
Articles
- Page Path
- HOME > Restor Dent Endod > Volume 43(3); 2018 > Article
-
Research Article
Retention of BioAggregate and MTA as coronal plugs after intracanal medication for regenerative endodontic procedures: an
ex vivo study -
Suzan Abdul Wanees Amin
 , Shaimaa Ismail Gawdat
, Shaimaa Ismail Gawdat -
Restor Dent Endod 2018;43(3):e18.
DOI: https://doi.org/10.5395/rde.2018.43.e18
Published online: April 26, 2018
Department of Endodontics, Faculty of Dentistry, Cairo University, Cairo, Egypt.
- Correspondence to Suzan Abdul Wanees Amin, BDS, MSc, PhD. Associate Professor, Department of Endodontics, Faculty of Dentistry, Cairo University, 12 El Saraya Street, Manial ElRoda, 11451 Cairo, Egypt. swanees@rocketmail.com
• Received: October 31, 2017 • Accepted: March 4, 2018
Copyright © 2018. The Korean Academy of Conservative Dentistry
This is an Open Access article distributed under the terms of the Creative Commons Attribution Non-Commercial License (https://creativecommons.org/licenses/by-nc/4.0/) which permits unrestricted non-commercial use, distribution, and reproduction in any medium, provided the original work is properly cited.
- 2,740 Views
- 10 Download
- 8 Crossref
Abstract
-
Objectives This study compared the retention of BioAggregate (BA; Innovative BioCeramix) and mineral trioxide aggregate (MTA; Angelus) as coronal plugs after applying different intracanal medications (ICMs) used in regenerative endodontics.
-
Materials and Methods One-hundred human maxillary central incisors were used. The canals were enlarged to a diameter of 1.7 mm. Specimens were divided into 5 groups (n = 20) according to the ICM used: calcium hydroxide (CH), 2% chlorhexidine (CHX), triple-antibiotic paste (TAP), double-antibiotic paste (DAP), and no ICM (control; CON). After 3 weeks of application, ICMs were removed and BA or MTA were placed as the plug material (n = 10). The push-out bond strength and the mode of failure were assessed. The data were analyzed using 2-way analysis of variance, the Tukey's test, and the χ2 test; p values < 0.05 indicated statistical significance.
-
Results The type of ICM and the type of plug material significantly affected bond strength (p < 0.01). Regardless of the type of ICM, BA showed a lower bond strength than MTA (p < 0.05). For MTA, CH showed a higher bond strength than CON, TAP and DAP; CHX showed a higher bond strength than DAP (p < 0.01). For BA, CH showed a higher bond strength than DAP (p < 0.05). The mode of failure was predominantly cohesive for BA (p < 0.05).
-
Conclusions MTA may show better retention than BA. The mode of bond failure with BA can be predominantly cohesive. BA retention may be less affected by ICM type than MTA retention.
INTRODUCTION
Disinfection of the root canal space is of paramount importance for a successful outcome. Disinfection can be performed mechanically, through canal instrumentation, or chemically, through irrigation and intracanal medication (ICM). Chemical disinfection plays a greater role for immature teeth subjected to regenerative endodontic procedures (REPs) because minimal mechanical instrumentation is allowed in such teeth [1].
Several irrigant/ICM combinations have been used in REPs, with triple-antibiotic paste (TAP) being the most commonly-used ICM [2], due to its possible discoloration potential [3]; however, alternatives, such as double-antibiotic paste (DAP) and calcium hydroxide (CH), have been used [2]. Chlorhexidine (CHX) has been used in endodontics as an irrigant and an ICM. It has been proposed as an alternative to CH and antibiotics in REPs, as it shows similar antibacterial effects [4] and may have fewer adverse effects on dentin [5,6]. It has been used alone or in combination with CH [2].
Calcium-silicate cements (CSCs) have been the top choice as coronal plugs, as they provide an efficient bacteria-tight and biocompatible seal [1,2]. CSC derivatives can be either Portland cement-based materials, such as mineral trioxide aggregate (MTA), or tricalcium silicate (TCS)-based materials, such as Biodentine and BioAggregate (BA; Innovative BioCeramix, Vancouver, BC, Canada) [7,8]. BA also contains monobasic calcium phosphate, amorphous silicon dioxide, and tantalum pentoxide for radiopacity [9,10]; it is considered a biphasic material (a material containing 2 cementitious materials), due to its calcium phosphate content [11,12]. BA shows a higher resistance to acids [10,13], exerts a longer-term strengthening effect on weakened teeth [14], and has less potential for discoloration [15] than MTA. It has shown similar success to MTA in treating immature teeth [16].
Some authors have investigated the effect of the ICM used in REPs on the bonding potential of MTA and Biodentine with varying results [17,18,19,20]. No studies to date have assessed the effect of such ICMs on the retention of BA; it was therefore of interest to conduct an ex vivo comparison of the retention of BA and MTA as coronal plugs after the prior application of different ICMs that are used in REPs.
MATERIALS AND METHODS
The protocol of this study was approved by the institutional review board of the Faculty of Dentistry (18/2/40). A total of 100 human maxillary central incisors that had been recently extracted were used. The teeth were examined visually, under a magnification of ×3.5 (Global G6, Global Surgical Corporation, St. Louis, MO, USA), and radiographically to exclude immature, carious, cracked, resorbed, or calcified teeth. Teeth with similar dimensions in both the labio-palatal and the mesio-distal aspects were selected. The measurements were done at the level of the cementoenamel junction (CEJ) using a digital caliper (Mitutoyo, Tokyo, Japan), and teeth with a maximum of 10% deviation from the mean in each dimension were included.
Teeth were coronally accessed and the working length was established using a size 15 K-file 1 mm shorter than the tooth length. A single operator instrumented all the canals using a rotary nickel-titanium system (ProTaper Universal, Dentsply Maillefer, Ballaigues, Switzerland). The canals were instrumented up to instrument F5, and then Peeso drills (Mani, Tochigi, Japan) were used from No. 1 up to No. 6 (1.7 mm in diameter), passing 1 mm beyond the apical foramen. The teeth were then shortened to 12 mm apical to the CEJ to mimic immature roots. The canals were irrigated with 2 mL of 2.5% sodium hypochlorite (NaOCl) between every 2 consecutive instruments. A final flush was then done using 5 mL of 2.5% NaOCl and 5 mL of 17% ethylenediaminetetraacetic acid (EDTA) followed by 10 mL of distilled water. The canals were then dried with paper points (Dentsply Maillefer).
The specimens were randomly divided according to the type of the ICM used inside the canal into 5 equal groups (n = 20): 1) the CH group, in which an injectable CH paste (Ultracal XS, Ultradent Products, South Jordan, UT, USA) was used; 2) the CHX group, in which an injectable 2% CHX gel (Gluco-CHeX 2% gel, PPH CERKAMED, Stalowa Wola, Poland) was used; 3) the TAP group, in which the ICM was a TAP containing a 1:1:1 ratio of doxycycline (Vibramycin 100 mg, Pfizer Inc., New York, NY, USA), ciprofloxacin (Cipro 500 mg, Schering-Plough, Kenilworth, NJ, USA), and metronidazole (Flagyl 500 mg, Sanofi-Aventis, Tours, France); 4) the DAP group, in which the ICM was a DAP containing a 1:1 ratio of ciprofloxacin and metronidazole; 5) the control (CON) group, where no ICM was applied.
The specimens within each group were further subdivided into 2 subgroups (n = 10) according to the plug material used, as follows: MTA (Angelus, Londrina, Brazil) or BA.
For TAP, equal portions of doxycycline, ciprofloxacin, and metronidazole (1:1:1) were mixed. The powder was then mixed with distilled water at a concentration of 1 g/mL to obtain a pasty slurry with a consistency that was clinically usable and somewhat similar to the consistency of the other ICMs that were used. For DAP, only ciprofloxacin and metronidazole (1:1) were used.
All the canals were apically sealed using sticky wax to ensure containment of the ICMs inside the root canal throughout the required duration. All the ICMs used, whether in the form of a paste or a gel, were injected inside the root canals. The coronal openings were sealed with a small cotton pellet and temporary filling (Cavit G, 3M ESPE, Seefeld, Germany). The specimens were stored at 37°C in 100% humidity for 3 weeks [17] after which the ICMs were removed by a combination of light instrumentation using the master apical file followed by rinsing with 10 mL of 2.5% NaOCl, 10 mL of 17% EDTA for 1 minute, and then 10 mL of distilled water.
All the teeth were placed in moistened floral foam. An internal collagen matrix (ETIK, Pierre Rolland, Acteon, France) was used to support the placement of plug materials. The instructions of each material's manufacturer were followed. A microapical placement system (MAP, Produits Dentaires SA, Vevey, Switzerland) was used for inserting the materials into the canals, and endodontic pluggers were used for the compaction of a 3-mm coronal plug. All procedures were done under magnification (×13). All access cavities were sealed using a temporary filling (Cavit G, 3M ESPE) placed over a moistened cotton pellet in the pulp chamber [17,18,19] for 3 days. The specimens were stored at 37ºC and 100% relative humidity [17,18,19,20].
For each specimen, a 2.0 ± 0.1 mm transverse section perpendicular to the long axis of the root was sliced using an isomet saw. A universal testing machine (Model 3345, Instron, Buckinghamshire, UK) was used to dislodge the plug materials utilizing a 1.3-mm-diameter cylindrical plunger in an apical-coronal direction at a load cell of 500 N and a crosshead speed of 0.5 mm/min until failure. The maximal force applied to the material before displacement was recorded in newtons (N). The following equation was used to calculate the push-out bond strength (MPa), as an indicator of retention: Push-out bond strength (MPa) = Force to dislodgement (N)/Adhesive surface area (mm2). For each section, the adhesion surface area (A) was calculated as follows: (πr1 + πr2) × L, and the value of L was calculated as the square root of (r1 − r2)2 + h2, where π is a constant equal to 3.14, r1 is the smaller radius, r2 is the larger radius, and h is the thickness of the section in millimeters as measured using a digital caliper.
The mode of failure was evaluated by examining the sections after material displacement using a stereomicroscope (×40 magnification, SZ-PT, Olympus, Tokyo, Japan). The mode of failure was classified as adhesive (failure at the dentin-material interface), cohesive (failure within the material), or mixed (a combination of adhesive and cohesive failure within the same specimen).
Push-out bond strength data were analyzed using the 2-way analysis of variance (ANOVA) test followed by the Tukey's post hoc test for multiple comparisons. The effects of ‘The type of ICM’ and ‘The type of plug material’, as the 2 independent variables, and the effect of the interaction between these 2 independent variables (The type of plug material × The type of ICM) on the push-out bond strength, as the dependent variable, were assessed. If a statistically significant effect was found for the interaction between the 2 independent variables on the push-out bond strength, the mean values of the bond strength recorded for the different types of ICMs used were compared for each plug material separately using the 1-way ANOVA test followed by the Tukey's post hoc test for pair-wise comparisons. The mean bond strength values recorded for the 2 plug materials were also compared separately for each ICM using the Student's t-test. The incidence of the different modes of failure was analyzed using the χ2 test. The p values less than 0.05 were considered to indicate statistical significance. Statistical analysis was performed using SPSS 20.0 for Windows (IBM Corp., Armonk, NY, USA).
RESULTS
The mean and standard deviation values of the bond strength for each subgroup are presented in Table 1. A statistically significant effect was found for the 2 independent variables, ‘The type of ICM’ (p < 0.001) and ‘The type of plug material’ (p < 0.001), and their interaction (The type of plug material × The type of ICM, p < 0.001) on bond strength, the dependent variable. Regardless of the type of ICM, MTA showed higher bond strength than BA.
Table 1
The push-out bond strength (MPa) of mineral trioxide aggregate (MTA) and BioAggregate (BA) after the prior use of different intracanal medications (ICMs)
The values are presented as means ± standard deviations.
Different lowercase letters indicate that there are statistically significant differences between the groups within the column.
CON, control; CH, calcium hydroxide; CHX, chlorhexidine; TAP, triple-antibiotic paste; DAP, double-antibiotic paste; ANOVA, analysis of variance.
*Indicates statistical significance at p < 0.05 according to the Student's t-test; †Indicates statistical significance at p < 0.05 according to 1-way ANOVA.
A statistically significant interaction of the 2 independent variables indicates that the effect of 1 independent variable on the dependent variable is influenced by the other independent variable. Due to the significant interaction of the 2 independent variables (p < 0.001) in this study, the mean values of bond strength recorded for the different ICMs were separately compared for each plug material. For MTA, there was a significant difference among the different ICMs (p < 0.001, Table 1). Compared to CON, CH had significantly higher bond strength (p < 0.001). CH showed a higher bond strength than TAP and DAP (p < 0.001 for each). CHX showed a higher bond strength than DAP (p = 0.001). For BA, there was also a significant difference among the different ICMs (p = 0.043, Table 1), with only CH showing significantly higher bond strength than DAP. For each ICM separately, MTA showed significantly higher bond strength than BA (p < 0.05) with all the ICMs except for DAP, where there was no significant difference between the 2 plug materials (p = 0.06) in bond strength.
The incidence of the different modes of failure within each subgroup is presented in Table 2. Regardless of the type of the ICM, there was no significant difference in the incidence of the different modes of failure for MTA (adhesive, 36%; mixed, 42%; cohesive, 22%; p = 0.206); for BA (n = 50); however, a significant difference was found in the incidence of the different modes of failure (adhesive, 14%; mixed, 38%; cohesive, 48%; p = 0.010) with the cohesive mode of failure being the most common. Regardless of the type of the plug material, no significant difference was found in the incidence of the different modes of failure for each ICM (CON, p = 0.116; CH, p = 0.157; CHX, p = 0.951; TAP, p = 0.449; DAP, p = 0.951). Representative specimens of each failure mode are shown in Figure 1.
Table 2
Mode of failure distribution of mineral trioxide aggregate (MTA) and BioAggregate (BA) after intracanal medication (ICM)
Figure 1
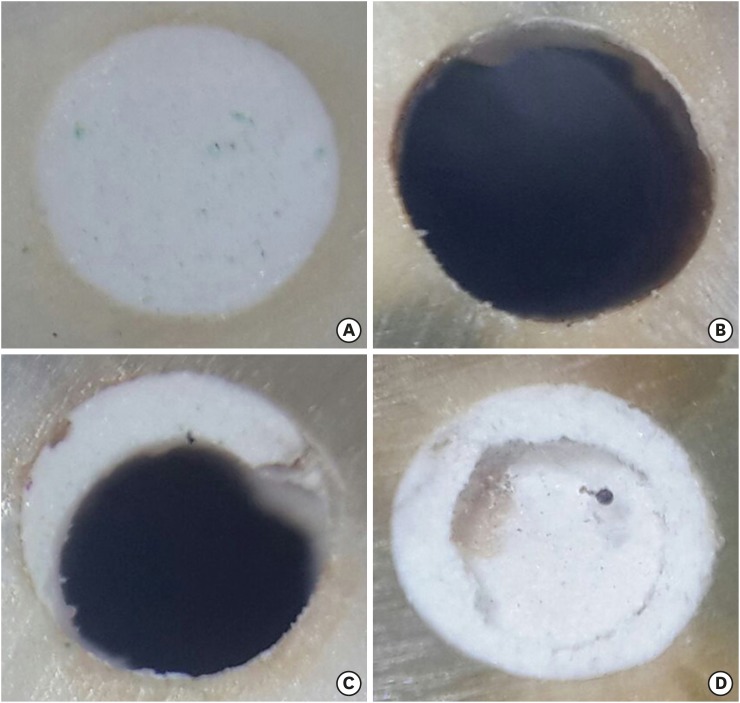
Representative specimens of the different modes of bond failure. (A) A specimen with the material in the root canal before displacement in the push-out test; (B) A specimen showing an adhesive mode of failure; (C) A specimen showing a mixed mode of failure; (D) A specimen showing a cohesive mode of failure.
A discolored material-dentin interface could be observed when TAP was used as an ICM (Figure 2). This was observed in 5 out of 10 specimens in the MTA subgroup and in 4 out of 10 specimens in the BA subgroup; this phenomenon was not observed for the other ICMs.
Figure 2
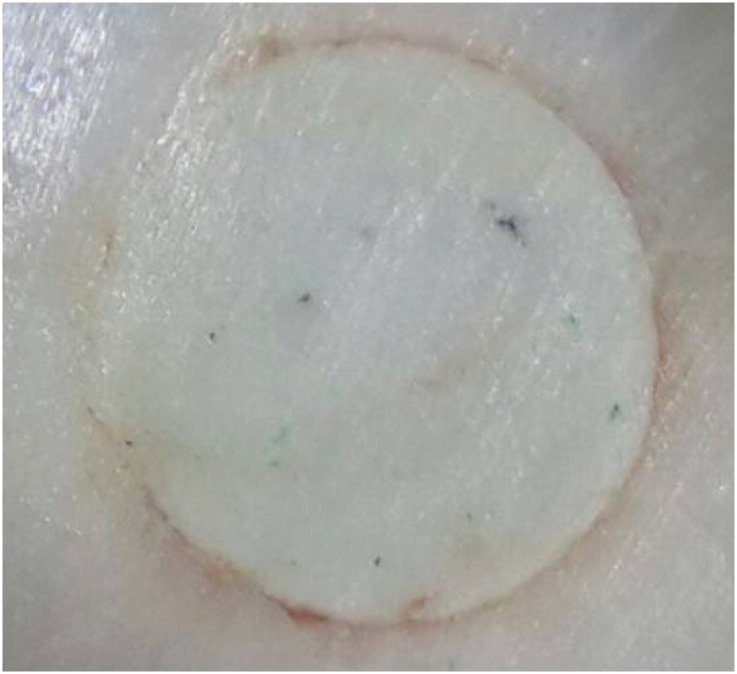
A specimen showing discoloration at the material-dentin interface with triple-antibiotic paste (TAP) as the intracanal medication (ICM).
DISCUSSION
Disinfection is pivotal during REPs, and is mostly done using irrigants and ICMs. A coronal seal is another important step in REPs, and this function is usually provided by CSCs. The retention of the coronal plug is important due to its potential exposure to forces either upon the application of overlying restorative materials or upon mastication. BA is a TCS-based cement [8] that may display better endurance of chemical attacks than MTA [10], particularly upon exposure to the remnants of acidic ICMs used during REPs, such as TAP and DAP. The effect of such residues on the retention of BA, when used as a coronal plug in REPs, has yet to be compared to the corresponding effects on MTA retention.
MTA showed better retention than BA. This finding is in accordance with previous studies [10,21,22,23], whereas it disagrees with another study in which both materials performed similarly [24]. In the latter study, MTA and BA were compared with Endosequence Root Repair Material (ERRM, Brasseler USA, Savannah, GA, USA), which recorded significantly higher bond strength than either material [24]; this could have masked the statistical significance of the difference between them if it existed. The variations in the bond strength among various CSCs can be attributed to differences in their hydration kinetics and, consequently, their mechanical properties.
Hydration kinetics is strongly affected by the additives present in CSCs, which can modify their end products and, consequently, their properties and clinical performance [8]. Most hydration reactions and the maturation of MTA occur within the first week of setting and continue well beyond the clinically-observed setting time. Hydration results in the formation of crystalline CH (portlandite) and calcium silicate hydrate (C-S-H) as its main products. Portlandite crystals are large, and therefore could play a role in the frictional retention of MTA to dentin [10,25,26]. BA differs mineralogically from MTA, as BA contains monobasic calcium phosphate, rendering it a biphasic material [11], and amorphous silicon dioxide [8]. The features of biphasic materials include the lack of formation of portlandite and the amorphous nature of hydroxyapatite (HA) [12]. Hydration of BA results in the initial formation of CH, which disappears as the reaction continues [8]. Two mechanisms can explain the elimination of CH from BA: first, monobasic calcium phosphate reacts rapidly with CH in an acid-base reaction, forming dicalcium phosphate dihydrate (DCPD) and/or HA; such a decrease in CH also causes the equilibrium of hydration of TCS to shift towards forming more C-S-H gel [11]. Second, the amorphous silicon dioxide in BA further reacts with CH, producing additional C-S-H [10,27]. Both C-S-H gel and HA are poorly-crystalline nanometer-level structures [10,12], which could adversely affect the mechanical properties of the material.
The mode of failure of CSCs is usually adhesive [21,23,28]. In the present study, MTA showed a similar incidence of the different modes of failure, whereas, interestingly, the incidence of cohesive failure with 3-day-set BA was more than 3 times that of adhesive failure. This is in agreement, at least partly, with some previous studies [17,21,22,23,29]. In a previous study, cohesive failure was reported to be predominant with ERRM at neutral and acidic pH and with MTA only at neutral pH [29]; ERRM is a biphasic material [12], like BA.
This finding could be explained on the basis of the biphasic nature of BA. The formation of more nanometer-level phases, such as C-S-H and HA, with BA than is expected from MTA can allow their easier penetration within the dentin structure, especially after demineralization with acidic ICM. This can lead to better mechanical interlocking with the dentin structure, causing cohesive failure to be predominant. A previous study has shown earlier bioactivity with BA than with MTA [30].
The mechanical properties of plug materials, such as compressive strength and microhardness, affect the interpretation of their push-out bond strength findings through their correlation with the material's rigidity [31,32,33,34]. Additionally, as most cohesive failures were found within the material with BA, the role of the material's mechanical properties in interpreting its bonding behavior is accentuated. MTA has better mechanical properties than BA [35,36,37]. This has been attributed to several factors. The lack of aluminate in BA causes a lack of ettringite crystals, a main hydration product contributing to the strength of CSCs [36]. The physical properties of CSCs are also affected by their porosity [7,8]. The specific surface area of BA is nearly 9 times that of MTA, which has been attributed to the internal porosity of BA's unhydrated particles; this entails a higher fluid uptake, resulting in the need for more water to obtain an adequate mix [8]. High water-to-powder ratios result in increased material porosity and reduce the material's strength [8,37]. Another contributing factor is the higher availability of calcium-phosphate-cement forms in hydrated biphasic materials such as BA; in contrast, a major disadvantage of calcium phosphate cements is their poor mechanical properties [11].
The retention of MTA was more strongly influenced by the type of the ICM than the retention of BA, which showed relatively stable behavior; this supports the findings of a previous study that reported that the bonding of BA to dentin was more resistant to exposure to acidic pH than MTA in the context of perforation repair [10]. Several studies have shown that the properties of MTA tend to be affected by environmental conditions [10,13,28]. BA, in contrast, seems to show better endurance of environmental conditions, which could be due to its composition [7]. The incorporation of a phosphate compound in the chemical composition of a CSC can protect it against acidic attack on its microstructure and provide it with early strength [38]. Being the weak link in the hydrated CSC structure due to its liability to chemical attack, the lower CH content in BA than in MTA could explain the higher resistance of BA to unfavorable environmental conditions [10,27]. The lower solubility of phosphate compounds (DCPD and HA) formed in biphasic materials such as BA could also explain the possible lower degradation of these materials than MTA [11]. In addition, the predominantly cohesive failure mode detected for BA may also support the finding that the ICMs had a smaller influence on BA by acting at the material-dentin interface to affect its bonding potential.
CH was the only ICM to improve the retention of MTA to dentin compared to the control group; the other tested ICMs performed similarly to the control. CH was associated with better MTA retention than TAP or DAP, while CHX only performed better than DAP. For BA, none of the ICMs differed from the control, and only CH showed better bond strength than DAP. However, variable results have been reported in the endodontic literature on the effects of the ICMs used in REPs on the retention of CSCs [17,18,19,20]. Our findings are in accordance with 1 study [20], partly in agreement with another [17], and in disagreement with others [18,19]. Variations among studies may primarily be due to variations in experimental design, including the CSC types and durations of setting, as well as the ICM form, concentration, and method of removal [39,40] and the differential effects of ICMs on dentin, with which they were usually in contact for 3 weeks, as is the case for REPs.
The distinctive physicochemcial properties of ICMs can significantly affect dentin in different ways. CH has a highly-alkaline pH (pH = 11.8 ± 0.1) compared to the highly-acidic pH of TAP (pH = 2.9 ± 0.1) and DAP (pH = 3.4 ± 0.1) [41]. Detectable TAP could be found deeper in the dentin (up to 350 µm) 28 days after application than was the case for residual CH, which was present at a shallower level [40]. A demineralizing effect has been detected and a collagen-rich matrix has been found to form on the surface of radicular dentin in contact with TAP and DAP [6,41].
The changes in the superficial dentin structure made by irrigants and ICMs can affect the potential of dentin to adhere to root canal filling materials [5]. Antibiotic pastes consistently decrease dentin microhardness, cause dentin erosion, and increase roughness [39,42,43,44,45]. However, the literature contains inconsistent results regarding the effects of CH on dentin properties within 1 month or less [46]. In more recent studies, dentin microhardness increased when EDTA was not used for CH removal [39,42], while it decreased when EDTA was used for 10 minutes [44]. In the present study, EDTA was used for only 1 minute. Altogether, it seems that CH allows CSCs to bond to a relatively ‘harder’ dentin, while antibiotic pastes allow them to bond to a ‘softer’ dentin; this could affect push-out bond strength readings.
Furthermore, the pH of dentin may help explain the effects of CH on the CSC bond. CH increases the pH of dentin [47]; this could improve the mechanical and bonding properties of CSCs [35,48]. CH remnants seem to remain superficial on the dentin surface [40], increasing frictional resistance at the dentin-material interface and thereby improving retention.
Relative variability exists in the effects of DAP compared to TAP on the retention of CSCs. In this study, TAP showed similar bond strength to CHX with both BA and MTA, and less bond strength than CH with MTA only. DAP, however, showed less bond strength than both CH and CHX with MTA and less bond strength than CH with BA. DAP could cause earlier softening of dentin than TAP after 1 week [45] and adversely affect tooth strength after 3 months, unlike TAP [39]. Scanning electron microscopic observations showed areas of collagen exposure with both DAP and TAP, and the native structure of the collagen fibrils was easily recognizable with TAP [41,43].
As both TAP and DAP show a similar potential of removability [49] and DAP has a higher pH than TAP [41], the variations in the effects of the 2 ICMs could be explained by differences in their composition. The addition of a tetracycline derivative to the antibiotic paste, as in TAP, seems to play a role in CSC-dentin bonding. Tetracycline and its semi-synthetic analogues, such as doxycycline and minocycline, are antibiotics with dentin-chelating properties. They inhibit matrix metalloproteinases (MMPs), collagenases, and gelatinases, thereby showing dentin-protective properties [50,51,52]. It can be postulated that tetracycline may keep the collagen framework within dentin uncollapsed under the acidic pH of the antibiotic pastes; this might allow better interlocking between the uncollapsed collagen fibrils and the hydration products of CSCs, which could lead to better bonding and retention.
CHX did not seem to affect the retention of either MTA or BA. In a recent study, CHX showed a lack of demineralizing or solving effect on the mineral or organic content of dentin [6]. Ari et al. [53] showed that 0.2% CHX used as an irrigant was harmless to dentin microhardness and roughness. The effect of CHX on dentin microhardness is less pronounced than that of CH [5].
CONCLUSIONS
Within the limitations of the present study, it can be concluded that MTA shows better retention as a coronal plug than BA, but the BA failure mode is more likely to be cohesive than adhesive. BA retention is less affected than MTA retention by the different types of ICMs used in REPs. CH seems to improve the bond of MTA to dentin as a coronal plug. BA may be considered as an alternative coronal plug material in REPs.
-
Conflict of Interest: No potential conflict of interest relevant to this article was reported.
-
Author Contributions:
Conceptualization: Amin SAW, Gawdat SI.
Data curation: Amin SAW, Gawdat SI.
Formal analysis: Amin SAW, Gawdat SI.
Funding acquisition: Amin SAW, Gawdat SI.
Investigation: Amin SAW, Gawdat SI.
Methodology: Amin SAW, Gawdat SI.
Project administration: Gawdat SI.
Resources: Amin SAW, Gawdat SI.
Software: Amin SAW, Gawdat SI.
Supervision: Amin SAW.
Validation: Amin SAW, Gawdat SI.
Visualization: Amin SAW, Gawdat SI.
Writing - original draft: Amin SAW, Gawdat SI.
Writing - review & editing: Amin SAW, Gawdat SI.
- 1. Galler KM. Clinical procedures for revitalization: current knowledge and considerations. Int Endod J 2016;49:926-936.ArticlePubMed
- 2. Kontakiotis EG, Filippatos CG, Tzanetakis GN, Agrafioti A. Regenerative endodontic therapy: a data analysis of clinical protocols. J Endod 2015;41:146-154.ArticlePubMed
- 3. Kahler B, Rossi-Fedele G. A review of tooth discoloration after regenerative endodontic therapy. J Endod 2016;42:563-569.ArticlePubMed
- 4. Tagelsir A, Yassen GH, Gomez GF, Gregory RL. Effect of antimicrobials used in regenerative endodontic procedures on 3-week-old Enterococcus faecalis biofilm. J Endod 2016;42:258-262.ArticlePubMed
- 5. Prabhakar A, Taur S, Hadakar S, Sugandhan S. Comparison of antibacterial efficacy of calcium hydroxide paste, 2% chlorhexidine gel and turmeric extract as an intracanal medicament and their effect on microhardness of root dentin: an in vitro study. Int J Clin Pediatr Dent 2013;6:171-177.ArticlePubMedPMC
- 6. Abu Zeid ST, Khafagi MG, Abou Neel EA. Effect of root canal medications on maturation and calcification of root canal dentin’ hydroxyapatite. Spectrosc Lett 2016;49:135-139.Article
- 7. Camilleri J, Grech L, Galea K, Keir D, Fenech M, Formosa L, Damidot D, Mallia B. Porosity and root dentine to material interface assessment of calcium silicate-based root-end filling materials. Clin Oral Investig 2014;18:1437-1446.ArticlePubMedPDF
- 8. Camilleri J, Sorrentino F, Damidot D. Characterization of un-hydrated and hydrated BioAggregate and MTA Angelus. Clin Oral Investig 2015;19:689-698.ArticlePubMedPDF
- 9. Zhang H, Pappen FG, Haapasalo M. Dentin enhances the antibacterial effect of mineral trioxide aggregate and bioaggregate. J Endod 2009;35:221-224.ArticlePubMed
- 10. Hashem AA, Wanees Amin SA. The effect of acidity on dislodgment resistance of mineral trioxide aggregate and bioaggregate in furcation perforations: an in vitro comparative study. J Endod 2012;38:245-249.ArticlePubMed
- 11. Huan Z, Chang J. Novel tricalcium silicate/monocalcium phosphate monohydrate composite bone cement. J Biomed Mater Res B Appl Biomater 2007;82:352-359.ArticlePubMed
- 12. Schembri-Wismayer P, Camilleri J. Why biphasic? Assessment of the effect on cell proliferation and expression. J Endod 2017;43:751-759.ArticlePubMed
- 13. Tian J, Zhang Y, Lai Z, Li M, Huang Y, Jiang H, Wei X. Ion release, microstructural, and biological properties of iRoot BP Plus and ProRoot MTA exposed to an acidic environment. J Endod 2017;43:163-168.ArticlePubMed
- 14. Guven Y, Tuna EB, Dincol ME, Ozel E, Yilmaz B, Aktoren O. Long-term fracture resistance of simulated immature teeth filled with various calcium silicate-based materials. Biomed Res Int 2016;2016:2863817.ArticlePubMedPMCPDF
- 15. Keskin C, Demiryurek EO, Ozyurek T. Color stabilities of calcium silicate-based materials in contact with different irrigation solutions. J Endod 2015;41:409-411.ArticlePubMed
- 16. Tuloglu N, Bayrak S. Comparative evaluation of mineral trioxide aggregate and bioaggregate as apical barrier material in traumatized nonvital, immature teeth: a clinical pilot study. Niger J Clin Pract 2016;19:52-57.ArticlePubMed
- 17. Topçuoğlu HS, Arslan H, Akçay M, Saygili G, Çakici F, Topçuoğlu G. The effect of medicaments used in endodontic regeneration technique on the dislocation resistance of mineral trioxide aggregate to root canal dentin. J Endod 2014;40:2041-2044.ArticlePubMed
- 18. Turk T, Fidler A. Effect of medicaments used in endodontic regeneration technique on push-out bond strength of MTA and Biodentine. Biotechnol Biotechnol Equip 2016;30:140-144.Article
- 19. Turk T, Ozisik B, Aydin B. Time-dependent effectiveness of the intracanal medicaments used for pulp revascularization on the dislocation resistance of MTA. BMC Oral Health 2015;15:130-135.ArticlePubMedPMCPDF
- 20. Nagas E, Cehreli ZC, Uyanik MO, Vallittu PK, Lassila LV. Effect of several intracanal medicaments on the push-out bond strength of ProRoot MTA and Biodentine. Int Endod J 2016;49:184-188.PubMed
- 21. Saghiri MA, Garcia-Godoy F, Gutmann JL, Lotfi M, Asatourian A, Ahmadi H. Push-out bond strength of a nano-modified mineral trioxide aggregate. Dent Traumatol 2013;29:323-327.ArticlePubMed
- 22. Saghiri MA, Asatourian A, Garcia-Godoy F, Gutmann JL, Sheibani N. The impact of thermocycling process on the dislodgement force of different endodontic cements. Biomed Res Int 2013;2013:317185.ArticlePubMedPMCPDF
- 23. Majeed A, AlShwaimi E. Push-out bond strength and surface microhardness of calcium silicate-based biomaterials: an in vitro study. Med Princ Pract 2017;26:139-145.ArticlePubMedPDF
- 24. Shokouhinejad N, Razmi H, Nekoofar MH, Sajadi S, Dummer PM, Khoshkhounejad M. Push-out bond strength of bioceramic materials in a synthetic tissue fluid. J Dent (Tehran) 2013;10:540-547.PubMedPMC
- 25. Chedella SC, Berzins DW. A differential scanning calorimetry study of the setting reaction of MTA. Int Endod J 2010;43:509-518.ArticlePubMed
- 26. Amin SA, Seyam RS, El-Samman MA. The effect of prior calcium hydroxide intracanal placement on the bond strength of two calcium silicate-based and an epoxy resin-based endodontic sealer. J Endod 2012;38:696-699.ArticlePubMed
- 27. Grattan-Bellew PE. Microstructural investigation of deteriorated Portland cement concretes. Construct Build Mater 1996;10:3-16.Article
- 28. Shokouhinejad N, Nekoofar MH, Iravani A, Kharrazifard MJ, Dummer PM. Effect of acidic environment on the push-out bond strength of mineral trioxide aggregate. J Endod 2010;36:871-874.ArticlePubMed
- 29. Shokouhinejad N, Yazdi KA, Nekoofar MH, Matmir S, Khoshkhounejad M. Effect of acidic environment on dislocation resistance of Endosequence root repair material and mineral trioxide aggregate. J Dent (Tehran) 2014;11:161-166.PubMedPMC
- 30. Shokouhinejad N, Nekoofar MH, Razmi H, Sajadi S, Davies TE, Saghiri MA, Gorjestani H, Dummer PM. Bioactivity of EndoSequence root repair material and bioaggregate. Int Endod J 2012;45:1127-1134.ArticlePubMed
- 31. Sideris K, Manita P. Estimation of ultimate modulus of elasticity and Poisson ratio of normal concrete. Cement Concr Compos 2004;26:623-631.Article
- 32. Twati WA, Wood DJ, Liskiewicz TW, Willmott NS, Duggal MS. An evaluation of the effect of non-setting calcium hydroxide on human dentine: a pilot study. Eur Arch Paediatr Dent 2009;10:104-109.ArticlePubMedPDF
- 33. Chen WP, Chen YY, Huang SH, Lin CP. Limitations of push-out test in bond strength measurement. J Endod 2013;39:283-287.ArticlePubMed
- 34. Pane ES, Palamara JE, Messer HH. Critical evaluation of the push-out test for root canal filling materials. J Endod 2013;39:669-673.ArticlePubMed
- 35. Saghiri MA, Garcia-Godoy F, Asatourian A, Lotfi M, Banava S, Khezri-Boukani K. Effect of pH on compressive strength of some modification of mineral trioxide aggregate. Med Oral Patol Oral Cir Bucal 2013;18:e714-e720.ArticlePubMedPMC
- 36. Bolhari B, Nekoofar MH, Sharifian M, Ghabrai S, Meraji N, Dummer PM. Acid and microhardness of mineral trioxide aggregate and mineral trioxide aggregate-like materials. J Endod 2014;40:432-435.ArticlePubMed
- 37. Jang YE, Lee BN, Koh JT, Park YJ, Joo NE, Chang HS, Hwang IN, Oh WM, Hwang YC. Cytotoxicity and physical properties of tricalcium silicate-based endodontic materials. Restor Dent Endod 2014;39:89-94.ArticlePubMedPMC
- 38. Shie MY, Huang TH, Kao CT, Huang CH, Ding SJ. The effect of a physiologic solution pH on properties of white mineral trioxide aggregate. J Endod 2009;35:98-101.ArticlePubMed
- 39. Yassen GH, Vail MM, Chu TG, Platt JA. The effect of medicaments used in endodontic regeneration on root fracture and microhardness of radicular dentine. Int Endod J 2013;46:688-695.ArticlePubMed
- 40. Berkhoff JA, Chen PB, Teixeira FB, Diogenes A. Evaluation of triple antibiotic paste removal by different irrigation procedures. J Endod 2014;40:1172-1177.ArticlePubMed
- 41. Yassen GH, Chu TM, Eckert G, Platt JA. Effect of medicaments used in endodontic regeneration technique on the chemical structure of human immature radicular dentin: an in vitro study. J Endod 2013;39:269-273.ArticlePubMed
- 42. Yassen GH, Chu TM, Gallant MA, Allen MR, Vail MM, Murray PE, Platt JA. A novel approach to evaluate the effect of medicaments used in endodontic regeneration on root canal surface indentation. Clin Oral Investig 2014;18:1569-1575.ArticlePubMedPDF
- 43. Prather BT, Ehrlich Y, Spolnik K, Platt JA, Yassen GH. Effects of two combinations of triple antibiotic paste used in endodontic regeneration on root microhardness and chemical structure of radicular dentine. J Oral Sci 2014;56:245-251.ArticlePubMed
- 44. Yassen GH, Eckert GJ, Platt JA. Effect of intracanal medicaments used in endodontic regeneration procedures on microhardness and chemical structure of dentin. Restor Dent Endod 2015;40:104-112.ArticlePubMed
- 45. Yilmaz S, Dumani A, Yoldas O. The effect of antibiotic pastes on microhardness of dentin. Dent Traumatol 2016;32:27-31.ArticlePubMed
- 46. Yassen GH, Platt JA. The effect of nonsetting calcium hydroxide on root fracture and mechanical properties of radicular dentine: a systematic review. Int Endod J 2013;46:112-118.ArticlePubMed
- 47. Shetty S, Manjunath MK, Tejaswi S. An in-vitro evaluation of the pH change through root dentin using different calcium hydroxide preparations as an intracanal medicament. J Clin Diagn Res 2014;8:ZC13-ZC16.Article
- 48. Saghiri MA, Shokouhinejad N, Lotfi M, Aminsobhani M, Saghiri AM. Push-out bond strength of mineral trioxide aggregate in the presence of alkaline pH. J Endod 2010;36:1856-1859.ArticlePubMed
- 49. Arslan H, Akcay M, Capar ID, Ertas H, Ok E, Uysal B. Efficacy of needle irrigation, EndoActivator, and photon-initiated photoacoustic streaming technique on removal of double and triple antibiotic pastes. J Endod 2014;40:1439-1442.ArticlePubMed
- 50. Mohammadi Z, Abbott PV. On the local applications of antibiotics and antibiotic-based agents in endodontics and dental traumatology. Int Endod J 2009;42:555-567.ArticlePubMed
- 51. Tjäderhane L, Nascimento FD, Breschi L, Mazzoni A, Tersariol IL, Geraldeli S, Tezvergil-Mutluay A, Carrilho M, Carvalho RM, Tay FR, Pashley DH. Strategies to prevent hydrolytic degradation of the hybrid layer: a review. Dent Mater 2013;29:999-1011.ArticlePubMedPMC
- 52. Sabatini C, Pashley DH. Mechanisms regulating the degradation of dentin matrices by endogenous dentin proteases and their role in dental adhesion. A review. Am J Dent 2014;27:203-214.PubMedPMC
- 53. Ari H, Erdemir A, Belli S. Evaluation of the effect of endodontic irrigation solutions on the microhardness and the roughness of root canal dentin. J Endod 2004;30:792-795.ArticlePubMed
REFERENCES
Tables & Figures
REFERENCES
Citations
Citations to this article as recorded by 
- An in vitro comparative evaluation of the effect of three intracanal medicaments – chlorhexidine gel, triple antibiotic paste, and calcium hydroxide paste on the push-out bond strength of MTA Plus, Biodentine, and calcium-enriched mixture
Gouthami Datta, Ramya Raghu, Ashish Shetty, Gautham P Manjunath, Dishant Patel, Subhashini Rajasekhara
Endodontology.2023; 35(1): 60. CrossRef - Effects of calcium hydroxide intracanal medicament on push‐out bond strength of endodontic sealers: A systematic review and meta‐analysis
Mohammed Nasser Alhajj, Fadhilah Daud, Sadeq Ali Al‐Maweri, Yanti Johari, Zuryati Ab‐Ghani, Mariatti Jaafar, Yoshihito Naito, Widyasri Prananingrum, Zaihan Ariffin
Journal of Esthetic and Restorative Dentistry.2022; 34(8): 1166. CrossRef - A Breakthrough in the Era of Calcium Silicate-Based Cements: A Critical Review
Payal S Chaudhari, Manoj G Chandak, Akshay A Jaiswal, Nikhil P Mankar, Priyanka Paul
Cureus.2022;[Epub] CrossRef - Modern Medicaments for Endodontic Treatment in Children
Н.В. Шаковец, О.С. Романова
Стоматология. Эстетика. Инновации.2021; (4): 408. CrossRef - Do intracanal medications used in regenerative endodontics affect the bond strength of powder-to-liquid and ready-to-use cervical sealing materials?
MarinaCarvalho Prado, Kevillin Martiniano, AndreaCardoso Pereira, KarineL Cortellazzi, MarinaA Marciano, Gabriel Abuna, Adriana de-Jesus-Soares
Journal of Conservative Dentistry.2021; 24(5): 464. CrossRef - In vivo Biocompatibility and Bioactivity of Calcium Silicate-Based Bioceramics in Endodontics
Wencheng Song, Wei Sun, Lili Chen, Zhenglin Yuan
Frontiers in Bioengineering and Biotechnology.2020;[Epub] CrossRef - Effect of Hydrogel-Based Antibiotic Intracanal Medicaments on Push-Out Bond Strength
Rayan B. Yaghmoor, Jeffrey A. Platt, Kenneth J. Spolnik, Tien Min Gabriel Chu, Ghaeth H. Yassen
European Journal of Dentistry.2020; 14(04): 575. CrossRef - Regenerative Endodontic Procedures, Disinfectants and Outcomes: A Systematic Review
Adam S. Kharchi, Nara Tagiyeva-Milne, Shalini Kanagasingam
Primary Dental Journal.2020; 9(4): 65. CrossRef
 ePub Link
ePub Link Cite
CiteRetention of BioAggregate and MTA as coronal plugs after intracanal medication for regenerative endodontic procedures: an ex vivo study

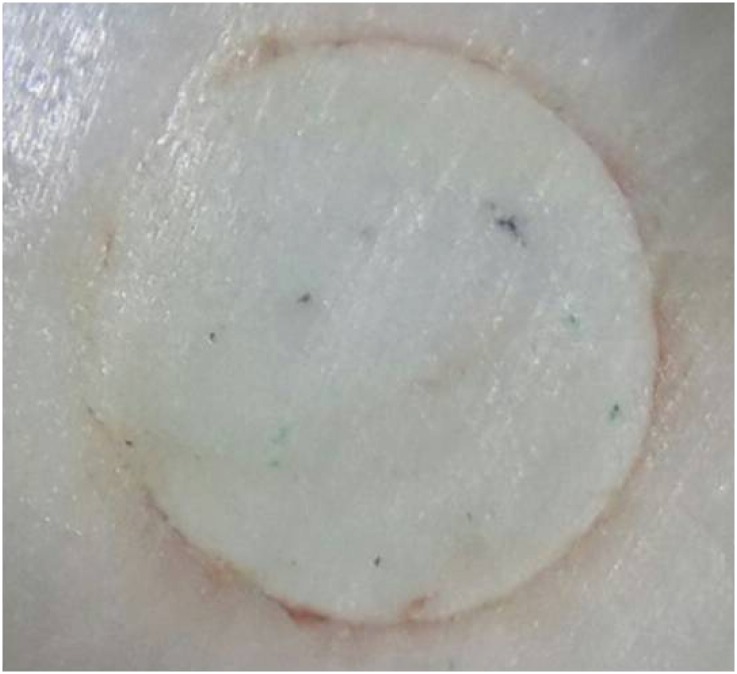
Figure 1 Representative specimens of the different modes of bond failure. (A) A specimen with the material in the root canal before displacement in the push-out test; (B) A specimen showing an adhesive mode of failure; (C) A specimen showing a mixed mode of failure; (D) A specimen showing a cohesive mode of failure.
Figure 2 A specimen showing discoloration at the material-dentin interface with triple-antibiotic paste (TAP) as the intracanal medication (ICM).
Figure 1
Figure 2
Retention of BioAggregate and MTA as coronal plugs after intracanal medication for regenerative endodontic procedures: an ex vivo study
The push-out bond strength (MPa) of mineral trioxide aggregate (MTA) and BioAggregate (BA) after the prior use of different intracanal medications (ICMs)
| ICM | Material | ||
|---|---|---|---|
| MTA | BA | p value | |
| CON | 1.300 ± 0.529b,c | 0.698 ± 0.184a,b | 0.003* |
| CH | 3.592 ± 1.387a | 1.109 ± 0.810a | < 0.001* |
| CHX | 2.406 ± 0.600a,b | 0.953 ± 0.696a,b | < 0.001* |
| TAP | 1.641 ± 1.044b,c | 0.599 ± 0.282a,b | 0.007* |
| DAP | 0.533 ± 0.196c | 0.357 ± 0.191b | 0.060 |
| p value | < 0.001† | 0.043† | |
The values are presented as means ± standard deviations.
Different lowercase letters indicate that there are statistically significant differences between the groups within the column.
CON, control; CH, calcium hydroxide; CHX, chlorhexidine; TAP, triple-antibiotic paste; DAP, double-antibiotic paste; ANOVA, analysis of variance.
*Indicates statistical significance at p < 0.05 according to the Student's t-test; †Indicates statistical significance at p < 0.05 according to 1-way ANOVA.
Mode of failure distribution of mineral trioxide aggregate (MTA) and BioAggregate (BA) after intracanal medication (ICM)
| ICM | Material | ||||||||
|---|---|---|---|---|---|---|---|---|---|
| MTA | BA | Total/ICM (n = 20) | |||||||
| A | M | C | A | M | C | A | M | C | |
| CON | 3 | 6 | 1 | 2 | 5 | 3 | 5/20 | 11/20 | 4/20 |
| CH | 3 | 4 | 4 | 0 | 3 | 6 | 3/20 | 7/20 | 10/20 |
| CHX | 5 | 4 | 2 | 2 | 3 | 4 | 7/20 | 7/20 | 6/20 |
| TAP | 3 | 4 | 2 | 1 | 4 | 6 | 4/20 | 8/20 | 8/20 |
| DAP | 4 | 3 | 2 | 2 | 4 | 5 | 6/20 | 7/20 | 7/20 |
| Total/material (n = 50) | 18/50 | 21/50 | 11/50 | 7/50 | 19/50 | 24/50 | |||
The values represent the counts of specimens with each mode of failure.
A, adhesive; M, mixed; C, cohesive; CON, control; CH, calcium hydroxide; CHX, chlorhexidine; TAP, triple-antibiotic paste; DAP, double-antibiotic paste.
Table 1 The push-out bond strength (MPa) of mineral trioxide aggregate (MTA) and BioAggregate (BA) after the prior use of different intracanal medications (ICMs)
The values are presented as means ± standard deviations.
Different lowercase letters indicate that there are statistically significant differences between the groups within the column.
CON, control; CH, calcium hydroxide; CHX, chlorhexidine; TAP, triple-antibiotic paste; DAP, double-antibiotic paste; ANOVA, analysis of variance.
*Indicates statistical significance at
Table 2 Mode of failure distribution of mineral trioxide aggregate (MTA) and BioAggregate (BA) after intracanal medication (ICM)
The values represent the counts of specimens with each mode of failure.
A, adhesive; M, mixed; C, cohesive; CON, control; CH, calcium hydroxide; CHX, chlorhexidine; TAP, triple-antibiotic paste; DAP, double-antibiotic paste.

