
Articles
- Page Path
- HOME > Restor Dent Endod > Volume 38(1); 2013 > Article
- Research Article Effective application duration of sodium ascorbate antioxidant in reducing microleakage of bonded composite restoration in intracoronally-bleached teeth
- Jae-Young Park1, Tae-Yub Kwon2, Young-Kyung Kim1
-
2013;38(1):-47.
DOI: https://doi.org/10.5395/rde.2013.38.1.43
Published online: February 26, 2013
1Department of Conservative Dentistry, Kyungpook National University School of Dentistry, Daegu, Korea.
2Department of Dental Biomaterials, Kyungpook National University School of Dentistry, Daegu, Korea.
- Correspondence to Young Kyung Kim, DDS, PhD. Associate Professor, Department of Conservative Dentistry, Kyungpook National University School of Dentistry, 2-188-1 Samduk-dong, Jung-gu, Daegu, Korea 700-412. TEL, +82-53-600-7601; FAX, +82-53-426-8958; wisekim@knu.ac.kr
• Received: November 27, 2012 • Revised: January 7, 2013 • Accepted: January 13, 2013
©Copyights 2013. The Korean Academy of Conservative Dentistry.
This is an Open Access article distributed under the terms of the Creative Commons Attribution Non-Commercial License (http://creativecommons.org/licenses/by-nc/3.0/) which permits unrestricted non-commercial use, distribution, and reproduction in any medium, provided the original work is properly cited.
- 2,414 Views
- 15 Download
- 10 Crossref
Abstract
-
Objectives The aim of this study was to determine an appropriate application duration of sodium ascorbate (SA) antioxidant gel in reducing microleakage of bonded composite restoration in intracoronally-bleached teeth.
-
Materials and Methods Eighty endodontically-treated human incisors were randomly divided into eight groups: control, no bleaching; IB and DB, immediate and delayed bonding after bleaching, respectively; S10m, S60m, S24h, S3d and S7d, bleaching + SA gel for 10 min, 60 min, 24 hr, 3 day and 7 day, respectively. For bleaching, a mixture of 30% hydrogen peroxide and sodium perborate was applied for 7 day. All access cavities were restored using One-Step adhesive (Bisco Inc.) and then Aelite LS Packable composite (Bisco Inc.). The bonded specimens were subjected to 500 thermal cycles, immersed in 1% methylene blue for 8 hr, and longitudinally sectioned. Microleakage was assessed with a 0 - 4 scoring system and analyzed using nonparametric statistical methods (α = 0.05).
-
Results Group IB showed a significantly higher microleakge than the control group (p = 0.006) and group DB a statistically similar score to the control group (p > 0.999). Although groups S10m, S60m, and S24h exhibited significantly higher scores than group DB (p < 0.05), the microleakage in groups S3d and S7d was statistically similar to that in group DB (p = 0.771, p > 0.999).
-
Conclusions Application of SA gel for 3 day after nonvital bleaching was effective in reducing microleakage of composite restoration in intracoronally-bleached teeth.
Introduction
Nonvital tooth bleaching is a conservative esthetic treatment for endodontically-treated discolored teeth, generally followed by adhesive restoration of the access cavity. However, residual oxygen on the bleached surface interferes with resin polymerization, reducing the sealing ability of composite restorations.1 Re-infection or recurrent discoloration from coronal leakage could impair the long-term success of both endodontic therapy and bleaching treatment.2 Because the residual oxygen after bleaching slowly dissipates over time, delayed bonding is commonly recommended clinically to avoid problems due to reduced sealing ability.3
It has been reported that the application of sodium ascorbate (SA) antioxidant into the access cavity of intracoronally-bleached tooth allows immediate composite restoration after nonvital bleaching through its ability to remove oxygen radicals.4,5 Notwithstanding the proven efficacy of SA application for the purpose, its effective application duration remains controversial. Türkün and Türkün reported that 3-hour application of 10% SA solution following nonvital bleaching was effective on 10% carbamide peroxide (CP)-treated tooth surface, while May et al. used the same antioxidant for only 10 minutes on the surface treated with a stronger bleaching agent, 35% CP.6,7 Lai et al. suggested that the use of SA to neutralize the oxidizing effect of a bleaching agent may involve at least one-third of the bleaching time.8
Accordingly, the aim of this study was to determine the minimally required application duration of SA gel in terms of microleakage of composite restoration in intracoronally-bleached teeth.
Materials and Methods
A total of eighty human incisors were collected with informed signed consent obtained under a protocol approved by the Ethics Committee of the School of Dentistry, Kyungpook National University, disinfected in 0.5% chloramine T, and stored in distilled water at 4℃ until use. After access openings (3 mm in diameter) were made using a round diamond bur in a high-speed handpiece under cooling with air/water, the canals were prepared and obturated with gutta-percha (META BIOMED Co., Ltd., Cheongwon, Korea) and AH26 sealer (Dentsply DeTrey, Konstanz, Germany). The gutta-percha was removed to 2 mm apical to the labial cemento-enamel junction and a 2-mm-thick glass ionomer base (Fuji II LC, GC Corp., Tokyo, Japan) was placed over the root filling. The specimens were randomly divided into eight groups of 10 specimens each. All specimens except for the control group (no bleaching) were subjected to a bleaching procedure by placing a mixture of 30% hydrogen peroxide (HP) and sodium perborate into the pulp chamber for 7 days.9
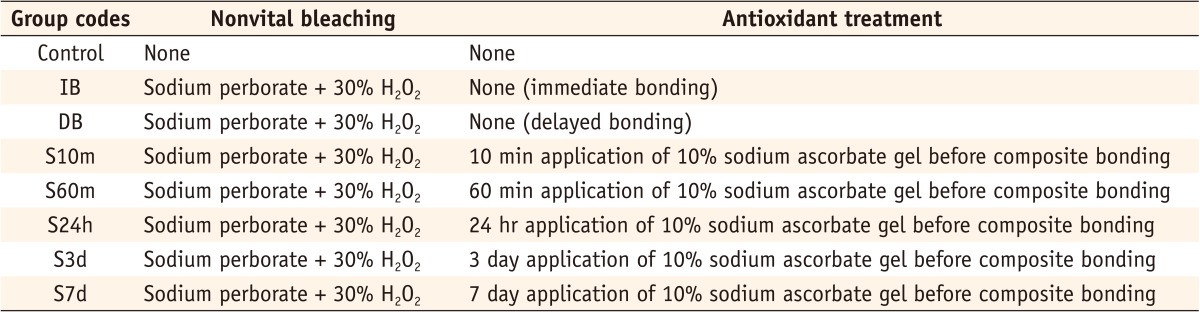
The cavities of group IB (immediate bonding) were restored immediately after bleaching using the bonding procedure. For group DB (delayed bonding), the teeth were immersed in distilled water for 7 days and subjected to bonding. For groups S10m, S60m, S24h, S3d and S7d, SA gel was prepared by dispersing the carbopol resin (2.5% wt/wt) in 10% SA solution and applied into the pulp chamber with an application period of 10 minutes, 60 minutes, 24 hours, 3 days and 7 days, respectively (Table 1).10 To prepare 10% SA solution, sodium ascorbate (L (+) Ascorbic acid sodium salt, Daejung Chemicals, Siheung, Korea) was dissolved in purified water at room temperature. In the bonding steps, all access cavities were etched with 32% phosphoric acid (Uni-Etch, Bisco Inc., Schaumburg, IL, USA) for 15 seconds. Adhesive (One-Step, Bisco Inc.) was applied to the etched surface and light-cured for 10 seconds using a halogen curing light (Optilux 501, SDS Kerr/Demetron, Orange, CA, USA; light intensity = 500 mW/cm2). Resin composite (Aelite LS Packable, A1 shade, Bisco Inc., A1 shade) was filled into the cavity and polymerized using an incremental technique with a 1.5 - 2.0 mm thick increment in three layers. Each composite layer was light-cured for 20 seconds and final cure was done for 30 seconds. All teeth of eight groups were stored in distilled water at 37℃ for 24 hours and restorations were finished and polished using the Enhance system (LD Caulk/Dentsply, Milford, DE, USA). The specimens were then subjected to 500 thermal cycles between water baths of 5 and 55℃, with a dwell time of 30 seconds and transfer time of 5 seconds.11
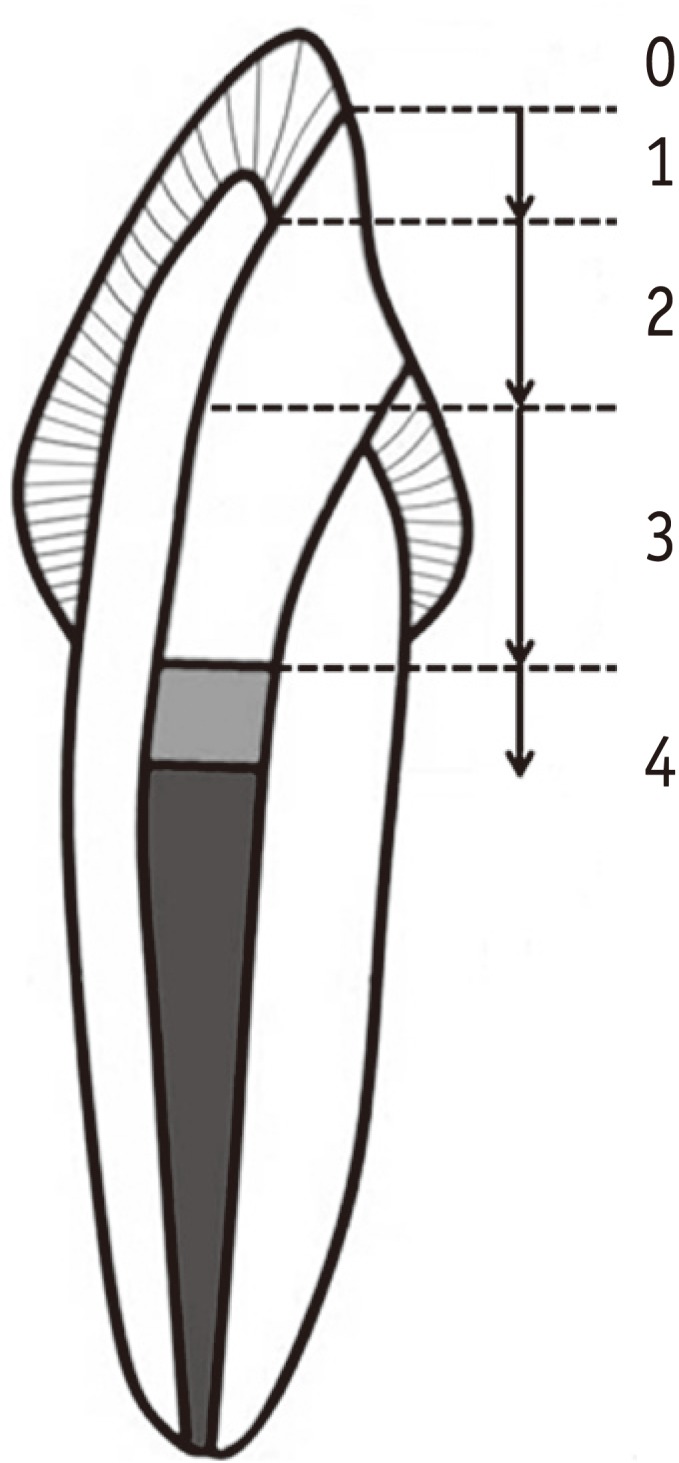
The specimens were covered with two coats of nail varnish except 1 mm around the tooth-restoration interface and the root apices were sealed with utility wax. After immersion in 1% methylene blue for 8 hours, teeth were washed in tap water, and nail varnish and utility wax were removed with a scalpel. The teeth were sectioned longitudinally from labial to lingual through the center of the restoration using a low-speed diamond saw (Isomet, Buehler Ltd., Lake Bluff, IL, USA). Microleakage was assessed by two cross-calibrated examiners using a stereomicroscope (Olympus Co., Tokyo, Japan) at ×20 magnification. Dye penetration was scored with a 0 - 4 rating system (Figure 1).
The microleakage data were analyzed by Kruskal-Wallis and Mann-Whitney U tests. The Benjamini and Hochberg false discovery rate was used to correct occurrence of false positives. All statistical analyses were performed using SPSS 12.0 (SPSS Inc., Chicago, IL, USA) at a significance level of 0.05.
Results
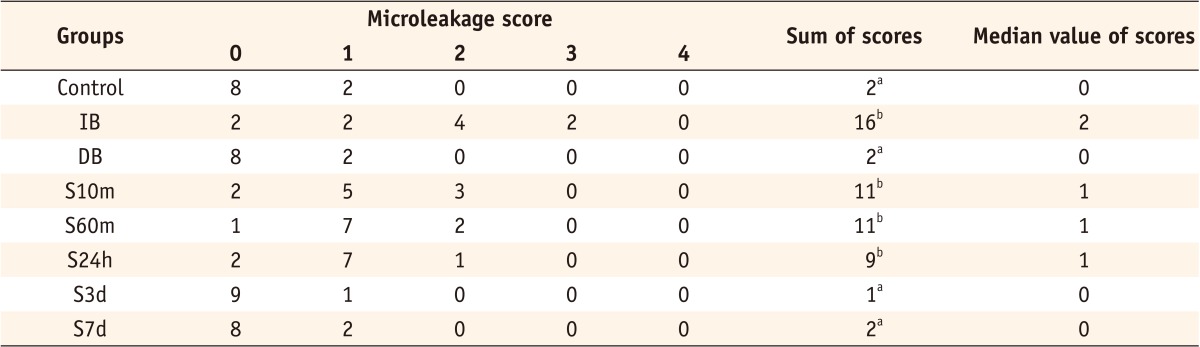
Table 2 shows the microleakage score results. Kruskal-Wallis analysis demonstrated significant differences among the test groups (p < 0.001). Group IB showed a significantly higher microleakge than the control group (p = 0.006) and group DB a statistically similar score to the control group (p > 0.999). Although groups S10m, S60m, and S24h exhibited significantly higher scores than group DB (p < 0.05), groups S3d and S7d scores were statistically similar to group DB (p = 0.771 and p > 0.999, respectively).
Discussion
The present in vitro study confirmed that immediate bonding after intracoronal bleaching produces incomplete sealing of composite restoration. In this study, when the composite restoration was delayed until 7 days after bleaching, the sealing ability of the restoration increased up to the level obtained in the non-bleached control. As Khoroushi et al. suggested, a certain waiting period is required to allow a gradual elimination of residual oxygen from the bleached surface before adhesive restoration.4 The present microleakage study also demonstrated that the 3-day application of 10% SA gel into the pulp chamber allows earlier composite restoration with improved sealing ability.
A previous study reported that the reaction between SA and 35% HP occurred as fast as 5 minutes after mixing so that the application of SA could allow bonding procedures to begin soon, without the elapsed time between bleaching and restoration.12 Although the median value (1) of S10m, S60m, and S24h was smaller than that of IB (median value: 2), there was no statistically significant difference in microleakage among the groups (Table 2). The complete reversal of reduced sealing ability was attained when SA gel was applied on the bleached tooth surface for 3 days.
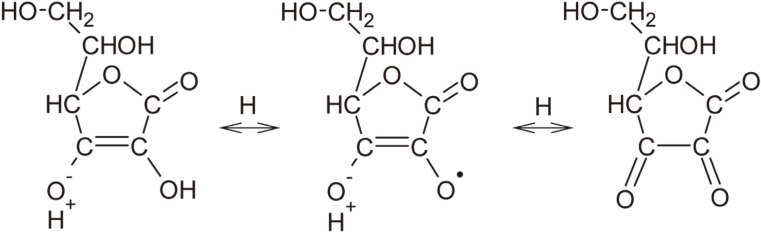
The carbon-carbon double bond of ascorbic acid, or ascorbate, possesses high reducing potential, readily donating hydrogen and electrons to oxidants.13,14 The first step in the oxidation of ascorbic acid is the formation of dehydroascorbic acid through a free radical intermediate (Figure 2).15 This reversible reaction is believed to be responsible for the antioxidant properties of ascorbic acid.15 However, the use of antioxidant to neutralize the oxidizing effect of bleaching agent is likely to need a long period of time.8 This result can be partly explained by slow uptake of SA gel into the bleached tooth surface. Ascorbate is highly water soluble and not suited to dissolve in the lipoidal components of membranes.16 Thus, its movement between body compartments by simple diffusion is so slow that active transport such as carrier-mediated movement is needed for rapid onset of its action.17 Considering that ascorbate is locally applied to the bleached tooth surface as in the present study, the penetration of ascorbate into the tissue would be hindered by its slow movement through simple diffusion, thereby retarding its antioxidant effect.
In addition, unlike previous studies in which 10% CP was used for nonvital bleaching,5,6 the use of a stronger bleaching agent, a mixture of 30% HP and sodium perborate, could be another factor in the delayed antioxidant effect of SA. Although the association of sodium perborate with 30% HP can be more effective in lightening tooth color, it may affect bonding more adversely due to the high concentration of peroxide.
Regarding dye leakage scores, in control, DB, S3d and S7d groups, dye penetrated only into enamel, while dye penetration up to half of the cavity depth was observed in groups S10m, S60m and S24h. However, dye did not reach the gutta-percha root filling in any of specimens, even in the immediately restored group. This result can be accounted for by the use of a glass ionomer base as a protective barrier over the gutta-percha, supporting that the placement of a protective base is a critical step in sealing the root canal from seepage of bleaching agent.18
The finding of this in vitro study suggests that 3-day application of SA antioxidant gel to intracoronally-bleached teeth by applying a mixture of 30% HP and sodium perborate for 7 days is needed to address the reduced sealing ability of composite restoration. Shorter application of the antioxidant (e.g. 2 days) should be evaluated in further studies. From the clinical standpoint, moreover, since immediate restoration after nonvital bleaching is preferred in completing the restoration of the access cavity to prevent microleakage, the use of faster-acting antioxidants should be further investigated.
Conclusions
Within the limitation of this study, application of SA gel for 3 days after nonvital bleaching was effective in reducing microleakage of composite restoration in intracoronally-bleached teeth.
-
This research was supported by the Basic Science Research Program through the National Research Foundation of Korea (NRF), funded by the Ministry of Education, Science and Technology (2011-0028242).
-
No potential conflict of interest relevant to this article was reported.
- 1. Rueggeberg FA, Margeson DH. The effect of oxygen inhibition on an unfilled/filled composite system. J Dent Res 1990;69:1652-1658.ArticlePubMedPDF
- 2. Howell RA. The prognosis of bleached root-filled teeth. Int Endod J 1981;14:22-26.ArticlePubMed
- 3. Cavalli V, Reis AF, Giannini M, Ambrosano GM. The effect of elapsed time following bleaching on enamel bond strength of resin composite. Oper Dent 2001;26:597-602.PubMed
- 4. Khoroushi M, Feiz A, Ebadi M. Influence of intermediary filling material on microleakage of intracoronally bleached and restored teeth. Dent Res J (Isfahan) 2009;6:17-22.PubMedPMC
- 5. Moosavi H, Moghaddas MJ, Ghoddusi J, Rajabi O. Effects of two antioxidants on the microleakage of resin-based composite restorations after nonvital bleaching. J Contemp Dent Pract 2010;11:E033-E040.Article
- 6. Türkün M, Türkün LS. Effect of nonvital bleaching with 10% carbamide peroxide on sealing ability of resin composite restorations. Int Endod J 2004;37:52-60.ArticlePubMed
- 7. May LG, Salvia AC, Souza RO, Michida SM, Valera MC, Takahashi FE, Bottino MA. Effect of sodium ascorbate and the time lapse before cementation after internal bleaching on bond strength between dentin and ceramic. J Prosthodont 2010;19:374-380.PubMed
- 8. Lai SC, Mak YF, Cheung GS, Osorio R, Toledano M, Carvalho RM, Tay FR, Pashley DH. Reversal of compromised bonding to oxidized etched dentin. J Dent Res 2001;80:1919-1924.ArticlePubMedPDF
- 9. Barkhordar RA, Kempler D, Plesh O. Effect of nonvital tooth bleaching on microleakage of resin composite restorations. Quintessence Int 1997;28:341-344.PubMed
- 10. Kimyai S, Valizadeh H. The effect of hydrogel and solution of sodium ascorbate on bond strength in bleached enamel. Oper Dent 2006;31:496-499.ArticlePubMedPDF
- 11. Teixeira EC, Hara AT, Turssi CP, Serra MC. Effect of non-vital tooth bleaching on microleakage of coronal access restorations. J Oral Rehabil 2003;30:1123-1127.ArticlePubMedPDF
- 12. Freire A, Souza EM, de Menezes Caldas DB, Rosa EA, Bordin CF, de Carvalho RM, Vieira S. Reaction kinetics of sodium ascorbate and dental bleaching gel. J Dent 2009;37:932-936.ArticlePubMed
- 13. Buettner GR. The pecking order of free radicals and antioxidants: lipid peroxidation, alpha-tocopherol, and ascorbate. Arch Biochem Biophys 1993;300:535-543.PubMed
- 14. May JM. Ascorbate function and metabolism in the human erythrocyte. Front Biosci 1998;3:d1-d10.ArticlePubMed
- 15. Deutsch JC. Ascorbic acid oxidation by hydrogen peroxide. Anal Biochem 1998;255:1-7.ArticlePubMed
- 16. Rose RC, Bode AM. Biology of free radical scavengers: an evaluation of ascorbate. FASEB J 1993;7:1135-1142.ArticlePubMedPDF
- 17. Rose RC. Transport of ascorbic acid and other water-soluble vitamins. Biochim Biophys Acta 1988;947:335-366.ArticlePubMed
- 18. Vosoughhosseini S, Lotfi M, Shahmoradi K, Saghiri MA, Zand V, Mehdipour M, Ranjkesh B, Mokhtari H, Salemmilani A, Doosti S. Microleakage comparison of glass-ionomer and white mineral trioxide aggregate used as a coronal barrier in nonvital bleaching. Med Oral Patol Oral Cir Bucal 2011;16:e1017-e1021.ArticlePubMed
REFERENCES
Tables & Figures
REFERENCES
Citations
Citations to this article as recorded by 
-
Effect of Herbal Antioxidant on Push-out Bond Strength of Resin-based Composite to Dentin after Intracoronal Bleaching: An
in vitro
Study
Parinitha MS, Akshay G, Vidya G. Doddawad, Ashwini Tumkur Shivakumar, Sowmya Halasabalu Kalgeri
Journal of Pharmacology and Pharmacotherapeutics.2025; 16(4): 439. CrossRef - Evaluation of the effect of the application of Quercus cerris extract and the use of fluoride bonding material on the bonding strength of orthodontic brackets after tooth bleaching with hydrogen peroxide
Ezgi Ay, Derya Dursun
PeerJ.2025; 13: e19335. CrossRef - Photon-Induced Photoacoustic Streaming Activation of the Postbleaching Antioxidant Application Rapidly Improves Bonding to Pulp Chamber Dentin
Nasibe Aycan Yilmaz, Hicran Dönmez Özkan
Photobiomodulation, Photomedicine, and Laser Surgery.2021; 39(4): 289. CrossRef - Hypericum perforatum L.: A Potent Antioxidant Source for the Treatment of Oxidized Dentin: An Experimental In Vitro Study
Nasibe Aycan Yilmaz, Rukiye Yavaser, Arife Alev Karagozler
Journal of Advanced Oral Research.2021; 12(1): 57. CrossRef - Influence of a short‐time antioxidant application on the dentin bond strength after intracoronal bleaching
Muhammet Karadas, Sezer Demirbuga
Microscopy Research and Technique.2019; 82(10): 1720. CrossRef - Composite resin shear bond strength on bleached dentin increased by 35% sodium ascorbate application
Tunjung Nugraheni, N Nuryono, Siti Sunarintyas, Ema Mulyawati
Dental Journal (Majalah Kedokteran Gigi).2017; 50(4): 178. CrossRef - Antioxidant therapy enhances pulpal healing in bleached teeth
Adriano Fonseca Lima, Marcelo Rocha Marques, Diana Gabriela Soares, Josimeri Hebling, Giselle Maria Marchi, Carlos Alberto de Souza Costa
Restorative Dentistry & Endodontics.2016; 41(1): 44. CrossRef - Influence of Ethanol Pretreatment on the Bonding of Resin Composite to Bleached Dentin
Ga-Eun Son, Tae-Yub Kwon, Young Kyung Kim
Korean Journal of Dental Materials.2015; 42(4): 279. CrossRef - Effect of 35% Sodium Ascorbate Treatment on Microtensile Bond Strength after Nonvital Bleaching
Jason R. Hansen, Kenneth J. Frick, Mary P. Walker
Journal of Endodontics.2014; 40(10): 1668. CrossRef - Pull-out bond strength of a self-adhesive resin cement to NaOCl-treated root dentin: effect of antioxidizing agents
Maryam Khoroushi, Marzieh Kachuei
Restorative Dentistry & Endodontics.2014; 39(2): 95. CrossRef
 ePub Link
ePub Link Cite
CiteEffective application duration of sodium ascorbate antioxidant in reducing microleakage of bonded composite restoration in intracoronally-bleached teeth
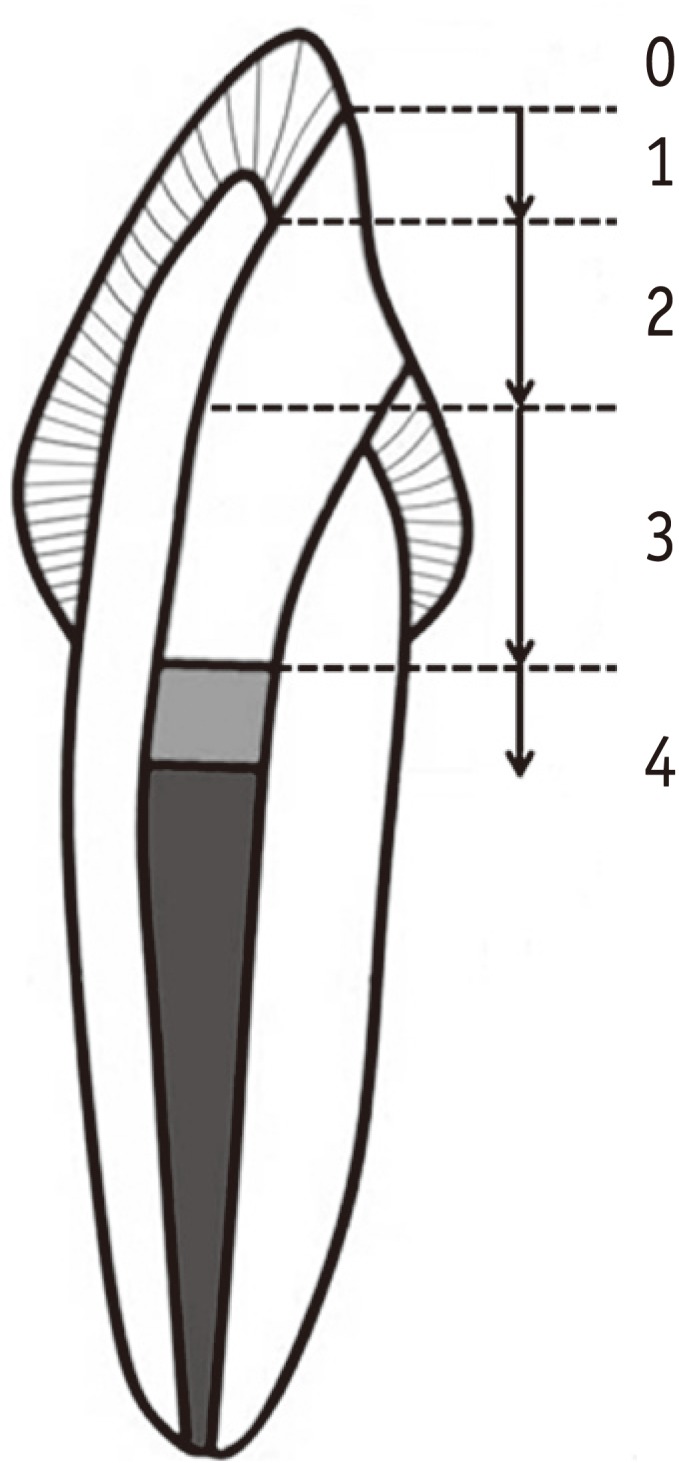
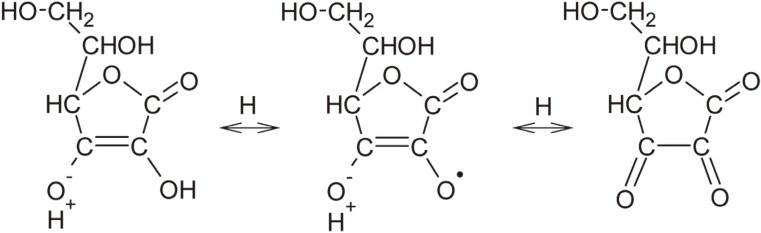
Figure 1 Criteria for evaluating microleakage scores. 0, No dye penetration; 1, Dye penetration only into the enemel; 2, Dye penetration up to half of the cavity depth; 3, Dye penetration greater than score 2 without involvement of gutta-percha; 4, Dye penetration with involvement of gutta-percha.
Figure 2 Oxidative mechanism of ascorbic acid representing its antioxidant properties.
Figure 1
Figure 2
Effective application duration of sodium ascorbate antioxidant in reducing microleakage of bonded composite restoration in intracoronally-bleached teeth
Group codes according to bleaching and antioxidant treatment

Microleakage score results

The same superscripts are not significantly different (p > 0.05).
Table 1 Group codes according to bleaching and antioxidant treatment
Table 2 Microleakage score results
The same superscripts are not significantly different (

