
Articles
- Page Path
- HOME > Restor Dent Endod > Volume 39(2); 2014 > Article
- Case Report Management of failed periodontal surgical intervention for a furcal lesion with a nonsurgical endodontic approach
- Saeed Asgary1, Mahta Fazlyab2
-
2014;39(2):-119.
DOI: https://doi.org/10.5395/rde.2014.39.2.115
Published online: March 21, 2014
1Iranian Center for Endodontic Research (ICER), Research Institute of Dental Sciences, Shahid Beheshti University of Medical Sciences, Tehran, Iran.
2Dental Research Center, Research Institute of Dental Sciences, Shahid Beheshti University of Medical Sciences, Tehran, Iran.
- Correspondence to Mahta Fazlyab, DDS, MS. Endodontist, Dental Research Center, Research Institute of Dental Sciences, Shahid Beheshti University of Medical Sciences Dental School, Evin, 1983963113, Tehran, Iran. TEL, +98-21-22413897; FAX, +98-21-22427753; dr.mfazlyab@gmail.com
• Received: September 14, 2013 • Accepted: December 22, 2013
©Copyights 2014. The Korean Academy of Conservative Dentistry.
This is an Open Access article distributed under the terms of the Creative Commons Attribution Non-Commercial License (http://creativecommons.org/licenses/by-nc/3.0/) which permits unrestricted non-commercial use, distribution, and reproduction in any medium, provided the original work is properly cited.
- 4,163 Views
- 18 Download
- 4 Crossref
Abstract
- As long as the prognosis of teeth remains a matter of concern, the endodontic-periodontal relationship will be considered a challenge for the clinician. Many etiologic factors, including bacteria, fungi, and viruses, plus other contributing factors, such as trauma, root resorptions/perforations, and dental malformations, play a role in the co-occurrence of endodontic and periodontal lesions. Whatever the cause, a correct diagnosis on which to base the treatment plan is the key to successful maintenance of the tooth. This article reports the successful endodontic management of a furcation lesion in a mandibular molar that was nonresponsive to a previous periodontal surgical graft. The case had presented a diagnostic challenge for the clinicians, and this article reviews the key points that can lead to a correct diagnosis and treatment planning.
Introduction
Despite having different origins, the dental pulp from the dental papilla and the periodontium from the dental follicle, they are closely related through pathways by which infection and irritants are exchanged.1,2 Seltzer et al. noted that inflammation in the pulp space and the spread of microorganisms and their toxic byproducts from the pulp to the periodontal ligament may cause an inflammatory reaction in the interradicular periodontal tissues and vice versa.3 This exchange can happen through the dentinal tubules, the apical foramen, and lateral/accessory canals.4
In the root dentin, numerous tubules extend from the pulp to the cemento-dentinal junction, which can serve as a pulp-periodontium communication pathway as a result of caries, developmental defects, or periodontal or surgical procedures.2,4 The apical foramen is believed to be the major pathway through which bacterial byproducts and inflammatory mediators in a diseased pulp are conducted, causing periapical pathosis.2,4 The opposite route is also possible, although unlikely, as the apex can serve as a portal of entry of inflammatory elements from deep periodontal pockets to the pulp.2,5 Lateral or accessory canals can exist anywhere along the root in about 30 - 40% of teeth and contain connective tissue and blood vessels.4,6 According to De Deus, the majority of lateral canals (17%), are found in the apical third area, 9% in the middle third, and less than 2% in the coronal third.6,7 In the furcation of molars, the patent accessory canals that occur in about 30 - 60% of all molars, may also be a direct pathway of communication between the pulp and the periodontium.4,8
When both the pulp and the periodontal tissues are involved, the endo-perio lesions are best classified as endodontic, periodontal, or a combined diseases.4 The combined diseases include (1) a primary endodontic disease with secondary periodontal involvement, (2) a primary periodontal disease with secondary endodontic involvement, and (3) true combined diseases.2,4 Irrespective of whether the primary disease is endodontic or periodontal, once the lesions progress to the final stage, they exhibit a similar radiographic appearance, and thus, a differential diagnosis becomes more challenging. An accurate understanding of the pathogenesis leads the clinician to an appropriate course of treatment and assessment of the prognosis.9 Primary endodontic diseases usually heal following a root canal treatment.8 The sinus tract extending into the gingival sulcus or the furcation area disappears at an early stage once the affected pulp is removed and the root canal system is well cleaned, shaped, and obturated.4
This case report represents the diagnostic and treatment challenges in a mandibular molar in which the infection of the previously treated pulp space has led to the involvement of the furcation area.
Case report
A 42-year-old female, complaining of a painful swelling beside her right first mandibular molar, demanded a dental visit. She had normal hygiene and mentioned regular dental visits. On tooth #46, a class 1 composite filling with stained margins was evident. On the buccal gingival tissue just below the gingival margin, an inflamed swelling was present that revealed pain upon palpation. On probing assessment of the furcation, a non-through-and-through furcation lesion could be penetrated. Orthoradial periapical radiography (Figure 1a) revealed that a root canal treatment had been performed on this tooth 5 years earlier following severe nocturnal pain. The radiographic quality of root canal therapy (RCT) was not good, and a large furcation lucency extending to the inter-radicular apical region was evident. It also seemed that a periapical lesion existed around the mesial root that had combined with the furcal lucency. The patient mentioned a visit to a periodontist a year before with the same chief complaint. He had diagnosed the problem to be periodontal in origin and performed an alloplastic operation on the furcation of the tooth. The graft was still visible in our radiography, and not only had the healing not occurred, but also, as mentioned before, the symptoms had started to recur.
Considering the furcation lucency that was not responsive to periodontal surgery, the poor quality of RCT, and the presence of the periapical lucency around the mesial root, a diagnosis of the primary endodontic, secondary periodontal lesion was made, and this lesion could be handled with endodontic intervention. The treatment plan was root canal retreatment, permanent restoration of the tooth, and patient follow-up. We also considered that further periodontal intervention might be required if the healing process was assumed to be insufficient during the follow-up.
After local anesthesia with 2% lidocaine containing epinephrine 1 : 80,000 (Darou Pakhsh, Tehran, Iran), the composite filling of the crown was removed. The filling had severe marginal discoloration and upon removal with a high-speed bur, was assumed to be debonded in some areas. The chamber floor was covered with a layer of gutta-percha, which was removed. The orifices of the canals filled with gutta-percha were detected, and then, the tooth was isolated with a rubber dam. Then, the filling material in the coronal portion of the three canals (distal, mesiobuccal, and mesiolingual) was removed with No. 1 - 4 Gates-Glidden drills (Mani, Inc., Tochigi, Japan) and then, subsequent to using a drop of chloroform, the rest of the canal filling was removed with a D-RaCe retreatment file, DR2 (RaCe, FKG Dentaire SA, La Chaux de Fonds, Switzerland) at 900 rpm until the canal was totally cleaned. After the determination of the working length with radiography, the canals were completely shaped to #35/0.04 of the RaCe system, with simultaneous 5.25% NaOCl irrigation. Thereafter, canal obturation and restoration of the access cavity was completed (Figure 1b). After two weeks, the clinical signs/symptoms faded away.
The patient was put on a follow-up schedule with 3-month intervals. Figure 1c shows the 12-month follow-up periapical radiography. Bone healing in the furcation area around the previously inserted graft is evident, and the periapical lucency of the mesial root has healed.
Discussion
This is a report of a diagnostic challenge and a treatment case in a mandibular molar involving the furcation representing a periodontal abscess. The tooth was previously non-responsive to alloplastic surgery following an incorrect etiologic diagnosis. The problem was accurately diagnosed to be an endo-perio lesion with a primary endodontic source. The patient was treated only with an endodontic intervention followed by appropriate coronal sealing.
For assessing the retention rate of endodontically treated teeth, the orthograde endodontic (re)treatment is a predictable procedure with excellent long-term prognosis, provided that the canal system is completely cleaned, shaped, and obturated in order to enhance successful outcomes.10 A poor endodontic treatment allows canal re-infection, which may often lead to treatment failure. In the current case, the previous endodontic treatment did not have a good radiographic quality as a lesion had formed around the mesial root.
Coronal leakage, which appears to be of equal (if not greater) clinical relevance as a factor in endodontic failure than apical leakage, is the term used for the designation of bacterial leakage from the oral environment along the restoration margins to the endodontic filling.11 Studies have indicated that this factor may be an important cause of endodontic treatment failure. Ray and Trope reported that defective restorations and adequate root canal fillings had a higher incidence of failures than inadequate root canal fillings and adequate restorations.12 In some studies, the influence of the coronal seal on the periapical status is stated to be considerably more than that of a well-qualified root canal treatment.11 As mentioned before, the restoration of this tooth, which was de-bonded in some areas, had severe marginal discoloration. This could be a reason for endodontic treatment failure. Moreover, the chamber floor was covered with gutta-percha, which does not provide a perfect seal in this area and could have led to the formation of the furcation lesion. It is recommended that excess gutta-percha filling be removed to the level of the canal orifices and that the floor of the pulp chamber be protected with a well-sealed restorative material.13
Primary endodontic disease with secondary periodontal involvement, primary periodontal disease with secondary endodontic involvement, and true combined diseases are clinically and radiographically very similar.2,4,14 In this case, the furcation abscess was previously diagnosed to have a primary periodontal cause. It is worth mentioning that primary periodontal lesions are caused primarily by periodontal pathogens. In this process, chronic marginal periodontitis progresses apically along the root surface. In most cases, pulp tests indicate a clinically normal pulpal reaction.2,14 Accumulation of plaque and calculus and the formation of wide pockets are frequent. The prognosis depends on the stage of the periodontal disease and the efficacy of the periodontal treatment.2,14 As mentioned earlier, our patient had normal oral hygiene and did not exhibit any signs of periodontitis or even gingivitis. She mentioned regular dental visits twice a year, and the last scaling was 6 months earlier. This reveals that her problem could not be of periodontal origin (primary periodontal or true combined lesion), and the non-responsiveness of the defect to the periodontal treatment confirms this diagnosis.
As a chronic apical lesion in a tooth with an infected pulp space may drain coronally through the periodontal ligament into the gingival sulcus, the same process can also occur in the presence of lateral canals extending from the chamber floor to the furcation area.2,4,14 This is what is believed to have occurred in our case, that is, a pre-existing infection in the pulp space subsequent to RCT or re-infection of the canal system due to coronal leakage, both leading to the spread of infection to the furcation area through furcal accessory canals. This condition clinically mimics the presence of a periodontal abscess but in reality, is a sinus tract of pulpal origin that opens through the periodontal ligament area.2,14 Further, for diagnostic purposes, it is essential for the clinician to insert a gutta-percha cone into the sinus tract and to take one or more radiographs to determine the origin of the lesion.4 Our patient did not have a traceable sinus tract at that time.
Our treatment plan consisted of a single-visit nonsurgical endodontic retreatment and patient follow-up. It is said that if a lesion is diagnosed and treated as a primary endodontic disease due to lack of evidence of marginal periodontitis, and there is soft-tissue healing on clinical probing and bone healing on a recall radiogragh, a valid retrospective diagnosis can be made.2,4 In the present case, the follow-up process revealed bone healing at the one-year follow-up. The degree of healing that takes place following the root canal treatment will determine the retrospective classification. In the absence of adequate healing, further periodontal treatment may be indicated, but it was not necessary in our case. Another issue is the selection of the single-visit endodontic treatment. Experts are of the opinion that although the multiple-visit treatment and the use of intracanal medication with a calcium hydroxide-water slurry, will lower the bacterial count in the infected root canals, it fails to obtain total elimination of bacterial organisms on a consistent basis.15 The effectiveness of calcium hydroxide in completely removing bacteria from the infected root canals in less than 4 weeks is under debate as persistent infection in 26% of the canals after 2 weeks of exposure to calcium hydroxide, has been shown.16,17 Moreover, the absence of difference in the radiological success of root canal therapy between single- and multiple-visit treatments has been addressed in many reviews.18,19 According to a Cochrane systematic review, no difference exists in the effectiveness of treatment, in terms of radiological success, between single- and multiple-visit root canal therapy.18 Others have questioned the routine use of calcium hydroxide on the basis of the resistance of certain bacteria such as Enterococcus faecalis to this chemical.8,13 From this perspective, firm justification for a multiple-treatment approach cannot be claimed. Considering the advantages of single-visit root canal therapy such as its being faster and better tolerated by patients, and its avoidance of the recontamination of the canal(s) between appointments, we decided to perform a single-visit retreatment. The successful outcome of the treatment confirms this treatment plan.20
On the other hand, eradication of the bacteria is the key to successful treatment outcomes.18 It has also been observed that the preparation of nonround canals leaves some canal surface uninstrumented, and this fact cannot be overlooked when treating infected canals.21 Disinfection of the root canal system by a combination of mechanical cleaning and chemical irrigation is critical for successful endodontic treatment outcomes.21 The ideal irrigant should kill all remaining bacteria and detoxify all bacterial substances within the canal and the dentinal tubules, all without risking appreciable host tissue damage.15 During the treatment of the present case, mechanical instrumentation of the canals was complemented by a synchronous irrigation of the root canal system by 5.25% NaOCl.
Another important issue is the size of apical preparation in this case (#35/0.04). It is stated that over-enlargement of the apical foramen carried out with successively larger files will often enlarge the foramen in such a way that an oval-shaped opening will be created. This can decrease the chances of a successful outcome of endodontic therapy.15 As a result, serum factors from the exudate released from the periapical area may provide a nutritional boost to the intracanal bacteria.15 The size of the canal prepared apically and the effect of the canal taper on the outcome are considered important to the success of the endodontic treatment, such that increased success rates have been reported in the case of greater canal flare.22 Sequeira et al. reported that increasing the size of apical preparation from #30 to #40 resulted in a significant reduction in the number of cultivable bacteria.23 However, when Coldero et al. studied the effect of the size of apical preparation on the number of bacteria remaining in the root canal, they concluded that additional apical enlargement to size #35 did not further reduce the number of surviving bacteria.24 For the present case, the master apical file was a #35/0.04. Thus, the increase in apical size and taper helped in bacterial reduction.
Conclusions
Pulp and periodontal tissues are intimately connected, and the pathology of one can negatively influence that of the other. As a result, a correct diagnosis of the etiology can establish appropriate treatments of different origins, periodontal or endodontic. This case report was based on a primary misdiagnosis that was time consuming and costly for the patient. This fact highlights the inevitable value of a correct diagnosis of the etiology that as in this case, can lead to successful treatment and outcome. Further, the efficiency of single-visit RCT cannot be overlooked.
- 1. Zuza EP, Toledo BE, Hetem S, Spolidório LC, Mendes AJ, Rosetti EP. Prevalence of different types of accessory canals in the furcation area of third molars. J Periodontol 2006;77:1755-1761.ArticlePubMed
- 2. Oved-Peleg E, Lin S. Periodontal-endodontal interactions. Refuat Hapeh Vehashinayim 2005;22:43-51. 91.
- 3. Seltzer S, Bender IB, Ziontz M. The interrelationship of pulp and periodontal disease. Oral Surg Oral Med Oral Pathol 1963;16:1474-1490.ArticlePubMed
- 4. Zehnder M, Gold SI, Hasselgren G. Pathologic interactions in pulpal and periodontal tissues. J Clin Periodontol 2002;29:663-671.ArticlePubMedPDF
- 5. Tanomaru JM, Leonardo MR, Tanomaru-Filho M, da Silva LA, Ito IY. Microbial distribution in the root canal system after periapical lesion induction using different methods. Braz Dent J 2008;19:124-129.ArticlePubMed
- 6. Uzun Ö, Topuz Ö, Aslan S, Tinaz AC. Effects of simulated lateral canals on the accuracy of measurements by an electronic apex locator. J Can Dent Assoc 2012;78:c65.PubMed
- 7. De Deus QD. Frequency, location, and direction of the lateral, secondary, and accessory canals. J Endod 1975;1:361-366.ArticlePubMed
- 8. Jansson LE, Ehnevid H. The influence of endodontic infection on periodontal status in mandibular molars. J Periodontol 1998;69:1392-1396.ArticlePubMed
- 9. Lin S, Tillinger G, Zuckerman O. Endodontic-periodontic bifurcation lesions: a novel treatment option. J Contemp Dent Pract 2008;9:107-114.Article
- 10. Alkahtani A, Al-Subait S, Anil S. An in vitro comparative study of the adaptation and sealing ability of two carrier-based root canal obturators. ScientificWorldJournal 2013;2013:532023.ArticlePubMedPMCPDF
- 11. Gillen BM, Looney SW, Gu LS, Loushine BA, Weller RN, Loushine RJ, Pashley DH, Tay FR. Impact of the quality of coronal restoration versus the quality of root canal fillings on success of root canal treatment: a systematic review and meta-analysis. J Endod 2011;37:895-902.ArticlePubMedPMC
- 12. Ray HA, Trope M. Periapical status of endodontically treated teeth in relation to the technical quality of the root filling and the coronal restoration. Int Endod J 1995;28:12-18.ArticlePubMed
- 13. Saunders WP, Saunders EM. Assessment of leakage in the restored pulp chamber of endodontically treated multirooted teeth. Int Endod J 1990;23:28-33.ArticlePubMed
- 14. Rotstein I, Simon JH. Diagnosis, prognosis and decision-making in the treatment of combined periodontal-endodontic lesions. Periodontol 2000 2004;34:165-203.ArticlePubMed
- 15. Trope M, Bergenholtz G. Microbiological basis for endodontic treatment: can a maximal outcome be achieved in one visit? Endodontic Topics 2002;1:40-53.ArticlePDF
- 16. Reit C, Molander A, Dahlén G. The diagnostic accuracy of microbiologic root canal sampling and the influence of antimicrobial dressings. Endod Dent Traumatol 1999;15:278-283.ArticlePubMed
- 17. Reit C, Dahlén G. Decision making analysis of endodontic treatment strategies in teeth with apical periodontitis. Int Endod J 1988;21:291-299.ArticlePubMed
- 18. Figini L, Lodi G, Gorni F, Gagliani M. Single versus multiple visits for endodontic treatment of permanent teeth. Cochrane Database Syst Rev 2007;4:CD005296.Article
- 19. Naito T. Single or multiple visits for endodontic treatment? Evid Based Dent 2008;9:24.ArticlePubMedPDF
- 20. K B. Trial suggests no difference between single-visit and two-visit root canal treatment. Evid Based Dent 2013;14:48.PubMed
- 21. Paqué F, Balmer M, Attin T, Peters OA. Preparation of oval-shaped root canals in mandibular molars using nickel-titanium rotary instruments: a micro-computed tomography study. J Endod 2010;36:703-707.ArticlePubMed
- 22. Gulabivala K, Patel B, Evans G, Ng YL. Effects of mechanical and chemical procedures on root canal surfaces. Endodontic Topics 2005;10:103-122.Article
- 23. Siqueira JF Jr, Lima KC, Magalhães FA, Lopes HP, de Uzeda M. Mechanical reduction of the bacterial population in the root canal by three instrumentation techniques. J Endod 1999;25:332-335.ArticlePubMed
- 24. Coldero LG, McHugh S, MacKenzie D, Saunders WP. Reduction in intracanal bacteria during root canal preparation with and without apical enlargement. Int Endod J 2002;35:437-446.ArticlePubMed
REFERENCES
Figure 1
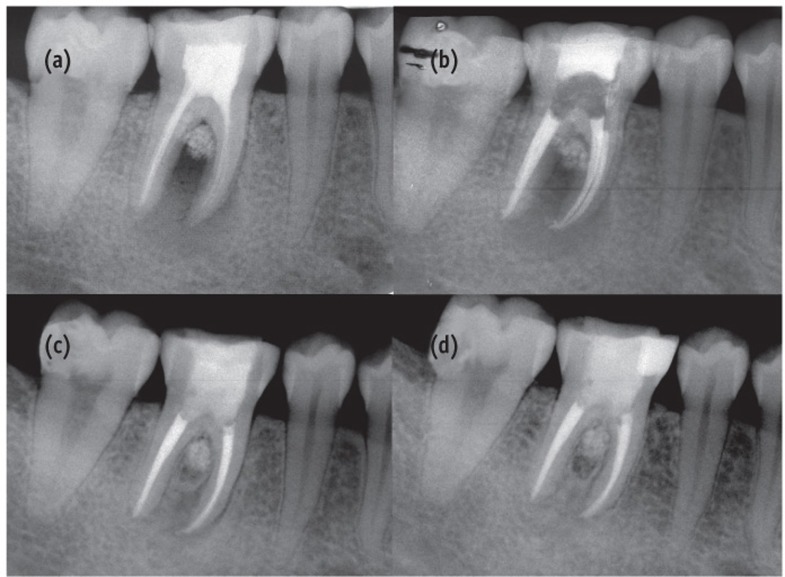
(a) Pretreatment radiography of tooth #46. Note the radiolucency in the furcation area and around the mesiobuccal root. Further, note the previous alloplastic graft in the furcation area, to which the lesion was nonresponsive; (b) Post-treatment radiography. The canals have been cleaned and obturated; (c) One-year follow-up radiography; (d) Two-year follow-up radiography. The tooth was restored one week after endodontic retreatment. The lesion in the furcation area and around the root healed completely. The alloplastic graft was not resorbed.
Tables & Figures
REFERENCES
Citations
Citations to this article as recorded by 
- NON-SURGICAL ENDODONTIC TREATMENT OF CHRONIC APICAL PERIODONTITIS WITH EXTENSIVE PERIAPICAL AND FURCATION BONE DESTRUCTION: A CASE REPORT WITH 18-MONTH FOLLOW-UP
Magomedov Ibragim, Supiev Lugman, Omarov Muslim
BULLETIN OF STOMATOLOGY AND MAXILLOFACIAL SURGERY.2026; : 34. CrossRef - Acute periodontal lesions (periodontal abscesses and necrotizing periodontal diseases) and endo‐periodontal lesions
David Herrera, Belén Retamal‐Valdes, Bettina Alonso, Magda Feres
Journal of Clinical Periodontology.2018;[Epub] CrossRef - Acute periodontal lesions (periodontal abscesses and necrotizing periodontal diseases) and endo‐periodontal lesions
David Herrera, Belén Retamal‐Valdes, Bettina Alonso, Magda Feres
Journal of Periodontology.2018;[Epub] CrossRef - The importance of correct diagnosis and treatment in endo-periodontal lesions: a two cases comparison
Sara Bernardi, Christian Frascarelli, Giulia Fantozzi, Silvia Caruso, Robert Gatto, Gianna Maria Nardi, Maria Adelaide Continenza
Dental Update.2016; 43(8): 766. CrossRef
 ePub Link
ePub Link Cite
CiteManagement of failed periodontal surgical intervention for a furcal lesion with a nonsurgical endodontic approach
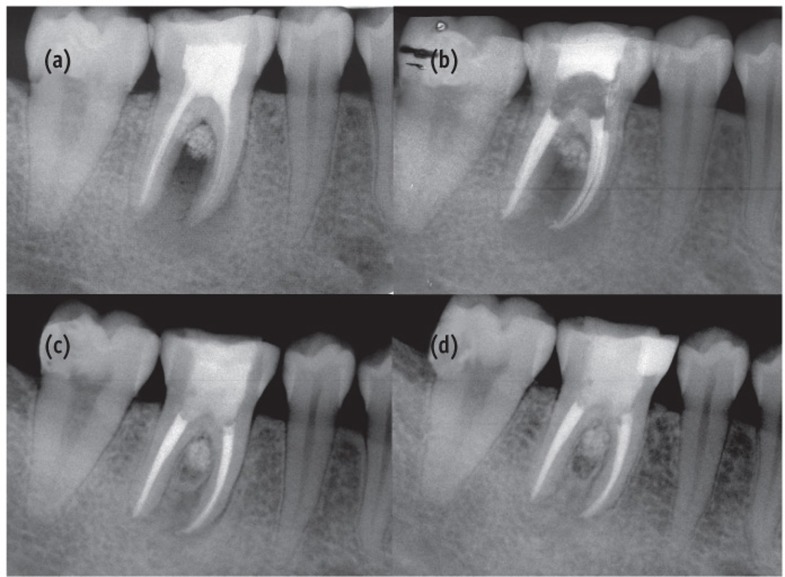
Figure 1 (a) Pretreatment radiography of tooth #46. Note the radiolucency in the furcation area and around the mesiobuccal root. Further, note the previous alloplastic graft in the furcation area, to which the lesion was nonresponsive; (b) Post-treatment radiography. The canals have been cleaned and obturated; (c) One-year follow-up radiography; (d) Two-year follow-up radiography. The tooth was restored one week after endodontic retreatment. The lesion in the furcation area and around the root healed completely. The alloplastic graft was not resorbed.
Figure 1
Management of failed periodontal surgical intervention for a furcal lesion with a nonsurgical endodontic approach

