
Search
- Page Path
- HOME > Search
Research Article
- Impact of post adhesion on stress distribution: an in silico study
- Kkot-Byeol Bae, Jae-Yoon Choi, Young-Tae Cho, Bin-Na Lee, Hoon-Sang Chang, Yun-Chan Hwang, Won-Mann Oh, In-Nam Hwang
- Restor Dent Endod 2025;50(2):e19. Published online May 21, 2025
- DOI: https://doi.org/10.5395/rde.2025.50.e19
-
 Abstract
Abstract
 PDF
PDF PubReader
PubReader ePub
ePub - Objectives
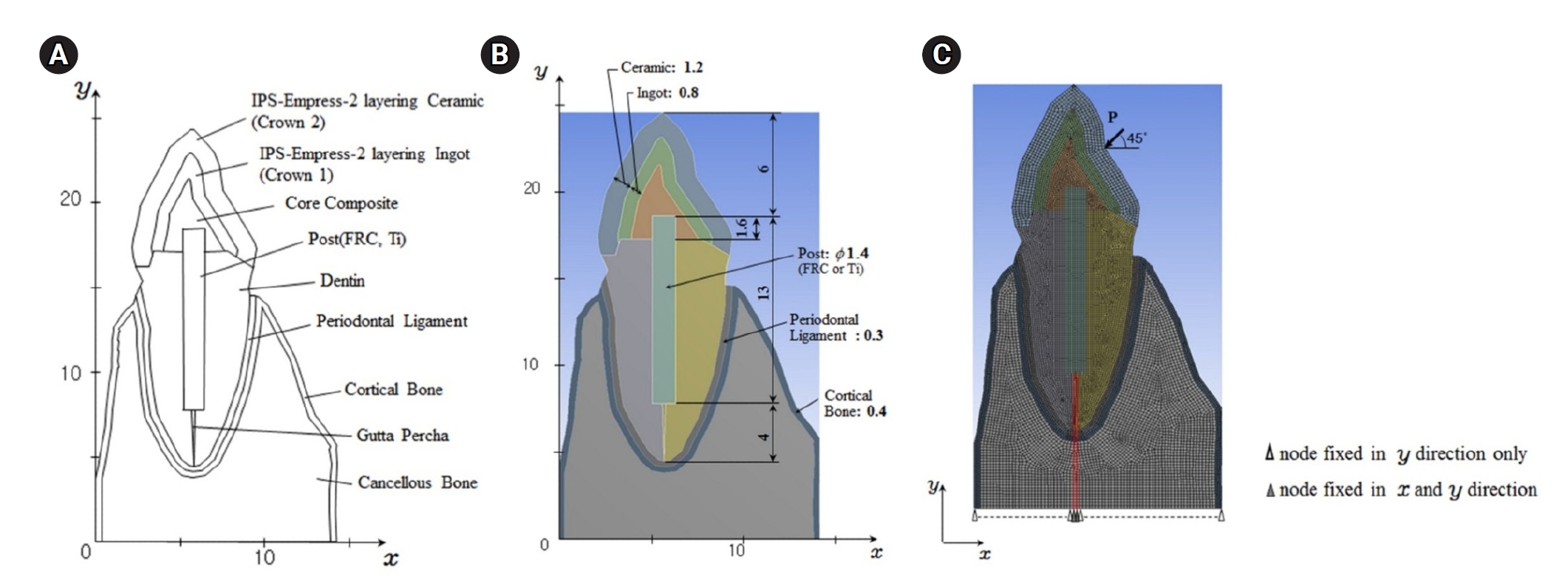
This study aimed to evaluate the stress distribution in teeth restored with different post materials and bonding conditions using finite element analysis (FEA).
Methods
A two-dimensional FEA model of a maxillary central incisor restored with IPS-Empress-2 crown (Ivoclar Vivadent), composite resin core, and posts were created. The model simulated bonded and non-bonded conditions for both fiber-reinforced composite (FRC) and titanium (Ti) posts. Stress distribution was analyzed using ANSYS 14.0 software under a 100-N load applied at a 45° angle to the long axis of the tooth.
Results
The results revealed that stress concentration was significantly higher in non-bonded posts compared to bonded ones. FRC posts exhibited stress values closer to those of dentin, whereas Ti posts demonstrated higher stress concentration, particularly in non-bonded states, increasing the potential risk of damage to surrounding tissues.
Conclusions
FRC posts, with elastic properties similar to dentin and proper adhesion, minimize stress concentration and potential damage to surrounding tissues. Conversely, materials with higher elastic modulus like Ti, can cause unfavorable stress concentrations if not properly bonded, emphasizing the importance of post adhesion in tooth restoration. -
Citations
Citations to this article as recorded by
- Advances in Ecofriendly and High-Strength Dental Composites: Structural and Functional Perspectives
Sayem A. Mulla, Amit Patil, Himmat Jaiswal, Bhavani Sangala Nagendra, Ashima Jakhar, Waseem Z. Khan
European Journal of General Dentistry.2026;[Epub] CrossRef
- Advances in Ecofriendly and High-Strength Dental Composites: Structural and Functional Perspectives
- 3,324 View
- 114 Download
- 1 Crossref

Case Reports
- Fiber-reinforced composite post removal using guided endodontics: a case report
- Changgi Cho, Hyo Jin Jo, Jung-Hong Ha
- Restor Dent Endod 2021;46(4):e50. Published online September 23, 2021
- DOI: https://doi.org/10.5395/rde.2021.46.e50
-
Abstract
PDFPubReaderePub
Although several techniques have been proposed to remove fiber-reinforced composite (FRC) post, no safe and efficient technique has been established. Recently, a guided endodontics technique has been introduced in cases of pulp canal obliteration. This study describes 2 cases of FRC post removal from maxillary anterior teeth using this guided endodontics technique with a dental operating microscope. Optically scanned data set from plaster cast model was superimposed with the data set of cone-beam computed tomography. By implant planning software, the path of a guide drill was selected. Based on them, a customized stent was fabricated and utilized to remove the FRC post. Employing guided endodontics, the FRC post was removed quickly and safely with minimizing the loss of the remaining tooth structure. The guided endodontics was a useful option for FRC post removal.
-
Citations
Citations to this article as recorded by- Comparing the Effectiveness of a Robotic and Dynamic Navigation System in Fiber Post removal: An In Vitro Study
Duo Zhou, Fulu Xu, Jiayun Dai, Xingyang Wang, Yifan Ping, Juan Wang
Journal of Endodontics.2026; 52(2): 261. CrossRef - Robot-assisted haptic guidance in endodontics: A pilot study evaluating efficiency and tooth structure preservation
Roshanak Momen, Joshua Dale, Mithun Suresh, Theodore D. Ravenel, Julie Marshall, Chin-Lo Hahn
Journal of Dentistry.2026; 173: 106854. CrossRef - Deviation analysis of guided fiber post removal using an assembled sleeveless guide system: A case series
Jingqi Zhu, Siyi Mo, Yuan Li, Yaojun Zhang, Xutong Song, Jingwen Liu, Ye Cao, Xiaoxiang Xu
The Journal of Prosthetic Dentistry.2026;[Epub] CrossRef - Static‐Guided Endodontics for Complex Intracanal Obstructions and Zirconia Post Removal: Report on Three Cases
Xinxuan Wang, Xuguang Li, Baicheng Yi
Clinical Case Reports.2026;[Epub] CrossRef - Application of 3D-printed resin guides for the removal of molar fiber posts
Yumin Wu, Lumei Huang, Bing Ge, Yuhang Zhang, Juan Zhang, Haifeng Xie, Ye Zhu, Chen Chen
Journal of Dentistry.2025; 153: 105462. CrossRef - Guided Removal of Long and Short Fiber Posts Using Endodontic Static Guides: A Case Report
Sahar Shafagh, Mamak Adel, Atiyeh Sabzpai
Clinical Case Reports.2025;[Epub] CrossRef - Guided versus non-guided fiber post removal: A systematic review and meta-analysis of the accuracy, efficiency, and dentin preservation of static navigation techniques in the removal of fiber posts
Mohamad Elabdalla, Farshad Khosraviani, Shahryar Irannejadrankouhi, Niloofar Ghadimi, Turgut Yağmur Yalçın, Shaheen Wathiq Tawfeeq Al Hajaj, Mahmood Dashti
The Journal of Prosthetic Dentistry.2025; 134(3): 630.e1. CrossRef - Top 100 Most-cited Scientific Articles in Guided Endodontic 2018–2024: A Bibliometric Analysis
Gustavo Adrián Morales Valladares, Raquel Esmeralda Guillén Guillén, Martha Elena Gallegos Intriago, Mary Yussely Burgos Barreiro, Claudia Jhelissa Campos Vélez, Andrés Alexander Castillo Chacón, Silvana Beatriz Terán Ayala
The Open Dentistry Journal.2025;[Epub] CrossRef - Nonsurgical Management of a Tooth With Intracanal Fiber Post and Periapical Lesion Using Guided Endodontic Technique
Mamak Adel, Zohreh Asgari
Clinical Case Reports.2025;[Epub] CrossRef - Impact of Guided Endodontics on the Success of Endodontic Treatment: An Umbrella Review of Systematic Reviews and Meta-Analyses
Aakansha Puri, Dax Abraham, Alpa Gupta
Cureus.2024;[Epub] CrossRef - Endodontia guiada por tomografia computadorizada de feixe cônico
Maysa Gaudereto Laurindo, Celso Neiva Campos, Anamaria Pessoa Pereira Leite, Paola Cantamissa Rodrigues Ferreira
Cadernos UniFOA.2024; 19(54): 1. CrossRef - Removal of fiber posts using conventional versus guided endodontics: a comparative study of dentin loss and complications
R. Krug, F. Schwarz, C. Dullin, W. Leontiev, T. Connert, G. Krastl, F. Haupt
Clinical Oral Investigations.2024;[Epub] CrossRef - Accuracy and Efficiency of the Surgical-Guide-Assisted Fiber Post Removal Technique for Anterior Teeth: An Ex Vivo Study
Ryota Ito, Satoshi Watanabe, Kazuhisa Satake, Ryuma Saito, Takashi Okiji
Dentistry Journal.2024; 12(10): 333. CrossRef - Endodontic management of severely calcified mandibular anterior teeth using guided endodontics: A report of a case and a review of the literature
Mina Davaji, Sahar Karimpour
Saudi Endodontic Journal.2024; 14(2): 245. CrossRef - A laboratory study comparing the static navigation technique using a bur with a conventional freehand technique using ultrasonic tips for the removal of fibre posts
Francesc Abella Sans, Zeena Tariq Alatiya, Gonzalo Gómez Val, Venkateshbabu Nagendrababu, Paul Michael Howell Dummer, Fernando Durán‐Sindreu Terol, Juan Gonzalo Olivieri
International Endodontic Journal.2024; 57(3): 355. CrossRef - A three‐dimensional printed assembled sleeveless guide system for fiber‐post removal
Yang Xue, Lei Zhang, Ye Cao, Yongsheng Zhou, Qiufei Xie, Xiaoxiang Xu
Journal of Prosthodontics.2023; 32(2): 178. CrossRef - Accuracy of a 3D printed sleeveless guide system used for fiber post removal: An in vitro study
Siyi Mo, Yongwei Xu, Lei Zhang, Ye Cao, Yongsheng Zhou, Xiaoxiang Xu
Journal of Dentistry.2023; 128: 104367. CrossRef - Expert consensus on digital guided therapy for endodontic diseases
Xi Wei, Yu Du, Xuedong Zhou, Lin Yue, Qing Yu, Benxiang Hou, Zhi Chen, Jingping Liang, Wenxia Chen, Lihong Qiu, Xiangya Huang, Liuyan Meng, Dingming Huang, Xiaoyan Wang, Yu Tian, Zisheng Tang, Qi Zhang, Leiying Miao, Jin Zhao, Deqin Yang, Jian Yang, Junqi
International Journal of Oral Science.2023;[Epub] CrossRef - Knowledge, attitude, practice and perception survey on post and core restorations
Aruna Kumari Veronica, Shamini Sai, Anand V Susila
Endodontology.2023; 35(3): 228. CrossRef
- Comparing the Effectiveness of a Robotic and Dynamic Navigation System in Fiber Post removal: An In Vitro Study
- 6,145 View
- 123 Download
- 14 Web of Science
- 19 Crossref
- Bioblock technique to treat severe internal resorption with subsequent periapical pathology: a case report
- Márk Fráter, Tekla Sáry, Sufyan Garoushi
- Restor Dent Endod 2020;45(4):e43. Published online August 18, 2020
- DOI: https://doi.org/10.5395/rde.2020.45.e43

-
Abstract
PDFPubReaderePub
A variety of therapeutic modalities can be used for the endodontic treatment of a traumatized tooth with internal root resorption (IRR). The authors present a case report of the successful restoration of a traumatized upper central incisor that was weakened due to severe IRR and subsequent periapical lesion formation. A 20-year-old female patient was referred to our clinic with severe internal resorption and subsequent periapical pathosis destroying the buccal bone wall. Root canal treatment had been initiated previously at another dental practice, but at that time, the patient's condition could not be managed even with several treatments. After cone-beam computed tomography imaging and proper chemomechanical cleaning, the tooth was managed with a mineral trioxide aggregate plug followed by root canal filling using short fiber-reinforced composite, known as the Bioblock technique. This report is the first documentation of the use of the Bioblock technique in the restoration of a traumatized tooth. The Bioblock technique appears to be ideal for restoring wide irregular root canals, as in cases of severe internal resorption, because it can uniquely fill out the hollow irregularities of the canal. However, further long-term clinical investigations are required to provide additional information about this new technique.
-
Citations
Citations to this article as recorded by- Influence of Endodontic Access Cavity Design on Fracture Strength of Teeth Restored with Bulk-fill and Fiber-reinforced Composites: An In vitro Study
Sakshi Sharad Agrawal, S. R. Srinidhi, Sourabh S. Barbhai, Ayush A. Agarwal, Muskan Dilip Hinduja
Journal of the International Clinical Dental Research Organization.2026; 18(1): 59. CrossRef - Üvegszálas fogászati kompozit tömőanyag keménysége a gyökércsatornában: nanoindentációs vizsgálat
András Jakab, Kata Lilla Vánkay, Tamás Tarjányi, Gábor Gulyás, Krisztián Bali, Pál Patrik Dézsi, Márton Sámi, Márk Fráter
Fogorvosi Szemle.2024; 117(2): 47. CrossRef - Evaluation of microhardness of short fiber-reinforced composites inside the root canal after different light curing methods – An in vitro study
Márk Fráter, János Grosz, András Jakab, Gábor Braunitzer, Tamás Tarjányi, Gábor Gulyás, Krisztián Bali, Paula Andrea Villa-Machado, Sufyan Garoushi, András Forster
Journal of the Mechanical Behavior of Biomedical Materials.2024; 150: 106324. CrossRef - Imaging techniques and various treatment modalities used in the management of internal root resorption: A systematic review
R. S Digholkar, S D Aggarwal, P S Kurtarkar, P. B Dhatavkar, V L Neil, D N Agarwal
Endodontology.2023; 35(2): 85. CrossRef - The Impact of the Preferred Reporting Items for Case Reports in Endodontics (PRICE) 2020 Guidelines on the Reporting of Endodontic Case Reports
Sofian Youssef, Phillip Tomson, Amir Reza Akbari, Natalie Archer, Fayjel Shah, Jasmeet Heran, Sunmeet Kandhari, Sandeep Pai, Shivakar Mehrotra, Joanna M Batt
Cureus.2023;[Epub] CrossRef - Fatigue performance of endodontically treated premolars restored with direct and indirect cuspal coverage restorations utilizing fiber-reinforced cores
Márk Fráter, Tekla Sáry, Janka Molnár, Gábor Braunitzer, Lippo Lassila, Pekka K. Vallittu, Sufyan Garoushi
Clinical Oral Investigations.2022; 26(4): 3501. CrossRef
- Influence of Endodontic Access Cavity Design on Fracture Strength of Teeth Restored with Bulk-fill and Fiber-reinforced Composites: An In vitro Study
- 5,183 View
- 128 Download
- 6 Crossref
- Fiber-reinforced composite resin bridges: an alternative method to treat root-fractured teeth
- Gun Heo, Eun-Hye Lee, Jin-Woo Kim, Kyung-Mo Cho, Se-Hee Park
- Restor Dent Endod 2020;45(1):e8. Published online December 27, 2019
- DOI: https://doi.org/10.5395/rde.2020.45.e8

-
Abstract
PDFPubReaderePub
The replacement of missing teeth, especially in the anterior region, is an essential part of dental practice. Fiber-reinforced composite resin bridges are a conservative alternative to conventional fixed dental prostheses or implants. It is a minimally invasive, reversible technique that can be completed in a single visit. The two cases presented herein exemplify the treatment of root-fractured anterior teeth with a natural pontic immediately after extraction.
-
Citations
Citations to this article as recorded by- Prosthodontic Aspects of Splinting the Mandibular Anterior Teeth by Fiber Reinforced Composites
Hrelja Miroslav, Laškarin Mirko, Čimić Samir, Kraljević Sonja, Dulčić Nikša, Badel Tomislav
Journal of Dental Problems and Solutions.2025; 12(1): 004. CrossRef - Current Evidence on the Fiber-reinforced Composite Bridges
Ramesh Chowdhary, Sunil Kumar Mishra
International Journal of Prosthodontics and Restorative Dentistry.2023; 12(4): 159. CrossRef - Bridging the Gap: A Case Report of Tooth Replacement using Resin-Bonded Fiber- Reinforced Composite Resin
Vineet Sharma, Sumit Bhansali, Sonal Priya Bhansali
Journal of Pierre Fauchard Academy (India Section).2023; : 66. CrossRef - Reconstruction of Natural Smile and Splinting with Natural Tooth Pontic Fiber‐Reinforced Composite Bridge
Maryam S. Tavangar, Fatemeh Aghaei, Massoumeh Nowrouzi, Andrea Scribante
Case Reports in Dentistry.2022;[Epub] CrossRef
- Prosthodontic Aspects of Splinting the Mandibular Anterior Teeth by Fiber Reinforced Composites
- 3,004 View
- 26 Download
- 4 Crossref
Research Article
- Fracture resistance of upper central incisors restored with different posts and cores
- Maryam Rezaei Dastjerdi, Kamran Amirian Chaijan, Saeid Tavanafar
- Restor Dent Endod 2015;40(3):229-235. Published online July 24, 2015
- DOI: https://doi.org/10.5395/rde.2015.40.3.229
-
Abstract
PDFPubReaderePub
Objectives To determine and compare the fracture resistance of endodontically treated maxillary central incisors restored with different posts and cores.
Materials and Methods Forty-eight upper central incisors were randomly divided into four groups: cast post and core (group 1), fiber-reinforced composite (FRC) post and composite core (group 2), composite post and core (group 3), and controls (group 4). Mesio-distal and bucco-lingual dimensions at 7 and 14 mm from the apex were compared to ensure standardization among the groups. Twelve teeth were prepared for crown restoration (group 4). Teeth in other groups were endodontically treated, decoronated at 14 mm from the apex, and prepared for posts and cores. Resin-based materials were used for cementation in groups 1 and 2. In group 3, composite was used directly to fill the post space and for core build-up. All samples were restored by standard metal crowns using glass ionomer cement, mounted at 135° vertical angle, subjected to thermomechanical aging, and then fractured using a universal testing machine. Kruskal-Wallis and Mann-Whitney
U tests were used to analyze the data.Results Fracture resistance of the groups was as follows: Control (group 4) > cast post and core (group 1) > fiber post and composite core (group 2) > composite post and core (group 3). All samples in groups 2 and 3 fractured in restorable patterns, whereas most (58%) in group 1 were non-restorable.
Conclusions Within the limitations of this study, FRC posts showed acceptable fracture resistance with favorable fracture patterns for reconstruction of upper central incisors.
-
Citations
Citations to this article as recorded by- Can Coronal Restorative Choices Influence Root Strength After RET? A Fracture Resistance Evaluation in Simulated Immature Teeth In Vitro
Emel Uzunoglu Ozyurek, Betül Eren Kaya, Ceren Bayraktutan, Uzay Koç Vural
Dental Traumatology.2026; 42(3): 377. CrossRef - The impact of restoration protocols on the fracture resistance of root canal treated anterior teeth: an in vitro study
Samar Yasir Ahmed Mohamed, Mohamed Adel Eldemellawy, Fatma Adel Mohamed Ahmed
The Saudi Dental Journal.2026;[Epub] CrossRef - Fracture resistance of endodontically treated teeth restored with polyetheretherketone (PEEK) versus glass fiber posts: A comparative in vitro analysis
Manduwada Vishal, Neha Mehra, Mamta Kaushik, Prabakaran Saravanan
Endodontology.2026; 38(2): 172. CrossRef - Influence of Different Post-core Restorative Modalities on Fracture Characteristics of Immature Endodontically Treated Premolars
Wafa H Alaajam, Khalid M Abdelaziz, Malaz M Mustafa, Mohammed S Al-Ak'hali, Ashraf A Khalil, Mohammed M Al Moaleem, Hoda L Abouzeid
The Journal of Contemporary Dental Practice.2026; 27(4): 399. CrossRef - Effect of Ferrule Height on the Fracture Resistance of Endodontically Treated Teeth Restored With Glass Fiber Posts: An In Vitro Study
Sneha Rathaur, Pankaj K Gupta, Sonal Dhote, Kumari S Pravin, Komal Kishlay, Seema Gupta
Cureus.2025;[Epub] CrossRef - Influence of Contracted Endodontic Cavity Design on the Debridement Efficacy of Three Different Irrigant Activation Systems in Human Permanent Mandibular Molars: A Scanning Electron Microscopy Analysis
Srilekha Jayakumar, Vignesh Srinivasan, Janani Karunakaran, Jwaalaa Rajkumar, Vashni Solomon, Aarthi Thiagarajan
World Journal of Dentistry.2025; 16(1): 62. CrossRef - The Effect of Additional Silane Pre-Treatment on the Microtensile Bond Strength of Resin-Based Composite Post-and-Core Build-Up Material
Chia-Ying Wu, Keigo Nakamura, Aya Miyashita-Kobayashi, Akiko Haruyama, Yukiko Yokoi, Akihiro Kuroiwa, Nobuo Yoshinari, Atsushi Kameyama
Applied Sciences.2024; 14(15): 6637. CrossRef - The Influence on Fracture Resistance of Different Composite Resins and Prefabricated Posts to Restore Endodontically Treated Teeth
Saulo Pamato, Weber Adad Ricci, Milton Carlos Kuga, Eliane Cristina Gulin de Oliveira, João Carlos Silos Moraes, Marcus Vinicius Reis Só, Tamara Carolina Trevisan, Newton Fahl Júnior, Jefferson Ricardo Pereira
Polymers.2023; 15(1): 236. CrossRef - Comparison of the pull-out bond strength of endodontically treated anterior teeth with monolithic zirconia endocrown and post-and-core crown restorations
Durmus A. Bozkurt, Emine B. Buyukerkmen, Arslan Terlemez
Journal of Oral Science.2023; 65(1): 1. CrossRef - Minimally invasive access cavities in endodontics
Lubna A Abdulrazaq, Ahmed H Ali, Federico Foschi
Journal of Baghdad College of Dentistry.2023; 35(2): 65. CrossRef - Comparison of Fracture Resistance of Endodontically Treated Teeth With Traditional Endodontic Access Cavity, Conservative Endodontic Access Cavity, Truss Endodontic Access Cavity, and Ninja Endodontic Access Cavity Designs: An In Vitro Study
Prasad Patil , Pooja Newase, Swapnil Pawar, Hasmukh Gosai , Dharmendra Shah, Sameer M Parhad
Cureus.2022;[Epub] CrossRef - Effect of different access cavity designs on fracture toughness of endodontically treated teeth: a systematic review and network meta-analysis
Momina A. Motiwala, Meisha Gul, Robia Ghafoor
Evidence-Based Dentistry.2022;[Epub] CrossRef - Fracture resistance of polyetheretherketone, Ni-Cr, and fiberglass postcore systems: An in vitro study
Hossein Pourkhalili, Donya Maleki
Dental Research Journal.2022; 19(1): 20. CrossRef - The effect of bulk-fill composites: Activa and Smart Dentin Replacement on cuspal deflection in endodontically treated teeth with different access cavity designs
Rupali Karale, BJ Prathima, BR Prashanth, NS Shivaranjan, Neha Jain
Journal of Conservative Dentistry.2022; 25(4): 375. CrossRef - Efficacy of Root Canal Instrumentation and Fracture Strength Assessment in Primary Molars after Preparing Two Different Shapes of Access Cavity: An Ex Vivo Histological Study
Yashika Singhal, Nikhil Srivastava, Vivek Rana, Noopur Kaushik, Vandana Reddy
International Journal of Clinical Pediatric Dentistry.2021; 14(4): 518. CrossRef - MANAGEMENT OF ELISS CLASS IV FRACTURE USING FIBER POST : A CASE REPORT
Shivangi Shreya, Neha Verma
INTERNATIONAL JOURNAL OF SCIENTIFIC RESEARCH.2021; : 13. CrossRef - Effect of intracanal diode laser irradiation on fracture resistance of roots restored with CAD/CAM posts
Flavia Florentino Teixeira da Silva, André Hayato Saguchi, Sidnea Aparecida Freitas Paiva, Guilherme Espósito Pires, Mariana Isidoro, Aldo Brugnera Junior, Paulo Francisco Cesar, Ângela Toshie Araki
Brazilian Journal of Oral Sciences.2021;[Epub] CrossRef - Does ultraconservative access affect the efficacy of root canal treatment and the fracture resistance of two‐rooted maxillary premolars?
A. A. Silva, F. G. Belladonna, G. Rover, R. T. Lopes, E. J. L. Moreira, G. De‐Deus, E. J. N. L. Silva
International Endodontic Journal.2020; 53(2): 265. CrossRef - Effect of Glass Fiber Post Diameter on Fracture Resistance of Endodontically Treated Teeth
Saied Nokar, Mahsa Sadat Mortazavi, Somayeh Niakan
Pesquisa Brasileira em Odontopediatria e Clínica Integrada.2020;[Epub] CrossRef - One‐step fiber post cementation and core build‐up in endodontically treated tooth: A clinical case report
José Mauricio dos Santos Nunes Reis, Carlos R. de Moura Oliveira, Erica G. J. Reis, Bruno A. Mascaro, Filipe de Oliveira Abi‐Rached
Journal of Esthetic and Restorative Dentistry.2020; 32(1): 5. CrossRef - Impact of contracted endodontic cavities on fracture resistance of endodontically treated teeth: a systematic review of in vitro studies
Emmanuel João Nogueira Leal Silva, Gabriela Rover, Felipe Gonçalves Belladonna, Gustavo De-Deus, Cleonice da Silveira Teixeira, Tatiana Kelly da Silva Fidalgo
Clinical Oral Investigations.2018; 22(1): 109. CrossRef - Fracture Strength of Endodontically Treated Teeth with Different Access Cavity Designs
Gianluca Plotino, Nicola Maria Grande, Almira Isufi, Pietro Ioppolo, Eugenio Pedullà, Rossella Bedini, Gianluca Gambarini, Luca Testarelli
Journal of Endodontics.2017; 43(6): 995. CrossRef - Comparison of push-out bond strength of fiber-reinforced composite resin posts according to cement thickness
Jun-Seong Park, Jeong-Sub Lee, Jeong-Won Park, Won-Gyun Chung, Eun-Hee Choi, Yoon Lee
The Journal of Prosthetic Dentistry.2017; 118(3): 372. CrossRef - Tratamiento restaurador de lesiones dentales traumáticas. Reporte de tres casos clínicos
Johann Vladimir Uzcátegui Quintero, Alinne Hernández Ayala, Ricardo González Plata, Enrique Ríos Szalay
Revista Odontológica Mexicana.2017; 21(3): 185. CrossRef - The effects of post and core material combination on the surface strain of the 4-unit zirconia fixed partial denture margins
Yoko ISHIKAWA, Wataru KOMADA, Tasuku INAGAKI, Reina NEMOTO, Satoshi OMORI, Hiroyuki MIURA
Dental Materials Journal.2017; 36(6): 798. CrossRef - Restorative treatment of traumatic dental injuries. Report of three clinical cases
Johann Vladimir Uzcátegui Quintero, Alinne Hernández Ayala, Ricardo González Plata, Enrique Ríos Szalay
Revista Odontológica Mexicana.2017; 21(3): e179. CrossRef
- Can Coronal Restorative Choices Influence Root Strength After RET? A Fracture Resistance Evaluation in Simulated Immature Teeth In Vitro
- 3,710 View
- 27 Download
- 26 Crossref
Case Reports
- An esthetic appliance for the management of crown-root fracture: a case report
- Sang-Min Jeon, Kang-Hee Lee, Bock-Young Jung
- Restor Dent Endod 2014;39(3):226-229. Published online May 22, 2014
- DOI: https://doi.org/10.5395/rde.2014.39.3.226
-
Abstract
PDFPubReaderePub
Orthodontic extrusion is usually performed by means of a fixed orthodontic appliance that utilizes arch wire attached to adjacent teeth and transfers the desired force by elastic from the wire to the root. However, clinicians often encounter cases where the bonding required for tooth traction is not possible because the adjacent teeth have been restored with ceramic or veneer. The purpose of this case report is to describe a modified orthodontic extrusion appliance that is useful when conventional orthodontic treatment is not possible. The modified appliance was fabricated using an artificial tooth, clear plastic sheeting, and a braided fiber-reinforced composite strip that covered adjacent teeth without bonding. It satisfied the esthetic and functional needs of the patient and established the optimal biologic width.
-
Citations
Citations to this article as recorded by- Esthetic enhancement of a traumatized anterior tooth with a combination of forced eruption and tooth alignment: a case report
So-Hee Kang, Jung-Hong Ha, Myoung-Uk Jin, Sung-Kyo Kim, Young-Kyung Kim
Restorative Dentistry & Endodontics.2016; 41(3): 210. CrossRef
- Esthetic enhancement of a traumatized anterior tooth with a combination of forced eruption and tooth alignment: a case report
- 1,927 View
- 5 Download
- 1 Crossref
- Esthetic rehabilitation of single anterior edentulous space using fiber-reinforced composite
- Hyeon Kim, Min-Ju Song, Su-Jung Shin, Yoon Lee, Jeong-Won Park
- Restor Dent Endod 2014;39(3):220-225. Published online May 19, 2014
- DOI: https://doi.org/10.5395/rde.2014.39.3.220
-
Abstract
PDFPubReaderePub
A fiber-reinforced composite (FRC) fixed prosthesis is an innovative alternative to a traditional metal restoration, as it is a conservative treatment method. This case report demonstrates a detailed procedure for restoring a missing anterior tooth with an FRC. A 44-year-old woman visited our department with an avulsed tooth that had fallen out on the previous day and was completely dry. This tooth was replanted, but it failed after one year. A semi-direct technique was used to fabricate a FRC fixed partial prosthesis for its replacement. The FRC framework and the pontic were fabricated using a duplicated cast model and nanofilled composite resin. Later on, interproximal contact, tooth shape, and shade were adjusted at chairside. This technique not only enables the clinician to replace a missing tooth immediately after extraction for minimizing esthetic problems, but it also decreases both tooth reduction and cost.
-
Citations
Citations to this article as recorded by- Anterior provisional fixed partial dentures: A finite element analysis
Nouf Almeganni, Rotana Abulaban, Ghada Naguib, Mohamed Tharwat, Hani M. Nassar
Journal of Prosthodontics.2024; 33(4): 367. CrossRef - FİBERLE GÜÇLENDİRİLMİŞ ADEZİV KÖPRÜLER VE UYGULAMA YÖNTEMLERİ
Gözde YALÇIN, Asude Dilek NALBANT
Atatürk Üniversitesi Diş Hekimliği Fakültesi Dergisi.2022; : 1. CrossRef - Fiber-reinforced composite resin bridges: an alternative method to treat root-fractured teeth
Gun Heo, Eun-Hye Lee, Jin-Woo Kim, Kyung-Mo Cho, Se-Hee Park
Restorative Dentistry & Endodontics.2020;[Epub] CrossRef - A New Technique for Direct Fabrication of Fiber-Reinforced Composite Bridge: A Long-Term Clinical Observation
Matías Ferrán Escobedo Martínez, Samuel Rodríguez López, Jairo Valdés Fontela, Sonsoles Olay García, Mario Mauvezín Quevedo
Dentistry Journal.2020; 8(2): 48. CrossRef - Customized Treatment Option for Malpositioned Dental Implant Placed in Aesthetic Zone
Priyanka N. Khungar, Trupti M. Dahane, Ramnath P. Revankar, Rupali Patel
Journal of Evolution of Medical and Dental Sciences.2020; 9(39): 2930. CrossRef - Fiber reinforced composite bridge as a replacement for missing upper permanent lateral incisor – a case report
Ana Todorović, Danica Popović, Igor Djordjević, Vojkan Lazić
Stomatoloski glasnik Srbije.2016; 63(3): 133. CrossRef - Evaluation of the Viability of Rat Periodontal Ligament Cells after Storing at 0℃/2 MPa Condition up to One Week: In Vivo MTT Method
Sun Mi Jang, Sin-Yeon Cho, Eui-Seong Kim, Il-Young Jung, Seung Jong Lee
Journal of Korean Dental Science.2016; 9(1): 1. CrossRef - Semidirect Restorations in Multidisciplinary Treatment: Viable Option for Children and Teenagers
Mateus Rodrigues Tonetto, Milton Carlos Kuga, Fausto Frizzera, Matheus Coelho Bandeca, Shilpa H Bhandi, Célia Regina Maio Pinzan-Vercelino, Monica Barros da Silva, Kamila Figueiredo Pereira
The Journal of Contemporary Dental Practice.2015; 16(4): 280. CrossRef
- Anterior provisional fixed partial dentures: A finite element analysis
- 2,565 View
- 10 Download
- 8 Crossref
Original Article
- Effect of fiber direction on the polymerization shrinkage of fiber-reinforced composites
- Joongwon Yom, In-Bog Lee
- J Korean Acad Conserv Dent 2009;34(4):364-370. Published online July 31, 2009
- DOI: https://doi.org/10.5395/JKACD.2009.34.4.364
-
Abstract
PDFPubReaderePub
The aim of this study was to evaluate the effect of fiber direction on the polymerization shrinkage of fiber-reinforced composite. The disc-shaped flowable composite specimens (d = 10 mm, h = 2 mm, Aeliteflo A2, Bisco, Inc., IL, USA) with or without glass fiber bundle (X-80821P Glass Fiber, Bisco, Inc., IL, USA) inside were prepared, and the longitudinal and transversal polymerization shrinkage of the specimens on radial plane were measured with strain gages (Linear S-series 350ω, CAS, Seoul, Korea). In order to measure the free polymerization shrinkage of the flowable composite itself, the disc-shaped specimens (d = 7 mm, h = 1 mm) without fiber were prepared, and the axial shrinkage was measured with an LVDT (linear variable differential transformer) displacement sensor. The cross-section of the polymerized specimens was observed with a scanning electron microscope to examine the arrangement of the fiber bundle in composite. The mean polymerization shrinkage value of each specimen group was analyzed with ANOVA and Scheffe post-hoc test (α=0.05).
The radial polymerization shrinkage of fiber-reinforced composite was decreased in the longitudinal direction of fiber, but increased in the transversal direction of fiber (p<0.05). We can conclude that the polymerization shrinkage of fiber-reinforced composite splint or restoratives is dependent on the direction of fiber.
- 1,301 View
- 2 Download
 First
First Prev
Prev

