A comparative study of biofilm removal with hand, rotary nickel-titanium, and self-adjusting file instrumentation using a novel in vitro biofilm model. J Endod 2013;39:658-663.ArticlePubMed
- 82. Metzger Z, Solomonov M, Kfir A. The role of mechanical instrumentation in the cleaning of root canals. Endod Topics 2013;29:87-109.Article
- 83. Alves FR, Marceliano-Alves MF, Sousa JC, Silveira SB, Provenzano JC, Siqueira JF Jr. Removal of root canal fillings in curved canals using either reciprocating single- or rotary multi-instrument systems and a supplementary step with the XP-Endo Finisher. J Endod 2016;42:1114-1119.ArticlePubMed
- 84. Arvaniti IS, Khabbaz MG. Influence of root canal taper on its cleanliness: a scanning electron microscopic study. J Endod 2011;37:871-874.ArticlePubMed
- 85. Kim HC, Lee MH, Yum J, Versluis A, Lee CJ, Kim BM. Potential relationship between design of nickel-titanium rotary instruments and vertical root fracture. J Endod 2010;36:1195-1199.ArticlePubMed
- 86. Philippas GG, Applebaum E. Age factor in secondary dentin formation. J Dent Res 1966;45:778-789.ArticlePubMedPDF
- 87. Tziafas D. Mechanisms controlling secondary initiation of dentinogenesis: a review. Int Endod J 1994;27:61-74.ArticlePubMed
- 88. Bender IB, Seltzer S. The effect of periodontal disease on the pulp. Oral Surg Oral Med Oral Pathol 1972;33:458-474.ArticlePubMed
- 89. Bergenholtz G, Lindhe J. Effect of experimentally induced marginal periodontitis and periodontal scaling on the dental pulp. J Clin Periodontol 1978;5:59-73.ArticlePubMed
- 90. Venkatesh S, Ajmera S, Ganeshkar SV. Volumetric pulp changes after orthodontic treatment determined by cone-beam computed tomography. J Endod 2014;40:1758-1763.ArticlePubMed
REFERENCES
Tables & Figures
REFERENCES
Citations
Citations to this article as recorded by 
- Effect of calcium silicate and epoxy resin-based sealers on postoperative pain: a randomized clinical trial
Jessica Waayen Caleffi de Oliveira, Ingrid Luiza Mendonça Cunha, Aida Renée Assayag Hanan, André Augusto Franco Marques, Fernando José Herkrath, Emílio Carlos Sponchiado Júnior
BMC Oral Health.2026;[Epub] CrossRef - Başarısız Endodontik Tedavilerde Gözden Kaçan Kanalların İnsidansı
Okan Turgut, Melike Bayram, Emre Bayram
Acta Odontologica Turcica.2026; 43(2): 83. CrossRef - Cross-Sectional Analysis of the Challenges Faced by Undergraduate Dental Students During Root Canal Treatment (RCT) and the Oral Health-Related Quality of Life in Patients After RCT
Mubashir Baig Mirza, Abdullah Bajran Almuteb, Abdulaziz Tariq Alsheddi, Qamar Hashem, Mohammed Ali Abuelqomsan, Ahmed AlMokhatieb, Shahad AlBader, Abdullah AlShehri
Medicina.2025; 61(2): 215. CrossRef - OUTCOMES OF COMBINED ENDODONTIC TREATMENT AND APICAL SURGERY IN MANAGING LARGE PERIAPICAL CYSTS: A CLINICAL STUDY
Sapna Pandey, P Nihar, Amit Kumar, Nitin Bhagat, Vikram Karande, Zameer Pasha, Anukriti Kumari
BULLETIN OF STOMATOLOGY AND MAXILLOFACIAL SURGERY.2025; : 329. CrossRef - El Uso del hipoclorito de sodio en endodoncia: concentración, temperatura y activación
Ábilson Josue Fabiani Ticona, Fernanda Camargo Espejo
Revista de investigación e información en salud.2025;[Epub] CrossRef - Assessment of Anatomical Dentin Thickness in Mandibular First Molar: An In Vivo Cone‐Beam Computed Tomographic Study
Sahil Choudhari, Kavalipurapu Venkata Teja, Sindhu Ramesh, Jerry Jose, Mariangela Cernera, Parisa Soltani, Emmanuel João Nogueira Leal da Silva, Gianrico Spagnuolo, Ricardo Danil Guiraldo
International Journal of Dentistry.2024;[Epub] CrossRef - Oral Health Concerns of the ‘Sunset Age’
Pradnya V. Kakodkar, Amandeep Kaur, Shivasakthy Manivasakan, Sounyala Rayannavar, Revati Deshmukh, Smita Athavale
Journal of Medical Evidence.2023; 4(2): 141. CrossRef - Root canal treatment of a six-canal first mandibular molar with extensive periapical lesion: A case report
Xin Li, Shuyu Sun, Tengyi Zheng
Medicine.2023; 102(30): e34336. CrossRef - Endodontic Dentistry: Analysis of Dentinal Stress and Strain Development during Shaping of Curved Root Canals
Laura Iosif, Bogdan Dimitriu, Dan Florin Niţoi, Oana Amza
Healthcare.2023; 11(22): 2918. CrossRef - Mechanisms of age-related changes in the morphology of the pulp system of the first lower molars
N.B. Petrukhina, O.A. Zorina, V.A. Venediktova
Stomatologiya.2022; 101(2): 19. CrossRef
 ePub Link
ePub Link Cite
CiteAge-dependent root canal instrumentation techniques: a comprehensive narrative review
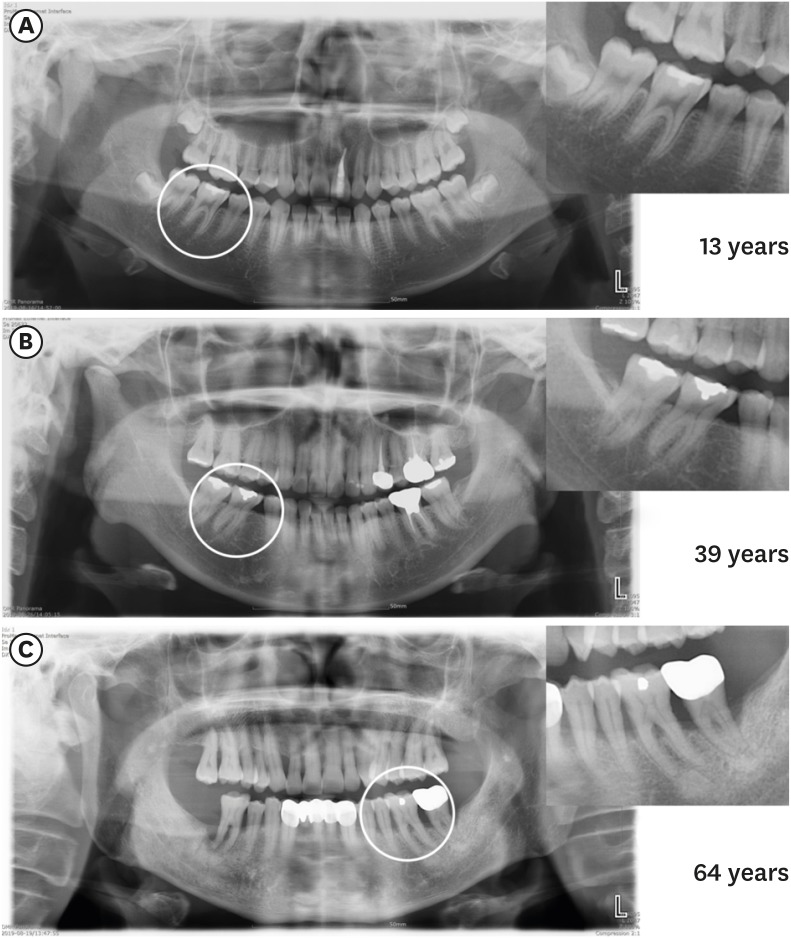
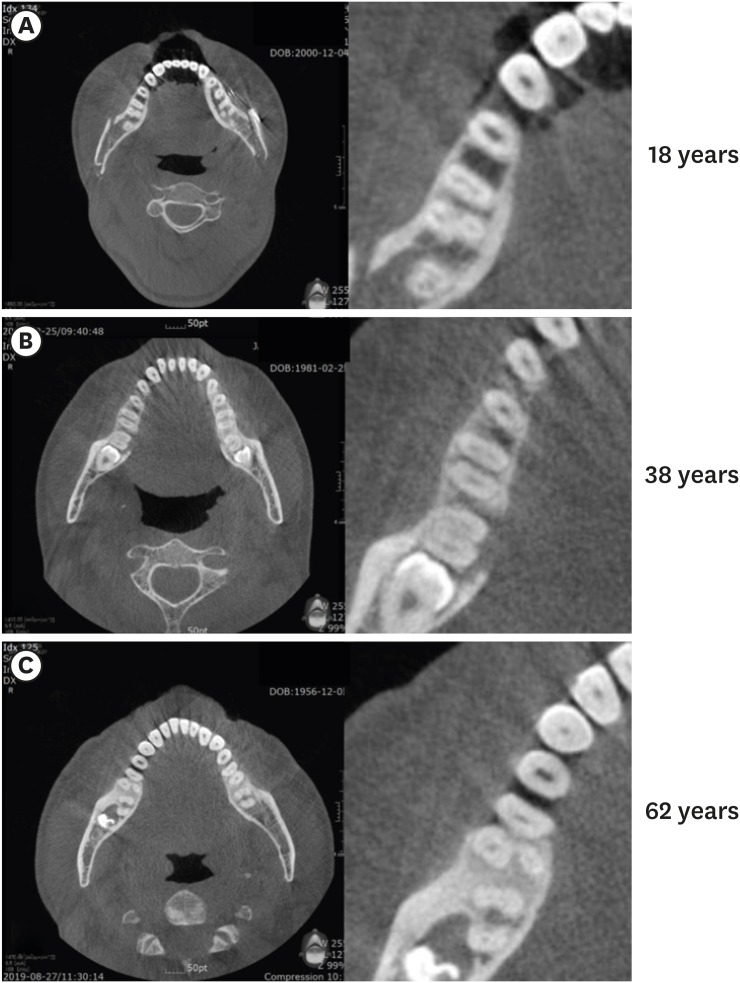
Figure 1 Panoramic radiography images showing the chamber and canal sizes according at different ages. (A) Individuals under 20 years old (13 years), (B) individuals between 20 and 40 years old (39 years), (C) individuals over 40 years old (64 years). The image in (A) shows a large chamber and a straight direction to the canal orifice. The image in (B) shows a dentin shelf area and an angulated direction to canal orifice. The image in (C) shows a thin chamber area and sclerotic canals.
Figure 2 Axial cone-beam computed tomography images of 3 mandibular first molars, showing isthmus characteristics at different ages. (A) Individuals under 20 years old (18 years): a wide canal without an isthmus, (B) individuals between 20 and 40 years old (38 years): an isthmus in the mesial root, (C) individuals who are 40 years old or more (62 years): sclerotic mesial canals without an isthmus, resembling a single canal.
Figure 1
Figure 2
Age-dependent root canal instrumentation techniques: a comprehensive narrative review
Characteristics of canal morphology and dentinal structure in different age groups
| Age groups | |||
|---|---|---|---|
| 20 years old or less | 21 to 40 years old | 41 years old or more | |
| Canal morphology [ | - Simple anatomy | - Oval and round canals | - Rounder canals with a small diameter |
| - Mostly wide-oval canal | - Prominent isthmuses | - Decreasing volume of isthmuses, more partial isthmuses up to disappearance | |
| - No isthmuses | - Auxiliary canals | - Fewer auxiliary canals | |
| - No auxiliary canals | |||
| Dentin structure [ | - Large number of tubules with large diameter | - Dentinal sclerosis starting at the apical region | - Massive obliteration of dentinal tubules |
| - Thin dentinal walls | - Reduction in the dentin water content and more modifications of collagen | ||
The algorithm for root canal instrumentation in different age groups
| 20 years old or less | 21 to 40 years old | 41 years old or more | |
|---|---|---|---|
| Instrumentation | Scraping instruments | Regular NiTi systems with subsequent agitation of sodium hypochlorite. Scraping instruments are considered in oval canals. | Manual stainless steel K-file (#06, #08, and #10) >> NiTi system for glide path >> NiTi instruments with a smaller core, with smaller taper (0.02, 0.04), and with flexible NiTi (control memory wire). |
NiTi, nickel-titanium.
Table 1 Characteristics of canal morphology and dentinal structure in different age groups
Table 2 The algorithm for root canal instrumentation in different age groups
NiTi, nickel-titanium.

