
Articles
- Page Path
- HOME > Restor Dent Endod > Volume 46(4); 2021 > Article
- Research Article Push-out bond strength and marginal adaptation of apical plugs with bioactive endodontic cements in simulated immature teeth
-
Maria Aparecida Barbosa de Sá1
 , Eduardo Nunes1, Alberto Nogueira da Gama Antunes1, Manoel Brito Júnior2, Martinho Campolina Rebello Horta1, Rodrigo Rodrigues Amaral1, Stephen Cohen3, Frank Ferreira Silveira1
, Eduardo Nunes1, Alberto Nogueira da Gama Antunes1, Manoel Brito Júnior2, Martinho Campolina Rebello Horta1, Rodrigo Rodrigues Amaral1, Stephen Cohen3, Frank Ferreira Silveira1 -
Restor Dent Endod 2021;46(4):e53.
DOI: https://doi.org/10.5395/rde.2021.46.e53
Published online: October 20, 2021
1Department of Dentistry, Pontifical Catholic University of Minas Gerais, Belo Horizonte, Minas Gerais, Brazil.
2Department Dentistry, Montes Claros, Minas Gerais, Brazil.
3Department of Endodontics, Arthur School of Dentistry, University of the Pacific, San Francisco, CA, USA.
- Correspondence to Frank Ferreira Silveira, DDS, MSc, PhD. Adjunct Professor, Department of Dentistry, Pontifical Catholic University of Minas Gerais, Avenida Dom José Gaspar, 500, Minas Gerais, Belo Horizonte 3035610, Brazil. frankfoui@uol.com.br
• Received: June 2, 2020 • Revised: October 18, 2020 • Accepted: October 22, 2020
Copyright © 2021. The Korean Academy of Conservative Dentistry
This is an Open Access article distributed under the terms of the Creative Commons Attribution Non-Commercial License (https://creativecommons.org/licenses/by-nc/4.0/) which permits unrestricted non-commercial use, distribution, and reproduction in any medium, provided the original work is properly cited.
Abstract
-
Objectives This study evaluates the bond strength and marginal adaptation of mineral trioxide aggregate (MTA) Repair HP and Biodentine used as apical plugs; MTA was used as reference material for comparison.
-
Materials and Methods A total of 30 single-rooted teeth with standardized, artificially created open apices were randomly divided into 3 groups (n = 10 per group), according to the material used to form 6-mm-thick apical plugs: group 1 (MTA Repair HP); group 2 (Biodentine); and group 3 (white MTA). Subsequently, the specimens were transversely sectioned to obtain 2 (cervical and apical) 2.5-mm-thick slices per root. Epoxy resin replicas were observed under a scanning electron microscope to measure the gap size at the material/dentin interface (the largest and smaller gaps were recorded for each replica). The bond strength of the investigated materials to dentin was determined using the push-out test. The variable bond strengths and gap sizes were evaluated independently at the apical and cervical root dentin slices. Data were analyzed using descriptive and analytic statistics.
-
Results The comparison between the groups regarding the variables' bond strengths and gap sizes showed no statistical difference (p > 0.05) except for a single difference in the smallest gap at the cervical root dentin slice, which was higher in group 3 than in group 1 (p < 0.05).
-
Conclusions The bond strength and marginal adaptation to root canal walls of MTA HP and Biodentine cement were comparable to white MTA.
INTRODUCTION
White mineral trioxide aggregate (MTA) is considered the gold standard for the single-visit apexification technique [1,2]. However, this material presents certain shortcomings including a long set-up time and handling difficulties [3]. Recently, a new type of MTA known as MTA Repair HP (Angelus, Londrina, Brazil) has been proposed. This cement comprises a vehicle containing both water and an organic plasticizer, resulting in greater plasticity, higher flow, and improved handling characteristics in comparison to white MTA (Angelus, Londrina, Brazil) [4]. In addition, the substitution of tungstate for bismuth oxide used as the radiopacifier has been shown to reduce the incidence of coronal color change [5,6].
Another commercially available bioactive material is Biodentine (Septodont, Saint-Maur-des-Fossés, France), which also offers color stability and is easier to apply in several clinical procedures including the management of immature necrotic teeth [7,8].
During apexification procedures, the apical plug must be able to remain bonded to the root canal walls without displacement while maintaining the dentin/material interfacial integrity either by frictional retention or adhesion [9,10].
Limited information is available concerning MTA HP and Biodentine cement performance in terms of adhesion and adaptation to root dentin in teeth with open apices. Considering the desirable properties of these materials, evaluations of the strength of the interfacial dentin when using the apical plug technique are pertinent [8]. In this context, the present study evaluated the bond strength and marginal adaptation of MTA HP and Biodentine cements when used as apical plugs in an ex vivo apexification model; MTA was used as reference material for comparison. The following hypothesis was tested: No differences between the 3 types of cement regarding the pertinent properties will be observed.
MATERIALS AND METHODS
The sample size for the primary outcome (push-out bond strength) was estimated from a given effect size f value of 0.72 calculated by a similar previous study, using a level of significance of 5% and a power of 90%, into a one-way analysis of variance (ANOVA) (G*Power 3.1.9.7 for Macintosh; Heinrich Heine, Universität Düsseldorf, Dusseldorf, Germany) [11]. The estimated total sample size was 30 for the 3 study groups (10 samples for each group). A total of 30 extracted single-rooted permanent human teeth were selected after the study was approved by the scientific review committee (protocol #2.660.333) of the local university.
Any extraneous tissue and calculus were removed using curettes; teeth with straight roots and similar lengths were selected. The specimens were analyzed under 13× magnification (M-900, Df Vasconcelos, São Paulo, Brazil). Teeth presenting caries, cracks/fractures, internal/external resorption, or root filled were excluded. Mesiodistal and buccolingual radiographs were used to ensure the complete root formation of the selected teeth. Prior to sectioning, the specimens were stored in sterile saline (0.9%) for 7 days at room temperature in a 100% moist environment.
To simulate an immature tooth, an open apex model was created by sectioning the dental crowns to the cemento-enamel junction using a low-speed diamond saw (S.S. White Artigos Dentários, Rio de Janeiro, Brazil) [12,13]. The roots were also sectioned in the apical portion to standardize root length at 13 mm. Subsequently, 3 mm of the apical third were removed to eliminate apical deltas and to standardize the canal exit at the center of the root, thereby maintaining a root length of 10 mm. The open apices were artificially created using Gates Glidden drills #6-1 (Dentsply Sirona, Baden, Switzerland) in a crown-down manner until the #1 bur passed through the apical foramen. Apical preparation divergence was conducted through retrograde instrumentation with a #40 taper 0.6 mm Reciproc instrument (VDW, Munich, Germany) inserted up to the length of the cutting blade and reaching a 1.36-mm-diameter in the foramen.
The canals were irrigated using conventional needle irrigation 23-G (2 mL after every instrument) coupled with a 3-mL syringe with a 5.25% sodium hypochlorite solution (VDW). After removing the smear layer with 5 mL of a 17% EDTA solution (Biodinâmica Química e Farmacêutica, Ibiporã, PR, Brazil) for 5 minutes, a final rinse consisting of 10-mL distilled water was used; the canals were then dried with #80 absorbing paper points (Tanari-Tanariman Indústrial, Manacapuru, AM, Brazil).
The samples were randomly divided into 3 groups according to the material used as an apical plug (n = 10 per group): group 1 – MTA Repair HP (Angelus); group 2 – Biodentine (Septodont); group 3 – white MTA (Angelus) (Table 1). The materials were manipulated according to the manufacturers’ recommendations, and their insertion into the root canal was aided by an MTA carrier (Angelus) using the microscopic view (M-900; Df Vasconcelos) at 13× magnification. Material condensation was performed with hand pluggers (Odous de Deus, Belo Horizonte, MG, Brazil) under ultrasound vibration by means of an ultrasonic device (ENAC; Osada, Los Angeles, CA, USA) for 5 seconds to form 6-mm-thick apical plugs. The thickness and quality of the apical plugs, as well as the coronal space, were verified using Schilder hand pluggers with cursors and through mesiodistal and buccolingual radiographs. A moistened foam was used to simulate periapical tissue characteristics and offer slight resistance to material extrusion [13]. The roots were stored at 37°C in a 100% moist environment for 7 days prior to cutting procedures.
Table 1
Composition of calcium silicate cements used, along with the manufacture instruction of its manipulation
The specimens were fixed to acrylic plates with wax (Asfer Indústria Química, São Caetano do Sul, SP, Brazil) so that the long axis of the root remained parallel to the plate surface. Next, the plates were coupled to a precision cutting machine (Buehler, Lake Bluff, IL, USA) fitted with a high-precision diamond disc (Buehler). The apical part of each specimen was then cut perpendicularly to the long axis at 350 rpm under continuous water cooling, producing 2 (cervical and apical) 2.5-mm-thick slices. The thickness of each slice was verified using a digital caliper (precision level +/− 0.001 mm).
The apical surface of each root slice was uniformly polished with 600-, 1200-, and 2000-grit SiC papers (3M ESPE, São Paulo, Brazil) for 10 seconds each. The surface needed to be polished in order to flatten the surface and eliminate roughness caused by the diamond saw as a rough surface would make it difficult to interpret images during SEM analysis. In addition, polishing to flatten the surface makes GAPS measurement more reliable as the assessment points are at the same height. After polishing, the specimens were washed with distilled water and dried with air blasts. Impressions of the root slice surfaces were obtained using a polyvinylsiloxane material (Aquasil ULV; Dentsply De Tray, Konstanz, Germany) delivered through microtip syringes. After 5 minutes, the impressions were removed from the root slices, and replicas were obtained with a low-viscosity epoxy resin (Polipox Indústria e Comércio, São Paulo, Brazil).
Resin replicas were fixated in aluminum stubs and sputter-coated with gold for SEM analysis of gaps between the apical plug and the dentin walls. The replicas were photographed at 60× and 700× magnifications, and interfacial gap measurements (μm) were performed by one calibrated and blinded examiner with the aid of the SEM Control User Interface software (Version 2.01, 2008, 2009; JEOL Technics, Tokyo, Japan). The largest and smaller gaps were recorded for each replica [14].
After 2 weeks of cement placements, the push-out test was performed on the original root slices individually positioned on a stainless steel base (2.5-mm orifice diameter) fixed to the testing machine (Instron Model 3344; Instron, Norwood, MA, USA). Slice positioning was performed in the same direction as the metal base orifice with the cervical face turned down.
A metal rod with an active 1-mm-diameter tip fixed in the superior portion of the testing machine was positioned over the apical plug, and the push-out test was conducted at 0.5 mm/min until the material was dislodged.
The newtons of force was divided by the internal area of the radicular dentin. The surface area was obtained using the following formula: A = π(R2+R1) [h2 + (R2-R1)2]0.5, where π = 3.14, R2 = coronal radius of the plug (larger radius), R1 = apical radius of the plug (smaller radius), and h = slice width.
The D'Agostino-Pearson test was applied to verify data distribution. An overall normal distribution was noted for the variable bond strength, while no normal distribution was verified for the variable gap size.
The 1-way ANOVA and Tukey's post-hoc test were used to assess differences in the variable bond strength between the 3 groups. This analysis was performed independently for the apical and cervical root dentin slices and for the mean values of both slices.
The Kruskal-Wallis test and Dunn's post-hoc test were conducted to assess differences in the variable gap size between the 3 groups. This analysis was performed independently for the apical section and for the cervical section as well as for the largest and the smallest gap.
All analyses were performed using GraphPad Prism software (Version 6.05; GraphPad Software, San Diego, CA, USA) at a significance level of 5%.
RESULTS
The push-out test results did not reveal significant differences in the bond strength variable between the 3 assessed groups, including apical and cervical root dentin slices as well as the mean values of both slices (p > 0.05; Table 2). No significant differences in the gap-size variable were noted in the SEM photomicrographic analyses of positive replicas between the 3 evaluated groups, either for apical or for cervical root dentin slices, independently evaluating both the largest and the smallest gap (p > 0.05; Table 3; Figure 1). A single exception was the difference in regard to the smallest gap at the cervical root dentin slice, which was higher in group 3 than in group 1 (p < 0.05; Table 3; Figure 1).
Table 2
Means and standard deviations of the bond strength values and comparisons among the investigated groups
Table 3
Median, minimum and maximum gap values and comparisons among groups
Figure 1
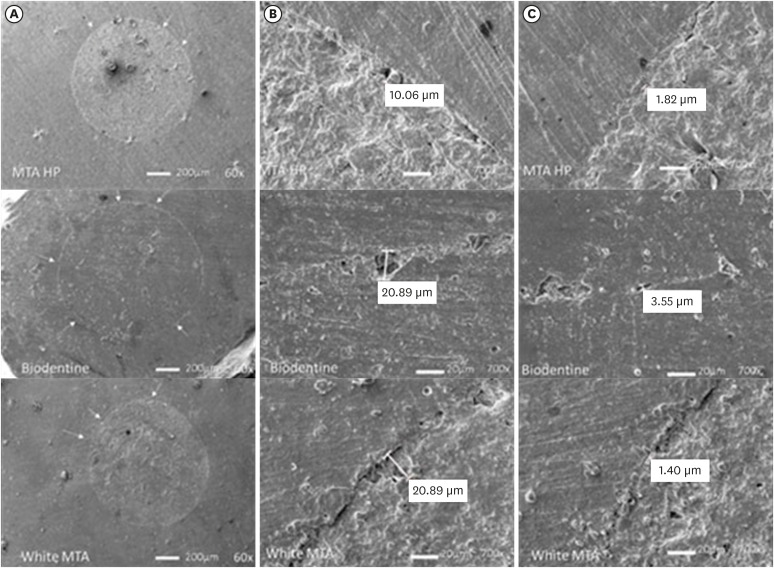
Scanning electron microscope resin replica photomicrographies of HP MTA, Biodentine and white MTA cements. Plug circumference (A); Largest gap (B); Smallest gap (C). Arrows indicate small defects seen at 60× magnification. The largest and smallest gaps are shown at 700×.
MTA, mineral trioxide aggregate.
DISCUSSION
The use of bioactive calcium silicate cement continues to spread and has gained increasing attention in the dental literature, especially in the field of endodontics. The satisfactory characteristics of this cement make it an excellent candidate for several clinical procedures including apexification [2,15].
Bond strength and marginal adaptation are crucial and desirable properties for all materials used for endodontic purposes, and failure to ensure these characteristics is one of the main causes of root canal treatment failure [16,17]. In the present study, the results for MTA HP, Biodentine, and white MTA cements revealed similar bond strength and marginal adaptation.
As in other studies, bond strength was assessed in vitro using the push-out test, a widely accepted method used to estimate the adherence of a certain material to root dentin simulating clinical stresses [18,19,20]. However, when comparing the 3 types of cement, no significant difference was observed, and the chemical/molecular similarity of the 3 materials may be a possible justification for this result. Few studies, however, have compared the bond strengths of MTA HP, Biodentine, and white MTA, thus limiting direct comparisons of these results with those reported in other investigations [21].
Previous assessments have also reported no significant differences when comparing the bond strength of MTA Angelus, ProRoot MTA, and Biodentine cements used as root-filling material, thereby corroborating the results presented herein [22].
By contrast, Silva et al. [23], in one of the few articles comparing white MTA, MTA HP, and Biodentine cements, observed significantly different performances when evaluating bond-strength values. The authors reported that Biodentine presented higher resistance values than MTA HP and white MTA. MTA and Biodentine particle-size variations and the high plasticity of MTA HP were 2 of the factors cited as justifications for this result [23].
According to Bodanezi et al. [24], restorative procedures with MTA should be postponed for at least 72–96 hours after mixing to allow the material to attain its ideal physical properties. Moreover, Bachoo et al. [25] reported that the initial reaction of Biodentine takes approximately 12 minutes, but the delivery of complete maturation takes 2 weeks to 1 month. Such factors could justify the non-significant but lower values of bond strength when compared to MTA.
The other property evaluated was marginal adaptation quality. The presence of marginal gaps between the cement and the root dentin can potentially be responsible for apical infiltration, allowing bacteria and their by-products to permeate the periapical tissue and generating several pathologies [26]. Thus, this property becomes critically important in the selection of material to be used in apexification procedures [27].
There are a variety of different approaches to testing marginal adaptation quality, including microleakage methods such as the dye penetration method, electrical method, the fluid filtration technique, radioisotope tracing, and marginal adaptation by SEM [28]. In accordance with several studies, SEM was applied to assess the quality of marginal cement adaptation due to its ability to provide high magnification and suitable resolution [29,30]. In this study, a SEM was utilized for marginal gap assessment. In SEM, the defects at the submicron level can be observed at required magnification, and final evaluations can be performed by preserving microphotographs.
In spite of the precautions taken, the process of preparing biological samples for analysis may be associated with the introduction of artifacts, consequently resulting in alterations. Evaporation under high vacuum and dehydration for sample spray coating culminate in expansion and/or contraction processes, which can, in turn, cause cracking in hard tissues and lead to the filling material shifting from the surrounding dental structure [31]. In the present study, the replication technique was used in order to mitigate these adverse situations and corroborate with other studies that have reported the successful use of this method [32,33]. According to Teaford et al. [34] and Gondim et al. [35], the replicas accurately maintain the details of the copied structure. Thus, its use allows for the preservation of the original specimens and enables their use in other tests and analyses [36].
Regarding marginal adaptation, no significant differences between the materials were observed in the present study. In addition, as noted for the property of strength of the joint, the number of articles that investigated the marginal adaptation between white MTA, MTA HP, and Biodentine is also minimal.
In line with the findings of this study, previous assessments have also detected similarities in the marginal adaptation of MTA and Biodentine when compared to two other calcium-silicate-based cements [37]. The authors attribute this to calcium silicate being the main constituent of these materials, as well as methodological similarities in sample preparation and material handling and insertion, which create similar consistencies and flow [37,38]. Findings from other studies also reveal the absence of significant differences between gap percentages and diameter in the interface when comparing MTA and Biodentine cement [11,39,40].
It is relevant to note that the present study has limitations resulting from an in vitro investigation. In addition, the sample comprised simulated immature teeth since the selection of human teeth in this condition, which would be ideal, is impractical. In addition, it is important to consider the limitations of the methodology used in relation to the gap assessment resource. If we consider sealing ability as the seal reproduction in the whole canal perimeter, a gap may not represent what has actually occurred in the entire apical plug. Therefore, it is extremely difficult to establish a correlation between sealing ability and marginal adaptation.
Considering the similar and excellent results for MTA application in recent years, it seems appropriate to emphasize the importance of the findings observed herein. Thus, the improvement in the clinical applicability of MTA Repair HP qualifies it as a highly suitable material, especially compared to white MTA. At the same time, the results obtained for the Biodentine cement also seem favorable since this material was developed to replace dentin, and its applicability has been proven in several therapies. Future studies are needed to corroborate the results of this study and to investigate the behavior of these materials when exposed to in vivo conditions.
CONCLUSIONS
Based on the results reported herein, it can be concluded that the bond strength and marginal adaptation quality of calcium silicate cement-based on MTA Repair HP, Biodentine, and white MTA are comparable when used as apical plugs.
ACKNOWLEDGEMENTS
School of Dentistry - Federal University of Minas Gerais - UFMG for using the testing machine (Instron Model 3344; Instron, Norwood, MA, USA) and carrying out the push-out test.
-
Funding: This study was financed in part by the Coordenação de Aperfeiçoamento de Pessoal de Nível Superior Brasil (CAPES) - Finance Code 001. MCRH is a research fellow of Fundação de Amparo à Pesquisa do Estado de Minas Gerais (FAPEMIG CDS-PPM-00653-16).
-
Conflict of Interest: No potential conflict of interest relevant to this article was reported.
-
Author Contributions:
Conceptualization: Sá MAB, Nunes E, Brito Jr M, Silveira FF.
Data curation: Sá MAB, Nunes E, Brito Jr M, Amaral RR, Silveira FF, Horta MCR, Antunes ANG, Cohen S.
formal analysis: Sá MAB, Horta MCR, Silveira FF.
Funding acquisition: Sá MAB, Brito Jr M, Silveira FF.
Investigation: Sá MAB, Silveira FF.
Methodology: Sá MAB, Brito Jr M, Silveira FF, Antunes ANG.
Project administration: Sá MAB, Brito Jr M, Silveira FF.
resources: Sá MAB, Silveira FF.
Software: Silveira FF, Horta MCR.
Supervision: Sá MAB, Nunes E, Brito Jr M, Amaral RR, Silveira FF, Horta MCR, Antunes ANG, Cohen S.
Validation: Sá MAB, Nunes E, Brito Jr M, Amaral RR, Silveira FF, Horta MCR, Antunes ANG, Cohen S.
Visualization: Sá MAB, Nunes E, Brito Jr M, Amaral RR, Silveira FF, Horta MCR, Antunes ANG, Cohen S.
Writing original draft: Sá MAB, Silveira FF.
Writing review and editing: Sá MAB, Nunes E, Brito Jr M, Amaral RR, Silveira FF, Horta MCR, Antunes ANG, Cohen S.
- 1. Sisli SN, Ozbas H. Comparative micro-computed tomographic evaluation of the sealing quality of ProRoot MTA and MTA Angelus apical plugs placed with various techniques. J Endod 2017;43:147-151.ArticlePubMed
- 2. Torabinejad M, Parirokh M, Dummer PM. Mineral trioxide aggregate and other bioactive endodontic cements: an updated overview - part II: other clinical applications and complications. Int Endod J 2018;51:284-317.ArticlePubMedPDF
- 3. Ber BS, Hatton JF, Stewart GP. Chemical modification of ProRoot MTA to improve handling characteristics and decrease setting time. J Endod 2007;33:1231-1234.ArticlePubMed
- 4. Guimarães BM, Prati C, Duarte MA, Bramante CM, Gandolfi MG. Physicochemical properties of calcium silicate-based formulations MTA Repair HP and MTA Vitalcem. J Appl Oral Sci 2018;26:e2017115.PubMedPMC
- 5. Marciano MA, Costa RM, Camilleri J, Mondelli RF, Guimarães BM, Duarte MA. Assessment of color stability of white mineral trioxide aggregate angelus and bismuth oxide in contact with tooth structure. J Endod 2014;40:1235-1240.ArticlePubMed
- 6. Możyńska J, Metlerski M, Lipski M, Nowicka A. Tooth discoloration induced by different calcium silicate-based cements: a systematic review of in vitro studies. J Endod 2017;43:1593-1601.PubMed
- 7. Rajasekharan S, Martens LC, Cauwels RG, Anthonappa RP, Verbeeck RM. Biodentine™ material characteristics and clinical applications: a 3 year literature review and update. Eur Arch Paediatr Dent 2018;19:1-22.ArticlePubMedPDF
- 8. Vidal K, Martin G, Lozano O, Salas M, Trigueros J, Aguilar G. Apical closure in apexification: a review and case report of apexification treatment of an immature permanent tooth with Biodentine. J Endod 2016;42:730-734.ArticlePubMed
- 9. Hachmeister DR, Schindler WG, Walker WA 3rd, Thomas DD. The sealing ability and retention characteristics of mineral trioxide aggregate in a model of apexification. J Endod 2002;28:386-390.ArticlePubMed
- 10. Yilmaz Z, Küçükkaya Eren S, Uzunoğlu E, Görduysus M, Görduysus MÖ. Interaction of backfilling techniques and MTA plugs with additives: Fracture strength and adaptation analyses. Dent Mater J 2017;36:809-815.ArticlePubMed
- 11. Kadić S, Baraba A, Miletić I, Ionescu A, Brambilla E, Ivanišević Malčić A, Gabrić D. Push-out bond strength of three different calcium silicate-based root-end filling materials after ultrasonic retrograde cavity preparation. Clin Oral Investig 2018;22:1559-1565.ArticlePubMedPDF
- 12. Tran D, He J, Glickman GN, Woodmansey KF. Comparative analysis of calcium silicate-based root filling materials using an open apex model. J Endod 2016;42:654-658.ArticlePubMed
- 13. Araújo AC, Nunes E, Fonseca AA, Cortes MI, Horta MC, Silveira FF. Influence of smear layer removal and application mode of MTA on the marginal adaptation in immature teeth: a SEM analysis. Dent Traumatol 2013;29:212-217.PubMed
- 14. Bidar M, Disfani R, Gharagozloo S, Khoynezhad S, Rouhani A. Medication with calcium hydroxide improved marginal adaptation of mineral trioxide aggregate apical barrier. J Endod 2010;36:1679-1682.ArticlePubMed
- 15. López-García S, Pecci-Lloret MP, Pecci-Lloret MR, Oñate-Sánchez RE, García-Bernal D, Castelo-Baz P, Rodríguez-Lozano FJ, Guerrero-Gironés J. In vitro evaluation of the biological effects of ACTIVA Kids BioACTIVE Restorative, Ionolux, and Riva Light Cure on human dental pulp stem cells. Materials (Basel) 2019;12:3694-3705.PubMedPMC
- 16. Ertas H, Kucukyilmaz E, Ok E, Uysal B. Push-out bond strength of different mineral trioxide aggregates. Eur J Dent 2014;8:348-352.ArticlePubMedPMC
- 17. Shokouhinejad N, Yazdi KA, Nekoofar MH, Matmir S, Khoshkhounejad M. Effect of acidic environment on dislocation resistance of endosequence root repair material and mineral trioxide aggregate. J Dent (Tehran) 2014;11:161-166.PubMedPMC
- 18. Thompson JI, Gregson PJ, Revell PA. Analysis of push-out test data based on interfacial fracture energy. J Mater Sci Mater Med 1999;10:863-868.ArticlePubMedPDF
- 19. Saghiri MA, Garcia-Godoy F, Gutmann JL, Lotfi M, Asatourian A, Ahmadi H. Push-out bond strength of a nano-modified mineral trioxide aggregate. Dent Traumatol 2013;29:323-327.ArticlePubMed
- 20. Shokouhinejad N, Nekoofar MH, Iravani A, Kharrazifard MJ, Dummer PM. Effect of acidic environment on the push-out bond strength of mineral trioxide aggregate. J Endod 2010;36:871-874.ArticlePubMed
- 21. Camilleri J. The chemical composition of mineral trioxide aggregate. J Conserv Dent 2008;11:141-143.ArticlePubMedPMC
- 22. Stefaneli Marques JH, Silva-Sousa YT, Rached-Júnior FJ, Macedo LM, Mazzi-Chaves JF, Camilleri J, Sousa-Neto MD. Push-out bond strength of different tricalcium silicate-based filling materials to root dentin. Braz Oral Res 2018;32:e18.PubMed
- 23. Silva EJ, Carvalho NK, Zanon M, Senna PM, De-Deus G, Zuolo ML, Zaia AA. Push-out bond strength of MTA HP, a new high-plasticity calcium silicate-based cement. Braz Oral Res 2016;30:S1806-83242016000100269.ArticlePubMed
- 24. Bodanezi A, Carvalho N, Silva D, Bernardineli N, Bramante CM, Garcia RB, de Moraes IG. Immediate and delayed solubility of mineral trioxide aggregate and Portland cement. J Appl Oral Sci 2008;16:127-131.ArticlePubMedPMC
- 25. Bachoo IK, Seymour D, Brunton P. A biocompatible and bioactive replacement for dentine: is this a reality? The properties and uses of a novel calcium-based cement. Br Dent J 2013;214:E5.ArticlePubMedPDF
- 26. Stabholz A, Friedman S, Abed J. Marginal adaptation of retrograde fillings and its correlation with sealability. J Endod 1985;11:218-223.ArticlePubMed
- 27. Johnson BR. Considerations in the selection of a root-end filling material. Oral Surg Oral Med Oral Pathol Oral Radiol Endod 1999;87:398-404.ArticlePubMed
- 28. Zafar M, Iravani M, Eghbal MJ, Asgary S. Coronal and apical sealing ability of a new endodontic cement. Iran Endod J 2009;4:15-19.PubMedPMC
- 29. Bolhari B, Ashofteh Yazdi K, Sharifi F, Pirmoazen S. Comparative scanning electron microscopic study of the marginal adaptation of four root-end filling materials in presence and absence of blood. J Dent (Tehran) 2015;12:226-234.PubMedPMC
- 30. Shokouhinejad N, Nekoofar MH, Ashoftehyazdi K, Zahraee S, Khoshkhounejad M. Marginal adaptation of new bioceramic materials and mineral trioxide aggregate: a scanning electron microscopy study. Iran Endod J 2014;9:144-148.PubMedPMC
- 31. Costa AT, Konrath F, Dedavid B, Weber JB, de Oliveira MG. Marginal adaptation of root-end filling materials: an in vitro study with teeth and replicas. J Contemp Dent Pract 2009;10:75-82.
- 32. Badr AE. Marginal adaptation and cytotoxicity of bone cement compared with amalgam and mineral trioxide aggregate as root-end filling materials. J Endod 2010;36:1056-1060.ArticlePubMed
- 33. Gondim E Jr, Zaia AA, Gomes BP, Ferraz CC, Teixeira FB, Souza-Filho FJ. Investigation of the marginal adaptation of root-end filling materials in root-end cavities prepared with ultrasonic tips. Int Endod J 2003;36:491-499.ArticlePubMedPDF
- 34. Teaford MF, Oyen OJ. Live primates and dental replication: new problems and new techniques. Am J Phys Anthropol 1989;80:73-81.ArticlePubMed
- 35. Gondim E Jr, Gomes BP, Ferraz CC, Teixeira FB, Souza-Filho FJ. Effect of sonic and ultrasonic retrograde cavity preparation on the integrity of root apices of freshly extracted human teeth: scanning electron microscopy analysis. J Endod 2002;28:646-650.ArticlePubMed
- 36. Bocker C, Kracker M, Rüssel C. Replica extraction method on nanostructured gold coatings and orientation determination combining SEM and TEM techniques. Microsc Microanal 2014;20:1654-1661.ArticlePubMed
- 37. Küçükkaya Eren S, Görduysus MÖ, Şahin C. Sealing ability and adaptation of root-end filling materials in cavities prepared with different techniques. Microsc Res Tech 2017;80:756-762.PubMed
- 38. Bolhari B, Yazdi KA, Sharifi F, Pirmoazen S. Comparative scanning electron microscopic study of the marginal adaptation of four root-end filling materials in presence and absence of blood. J Dent (Tehran) 2015;12:226-234.PubMedPMC
- 39. Torres FFE, Jacobs R, EzEldeen M, Guerreiro-Tanomaru JM, Dos Santos BC, Lucas-Oliveira É, Bonagamba TJ, Tanomaru-Filho M. Micro-computed tomography high resolution evaluation of dimensional and morphological changes of 3 root-end filling materials in simulated physiological conditions. J Mater Sci Mater Med 2020;31:14.ArticlePubMedPDF
- 40. Küçükkaya Eren S, Aksel H, Askerbeyli Örs S, Serper A, Koçak Y, Ocak M, Çelik HH. Obturation quality of calcium silicate-based cements placed with different techniques in teeth with perforating internal root resorption: a micro-computed tomographic study. Clin Oral Investig 2019;23:805-811.ArticlePubMedPDF
REFERENCES
Tables & Figures
REFERENCES
Citations
Citations to this article as recorded by 
- Evaluation of marginal adaptation and bond strength of apical root canal plugs using different bioceramic cements
Michel Sena Fernandes Faria Lima, Alberto Nogueira da Gama Antunes, Kênia Maria Pereira Soares de Toubes, Fábio Fernandes Borém Bruzinga, Camila de Sousa Caneschi, Luís Fernando dos Santos Alves Morgan, Frank Ferreira Silveira
BMC Oral Health.2026;[Epub] CrossRef - Application of Biodentine for Apexification of Immature Teeth of Children: A Scoping Review
Liz M Gerard, Sumit Gaur
International Journal of Clinical Pediatric Dentistry.2025; 18(5): 573. CrossRef - Evaluation of the root dentin bond strength and intratubular biomineralization of a premixed calcium aluminate-based hydraulic bioceramic endodontic sealer
Yu-Na Lee, Min-Kyeong Kim, Hee-Jin Kim, Mi-Kyung Yu, Kwang-Won Lee, Kyung-San Min
Journal of Oral Science.2024; 66(2): 96. CrossRef - Managing Cracked Teeth with Root Extension: A Prospective Preliminary Study Using Biodentine™ Material
Kênia Maria Soares de Toubes, Isabella Sousa Corrêa, Regina Célia Lopes Valadares, Stephanie Quadros Tonelli, Fábio Fernandes Borém Bruzinga, Frank Ferreira Silveira, Dr Karthikeyan Ramalingam
International Journal of Dentistry.2024;[Epub] CrossRef - Marginal adaptation of customized gutta percha cone with calcium silicate based sealer versus MTA and biodentine apical plugs in simulated immature permanent teeth (an in vitro study)
Mary M. Mina, Sybel M. Moussa, Mahmoud R. Aboelseoud
BMC Oral Health.2024;[Epub] CrossRef - Comparative Evaluation of Push-Out Bond Strength of Conventional Mineral Trioxide Aggregate, Biodentine, a Modified Mineral Trioxide Aggregate, and Two Novel Antibacterial-Enhanced Mineral Trioxide Aggregates
Arokia Rajkumar Shancy Merlin, Vignesh Ravindran, Ganesh Jeevanandan, Rajalakshmanan Eswaramoorthy, Abirami Arthanari
Cureus.2024;[Epub] CrossRef - Push out bond strength of hydraulic cements used at different thicknesses
C. Ruiz Durán, Dra L. Gancedo-Caravia, V. Vera González, C. González Losada
BMC Oral Health.2023;[Epub] CrossRef - Effects of different calcium-silicate based materials on fracture resistance of immature permanent teeth with replacement root resorption and osteoclastogenesis
Gabriela Leite de Souza, Gabrielle Alves Nunes Freitas, Maria Tereza Hordones Ribeiro, Nelly Xiomara Alvarado Lemus, Carlos José Soares, Camilla Christian Gomes Moura
Restorative Dentistry & Endodontics.2023;[Epub] CrossRef
 ePub Link
ePub Link Cite
CitePush-out bond strength and marginal adaptation of apical plugs with bioactive endodontic cements in simulated immature teeth
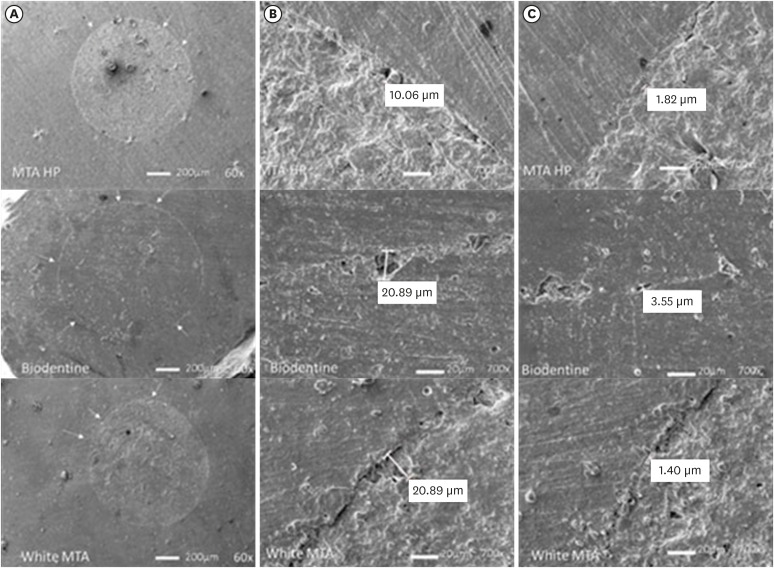
Figure 1 Scanning electron microscope resin replica photomicrographies of HP MTA, Biodentine and white MTA cements. Plug circumference (A); Largest gap (B); Smallest gap (C). Arrows indicate small defects seen at 60× magnification. The largest and smallest gaps are shown at 700×.MTA, mineral trioxide aggregate.
Figure 1
Push-out bond strength and marginal adaptation of apical plugs with bioactive endodontic cements in simulated immature teeth
Composition of calcium silicate cements used, along with the manufacture instruction of its manipulation
| Calcium silicate cement | Composition | Manufacture instruction of its manipulation |
|---|---|---|
| MTA Repair HP | Powder: Tricalcium silicate 3CaO, SiO2; Dicalcium silicate 2CaO.SiO2; Tricalcium aluminate 3CaO.Al2O3; Oxide Calcium CaO; Calcium Tungsate CaWO4 | 1) Dispense the contents of 1 pack of MTA Repair HP and 2 drops of liquid on the glass plate; 2) Mix for 40 seconds. until complete homogenization of the powder and liquid. The cement obtained is similar to a modeling clay; 3) Take the MTA Repair HP to the desired location with an MTA carrier condensing it with appropriate instruments for this purpose. |
| Liquid: Water and Plasticizer | ||
| Biodentine | Powder: Tricalcium silicate, zirconium oxide, calcium oxide, yellow pigment, red pigment, brown iron oxide | 1) Open a capsule and place it in the capsule holder; 2) Detach an ampoule containing the liquid and gently tap the cap to force all the liquid to flow into the flacon; 3) Rotate the lid to open; 4) Place 5 drops of liquid in the capsule; 5) Close the capsule. Place it and an amalgamator at a speed of 4,000–4,200 revolutions min; 6) Let it stir for 30 seconds; 7) Open the capsule and check the consistency of the material; 8) Remove the Biodentine with the help of the spatula provided. Depending on the desired application, it is possible to apply Biodentine with an amalgam holder, a spatula or an MTA carrier. |
| Liquid: Calcium chloride dihydrate, air, purified water | ||
| White MTA | Tricalcium silicate, dicalcium silicate, tricalcium aluminate, calcium oxide, bismuth oxide | 1) Mix for 30 seconds the content of 1 sachet of (or 1 spoon) with 1 drop of distilled water. The mixture should be homogeneous and with a consistency similar to wet sand; 2) Place the cement on the selected site with a sterilized amalgam carrier or other appropriate instrument; 3) Condense the cement with instruments such as amalgam condensers, a number 1 spatula or absorbent paper points moistened with distilled water. |
MTA, mineral trioxide aggregate.
Means and standard deviations of the bond strength values and comparisons among the investigated groups
| Root dentin slices | MTA Repair HP (group 1) | Biodentine (group 2) | White MTA (group 3) | |||
|---|---|---|---|---|---|---|
| Mean ± SD | Mean ± SD | Mean ± SD | 1 × 2 | 1 × 3 | 2 × 3 | |
| Apical | 17.69 ± 8.00 | 12.97 ± 10.89 | 16.60 ± 7.80 | ns | ns | ns |
| Cervical | 27.53 ± 6.49 | 17.68 ± 9.51 | 23.42 ± 11.17 | ns | ns | ns |
| Mean values of both slices | 22.61 ± 5.07 | 15.32 ± 8.47 | 20.01 ± 7.09 | ns | ns | ns |
MTA, mineral trioxide aggregate; SD, standard deviation; ns, not significant (
*
Median, minimum and maximum gap values and comparisons among groups
| Root dentin slices | MTA Repair HP (group 1) | Biodentine (group 2) | White MTA (group 3) | |||
|---|---|---|---|---|---|---|
| Median (minimum–maximum) | Median (minimum–maximum) | Median (minimum–maximum) | 1 × 2 | 1 × 3 | 2 × 3 | |
| Apical (largest gap) | 15.78 (0.00–86.03) | 18.68 (5.94–55.07) | 29.86 (1.33–71.62) | ns | ns | ns |
| Cervical (largest gap) | 7.86 (0.00–411.0) | 19.72 (5.02–145.5) | 45.68 (4.13–208.4) | ns | ns | ns |
| Apical (smallest gap) | 1.48 (0.00–25.96) | 2.37 (0.82–8.87) | 1.52 (0.58–87.54) | ns | ns | ns |
| Cervical (smallest gap) | 1.11 (0.00–6.82) | 2.62 (0.00–12.48) | 6.26 (0.75–21.20) | ns | < 0.05 | ns |
MTA, mineral trioxide aggregate; ns, not significant (
*
Table 1 Composition of calcium silicate cements used, along with the manufacture instruction of its manipulation
MTA, mineral trioxide aggregate.
Table 2 Means and standard deviations of the bond strength values and comparisons among the investigated groups
MTA, mineral trioxide aggregate; SD, standard deviation; ns, not significant (
*
Table 3 Median, minimum and maximum gap values and comparisons among groups
MTA, mineral trioxide aggregate; ns, not significant (
*

