
Articles
- Page Path
- HOME > Restor Dent Endod > Volume 49(4); 2024 > Article
- Research Article Predictive factors in the retrieval of endodontic instruments: the relationship between the fragment length and location
-
Ricardo Portigliatti
 , Eugenia Pilar Consoli Lizzi, Pablo Alejandro Rodríguez
, Eugenia Pilar Consoli Lizzi, Pablo Alejandro Rodríguez -
Restor Dent Endod 2024;49(4):e35.
DOI: https://doi.org/10.5395/rde.2024.49.e35
Published online: September 9, 2024
Department of Endodontic, School of Dentistry, University of Buenos Aires, Buenos Aires, Argentina.
- Correspondence to Ricardo Portigliatti, DDS, PhD. Department of Endodontic, School of Dentistry, University of Buenos Aires, Marcelo Torcuato de Alvear 2142, CABA, Buenos Aires C1053ABH, Argentina. rportig@intramed.net
• Received: April 25, 2024 • Revised: June 23, 2024 • Accepted: June 27, 2024
Copyright © 2024. The Korean Academy of Conservative Dentistry
This is an Open Access article distributed under the terms of the Creative Commons Attribution Non-Commercial License (https://creativecommons.org/licenses/by-nc/4.0/) which permits unrestricted non-commercial use, distribution, and reproduction in any medium, provided the original work is properly cited.
Abstract
-
Objectives This study aimed to relate the file fragment length and location in the root canal to the retrieval chances, the clinical time required and the occurrence of secondary fractures.
-
Materials and Methods Sixty clinical cases of fractured instruments were included in this study. They were classified according to the instrument length and the location of the root canal. In each group, the success rate in the instrument retrieval, the clinical time required and the occurrence of secondary fractures were evaluated. The collected data were analyzed using the Kruskal-Wallis test on the basis of a 0.05 significance level.
-
Results The fragment length showed no significant influence on the assessed variables (p > 0.05). The root third where the instrument was located resulted in an increased clinical time, with statistically significant differences (p < 0.05). However, the procedure success rate and the occurrence of secondary fractures showed no association with these variables.
-
Conclusions In accordance with the findings of this study, the fractured fragment length did not influence any of the variables assessed, but it is suggested to focus on the fragment location inside the root canal to decide the retrieval of a fractured instrument.
INTRODUCTION
During the root canal preparation, fractures of the endodontic instrument can occur, affecting the prognosis of the treated tooth. Attempting fragment retrieval, lateral bypassing, treating the root canal up to the level of the fragment, or a surgical procedure can be the treatment options to perform when instruments are broken [1]. The decision depends on the operator's expertise in performing the retrieval, magnification management, and the availability of extraction systems for fractured fragments [2,3]. In the case of attempting the retrieval, it becomes challenging to predict the success rate as well as the occurrence of procedural accidents and the clinical time required [4]. Currently, scientific progress is focused on the study of the causes of instrument fractures in order to prevent this type of accident [5]. However, file fracture remains a problem even today in clinical practice [6].
The main causes of the file fracture are cyclic flexural fatigue and torsional stress [7]. The flexural cyclic fatigue occurs when a wire is bent over and over again at the same point and, for this reason, this event is referred to as cyclic fatigue. This occurs both in instruments with rotatory and reciprocating kinematics [8,9,10,11]. The resistance of an instrument to the CF is inversely related to its size. So, the larger the diameter of the wire subjected to flexion, the lower the resistance to cyclic fatigue [12]. As regards the metallography, the predominance of the martensitic phase favors the resistance when compared to the instruments with higher austenitic expression [13]. On the other hand, the torsional stress arises from the mechanical locking of the instrument within the root canal, usually in a location close to the tip. This friction hinders the instrument movement, either engine-driven or handled by the operator [14]. When the rotational force applied exceeds the resistance limit, plastic deformations occur in the shank of the file, leading to separation [7]. The resistance to torsional stress increases with the increase in the size of the file. Since the tip of the file is its thinnest part, this is the site of the instrument most sensitive to torsional fracture [15,16]. Furthermore, the files with austenitic configuration show higher resistance to torsional fracture than those with martensitic configuration [17].
The intracanal location and the length of the fragment are other factors affecting the removal procedures [12,18,19]. If the choice is to remove the fragment, the procedure protocol includes the use of magnification, specific ultrasonic tips, and removal systems such as micro-tweezers, microloops, and microtube devices [4,20,21]. Procedural risks involved in all these techniques are the root weakening in particular, or the occurrence of a secondary fracture, that is, the separation of the fragment while trying to dislodge it [22,23].
This clinical study was designed to take into account the risks of the procedures and those variables affecting the prognosis and the final success predictability. The objective of this study is to establish a relation between the fragment length and location with the retrieval possibility, the clinical time required and the occurrence of secondary fractures.
MATERIALS AND METHODS
The present study protocol was reviewed and approved by the Institutional Review Board of the Ethics Committee of the School of Dentistry of the University of Buenos Aires (approval No. 006/2020), and the informed consent was submitted by all participants. Sixty clinical cases of fractured instruments in patients attending the Postgraduate Program of Endodontics, University of Buenos Aires, Argentina, were included in this study. Inclusion criteria comprised teeth that required endodontic treatment and exhibited fragments of endodontic instruments. The exclusion criteria ruled out teeth in which the straight line access from the pulp chamber to the cervical portion of the fragment could lead to a root perforation. The broken instruments were classified according to the fragment length and the fragment location in the root.
• The fragment length: the subcategories were short (shorter than 3 mm), medium (3 to 4.5 mm), and long (larger than 4.5 mm) (Figure 1A-1C).
• The fragment location: The cervical, middle, and apical thirds were considered, according to the location of the top coronal part of the fragment (Figure 1D-1F).
Figure 1
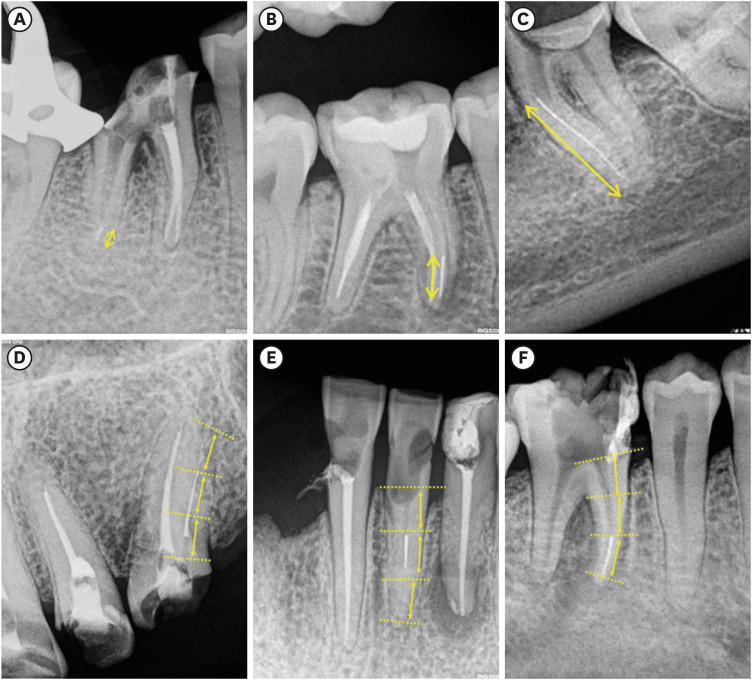
Upper row, fragments length: (A) short, 1.5 mm3; (B) medium, 3.5 mm; (C) long, 11 mm. Lower row, location of the fragment by thirds: (D) cervical; (E) middle; (F) apical.
All the patients were treated by the same operator, with technical resources available in the university clinic, such as specific ultrasonic tips (E18, E5 Helse Ultrasonic, Brazil; E6, E7 Guilin Woodpecker Med Co., Guilin, China), micro-tweezers (Zumax Medical Co., Suzhou, China), loops system (BTR pen, Cerkamed, Stalowa Wola, Poland), and handmade tube systems (Figure 2). Once the removal procedure was performed, all the groups were related according to the following variables:
• Removal success rate.
• Time required from the tooth isolation and the removal of the dental filling until the fragment extraction or the cancellation of the removal attempt.
• Occurrence of a secondary fracture of the fragment to be retrieved.
Figure 2
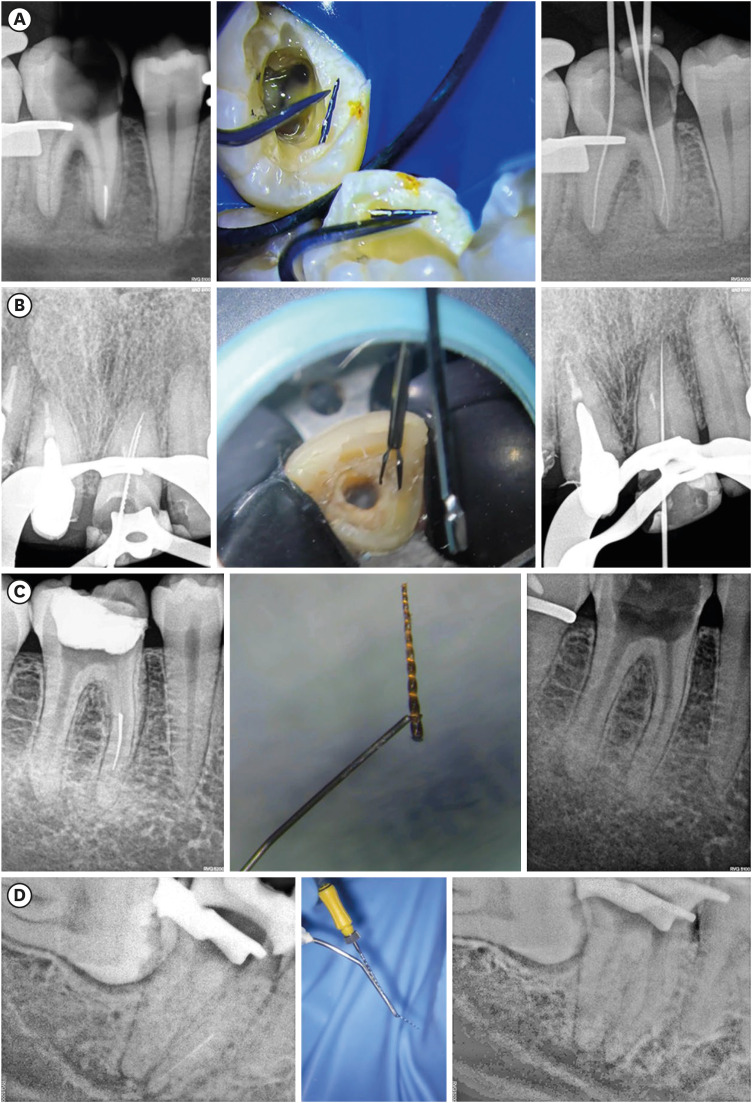
Removal system of fragments. (A) Ultrasonic tips; (B) micro-tweezer; (C) loop; (D) tube system.
The information was collected in spreadsheets. The 2 independent variables (length and location of the fragment) were analyzed separately from the dependent variables (success rate, working time and occurrence of secondary fracture). The statistical software R-medic was used [24]. The statistical assessment was analyzed using the Kruskal-Wallis test on the basis of a p < 0.05 significance level.
RESULTS
In this study, the cases of patients who presented with fractured instruments during the 2023 academic year in the Endodontic Program at the Faculty of Dentistry, University of Buenos Aires, were analyzed, and out of the 60 fragments intended for removal, 59 were successfully retrieved. In 3 of the cases, secondary fractures were reported. In one of them, the attempt to remove was abandoned as the reduced fragment did not allow access without a risk of perforation. The removal system used in each case can be seen in Table 1. The fragment location in the cervical, middle, or apical thirds was a significant influence on the retrieval time as the statistics show. Less removal time was required for those fragments accessible in the root canal cervical third (Figure 3, Table 2). Regarding the fragment length and the time required, the results did not show statistically significant differences with any of the assessed variables (Figure 4, Table 3). Regarding the success rate and the secondary fractures, none of the studied groups showed significant differences.
Table 1
Retrieval technique used
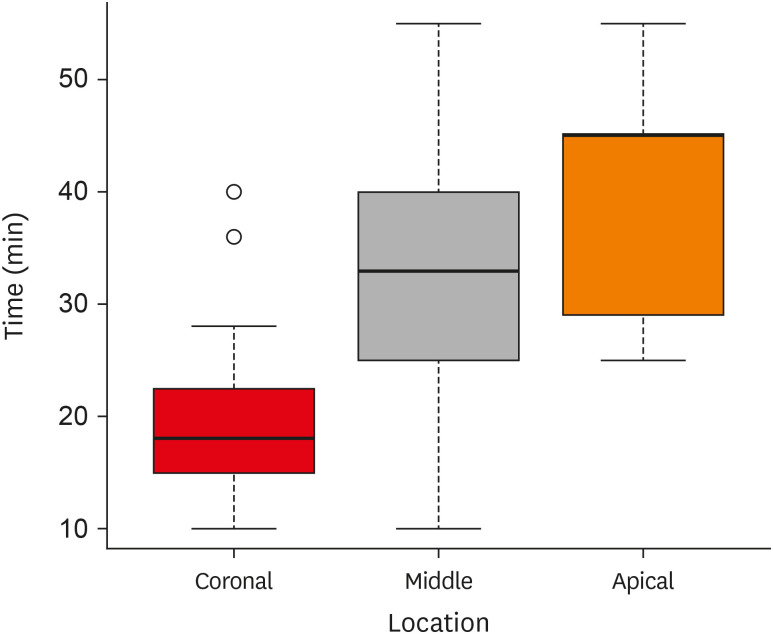
Table 2
Time in minutes required to retrieve broken files according to location
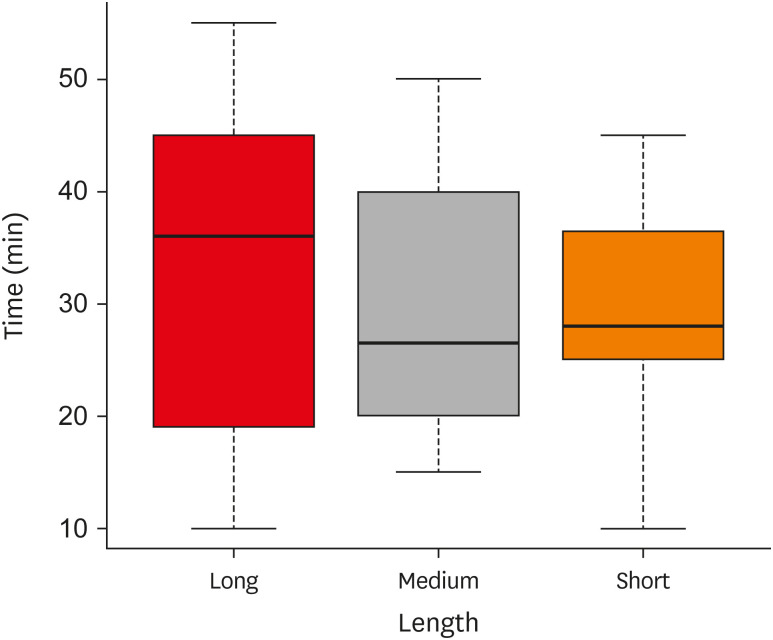
Table 3
Time in minutes required to retrieve broken files according to length
| Length of the fragment | Minimum | Mean | Median | Maximum | Standard deviation | No. |
|---|---|---|---|---|---|---|
| Long | 10.00 | 33.52 | 36.00 | 55.00 | 14.20 | 27 |
| Medium | 15.00 | 29.21 | 26.50 | 50.00 | 11.54 | 14 |
| Short | 10.00 | 29.42 | 28.00 | 45.00 | 9.95 | 19 |
DISCUSSION
The removal of a fractured instrument fragment in the root canal involves different degree variables of complication, making the prediction of the outcome difficult. These difficulties determine the clinical decision-making and occasionally lead to dismissing the attempt [1,21]. Therefore, the search for more and better tools to improve the procedure predictability could be very helpful to the endodontic community. In this work, the release of the fragment began with the use of ultrasonic tips. When the fragment was short, this action was sufficient to detach it and let it flow with irrigation. However, when the fragment was long, the space created with the ultrasonic tips was used to capture the fragment with systems such as tubes, loops, or micro-tweezers. Additionally, when the mechanical retention was very high, tube systems were selected; for intermediate retention, loop systems were used; and in cases of minimal retention, micro-tweezers were employed.
The original protocols previously published by Madarati et al. [2] and Parashos and Messer [3] suggested avoiding removal attempts when the intracanal fragment is located in the apical third. However, in this study, the apical location of the fractured files showed no influence on the procedure success rate, although the removal time required was increased. This may be due to better visualization and handling of the fragment when it is closer to the dental pulp chamber.
Clinical cases were classified based on the cervical position of the fragment. Therefore, when the fragment was long, occupying the entire canal, and accessible in the cervical third, it was considered to be in a cervical location. This factor can explain why the time required varied greatly among different clinical cases. Regarding the length of the fragment, Terauchi claims that those longer require more removal time [4]. Furthermore, in the present study, no differences were observed in the time required by short, medium, and long fragments. However, a wide data dispersion was observed for this variable. This suggests that the difficulty related to the length depends on other associated factors, such as the cause of the fracture. Moreover, in this study, when the short fragments were easily accessible, allowed a quick removal, because they were easily dragged by the irrigation turbulence along with the removed dentin released from the surroundings of the first threads. However, when they were located in the apical third, they exhibited a greater visualization and access difficulty, as well as a higher risk of perforation because of the diminished thickness of the surrounding dentin.
The literature mentions the different accidents that can occur because of the removal procedure of fractured fragments. In this study, the secondary fractures were only considered. The introduction of a variable such as the weakening of the root housing the fragment, that can later lead to a fracture, can be introduced in in vitro studies [18]. However, in this clinical study, the measurement of this factor is hindered by the lack of standardization of cases and the anatomic variables. On the other hand, certain treated teeth exhibited weakened roots before their inclusion in the protocol because of the removal attempts previously made by other dental care professionals. In the present research, the occurrence of secondary fractures increased the working time twice, with no effect on the final outcome. However, in another clinical case, it was necessary to stop the removal attempt because the access to the fragment might have led to a perforation.
Terauchi et al. [19] concluded that the long fragments have to be removed by means of retrieval systems and not only by using ultrasonic tips. Nevertheless, according to the experience of the current report, when the long fragment did not exhibit mechanical retention, it was easily retrieved with micro-tweezers, without exerting any force in the retrieval. But when there was mechanical locking, it became necessary to exert retrieving force, so the loop and tube devices appeared to be more effective.
CONCLUSIONS
Within the limitations of this clinical report, none of the assessed variables influenced either the success rate or the generation of secondary fractures. Moreover, the fractured fragment length did not influence any of the variables assessed. However, the location of the fragment influenced the removal time. For this reason, it is suggested to consider this parameter when making the decision to remove a fractured file.
-
Conflict of Interest: No potential conflict of interest relevant to this article was reported.
-
Author Contributions:
Conceptualization: Portigliatti R.
Data curation: Portigliatti R.
Formal analysis: Portigliatti R.
Investigation: Portigliatti R, Consoli Lizzi EP, Rodríguez PA.
Methodology: Portigliatti R.
Project administration: Rodríguez PA.
Resources: Portigliatti R.
Software: Portigliatti R.
Supervision: Portigliatti R.
Validation: Portigliatti R.
Visualization: Portigliatti R.
Writing - original draft: Portigliatti R, Consoli Lizzi EP, Rodríguez PA.
Writing - review & editing: Portigliatti R, Consoli Lizzi EP, Rodríguez PA.
- 1. Nevares G, Cunha RS, Zuolo ML, Bueno CE. Success rates for removing or bypassing fractured instruments: a prospective clinical study. J Endod 2012;38:442-444.ArticlePubMed
- 2. Madarati AA, Hunter MJ, Dummer PMH. Management of intracanal separated instruments. J Endod 2013;39:569-581.ArticlePubMed
- 3. Parashos P, Messer HH. Rotary NiTi instrument fracture and its consequences. J Endod 2006;32:1031-1043.ArticlePubMed
- 4. Terauchi Y, Ali WT, Abielhassan MM. Present status and future directions: Removal of fractured instruments. Int Endod J 2022;55(Supplement 3):685-709.ArticlePDF
- 5. Mishra L, Kim HC, Singh NR, Rath PP. The top 10 most-cited articles on the management of fractured instruments: a bibliometric analysis. Restor Dent Endod 2018;44:e2.ArticlePubMedPMCPDF
- 6. Eskibağlar M, Özata MY, Ocak MS, Öztekin F. Investigation of fracture prevalence of instruments used in root canal treatments at a faculty of dentistry: a prospective study. Restor Dent Endod 2023;48:e38.PubMedPMC
- 7. Setzer FC, Böhme CP. Influence of combined cyclic fatigue and torsional stress on the fracture point of nickel-titanium rotary instruments. J Endod 2013;39:133-137.ArticlePubMed
- 8. Alcalde MP, Tanomaru-Filho M, Bramante CM, Duarte MAH, Guerreiro-Tanomaru JM, Camilo-Pinto J, et al. Cyclic and torsional fatigue resistance of reciprocating single files manufactured by different nickel-titanium alloys. J Endod 2017;43:1186-1191.ArticlePubMed
- 9. Ferreira F, Adeodato C, Barbosa I, Aboud L, Scelza P, Zaccaro Scelza M. Movement kinematics and cyclic fatigue of NiTi rotary instruments: a systematic review. Int Endod J 2017;50:143-152.ArticlePubMedPDF
- 10. Mena-Álvarez J, Almanzor-López M, Quispe-López N, De Pedro-Muñoz A, Rico-Romano C. Analysis of the importance of the motion used in the resistance of different mechanical instrumentation systems in endodontics: a comparative study. Materials (Basel) 2022;15:4443.ArticlePubMedPMC
- 11. Thu M, Ebihara A, Maki K, Miki N, Okiji T. Cyclic fatigue resistance of rotary and reciprocating nickel-titanium instruments subjected to static and dynamic tests. J Endod 2020;46:1752-1757.ArticlePubMed
- 12. Alghamdi S, Huang X, Haapasalo M, Mobuchon C, Hieawy A, Hu J, et al. Effect of curvature location on fatigue resistance of five nickel-titanium files determined at body temperature. J Endod 2020;46:1682-1688.ArticlePubMed
- 13. Silva EJNL, Vieira VTL, Hecksher F, Dos Santos Oliveira MRS, Dos Santos Antunes H, Moreira EJL. Cyclic fatigue using severely curved canals and torsional resistance of thermally treated reciprocating instruments. Clin Oral Investig 2018;22:2633-2638.ArticlePubMedPDF
- 14. Pedullà E, Kharouf N, Caruso S, La Rosa GRM, Jmal H, Haikel Y, et al. Torsional, static, and dynamic cyclic fatigue resistance of reciprocating and continuous rotating nickel-titanium instruments. J Endod 2022;48:1421-1427.ArticlePubMed
- 15. Ninan E, Berzins DW. Torsion and bending properties of shape memory and superelastic nickel-titanium rotary instruments. J Endod 2013;39:101-104.ArticlePubMed
- 16. Xu X, Eng M, Zheng Y, Eng D. Comparative study of torsional and bending properties for six models of nickel-titanium root canal instruments with different cross-sections. J Endod 2006;32:372-375.ArticlePubMed
- 17. Silva E, Oliveira de Lima C, Vieira V, Antunes H, Lima Moreira EJ, Versiani M. Cyclic fatigue and torsional resistance of four martensite-based nickel titanium reciprocating instruments. Eur Endod J 2020;5:231-235.ArticlePubMedPMCPDF
- 18. Fu M, Huang X, Zhang K, Hou B. Effects of ultrasonic removal of fractured files from the middle third of root canals on the resistance to vertical root fracture. J Endod 2019;45:1365-1370.ArticlePubMed
- 19. Terauchi Y, Sexton C, Bakland LK, Bogen G. Factors affecting the removal time of separated instruments. J Endod 2021;47:1245-1252.ArticlePubMed
- 20. Pruthi PJ, Nawal RR, Talwar S, Verma M. Comparative evaluation of the effectiveness of ultrasonic tips versus the Terauchi file retrieval kit for the removal of separated endodontic instruments. Restor Dent Endod 2020;45:e14.ArticlePubMedPMCPDF
- 21. Yang Q, Shen Y, Huang D, Zhou X, Gao Y, Haapasalo M. Evaluation of two trephine techniques for removal of fractured rotary nickel-titanium instruments from root canals. J Endod 2017;43:116-120.ArticlePubMed
- 22. Terauchi Y, O’Leary L, Yoshioka T, Suda H. Comparison of the time required to create secondary fracture of separated file fragments by using ultrasonic vibration under various canal conditions. J Endod 2013;39:1300-1305.ArticlePubMed
- 23. Arslan H, Doğanay Yıldız E, Taş G, Akbıyık N, Topçuoğlu HS. Duration of ultrasonic activation causing secondary fractures during the removal of the separated instruments with different tapers. Clin Oral Investig 2020;24:351-355.ArticlePubMedPDF
- 24. Mangeaud A, Elías Panigo DH. R-Medic. A simple and intuitive statistical analysis software. Rev Methodo 2018;3:18-22.ArticlePDF
REFERENCES
Tables & Figures
REFERENCES
Citations
Citations to this article as recorded by 
- A Study of Adverse Events Associated with Endodontic Files Utilizing the Manufacturer and User Facility Device Experience (MAUDE) Database
Luaibi S, Timban SA, Boopalan K, Nalliah RP
Journal of Dental Health and Oral Research.2026; 7(1): 1. CrossRef - Efficiency of ultrasonic retrieval for separated instruments within the middle third of root canals using modified staging platform: a comparative in-vitro study
Basim Samir Mohamed, Nihal Ezzat Sabet, Dina Ahmed Morsy
BMC Oral Health.2026;[Epub] CrossRef - Influence of the Cause of File Fracture on the Successful Removal of Fragments from Root Canals: An In Vivo Study
Ricardo Portigliatti, Eugenia Pilar Consoli Lizzi, Pablo Alejandro Rodríguez
Applied Sciences.2026; 16(8): 3832. CrossRef - Fractured instruments in endodontics: understanding incidence, mechanisms, and emerging retrieval techniques
Ali Robaian AlQahtani
Libyan Journal of Medicine.2026;[Epub] CrossRef - Neodymium-Doped Yttrium Aluminum Perovskite (Nd:YAP) Laser in the Elimination of Endodontic Nickel-Titanium Files Fractured in Rooted Canals (Part 2: Teeth With Significant Root Curvature)
Amaury Namour, Marwan El Mobadder, Clément Cerfontaine, Patrick Matamba, Lucia Misoaga, Delphine Magnin , Praveen Arany, Samir Nammour
Cureus.2025;[Epub] CrossRef
 ePub Link
ePub Link Cite
CitePredictive factors in the retrieval of endodontic instruments: the relationship between the fragment length and location
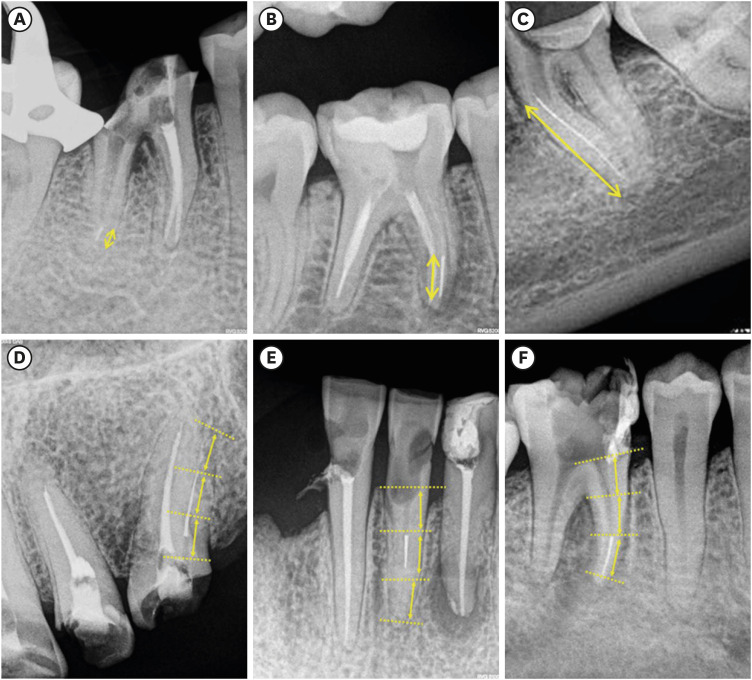
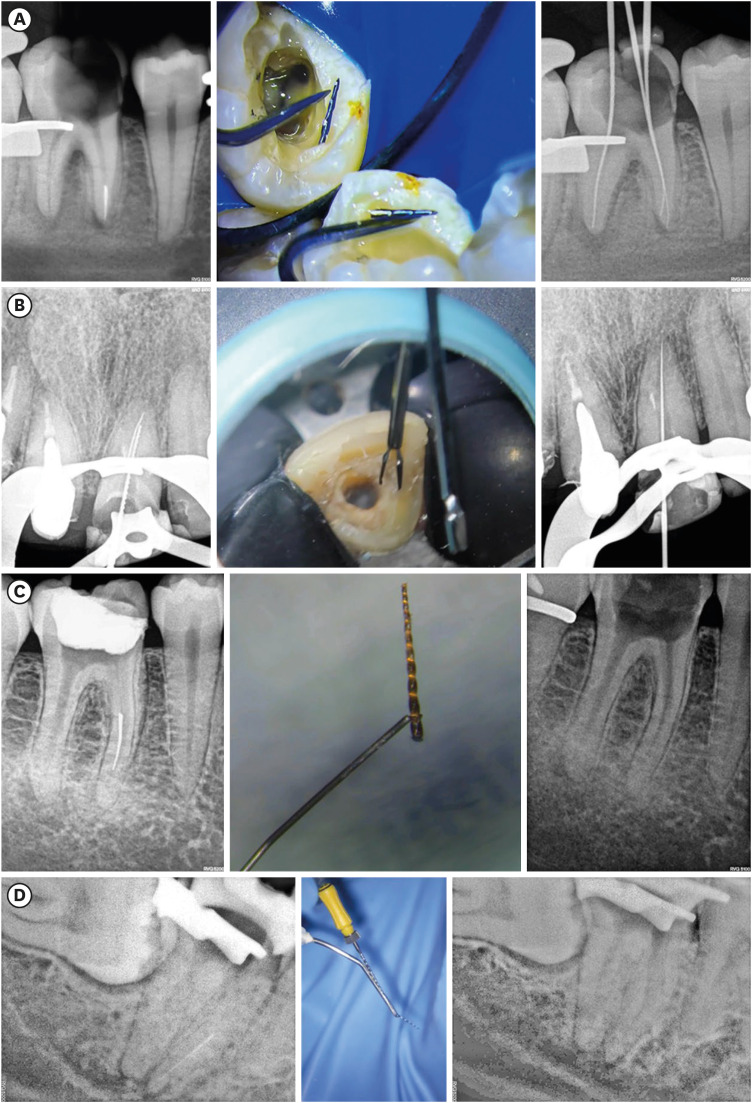
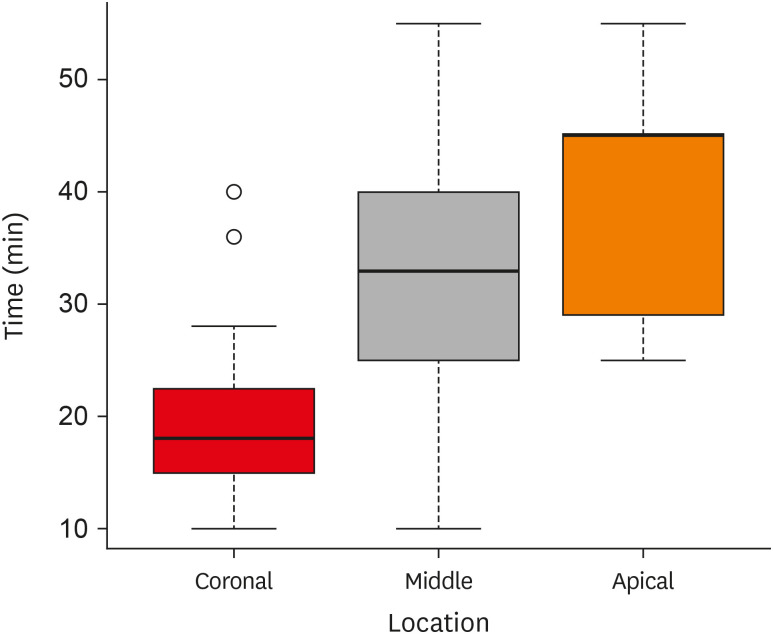
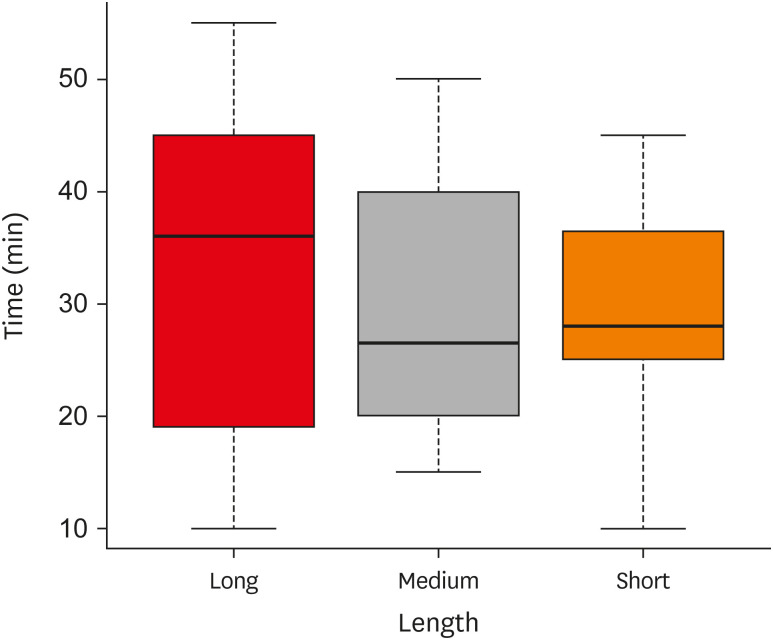
Figure 1 Upper row, fragments length: (A) short, 1.5 mm3; (B) medium, 3.5 mm; (C) long, 11 mm. Lower row, location of the fragment by thirds: (D) cervical; (E) middle; (F) apical.
Figure 2 Removal system of fragments. (A) Ultrasonic tips; (B) micro-tweezer; (C) loop; (D) tube system.
Figure 3 Box plot relating the location of the fragment and the removal time.
Figure 4 Box plot relating the length of the fragment and the removal time.
Figure 1
Figure 2
Figure 3
Figure 4
Predictive factors in the retrieval of endodontic instruments: the relationship between the fragment length and location
Retrieval technique used
| Technique | Location | Length | No. | ||||
|---|---|---|---|---|---|---|---|
| Coronal | Medium | Apical | Long | Medium | Short | ||
| US tips | 7 | 15 | 9 | 5 | 11 | 16 | 31 |
| Tubes | 3 | 14 | 1 | 13 | 2 | 3 | 18 |
| Loops | 4 | 3 | 0 | 6 | 1 | 0 | 7 |
| Micro-tweezers | 1 | 2 | 0 | 3 | 0 | 0 | 3 |
| Attempt abandoned | 0 | 0 | 1 | 0 | 1 | 0 | 1 |
| Total | 15 | 34 | 11 | 27 | 15 | 19 | 60 |
Time in minutes required to retrieve broken files according to location
| Location of the fragment | Minimum | Mean | Median | Maximum | Standard deviation | No. |
|---|---|---|---|---|---|---|
| Coronal third | 10.00 | 20.20 | 18.00 | 40.00 | 8.48 | 15 |
| Middle third | 10.00 | 33.38 | 33.00 | 55.00 | 11.21 | 34 |
| Apical third | 25.00 | 39.55 | 45.00 | 55.00 | 10.59 | 11 |
Time in minutes required to retrieve broken files according to length
| Length of the fragment | Minimum | Mean | Median | Maximum | Standard deviation | No. |
|---|---|---|---|---|---|---|
| Long | 10.00 | 33.52 | 36.00 | 55.00 | 14.20 | 27 |
| Medium | 15.00 | 29.21 | 26.50 | 50.00 | 11.54 | 14 |
| Short | 10.00 | 29.42 | 28.00 | 45.00 | 9.95 | 19 |
Table 1 Retrieval technique used
Table 2 Time in minutes required to retrieve broken files according to location
Table 3 Time in minutes required to retrieve broken files according to length

