
Articles
- Page Path
- HOME > Restor Dent Endod > Volume 45(2); 2020 > Article
- Case Report Observation of an extracted premolar 2.5 years after mineral trioxide aggregate apexification using micro-computed tomography
-
Gayeon Lee1
 , Chooryung Chung2, Sunil Kim3, Su-Jung Shin1
, Chooryung Chung2, Sunil Kim3, Su-Jung Shin1 -
Restor Dent Endod 2019;45(2):e4.
DOI: https://doi.org/10.5395/rde.2020.45.e4
Published online: November 22, 2019
1Department of Conservative Dentistry, Gangnam Severance Hospital, Yonsei University College of Dentistry, Seoul, Korea.
2Department of Orthodontics, Gangnam Severance Hospital, Yonsei University College of Dentistry, Seoul, Korea.
3Department of Conservative Dentistry, Yonsei University College of Dentistry, Seoul, Korea.
- Correspondence to Su-Jung Shin, DDS, PhD. Professor, Department of Conservative Dentistry, Gangnam Severance Hospital, Yonsei University College of Dentistry, 211 Eonju-ro, Gangnam-gu, Seoul 06273 Korea. sujungshin@yuhs.ac
- Correspondence to Sunil Kim, DDS, PhD. Professor, Microscope Center, Department of Conservative Dentistry and Oral Science Research Center, Yonsei University College of Dentistry, 50-1 Yonsei-ro, Seodaemun-gu, Seoul 03722, Korea. seone1@yuhs.ac
• Received: September 7, 2019 • Revised: October 5, 2019 • Accepted: October 7, 2019
Copyright © 2020. The Korean Academy of Conservative Dentistry
This is an Open Access article distributed under the terms of the Creative Commons Attribution Non-Commercial License (https://creativecommons.org/licenses/by-nc/4.0/) which permits unrestricted non-commercial use, distribution, and reproduction in any medium, provided the original work is properly cited.
- 2,005 Views
- 16 Download
- 1 Crossref
Abstract
- Although numerous studies have been conducted on apexification using mineral trioxide aggregate (MTA), direct observation of extracted human teeth after the procedure has been rarely reported. This case report describes a mandibular premolar treated 2.5 years ago and extracted recently for orthodontic treatment. The tubercle of the right mandibular premolar of a 12-year-old boy with dens evaginatus was fractured and the pulp was exposed. The tooth was diagnosed with pulp necrosis and asymptomatic periapical abscess. During the first visit, copious irrigation was performed with 2.5% sodium hypochlorite. Calcium hydroxide paste was placed as an intracanal medicament. The sinus tract had disappeared at the second visit after 3 weeks. MTA was applied on to the bleeding point as a 4-mm-thick layer, followed by a 3-mm-thick gutta-percha filling and resin core build-up. After 2.5 years, the tooth and three other premolars were extracted for orthodontic treatment. The right and left mandibular premolars were scanned with micro-computed tomography to determine the root shape and canal anatomy. Irregular root growth was observed and the root outline of the right mandibular premolar differed from that of the contralateral tooth. Apexification with MTA leads to the formation of roots with irregular morphology, without any pulpal space.
INTRODUCTION
Single-visit apexification has been used for the endodontic treatment of teeth with necrotic pulps and open apices [1,2]. Single one-visit apexification has taken precedence over the previous technique that used calcium hydroxide, after the introduction of calcium silicate cements, including ProRoot mineral trioxide aggregate (MTA) (Dentsply-Sirona, Ballaigues, Switzerland) [2]. Witherspoon et al. [2] reported that over 90% of teeth treated with MTA demonstrated healing. Although pulp regeneration therapy has become an increasingly valuable and standard protocol in current endodontic practice [3,4,5,6], apexification has been reported as a successful treatment option [7]. Alobaid et al. [7] reported a favorable result in their retrospective cohort study, with retention of 100% of teeth in recalled cases, following apexification. There have been several case reports and clinical studies related to MTA apexification or revascularization [8,9,10]; however, direct observation of extracted human teeth after apexification using an MTA barrier has been rarely reported. Several histological studies on extracted human teeth after pulp regenerative therapy have been conducted [11,12,13]. Herein, we report a case of an extracted lower premolar that was endodontically treated 2.5 years ago using apexification with MTA barrier and extracted recently for orthodontic treatment.
CASE REPORT
A 12-year old boy was referred to our institution for the evaluation and treatment of the right mandibular premolar (tooth #45) (Figure 1A and 1E). He had experienced swelling and pain on the gingiva and mucosa of tooth #45 several days before the visit. A sinus tract with purulent discharge was observed and there was no response to cold and electric pulp testing with tooth #45. The tubercle of the dens evaginatus tooth had fractured, with pulp exposure. Tooth #45 was diagnosed with pulp necrosis and an asymptomatic apical abscess due to dens evaginatus. Regenerative pulp treatment was planned initially, and the access cavity was prepared under isolation. During the first visit, copious irrigation was performed using 2.5% sodium hypochlorite (NaOCl), saline, and 17% ethylenediaminetetraacetic acid (EDTA) solution, with a 27-G needle with a rubber stopper, up to 1 mm short of the tentative length of root apex, followed by an intracanal dressing with a calcium hydroxide paste (Calcipex II, Nippon Shika Yakujin Co., Simonoseki, Japan). At the second visit after 3 weeks, the sinus tract had disappeared and the tooth was asymptomatic. The tooth was isolated and irrigated copiously with 2.5% NaOCl and 17% EDTA, following which bleeding was initiated using a curved K-type file (Dentsply-Sirona), without local anesthesia. However, the bleeding induced was insufficient and the bleeding point was detected 16 mm from the buccal cusp. Consequently, we decided to perform apexification using ProRoot MTA (Dentsply-Sirona). The cement was mixed with water according to the manufacturer's instructions and applied to the bleeding point as a 4-mm thick layer. After confirming that the MTA filling was 4–5 mm thick and without any defects, a 3-mm gutta-percha filling, and resin core build-up were performed using Tetric N-Ceram (Ivoclar-Vivadent, Schaan, Liechtenstein) and Clearfil SE bond (Kuraray Dental, New York, NY, USA) (Figure 1B). The patient was asymptomatic and root growth was observed at the 6-months recall (Figure 1C). The patient was asymptomatic for 1.5 years (Figure 1D).
Figure 1

Series of periapical radiographs taken during the treatment of tooth #45. (A) A preoperative periapical radiograph showing an immature root with periapical radiolucency with tooth #45. A gutta-percha cone was used to trace the periapical lesion to tooth #45. (B) A postoperative periapical radiograph showing apexification with tooth #45. (C) A periapical radiograph taken 6 months after the treatment demonstrating the resolution of the previous periapical radiolucency. (D) A periapical radiograph taken 1.5 years after the treatment showing the formation of the root apex. (E) A preoperative panoramic view. (F) A panoramic view taken 2.5 years after the root canal treatment with tooth #45.
op, operative.
This tooth and the other three second premolars were to be extracted for orthodontic treatment, 2.5 years after the endodontic treatment (Figure 1F). After obtaining the patient's written consent form, the extracted teeth (tooth #45 and its contralateral tooth, tooth #35) were scanned using micro-CT (SkyScan1173, Bruker-CT, Kontich, Belgium) to observe the root shape and canal anatomy (Figure 2).
Figure 2
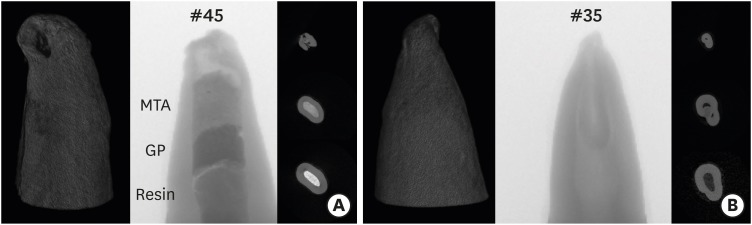
Reconstructed 3D images of teeth #45 and #35 obtained by micro-computed tomography. (A) Reconstructed 3D image of tooth #35. (B) Reconstructed 3D image of tooth #45.
3D, three-dimensional; MTA, mineral trioxide aggregate; GP, gutta-percha.
Micro-CT imaging revealed irregular root growth with tooth #45, after the apexification procedure. The outline of the root shape of tooth #45 was different from its contralateral tooth. The lengths of both premolars were similar. Dentinal bridge formation was not observed to be in direct contact with the MTA filling. The newly formed root portion seemed calcified without an obvious canal space (Figure 3).
Figure 3
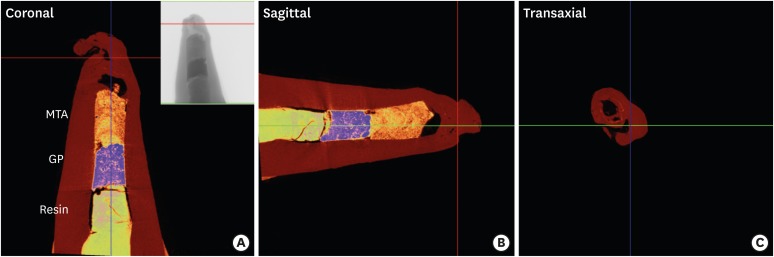
Representative colored images of tooth #45 obtained by micro-computed tomography (micro-CT). (A) A coronal image of micro-CT of tooth #45 showing composite resin, gutta-percha (GP), and mineral trioxide aggregate (MTA) filling in the canal. An irregularly shaped root tip was observed. (B) A sagittal image of tooth #45. (C) A transaxial view of tooth #45.
DISCUSSION
This case demonstrated an increase in the root length, although the results of earlier studies have been controversial. There was no root length increase in the teeth treated by MTA apexification in some studies [14,15]. However, Alobaid et al. [7] demonstrated that the apexification group also showed an increase in root length and width. We speculated that root growth occurred in this case, due to some leftover vital tissue at the apical portion, since we tried to induce bleeding before MTA apexification.
As discussed previously, a pulp regenerative therapy would have been a better choice in this case. As described in the case report section, the bleeding induced up to coronal root was insufficient. Moreover, there was concern regarding irritating the mental foramen, which appeared close on radiographs, if the K-file was extruded further beyond the apex. Another concern was the lack of sufficient bleeding after manipulation with the K-file. During the first visit, calcium hydroxide paste was applied, which could have dissolved some vital tissue around the root apex. Yassen et al. [16] demonstrated superficial collagen degradation in the radicular dentin, if calcium hydroxide was used as an intracanal medicament. Some studies [17,18] advocated the usage of triple antibiotic paste, although the best intracanal medicament is still controversial [3,16].
Hard tissue formation around the MTA filling was an interesting finding of micro-CT imaging. MTA enhances osteogenesis/dentinogenesis by pulp cells or other cells [19]. Yan et al. [19] claimed that MTA could induce dentinogenesis and osteogenesis by apical papillary stem cells. A gap was observed between the MTA filling and hard tissue in this case. This was a limitation of micro-CT evaluation, since we were unable to confirm the nature of this gap. An animal study by Tobias Duarte et al. [20] showed that vital tissue was observed in 67% of specimens after complete pulpal necrosis in immature rat teeth.
Although we tried to obtain a histological section of #45, the specimen had unfortunately broken during sectioning of the decalcified tooth. The thick composite filling may have damaged the tooth specimen damaged during sectioning. Norstat et al. [11] reported that they removed the glass ionomer filling before embedding the histologic section. Peng et al. [12] demonstrated the presence of pulp-like tissue and cementocyte-like cells in the root canal space, in their study of an extracted lower premolar treated with pulp regeneration one year ago. They failed to demonstrate the interface between MTA filling and pulp space in their imaging findings. Another histological study by Norstat et al. [13] showed that MTA was involved in pulp regeneration and the pulp-like tissue was in direct contact with the layer of MTA. However, they used teeth extracted 4 months after regenerative treatment, which was considered a relatively short period for hard tissue formation.
To the best of our knowledge, this is the first case report demonstrating the morphology of a tooth treated by apexification using an MTA barrier and its contralateral tooth using micro-CT. The advantages of micro-CT observation included preservation of the tooth structure and precise observation of the root canal space and apical anatomy. Therefore, apexification or pulp regenerative therapy could be performed in young patients and more information could be obtained if these teeth require extraction for orthodontic or other purposes.
CONCLUSIONS
There was an irregular root growth observed in the tooth after apexification with MTA barrier. The outline of the root shape and canal system of tooth #45 was different from its contralateral tooth.
-
Funding: This study was supported by the National Research Foundation of Korea (NRF) grant funded by the Korea government (MSIP) (No. 2017R1A2B1008405).
-
Conflict of Interest: No potential conflict of interest relevant to this article was reported.
-
Author Contributions:
Conceptualization: Lee GY, Kim S, Chung C, Shin SJ.
Data curation: Chung C, Shin SJ.
Formal analysis: Kim S, Shin SJ.
Funding acquisition: Shin SJ.
Investigation: Lee GY, Kim S, Shin SJ.
Methodology: Chung C, Shin SJ.
Project administration: Shin SJ.
Resources: Shin SJ.
Software: Lee GY.
Supervision: Shin SJ.
Validation: Kim S, Chung C, Shin SJ.
Visualization: Lee GY.
Writing - original draft: Lee GY.
Writing - review & editing: Kim S, Chung C, Shin SJ.
- 1. Simon S, Rilliard F, Berdal A, Machtou P. The use of mineral trioxide aggregate in one-visit apexification treatment: a prospective study. Int Endod J 2007;40:186-197.ArticlePubMed
- 2. Witherspoon DE, Small JC, Regan JD, Nunn M. Retrospective analysis of open apex teeth obturated with mineral trioxide aggregate. J Endod 2008;34:1171-1176.ArticlePubMed
- 3. Farhad AR, Shokraneh A, Shekarchizade N. Regeneration or replacement? A case report and review of literature. Dent Traumatol 2016;32:71-79.ArticlePubMed
- 4. Huang GT. A paradigm shift in endodontic management of immature teeth: conservation of stem cells for regeneration. J Dent 2008;36:379-386.ArticlePubMed
- 5. Hargreaves KM, Diogenes A, Teixeira FB. Treatment options: biological basis of regenerative endodontic procedures. Pediatr Dent 2013;35:129-140.ArticlePubMed
- 6. Shabahang S. Treatment options: apexogenesis and apexification. J Endod 2013;39(Supplement):S26-S29.ArticlePubMed
- 7. Alobaid AS, Cortes LM, Lo J, Nguyen TT, Albert J, Abu-Melha AS, Lin LM, Gibbs JL. Radiographic and clinical outcomes of the treatment of immature permanent teeth by revascularization or apexification: a pilot retrospective cohort study. J Endod 2014;40:1063-1070.ArticlePubMedPMC
- 8. Fouad AF, Verma P. Healing after regenerative procedures with and without pulpal infection. J Endod 2014;40(Supplement):S58-S64.ArticlePubMed
- 9. Linsuwanont P, Sinpitaksakul P, Lertsakchai T. Evaluation of root maturation after revitalization in immature permanent teeth with nonvital pulps by cone beam computed tomography and conventional radiographs. Int Endod J 2017;50:836-846.ArticlePubMedPDF
- 10. Jung IY, Lee SJ, Hargreaves KM. Biologically based treatment of immature permanent teeth with pulpal necrosis: a case series. J Endod 2008;34:876-887.ArticlePubMed
- 11. Nosrat A, Kolahdouzan A, Hosseini F, Mehrizi EA, Verma P, Torabinejad M. Histologic outcomes of uninfected human immature teeth treated with regenerative endodontics: 2 case reports. J Endod 2015;41:1725-1729.ArticlePubMed
- 12. Peng C, Zhao Y, Wang W, Yang Y, Qin M, Ge L. Histologic findings of a human immature revascularized/regenerated tooth with symptomatic irreversible pulpitis. J Endod 2017;43:905-909.ArticlePubMed
- 13. Shimizu E, Jong G, Partridge N, Rosenberg PA, Lin LM. Histologic observation of a human immature permanent tooth with irreversible pulpitis after revascularization/regeneration procedure. J Endod 2012;38:1293-1297.ArticlePubMed
- 14. Bose R, Nummikoski P, Hargreaves K. A retrospective evaluation of radiographic outcomes in immature teeth with necrotic root canal systems treated with regenerative endodontic procedures. J Endod 2009;35:1343-1349.ArticlePubMed
- 15. Holden DT, Schwartz SA, Kirkpatrick TC, Schindler WG. Clinical outcomes of artificial root-end barriers with mineral trioxide aggregate in teeth with immature apices. J Endod 2008;34:812-817.ArticlePubMed
- 16. Yassen GH, Chu TM, Eckert G, Platt JA. Effect of medicaments used in endodontic regeneration technique on the chemical structure of human immature radicular dentin: an in vitro study. J Endod 2013;39:269-273.ArticlePubMed
- 17. Hoshino E, Kurihara-Ando N, Sato I, Uematsu H, Sato M, Kota K, Iwaku M. In-vitro antibacterial susceptibility of bacteria taken from infected root dentine to a mixture of ciprofloxacin, metronidazole and minocycline. Int Endod J 1996;29:125-130.ArticlePubMed
- 18. Windley W 3rd, Teixeira F, Levin L, Sigurdsson A, Trope M. Disinfection of immature teeth with a triple antibiotic paste. J Endod 2005;31:439-443.ArticlePubMed
- 19. Yan M, Wu J, Yu Y, Wang Y, Xie L, Zhang G, Yu J, Zhang C. Mineral trioxide aggregate promotes the odonto/osteogenic differentiation and dentinogenesis of stem cells from apical papilla via nuclear factor kappa B signaling pathway. J Endod 2014;40:640-647.ArticlePubMed
- 20. Tobias Duarte PC, Gomes-Filho JE, Ervolino E, Marçal Mazza Sundefeld ML, Tadahirowayama M, Lodi CS, Dezan-Júnior E, Angelo Cintra LT. Histopathological condition of the remaining tissues after endodontic infection of rat immature teeth. J Endod 2014;40:538-542.ArticlePubMed
REFERENCES
Tables & Figures
REFERENCES
Citations
Citations to this article as recorded by 
- Incorporation of amoxicillin-loaded microspheres in mineral trioxide aggregate cement: an in vitro study
Fábio Rocha Bohns, Vicente Castelo Branco Leitune, Isadora Martini Garcia, Bruna Genari, Nélio Bairros Dornelles, Silvia Stanisçuaski Guterres, Fabrício Aulo Ogliari, Mary Anne Sampaio de Melo, Fabrício Mezzomo Collares
Restorative Dentistry & Endodontics.2020;[Epub] CrossRef
 ePub Link
ePub Link Cite
CiteObservation of an extracted premolar 2.5 years after mineral trioxide aggregate apexification using micro-computed tomography
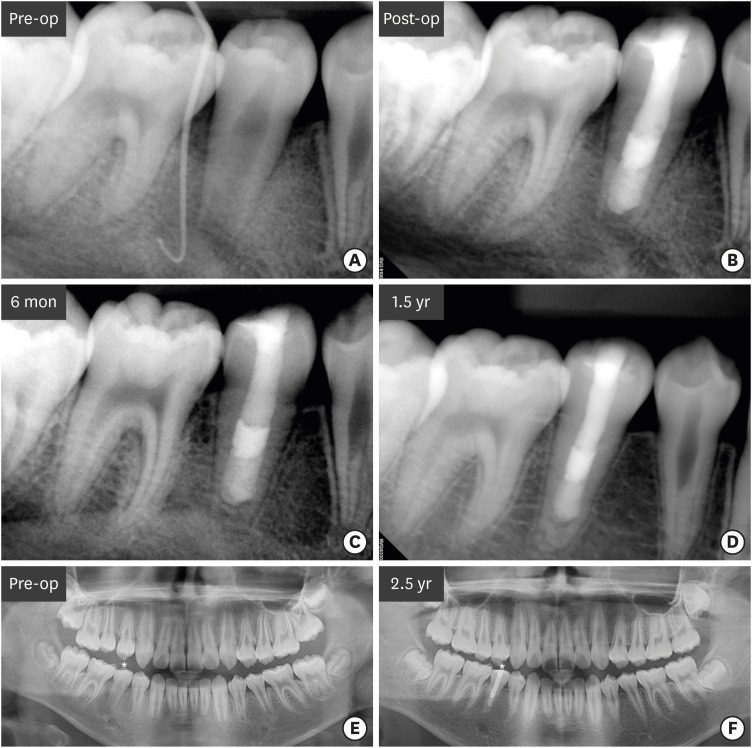
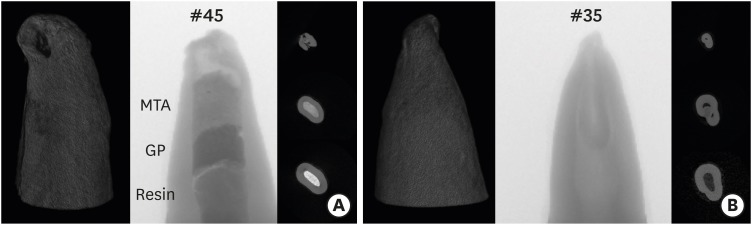
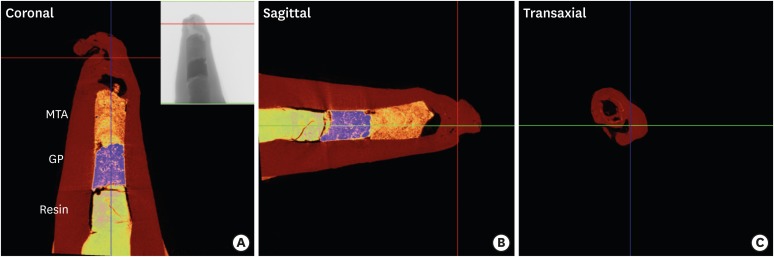
Figure 1 Series of periapical radiographs taken during the treatment of tooth #45. (A) A preoperative periapical radiograph showing an immature root with periapical radiolucency with tooth #45. A gutta-percha cone was used to trace the periapical lesion to tooth #45. (B) A postoperative periapical radiograph showing apexification with tooth #45. (C) A periapical radiograph taken 6 months after the treatment demonstrating the resolution of the previous periapical radiolucency. (D) A periapical radiograph taken 1.5 years after the treatment showing the formation of the root apex. (E) A preoperative panoramic view. (F) A panoramic view taken 2.5 years after the root canal treatment with tooth #45.op, operative.
Figure 2 Reconstructed 3D images of teeth #45 and #35 obtained by micro-computed tomography. (A) Reconstructed 3D image of tooth #35. (B) Reconstructed 3D image of tooth #45.3D, three-dimensional; MTA, mineral trioxide aggregate; GP, gutta-percha.
Figure 3 Representative colored images of tooth #45 obtained by micro-computed tomography (micro-CT). (A) A coronal image of micro-CT of tooth #45 showing composite resin, gutta-percha (GP), and mineral trioxide aggregate (MTA) filling in the canal. An irregularly shaped root tip was observed. (B) A sagittal image of tooth #45. (C) A transaxial view of tooth #45.
Figure 1
Figure 2
Figure 3
Observation of an extracted premolar 2.5 years after mineral trioxide aggregate apexification using micro-computed tomography

