
Articles
- Page Path
- HOME > Restor Dent Endod > Volume 41(3); 2016 > Article
- Case Report A combined approach to non-carious cervical lesions associated with gingival recession
- SungEun Yang1, HyeJin Lee1, Sung-Ho Jin2
-
2016;41(3):-224.
DOI: https://doi.org/10.5395/rde.2016.41.3.218
Published online: May 2, 2016
1Department of Conservative Dentistry, Seoul St. Mary's Dental Hospital, College of Medicine, The Catholic University of Korea, Seoul, Korea.
2Department of Periodontology, Seoul St. Mary's Dental Hospital, College of Medicine, The Catholic University of Korea, Seoul, Korea.
- Correspondence to SungEun Yang, DDS, MSD, PhD. Associate Professor, Department of Conservative Dentistry, Seoul St. Mary's Hospital, College of Medicine, The Catholic University of Korea, 222, Banpo-daero, Seochogu, Seoul, Korea 06591. TEL: +82-2-2258-6296, FAX: +82-2-537-2374, dentyeun@catholic.ac.kr
• Received: January 12, 2016 • Accepted: March 17, 2016
©Copyrights 2016. The Korean Academy of Conservative Dentistry.
This is an Open Access article distributed under the terms of the Creative Commons Attribution Non-Commercial License (http://creativecommons.org/licenses/by-nc/3.0/) which permits unrestricted non-commercial use, distribution, and reproduction in any medium, provided the original work is properly cited.
- 4,926 Views
- 108 Download
- 6 Crossref
Abstract
- Non-carious cervical lesions (NCCLs) with gingival recession require specific consideration on both aspects of hard and soft tissue lesion. In the restorative aspect, careful finishing and polishing of the restorations prior to mucogingival surgery is the critical factor contributing to success. Regarding surgery, assessment of the configuration of the lesion and the choice of surgical technique are important factors. The precise diagnosis and the choice of the proper treatment procedure should be made on the basis of both restorative and surgical considerations to ensure the successful treatment of NCCLs.
Introduction
A non-carious cervical lesion (NCCL) is described as the loss of hard tissue at the cemento-enamel junction (CEJ) in the absence of caries.1 These lesions can lead to tooth hypersensitivity, plaque deposition, and further gingival irritation.2 Frequently, they are associated with gingival recession, causing structural weaknesses reflected in a poor crown-root ratio and esthetic complaints. Unfortunately, the restoration of the cervical area using a resin composite or glass ionomer (GI) has shown a high failure rate due to the difficulty of isolating the area subject to restoration from the gingival tissue and the poor adhesion of these substances to sclerotic dentin and root surfaces.3
Since NCCLs often involve the simultaneous loss of tooth structure and gingival recession, the diagnostic assessment and approach should be based on a thorough understanding of the periodontal and restorative aspects of treatment. Therefore, esthetic and long-term structural success can be obtained through a multidisciplinary approach of this type. As treatment strategies may vary according to the type of gingival recession, the marginal level, and the extent of the NCCL, the clinical features of each defect site must be considered before treatment.
Zucchelli et al. classified NCCLs and introduced guidelines for the clinical decision-making process.4 If the lesion only occurs on the root surface (NCCL types I and II), a periodontal surgical approach may be sufficient for covering it. In contrast, NCCLs above the CEJ (NCCL type V) can only be restored properly with a resin composite or a GI filling. Crown-radicular NCCLs associated with gingival recession (NCCL types III and IV) are the most challenging, and the treatment of these lesions requires more delicate care. The restorative procedure on the crown part of the lesion should be performed first before mucogingival surgery and surgical gingival recovery should be applied on radicular part of the lesion.
The choice of restorative material is also important for long-term clinical success. The material should have mechanical properties suitable for retention, appropriate esthetic properties, and be biocompatible in order to ensure gingival reattachment. GI or resin-modified GI can be recommended for NCCLs due to the high retention rates of these materials and their favorable biocompatibility for gingival reattachment.5,6 However, those materials have the disadvantage of poor esthetic properties. Therefore, several studies have suggested the alternative use of microfilled resin composites and resin composites, with no significant differences observed in the gingival reattachment level between resin-modified GI and flowable resin composite.7,8,9 The purpose of the present study was to report an esthetically favorable and clinically predictable technique of treating NCCLs with concomitant severe gingival recession.
Case Report
A 43 year old female in good general medical condition complained of old resin restorations that had fallen out and increasing teeth sensitivity. She had a dental history of orthodontic treatment and extraction of all of her second premolars. The maxillary right first molar, first premolar, canine, central incisor, left central incisor, lateral incisor, and canine showed NCCLs, and multiple gingival recessions were present simultaneously. These teeth had been previously restored with resin composite on the cervical lesions, but most of those restorations had fallen out (Figure 1). For the diagnosis and treatment planning, full-mouth radiographs, a periodontal examination, and the fabrication of study casts were performed, and a full-mouth photograph was taken. The treatment procedures focused on the rehabilitation of the structural integrity of the teeth, esthetic improvement through the correction of hard and soft tissue defects, and ultimately, the patient's satisfaction.
In this case, the cervical lesions were characterized by abrasion extending beyond the CEJ. The severity of gingival recession corresponded to Miller Class I, with no loss of interproximal periodontal attachment and bone level.10 In order to recover the original cervical configuration, maximum root coverage (MRC) was simulated on the study models.11
Before starting the treatment, the patient underwent professional prophylaxis with oral hygiene instructions and was encouraged to avoid any further trauma of the gingival tissues and to ensure optimal plaque control. The restorative and surgical procedures were separately performed by two clinicians of the Departments of Conservative Dentistry and Periodontology. This case report was approved by the Institutional Review Board of Seoul St. Mary's Hospital, the Catholic University of Korea (KC 16ZISE0136).
The restorative procedures in the maxillary arch were carried out over the course of two separate visits. Under local anesthesia, a gingival cord was inserted to isolate the field of restoration. The MRC of each lesion was marked with an oil-based pen. The radicular part contained within the MRC was not prepared and the superficial dentin of the coronal part above the MRC was removed gently with diamond burs set at high speed under abundant cooling. Mild enameloplasty and cervical finishing line formation were also performed in order to minimize over-contouring of the restoration, which may lead to plaque entrapment, tissue inflammation, and tissue contraction during the early healing phase. After the cavity was prepared, adhesive procedures were performed (Figures 2 and 3). After selective enamel etching (Figures 2b and 3a), a two-step self-etch adhesive system (Clearfil SE Bond, Kuraray Medical Inc., Kurashiki, Japan) was used according to the manufacturer's instructions (Figure 3b). A micro-hybrid resin composite (Filtek Z-250, 3M ESPE, St. Paul, MN, USA) was used as the filling material. The composite was progressively layered with straight and curved composite applicators (Satin Steel XTS Composite Instrument TNCIGFT #3 and 4, Hu-Friedy, Chicago, IL, USA) and microbrushes were also used to increase the adaptation of these composite increments. The cervical line of the final restoration was located approximately 1 mm apical to the MRC because the original CEJ is usually located 1 - 2 mm apical to the gingival margin (Figures 2c and 3c).12 This allows a smoother emergence profile and can prevent the exposure of the root surface, which may contribute to the persistence of hypersensitivity.9 All of the over-contoured areas were removed using diamond fine and extra-fine burs to prevent plaque accumulation.13 For gingival reattachment on the restored surface, the surface of resin composite should be made of a stable, smooth, and convex substrate. Therefore, the finest finishing and polishing procedures must completed before mucogingival therapy.14 The polishing procedures were implemented twice in order to ensure the smoothest possible surface: immediately and after a week.
After the use of a fine silicon point (Venus Supra, Hanau, Germany), a series of Sof-lex Discs (3M ESPE) were used to improve the esthetic quality of the restoration and to achieve the highest level of smoothness possible (Figures 2d and 3d). Finally, Biscover LV (Bisco Inc., Schaumburg, IL, USA) was applied after the acid etching to seal the composite restorations.
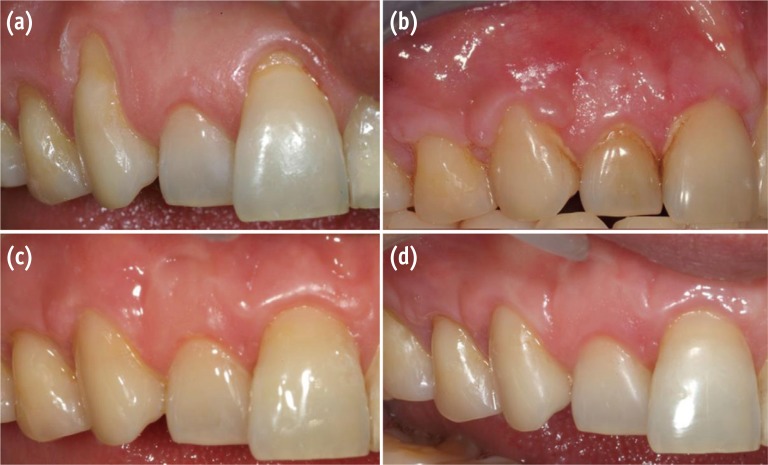
The surgical procedure was carried out after the resin composite filling by a periodontist. The maxillary left side was treated using the envelope technique, employing a coronally advanced flap without any vertical releasing incisions. This surgical technique enables the simultaneous treatment of multiple adjacent recessions (Figures 4a and 4b).15 Beveled oblique incisions in the interproximal areas were outlined under local anesthesia and a split-thickness flap was raised to the base of the papillae, followed by a full-thickness elevation. The flap was then released above the mucogingival junction by a split-thickness elevation again. Root surface preparation was also performed using hand and ultrasonic instrumentation. The residual interproximal papillae were carefully de-epithelized to provide a good recipient bed for flap attachment (Figure 4c). In order to allow tension-free stabilization of the flap, a double horizontal mattress suture was performed buccally across the entire flap extension with a sling suture (Figure 4d). In the maxillary right side, a modification of the coronally advanced flap was used. Since the right lateral incisor showed a normal gingival level, two independent coronally advanced flaps were performed separately on both sides of the right lateral incisor (Figure 5). Postoperative management included an anti-inflammatory medication and 0.2% chlorhexidine mouthwash twice a day until the sutures were removed and brushing could be resumed. The sutures were removed approximately 10 days later. The patient was seen for follow-up four weeks, eight weeks, and six months later (Figures 6 and 7). Complete coverage of the recession defects was achieved, and the patient complained of no hypersensitivity. At the six month follow-up, excellent esthetic results were observed, with the physiological integration of the restorative material and the new gingival architecture (Figure 8).
Discussion
The treatment of NCCLs that include a radicular area, especially if accompanied by gingival recession, is challenging for clinicians. Parameters for predicting the possible amount of gingival recovery are needed before embarking on the treatment of gingival recession. Zucchelli et al. have proposed a prognostic method based on the calculation of the ideal height of the anatomic interdental papilla.16,17
Gingival attachment on the restored surface can be questioned in a combined treatment strategy involving a restorative procedure on the coronal portion of the MRC followed by surgical coverage on the apical portion of the lesion. Some studies have shown that the presence of a restoration did not interfere with root coverage by flap surgery,9 and moreover, creeping attachment on the resin-restored surface was observed, which reflected gingival migration in the coronal direction.18 Favorable periodontal tissue responses can be observed, resulting from careful finishing and polishing of the restorations prior to flap closure and care taken with bacterial plaque control throughout the treatment procedure.19,20
Although not many studies have evaluated long-term data pertaining to the combined approach described in this report, firm gingival re-attachment on the composite and the exposed root surface was observed in the present case. Although the gingival margin had not healed completely and mild gingivitis was observed in the early stage of recovery, three weeks after the surgical procedure, no abnormal periodontal pockets, redness, or bleeding on probing was observed, and the patient was satisfied with the treatment results.
The right and left surgical flap designs were different. On the right side, the flap had vertical incisions, while on the other side, only horizontal incisions were perform. Additional vertical incisions may impede blood supply to the flap and often result in scars or keloid tissue. Some clinical and esthetic advantages have been reported in cases of flap opening without any vertical incisions.15,21 In contrast, when vertical incisions are performed, the tissue tension may be decreased and relapse or recurrence of gingival recession is less likely to occur.21,22,23 Therefore, a vertical releasing incision may be helpful in flap design for the purpose of preventing recurrence of the gingival recession and minimizing the exposure of the unrestored root surface, thereby eventually improving the esthetic appearance.
Conclusions
NCCLs combined with simultaneous gingival recession require particular consideration on both aspects of hard and soft tissue lesion. In the restorative aspect, careful finishing and polishing of the restorations prior to mucogingival surgery is a critical factor contributing to success. Regarding surgery, assessment of the configuration of the lesion and the choice of a surgical technique are important factors. The precise diagnosis and the choice of the proper treatment procedure should be made on the basis of both restorative and surgical considerations to ensure the successful treatment of NCCLs.
Acknowledgement
This report was supported by the Research Fund of Seoul St. Mary's Hospital, The Catholic University of Korea.
- 1. Mair LH. Wear in dentistry – current terminology. J Dent 1992;20:140-144.ArticlePubMed
- 2. Aw TC, Lepe X, Johnson GH, Mancl L. Characteristics of noncarious cervical lesions: a clinical investigation. J Am Dent Assoc 2002;133:725-733.PubMed
- 3. Tyas MJ. Clinical performance of three dentine bonding agents in Class V abrasion lesions without enamel etching. Aust Dent J 1988;33:177-180.ArticlePubMed
- 4. Zucchelli G, Gori G, Mele M, Stefanini M, Mazzotti C, Marzadori M, Montebugnoli L, De Sanctis M. Non-carious cervical lesions associated with gingival recessions: a decision-making process. J Periodontol 2011;82:1713-1724.ArticlePubMed
- 5. Jonck LM, Grobbelaar CJ, Strating H. The biocompatibility of glass-ionomer cement in joint replacement: bulk testing. Clin Mater 1989;4:85-107.Article
- 6. Vandewalle KS, Vigil G. Guidelines for the restoration of Class V lesions. Gen Dent 1997;45:254-260.PubMed
- 7. Deliberador TM, Martins TM, Furlaneto FA, Klingenfuss M, Bosco AF. Use of connective tissue graft for the coverage of composite resin-restored root surfaces in maxillary central incisors. Quintessence Int 2012;43:597-602.PubMed
- 8. Lucchesi JA, Santos VR, Amaral CM, Peruzzo DC, Duarte PM. Coronally positioned flap for treatment of restored root surfaces: a 6-month clinical evaluation. J Periodontol 2007;78:615-623.ArticlePubMed
- 9. Santamaria MP, Ambrosano GM, Casati MZ, Nociti FH Jr, Sallum AW, Sallum EA. Connective tissue graft and resin glass ionomer for the treatment of gingival recession associated with noncarious cervical lesions: a case series. Int J Periodontics Restorative Dent 2011;31:e57-e63.PubMed
- 10. Miller PD Jr. A classification of marginal tissue recession. Int J Periodontics Restorative Dent 1985;5:8-13.
- 11. Zucchelli G, Mele M, Stefanini M, Mazzotti C, Mounssif l, Marzadori M, Montebugnoli L. Predetermination of root coverage. J Periodontol 2010;81:1019-1026.ArticlePubMed
- 12. Wennstrom JL. Mucogingival surgery. In: Lang NP, Karring T, editors. Proceedings of the 1st European Workshop on Periodontology. Berlin: Quintessence Publishing Co. Inc.; 1994. p. 193-209.
- 13. Camargo PM, Lagos RA, Lekovic V, Wolinsky LE. Soft tissue root coverage as treatment for cervical abrasion and caries. Gen Dent 2001;49:299-304.PubMed
- 14. Schätzle M, Land NP, Anerud A, Boysen H, Bürgin W, Löe H. The influence of margins of restorations of the periodontal tissues over 26 years. J Clin Periodontol 2001;28:57-64.ArticlePubMed
- 15. Zucchelli G, De Sanctis M. Treatment of multiple recession-type defects in patients with esthetic demands. J Periodontol 2000;71:1506-1514.ArticlePubMed
- 16. Zucchelli G, Testori T, De Sanctis M. Clinical and anatomical factors limiting treatment outcomes of gingival recession: a new method to predetermine the line of root coverage. J Periodontol 2006;77:714-721.ArticlePubMed
- 17. Bignozzi I, Littarru C, Crea A, Vittorini Orgeas G, Landi L. Surgical treatment options for grafting areas of gingival recession association with cervical lesions: a review. J Esthet Restor Dent 2013;25:371-382.ArticlePubMedPDF
- 18. Alkan A, Keskiner I, Yuzbasioglu E. Connective tissue grafting on resin ionomer in localized gingival recession. J Periodontol 2006;77:1446-1451.ArticlePubMed
- 19. Martins TM, Bosco AF, Nóbrega FJ, Nagata MJ, Garcia VG, Fucini SE. Periodontal tissue response to coverage of root cavities restored with resin materials: a histomorphometric study in dogs. J Periodontol 2007;78:1075-1082.ArticlePubMed
- 20. Gomes SC, Miranda LA, Soares I, Oppermann RV. Clinical and histologic evaluation of the periodontal response to restorative procedures in the dog. Int J Periodontics Restorative Dent 2005;25:39-47.PubMed
- 21. Bruno JF. Connective tissue graft technique assuring wide root coverage. Int J Periodontics Restorative Dent 1994;14:126-137.PubMed
- 22. Harris RJ. Connective tissue grafts combined with either double pedicle grafts or coronally positioned pedicle grafts: results of 266 consecutively treated defects in 200 patients. Int J Periodontics Restorative Dent 2002;22:463-471.PubMed
- 23. Langer B, Langer L. Subepithelial connective tissue graft technique for root coverage. J Periodontol 1985;56:715-720.ArticlePubMed
REFERENCES
Figure 1

Preoperative frontal view. Note the presence of a non-carious cervical lesion on the maxillary left central incisor, the lateral incisor, and the canines on both sides. Old resin restorations on right first premolar and central incisor showed ill-fitting margins and poor color matching.
Figure 2
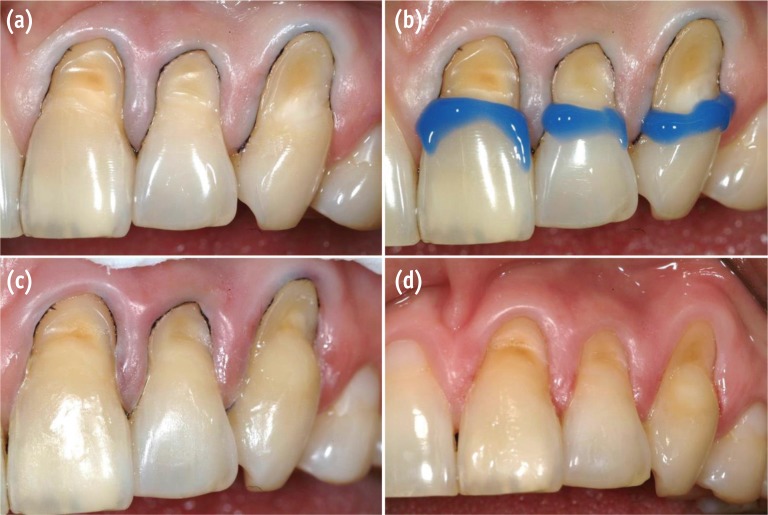
Restorative procedures on the maxillary left side. (a) Field isolation and cavity preparation; (b) Phosphoric acid-selective enamel etching; (c) Adhesive system application and incremental resin filling; (d) Photograph after finishing and polishing.
Figure 3
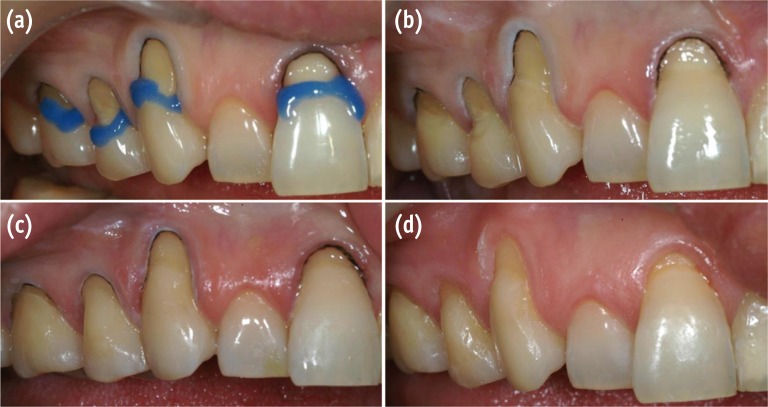
Restorative procedures on the maxillary right side. (a) Phosphoric acid-selective enamel etching after removal of the old restoration and cavity preparation; (b) Adhesive system application; (c) Incremental resin filling; (d) Photograph after finishing and polishing.
Figure 4
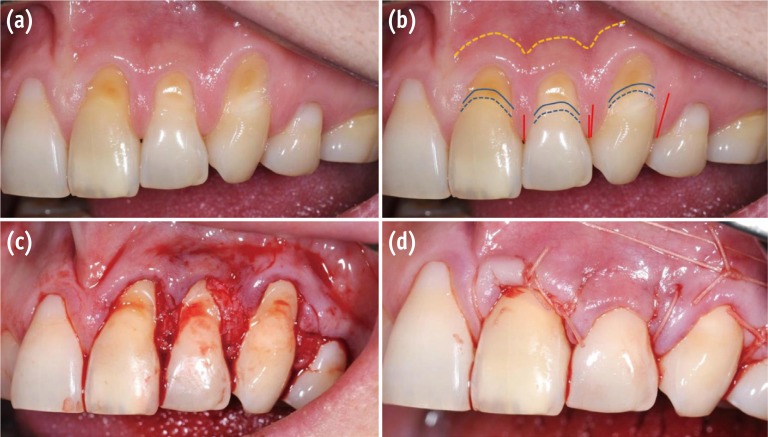
Surgical procedures on the maxillary left side. (a) Multiple adjacent NCCLs; (b) Schematic illustration of the surgery plan; (c) Flap reflection view; (d) Postoperative view after suturing. NCCL, non-carious cervical lesion.
Figure 5
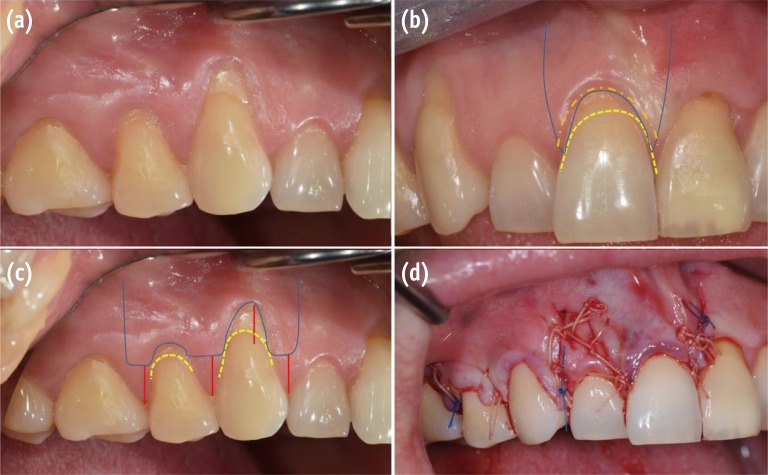
Surgical procedures on the maxillary right side. (a) Multiple adjacent NCCLs; (b and c) Schematic illustration of the surgery plan; (d) Postoperative view after suturing. NCCL, non-carious cervical lesion.
Figure 6
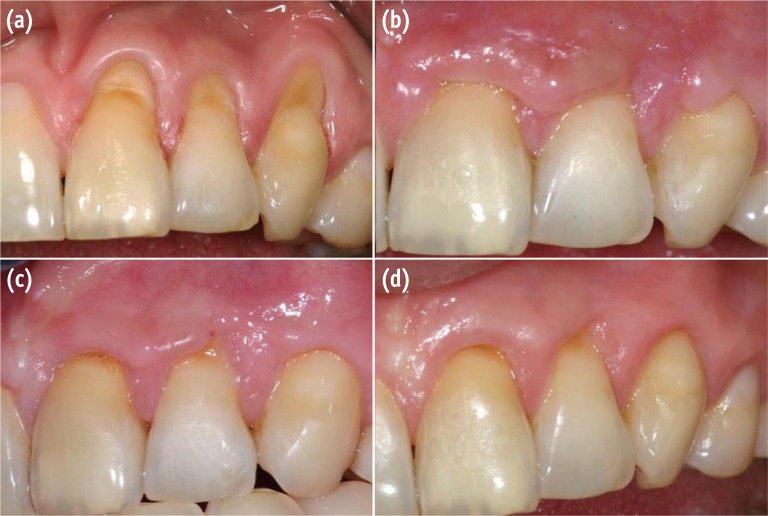
Postoperative view of the maxillary left side. (a) Preoperative view; (b) Four week follow-up; (c) Eight week follow-up; (d) Six month follow-up.

Tables & Figures
REFERENCES
Citations
Citations to this article as recorded by 
- Factors affecting clinical decision-making for the management of non-carious cervical lesions - a qualitative analysis
Wai Ling TSE, Johnson Chun Ming LEE, Tong Wah LIM, Michael George BOTELHO
Journal of Dentistry.2026; 164: 106225. CrossRef - Effect of different material protocols on the control of dentin hypersensitivity: a split-mouth randomized controlled clinical trial
Júlia Marques Martins, Maria Fernanda Ferreira Nogueira, Guilherme José Pimentel Lopes de Oliveira, Alexandre Coelho Machado, Paulo César de Freitas Santos Filho, Hugo Lemes Carlo, Carlos José Soares, Gisele Rodrigues da Silva
Clinical Oral Investigations.2026;[Epub] CrossRef - The link between Noncarious Cervical Lesions (NCCL) and gingival recession. Etiology and treatment. A narrative review.
Luminița Lazăr, Zsigmond-Loránd Makkai, Timea Dakó, Mircea Suciu, Ana-Petra Lazăr
Acta Stomatologica Marisiensis Journal.2023; 6(1): 5. CrossRef - Treatment efficacy of gingival recession defects associated with non-carious cervical lesions: a systematic review
Lívia Maria Lopes de Oliveira, Camila Agra Souza, Sinara Cunha, Rafael Siqueira, Bruna de Carvalho Farias Vajgel, Renata Cimões
Journal of Periodontal & Implant Science.2022; 52(2): 91. CrossRef - Clinical Behavior of the Gingival Margin following Conservative “Coronally Dynamic” Restorations in the Presence of Non-Carious Cervical Lesions Associated with Gingival Recession: A Pilot Study
Felice Femiano, Rossella Sorice, Rossella Femiano, Luigi Femiano, Ludovica Nucci, Vincenzo Grassia, Marco Annunziata, Andrea Baldi, Nicola Scotti, Livia Nastri
Dentistry Journal.2022; 10(7): 132. CrossRef - Effects of cervical restorations on the periodontal tissues: 5-year follow-up results of a randomized clinical trial
Morgana Favetti, Anelise Fernandes Montagner, Silvia Terra Fontes, Thiago Marchi Martins, Alexandre Severo Masotti, Patricia dos Santos Jardim, Fernanda Oliveira Bello Corrêa, Maximiliano Sergio Cenci, Francisco Wilker Mustafa Gomes Muniz
Journal of Dentistry.2021; 106: 103571. CrossRef
 ePub Link
ePub Link Cite
CiteA combined approach to non-carious cervical lesions associated with gingival recession


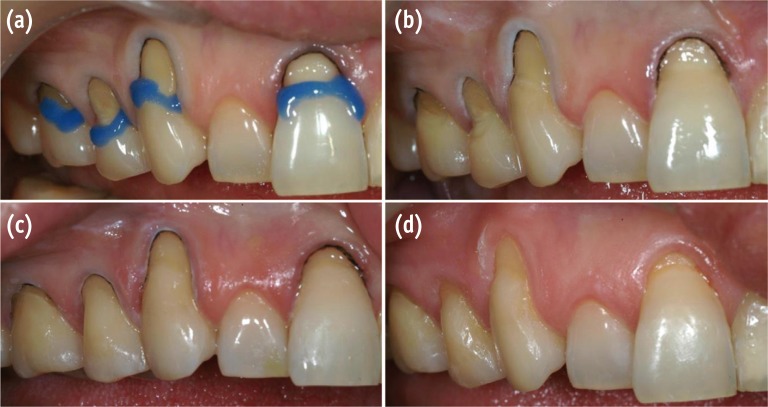
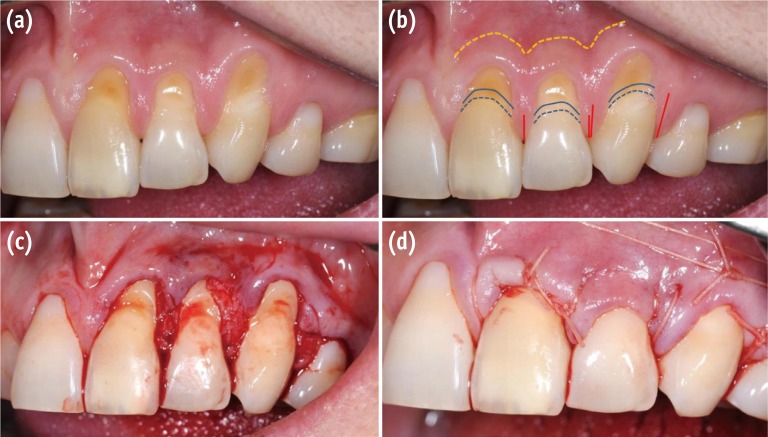
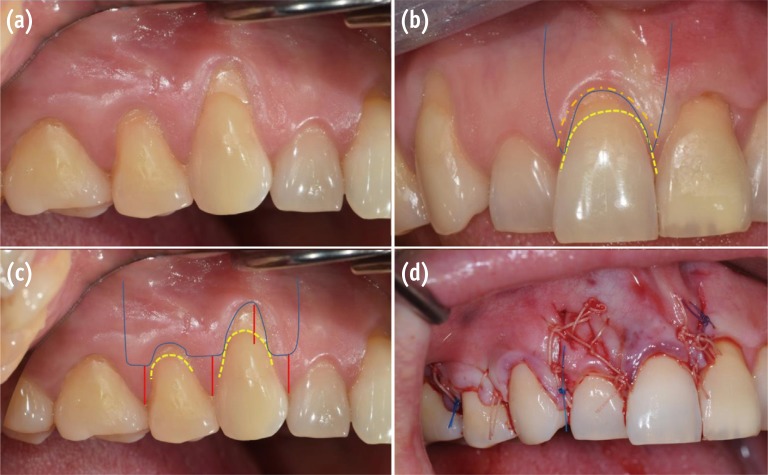
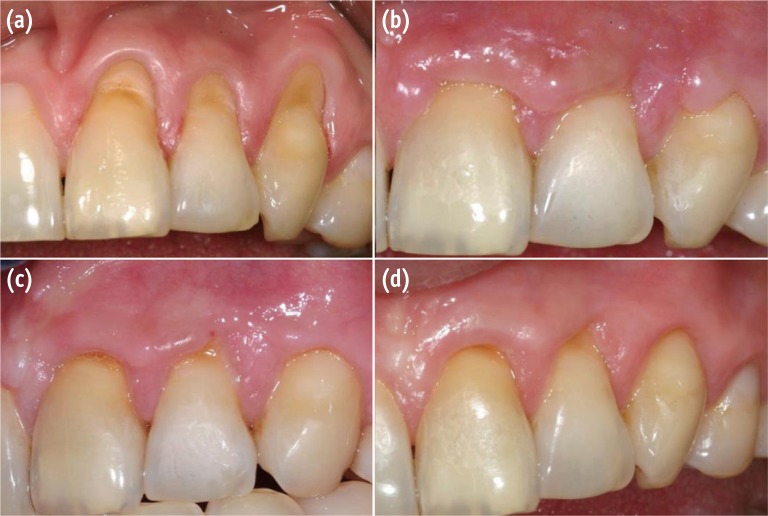
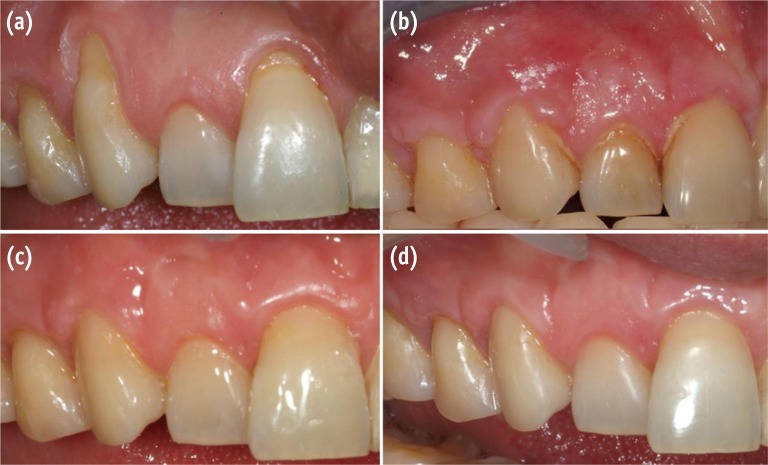

Figure 1 Preoperative frontal view. Note the presence of a non-carious cervical lesion on the maxillary left central incisor, the lateral incisor, and the canines on both sides. Old resin restorations on right first premolar and central incisor showed ill-fitting margins and poor color matching.
Figure 2 Restorative procedures on the maxillary left side. (a) Field isolation and cavity preparation; (b) Phosphoric acid-selective enamel etching; (c) Adhesive system application and incremental resin filling; (d) Photograph after finishing and polishing.
Figure 3 Restorative procedures on the maxillary right side. (a) Phosphoric acid-selective enamel etching after removal of the old restoration and cavity preparation; (b) Adhesive system application; (c) Incremental resin filling; (d) Photograph after finishing and polishing.
Figure 4 Surgical procedures on the maxillary left side. (a) Multiple adjacent NCCLs; (b) Schematic illustration of the surgery plan; (c) Flap reflection view; (d) Postoperative view after suturing. NCCL, non-carious cervical lesion.
Figure 5 Surgical procedures on the maxillary right side. (a) Multiple adjacent NCCLs; (b and c) Schematic illustration of the surgery plan; (d) Postoperative view after suturing. NCCL, non-carious cervical lesion.
Figure 6 Postoperative view of the maxillary left side. (a) Preoperative view; (b) Four week follow-up; (c) Eight week follow-up; (d) Six month follow-up.
Figure 7 Postoperative view of the maxillary right side. (a) Preoperative view; (b) Four week follow-up; (c) Eight week follow-up; (d) Six month follow-up.
Figure 8 Frontal view. (a) Preoperative view; (b) Postoperative view.
Figure 1
Figure 2
Figure 3
Figure 4
Figure 5
Figure 6
Figure 7
Figure 8
A combined approach to non-carious cervical lesions associated with gingival recession

