
Articles
- Page Path
- HOME > Restor Dent Endod > Volume 37(3); 2012 > Article
- Case Report Diagnostic challenges of nonodontogenic toothache
- Hyung-Ok Park, Jung-Hong Ha, Myoung-Uk Jin, Young-Kyung Kim, Sung-Kyo Kim
-
2012;37(3):-174.
DOI: https://doi.org/10.5395/rde.2012.37.3.170
Published online: August 29, 2012
Department of Conservative Dentistry, Kyungpook National University School of Dentistry, Daegu, Korea.
- Correspondence to Sung-Kyo Kim, DDS, MSD, PhD. Professor, Department of Conservative Dentistry, Kyungpook National University School of Dentistry, 188-1 Samdeok 2-ga, Jung-gu, Daegu, Korea 700-705. TEL, +82-53-600-7601; FAX, +82-53-426-8958; skykim@knu.ac.kr
• Received: November 4, 2011 • Revised: May 31, 2012 • Accepted: June 3, 2012
©Copyights 2012. The Korean Academy of Conservative Dentistry.
This is an Open Access article distributed under the terms of the Creative Commons Attribution Non-Commercial License (http://creativecommons.org/licenses/by-nc/3.0/) which permits unrestricted non-commercial use, distribution, and reproduction in any medium, provided the original work is properly cited.
- 3,148 Views
- 32 Download
- 9 Crossref
Abstract
- The objective of this article was to present two nonodontogenic conditions that may mimic odontogenic toothache: trigeminal neuralgia and burning mouth syndrome. Two cases are presented in which one is related to the upper left second premolar and the other is related to the upper left first molar. Both showed pain when chewing. These two cases highlight the complexities involved in diagnosing nonodontogenic toothache. This article demonstrates the importance of having a thorough knowledge of both odontogenic and nonodontogenic toothache, as well as the need for careful evaluation of the nature of the pain and history, clinical and radiographic examinations.
Introduction
One of the most challenging and rewarding aspects of general practice is the diagnosis and treatment of pain. Chung et al. reported nearly 42% of the general population experienced at least one of five types of orofacial pain in the past 6 months.1 The most common type of orofacial pain was toothache, which was reported by 26.8% of the population. Because toothache is so common, it is essential for the clinician who is managing orofacial pain to have a thorough understanding of its clinical presentation. Once proper diagnosis is established, successful treatment for pain of dental origin is usually quite predictable.
An essential component of the diagnostic process depends on the patient's history of pain and the description or reaction to diagnostic tests. If pain were purely a sensory phenomenon, diagnosis would be fairly straightforward. However, pain has both sensory and emotional components. This complex nature of pain may make it difficult for patients to adequately describe the essential components for diagnosis such as intensity, location and duration.2 Also, toothaches can present a diagnostic problem for the clinician because pain felt in one tooth may be referred from another tooth or from other orofacial structures.3 To complicate matters further, other facial pain disorders may mimic the symptoms of toothache because the primary afferent neuron synapses with a second-order neuron in the trigeminal nucleus.4-6
Diagnostic procedures may therefore be limited to identifying a suspect tooth rather than a nonodontogenic source of pain. A misdiagnosis will lead to unnecessary treatment for the patient and may also exacerbate the symptoms for which the patient sought treatment. To treat toothache effectively, the clinician must first determine if the pain is truly odontogenic in origin. If it is not, the clinician is faced with the challenge of determining the true origin of the pain.
This article presents two cases that may mimic odontogenic pain: trigeminal neuralgia and burning mouth syndrome and illustrates the complexities of diagnosing nonodontogenic pain.
Case reports
A 50-year-old female was referred for evaluation of pain on #15, the upper left second premolar. She complained sharp pain on #15 when chewing that started 2 weeks ago. To resolve her discomfort, she visited her general dental practitioner and root canal therapy was started on this tooth. The patient was subsequently referred to the Department of Conservative Dentistry, Kyungpook National Dental Hospital when the pain was not resolved.
Clinical examination revealed that tooth #15 was restored with temporary filling material. The tooth was positive to percussion and periodontal probing depths on distopalatal area of was more than 7 mm. Pain could be elicited by bite test of the tooth. All adjacent teeth responded within normal limits to percussion, palpation and bite test and showed positive response to vitality tests with cold spray and electronic pulp tester. No noticeable pathologies were observed on the radiographs except alveolar bone resorption on distopalatal area of #15 (Figure 1a). On the basis of clinical findings and history of pain, a diagnosis of acute apical periodontitis was suspected. Root canal treatment was performed on this tooth (Figure 1b).
On follow-up 2 week later, the patient was still experiencing what she described as 'sharp pain' from her lower right tooth not from tooth #15. At this time she pointed to tooth #45 and insisted that sharp pain resulted when chewing. Tooth #45 was slightly sensitive to percussion and pain could be elicited by bite test of the tooth. Tooth #45 responded within normal limits when tested with cold and electronic pulp tester. A caries cavity was observed at the distal surface of #45 on the radiograph (Figure 2a). Intraligamental injection on #45 area resulted in relieving the pain. A definitive diagnosis could not be made from the clinical findings. Distal caries on #45 was removed and the tooth was restored with composite resin (Figure 2b).
On follow-up 1 week later, the patient informed us that the sharp pain on chewing had not resolved. The failure of standard dental tests to ascertain the cause of pain necessitated further investigation. Palpating of the right masseter muscle, medial pterygoid muscle, lateral pterygoid muscle and temporalis muscle was performed. When palpating of the right lateral pterygoid muscle, the pain was elicited. Based on contributing factors of the pain that were chewing on #45 and palpation of the right lateral pterygoid muscle and the pattern and nature of the pain, a possible diagnosis of myofascial pain or trigeminal neuralgia was suspected. The patient was referred to the Department of Oral Medicine, Kyungpook National Dental Hospital. Further questioning revealed the pain episodes consisted of 'severe stabbing pain' that radiated to the right cheek and continued less than 1 minute. The pain could be elicited by chewing right side and tooth brushing. The presenting complaint was diagnosed as trigeminal neuralgia, and carbamazepine was recommended as the treatment of choice. 200 mg of carbamazepine, taken twice daily, was prescribed. The patient's symptoms resolved within 2 weeks.
A 57-year-old female was referred for evaluation of pain on #26, the upper left first molar. She complained dull pain on #26 when chewing. The patient reported a history of pain on #26 five months ago. To resolve her discomfort, she visited her general dental practitioner and root canal therapy was performed on this tooth. The patient had some relief of pain for approximately 2 weeks after root canal treatment of #26 was completed, but the pain returned. The patient was subsequently referred when the pain did not abate.
Clinical examination revealed that tooth #26 was restored with gold crown. Percussion and bite testing of #26 were positive and periodontal probing depths of #26 were less than 3 mm. All adjacent teeth responded within normal limits for percussion, palpation, bite test and vitality when tested with cold and electronic pulp tester. Radiographic examination revealed tooth #26 had root canal treatment and no noticeable pathologies were observed (Figure 3a). On the basis of clinical findings and history of pain, a diagnosis of acute apical periodontitis was suspected. Root canal retreatment was performed on this tooth. During the treatment, missing canal MB2 of #26 was found. After canal enlargement and canal dressing with calcium hydroxide on MB2 canal of #26, the pain was relieved and root canal retreatment was completed (Figure 2b) on assumption that acute apical periodontitis because of untreated canal, MB2 of #26 was the source of her pain.
The patient visited again 9 months later complaining that the pain returned to the area of tooth #26. The patient reported spontaneous dull pain and gingival pain of #26. The patient also wanted removal of gold crown on #26 because she felt odd taste of crown. Percussion, palpation and bite testing of #26 were negative. A Radiograph was taken, which revealed no noticeable pathologies (Figure 3c) As well, all adjacent teeth responded within normal limits for percussion, palpation, bite test and vitality when tested with cold and electronic pulp tester. Intraligamental injection on this area was not effective in reducing the pain. A definitive diagnosis could not be made from the clinical findings, the following treatment options were discussed with the patient: (1) no treatment and follow-up check for monthly, (2) apical surgery, or (3) extraction. The patient was told that the pain may be referred from another source or from another tooth. The patient elected to have no treatment and follow-up check for monthly.
On follow-up 1 month later, the patient reported continued pain in the area of the treated tooth. The dull pain on #26 was exacerbated and tingling on the right maxillary posterior area and burning sensation of left lateral side of tongue were appeared. The patient insisted that treated tooth #26 was the source of the pain. Radiographic examination revealed that no noticeable pathologies were observed on #26 (Figure 3d). There were no mucosal abnormalities and the patient is a postmenopausal woman. A possible diagnosis of burning mouth syndrome was suspected. The patient was referred to the Department of Oral Medicine, Kyungpook National Dental Hospital. Further questioning revealed that the onset of pain was spontaneous and the burning sensation often occurred in more than one oral site, those were the left posterior palate, buccal gingiva and left lateral side of tongue. Alterations in taste also occurred. The presenting complaint was diagnosed as burning mouth syndrome. 10 mg of benzodiazepine (Rivotril, a chlonazepam, Roche, Basal, Switzerland) taken twice daily, was prescribed. This provided a reduction in pain from 8 of VAS scale to 4 after four weeks and to 1 after ten weeks, this was effective in controlling the symptoms.
Discussion
It is not unusual for a patient to report to a dental practitioner with orofacial pain of an unclear origin. Without a thorough diagnosis, or in the absence of conclusive findings, a dentist may treat the pain as odontogenic toothache.7 These conditions that may mimic symptoms of odontogenic toothache are trigeminal neuralgia and burning mouth syndrome.
Trigeminal neuralgia, because of its varied presentation and distressing nature, can be especially challenging to the dental practitioner.8 Trigeminal neuralgia is characterized by sudden, sharp, severe unilateral pain. It is often described as a stabbing, shooting, burning or paresthesia sensation.9,10 The pain follows one or more branches of the trigeminal nerve.9-11 It can last seconds to minutes, then disappear leaving pain-free intervals between attacks.11 Trigger zones around the nose and mouth are a characteristic feature of trigeminal neuralgia. Attacks can be provoked by such innocuous stimuli as taking, chewing, tooth brushing or light touch.9,10 Local anesthetic placed in the trigger zone reduces the pain.4 Trigeminal neuralgia may be triggered from the teeth and felt as pain in the teeth. Unfortunately, anesthetic blocking arrests the paroxysms of pain, which may lead to a mistaken diagnosis of odontogenic pain. Also, dental therapy, especially if a local anesthetic block is used, may induce a remission, thereby leading both patient and dentist to assume that the diagnosis is correct and that a proper treatment has been completed. In case 1, on one week follow-up, muscles were palpated in order to rule out the possibility of myofacial pain and pain was elicited, which did not reach acceptable values of specificity.12 Trigger zone associated with #45 was provoked by chewing right side presenting 'severe stabbing pain' that radiated to the right cheek. At first, the patient felt the pain on #15 and root canal treatment of #15 was performed.13 It was similar to a situation termed pre-trigeminal neuralgia, which can greatly confuse initial diagnosis and delay the delivery of a definitive diagnosis of trigeminal neuralgia.14 Subsequently the patient felt the pain on #45 not on #15 and the pain was relieved when local anesthetic placed in this area. This made difficult to diagnosis with the challenge of determining the true origin of the pain.
Burning mouth syndrome is defined as burning pain in the tongue or other oral mucous membrane associated with normal signs and laboratory findings lasting at least 4 to 6 months.15,16 Burning mouth syndrome has a higher prevalence in postmenopausal women.17 The burning sensation often occurs in more than one oral site, with the anterior two thirds of the tongue, the anterior hard palate and the mucosa of the lower lip most frequently involved and oral burning is often accompanied by other symptoms, including dry mouth and altered taste.18 In case 2, the origin of the pain of #26, at first, was dental structure and the initial diagnosis was correct. 9 months later, however, the origin of the pain of #26 was referred from other orofacial structures and based on the nature of the patient's pain, the finally diagnosis was burning mouth syndrome. In recent study, Nixdorf et al. reported the frequency of nonodontogenic pain in patients who had undergone endodontic procedures was approximately 3.4%, that is, nonodontogenic pain is not an uncommon outcome after root canal treatment.19 In other recent study, Takenoshita et al. reported that for burning mouth syndrome, the complaints occurred after dental treatment in 38.9%, after other medical treatment in 10.3%, after stressful or emotional events in 10.3%, and spontaneously in 36.5%, that is, more than on third of patients of Burning mouth syndrome relate time of onset to a dental procedures.20 The patient can misunderstand the pain which is actually nonodontogenic pain, occurs because of the dental procedures. In this case 2, the patient insisted the cause of the pain was treated tooth #26, however, final diagnosis was burning mouth syndrome.
These cases, case 1 and case 2 illustrates the difficulties often encountered in diagnosing orofacial pain. First, the patient's interpretation of symptoms and reaction to clinical testing can reflect both emotional and physical components of pain.2 To further complicate the issue, a patient's interpretation of the discomfort may not truly reflect the area in which the pathology is present.21,22 Second, despite careful examination of the symptoms, differential diagnosis of orofacial pain conditions can be challenging.
These two case reports emphasize the necessity for a thorough knowledge of the orofacial pain which includes both odontogenic and nonodontogenic pain because knowing the pain characteristic for each disorders is an essential key to diagnosis. Careful history and clinical and radiologic examination are important. As well, thorough evaluations of the nature of pain, including aggravating and relieving factors and associated symptoms, are necessary.23
Conclusions
Nonodontogenic toothaches are often difficult to identify and can challenge the diagnostic ability of the clinician. The most important step toward proper management of toothache is to consider that the pain may not be of dental origin. To aid correct diagnosis, precise understanding of clinical characteristics of odontogenic and nonodontogenic toothache, careful history, clinical and radiologic examination, and thorough evaluation of the nature of the pain are recommend. That can lead to deliver appropriate therapy and avoid unnecessary procedures and aggravating the condition.
- 1. Chung JW, Kim JH, Kim HD, Kho HS, Kim YK, Chung SC. Chronic orofacial pain among Korean elders: prevalence, and impact using the graded chronic pain scale. Pain 2004;112:164-170.PubMed
- 2. Lilly JP, Law AS. Atypical odontalgia misdiagnosed as odontogenic pain: a case report and discussion of treatment. J Endod 1997;23:337-339.ArticlePubMed
- 3. DuPont JS Jr. Neuritic toothache. Gen Dent 2001;49:178-181.PubMed
- 4. Okeson JP, Falace DA. Nonodontogenic toothache. Dent Clin North Am 1997;41:367-383.ArticlePubMed
- 5. Mattscheck D, Law AS, Nixdorf DR. In: Hargreaves KM, Cohen S, editors. Diagnosis of nonodontogenic toothache. Cohen's pathways of the pulp. 2011. 10th ed. St Louis: Mosby Elsevier; p. 51.
- 6. Ohn YS, Park SJ. The study on the characteristics of nociceptive neurons in trigeminal subnucleus oralis. J Korean Acad Conserv Dent 1999;24:614-622.
- 7. Yang SH, Jung DH, Lee HD, Lee Y, Chang HS, Min KS. Clinical diagnosis of herpes zoster presenting as odontogenic pain. J Korean Acad Conserv Dent 2008;33:452-456.Article
- 8. Shankland WE 2nd. Trigeminal neuralgia: typical or atypical? Cranio 1993;11:108-112.ArticlePubMed
- 9. Zakrzewska JM. Diagnosis and differential diagnosis of trigeminal neuralgia. Clin J Pain 2002;18:14-21.PubMed
- 10. Gass A, Kitchen N, McManus DG, Moseley IF, Hennerici MG, Miller DH. Trigeminal neuralgia in patients with multiple sclerosis: lesion localization with magnetic resonance imaging. Neurololgy 1997;49:1142-1144.Article
- 11. Burchiel KJ, Slavin KV. On the natural history of trigeminal neuralgia. Neurosurgery 2000;46:152-154.ArticlePubMed
- 12. Conti PC, Dos Santos Silva R, Rossetti LM, De Oliveira Ferreira Da Silva R, Do Valle AL, Gelmini M. Palpation of the lateral pterygoid area in the myofascial pain diagnosis. Oral Surg Oral Med Oral Pathol Oral Radiol Endod 2008;105:e61-e66.ArticlePubMed
- 13. Headache Classification Subcommittee of the International Headache Society (IHS). The International Classification of Headache Disorders. 2005;2nd ed. 1st revision. Available from: http://www.ihs-headache.org/frame_non_members.asp (updated 2005 May).
- 14. Fromm GH, Graff-Radford SB, Terrence CF, Sweet WH. Pre-trigeminal neuralgia. Neurology 1990;40:1493-1495.PubMed
- 15. Grinspan D, Fernández Blanco G, Allevato MA, Stengel FM. Burning mouth syndrome. Int J Dermatol 1995;34:483-487.ArticlePubMed
- 16. Grushka M. Clinical features of burning mouth syndrome. Oral Surg Oral Med Oral Pathol 1987;63:30-36.ArticlePubMed
- 17. Grushka M, Epstein JB, Gorsky M. Burning mouth syndrome. Am Fam Physician 2002;65:615-620.ArticlePubMed
- 18. Ship JA, Grushka M, Lipton JA, Mott AE, Sessle BJ, Dionne RA. Burning mouth syndrome: an update. J Am Dent Assoc 1995;126:842-853.PubMed
- 19. Nixdorf DR, Moana-Filho EJ, Law AS, McGuire LA, Hodges JS, John MT. Frequency of nonodontogenic pain after endodontic therapy: a systematic review and meta-analysis. J Endod 2010;36:1494-1498.ArticlePubMedPMC
- 20. Takenoshita M, Sato T, Kato Y, Katagiri A, Yoshikawa T, Sato Y, Matsushima E, Sasaki Y, Toyofuku A. Psychiatric diagnoses in patients with burning mouth syndrome and atypical odontalgia referred from psychiatric to dental facilities. Neuropsychiatr Dis Treat 2010;13:699-705.
- 21. Shankland WE 2nd. Differential diagnosis of two disorders that produce common orofacial pain symptoms. Gen Dent 2001;49:150-155.PubMed
- 22. Gremillion HA. Multidisciplinary diagnosis and management of orofacial pain. Gen Dent 2002;50:178-186.PubMed
- 23. Matwychuk MJ. Diagnostic challenges of neuropathic tooth pain. J Can Dent Assoc 2004;70:542-546.PubMed
REFERENCES

Tables & Figures
REFERENCES
Citations
Citations to this article as recorded by 
- Analysis of Final Diagnosis of Patients with Suspected Nonodontogenic Toothache: A Retrospective Study
Jeong Yeop Chun, Young Joo Shim
Journal of Oral Medicine and Pain.2024; 49(3): 57. CrossRef - Interactions of Acetyl-11-Keto-Beta-Boswellic Acid on Catechol-O-Methyltransferase in the Management of Masticatory Myofascial Pain Syndrome
Ramya Suresh, Pradeep Kumar Yadalam, Ramya Ramadoss, Karthikeyan Ramalingam, Arvind Muthukrishnan
Cureus.2024;[Epub] CrossRef - Assessment of Concordance between Chairside Ultrasonography and Digital Palpation in Detecting Myofascial Trigger Points in Masticatory Myofascial Pain Syndrome
Mohamed Elbarbary, Michael Goldberg, Howard C. Tenenbaum, David K. Lam, Bruce V. Freeman, David J. Pustaka, David Mock, Joseph Beyene, Amir Azarpazhooh
Journal of Endodontics.2023; 49(2): 129. CrossRef - Masticatory Myofascial Pain Syndrome: Implications for Endodontists
Mohamed Elbarbary, Ariel Oren, Michael Goldberg, Bruce V. Freeman, David Mock, Howard C. Tenenbaum, Amir Azarpazhooh
Journal of Endodontics.2022; 48(1): 55. CrossRef - PRICE 2020 guidelines for reporting case reports in Endodontics: explanation and elaboration
V. Nagendrababu, B. S. Chong, P. McCabe, P. K. Shah, E. Priya, J. Jayaraman, S. J. Pulikkotil, P. M. H. Dummer
International Endodontic Journal.2020; 53(7): 922. CrossRef - Clinical Outline of Oral Diseases
Arvind Babu Rajendra Santosh, Doryck Boyd, Kumaraswamy Kikeri Laxminarayana
Dental Clinics of North America.2020; 64(1): 1. CrossRef - Nonodontogenic Sources of Dental Pain
Scott E. Schames, Michael Jordan, Hila Robbins, Lenard Katz, Kaitlyn Tarbert
Journal of the California Dental Association.2016; 44(8): 507. CrossRef - Nonodontogenic toothaches
Edward F. Wright
The Journal of the American Dental Association.2015; 146(6): 406. CrossRef - Síndrome de boca ardiente: claves diagnósticas y terapéuticas
Eduardo Chimenos-Küstner, Cristina Arcos-Guerra, Maria Sueli Marques-Soares
Medicina Clínica.2014; 142(8): 370. CrossRef
 ePub Link
ePub Link Cite
CiteDiagnostic challenges of nonodontogenic toothache
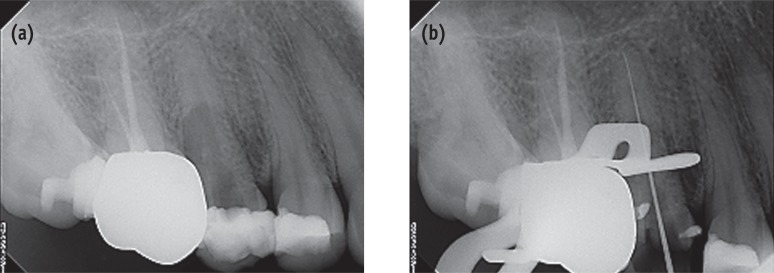
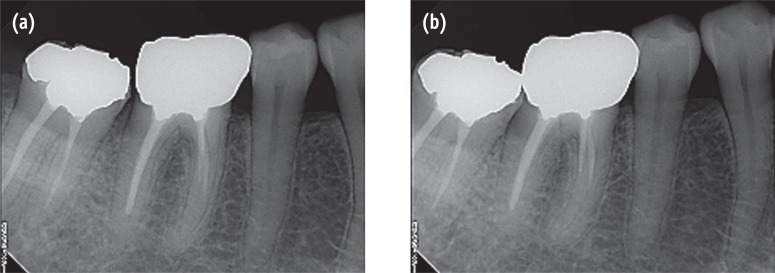
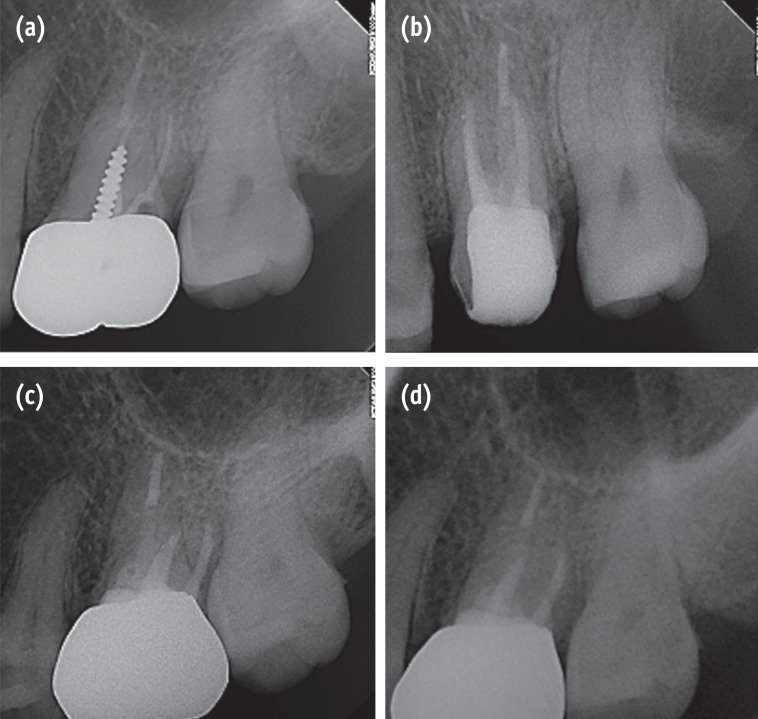
Figure 1 (a) Periapical radiography of tooth #15 at initial presentation; (b) Determination of working length on tooth #15.
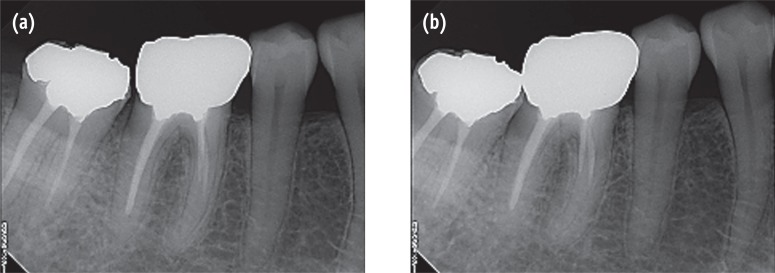
Figure 2 (a) Radiographic image showing distal caries of tooth #45; (b) Tooth is restored with composite resin.
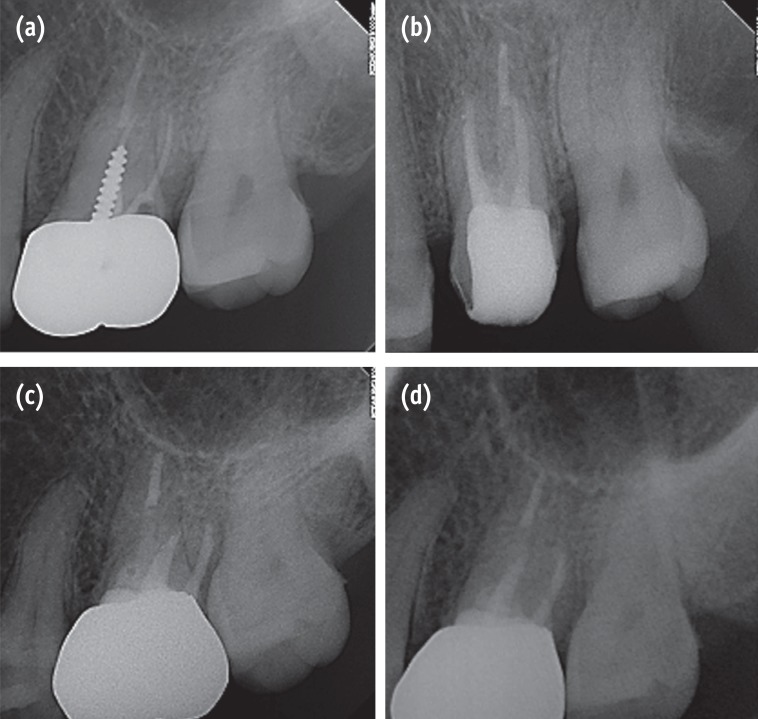
Figure 3 (a) Periapical radiography of tooth #26 at initial presentation; (b) Completion of root canal retreatment; (c) 9-month follow-up radiography; (d) 10-month follow-up radiography.
Figure 1
Figure 2
Figure 3
Diagnostic challenges of nonodontogenic toothache

