
Search
- Page Path
- HOME > Search
Case Report
- The application of “bone window technique” using piezoelectric saws and a CAD/CAM-guided surgical stent in endodontic microsurgery on a mandibular molar case
- Ukseong Kim, Sunil Kim, Euiseong Kim
- Restor Dent Endod 2020;45(3):e27. Published online May 21, 2020
- DOI: https://doi.org/10.5395/rde.2020.45.e27
-
 Abstract
Abstract
 PDF
PDF PubReader
PubReader ePub
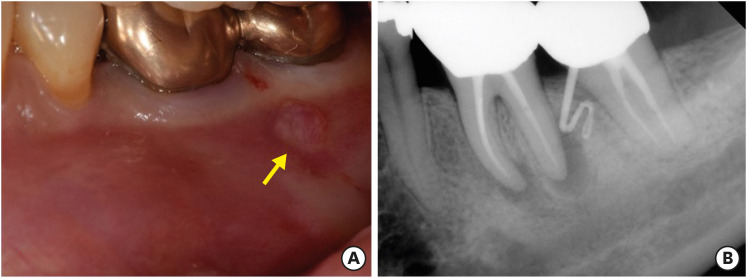
ePub Apical surgery for a mandibular molar is still challenging for many reasons. This report describes the applications of computer-guided cortical ‘bone-window technique’ using piezoelectric saws that prevented any nerve damage in performing endodontic microsurgery of a mandibular molar. A 49-year-old woman presented with gumboil on tooth #36 (previously endodontically treated tooth) and was diagnosed with chronic apical abscess. Periapical lesions were confirmed using cone-beam computed tomography (CBCT). Endodontic microsurgery for the mesial and distal roots of tooth #36 was planned. Following the transfer of data of the CBCT images and the scanned cast to an implant surgical planning program, data from both devices were merged. A surgical stent was designed, on the superimposed three-dimensional model, to guide the preparation of a cortical window on the buccal side of tooth #36. Endodontic microsurgery was performed with a printed surgical template. Minimal osteotomy was required and preservation of the buccal cortical plate rendered this endodontic surgery less traumatic. No postoperative complications such as mental nerve damage were reported. Window technique guided by a computer-aided design/computer-aided manufacture based surgical template can be considerably useful in endodontic microsurgery in complicated cases.
-
Citations
Citations to this article as recorded by
- Optimising Outcomes in Endodontic Microsurgery: Evidence, Uncertainties and Future Directions
Ukseong Kim, Euiseong Kim
International Endodontic Journal.2026; 59(5): 746. CrossRef - Accuracy of Guided Dual Technique in Esthetic Crown Lengthening: A Prospective Case‐Series Study
Meritxell Enfedaque‐Prat, Albert González‐Barnadas, Adrià Jorba‐García, Javi Vilarrasa, Jorge Toledano‐Serrabona, Rui Figueiredo, Eduard Valmaseda‐Castellón, Octavi Camps‐Font
Journal of Esthetic and Restorative Dentistry.2025; 37(6): 1284. CrossRef - Guided endodontics in the application of personalized mini-invasive treatment in clinical cases: a literature review
Shuangshuang Ren, Wanping Wang, Mingyue Cheng, Wenyue Tang, Yue Zhao, Leiying Miao
The Saudi Dental Journal.2025;[Epub] CrossRef - Accurately Defining the Location and Dimension of the Bony Lid Under the Guidance of Dynamic Navigation: Report on Three Cases
Kailiang Tang, Xiaole Zhang, Qibao Wang, Xinyu Zhao, Xijiao Yu, Yi Du
Australian Endodontic Journal.2025; 51(3): 785. CrossRef - Minimally Invasive Vertical Incision Subperiosteal Tunnelling Technique for Targeted Endodontic Surgery: Technical Overview and a Case Report
Francesc Abella Sans, Jaime Barragán Montes, Tomasz Zbozen, Nandini Suresh, Lalli Dharmarajan, Paul M. H. Dummer, Venkateshbabu Nagendrababu
International Endodontic Journal.2025; 58(11): 1799. CrossRef - Endodontic Microsurgery of Mandibular Molars with an Autonomous Robotic System
Haiying Zhang, Zi Yang, Mangnan Liu, Yaoxin Wang, Mei Fu, Benxiang Hou, Chen Zhang
Journal of Endodontics.2025; 51(12): 1830. CrossRef - Endodontic Microsurgery of a Mandibular Molar Using a Dynamic Navigation System (DNS) and Cortical Window Technique: A Case Report
Gustavo Castillo, Silvia Restrepo-Méndez, Oscar Zuluaga, Paola Escobar-Villegas
Journal of Endodontic Microsurgery.2024; 3: 1. CrossRef - The bone lid technique in endodontic microsurgery
Min Zhang, He Liu, Ya Shen
Asian Journal of Surgery.2024; 47(7): 3126. CrossRef - Guided Periradicular Surgery with Er,Cr:YSGG Laser Osteotomy: A Case Report
Julian Torres Celeita, Johanna Hernández la Rotta, Amdie Chirinos Salazar, Jorge Fandiño Rodríguez, Laura López Rincón, Mauren Orduz Solorzano, Diana Parra Galvis, Oscar Jiménez Peña
Journal of Endodontic Microsurgery.2024;[Epub] CrossRef - Piezoelectric Endodontic Microsurgery with Modified Cortical Window Technique: A Case Report
Rafael Fernández-Grisales, Wilder Rojas, Carolina Berruecos-Orozco
Journal of Endodontic Microsurgery.2023; 2: 34. CrossRef - The Impact of the Preferred Reporting Items for Case Reports in Endodontics (PRICE) 2020 Guidelines on the Reporting of Endodontic Case Reports
Sofian Youssef, Phillip Tomson, Amir Reza Akbari, Natalie Archer, Fayjel Shah, Jasmeet Heran, Sunmeet Kandhari, Sandeep Pai, Shivakar Mehrotra, Joanna M Batt
Cureus.2023;[Epub] CrossRef - Clinical and radiological outcomes of dynamic navigation in endodontic microsurgery: a prospective study
Chen Chen, Rui Zhang, Wei Zhang, Fangzhe Li, Zan Wang, Li Qin, Yun Chen, Zhuan Bian, Liuyan Meng
Clinical Oral Investigations.2023; 27(9): 5317. CrossRef - New-designed 3D printed surgical guide promotes the accuracy of endodontic microsurgery: a study of 14 upper anterior teeth
Dan Zhao, Weige Xie, Tianguo Li, Anqi Wang, Li Wu, Wen Kang, Lu Wang, Shiliang Guo, Xuna Tang, Sijing Xie
Scientific Reports.2023;[Epub] CrossRef - Failure case analysis during each stage of endodontic microsurgery: A retrospective study based on clinical databases
Changwoo Ryu, Sooil Shin, Yong-Bum Cho, Euiseong Kim, Minju Song
Saudi Endodontic Journal.2023; 13(2): 160. CrossRef - Piezoelectric Device and Dynamic Navigation System Integration for Bone Window-Guided Surgery
Frederico C. Martinho, Ina L. Griffin, Patricia A. Tordik
Journal of Endodontics.2023; 49(12): 1698. CrossRef - Bone Window Technique in Endodontic Microsurgery – Report of Two Cases
Spyros Floratos, Vasileios Molonis, Apostolos Tsolakis, Stylianos Kykalos, Konstantinos Kontzoglou
Journal of Endodontic Microsurgery.2022; 2: 24. CrossRef - An Update on Endodontic Microsurgery of Mandibular Molars: A Focused Review
Sun Mi Jang, Euiseong Kim, Kyung-San Min
Medicina.2021; 57(3): 270. CrossRef
- Optimising Outcomes in Endodontic Microsurgery: Evidence, Uncertainties and Future Directions
- 3,267 View
- 61 Download
- 17 Crossref

Review Articles
- Biologic response of local hemostatic agents used in endodontic microsurgery
- Youngjune Jang, Hyeon Kim, Byoung-Duck Roh, Euiseong Kim
- Restor Dent Endod 2014;39(2):79-88. Published online March 21, 2014
- DOI: https://doi.org/10.5395/rde.2014.39.2.79
-
Abstract
PDFPubReaderePub
Appropriate use of local hemostatic agent is one of the important factors on the prognosis of endodontic microsurgery. However, most investigations to date focus on the hemostatic efficacy of the agents, whereas their biologic characteristics have not received enough attention. The purpose of this paper was to review the biologic response of local hemostatic agents, and to provide clinical guidelines on their use during endodontic microsurgery. Electronic database (PUBMED) was screened to search related studies from 1980 to 2013, and 8 clinical studies and 18 animal studies were identified. Among the materials used in these studies, most widely-investigated and used materials, epinephrine, ferric sulfate (FS) and calcium sulfate (CS), were thoroughly discussed. Influence of these materials on local tissue and systemic condition, such as inflammatory and foreign body reaction, local ischemia, dyspigmentation, delayed or enhanced bone and soft tissue healing, and potential cardiovascular complications were assessed. Additionally, biological property of their carrier materials, cotton pellet and absorbable collagen, were also discussed. Clinicians should be aware of the biologic properties of local hemostatic agents and their carrier materials, and should pay attention to the potential complications when using them in endodontic microsurgery.
-
Citations
Citations to this article as recorded by- Hemostatic Agents in Periapical Surgery: Systematic Review and Meta-analysis
Fabio Genchi, Juan Antonio Blaya Tárraga, Cristina Palma Carrió, Raquel Estévez Llorens, Isabel Menéndez Nieto
Journal of Endodontics.2026; 52(6): 850. CrossRef - Expert consensus on apical microsurgery
Hanguo Wang, Xin Xu, Zhuan Bian, Jingping Liang, Zhi Chen, Benxiang Hou, Lihong Qiu, Wenxia Chen, Xi Wei, Kaijin Hu, Qintao Wang, Zuhua Wang, Jiyao Li, Dingming Huang, Xiaoyan Wang, Zhengwei Huang, Liuyan Meng, Chen Zhang, Fangfang Xie, Di Yang, Jinhua Yu
International Journal of Oral Science.2025;[Epub] CrossRef - A drug-carrying, multiscene, absorbable biological suture from fish swim bladder
Peng Sun, Hao Cui, Jinwei Zhang, Jingan Li, Changwei Ren, Yongqiang Lai
International Journal of Surgery.2025; 111(10): 6663. CrossRef - Assessing the efficacy of apicoectomy without retrograde filling in treating periapical inflammatory cysts
Jeong-Kui Ku, Woo-Young Jeon, Seung-O Ko, Ji-Young Yoon
Journal of the Korean Association of Oral and Maxillofacial Surgeons.2024; 50(3): 140. CrossRef - Functional and structural neurodegenerative activities of Ankaferd BloodStopper in a mouse sciatic nerve model
Ramazan Üstün, Elif Oğuz, Ayşe Şeker, Filiz Taspinar
Experimental and Therapeutic Medicine.2024;[Epub] CrossRef - Local and Systemic Hemostatic Agents: A Comprehensive Review
Bardia Jamali, Saeed Nouri, Salimeh Amidi
Cureus.2024;[Epub] CrossRef - PLGA Nanoparticle Rapamycin- or Necrostatin-1-Coated Sutures Inhibit Inflammatory Reactions after Arterial Closure in Rats
Liwei Zhang, Wang Wang, Boao Xie, Peng Sun, Shunbo Wei, Haoliang Wu, Cong Zhang, Jingan Li, Zhuo Li, Hualong Bai
ACS Applied Bio Materials.2022; 5(4): 1501. CrossRef - COMPARING THE CLINICAL AND RADIOGRAPHIC OUTCOMES OF PULPOTOMIES IN PRIMARY MOLARS USING BIOACTIVE ENDODONTIC MATERIALS AND FERRIC SULFATE – A SYSTEMATIC REVIEW AND META-ANALYSIS OF RANDOMIZED CLINICAL TRIALS
VELLORE KANNAN GOPINATH, SHAJU JACOB PULIKKOTIL, SAJESH K VEETTIL, LALLI DHARMARAJAN, PONNUDURAI SAMUEL GNANA PRAKASH, VINEET DHAR, JAYAKUMAR JAYARAMAN
Journal of Evidence-Based Dental Practice.2022; 22(4): 101770. CrossRef - Perioperative Antiplatelet and Anticoagulant Management with Endodontic Microsurgical Techniques
Anita Aminoshariae, Mark Donaldson, Michael Horan, James C. Kulild, Dale Baur
Journal of Endodontics.2021; 47(10): 1557. CrossRef - Effect of blood contamination and various hemostatic procedures on the push-out bond strength of Biodentine when used for furcation perforation repair
Shanthana Reddy, Ramya Shenoy, LohithReddy Mandadi, Ishani Saluja, ManuelS Thomas
Journal of Conservative Dentistry.2021; 24(3): 260. CrossRef - Endodontic Perforation Closure by Five Mineral Oxides Silicate-Based Cement with/without Collagen Sponge Matrix
Talal Al-Nahlawi, Maisour Ala Rachi, Amjad Abu Hasna, Zohaib Khurshid
International Journal of Dentistry.2021; 2021: 1. CrossRef - Hemostatic agents in periapical surgery: The systematic review
Z. S. Khabadze, D. A. Nazarova, E. S. Shilyaeva, A. P. Kotelnikova, Yu. A. Bakayev, S. M. Abdulkerimova, Kh. O. Omarova
Endodontics Today.2021; 19(3): 184. CrossRef - An Innovative Bioceramic Bone Graft Substitute for Bone Defect Treatment: In Vivo Evaluation of Bone Healing
Syamsiah Syam, Yung-Chieh Cho, Chung-Ming Liu, Mao-Suan Huang, Wen-Chien Lan, Bai-Hung Huang, Takaaki Ueno, Chi-Hsun Tsai, Takashi Saito, May-Show Chen, Keng-Liang Ou
Applied Sciences.2020; 10(22): 8303. CrossRef - Trial finds better haemostasis with aluminium chloride during periapical surgery
Niall Mc Goldrick, Carly Ross, James Nelson
Evidence-Based Dentistry.2017; 18(2): 50. CrossRef - Comparison of the Hemostatic Activity of Quercus persica Jaub. & Spach. (Oak) With Ferric Sulfate in Bony Crypts
Mohammad Reza Nabavizadeh, Arman Zargaran, Fariborz Moazami, Fatemeh Askari, Safoora Sahebi, Alireza Farhadpoor, Pouya Faridi
Journal of Evidence-Based Complementary & Alternative Medicine.2016; 21(1): 34. CrossRef - Effect of the plant-based hemostatic agent Ankaferd Blood Stopper® on the biocompatibility of mineral trioxide aggregate
Muzaffer Emir Dinçol, Hakan Ozbas, Bulent Yılmaz, Handan Ersev, Selcuk Gokyay, Vakur Olgac
BMC Oral Health.2016;[Epub] CrossRef
- Hemostatic Agents in Periapical Surgery: Systematic Review and Meta-analysis
- 3,850 View
- 27 Download
- 16 Crossref
- Cardiovascular effect of epinephrine in endodontic microsurgery: a review
- Youngjune Jang, Euiseong Kim
- Restor Dent Endod 2013;38(4):187-193. Published online November 12, 2013
- DOI: https://doi.org/10.5395/rde.2013.38.4.187
-
Abstract
PDFPubReaderePub
Epinephrine is one of the most widely-used vasoconstrictors in dental treatment including endodontic microsurgery. However, the systemic safety of epinephrine has been in debate for many years because of its potential risk to cause cardiovascular complications. The purpose of this review was to assess the cardiovascular effect of epinephrine use in endodontic microsurgery. Endodontic microsurgery directly applies epinephrine into the bone cavity, and the amount is reported to be much larger than other dental surgeries. Moreover, when considering that systemic potency of intraosseous application is reported to be comparable to intravenous application, the systemic influence of epinephrine could be increased in endodontic microsurgery. Besides, pre-existing cardiovascular complications or drug interactions can enhance its systemic influence, resulting in increased susceptibility to cardiovascular complications. Although clinical studies have not reported significant complications for patients without severe systemic complications, many epinephrine-induced emergency cases are warning the cardiovascular risk related with pre-existing systemic disease or drug interactions. Epinephrine is a dose-sensitive drug, and its hypersensitivity reaction can be fatal to patients when it is related to cardiovascular complications. Therefore, clinicians should recognize the risk, and the usage of pre-operative patient evaluation, dose control and patient monitoring are required to ensure patient's safety during endodontic microsurgery.
-
Citations
Citations to this article as recorded by- Expert consensus on apical microsurgery
Hanguo Wang, Xin Xu, Zhuan Bian, Jingping Liang, Zhi Chen, Benxiang Hou, Lihong Qiu, Wenxia Chen, Xi Wei, Kaijin Hu, Qintao Wang, Zuhua Wang, Jiyao Li, Dingming Huang, Xiaoyan Wang, Zhengwei Huang, Liuyan Meng, Chen Zhang, Fangfang Xie, Di Yang, Jinhua Yu
International Journal of Oral Science.2025;[Epub] CrossRef - Comparative Evaluation of Local Hemostatic Agents in Minor Oral Surgical Procedures: A Randomized Clinical Trial
Kshitija Patil, Jay N Goyal, Saurabh Dudhe, Janice John, Simona Joseph, Sanchi Kadbe, Seema Gupta
Cureus.2025;[Epub] CrossRef - Pharmacological Interactions of Epinephrine at Concentrations Used in Dental Anesthesiology: An Updated Narrative Review
Maria Aikaterini Saraga, Ioannis Fotopoulos, Vasileios Zisis, Athanasios Poulopoulos, Nikolaos Dabarakis, Theodoros Lillis
Reports.2025; 8(4): 224. CrossRef - Effects of nasal desmopressin spray versus topical epinephrine on surgical field clarity and hemodynamics in endonasal dacryocystorhinostomy: a randomized clinical study
Mohamed G.M. El Sayed, Marwa M. Medhat, Dina A.E. Salem, Marwa A.M. Khedr, Alshaimaa A.F. Kamel
Research and Opinion in Anesthesia & Intensive Care.2024; 11(1): 1. CrossRef - Is 1:1000 adrenaline as a topical haemostat an effective alternative to control bleeding in dentistry and oral surgery?
Raj D. Aslam, Jonathan Liew, Eleni Besi
British Dental Journal.2023; 235(1): 29. CrossRef - Effect of Flumazenil on Emergence Agitation after Orthognathic Surgery: A Randomized Controlled Trial
Young Hyun Koo, Geun Joo Choi, Hyun Kang, Yong Hun Jung, Young Cheol Woo, Young-Jun Choi, Chong Wha Baek
Journal of Personalized Medicine.2022; 12(3): 416. CrossRef - Hemostatic agents in periapical surgery: The systematic review
Z. S. Khabadze, D. A. Nazarova, E. S. Shilyaeva, A. P. Kotelnikova, Yu. A. Bakayev, S. M. Abdulkerimova, Kh. O. Omarova
Endodontics Today.2021; 19(3): 184. CrossRef - THE EFFECT OF ADRENALINE ON DYNAMICS OF CARBOHYDRATE METABOLISM INDICES IN RATS
S. Shkurashivska, H. Ersteniuk
Visnyk of Lviv University. Biological series.2017; (75): 151. CrossRef - The Correlation between the Blood Sugar and Allergy of the Trauma Patient
Jeong Soo Lee, Sung Hee Hyun, Ji-Sook Lee, In Sik Kim
Korean Journal of Clinical Laboratory Science.2014; 46(1): 22. CrossRef - Biologic response of local hemostatic agents used in endodontic microsurgery
Youngjune Jang, Hyeon Kim, Byoung-Duck Roh, Euiseong Kim
Restorative Dentistry & Endodontics.2014; 39(2): 79. CrossRef
- Expert consensus on apical microsurgery
- 2,806 View
- 10 Download
- 10 Crossref
- Is stopping of anticoagulant therapy really required in a minor dental surgery? - How about in an endodontic microsurgery?
- Yong-Wook Cho, Euiseong Kim
- Restor Dent Endod 2013;38(3):113-118. Published online August 23, 2013
- DOI: https://doi.org/10.5395/rde.2013.38.3.113
-
Abstract
PDFPubReaderePub
Nowadays, oral anticoagulants are commonly prescribed to numerous patients for preventing cardiovascular accident such as thromboembolism. An important side effect of anticoagulant is anti-hemostasis. In a major surgery, the oral anticoagulant therapy (OAT) regimen must be changed before the surgery for proper post-operative bleeding control. However, in a minor dental surgery and endodontic surgery, the necessity for changing or discontinuing the OAT is open to debate. In this study, risks of the consequences were weighed and analyzed. In patients who stop the OAT, the occurrence of thromboembolic complication is rare but the result is fatal. In patients who continuing the OAT, post-operative bleeding can be controlled well with the local hemostatic measures. In the endodontic surgery, there are almost no studies about this issue. The intra-operative bleeding control is particularly important in the endodontic surgery because of its delicate and sensitive procedures such as inspection of resected root surface using dental microscope and retrograde filling. Further studies are necessary about this issue in the viewpoint of endodontic surgery.
-
Citations
Citations to this article as recorded by- Expert consensus on apical microsurgery
Hanguo Wang, Xin Xu, Zhuan Bian, Jingping Liang, Zhi Chen, Benxiang Hou, Lihong Qiu, Wenxia Chen, Xi Wei, Kaijin Hu, Qintao Wang, Zuhua Wang, Jiyao Li, Dingming Huang, Xiaoyan Wang, Zhengwei Huang, Liuyan Meng, Chen Zhang, Fangfang Xie, Di Yang, Jinhua Yu
International Journal of Oral Science.2025;[Epub] CrossRef - Management of Patients Receiving Anticoagulation Therapy in Dental Practice: A Systematic Review
Francesco Inchingolo, Angelo Michele Inchingolo, Fabio Piras, Laura Ferrante, Antonio Mancini, Andrea Palermo, Alessio Danilo Inchingolo, Gianna Dipalma
Healthcare.2024; 12(15): 1537. CrossRef - Hemostatic Alginate/Nano-Hydroxyapatite Composite Aerogel Loaded with Tranexamic Acid for the Potential Protection against Alveolar Osteitis
Mai El Halawany, Randa Latif, Mohamed H. H. AbouGhaly
Pharmaceutics.2022; 14(10): 2255. CrossRef - Perioperative Antiplatelet and Anticoagulant Management with Endodontic Microsurgical Techniques
Anita Aminoshariae, Mark Donaldson, Michael Horan, James C. Kulild, Dale Baur
Journal of Endodontics.2021; 47(10): 1557. CrossRef - Administration of Coagulation-Altering Therapy in the Patient Presenting for Oral Health and Maxillofacial Surgery
Thomas M. Halaszynski
Oral and Maxillofacial Surgery Clinics of North America.2016; 28(4): 443. CrossRef - Biologic response of local hemostatic agents used in endodontic microsurgery
Youngjune Jang, Hyeon Kim, Byoung-Duck Roh, Euiseong Kim
Restorative Dentistry & Endodontics.2014; 39(2): 79. CrossRef - Cardiovascular effect of epinephrine in endodontic microsurgery: a review
Youngjune Jang, Euiseong Kim
Restorative Dentistry & Endodontics.2013; 38(4): 187. CrossRef
- Expert consensus on apical microsurgery
- 2,993 View
- 6 Download
- 7 Crossref
- Does apical root resection in endodontic microsurgery jeopardize the prosthodontic prognosis?
- Sin-Yeon Cho, Euiseong Kim
- Restor Dent Endod 2013;38(2):59-64. Published online May 28, 2013
- DOI: https://doi.org/10.5395/rde.2013.38.2.59
-
Abstract
PDFPubReaderePub
Apical surgery cuts off the apical root and the crown-to-root ratio becomes unfavorable. Crown-to-root ratio has been applied to periodontally compromised teeth. Apical root resection is a different matter from periodontal bone loss. The purpose of this paper is to review the validity of crown-to-root ratio in the apically resected teeth. Most roots have conical shape and the root surface area of coronal part is wider than apical part of the same length. Therefore loss of alveolar bone support from apical resection is much less than its linear length.The maximum stress from mastication concentrates on the cervical area and the minimum stress was found on the apical 1/3 area. Therefore apical root resection is not so harmful as periodontal bone loss. Osteotomy for apical resection reduces longitudinal width of the buccal bone and increases the risk of endo-perio communication which leads to failure. Endodontic microsurgery is able to realize 0 degree or shallow bevel and precise length of root resection, and minimize the longitudinal width of osteotomy. The crown-to-root ratio is not valid in evaluating the prosthodontic prognosis of the apically resected teeth. Accurate execution of endodontic microsurgery to preserve the buccal bone is essential to avoid endo-perio communication.
-
Citations
Citations to this article as recorded by- Coexistence of horizontal bone loss and dehiscence with the bundle and conventional fiber post: a finite element analysis
Deniz Yanık, Nurullah Türker, Ahmet Mert Nalbantoğlu
Computer Methods in Biomechanics and Biomedical Engineering.2026; 29(5): 1007. CrossRef - Influence of apical root resection level and filling technique on the fracture resistance of endodontically treated teeth: a biomechanical study
Guilherme Pauletto, Sidnei Flores de Pellegrin, Yasmin Padoin, Andressa Weber Vargas, Duvan Cala Castillo, Gabriel Kalil Rocha Pereira, Carlos Alexandre Souza Bier, Renata Dornelles Morgental
Odontology.2026; 114(3): 1248. CrossRef - Expert consensus on apical microsurgery
Hanguo Wang, Xin Xu, Zhuan Bian, Jingping Liang, Zhi Chen, Benxiang Hou, Lihong Qiu, Wenxia Chen, Xi Wei, Kaijin Hu, Qintao Wang, Zuhua Wang, Jiyao Li, Dingming Huang, Xiaoyan Wang, Zhengwei Huang, Liuyan Meng, Chen Zhang, Fangfang Xie, Di Yang, Jinhua Yu
International Journal of Oral Science.2025;[Epub] CrossRef - Approaches in apical microsurgery: conventional vs. guided. A systematic review
Germán Sánchez-Herrera, Matteo Facchera, Cristina Palma-Carrió, Martín Pérez-Leal
Oral and Maxillofacial Surgery.2025;[Epub] CrossRef - The tooth survival of non‐surgical root‐filled posterior teeth and the associated prognostic tooth‐related factors: A systematic review and meta‐analysis
S. R. Patel, F. Jarad, E. Moawad, A. Boland, J. Greenhalgh, Maria Liu, Michelle Maden
International Endodontic Journal.2024; 57(10): 1404. CrossRef - New-designed 3D printed surgical guide promotes the accuracy of endodontic microsurgery: a study of 14 upper anterior teeth
Dan Zhao, Weige Xie, Tianguo Li, Anqi Wang, Li Wu, Wen Kang, Lu Wang, Shiliang Guo, Xuna Tang, Sijing Xie
Scientific Reports.2023;[Epub] CrossRef - Multifactorial Analysis of Endodontic Microsurgery Using Finite Element Models
Raphael Richert, Jean-Christophe Farges, Jean-Christophe Maurin, Jérôme Molimard, Philippe Boisse, Maxime Ducret
Journal of Personalized Medicine.2022; 12(6): 1012. CrossRef - Mid‐term outcomes and periodontal prognostic factors of autotransplanted third molars: A retrospective cohort study
Ernest Lucas‐Taulé, Marc Llaquet, Jesús Muñoz‐Peñalver, José Nart, Federico Hernández‐Alfaro, Jordi Gargallo‐Albiol
Journal of Periodontology.2021; 92(12): 1776. CrossRef - Effect of length of apical root resection on the biomechanical response of a maxillary central incisor in various occlusal relationships
S. J. Ran, X. Yang, Z. Sun, Y. Zhang, J. X. Chen, D. M. Wang, B. Liu
International Endodontic Journal.2020; 53(1): 111. CrossRef - Changes of Root Length and Root-to-Crown Ratio after Apical Surgery: An Analysis by Using Cone-beam Computed Tomography
Thomas von Arx, Simon S. Jensen, Michael M. Bornstein
Journal of Endodontics.2015; 41(9): 1424. CrossRef - Influence of Apical Root Resection on the Biomechanical Response of a Single-rooted Tooth—Part 2: Apical Root Resection Combined with Periodontal Bone Loss
Youngjune Jang, Hyoung-Taek Hong, Heoung-Jae Chun, Byoung-Duck Roh
Journal of Endodontics.2015; 41(3): 412. CrossRef - Influence of Apical Root Resection on the Biomechanical Response of a Single-rooted Tooth: A 3-dimensional Finite Element Analysis
Youngjune Jang, Hyoung-Taek Hong, Byoung-Duck Roh, Heoung-Jae Chun
Journal of Endodontics.2014; 40(9): 1489. CrossRef
- Coexistence of horizontal bone loss and dehiscence with the bundle and conventional fiber post: a finite element analysis
- 3,236 View
- 26 Download
- 12 Crossref
- Success and failure of endodontic microsurgery
- Minju Song, Euiseong Kim
- J Korean Acad Conserv Dent 2011;36(6):465-476. Published online November 30, 2011
- DOI: https://doi.org/10.5395/JKACD.2011.36.6.465
-
Abstract
PDFPubReaderePub
In current endodontic practice, introduction of operating microscope, ultrasonic instruments, and microinstruments has induced a big change in the field of surgical retreatment. In this study, we aimed to offer key steps of endodontic microsurgery procedure compared with traditional root-end surgery, and to evaluate factors influencing success and failure based on published articles.
Endodontic microsurgery is a surgical procedure performed with the aid of a microscope, ultrasonic instruments and modern microsurgical instruments. The microscope provides magnification and illumination - essential for identifying minute details of the apical anatomy. Ultrasonic instruments facilitate the precise root-end preparation that is within the anatomical space of the canal. Modern endodontics can therefore be performed with precision and predictability, thus eliminating the disadvantages inherent in traditional periapical surgery such as large osteotomy, beveled apicoectomy, inaccurate root-end preparation and the inability to observe isthmus.
Factors influencing the outcomes of endodontic microsurgery may be diverse, but standardization of procedures can minimize its range. Among patient and tooth-related factors, periodontal status and tooth position are known to be prognostic, but there are only few articles concerning this matter. High-evidence randomized clinical trials or prospective cohort studies are needed to confirm these findings.
-
Citations
Citations to this article as recorded by- Treatment-Related Factors Affecting the Success of Endodontic Microsurgery and the Influence of GTR on Radiographic Healing—A Cone-Beam Computed Tomography Study
Daniel Bieszczad, Jarosław Wichlinski, Tomasz Kaczmarzyk
Journal of Clinical Medicine.2023; 12(19): 6382. CrossRef - Factors Affecting the Success of Endodontic Microsurgery: A Cone-Beam Computed Tomography Study
Daniel Bieszczad, Jaroslaw Wichlinski, Tomasz Kaczmarzyk
Journal of Clinical Medicine.2022; 11(14): 3991. CrossRef - Comparison of Clinical Outcomes of Endodontic Microsurgery: 1 Year versus Long-term Follow-up
Minju Song, Taekjin Nam, Su-Jung Shin, Euiseong Kim
Journal of Endodontics.2014; 40(4): 490. CrossRef - The Influence of Bone Tissue Deficiency on the Outcome of Endodontic Microsurgery: A Prospective Study
Minju Song, Sahng Gyoon Kim, Su-Jung Shin, Hyeon-Cheol Kim, Euiseong Kim
Journal of Endodontics.2013; 39(11): 1341. CrossRef - Prognostic Factors of Clinical Outcomes in Endodontic Microsurgery: A Prospective Study
Minju Song, Sahng Gyoon Kim, Seung-Jong Lee, Baekil Kim, Euiseong Kim
Journal of Endodontics.2013; 39(12): 1491. CrossRef - Is stopping of anticoagulant therapy really required in a minor dental surgery? - How about in an endodontic microsurgery?
Yong-Wook Cho, Euiseong Kim
Restorative Dentistry & Endodontics.2013; 38(3): 113. CrossRef
- Treatment-Related Factors Affecting the Success of Endodontic Microsurgery and the Influence of GTR on Radiographic Healing—A Cone-Beam Computed Tomography Study
- 3,211 View
- 41 Download
- 6 Crossref
 First
First Prev
Prev

