
Articles
- Page Path
- HOME > Restor Dent Endod > Volume 47(3); 2022 > Article
- Research Article Association between cigarette smoking and the prevalence of post-endodontic periapical pathology: a systematic review and meta-analysis
-
Néstor Ríos-Osorio1
 , Hernan Darío Muñoz-Alvear2, Fabio Andrés Jiménez-Castellanos3, Sara Quijano-Guauque1, Oscar Jiménez-Peña1, Herney Andrés García-Perdomo4, Javier Caviedes-Bucheli5
, Hernan Darío Muñoz-Alvear2, Fabio Andrés Jiménez-Castellanos3, Sara Quijano-Guauque1, Oscar Jiménez-Peña1, Herney Andrés García-Perdomo4, Javier Caviedes-Bucheli5 -
Restor Dent Endod 2022;47(3):e27.
DOI: https://doi.org/10.5395/rde.2022.47.e27
Published online: June 13, 2022
1Research Department COC-CICO, Institución Universitaria Colegios de Colombia UNICOC, Bogotá, Colombia.
2Department of Endodontics Universidad cooperativa de Colombia, Bogotá, Colombia.
3Department of Periodontics, Universidad Antonio Nariño, Bogotá, Colombia.
4Department of Surgery and Urology, School of Medicine Universidad del Valle, Cali, Colombia.
5Centro de Investigaciones Odontologicas, Pontificia Universidad Javeriana, Bogota, Colombia.
- Correspondence to Néstor Ríos-Osorio, DDS, MSc. Associate Professor, Research Department COC-CICO, Institución Universitaria Colegios de Colombia UNICOC, Km 20, Autonorte I-55, Chía, Cundinamarca, Bogotá, Colombia. dadopi1981@gmail.com
• Received: September 7, 2021 • Revised: November 7, 2021 • Accepted: November 12, 2021
Copyright © 2022. The Korean Academy of Conservative Dentistry
This is an Open Access article distributed under the terms of the Creative Commons Attribution Non-Commercial License (https://creativecommons.org/licenses/by-nc/4.0/) which permits unrestricted non-commercial use, distribution, and reproduction in any medium, provided the original work is properly cited.
Abstract
-
Objectives This systematic review and meta-analysis aimed to assess the association of cigarette smoking with the prevalence of post-endodontic apical periodontitis in humans.
-
Materials and Methods We searched through PubMed/Medline, Web of Science, and Scopus from inception to December 2020. Risk of bias was performed by using the Newcastle-Ottawa Scale for cross-sectional, cohort, and case-control studies. We performed the statistical analysis in Review Manager 5.3 (RevMan 5.3).
-
Results 6 studies met the inclusion criteria for qualitative and quantitative synthesis. Statistical analysis of these studies suggests that there were no differences in the prevalence of post endodontic apical periodontitis (AP) when comparing non-smokers vs smoker subjects regarding patients (odds ratio [OR], 0.68; 95% confidence interval [CI], 0.31–1.49; I2 = 58%) and teeth (OR, 1.71; 95% CI, 0.99–2.93; I2 = 72%).
-
Conclusions Our findings suggest that there was no association between cigarette smoking and post-endodontic apical periodontitis, as we did not find statistical differences in the prevalence of post-endodontic AP when comparing non-smokers vs smoker subjects. Therefore, smoking should not be considered a risk factor associated with endodontic failure.
INTRODUCTION
Around 16 million people in the world experience serious health problems related to the habit of cigarette smoking (CS). CS causes approximately 7 million global deaths annually, and it is expected that by 2030 tobacco consumption will cause mortality of 10 million people per year [1,2]. Smokers are more likely to develop cerebrovascular diseases, chronic obstructive pulmonary disease, bronchitis, pneumonia, tachycardia, arterial hypertension, and type 2 diabetes mellitus, as well as neurological degenerations such as depression and cognitive impairment [3]. Furthermore, CS is known to cause deleterious effects on the immune system. Impaired immune reactions related to phagocytosis, neutrophil diapedesis and chemotaxis, in addition to high systemic concentrations of free radical and pro-inflammatory cytokines are directly linked to the release of chemical compounds during tobacco combustion, including nicotine, carbon monoxide, nitrosamine, oxidation radicals, and hydrogen cyanide among others [4,5,6,7].
Likewise, CS has deleterious effects on local and systemic blood flow, as it causes vascular dysfunction given the modification of the osmotic pressure. Moreover, some chemical compounds of cigarettes such as nicotine induce vasoconstriction, thus restricting the supply of nutrients to tissues and preventing cell proliferation and tissue repair, consequently leading to a progressive tissue breakdown [8,9,10]. Notably, both the immune and vascular systems are key components of all tissue remodeling and healing processes [9].
Endodontic disease manifests both, at pulpal and periapical levels. Pulp and periapical reactions to noxious stimuli are characterized by an initial neurogenic inflammatory response, as the nervous system governs the vascular system by the release of potent vasoactive neuropeptides which act directly on the endothelial and smooth muscle cells, thus affecting the vascular permeability, and exerting pro-inflammatory and immune reactions at the site of the injury [11]. Such inflammatory responses depend on the course, the nature and magnitude of the causal agent, and the ability of the tissue to respond and recover from the noxious stimuli [12].
Several authors have suggested that once the bacterial infection reaches the periapical tissues, smokers are less likely to limit and repair the periapical osteolytic lesion due to the elevated expression of inflammatory mediators, such as tumor necrosis factor-alpha (TNF-α), interleukin 6 (IL-6), C-reactive protein and other substances associated to bone destruction such as reactive oxygen species, collagenase, and serine proteases in addition to elevated levels of carboxyhemoglobin in the blood, which in turn decreases tissue oxygenation and compromise the tissue healing capability in comparison to non-smokers [12,13,14,15,16]. CS has also been associated with endothelial cell injury and impaired microvascular function [14]. Furthermore, 2 recent systematic reviews evaluated the prevalence of periapical lesions of endodontic origin in endodontically untreated teeth in non-smokers vs smoker patients. These studies concluded that smoker patients are more likely to present apical periodontitis (AP) than non-smokers [17,18]. However, much is still not known about the impact of CS on the post-endodontic healing capacity of periapical tissues. Therefore, this systematic review aimed to assess the association of CS with the prevalence of post-endodontic AP in humans.
MATERIALS AND METHODS
This systematic review of the literature was developed following the recommendations of the Cochrane Collaboration and following the PRISMA statement [19].
Using the PICO strategy, the focused question and the inclusion criteria were framed:
Population: CS patients.
Intervention: History of conventional root canal treatment (RCT).
Comparison: Non-CS patients.
Outcome: Prevalence of post-endodontic apical periodontitis.
In CS patients with a history of conventional RCT, what is the effect of CS on the prevalence of post endodontic AP in comparison with non-smoker patients?
The inclusion criteria were observational studies, reporting the association between CS with the prevalence of post-endodontic AP in smokers vs non-smoker patients. Studies that did not define the evaluation method, in vitro or animal studies, narrative reviews, case reports, and expert opinions were excluded.
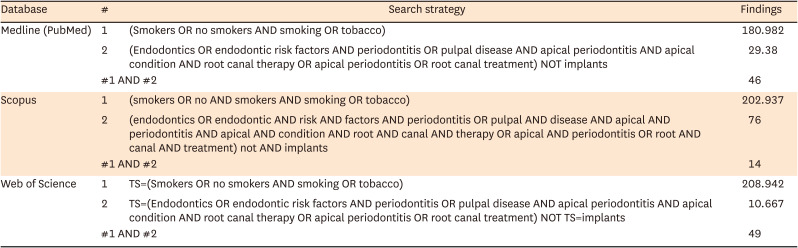
The literature search was conducted following the recommendations of the Cochrane Collaboration. Medical subject headings (MeSH), Emtree language, Descriptors in health sciences (DeCS), and text words related to a complete search strategy were used. Medline (PubMed), Web of Science, and Scopus were searched from inception to December 2020. The search strategy was translated for each database, several keywords were used for each one of the elements of interest and we used the following keyword combinations: 1 AND 2 to report the final results from each database (Appendix 1):
Medline (PubMed) using MeSH terms:
1. (Smokers OR no smokers AND smoking OR tobacco)
2. (Endodontics OR endodontic risk factors AND periodontitis OR pulpal disease AND apical periodontitis AND apical condition AND root canal therapy OR apical periodontitis OR root canal treatment) NOT implants
Scopus using Key word plus:
1. (smokers OR no AND smokers AND smoking OR tobacco)
2. (endodontics OR endodontic AND risk AND factors AND periodontitis OR pulpal AND disease AND apical AND periodontitis AND apical AND condition AND root AND canal AND therapy OR apical AND periodontitis OR root AND canal AND treatment) not AND implants
Web of Science using Key words:
1. TS=(Smokers OR no smokers AND smoking OR tobacco)
2. TS=(Endodontics OR endodontic risk factors AND periodontitis OR pulpal disease AND apical periodontitis AND apical condition AND root canal therapy OR apical periodontitis
To ensure literature saturation, references from relevant articles identified through the search, conferences, thesis databases, Open Grey, Google Scholar, and ClinicalTrials.gov were scanned, among others. There was no language limitation.
Two researchers (HM, NR) initially reviewed the titles and abstracts. Then they reviewed the full texts to apply the pre-specified inclusion and exclusion criteria. Disagreements were resolved by consensus and where disagreement could not be solved, a third reviewer decided. Relevant data were collected in duplicate by using a standardized data extraction sheet that contained the following information: author names, year of publication, title, study design, geographic location, objectives, inclusion and exclusion criteria, number of patients included, losses to follow- up, timing, the definition of outcomes, outcomes, association measures, and funding source.
The assessment of the risk of bias was performed independently by 2 evaluators (OJ, NR) by using the Newcastle-Ottawa Scale for cross-sectional, cohort, and case-control studies [20].
We performed the statistical analysis in Review Manager 5.3 (RevMan 5.3). We reported the information about categorical variables on odds ratio (OR) with 95% confidence intervals (Cis). We also pooled the information with a random effect meta-analysis according to the heterogeneity expected. Heterogeneity was evaluated using the I2 test. For the interpretation, values of < 50%, and >50% correspond to low, and high levels of heterogeneity, respectively.
There was not enough data to perform this analysis.
We performed sensitivity analysis extracting weighted studies and running the estimated effect to find differences.
We did not perform a subgroup analysis since we did not have enough data.
RESULTS
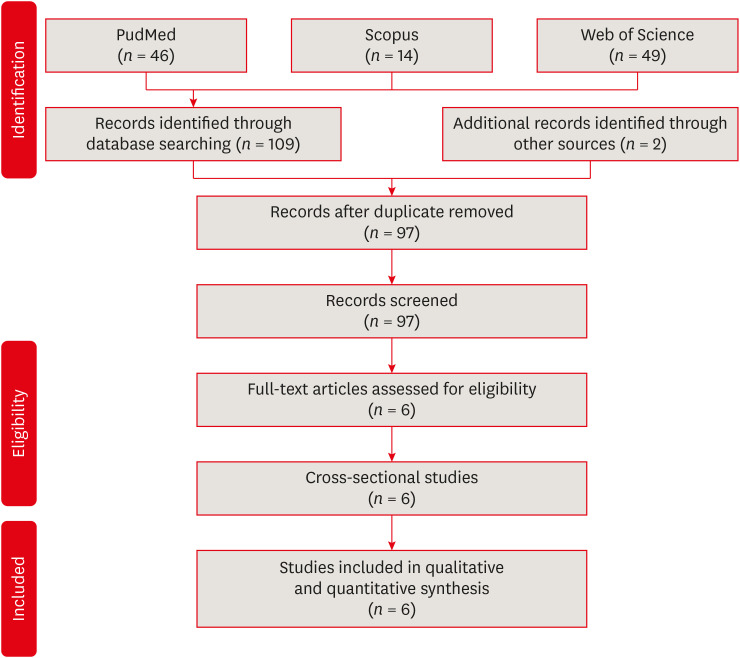
We initially identified 111 references with the search strategy. After the removal of 14 duplicates, we screened 97 titles/abstracts. Finally, 6 studies met the inclusion criteria for qualitative and quantitative synthesis (Figure 1).
All 6 studies were cross-sectional, published from 2004 to 2020 [21,22,23,24,25,26]. The studies compared the post endodontic prevalence of AP in smokers vs non-smokers. The studies were conducted in Croatia, Saudi Arabia, Spain, and Poland. The average group of participants in the studies included individuals between 18 and 65 years. Analysis of these 6 studies shows that the prevalence of post endodontic AP is similar between smokers and non-smokers subjects (Table 1).
Table 1
Characteristics of studies assessing the post endodontic prevalence of AP in smokers vs non-smokers patient
| Article | Author, year, country | Sample (n) | Age | Sample characteristics (smoker and/or non-smoker) | Teeth (n) (smoker and/or non-smoker) | Periapical diagnosis | PAI | Main results | Statistical analysis | Confidence level | Conclusion |
|---|---|---|---|---|---|---|---|---|---|---|---|
| 1 | Bergström et al. [21], 2004, Sweden | Subjects n = 247, male (n = 213), female (n = 34) | 20–65 | Current smokers (n = 81), former smokers (n = 63), non-smokers (n = 103) | On average for the total sample: 38.7 out of a maximum of 42 dental roots per person (i.e. 92%) were available for assessment. | Periapical radiographs | No | The mean numbers of periapical lesions per person related to endodontically treated teeth for current smokers: n = 0.86 mean; 95% CI, 0.5–1.2. Former smokers: n = 0.53 mean; 95% CI, 0.3–0.8. Non-smokers: n = 0.68 mean; 95% CI, 0.4–0.9. Total: n = 0.30 mean; 95% CI, 0.5–0.8. The smoking prevalence of individuals exhibiting one or more teeth with a periapical lesion: current smokers (56%), former smokers (57%), and non-smokers (46%) (p > 0.05). The prevalence of periapical lesions among individuals with RCT: current smokers (69%), former-smokers (74%), and non-smokers (85%) (p > 0.05). | Kolmogorov–Smirnov test, Kruskal–Wallis non-parametric ANOVA, two-factor ANOVA, and Scheffé post hoc multiple comparisons test | p < 0.05 | It is concluded that these observations do not support the assumption that smoking is associated with apical periodontitis. Moreover, there was no statistically difference (p > 0.05) in terms of root-filled teeth with AP when comparing smokers vs non-smokers. |
| 2 | Segura-egea et al. [22], 2008, Spain | Subjects n = 180, male (n = 66, 36.7%), female (n = 114, 63.3%) | 37.1 ± 15.7 | Current smokers (n = 109, 61%) and non-smokers (n = 71, 39%) | Total number of teeth examined in smokers was 2,722 and 1,731 teeth in non-smokers. The average number of teeth per patient: smokers (n = 25.0 ± 3.8), non-smoker (n = 24.4 ± 4.5) (p > 0.05). | Periapical radiographs | Yes | AP in one or more teeth in smokers (n = 81, 74%) and non-smokers (n = 29, 41%) (p < 0.01; OR, 4.2; 95% CI, 2.2–7.9). Among smokers, 45 root-filled teeth had AP, whereas in non-smokers 15 (OR non-smokers = 1.0, OR smokers = 1.5, p > 0.05). | Cohen’s Kappa test, ANOVA and logistic regression | p < 0.05 | Smoking was significantly associated with a higher frequency and prevalence of root canal treatment and apical periodontitis. However, there was no statistically difference (p > 0.05) in terms of root-filled teeth with AP when comparing smokers vs non-smokers. |
| 3 | Sopińska and Bołtacz-Rzepkowska [23], 2020, Poland | Subjects n = 703, male (n = 277, 39.4%), female (n = 426, 60.6%) | 18–91 | Non-smokers (n = 317), smokers (n = 386) | Total number of teeth examined in smokers was 8,726 and 7,487 teeth in non-smokers. | Panoramic radiographs | No | Smokers presented a higher prevalence of teeth with AP than non-smokers (7.2% and 5.2% respectively, p < 0.0005). Among smokers, 352 root-filled teeth had AP, whereas in non-smokers 257 (χ2 test p = 0.451; Mantel-Haenszel test 0.760; common OR estimate 0.963; 95% CI, 0.783–1.184). | χ2 and the Mantel-Haenszel test | p > 0.05 | Smokers are a group facing an increased risk of AP. However, no difference was observed in the frequency of AP in the endodontically treated teeth in both groups (37.6% vs 35.8%) (p = 0.451). |
| 4 | Bahammam [24], 2012, Saudi Arabia | Subjects n = 98 male individuals | 20–60 | Non-smokers (n = 78), smokers (n = 20) | The average number of teeth per patient was 24.65 ± 3.28 and 24.58 ± 4.41 in smokers and non-smokes, respectively (p = 0.953). | Periapical radiographs | No | The prevalence of patients with AP was 8.59% in smoker and 6.18% in non-smokers. The frequency of patients having AP with RCT in smoker and in non-smokers was 5.73% and 5.12%, respectively (p = 0.195). | t-test | p < 0.05 | Results from this study do not favor the assumption that smoking is associated with AP. Likewise, there was no statistically difference (p > 0.05) in terms of root-filled teeth with AP when comparing smokers vs non-smokers. |
| 5 | Peršić Bukmir et al. [25], 2015, Croatia | Subjects n = 259, 82 male subjects (31.7%) and 177 female subjects (68.3%). | 40.3 ± 15.1 | Non-smokers (n = 151), smokers (n = 108) | The average number of teeth per patient was 22.9 ± 5.2 and 23.2 ± 4.9 in smokers and non-smokes, respectively (p = 0.636). | Panoramic radiographs and Periapical radiographs | Yes | Smokers had higher prevalence of teeth with AP than non-smokers (0.13 vs 0.10; p = 0.025). Among smokers, 67 patients (72.0%) had AP affecting at least one treated tooth, whereas in non-smokers, 93 patients (78.8%) had AP affecting at least one treated tooth (p = 0.328). Likewise, fractions of endodontically treated teeth with AP did not differ significantly between smokers vs non-smokers (mean, 0.06; SD, 0.07; 95% CI, 0.05–0.07; p = 0.832). | Kolmogorov–Smirnov test, t-test and χ2 test | p < 0.05 | Smokers will on average have two teeth with AP more than non-smokers, thus supporting the hypothesis that smoking influences the periapical status of teeth. However, no difference was observed in the prevalence of AP in the endodontically treated teeth when comparing smokers vs non-smokers (72.0% and 78.8% respectively) (p = 0.328). |
| 6 | Segura-egea et al. [26], 2011, Spain | Subjects n = 100, men (n = 53, 53%) women (n = 47, 47%) | 58.7 ± 9.6 | 50 smokers and 50 non-smokers | Total number of teeth examined in smokers was 1,039 and 1,124 teeth in non-smokers. The average number of teeth per patient: smokers (n = 20.8 ± 4.0), non-smokers (n = 22.3 ± 4.3) (p > 0.05). | Periapical radiographs | Yes | AP in one or more teeth in smokers (n = 46, 92%) and non-smokers (n = 22, 44%) (p < 0.01; OR, 14.6; 95% CI: 4.6–46.9). Among smokers, 24 root-filled teeth had AP whereas in non-smokers, 9 root-filled teeth exhibited AP (p > 0.05). | Student t-test, logistic regression and χ2 test | p < 0.05 | The prevalence of apical periodontitis and root canal treatment was significantly higher in hypertensive smoking patients compared to non-smokers. However, there was no statistically difference (p > 0.05) in terms of root-filled teeth with AP when comparing smokers vs non-smokers. |
Most of the studies had a high risk of bias (66.6%) because they obtained less than 7 points out of 10 possible in the global rating [21,22,24,26].
From the evaluation by categories, it can be observed that all the studies included in this systematic review and meta-analysis presented a high risk of bias in the item “selection” since the 6 studies obtained 2 or fewer points out of 5 possible, mainly due to the fact that none of the studies adequately reported on how the calculation to determine the sample size was performed. Furthermore, the determination of the exposure of the subjects to the risk factor was not standardized. On the other hand, only 2 studies used a representative sample of the population through random sampling [24,25]; and only 2 studies reported on the characteristics of the excluded or not studied subjects [23,25].
In contrast, in the item “comparability “, most of the included studies were evaluated as having a low risk of bias, because they obtained 2 points out of 2 possible [21,22,23,25,26]. The study performed by Bahammam [24] did not obtain any points in this category, as it did not provide information on how the confounding factors were controlled. Finally, for the item “Outcome/Exposure “all studies [21,22,23,24,25,26], were rated as low risk of bias, since they obtained 2 or more points out of 3 possible for this category, mainly because they used objective validated evaluation methods and because they clearly described the statistical tests they used to analyze the data and the level of probability (p-value) (Table 2).
Table 2
Evaluation according to the Newcastle-Ottawa quality assessment scale
| Study | Selection | Comparability | Outcome | Conclusion | |
|---|---|---|---|---|---|
| Cross-sectional studies | |||||
| Bergström et al. [21], 2004 | - | ★★ | ★★★ | HIGH RISK | |
| Segura-Egea et al. [22], 2008 | - | ★★ | ★★★ | HIGH RISK | |
| Sopińska and Bołtacz-Rzepkowska [23], 2020 | ★★ | ★★ | ★★★ | LOW RISK | |
| Bahammam [24], 2012 | ★ | - | ★★★ | HIGH RISK | |
| Peršić Bukmir et al. [25], 2016 | ★★ | ★★ | ★★★ | LOW RISK | |
| Segura-Egea et al. [26], 2011 | - | ★★ | ★★★ | HIGH RISK | |
Regarding the information for patients, we included 3 studies [21,24,25] and found an OR of 0.68 95%CI (0.31 to 1.49) I2: 58%. There were no differences between smokers and no smokers in the apical periodontitis events (Figure 2). Likewise, for teeth, we included 3 studies [22,23,26] and found an OR of 1.71, 95% CI (0.99–2.93), and I2 = 72%. We did not find any differences (Figure 3). Nonetheless, there was high heterogeneity in the 2 analyses, making it difficult to interpret these results.
Figure 2
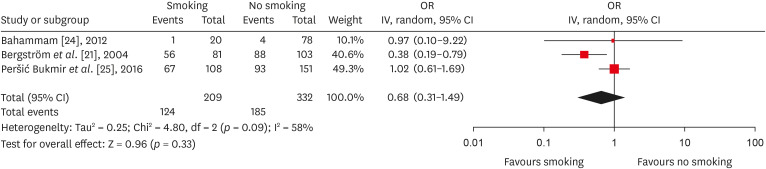
Forest plot of association between root canal treatment with apical periodontitis in smokers vs non-smokers subjects (analysis by patients).
OR, odds ratio; CI, Confidence interval.
Figure 3
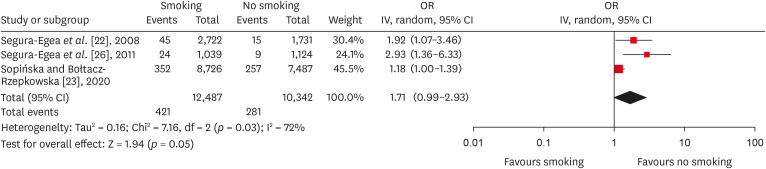
Forest plot of association between root canal treatment with apical periodontitis in smokers vs non-smokers subjects (analysis by teeth).
OR, odds ratio; CI, Confidence interval.
There were no changes in the estimated effect when performing the sensitivity analysis.
DISCUSSION
Evaluation of the 6 articles included in this systematic review suggests that apparently and under the limitations of this study, there were no statistical differences in the prevalence of post endodontic AP when comparing non-smokers vs smoker subjects regarding patients (OR, 0.68; 95% CI, 0.31–1.49; I2 = 58%) and teeth (OR, 1.71; 95% CI, 0.99–2.93; I2 = 72%).
The apical osteolytic lesion is the result of the dynamic encounter between bacteria and the immune system in an attempt of the host to prevent endodontic bacteria from spreading into the alveolar bone or even to distant organs. Bacteria emerging from the infected root canal provide a continuous stimulus for the recruitment of polymorphonuclear granulocyte neutrophils at the periapical level in order to contain and phagocytize such bacteria [27].
Chronic exposure to endodontic pathogenic bacteria or their sub-products may result in the local production by plasma cells of specific IgG to endodontic bacteria, which in turn will activate the complement system, thus amplifying the immune reaction [28,29]. However, this dynamic encounter between bacteria and the immune system also causes local bone damage in the form of an osteolytic lesion. During the apical inflammatory reaction, different cytokines such as IL-1β and TNF-β (which are the primary causes of the local bone lysis) are generated, which in turn, initiate and maintain an osteoclastic response through the activation of the receptor activator of nuclear factor kappa-B ligand (RANKL)–RANK molecular complex [27,30,31,32]. When a successful RCT eliminates the pathogenic endodontic bacteria, the inflammatory apical reaction together with the osteoclastic activity will cease to exist and the local osteogenic potential will take over, as it has been demonstrated that osteoprogenitor cells are present within the apical lesion [30,33,34]. Osteogenic cells provide the apposition of a new bone matrix, followed by cycles of bone remodeling which will finally end up in the periapical healing of the bone defect [31,32]. Ørstavik [35] found that complete healing of AP may require up to 4 years, however, signs of periapical healing were visible in at least 89% of the cases after 1-year of follow-up. Ng et al. [36] in a random-effects meta-analysis, revealed that the weighted pooled healing success rate of AP was 29.6% over a 6-month time period. Siqueira et al. [37] found that AP shows clear repair criteria compatible with successful RCT in 75% of cases in a 2-year follow-up period. Azim et al. [38] reported that the average time required for complete healing of an AP was 11.78 months.
On the other hand, it has been reported that a range of toxic substances such as nicotine, carbon monoxide, and hydrogen cyanide released during combustion and pyrolysis of the tobacco, would probably have a negative impact on the healing of AP [39], since such toxicants may potentially cause endothelial cell injury and affect the microvasculature of the periapical tissues, which in turn, could lead to a lower contribution of nutrients and oxygen, both essential in healing processes [40,41]. Furthermore, tobacco smoking has been associated with fibroblast dysfunction, thus leading to impaired tissue repair [40,42].
However, the 6 articles included in this review, agreed to suggest that there is no association between the prevalence of post endodontic AP and CS, in contrast to 2 recent systematic reviews that reported a negative influence of smoking on periapical disease in endodontically untreated teeth in terms of the prevalence of AP [17,18]. Therefore, it could be hypothesized that once the intraradicular microbial component causing the periapical inflammatory phenomenon has been removed, the molecular healing processes of AP could not be completely altered as a consequence of the local and systemic deleterious effects inherent to the habit of smoking and therefore smoking behavior should not be considered as a risk factor for the failure of endodontic therapy.
This is in line with Marending et al. [43] who reported that smoking is not a factor affecting the outcome of orthograde root canal therapy in the long term and Touré et al. [44] who found that smoking is not a factor related to failure or extraction of Endodontically Treated Teeth. Further, Danin et al. [45] suggested that the concentration of some proinflammatory cytokines such as TNF-α and transforming growth factor-beta 1 (TGF-β1) in AP does not differ in smokers vs non-smokers.
As the most important strength, we carefully followed Cochrane’s recommendations to perform this systematic review and meta-analysis. Moreover, to the best of our knowledge, this is the first systematic review that assessed the prevalence of AP associated with RCT in non-smokers vs smoker patients. On the other hand, this study has several limitations. First, all the studies included in this systematic review were of cross-sectional design [21,22,23,24,25,26], which does not assess variables such as: if the post endodontic AP is healing or not, the diagnosis prior to endodontic therapy, who and how was carried out the RCT (a general dentist or an endodontist and the techniques and materials used). Therefore, longitudinal studies would be very useful to evaluate the evolution of the AP in the long term and at the same time avoid the overestimation of AP. Secondly, the identification of AP in the 6 articles included in this systematic review was carried out by using 2- dimensional imaging techniques (Panoramic and or Periapical radiographs), which although accepted for the identification of AP as they provide reliable results under lower radiation doses, have great limitations in estimating the presence and size of AP and possess lower precision and sensibility when compared to cone-beam computed tomography [17,46,47]. Further, although the periapical index (PAI) is currently the gold standard index for the evaluation of AP at the radiographic level, only 3 studies [22,25,26] applied this evaluation method, and the remaining studies [21,23,24] designed their own evaluation criteria, which compromises the possibility of comparison among studies due to lack of standardization. Finally, in 5 of the 6 studies of this systematic review, smoking was analyzed as a dichotomous variable, however, the influence of aspects such as intensity, duration, and amount of smoking habit was not reported [21,22,24,25,26]. Only one study done by Sopińska and Bołtacz-Rzepkowska [23] categorized the history of smoking (smokers: “subjects who had been smoking in the past for 5 years without interruption, at least 10 cigarettes a day”).
In view of the foregoing, it is important to emphasize that results from this systematic review are inconclusive, as there is a lack of well-designed clinical studies with longitudinal designs that allow to clearly elucidate the influence of CS on the prevalence of post endodontic AP.
CONCLUSIONS
Our findings suggest that there was no association between CS and post endodontic AP, as we did not find statistical differences in the prevalence of post endodontic AP when comparing non-smokers vs smoker subjects. Therefore, CS should not be considered a risk factor associated with endodontic failure. Nonetheless, there were important limitations that prevent the extrapolation of these results. We strongly suggest improving the quality of studies to improve the strength of these results.
-
Conflict of Interest: No potential conflict of interest relevant to this article was reported.
-
Author Contributions:
Conceptualization: Ríos-Osorio N.
Data curation: Jiménez-Peña O, Muñoz-Alvear HD.
Formal analysis: García-Perdomo HA.
Investigation: Quijano S, Caviedes-Bucheli J.
Methodology: Muñoz-Alvear HD, Jiménez- Peña O, Caviedes-Bucheli J.
Project administration: Ríos-Osorio N.
Software: Muñoz-Alvear HD.
Supervision: Jiménez-Castellanos FA.
Validation: Quijano S, Caviedes-Bucheli J.
Visualization: Quijano S.
Writing - original draft: Ríos-Osorio N.
Writing - review & editing: Ríos-Osorio N, Jiménez-Castellanos FA, García-Perdomo HA.
- 1. Calafat AM, Polzin GM, Saylor J, Richter P, Ashley DL, Watson CH. Determination of tar, nicotine, and carbon monoxide yields in the mainstream smoke of selected international cigarettes. Tob Control 2004;13:45-51.ArticlePubMedPMC
- 2. Manuela R, Mario M, Vincenzo R, Filippo R. Nicotine stimulation increases proliferation and matrix metalloproteinases-2 and -28 expression in human dental pulp cells. Life Sci 2015;135:49-54.ArticlePubMed
- 3. Kissela BM, Khoury J, Kleindorfer D, Woo D, Schneider A, Alwell K, Miller R, Ewing I, Moomaw CJ, Szaflarski JP, Gebel J, Shukla R, Broderick JP. Epidemiology of ischemic stroke in patients with diabetes: the greater Cincinnati/Northern Kentucky Stroke Study. Diabetes Care 2005;28:355-359.PubMed
- 4. Esfahrood ZR, Zamanian A, Torshabi M, Abrishami M. The effect of nicotine and cotinine on human gingival fibroblasts attachment to root surfaces. J Basic Clin Physiol Pharmacol 2015;26:517-522.ArticlePubMed
- 5. Kinnula VL. Focus on antioxidant enzymes and antioxidant strategies in smoking related airway diseases. Thorax 2005;60:693-700.ArticlePubMedPMC
- 6. Reibel J. Tobacco and oral diseases. Update on the evidence, with recommendations. Med Princ Pract 2003;12(Suppl 1):22-32.ArticlePubMedPDF
- 7. Cano M, Thimmalappula R, Fujihara M, Nagai N, Sporn M, Wang AL, Neufeld AH, Biswal S, Handa JT. Cigarette smoking, oxidative stress, the anti-oxidant response through Nrf2 signaling, and Age-related Macular Degeneration. Vision Res 2010;50:652-664.ArticlePubMed
- 8. Özsezer Demiryürek E, Sakallıoğlu EE, Kalyoncuoğlu E, Yılmaz Miroğlu Y, Sakallıoğlu U. The effects of smoking on the osmotic pressure of human dental pulp tissue. Med Princ Pract 2015;24:465-469.ArticlePubMedPMCPDF
- 9. Scott DA, Poston RN, Wilson RF, Coward PY, Palmer RM. The influence of vitamin C on systemic markers of endothelial and inflammatory cell activation in smokers and non-smokers. Inflamm Res 2005;54:138-144.ArticlePubMedPDF
- 10. Krall EA, Abreu Sosa C, Garcia C, Nunn ME, Caplan DJ, Garcia RI. Cigarette smoking increases the risk of root canal treatment. J Dent Res 2006;85:313-317.ArticlePubMedPMCPDF
- 11. Caviedes-Bucheli J, Gomez-Sosa JF, Azuero-Holguin MM, Ormeño-Gomez M, Pinto-Pascual V, Munoz HR. Angiogenic mechanisms of human dental pulp and their relationship with substance P expression in response to occlusal trauma. Int Endod J 2017;50:339-351.ArticlePubMedPDF
- 12. Ríos-Osorio N, Muñoz-Alvear HD, Montoya Cañón S, Restrepo-Mendez S, Aguilera-Rojas SE, Jiménez-Peña O, García-Perdomo HA. Association between type 2 diabetes mellitus and the evolution of endodontic pathology. Quintessence Int 2020;51:100-107.PubMed
- 13. Fröhlich M, Sund M, Löwel H, Imhof A, Hoffmeister A, Koenig W. Independent association of various smoking characteristics with markers of systemic inflammation in men. Results from a representative sample of the general population (MONICA Augsburg Survey 1994/95). Eur Heart J 2003;24:1365-1372.ArticlePubMed
- 14. Ijzerman RG, Serne EH, van Weissenbruch MM, de Jongh RT, Stehouwer CD. Cigarette smoking is associated with an acute impairment of microvascular function in humans. Clin Sci (Lond) 2003;104:247-252.ArticlePubMedPDF
- 15. Barbieri SS, Zacchi E, Amadio P, Gianellini S, Mussoni L, Weksler BB, Tremoli E. Cytokines present in smokers’ serum interact with smoke components to enhance endothelial dysfunction. Cardiovasc Res 2011;90:475-483.ArticlePubMed
- 16. Johannsen A, Susin C, Gustafsson A. Smoking and inflammation: evidence for a synergistic role in chronic disease. Periodontol 2000 2014;64:111-126.ArticlePubMed
- 17. Pinto KP, Ferreira CM, Maia LC, Sassone LM, Fidalgo TK, Silva EJ. Does tobacco smoking predispose to apical periodontitis and endodontic treatment need? A systematic review and meta-analysis. Int Endod J 2020;53:1068-1083.ArticlePubMedPDF
- 18. Aminoshariae A, Kulild J, Gutmann J. The association between smoking and periapical periodontitis: a systematic review. Clin Oral Investig 2020;24:533-545.ArticlePubMedPDF
- 19. Urrútia G, Bonfill X. PRISMA declaration: a proposal to improve the publication of systematic reviews and meta-analyses. Med Clin (Barc) 2010;135:507-511.PubMed
- 20. Wells GA, Shea B, O’Connell D, Peterson J, Welch V, Losos M, Tugwell P. The Newcastle-Ottawa Scale (NOS) for assessing the quality of nonrandomised studies in meta-analyses [Internet]. Ottawa, ON: Ottawa Hospital Research Institute; 2019. cited 2020 Nov 4]. Available from: http://www.ohri.ca/programs/clinical_epidemiology/oxford.asp.
- 21. Bergström J, Babcan J, Eliasson S. Tobacco smoking and dental periapical condition. Eur J Oral Sci 2004;112:115-120.ArticlePubMed
- 22. Segura-Egea JJ, Jiménez-Pinzón A, Ríos-Santos JV, Velasco-Ortega E, Cisneros-Cabello R, Poyato-Ferrera MM. High prevalence of apical periodontitis amongst smokers in a sample of Spanish adults. Int Endod J 2008;41:310-316.ArticlePubMed
- 23. Sopińska K, Bołtacz-Rzepkowska E. The influence of tobacco smoking on dental periapical condition in a sample of an adult population of the Łódź region, Poland. Int J Occup Med Environ Health 2020;33:45-57.ArticlePubMed
- 24. Bahammam LA. Tobacco smoking and dental periapical condition in a sample of Saudi Arabian sub-population. J King Abdulaziz Univ Med Sci 2012;19:35-41.Article
- 25. Peršić Bukmir R, Jurčević Grgić M, Brumini G, Spalj S, Pezelj-Ribaric S, Brekalo Pršo I. Influence of tobacco smoking on dental periapical condition in a sample of Croatian adults. Wien Klin Wochenschr 2016;128:260-265.ArticlePubMedPDF
- 26. Segura-Egea JJ, Castellanos-Cosano L, Velasco-Ortega E, Ríos-Santos JV, Llamas-Carreras JM, Machuca G, López-Frías FJ. Relationship between smoking and endodontic variables in hypertensive patients. J Endod 2011;37:764-767.ArticlePubMed
- 27. Metzger Z, Abramovitz I. Periapical lesions of endodontic origin. In: Ingle JI, Bakland LK, Baumgartner JC, editors. Ingle’s endodontics. 6th ed. Hamilton, ON: BC Decker; 2009. p. 494-519.
- 28. Kettering JD, Torabinejad M, Jones SL. Specificity of antibodies present in human periapical lesions. J Endod 1991;17:213-216.ArticlePubMed
- 29. Baumgartner JC, Falkler WA Jr. Biosynthesis of IgG in periapical lesion explant cultures. J Endod 1991;17:143-146.ArticlePubMed
- 30. Lieberman JR, Daluiski A, Einhorn TA. The role of growth factors in the repair of bone. Biology and clinical applications. J Bone Joint Surg Am 2002;84:1032-1044.PubMed
- 31. Hofbauer LC, Heufelder AE. Role of receptor activator of nuclear factor-kappaB ligand and osteoprotegerin in bone cell biology. J Mol Med (Berl) 2001;79:243-253.PubMed
- 32. Hofbauer LC, Kühne CA, Viereck V. The OPG/RANKL/RANK system in metabolic bone diseases. J Musculoskelet Neuronal Interact 2004;4:268-275.PubMed
- 33. Holland R, Gomes JE, Cintra LTA, Queiroz ÍOA, Estrela C. Factors affecting the periapical healing process of endodontically treated teeth. J Appl Oral Sci 2017;25:465-476.ArticlePubMedPMC
- 34. Maeda H, Wada N, Nakamuta H, Akamine A. Human periapical granulation tissue contains osteogenic cells. Cell Tissue Res 2004;315:203-208.ArticlePubMedPDF
- 35. Ørstavik D. Time-course and risk analyses of the development and healing of chronic apical periodontitis in man. Int Endod J 1996;29:150-155.ArticlePubMed
- 36. Ng YL, Mann V, Rahbaran S, Lewsey J, Gulabivala K. Outcome of primary root canal treatment: systematic review of the literature - part 1. Effects of study characteristics on probability of success. Int Endod J 2007;40:921-939.ArticlePubMed
- 37. Siqueira JF Jr, Rôças IN, Riche FN, Provenzano JC. Clinical outcome of the endodontic treatment of teeth with apical periodontitis using an antimicrobial protocol. Oral Surg Oral Med Oral Pathol Oral Radiol Endod 2008;106:757-762.ArticlePubMed
- 38. Azim AA, Griggs JA, Huang GT. The Tennessee study: factors affecting treatment outcome and healing time following nonsurgical root canal treatment. Int Endod J 2016;49:6-16.ArticlePubMed
- 39. Duncan HF, Pitt Ford TR. The potential association between smoking and endodontic disease. Int Endod J 2006;39:843-854.ArticlePubMed
- 40. Segura-Egea JJ, Martín-González J, Castellanos-Cosano L. Endodontic medicine: connections between apical periodontitis and systemic diseases. Int Endod J 2015;48:933-951.ArticlePubMed
- 41. Lehr HA. Microcirculatory dysfunction induced by cigarette smoking. Microcirculation 2000;7:367-384.ArticlePubMed
- 42. Wong LS, Green HM, Feugate JE, Yadav M, Nothnagel EA, Martins-Green M. Effects of “second-hand” smoke on structure and function of fibroblasts, cells that are critical for tissue repair and remodeling. BMC Cell Biol 2004;5:13.ArticlePubMedPMCPDF
- 43. Marending M, Peters OA, Zehnder M. Factors affecting the outcome of orthograde root canal therapy in a general dentistry hospital practice. Oral Surg Oral Med Oral Pathol Oral Radiol Endod 2005;99:119-124.ArticlePubMed
- 44. Touré B, Faye B, Kane AW, Lo CM, Niang B, Boucher Y. Analysis of reasons for extraction of endodontically treated teeth: a prospective study. J Endod 2011;37:1512-1515.ArticlePubMed
- 45. Danin J, Linder LE, Lundqvist G, Andersson L. Tumor necrosis factor-alpha and transforming growth factor-beta1 in chronic periapical lesions. Oral Surg Oral Med Oral Pathol Oral Radiol Endod 2000;90:514-517.ArticlePubMed
- 46. Wu MK, Shemesh H, Wesselink PR. Limitations of previously published systematic reviews evaluating the outcome of endodontic treatment. Int Endod J 2009;42:656-666.ArticlePubMed
- 47. Patel S, Dawood A, Whaites E, Pitt Ford T. New dimensions in endodontic imaging: part 1. Conventional and alternative radiographic systems. Int Endod J 2009;42:447-462.ArticlePubMed
REFERENCES
Appendix
Tables & Figures
REFERENCES
Citations
Citations to this article as recorded by 
- The role of smoking as a risk indicator for apical periodontitis and endodontic status: a cross-sectional study of a portuguese adult sample
Isabel Silva Martins, Natália Pestana de Vasconcelos, Américo Santos Afonso, Ana Cristina Braga, Irene Pina-Vaz
Odontology.2026;[Epub] CrossRef - RISK FACTORS FOR CHRONIC APICAL PERIODONTITIS ACCORDING TO THE CASE-CONTROL STUDY
N. Bagryantseva
Vrach.2026; : 43. CrossRef
 ePub Link
ePub Link Cite
CiteAssociation between cigarette smoking and the prevalence of post-endodontic periapical pathology: a systematic review and meta-analysis
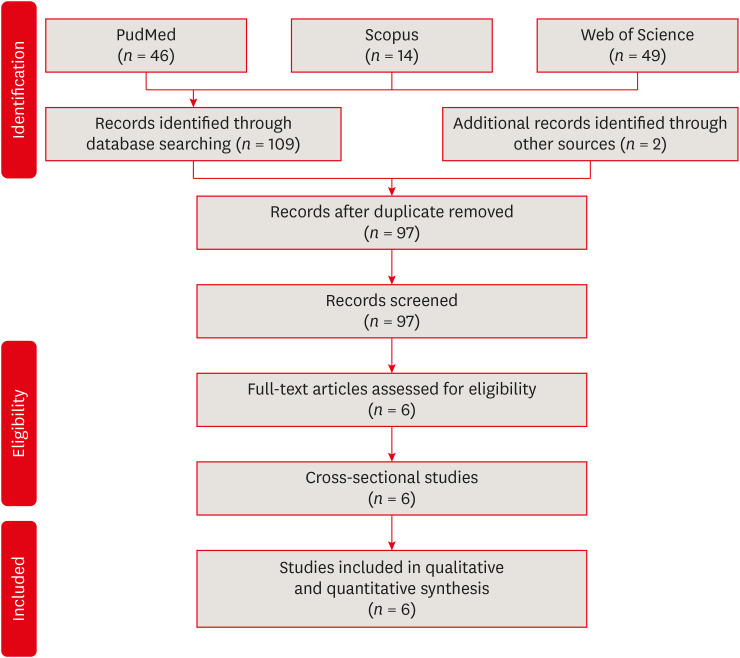
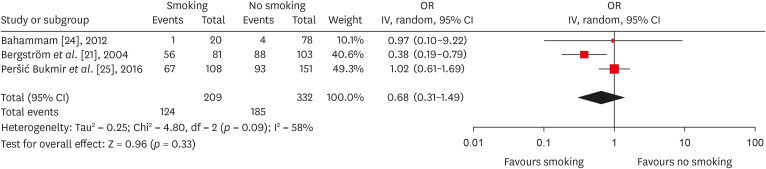
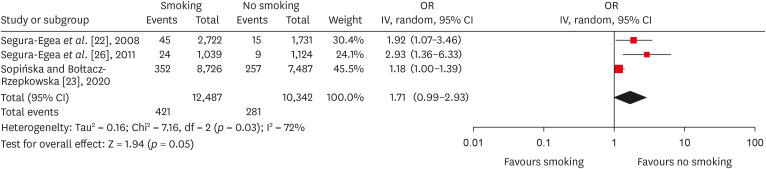
Figure 1 Flowchart of included studies.
Figure 2 Forest plot of association between root canal treatment with apical periodontitis in smokers vs non-smokers subjects (analysis by patients).OR, odds ratio; CI, Confidence interval.
Figure 3 Forest plot of association between root canal treatment with apical periodontitis in smokers vs non-smokers subjects (analysis by teeth).OR, odds ratio; CI, Confidence interval.
Figure 1
Figure 2
Figure 3
Association between cigarette smoking and the prevalence of post-endodontic periapical pathology: a systematic review and meta-analysis
Characteristics of studies assessing the post endodontic prevalence of AP in smokers vs non-smokers patient
| Article | Author, year, country | Sample ( | Age | Sample characteristics (smoker and/or non-smoker) | Teeth ( | Periapical diagnosis | PAI | Main results | Statistical analysis | Confidence level | Conclusion |
|---|---|---|---|---|---|---|---|---|---|---|---|
| 1 | Bergström | Subjects | 20–65 | Current smokers ( | On average for the total sample: 38.7 out of a maximum of 42 dental roots per person (i.e. 92%) were available for assessment. | Periapical radiographs | No | The mean numbers of periapical lesions per person related to endodontically treated teeth for current smokers: | Kolmogorov–Smirnov test, Kruskal–Wallis non-parametric ANOVA, two-factor ANOVA, and Scheffé | It is concluded that these observations do not support the assumption that smoking is associated with apical periodontitis. Moreover, there was no statistically difference ( | |
| 2 | Segura-egea | Subjects | 37.1 ± 15.7 | Current smokers ( | Total number of teeth examined in smokers was 2,722 and 1,731 teeth in non-smokers. The average number of teeth per patient: smokers ( | Periapical radiographs | Yes | AP in one or more teeth in smokers ( | Cohen’s Kappa test, ANOVA and logistic regression | Smoking was significantly associated with a higher frequency and prevalence of root canal treatment and apical periodontitis. However, there was no statistically difference ( | |
| 3 | Sopińska and Bołtacz-Rzepkowska [ | Subjects | 18–91 | Non-smokers ( | Total number of teeth examined in smokers was 8,726 and 7,487 teeth in non-smokers. | Panoramic radiographs | No | Smokers presented a higher prevalence of teeth with AP than non-smokers (7.2% and 5.2% respectively, | χ2 and the Mantel-Haenszel test | Smokers are a group facing an increased risk of AP. However, no difference was observed in the frequency of AP in the endodontically treated teeth in both groups (37.6% | |
| 4 | Bahammam [ | Subjects | 20–60 | Non-smokers ( | The average number of teeth per patient was 24.65 ± 3.28 and 24.58 ± 4.41 in smokers and non-smokes, respectively ( | Periapical radiographs | No | The prevalence of patients with AP was 8.59% in smoker and 6.18% in non-smokers. The frequency of patients having AP with RCT in smoker and in non-smokers was 5.73% and 5.12%, respectively ( | Results from this study do not favor the assumption that smoking is associated with AP. Likewise, there was no statistically difference ( | ||
| 5 | Peršić Bukmir | Subjects | 40.3 ± 15.1 | Non-smokers ( | The average number of teeth per patient was 22.9 ± 5.2 and 23.2 ± 4.9 in smokers and non-smokes, respectively ( | Panoramic radiographs and Periapical radiographs | Yes | Smokers had higher prevalence of teeth with AP than non-smokers (0.13 | Kolmogorov–Smirnov test, | Smokers will on average have two teeth with AP more than non-smokers, thus supporting the hypothesis that smoking influences the periapical status of teeth. However, no difference was observed in the prevalence of AP in the endodontically treated teeth when comparing smokers | |
| 6 | Segura-egea | Subjects | 58.7 ± 9.6 | 50 smokers and 50 non-smokers | Total number of teeth examined in smokers was 1,039 and 1,124 teeth in non-smokers. The average number of teeth per patient: smokers ( | Periapical radiographs | Yes | AP in one or more teeth in smokers ( | Student | The prevalence of apical periodontitis and root canal treatment was significantly higher in hypertensive smoking patients compared to non-smokers. However, there was no statistically difference ( |
AP, apical periodontitis; PAI, periapical index; CI, Confidence interval; RCT, root canal treatment; ANOVA, analysis of variance; OR, odds ratio; SD, standard deviation.
Evaluation according to the Newcastle-Ottawa quality assessment scale
| Study | Selection | Comparability | Outcome | Conclusion | |
|---|---|---|---|---|---|
|
| |||||
| Bergström | - | ★★ | ★★★ | HIGH RISK | |
| Segura-Egea | - | ★★ | ★★★ | HIGH RISK | |
| Sopińska and Bołtacz-Rzepkowska [ | ★★ | ★★ | ★★★ | LOW RISK | |
| Bahammam [ | ★ | - | ★★★ | HIGH RISK | |
| Peršić Bukmir | ★★ | ★★ | ★★★ | LOW RISK | |
| Segura-Egea | - | ★★ | ★★★ | HIGH RISK | |
Table 1 Characteristics of studies assessing the post endodontic prevalence of AP in smokers vs non-smokers patient
AP, apical periodontitis; PAI, periapical index; CI, Confidence interval; RCT, root canal treatment; ANOVA, analysis of variance; OR, odds ratio; SD, standard deviation.
Table 2 Evaluation according to the Newcastle-Ottawa quality assessment scale

