
Articles
- Page Path
- HOME > Restor Dent Endod > Volume 44(3); 2019 > Article
-
Research Article
Coronal tooth discoloration induced by regenerative endodontic treatment using different scaffolds and intracanal coronal barriers: a 6-month
ex vivo study -
Noushin Shokouhinejad1,2
 , Hassan Razmi1, Maryam Farbod1, Marzieh Alikhasi2,3,4, Josette Camilleri5
, Hassan Razmi1, Maryam Farbod1, Marzieh Alikhasi2,3,4, Josette Camilleri5 -
Restor Dent Endod 2019;44(3):e25.
DOI: https://doi.org/10.5395/rde.2019.44.e25
Published online: July 16, 2019
1Department of Endodontics, School of Dentistry, Tehran University of Medical Sciences, Tehran, Iran.
2Dental Research Center, Dentistry Research Institute, Tehran University of Medical Sciences, Tehran, Iran.
3Dental Implant Research Center, Dentistry Research Institute, Tehran University of Medical Sciences, Tehran, Iran.
4Department of Prosthodontics, School of Dentistry, Tehran University of Medical Sciences, Tehran, Iran.
5School of Dentistry, Institute of Clinical Sciences, College of Medical and Dental Sciences, University of Birmingham, Edgbaston, Birmingham, UK.
- Correspondence to Josette Camilleri. School of Dentistry, Institute of Clinical Sciences, College of Medical and Dental Sciences, University of Birmingham, 5 Mill Pool Way, Edgbaston, Birmingham B5 7EG, UK. J.Camilleri@bham.ac.uk
• Received: February 26, 2019 • Revised: June 13, 2019 • Accepted: June 27, 2019
Copyright © 2019. The Korean Academy of Conservative Dentistry
This is an Open Access article distributed under the terms of the Creative Commons Attribution Non-Commercial License (https://creativecommons.org/licenses/by-nc/4.0/) which permits unrestricted non-commercial use, distribution, and reproduction in any medium, provided the original work is properly cited.
- 3,087 Views
- 29 Download
- 20 Crossref
Abstract
-
Objective The aim of this study was to evaluate discoloration of teeth undergoing regenerative endodontic procedures (REPs) using blood clot or platelet-rich fibrin (PRF) as the scaffolds and different calcium silicate-based materials as the intracanal coronal barriers in an ex vivo model.
-
Materials and Methods Forty-eight bovine incisors were prepared and disinfected using 1 mg/mL double antibiotic paste (DAP). The specimens were then randomly divided into 2 groups (n = 24) according to the scaffolds (blood or PRF). After placement of scaffolds each group was divided into 2 subgroups (n = 12) according to the intracanal coronal barriers (ProRoot MTA or Biodentine). The pulp chamber walls were sealed with dentin bonding agent before placement of DAP and before placement of scaffolds. The color changes (∆E) were measured at different steps. The data were analyzed using 2-way analysis of variance.
-
Results Coronal discoloration induced by DAP was not clinically perceptible (ΔE ≤ 3.3). Regarding the type of the scaffold, coronal discoloration was significantly higher in blood groups compared with PRF groups at the end of REP and after 1 month (p < 0.05). However, no significant difference was found between PRF and blood clot after 6 months (p > 0.05). Considering the type of intracanal coronal barrier, no significant difference existed between ProRoot MTA and Biodentine (p > 0.05).
-
Conclusions With sealing the dentinal tubules of pulp chamber with a dentin bonding agent and application of DAP as an intracanal medicament, coronal color change of the teeth following the use of PRF and blood sealed with either ProRoot MTA or Biodentine was not different at 6-month follow-up.
INTRODUCTION
Endodontic management of immature permanent necrotic teeth is a challenging clinical procedure [1]. It has been shown that regenerative endodontic procedures (REPs) result in healing of apical periodontitis, continued radiographic root development, increasing fracture resistance and improved tooth survival in immature necrotic teeth [2,3]. However, it may contribute to tooth discoloration which is an unfavorable outcome [4,5].
Despite the increase in the number of cases reported in the literature and studies related to REPs, there is no established standardized protocol for REPs because of the lack of high levels of evidence for the outcome of regenerative treatment. REPs involve disinfection of the root canal system followed by introduction of a scaffold which is subsequently sealed with hydraulic silicate cements such as mineral trioxide aggregate (MTA) [6,7,8].
There are various types of intracanal medicaments used in REPs for disinfection of the root canal system. Triple antibiotic paste (TAP) consisting of ciprofloxacin, metronidazole, and minocycline is the most commonly used medicament in REPs [9]. However, tooth discoloration caused by TAP is well documented [4,10,11,12,13]. It has been shown that minocycline is the major cause of discoloration [4,13]. The efficacy of dentin bonding agent (DBA) for sealing the dentinal tubules of pulp chamber to decrease tooth discoloration caused by TAP has been supported by some articles [4,11,12], but it is not completely effective [12]. Therefore, it is suggested to use double antibiotic paste containing ciprofloxacin and metronidazole [10] or calcium hydroxide [7] instead of TAP, as well as to substitute minocycline with other antibiotics [10,14].
In several reports in REPs, evoked bleeding technique has been used to produce a blood clot scaffold [8], which promotes proliferation and differentiation of progenitor/stem cells [1]. Recent studies have used alternative scaffolds such as platelet-rich fibrin (PRF) and platelet-rich plasma (PRP) in regenerative endodontic treatment [15,16,17]. It has been stated that PRF is an ideal purely autologous scaffold for regeneration, which constitutes key growth factors for promoting the proliferation and differentiation of progenitor/stem cells [3,18].
After introduction of scaffolds to the root canal, it should be sealed coronally. It has been shown that MTA was the most popular intracanal barrier [8]. However, several studies have revealed the tooth discoloration potential of MTA, especially when it is in contact to blood [19,20]. To overcome tooth discoloration induced by MTA, it has been suggested to select other calcium silicate-based cements with lower potential of crown discoloration in teeth where there is an aesthetic concern [6].
To the best of our knowledge, there is no information regarding the discoloration ability of calcium silicate-based materials in contact to PRF as a scaffold in REPs. Therefore, the aim of this study was to evaluate coronal discoloration of teeth undergoing REPs using blood clot or PRF as the scaffolds, and ProRoot MTA (Dentsply Tulsa Dental Products, Tulsa, OK, USA) or Biodentine (Septodont, Saint Maur des Fosses, France) as the intracanal coronal barrier in an ex vivo model of regenerative endodontic procedure.
MATERIALS AND METHODS
Forty-eight bovine mandibular incisors from animals of nearly the same age and with almost similar crown and root size were selected. After disinfection by immersion in 0.5% chloramine T solution for 48 hours, teeth were stored in normal saline solution until use.
The apical part of each specimen was resected perpendicular to its long axis to create a standardized root length of 15 mm below the labial cementoenamel junction (CEJ). The apical 4 mm of the root canals was sealed with a composite resin material (Grandio; Voco GmbH, Cuxhaven, Germany) according to the manufacturer's instructions. Endodontic access cavities were then prepared and the root canals were shaped using #3 to #6 Gates Glidden drills, and irrigated with 20 mL 1.5% NaOCl followed by 20 mL 17% ethylenediaminetetraacetic acid (EDTA) each for 5 minutes [6,7]. Afterwards, the internal walls of the pulp chamber were sealed with a DBA according to the manufacturer's instructions as follows: after the inner surfaces of the pulp chamber was etched for 15 seconds with 35% phosphoric acid (Vococid; Voco GmbH), the dentin bonding agent (Solobond M; Voco GmbH) was applied to the etched surfaces and cured for 20 seconds.
Double antibiotic mixture was prepared by mixing equal proportions of ciprofloxacin and metronidazole (1:1) with sterile water to a final concentration of 1 mg/mL. Antibiotic mixture was inserted into the canal with a syringe to ensure that the solution remained below the labial CEJ. Access cavities were then filled with a temporary filling material (Zonalin; Kemdent, Swindon, UK). The specimens were incubated at 37°C in fully saturated humidity for 4 weeks. The access cavities were reopened and the root canals were irrigated with 20 mL 17% EDTA for 5 minutes and dried with paper points. For dealing with the possibility of damaged previous DBA layer during temporary filling material removal, DBA was reapplied on the access cavity walls in the same manner described for the first application of DBA. After that, it was attempted to perform the random sampling allocation stratified by the initial color of specimens or to one of these two groups as follows:
Group 1: the root canals were filled with human blood using a syringe up to 4 mm below the facial CEJ and it was allowed to form a blood clot for 15 minutes.
Group 2: the root canals were filled with PRF as a scaffold up to 4 mm below the facial CEJ. For the PRF preparation, human blood was collected in sterile tubes from the cubital vein. The tubes were centrifuged for 8 minutes with a speed of 1,300 rpm (DUO Quattro Centrifuge, Nice, France). Three layers were formed inside each test tube: a base layer containing erythrocytes, an intermediate layer of PRF, and a surface layer of platelet poor plasma. The PRF was separated from the other layers.
The whole fresh human blood used in this study was collected from healthy consented volunteers by a trained individual, and approved by a panel from the Tehran University of Medical Sciences Ethical Committee (Ethics code: IR.TUMS.VCR.REC. 1396.2977).
The specimens in each group were randomly divided into two experimental subgroups (n = 12) and labeled according to the applied intracanal coronal barrier. ProRoot MTA and Biodentine was prepared according to the manufacturers' instructions, and a 3-mm layer of material was placed on the top of the scaffold. A wet cotton pellet with saline was placed over the endodontic materials and the cavity was temporarily sealed with Coltosol (Coltene, Altstätten, Switzerland). The specimens were incubated at 37°C in fully saturated humidity for 72 hours. Subsequently, after confirming the setting of coronal barriers, the access cavities were filled with composite resin material, A1 shade (Grandio; Voco GmbH). The shade of the composite was matched to the coronal tooth structure measured with a spectrophotometer (Vita Easyshad; VITA Zahnfabrik, Bad Säckingen, Germany).
The specimens were incubated at 37 °C in fully saturated humidity between the steps until the end of the study.
For reproducible color assessment, a rectangular window measuring 3 × 3 mm was created at the cervical third of the crown using a needle-shaped diamond bur. A spectrophotometer (Vita Easyshad; VITA Zahnfabrik) was used to measure the L*, a*, and b* values. L* indicates the value of lightness-darkness, a* indicates greenness-redness, and b* indicates blueness-yellowness. The device was calibrated before use for each specimen. Color measurements were performed at the following 5 steps:
1. Initial: prior to application of antibiotic mixture as the baseline color
2. After DAP therapy: 4 weeks after placement of antibiotic mixture
3. After REP: after placement of scaffolds, intracanal coronal barriers and coronal restoration
4. At 1-month follow-up
5. At 6-month follow-up
The color measurements were taken 3 times inside the marked window. The mean value of 3 measurements was calculated at each time interval. The color change (ΔE) between the initial step and the other steps was calculated using the following formula:
Photographs were taken of the specimens at each treatment step using a digital camera for informal visual comparison.
Data were evaluated using SPSS software (PASW Statistics 18; SPSS Inc, Chicago, IL, USA). To evaluate the effect of the type of intracanal coronal barrier and scaffold on color change, the data were analyzed using 2-way analysis of variance. The level of statistically significant difference was set at p < 0 .05.
RESULTS
The mean values for the color changes in each subgroup are shown in Figures 1 and 2. The findings showed that coronal discoloration after 4-week DAP therapy was under clinically perceptible threshold (ΔE ≤ 3.3). The results revealed that considering the type of the scaffold, crown discoloration was significantly higher in blood clot groups compared with PRF groups at the end of REP, and also 1 month later (p < 0.05). However, at the 6-month follow-up, no significant difference existed between PRF and blood clot groups (p > 0.05). Regarding the type of intracanal coronal barrier, the results showed that the type of coronal barrier (ProRoot MTA or Biodentine) had no significant effect on coronal discoloration (p > 0.05).
Figure 1
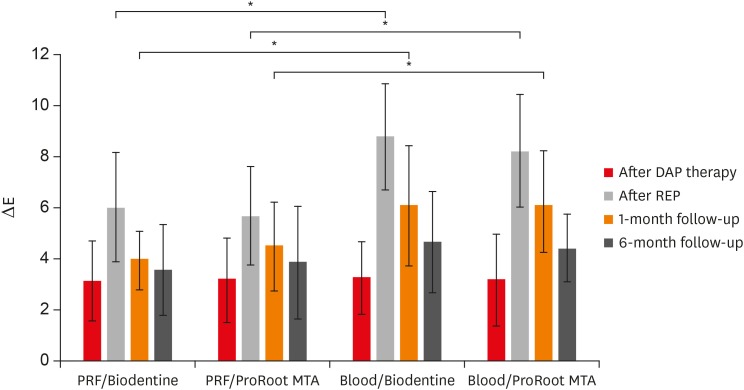
ΔE values (mean and standard deviation) of the experimental groups at the different steps. Significant difference between scaffolds (blood and platelet-rich fibrin [PRF]) was shown at the end of regenerative endodontic procedure (REP) and 1-month follow-up.
DAP, double antibiotic paste; MTA, mineral trioxide aggregate.
*p < 0.05.
Figure 2
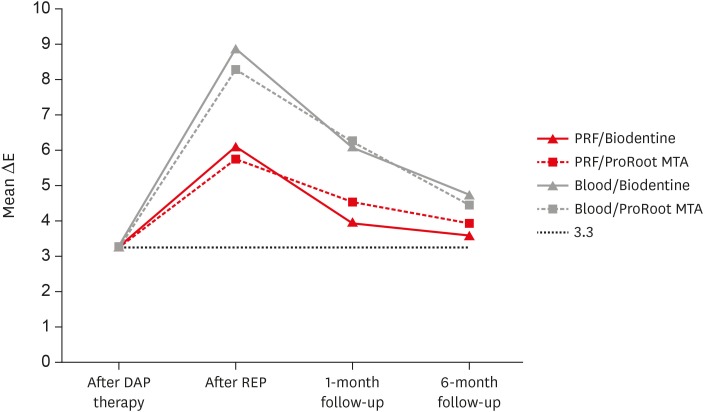
The color changes at each treatment step. The dotted line represents clinically perceptible discoloration of ΔE ≥ 3.3.
DAP, double antibiotic paste; MTA, mineral trioxide aggregate; PRF, platelet-rich fibrin; REP, regenerative endodontic procedure.
Photos of a specimen from each group are shown in Figure 3.
Figure 3

Photographs of teeth in each group. (A) At the end of 4-week antibiotic therapy. (B) At the end of endodontic regenerative procedure. (C) At 1-month follow-up. (D) At 6-month follow-up. The color changes were measured within the defined area.
MTA, mineral trioxide aggregate; PRF, platelet-rich fibrin.
DISCUSSION
Crown discoloration is a commonly reported complication of the current clinical protocols of REPs. This is the first study to evaluate and compare the crown discoloration potential of two different scaffolds sealed by 2 different calcium silicate-based materials using an ex vivo model for regeneration. Studies have shown many advantages in using bovine teeth instead of human ones [10,21,22], including a sufficient flat surface in large numbers without any restorations, caries [21], and no concern about ethical issues [23]. However, the number of tubules is higher in bovine specimens compared with human dentin [23], which might influence the penetration of the materials in the dentin.
In the study, DAP was used as intracanal medicament. The most common medicament used in REPs is TAP containing minocycline and it has been applied as intracanal medicament in 80% of the clinical articles [9]. However, it poses disadvantage of severe tooth discoloration even in low concentrations [4,10,12]. It has been shown that coronal discoloration caused by TAP could not be prevented even with sealing the dentinal tubules of pulp chamber walls [12]. Although the European Sciety of Endodontology (ESE) position statement advocates a nondiscoloring calcium hydroxide as an intracanal medicament [7], antibiotic mixtures are still recommended by the American Association of Endodontists [6]. Double antibiotic paste has been recommended to prevent discoloration caused by minocycline in TAP [6], and was succesfully used in endodotic regeneration [24,25]. The precise preparation method of TAP and DAP is not mentioned in most of the studies and case reports. It has been shown that residual antibacterial effect of TAP or DAP at a concentration of 1 mg/mL was comparable with those concentrations currently used in REPs (1,000 mg/mL) [26]. Therefore, 1 mg/mL DAP was used in this study which may also have less cytotoxicity in clinical conditions due to lower concentration [27].
A ΔE value greater than 3.3 is considered to be perceivable color change [28]. In this study, coronal discoloration after a 4-week antibiotic therapy period was less than the clinically perceptible value (ΔE ≤ 3.3). This finding is in accordance with Akcay et al. [10] which showed that using DAP for 3 weeks did not cause any noticeable coronal discoloration unlike TAP.
This study revealed that application of PRF instead of blood clot as a scaffold resulted in significant decreased crown discoloration at the end of REPs and 1 month later. Several studies have shown tooth discoloration potential of blood [20,29], possibly due to the penetration of erythrocytes into the tooth structure [20], and accumulation of hemoglobin and hematin molecules in dentinal tubules after hemolysis of erythrocytes [30]. In current study, greater discoloration in the blood groups does not seem to be related to the penetration of erythrocytes into the coronal tooth structure as the dental walls of the pulp chamber had been sealed using DBA. Furthermore, it was attempted to deliver blood into the canals without contamination of the pulp chamber. However, the proximity of blood contaminated cervical root dentin to the cervical third of the crown where assessment of discoloration was evaluated can be a reason for this finding. Moreover, absorption of blood into the fresh unset calcium silicate-based materials which were located in the cervical area of the root might be another reason for more discoloration in blood groups. Ferrous (Fe2+) ion in the center of heme group of blood which possesses a red color becomes ferric (Fe3+) which has a dark brown color due to a natural redox reaction that may result in discoloration of materials [20,
31]. It has been shown that blood contamination exacerbated discoloration induced by calcium silicate-based materials containing bismuth oxide or other radiopacifiers [19,29,31]. Therefore, the higher tooth discoloration in blood groups at the end of regenerative endodontic procedure and 1-m later could be attributed to color changes of intracanal coronal barriers exposed to blood. The lower discoloration induced by PRF at mentioned steps might be associated with the lack of erythrocytes in platelet derivatives.
It is suggested to use alternatives to ProRoot MTA such as Biodentine to seal the scaffolds where there is an esthetic concern [6]. In a systematic review, Możyńska et al. [32] reported that ProRoot MTA showed a strong potential for staining compared to Biodentine. However, the results of the present study showed no significant difference between discoloration potential of Biodentine and ProRoot MTA. This result is in accordance with the findings of our previous study [12] which did not reveal significant difference between tooth color change induced by ProRoot MTA and Biodentine placed over the blood clot when the pulp chamber walls were sealed with DBA. However, in studies that showed more coronal discoloration associated with ProRoot MTA, MTA-dentin interface was not sealed [28,33]. The amino acids in dentin collagen seem to destabilize bismuth oxide molecule in MTA, resulting in eventual change in color to black [34]. Tooth discoloration has been shown to be caused by movement of discolored bismuth from the material to the tooth structure by ion exchange [35]. Thus, less color change seen following the use of ProRoot MTA in the present study might be related to the sealing of the pulp chamber dentinal walls with DBA, leading to prevention of bismuth migration to the tooth structure.
Despite the more significant crown discoloration found in the blood groups at the end of regenerative endodontic procedure and 1-month follow-up, no significant difference existed at 6-month follow-up among blood and PRF groups. At 6-month follow-up, regenerative protocols used in the current study resulted in color change values which were slightly more than the clinically perceptible ones.
In the present study, color change was not incremental, and reverted from the end of REP to 6-month follow-up. Furthermore, reduction of color changes was more evident in blood groups compared with PRF groups. This finding might be related to the alteration of erythrocytes via physiological degradation over time, thus resulting in the change of optical properties of materials and dental tissues [20]. This finding should be further investigated.
Although there is little information on color stability of calcium silicate-based materials exposed to PRF, the protocol used in this study, including covering the dentinal tubules of pulp chamber with DBA and application of DAP as the intracanal medicament seems promising to decrease the coronal color change in teeth undergoing REPs even after introduction of blood into the root canals and sealing the scaffolds using bismuth oxide containing calcium silicate based materials.
It is worth to mention that in this study, both scaffold materials were not in contact to neither bone fluids nor blood from the normal human body stream. Further clinical studies are needed to evaluate the outcome of this protocol in REPs.
CONCLUSIONS
Under the conditions of this study, the use of a low concentration of DAP (1 mg/mL) following covering dentinal walls of the pulp chamber led to slight coronal color change which was less than the clinically noticeable value. No significant difference was found between the crown color change following the application of ProRoot MTA and Biodentine placed below the labial CEJ for sealing the scaffolds at any time intervals.
ACKNOWLEDGEMENTS
The authors wish to thank Dr. MJ. Kharrazifard for his assistance in statistical analysis. The authors deny any conflicts of interest related to this study.
-
Funding: This study was funded by Tehran University of Medical Sciences (grant No. 35610).
-
Conflict of Interest: No potential conflict of interest relevant to this article was reported.
-
Author Contributions:
Conceptualization: Shokouhinejad N, Razmi H, Alikhasi M, Farbod M, Camilleri J.
Data curation: Shokouhinejad N, Farbod M.
Formal analysis: Alikhasi M.
Investigation: Shokouhinejad N, Farbod M, Alikhasi M.
Methodology: Shokouhinejad N, Razmi H, Alikhasi M.
Supervision: Shokouhinejad N, Razmi H, Camilleri J.
Writing - original draft: Farbod M, Alikhasi M.
Writing - review & editing: Shokouhinejad N, Camilleri J.
- 1. Nosrat A, Homayounfar N, Oloomi K. Drawbacks and unfavorable outcomes of regenerative endodontic treatments of necrotic immature teeth: a literature review and report of a case. J Endod 2012;38:1428-1434.ArticlePubMed
- 2. Hargreaves KM, Diogenes A, Teixeira FB. Treatment options: biological basis of regenerative endodontic procedures. J Endod 2013;39:S30-S43.ArticlePubMedPMC
- 3. Hargreaves KM, Giesler T, Henry M, Wang Y. Regeneration potential of the young permanent tooth: what does the future hold? J Endod 2008;34:S51-S56.ArticlePubMed
- 4. Kim JH, Kim Y, Shin SJ, Park JW, Jung IY. Tooth discoloration of immature permanent incisor associated with triple antibiotic therapy: a case report. J Endod 2010;36:1086-1091.ArticlePubMed
- 5. Park HB, Lee BN, Hwang YC, Hwang IN, Oh WM, Chang HS. Treatment of non-vital immature teeth with amoxicillin-containing triple antibiotic paste resulting in apexification. Restor Dent Endod 2015;40:322-327.ArticlePubMedPMC
- 6. American Association of Endodontists. AAE clinical considerations for a regenerative procedure. Revised 6-8-16 [Internet]. Chicago (IL): American Association of Endodontists; 2017. cited 2017 Jul 30]. Available from: https://www.aae.org/specialty/wp-content/uploads/sites/2/2017/06/currentregenerativeendodonticconsiderations.pdf.
- 7. Galler KM, Krastl G, Simon S, Van Gorp G, Meschi N, Vahedi B, Lambrechts P. European Society of Endodontology position statement: revitalization procedures. Int Endod J 2016;49:717-723.ArticlePubMed
- 8. Lee BN, Moon JW, Chang HS, Hwang IN, Oh WM, Hwang YC. A review of the regenerative endodontic treatment procedure. Restor Dent Endod 2015;40:179-187.ArticlePubMedPMC
- 9. Kontakiotis EG, Filippatos CG, Tzanetakis GN, Agrafioti A. Regenerative endodontic therapy: a data analysis of clinical protocols. J Endod 2015;41:146-154.ArticlePubMed
- 10. Akcay M, Arslan H, Yasa B, Kavrık F, Yasa E. Spectrophotometric analysis of crown discoloration induced by various antibiotic pastes used in revascularization. J Endod 2014;40:845-848.ArticlePubMed
- 11. Reynolds K, Johnson JD, Cohenca N. Pulp revascularization of necrotic bilateral bicuspids using a modified novel technique to eliminate potential coronal discolouration: a case report. Int Endod J 2009;42:84-92.ArticlePubMed
- 12. Shokouhinejad N, Khoshkhounejad M, Alikhasi M, Bagheri P, Camilleri J. Prevention of coronal discoloration induced by regenerative endodontic treatment in an ex vivo model. Clin Oral Investig 2018;22:1725-1731.ArticlePubMedPDF
- 13. Porter ML, Münchow EA, Albuquerque MT, Spolnik KJ, Hara AT, Bottino MC. Effects of novel 3-dimensional antibiotic-containing electrospun scaffolds on dentin discoloration. J Endod 2016;42:106-112.ArticlePubMed
- 14. Kahler B, Mistry S, Moule A, Ringsmuth AK, Case P, Thomson A, Holcombe T. Revascularization outcomes: a prospective analysis of 16 consecutive cases. J Endod 2014;40:333-338.ArticlePubMed
- 15. Torabinejad M, Faras H. A clinical and histological report of a tooth with an open apex treated with regenerative endodontics using platelet-rich plasma. J Endod 2012;38:864-868.ArticlePubMed
- 16. Güven Polat G, Yıldırım C, Akgün OM, Altun C, Dinçer D, Ozkan CK. The use of platelet rich plasma in the treatment of immature tooth with periapical lesion: a case report. Restor Dent Endod 2014;39:230-234.ArticlePubMedPMC
- 17. Shivashankar VY, Johns DA, Maroli RK, Sekar M, Chandrasekaran R, Karthikeyan S, Renganathan SK. Comparison of the effect of PRP, PRF and induced bleeding in the revascularization of teeth with necrotic pulp and open apex: a triple blind randomized clinical trial. J Clin Diagn Res 2017;11:ZC34-ZC39.ArticlePubMedPMC
- 18. Huang FM, Yang SF, Zhao JH, Chang YC. Platelet-rich fibrin increases proliferation and differentiation of human dental pulp cells. J Endod 2010;36:1628-1632.ArticlePubMed
- 19. Shokouhinejad N, Nekoofar MH, Pirmoazen S, Shamshiri AR, Dummer PM. Evaluation and comparison of occurrence of tooth discoloration after the application of various calcium silicate-based cements: an ex vivo study. J Endod 2016;42:140-144.ArticlePubMed
- 20. Felman D, Parashos P. Coronal tooth discoloration and white mineral trioxide aggregate. J Endod 2013;39:484-487.ArticlePubMed
- 21. Schilke R, Lisson JA, Bauss O, Geurtsen W. Comparison of the number and diameter of dentinal tubules in human and bovine dentine by scanning electron microscopic investigation. Arch Oral Biol 2000;45:355-361.ArticlePubMed
- 22. Kato MT, Hannas AR, Leite AL, Bolanho A, Zarella BL, Santos J, Carrilho M, Tjäderhane L, Buzalaf MA. Activity of matrix metalloproteinases in bovine versus human dentine. Caries Res 2011;45:429-434.ArticlePubMedPDF
- 23. Camargo MA, Marques MM, de Cara AA. Morphological analysis of human and bovine dentine by scanning electron microscope investigation. Arch Oral Biol 2008;53:105-108.ArticlePubMed
- 24. Fahmy SH, Hassanien EE, Nagy MM, El Batouty KM, Mekhemar M, Fawzy El Sayed K, Hassanein EH, Wiltfang J, Dörfer C. Investigation of the regenerative potential of necrotic mature teeth following different revascularisation protocols. Aust Endod J 2017;43:73-82.ArticlePubMedPDF
- 25. Iwaya SI, Ikawa M, Kubota M. Revascularization of an immature permanent tooth with apical periodontitis and sinus tract. Dent Traumatol 2001;17:185-187.ArticlePubMedPDF
- 26. Sabrah AH, Yassen GH, Spolnik KJ, Hara AT, Platt JA, Gregory RL. Evaluation of residual antibacterial effect of human radicular dentin treated with triple and double antibiotic pastes. J Endod 2015;41:1081-1084.ArticlePubMed
- 27. Ruparel NB, Teixeira FB, Ferraz CC, Diogenes A. Direct effect of intracanal medicaments on survival of stem cells of the apical papilla. J Endod 2012;38:1372-1375.ArticlePubMed
- 28. Marconyak LJ Jr, Kirkpatrick TC, Roberts HW, Roberts MD, Aparicio A, Himel VT, Sabey KA. A comparison of coronal tooth discoloration elicited by various endodontic reparative materials. J Endod 2016;42:470-473.ArticlePubMed
- 29. Lenherr P, Allgayer N, Weiger R, Filippi A, Attin T, Krastl G. Tooth discoloration induced by endodontic materials: a laboratory study. Int Endod J 2012;45:942-949.ArticlePubMed
- 30. Marin PD, Heithersay GS, Bridges TE. A quantitative comparison of traditional and non-peroxide bleaching agents. Endod Dent Traumatol 1998;14:64-67.ArticlePubMed
- 31. Guimarães BM, Tartari T, Marciano MA, Vivan RR, Mondeli RF, Camilleri J, Duarte MA. Color stability, radiopacity, and chemical characteristics of white mineral trioxide aggregate associated with 2 different vehicles in contact with blood. J Endod 2015;41:947-952.ArticlePubMed
- 32. Możyńska J, Metlerski M, Lipski M, Nowicka A. Tooth discoloration induced by different calcium silicate-based cements: a systematic review of in vitro studies. J Endod 2017;43:1593-1601.ArticlePubMed
- 33. Vallés M, Roig M, Duran-Sindreu F, Martínez S, Mercadé M. Color stability of teeth restored with biodentine: a 6-month in vitro study. J Endod 2015;41:1157-1160.ArticlePubMed
- 34. Marciano MA, Costa RM, Camilleri J, Mondelli RF, Guimarães BM, Duarte MA. Assessment of color stability of white mineral trioxide aggregate angelus and bismuth oxide in contact with tooth structure. J Endod 2014;40:1235-1240.ArticlePubMed
- 35. Marciano MA, Duarte MA, Camilleri J. Dental discoloration caused by bismuth oxide in MTA in the presence of sodium hypochlorite. Clin Oral Investig 2015;19:2201-2209.ArticlePubMedPDF
REFERENCES
Tables & Figures
REFERENCES
Citations
Citations to this article as recorded by 
- Effect of Addition of Zinc Oxide on Color Stability of a Calcium Silicate–Based Cement Containing Bismuth Oxide in the Presence of Blood and Sodium Hypochlorite
Mehrfam Khoshkhounejad, Noushin Shokouhinejad, Pegah Sarraf, MohammadHossein Mirisiahi, Hannah Wesley
International Journal of Dentistry.2026;[Epub] CrossRef - Calcium Silicate-Based Cements for Vital Pulp Therapy: Integrated Assessment of Radiopacity, Elemental Composition, and 24-h Pulp Cell Responses
Belen Şirinoğlu Çapan, Vasfiye Işık, Tugba Elgün, Zeynep Hale Keleş, Soner Şişmanoğlu
Biomimetics.2026; 11(4): 280. CrossRef - Effect of output intensity of light curing unit on coronal tooth discoloration induced by silicate calcium-based materials: an ex vivo study
Fatemeh Farshad, Noushin Shokouhinejad, Parham Pedram, Mohammad Javad KharaziFard, Elham Ahmadi
Biomaterial Investigations in Dentistry.2026; 13: 379. CrossRef - Efficacy of combined scaffolds and sodium hypochlorite in regenerative endodontics of immature teeth (in-vivo study)
Hanan Arb, Abeer Darrag, Neveen Shaheen, Dina Attia
Tanta Dental Journal.2026; 23(2): 240. CrossRef - Bridging Developmental Biology and Regenerative Endodontics: Postnatal Rat Tooth Germ as A Model for Root Dentinogenesis
Maryam Hameed Alwan, Jwan Arkan M. Saeed
Odovtos - International Journal of Dental Sciences.2026;[Epub] CrossRef - Impact of Biodentine Placement on Fracture Resistance and its Influence on Discoloration with Different Scaffolds
Evren Sarıyılmaz, Öznur Sarıyılmaz, Burak Çarıkçıoğlu, Gülşah Uslu, Raif Alan
Journal of Endodontics.2025; 51(9): 1199. CrossRef - Effect of pH on the solubility and volumetric change of ready-to-use Bio-C Repair bioceramic material
Luana Raphael da SILVA, Jader Camilo PINTO, Juliane Maria GUERREIRO-TANOMARU, Mário TANOMARU-FILHO
Brazilian Oral Research.2024;[Epub] CrossRef - Efficacy of Potassium Iodide and Glutathione for Correlation of Dentin Discoloration Caused by Silver Diamine Fluoride
Mahsa Samani, Hamid Majzoub, Faramarz Zakavi, Ayyub Mojaddami
Cureus.2024;[Epub] CrossRef - Intracanal medicaments and coronal sealing materials influence on root fracture resistance and coronal discoloration: An in vitro study
Rasoul Sahebalam, Marzie Boskabady, Maryam Naghavi, Samira Dehghanitafti
Saudi Endodontic Journal.2024; 14(2): 199. CrossRef - Potential Crown Discoloration Induced by the Combination of Various Intracanal Medicaments and Scaffolds Applied in Regenerative Endodontic Therapy
NB Altun, A Turkyilmaz
Nigerian Journal of Clinical Practice.2024; 27(7): 897. CrossRef - Evaluation of the effectiveness of different treatment approaches in preventing coronal discoloration caused by regenerative endodontic treatment
Melis Oya Ateş, Zeliha Uğur Aydın
Clinical Oral Investigations.2023; 27(8): 4595. CrossRef - Evaluation of the Effectiveness of Laser‐Assisted Bleaching of the Teeth Discolored due to Regenerative Endodontic Treatment
Noushin Shokouhinejad, Mehrfam Khoshkhounejad, Fatemeh Hamidzadeh, Murilo Baena Lopes
International Journal of Dentistry.2022;[Epub] CrossRef - Effectiveness of Teeth Whitening after Regenerative Endodontics Procedures: An In Vitro Study
Irini Fagogeni, Joanna Metlerska, Tomasz Falgowski, Maciej Górski, Mariusz Lipski, Alicja Nowicka
Journal of Clinical Medicine.2022; 11(23): 7016. CrossRef - Microstructure and color stability of calcium silicate-based dental materials exposed to blood or platelet-rich fibrin
Noushin Shokouhinejad, Ibrahim Abu Tahun, Shima Saber Tahan, Fatemeh Mohandes, Mohammad H. Nekoofar, Paul M. H. Dummer
Clinical Oral Investigations.2022; 27(3): 1193. CrossRef - Spectrophotometric analysis of internal bleaching of traumatized teeth with coronal discoloration following regenerative endodontic procedures
Jaqueline Lazzari, Walbert Vieira, Vanessa Pecorari, Brenda Paula Figueiredo de Almeida Gomes, José Flávio Affonso de Almeida, Adriana De-Jesus-Soares
Brazilian Journal of Oral Sciences.2021;[Epub] CrossRef - Biological parameters, discolouration and radiopacity of calcium silicate‐based materials in a simulated model of partial pulpotomy
Lilian Vieira Oliveira, Gabriela Leite de Souza, Gisele Rodrigues da Silva, Thamara Eduarda Alves Magalhães, Gabrielle Alves Nunes Freitas, Ana Paula Turrioni, Gabriella Lopes de Rezende Barbosa, Camilla Christian Gomes Moura
International Endodontic Journal.2021; 54(11): 2133. CrossRef - Effect of hydrogel-based antibiotic intracanal medicaments on crown discoloration
Rayan B. Yaghmoor, Jeffrey A. Platt, Kenneth J. Spolnik, Tien Min Gabriel Chu, Ghaeth H. Yassen
Restorative Dentistry & Endodontics.2021;[Epub] CrossRef - The effect of different calcium silicate-based pulp capping materials on tooth discoloration: an in vitro study
Ahmad S. Al-Hiyasat, Dana M. Ahmad, Yousef S. Khader
BMC Oral Health.2021;[Epub] CrossRef - Knowledge, attitudes, and practices of undergraduate students concerning Regenerative Endodontics
Ligia B. da Silva, Mariana Gabriel, Márcia M. Marques, Fernanda C. Carrer, Flávia Gonçalves, Giovanna Sarra, Giovanna L. Carvalho, Ana Armas-Vega, Maria S. Moreira
Minerva Stomatologica.2020;[Epub] CrossRef - Coronal Discoloration Related to Bioceramic and Mineral Trioxide Aggregate Coronal Barrier in Non-vital Mature Teeth Undergoing Regenerative Endodontic Procedures
Mazen Doumani, Mohammad Yaman Seirawan, Kinda Layous, Mohammad Kinan Seirawan
World Journal of Dentistry.2020; 11(1): 52. CrossRef
 ePub Link
ePub Link Cite
CiteCoronal tooth discoloration induced by regenerative endodontic treatment using different scaffolds and intracanal coronal barriers: a 6-month ex vivo study
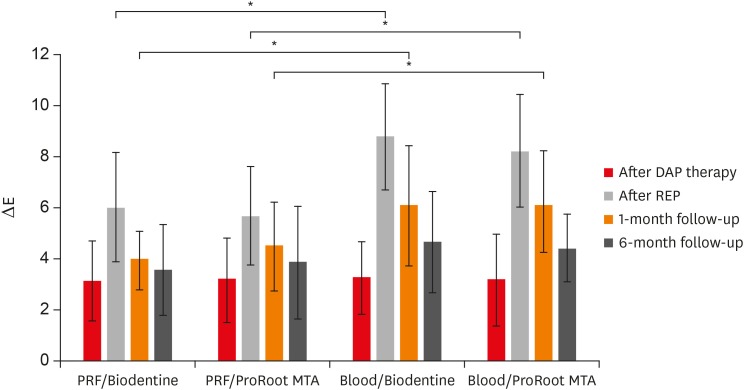
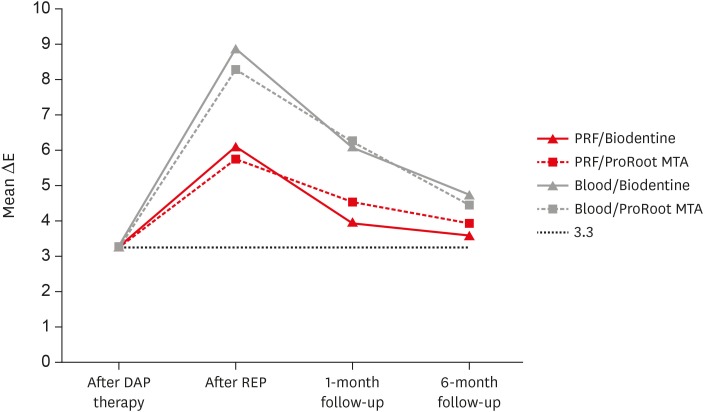
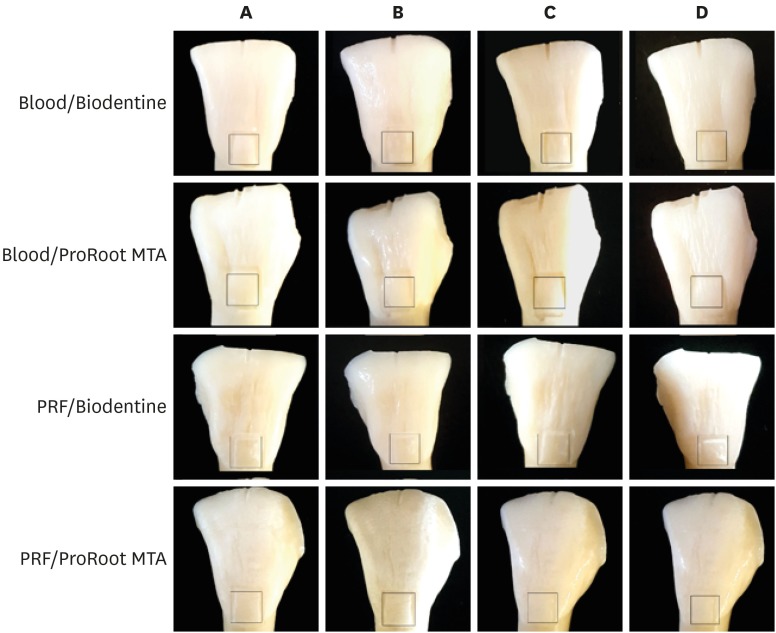
Figure 1 ΔE values (mean and standard deviation) of the experimental groups at the different steps. Significant difference between scaffolds (blood and platelet-rich fibrin [PRF]) was shown at the end of regenerative endodontic procedure (REP) and 1-month follow-up.DAP, double antibiotic paste; MTA, mineral trioxide aggregate.*p < 0.05.
Figure 2 The color changes at each treatment step. The dotted line represents clinically perceptible discoloration of ΔE ≥ 3.3.DAP, double antibiotic paste; MTA, mineral trioxide aggregate; PRF, platelet-rich fibrin; REP, regenerative endodontic procedure.
Figure 3 Photographs of teeth in each group. (A) At the end of 4-week antibiotic therapy. (B) At the end of endodontic regenerative procedure. (C) At 1-month follow-up. (D) At 6-month follow-up. The color changes were measured within the defined area.MTA, mineral trioxide aggregate; PRF, platelet-rich fibrin.
Figure 1
Figure 2
Figure 3
Coronal tooth discoloration induced by regenerative endodontic treatment using different scaffolds and intracanal coronal barriers: a 6-month ex vivo study

